SEARCH RESULTS FOR:
Myocardial Infarction: Findings on History
 L).(Onset: often at rest; crescendo)Activation of reflexive vagal responses (listed below)Weakness, dizziness, nausea, vomitingInflammatory mediators irritates nerves innervating the heart (the cardiac plexus)Cytokines act on hypothalamic T0 regulatorMild fever? Sweating (diaphoresis)Inflammatory cytokines can spread systemicallyBrain perceives nerve irritation as pain coming from T1-T4 dermatomesBlood backs up from the LV, into the left atrium and eventually accumulates in the pulmonary vasculatureHigh pulmonary venous blood pressure forces fluid out of capillaries, into pulmonary interstitium & alveoliRespiratory muscles work harder to ventilate lungsSoggier lung interstitium ? lung complianceDyspnea(Shortness of breath)Fluid compresses airways, ? resistance to airflow
102 kB / 204 words" title="Yu Yan - MI Findings on History - FINAL.pptx -
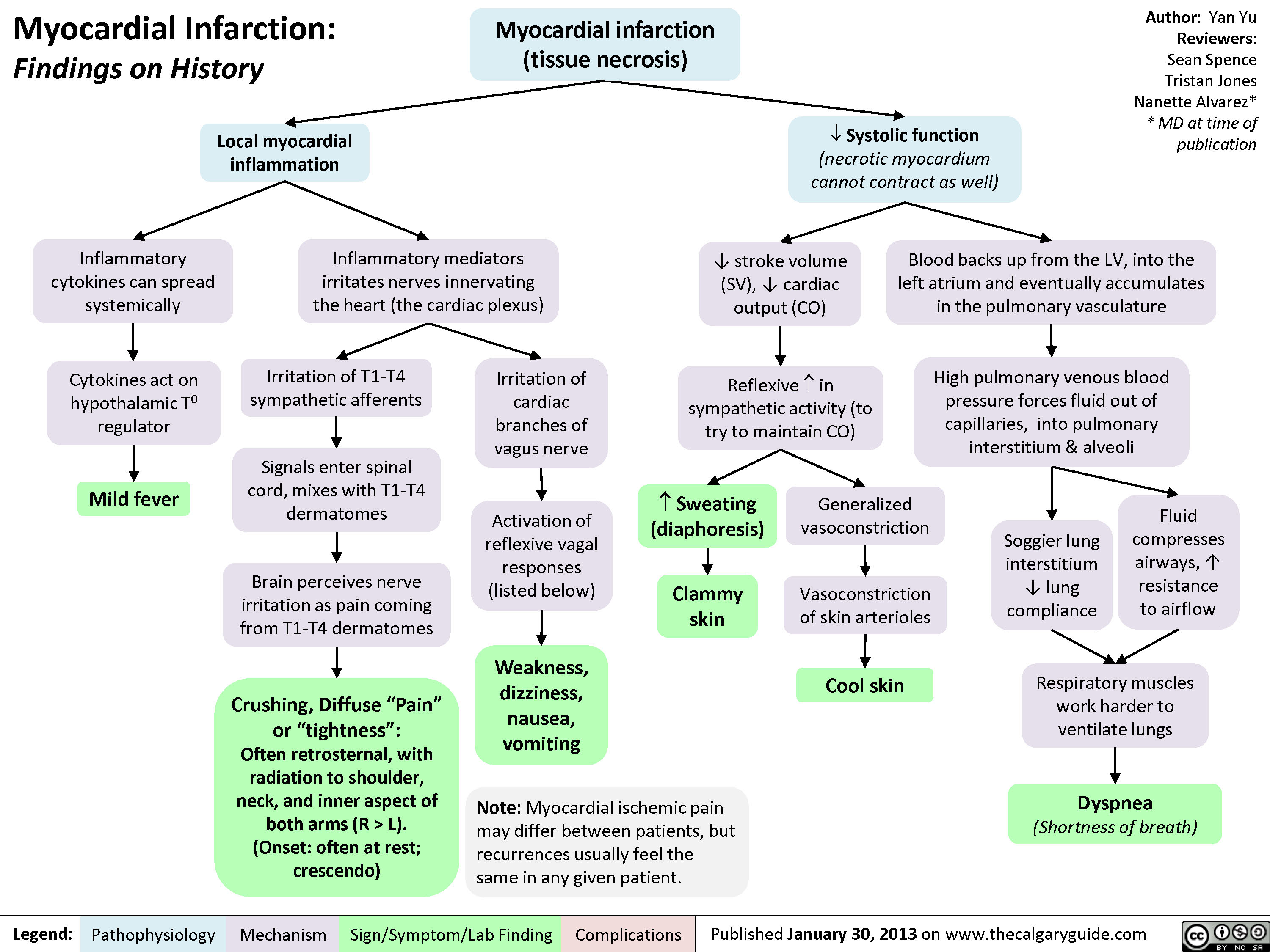
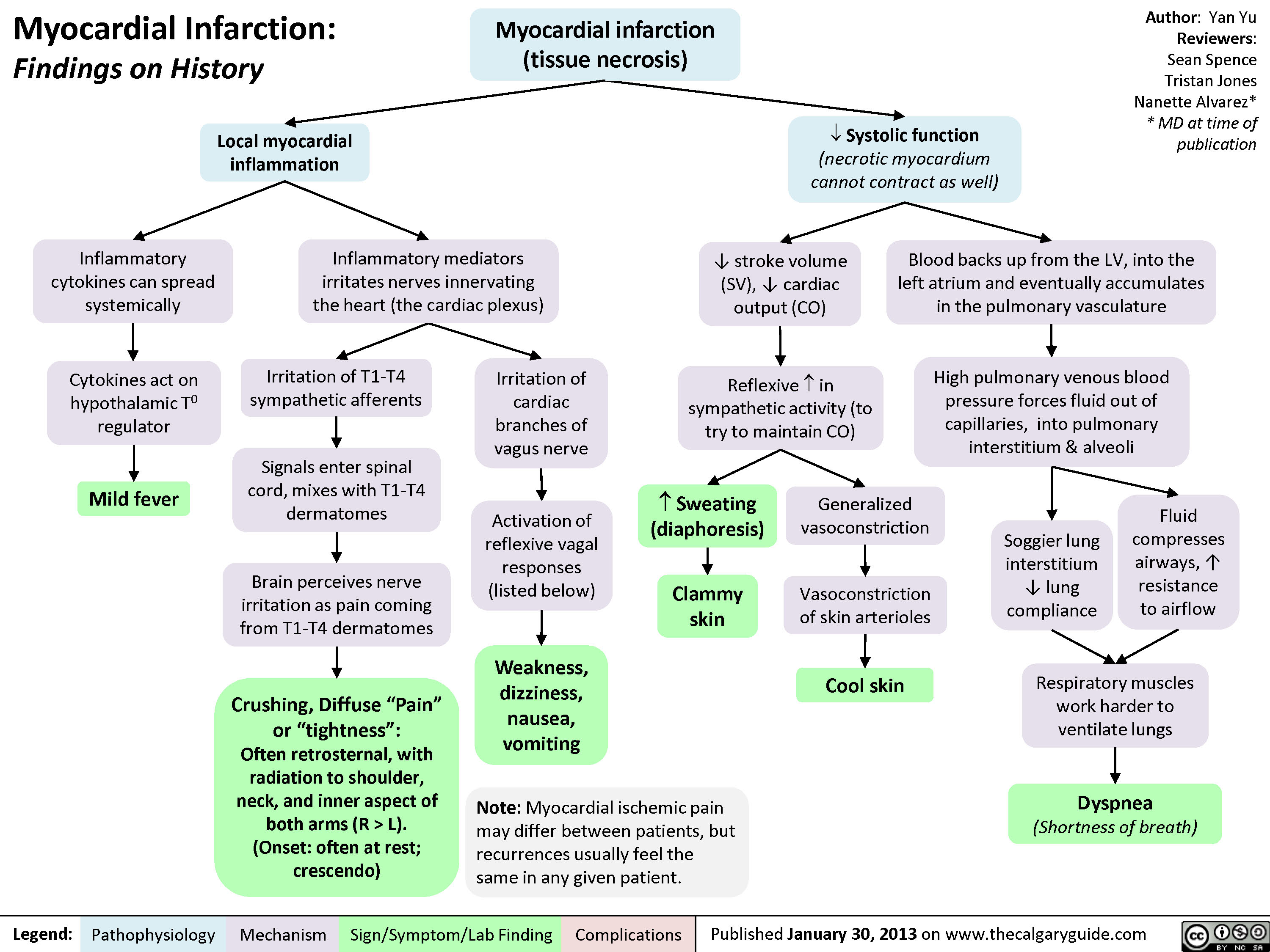
Myocardial Infarction: Findings on HistoryLegend:Published January 30, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsAuthor: Yan YuReviewers:Sean SpenceTristan JonesNanette Alvarez** MD at time of publication Systolic function(necrotic myocardium cannot contract as well)Reflexive ? in sympathetic activity (to try to maintain CO)Clammy skin? stroke volume (SV), ? cardiac output (CO)Myocardial infarction (tissue necrosis)Note: Myocardial ischemic pain may differ between patients, but recurrences usually feel the same in any given patient.Generalized vasoconstrictionVasoconstriction of skin arteriolesCool skinLocal myocardial inflammationIrritation of T1-T4 sympathetic afferentsIrritation of cardiac branches of vagus nerveSignals enter spinal cord, mixes with T1-T4 dermatomesCrushing, Diffuse "Pain" or "tightness": Often retrosternal, with radiation to shoulder, neck, and inner aspect of both arms (R > L).(Onset: often at rest; crescendo)Activation of reflexive vagal responses (listed below)Weakness, dizziness, nausea, vomitingInflammatory mediators irritates nerves innervating the heart (the cardiac plexus)Cytokines act on hypothalamic T0 regulatorMild fever? Sweating (diaphoresis)Inflammatory cytokines can spread systemicallyBrain perceives nerve irritation as pain coming from T1-T4 dermatomesBlood backs up from the LV, into the left atrium and eventually accumulates in the pulmonary vasculatureHigh pulmonary venous blood pressure forces fluid out of capillaries, into pulmonary interstitium & alveoliRespiratory muscles work harder to ventilate lungsSoggier lung interstitium ? lung complianceDyspnea(Shortness of breath)Fluid compresses airways, ? resistance to airflow
102 kB / 204 words" />
L).(Onset: often at rest; crescendo)Activation of reflexive vagal responses (listed below)Weakness, dizziness, nausea, vomitingInflammatory mediators irritates nerves innervating the heart (the cardiac plexus)Cytokines act on hypothalamic T0 regulatorMild fever? Sweating (diaphoresis)Inflammatory cytokines can spread systemicallyBrain perceives nerve irritation as pain coming from T1-T4 dermatomesBlood backs up from the LV, into the left atrium and eventually accumulates in the pulmonary vasculatureHigh pulmonary venous blood pressure forces fluid out of capillaries, into pulmonary interstitium & alveoliRespiratory muscles work harder to ventilate lungsSoggier lung interstitium ? lung complianceDyspnea(Shortness of breath)Fluid compresses airways, ? resistance to airflow
102 kB / 204 words" title="Yu Yan - MI Findings on History - FINAL.pptx -
Myocardial Infarction: Findings on HistoryLegend:Published January 30, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsAuthor: Yan YuReviewers:Sean SpenceTristan JonesNanette Alvarez** MD at time of publication Systolic function(necrotic myocardium cannot contract as well)Reflexive ? in sympathetic activity (to try to maintain CO)Clammy skin? stroke volume (SV), ? cardiac output (CO)Myocardial infarction (tissue necrosis)Note: Myocardial ischemic pain may differ between patients, but recurrences usually feel the same in any given patient.Generalized vasoconstrictionVasoconstriction of skin arteriolesCool skinLocal myocardial inflammationIrritation of T1-T4 sympathetic afferentsIrritation of cardiac branches of vagus nerveSignals enter spinal cord, mixes with T1-T4 dermatomesCrushing, Diffuse "Pain" or "tightness": Often retrosternal, with radiation to shoulder, neck, and inner aspect of both arms (R > L).(Onset: often at rest; crescendo)Activation of reflexive vagal responses (listed below)Weakness, dizziness, nausea, vomitingInflammatory mediators irritates nerves innervating the heart (the cardiac plexus)Cytokines act on hypothalamic T0 regulatorMild fever? Sweating (diaphoresis)Inflammatory cytokines can spread systemicallyBrain perceives nerve irritation as pain coming from T1-T4 dermatomesBlood backs up from the LV, into the left atrium and eventually accumulates in the pulmonary vasculatureHigh pulmonary venous blood pressure forces fluid out of capillaries, into pulmonary interstitium & alveoliRespiratory muscles work harder to ventilate lungsSoggier lung interstitium ? lung complianceDyspnea(Shortness of breath)Fluid compresses airways, ? resistance to airflow
102 kB / 204 words" />
process
lower-urinary-tract-infections-complications
, stagnant
urine (anatomical variant, obstruction,
neurogenic bladder, urinary reflux)
Bacterial entry (Less Common):
Indwelling catheter, surgical inoculation,
hematogenousspread, trauma
(Staphylococcus, Enterococcus, Candida)
Fecal bacteria access urethra
(E. coli, Proteus, Klebsiella)
Impairment of body's natural defense
systems, or stagnant urine, allow for
bacterial accumulation
Portal of entry bypasses body's physical
defenses (gravity and repetitive outward
urine flow)
Bacterial fimbriae and pili allow
them to ascend urethra and
adhere to epithelium
Lower Urinary Tract Infection (LUTI): Pathogenesis and clinical findings
Suprapubic
Tenderness
Bacterial colony irritates
urinary epithelium
Urgency:
Sensation of need to urinate
quickly or impending
incontinence
Stimulation of
inflammatory
response
Stimulation of urinary reflex
Pathogens use
enzymes to reduce
nitrate to nitrite
Delirium in Elderly
Frequency:
Repetitive need to
urinate
Unique response of altered fluid
status, electrolytes and mental
status, likely as a result of
increased inflammatory cytokines
Lower Urinary Tract Infection (“Cystitis”):
Infection of bladder or distal tract by capable bacteria
colonizing epithelium and causing symptoms
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications Published March 16, 2014 on www.thecalgaryguide.com
Author:
Brett Edwards
Reviewers:
Riley Hartmann
Jan Rudzinski
Haotian Wang
Steve Vaughan*
* MD at time of publication
Usual Pathogens (“KEEPS”):
K – Klebsiella
E – E. coli (90%)
E – Enterococcus, Enterobacteriaceae
P – Proteus, Pseudomonas
S – Staph. saprophyticus, Serratia
Urine Findings:
↑ Colony Count (>107 CFU/L)
↑ WBC (>10 WBC/μL)
(+) Bacterial culture
(+) Nitrites, Leukocyte Esterase
(+) Foul, turbid urine
+/- Hematuria (rare)")
lower-urinary-tract-infection-pathogenesis-and-clinical-findings
, stagnant
urine (anatomical variant, obstruction,
neurogenic bladder, urinary reflux)
Bacterial entry (Less Common):
Indwelling catheter, surgical inoculation,
hematogenousspread, trauma
(Staphylococcus, Enterococcus, Candida)
Fecal bacteria access urethra
(E. coli, Proteus, Klebsiella)
Impairment of body's natural defense
systems, or stagnant urine, allow for
bacterial accumulation
Portal of entry bypasses body's physical
defenses (gravity and repetitive outward
urine flow)
Bacterial fimbriae and pili allow
them to ascend urethra and
adhere to epithelium
Lower Urinary Tract Infection (LUTI): Pathogenesis and clinical findings
Suprapubic
Tenderness
Bacterial colony irritates
urinary epithelium
Urgency:
Sensation of need to urinate
quickly or impending
incontinence
Stimulation of
inflammatory
response
Stimulation of urinary reflex
Pathogens use
enzymes to reduce
nitrate to nitrite
Delirium in Elderly
Frequency:
Repetitive need to
urinate
Unique response of altered fluid
status, electrolytes and mental
status, likely as a result of
increased inflammatory cytokines
Lower Urinary Tract Infection (“Cystitis”):
Infection of bladder or distal tract by capable bacteria
colonizing epithelium and causing symptoms
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications Published March 16, 2014 on www.thecalgaryguide.com
Author:
Brett Edwards
Reviewers:
Riley Hartmann
Jan Rudzinski
Haotian Wang
Steve Vaughan*
* MD at time of publication
Usual Pathogens (“KEEPS”):
K – Klebsiella
E – E. coli (90%)
E – Enterococcus, Enterobacteriaceae
P – Proteus, Pseudomonas
S – Staph. saprophyticus, Serratia
Urine Findings:
↑ Colony Count (>107 CFU/L)
↑ WBC (>10 WBC/μL)
(+) Bacterial culture
(+) Nitrites, Leukocyte Esterase
(+) Foul, turbid urine
+/- Hematuria (rare)
WBCs onsite
release enzymes
Cytokines released
systemically
Fever, Malaise,
↑WBC
(>11 x 109 cells/L)
(Rare in LUTI)")
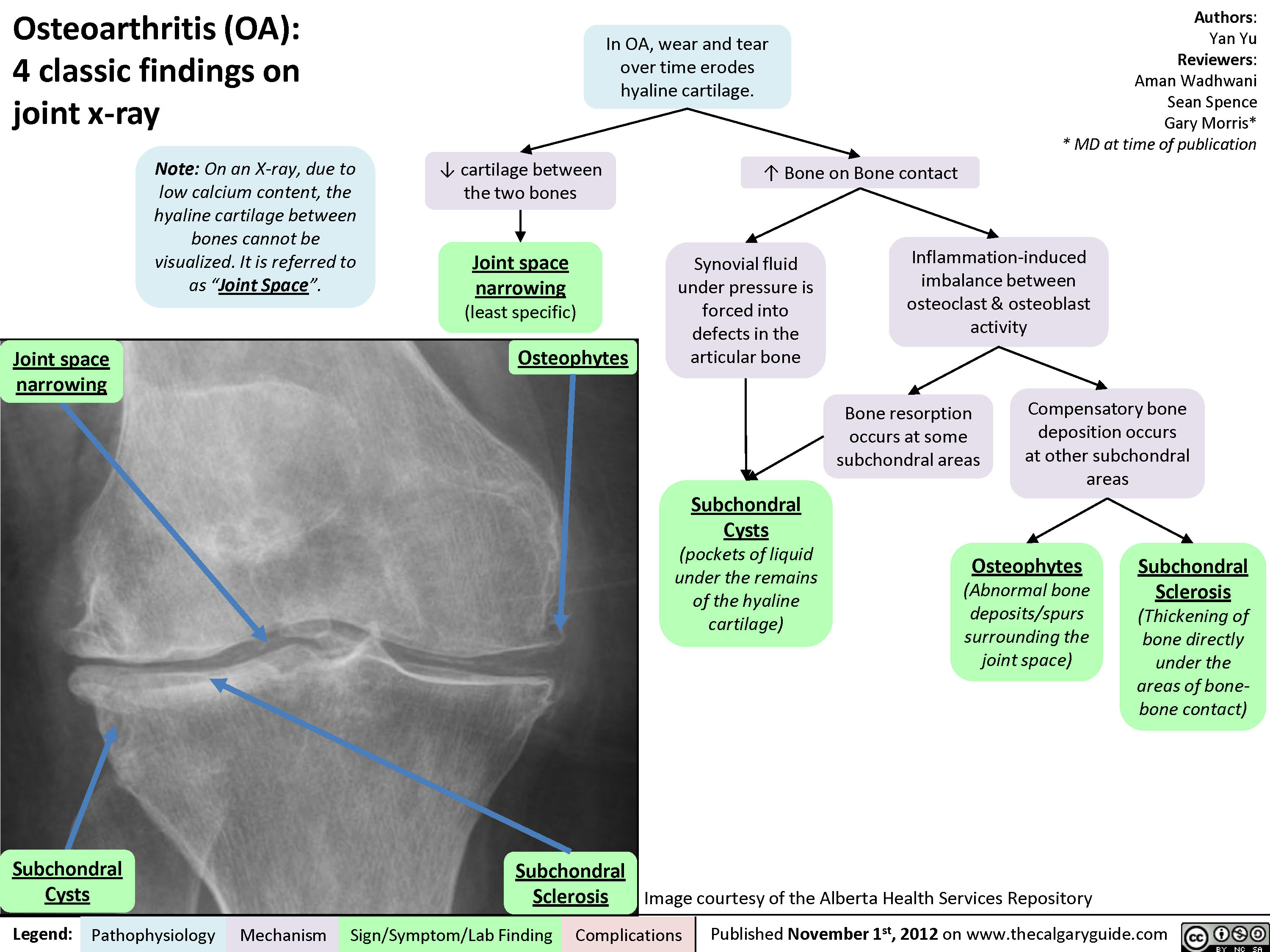
Osteoarthritis (OA): Clinical findings

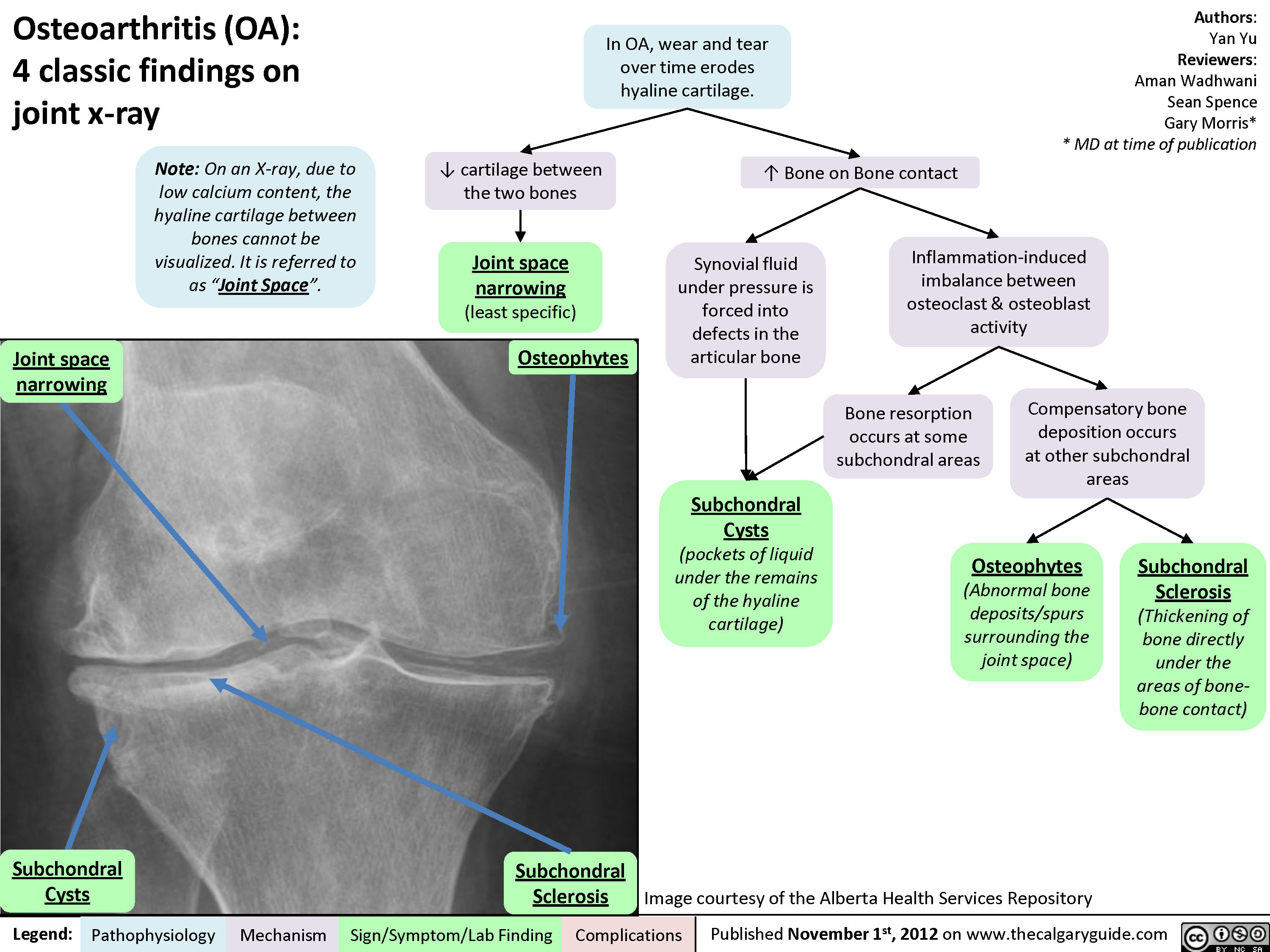
Osteoarthritis (OA): X-ray features
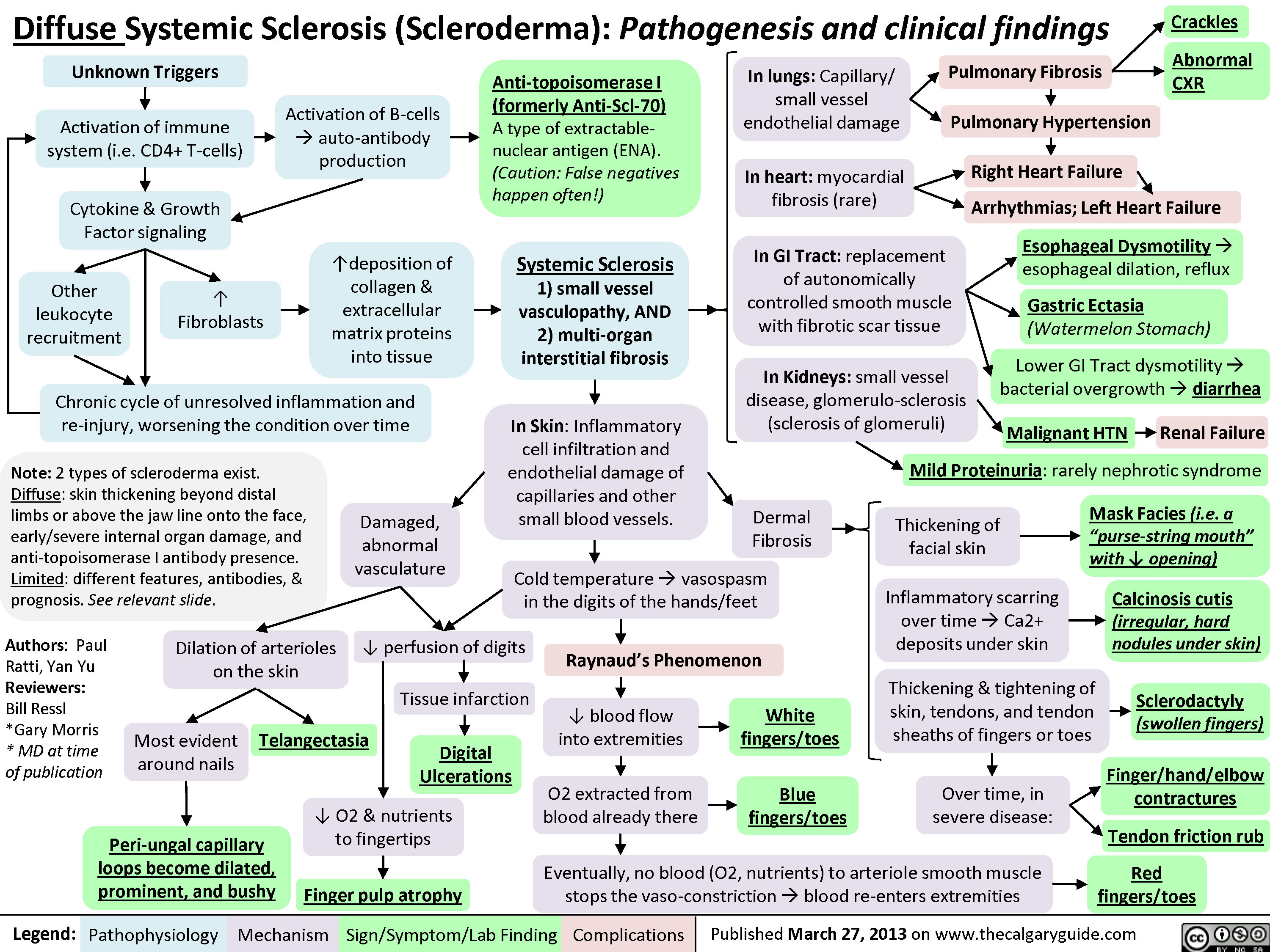
Diffuse Systemic Sclerosis (Scleroderma)
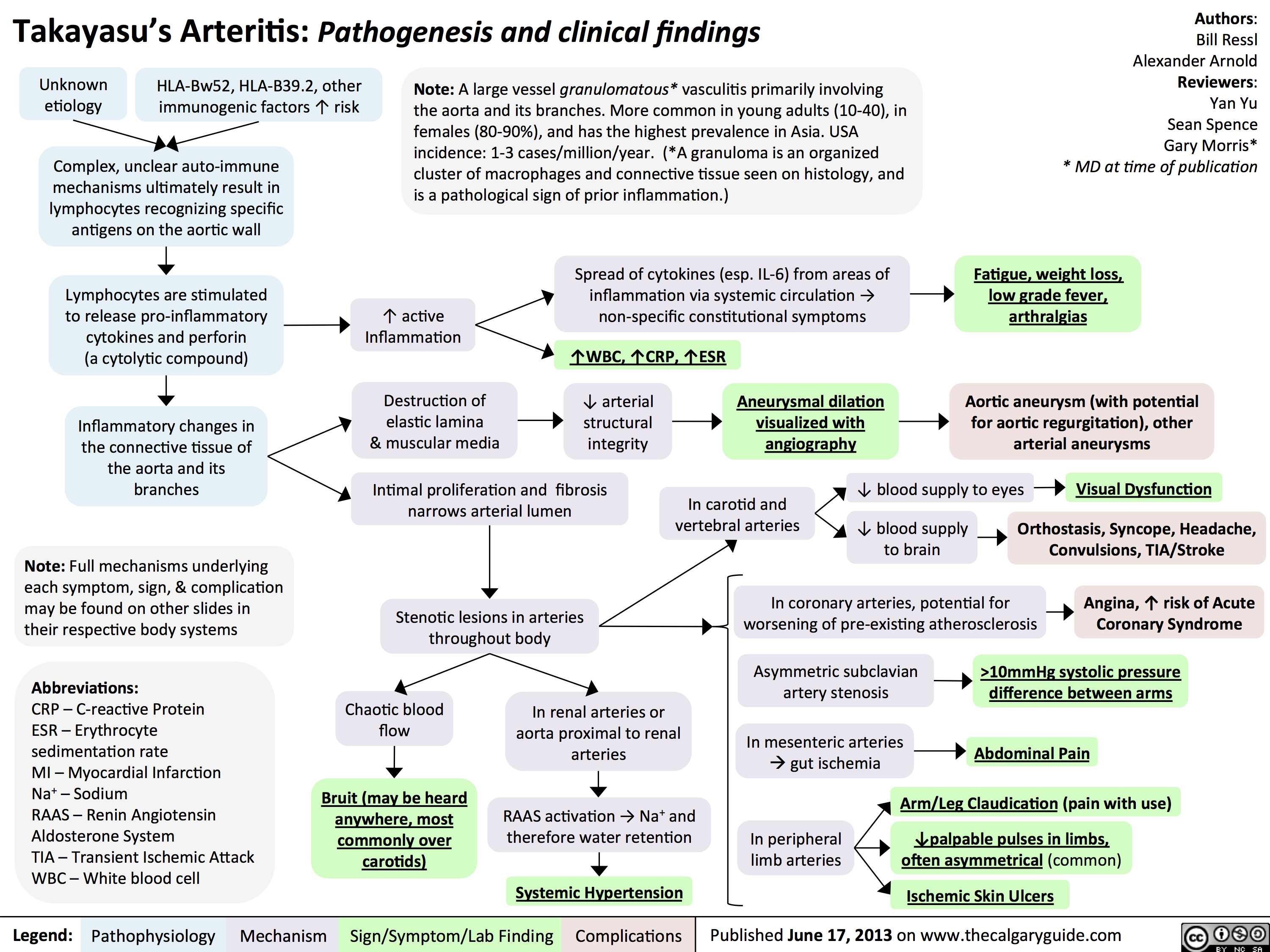
Takayasu's Arteritis: Pathogenesis and clinical findings
Giant Cell (Temporal) Arteritis: Pathogenesis and investigations

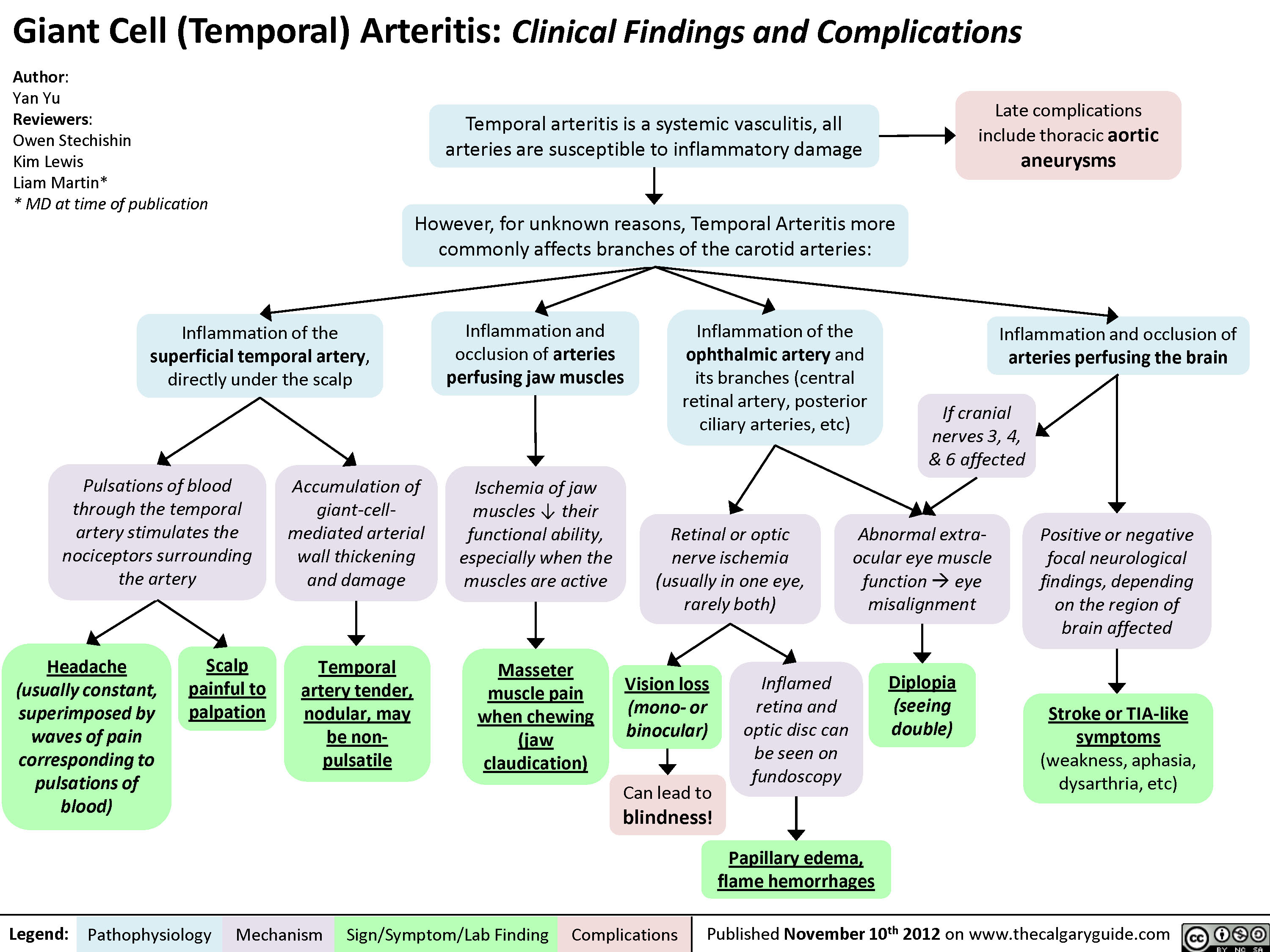
Giant Cell (Temporal) Arteritis: Clinical findings and Complications
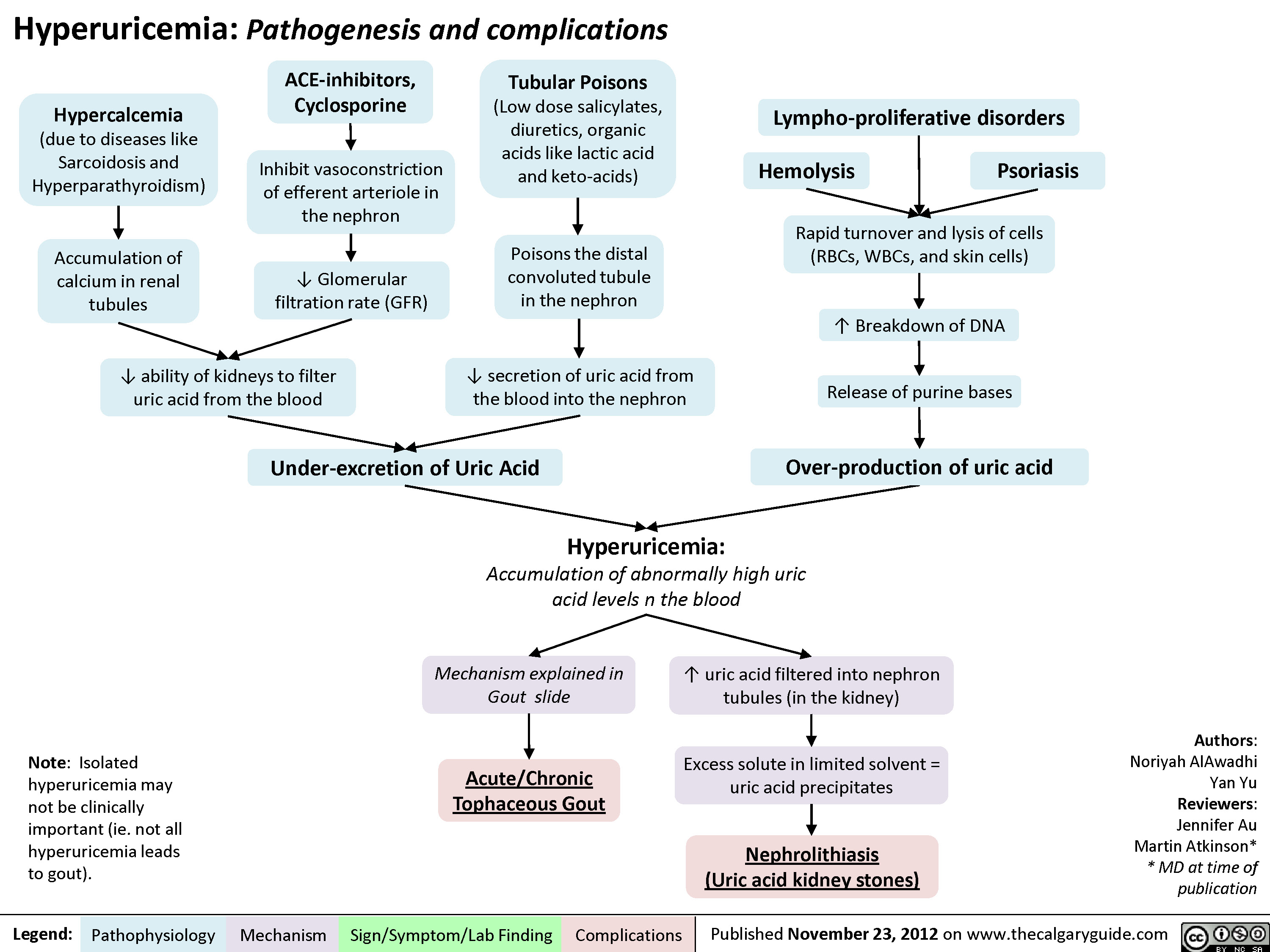
Hyperuricemia Pathogenesis and Complications
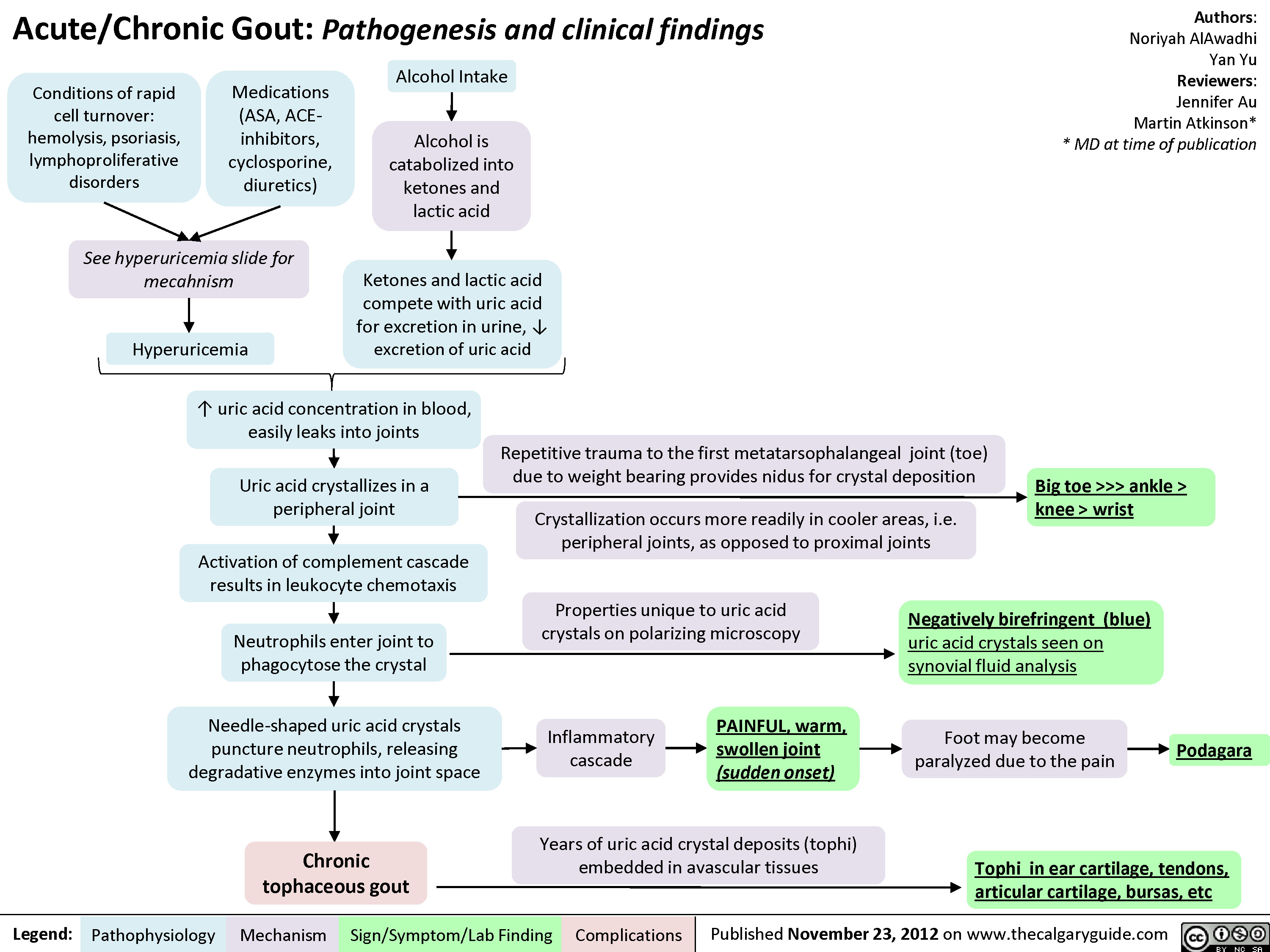
Gout Pathogenesis and Clinical Findings
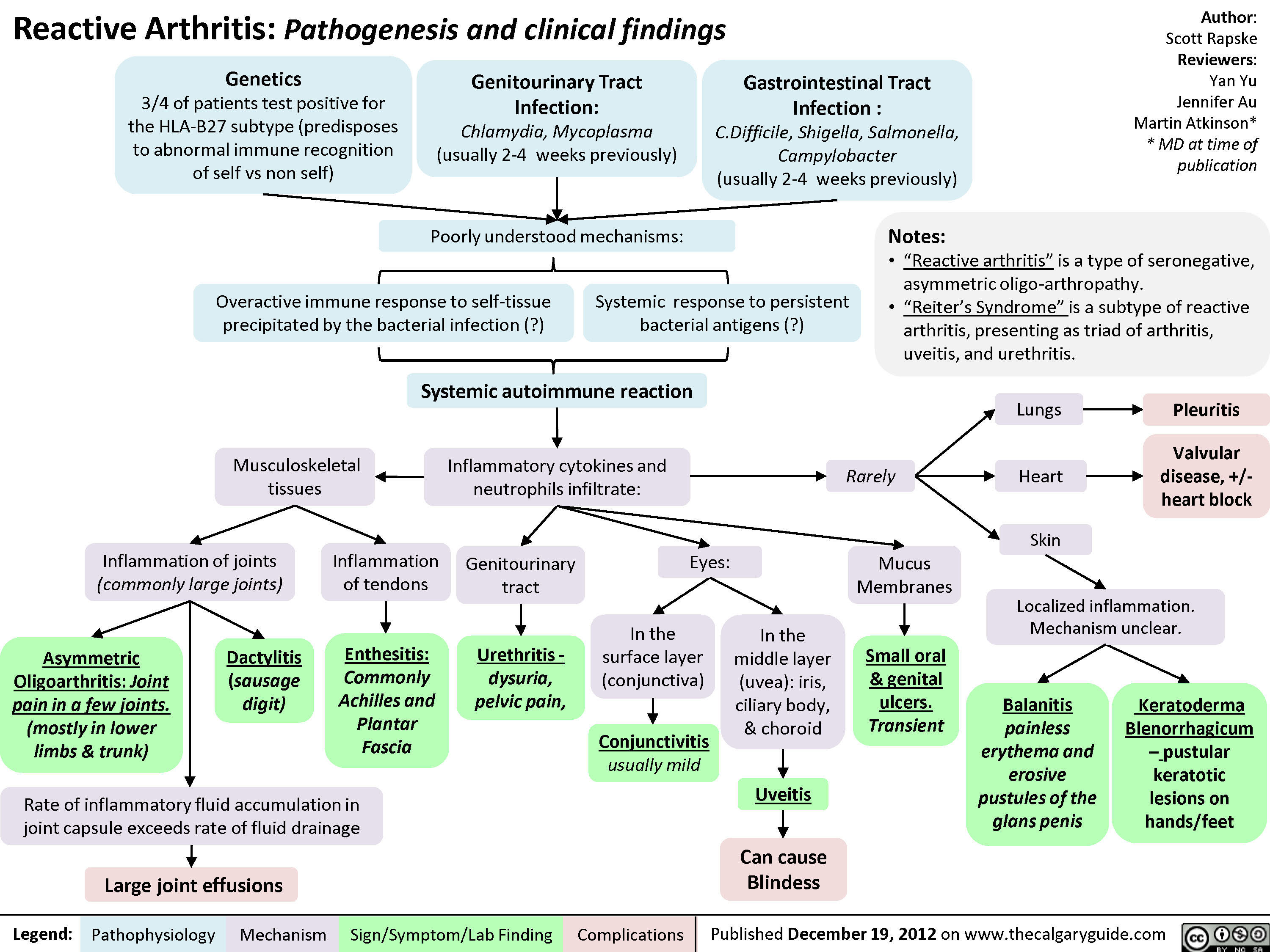
Reactive Arthritis
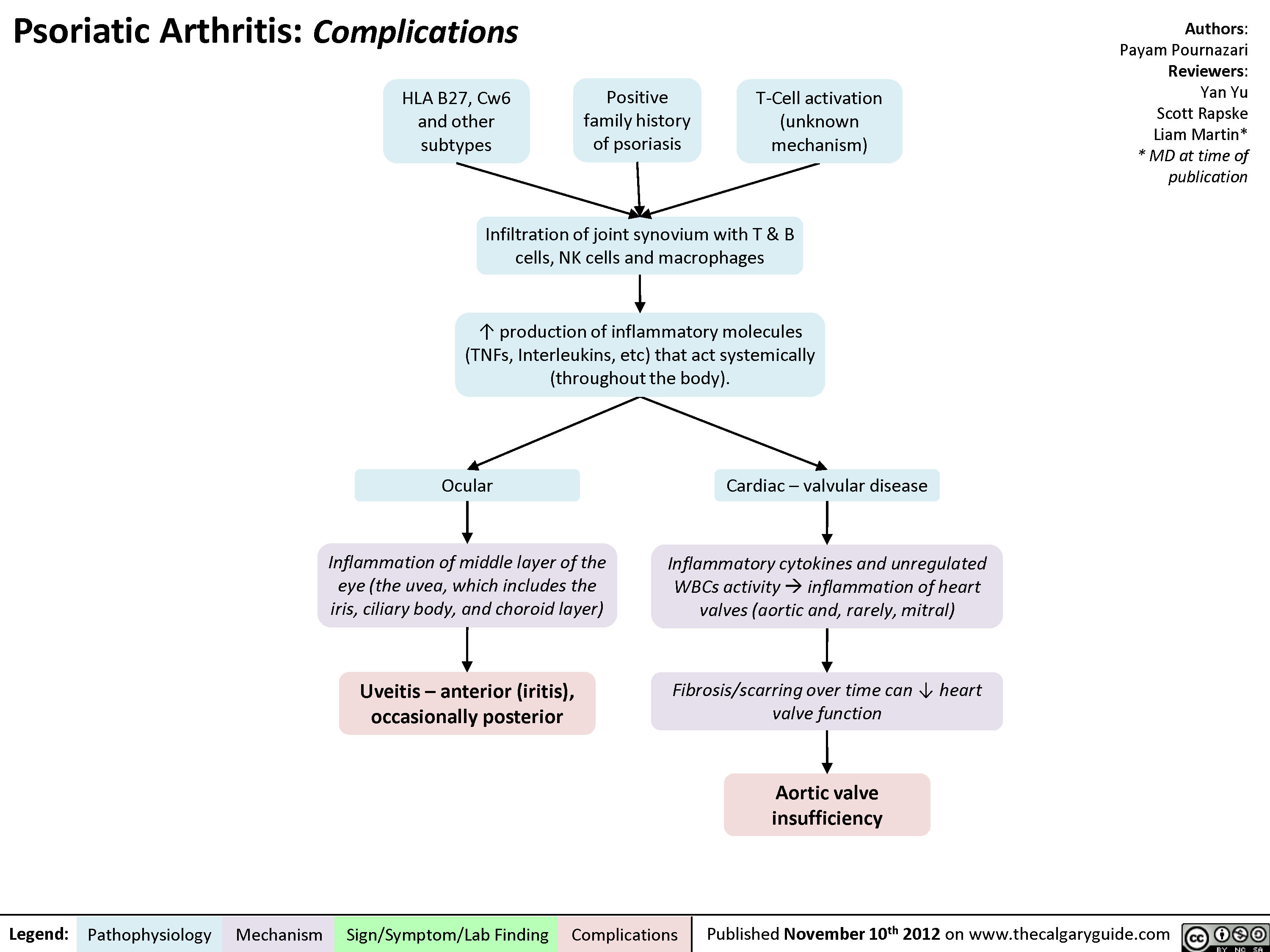
Psoriatic Arthritis: Complications
Psoriatic Arthritis - Pathogenesis and Clinical findings

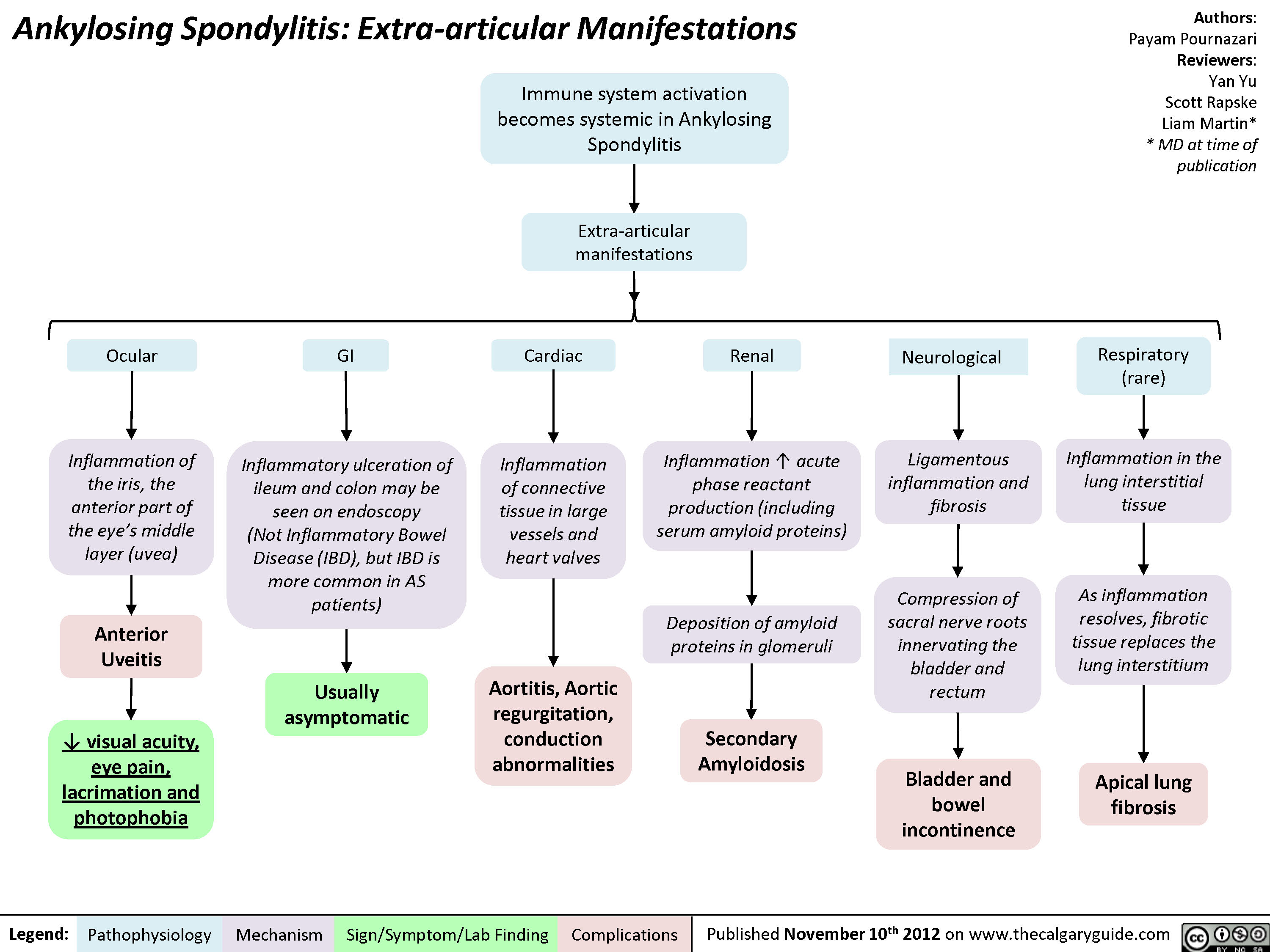
Ankylosing Spondylitis: Extra-articular Manifestations
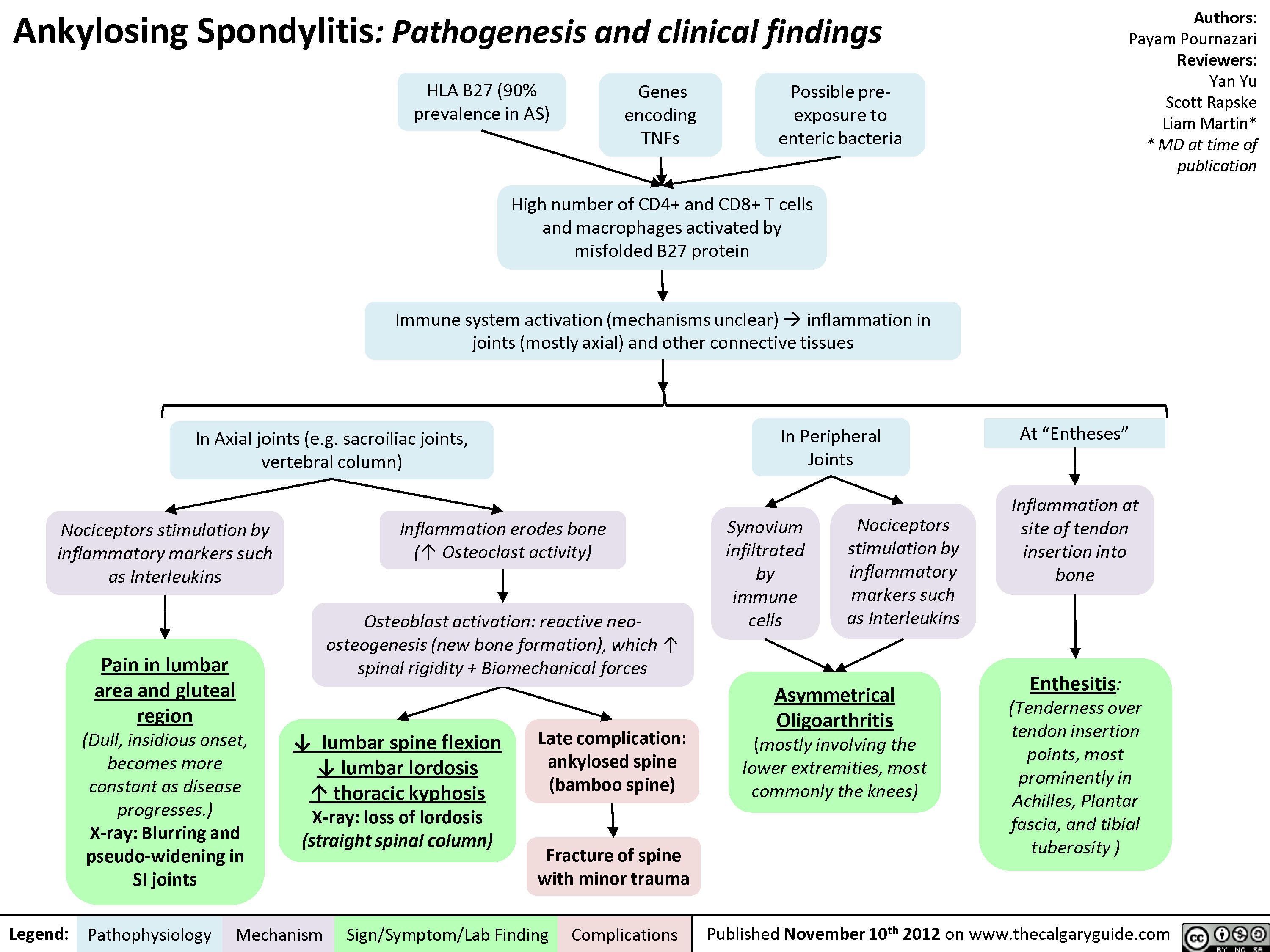
Ankylosing Spondylitis: Pathogenesis and Clinical findings
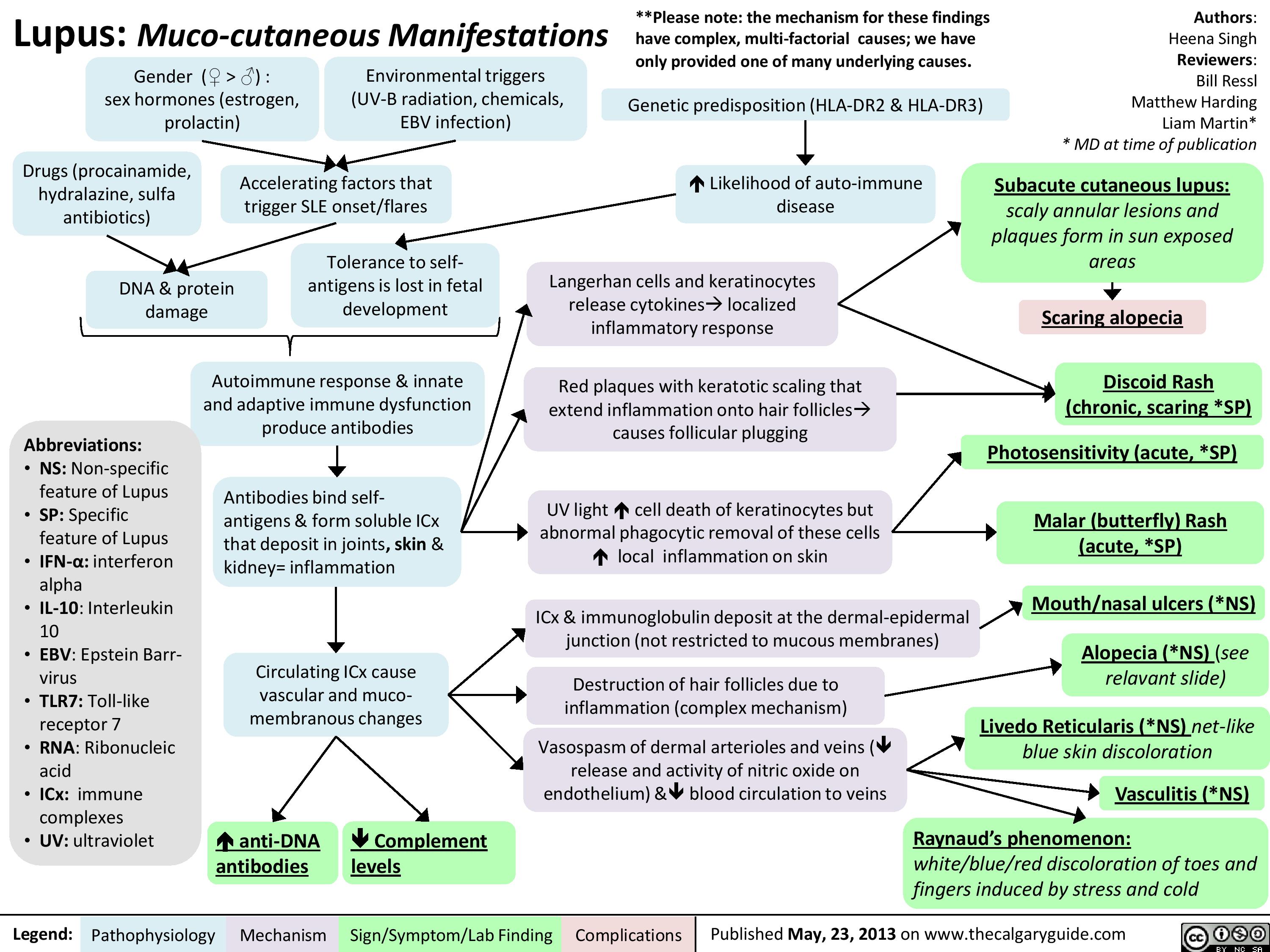
Lupus: Muco-cutaneous manifestations
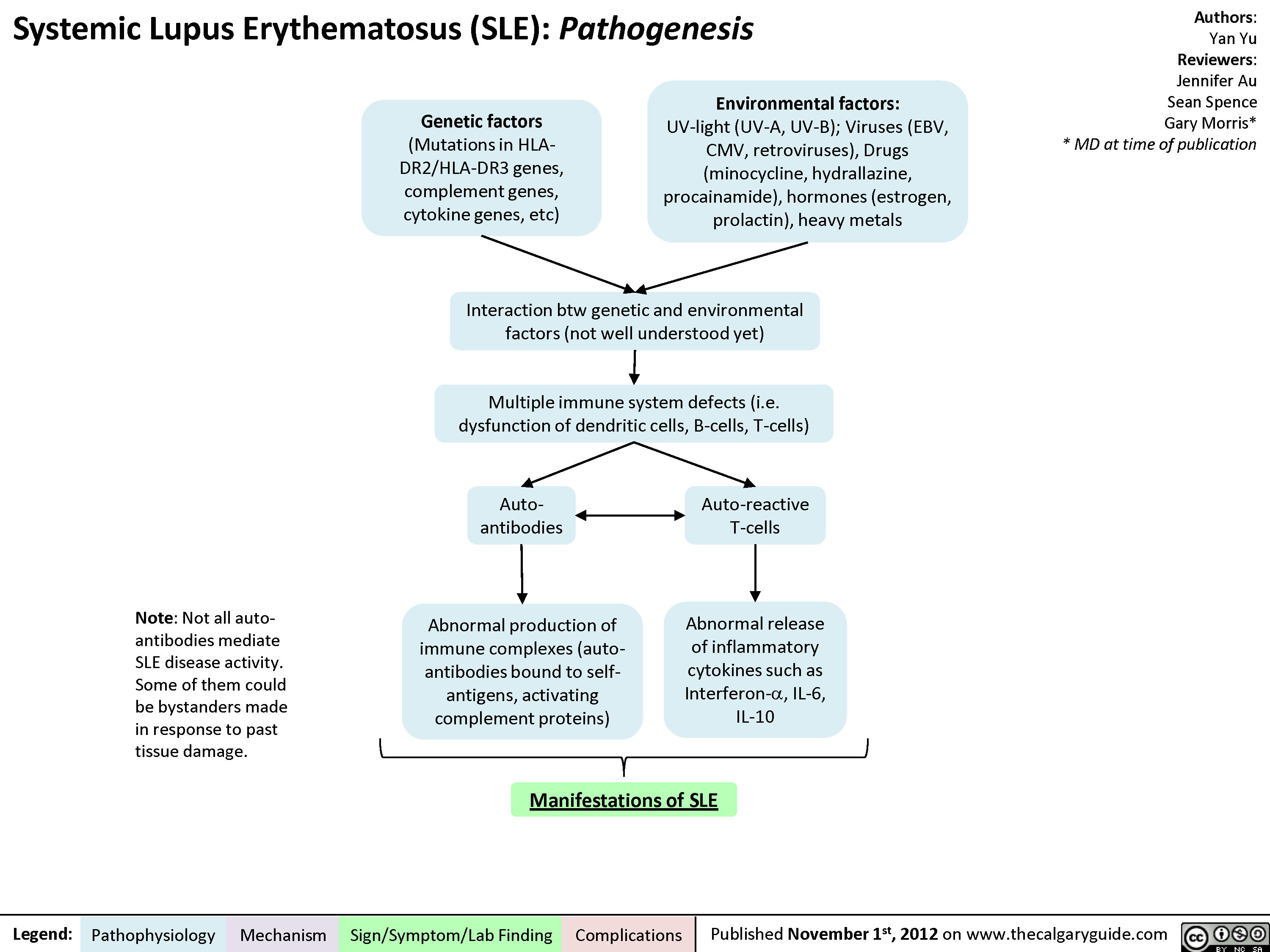
Pathogenesis of Lupus
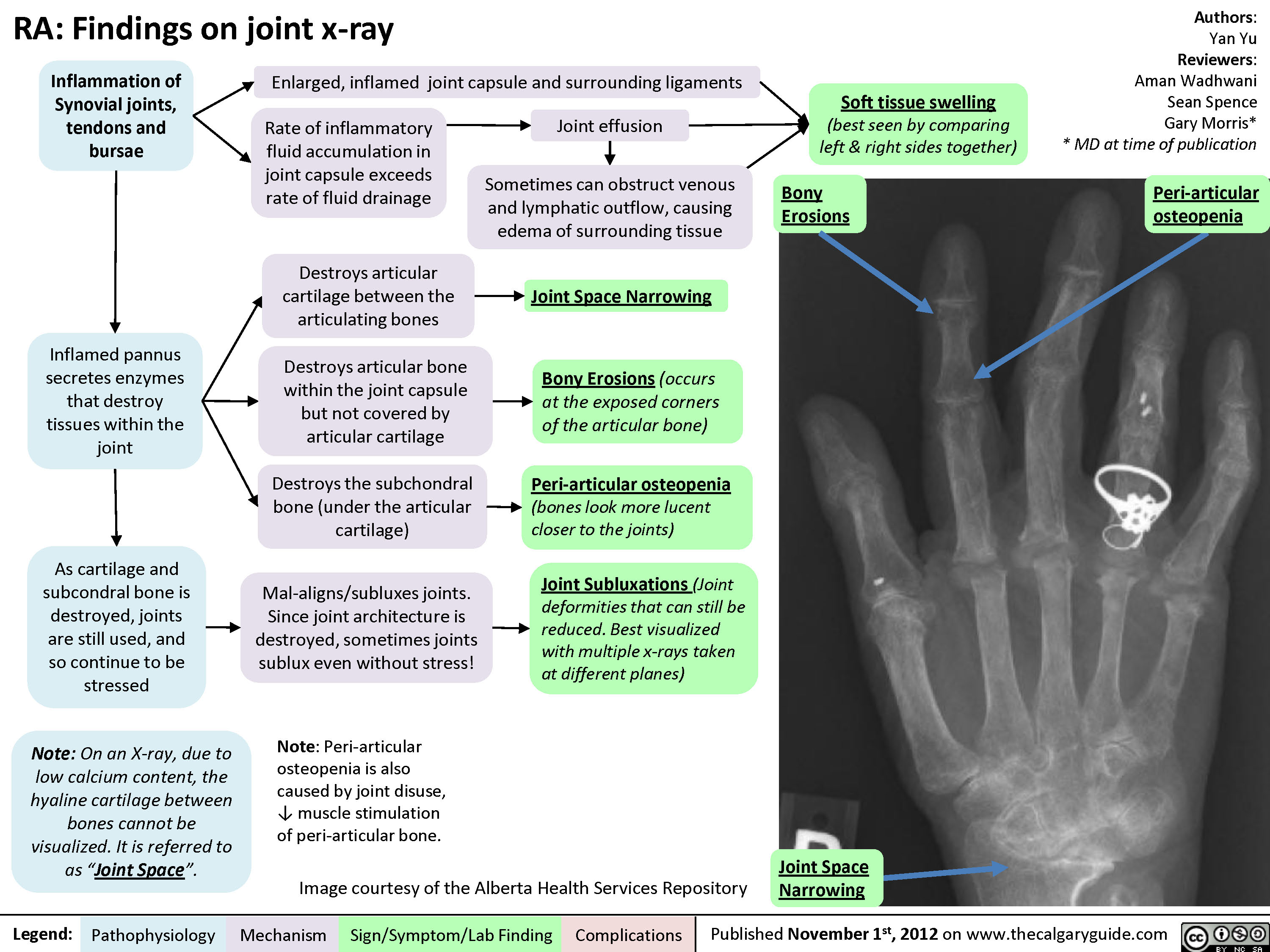
Rheumatoid arthritis (RA): X-ray features
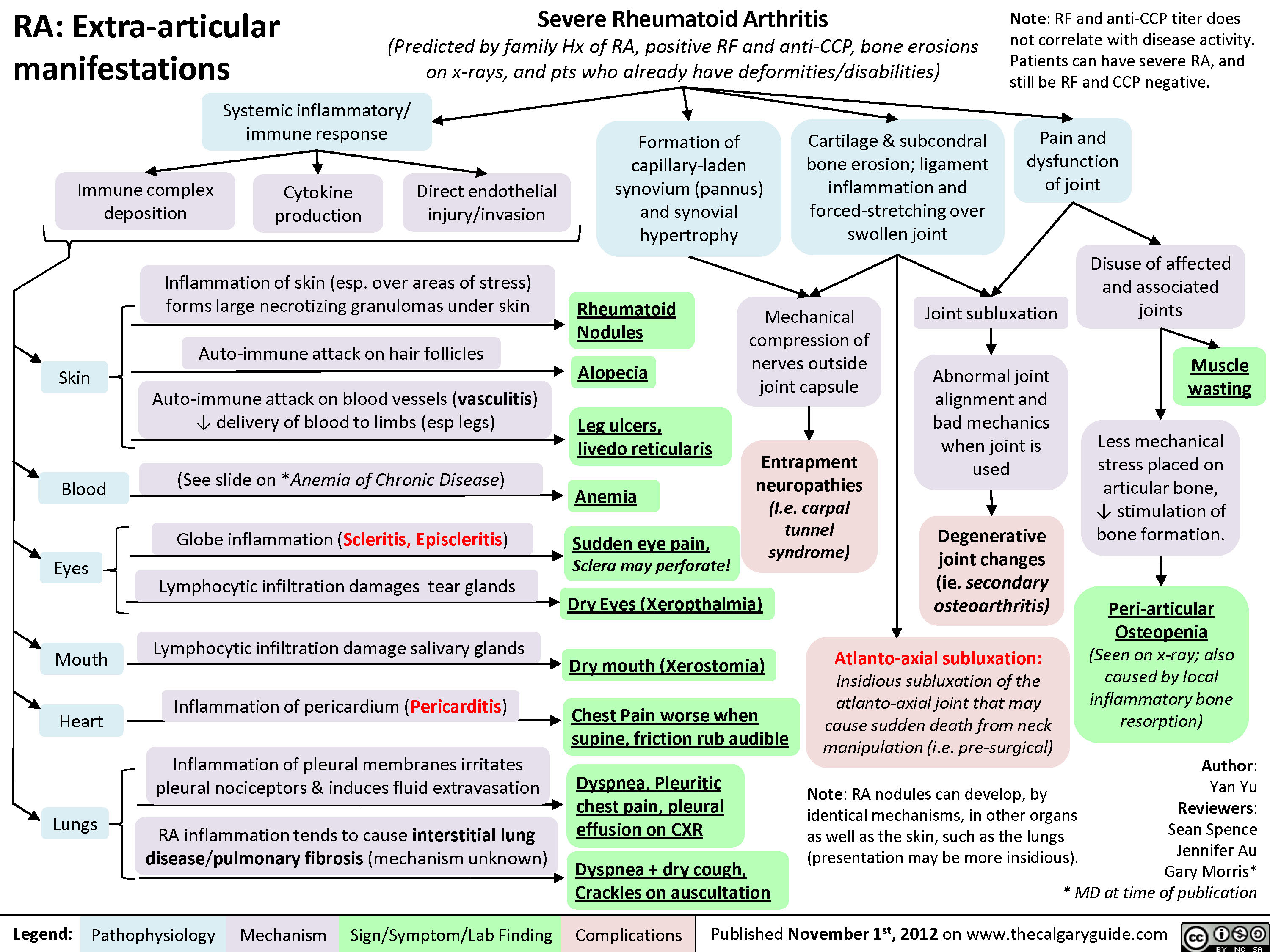
Rheumatoid arthritis (RA): Extra-articular manifestations
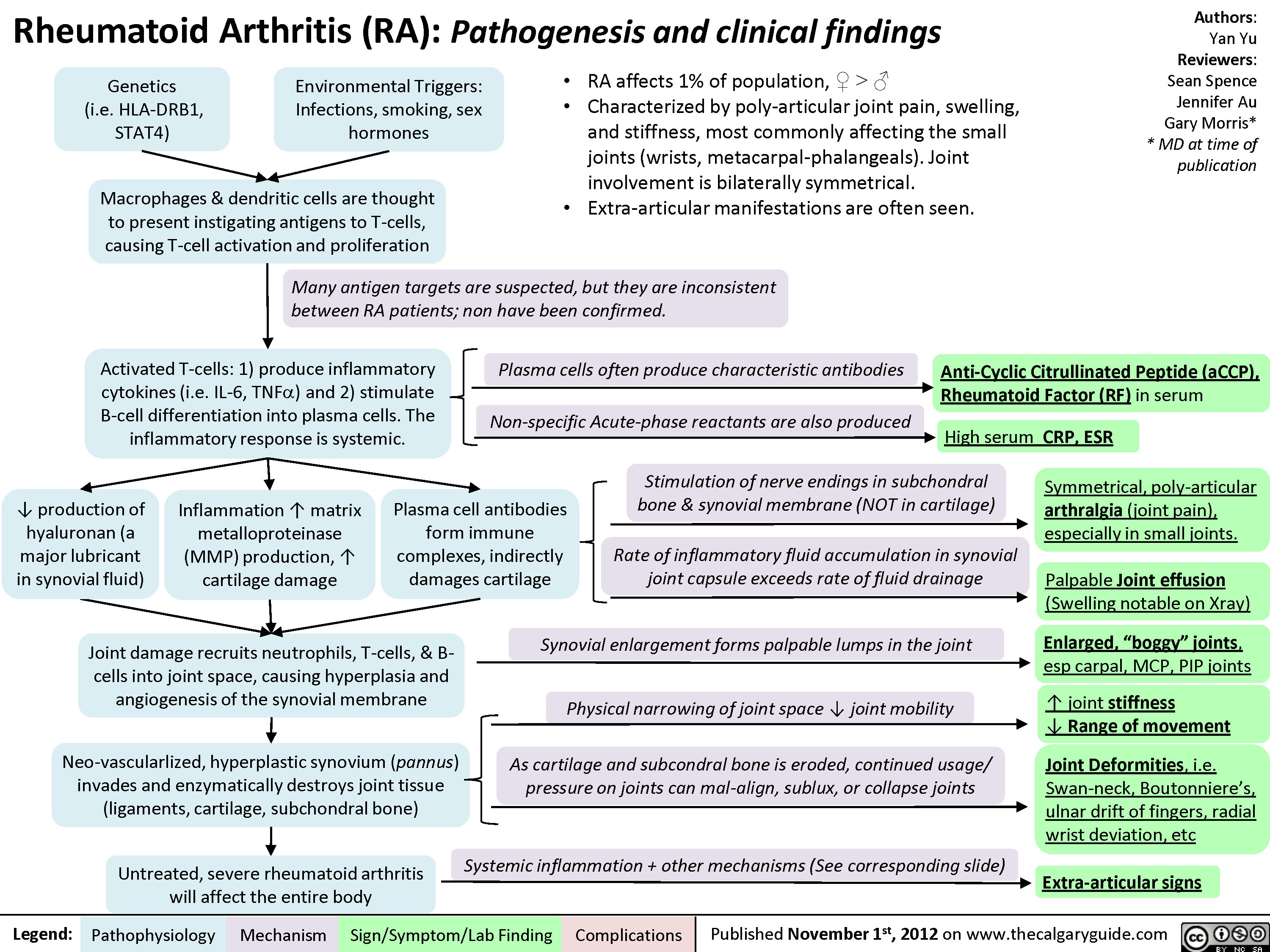
Rheumatoid arthritis (RA): Pathogenesis and Joint diseases features
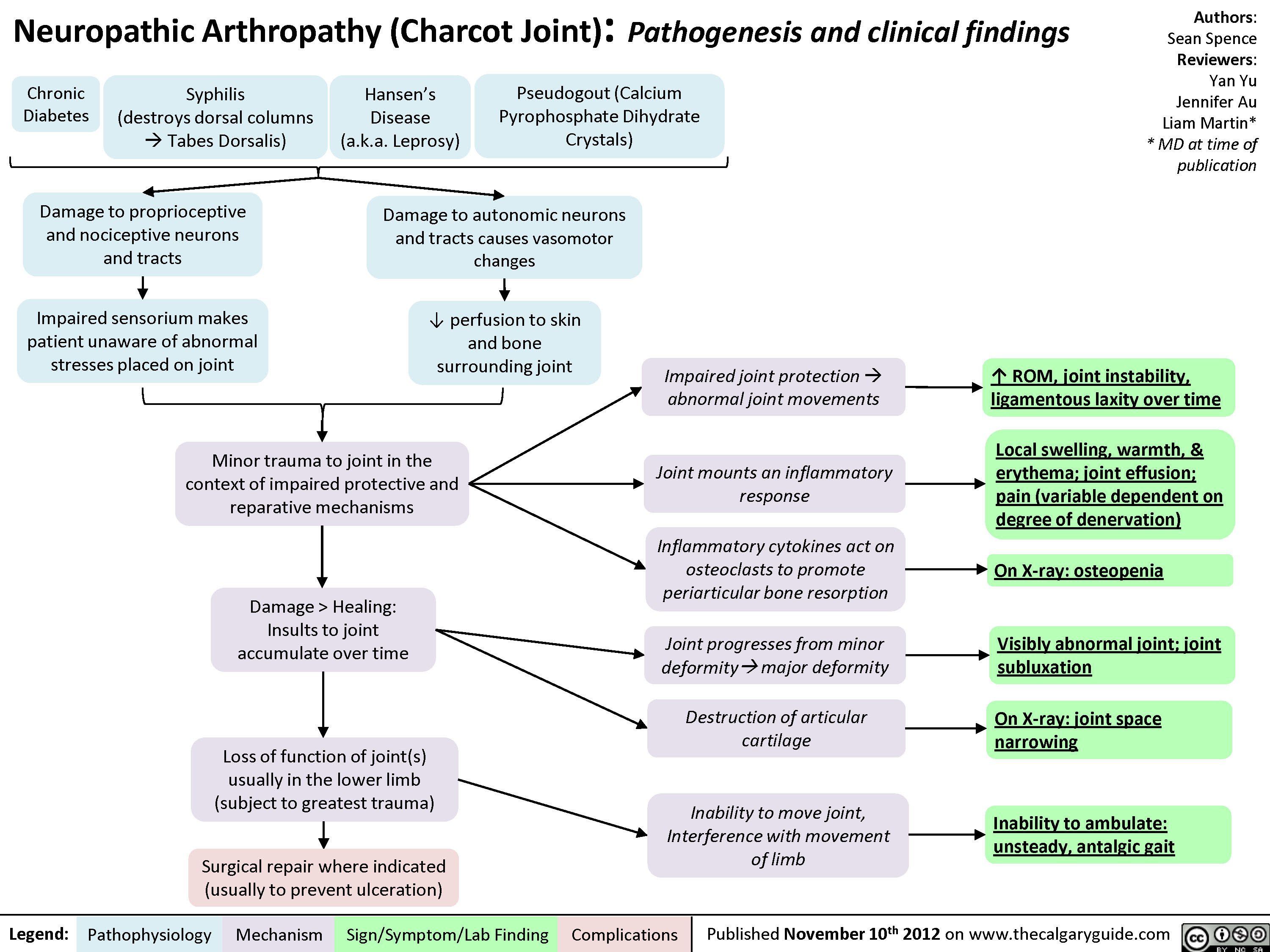
Charcot Joint: Pathogenesis and Clinical findings
Osteoarthritis (OA): X-ray features
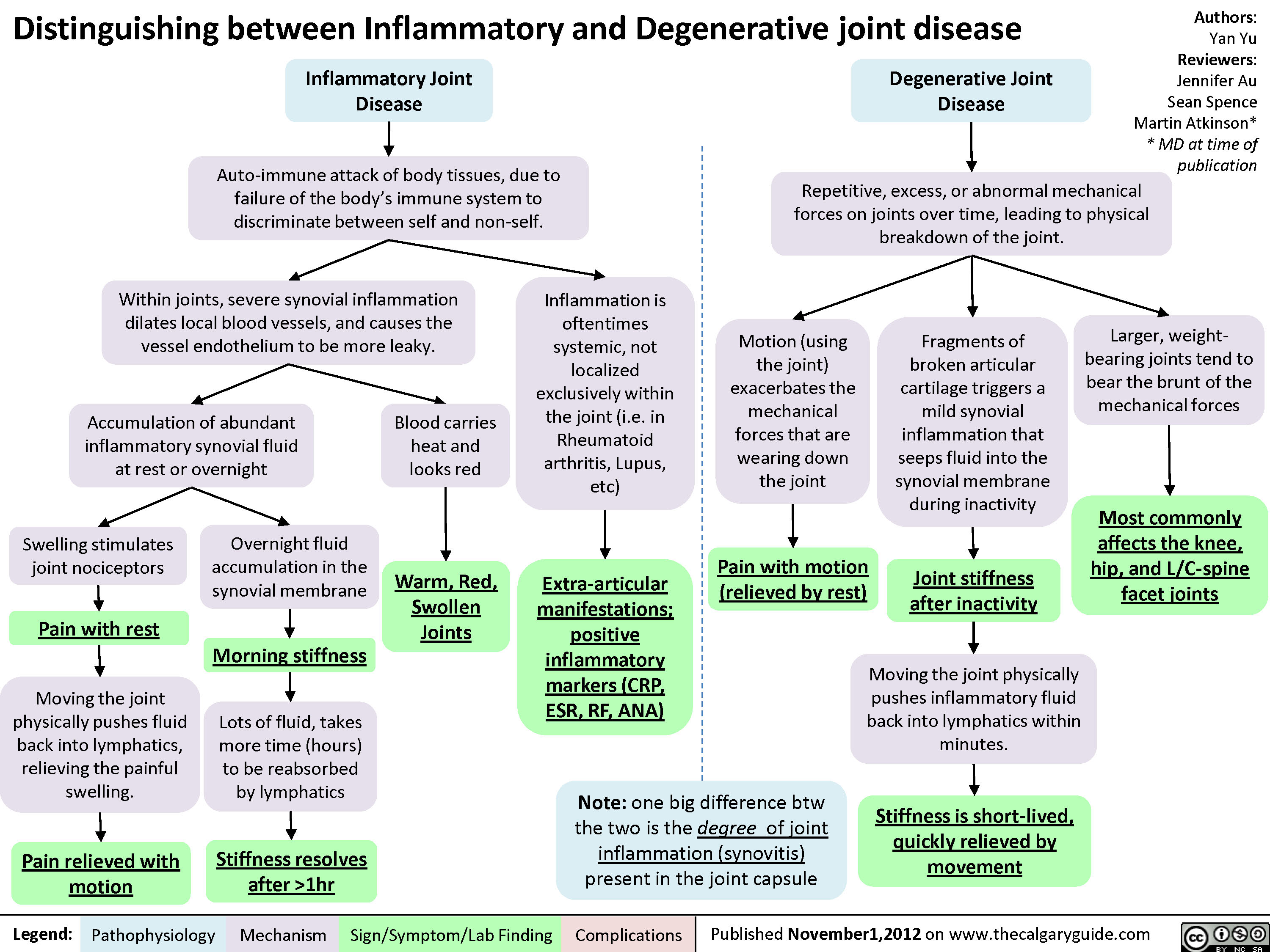
Degenerative Vs Inflammatory Joint Disease
Hypersensitivity: Definitions
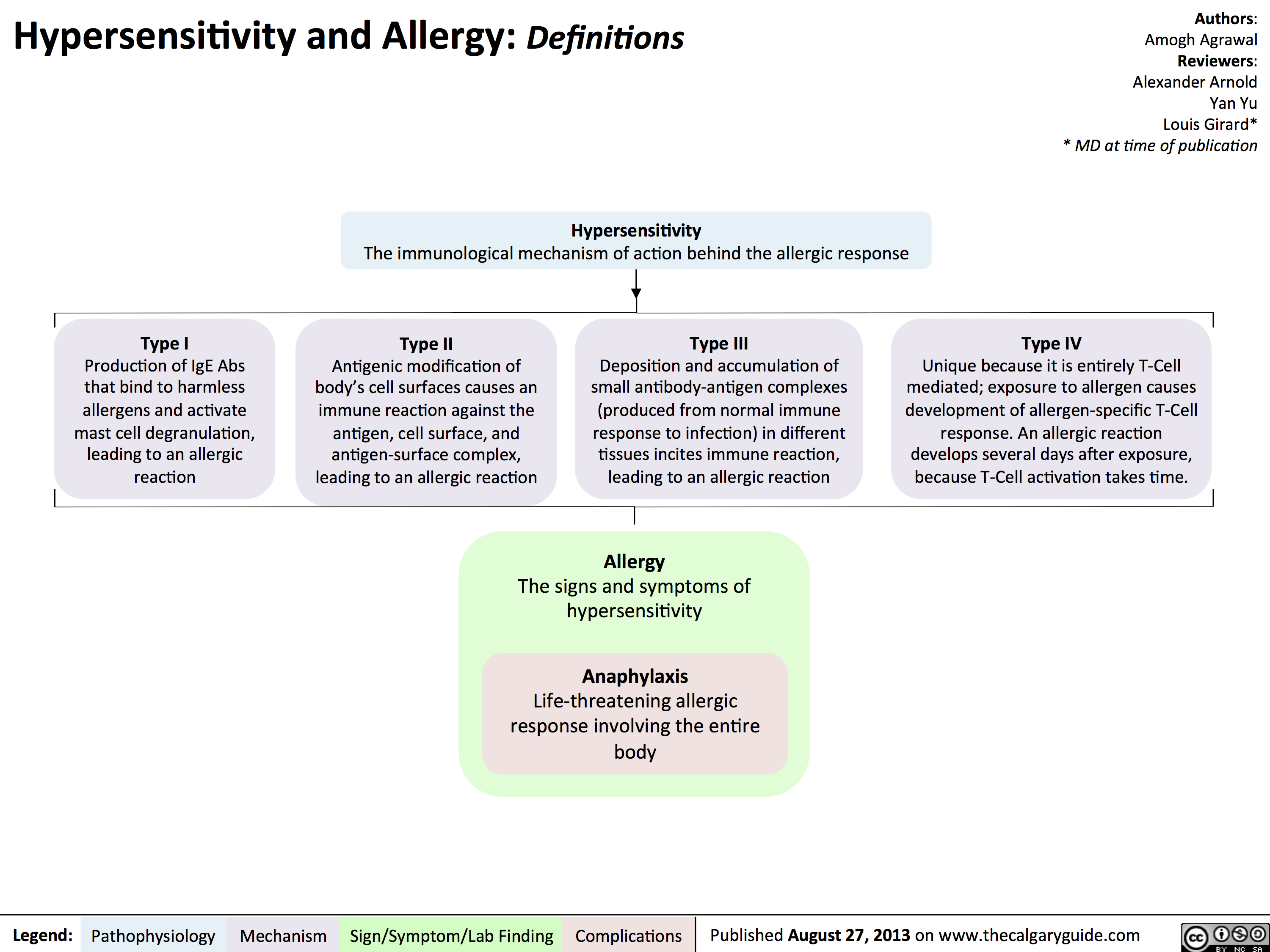
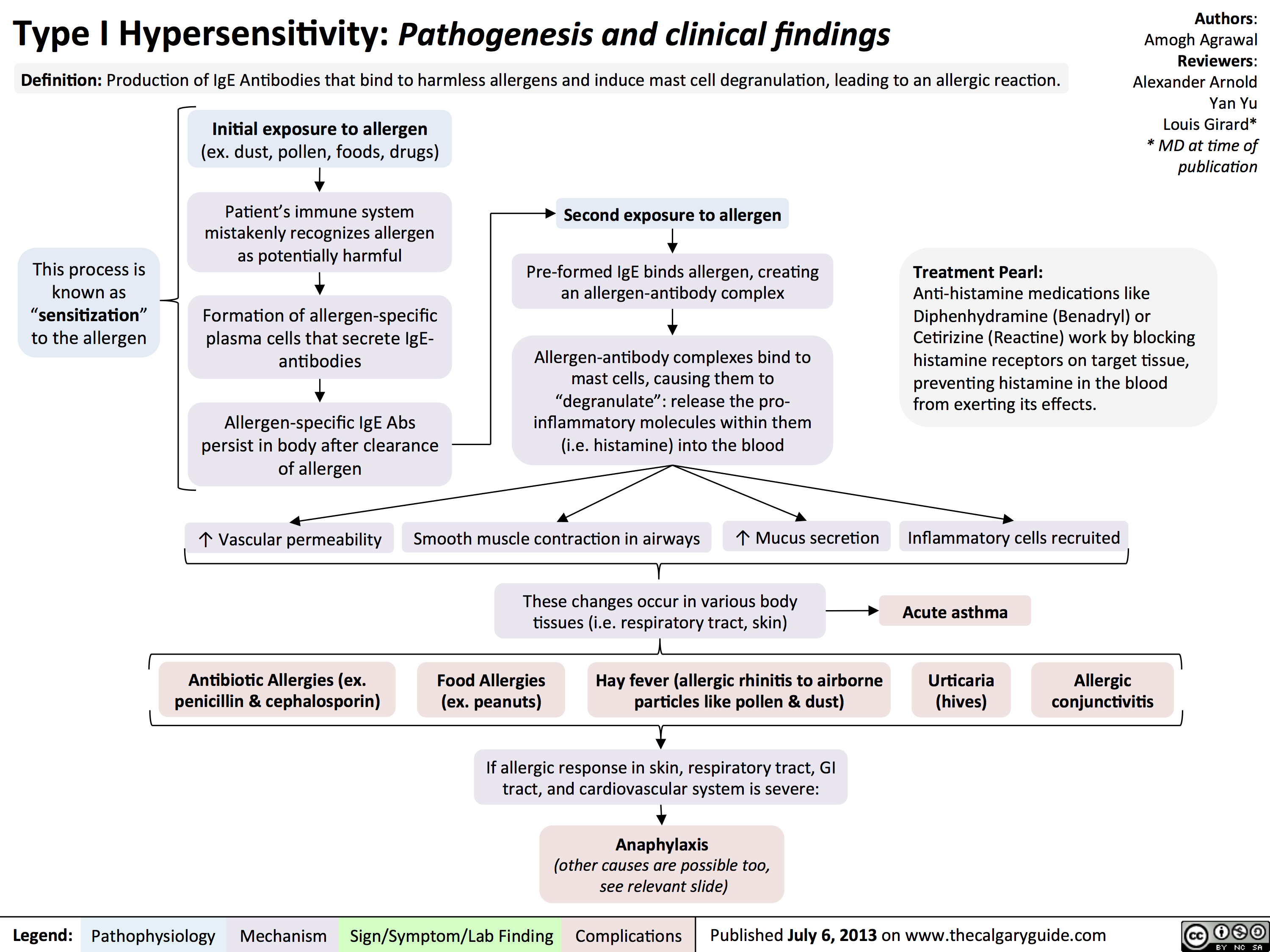
Type I Hypersensitivity: Pathogenesis and clinical findings
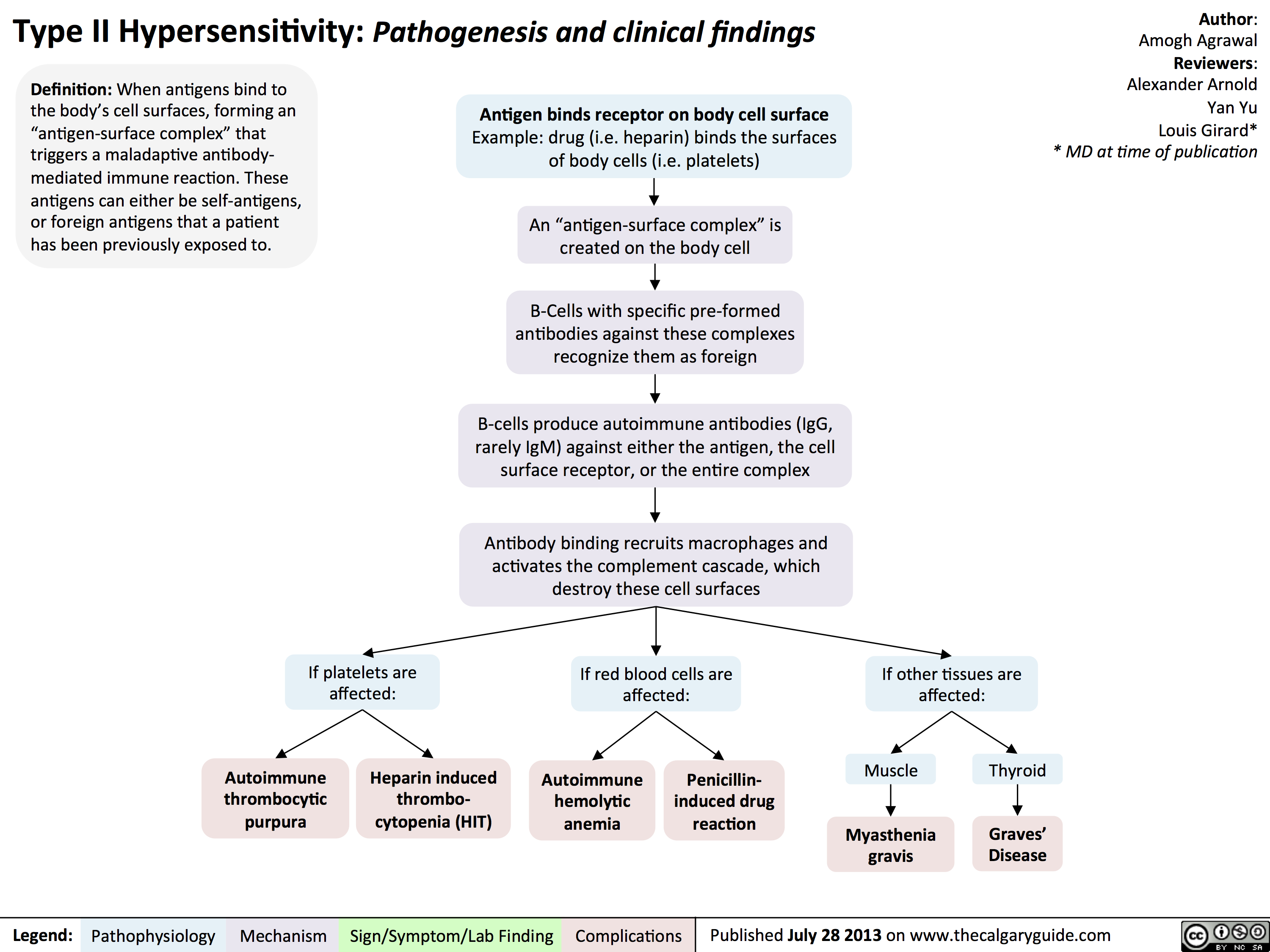
Type II Hypersensitivity: Pathogenesis and clinical findings
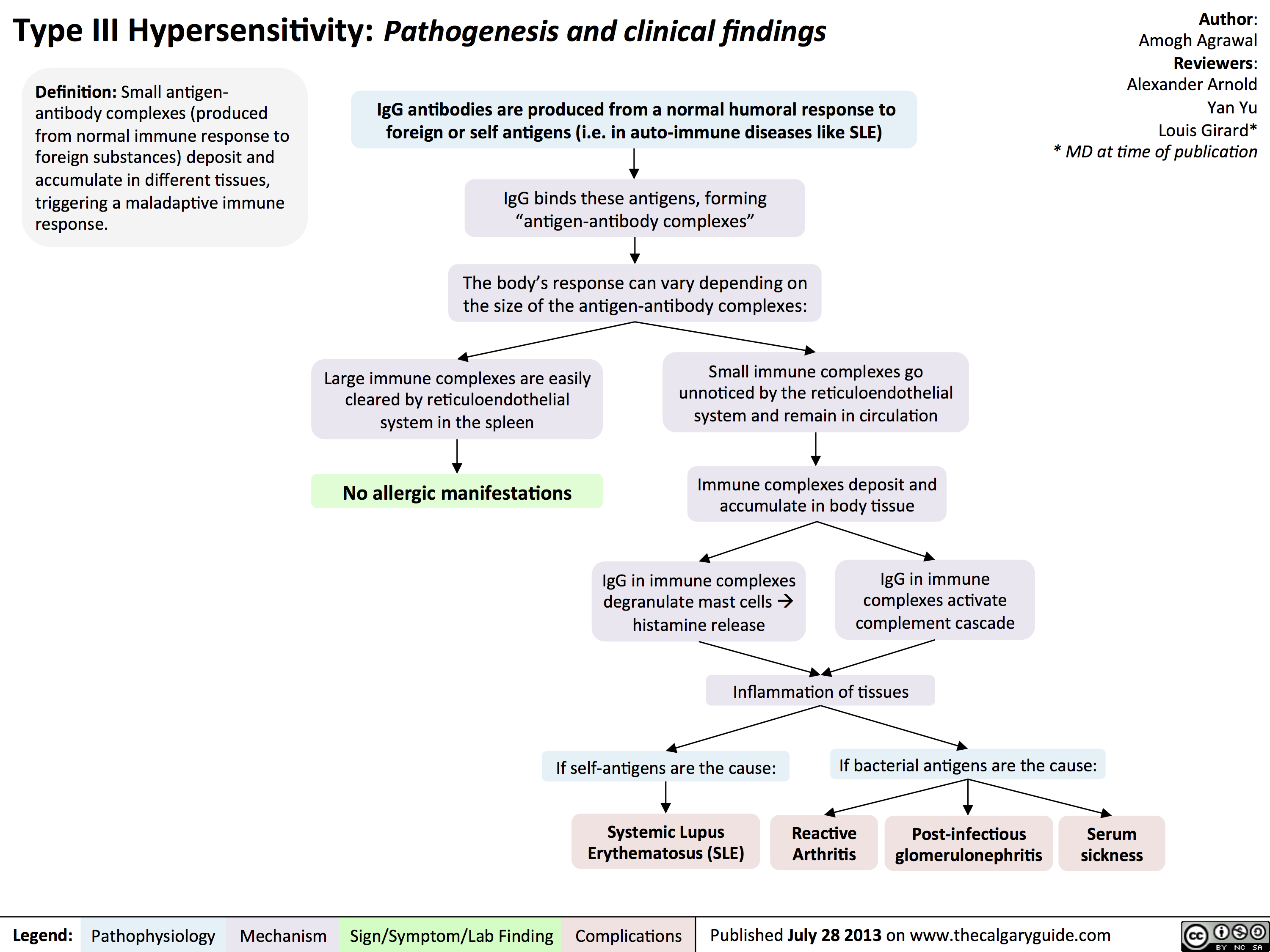
Type III Hypersensitivity: Pathogenesis and clinical findings
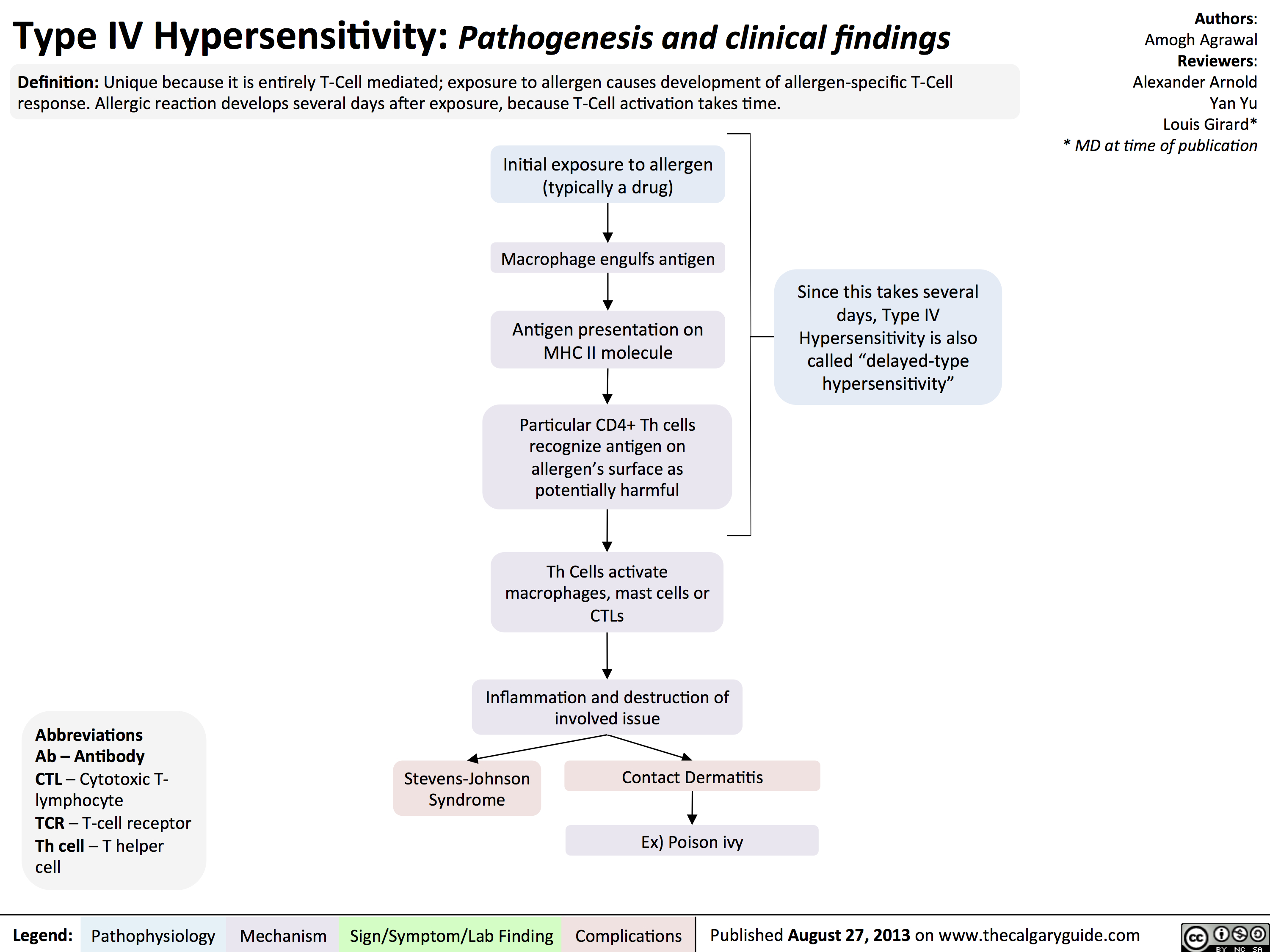
Type IV Hypersensitivity: Pathogenesis and clinical findings
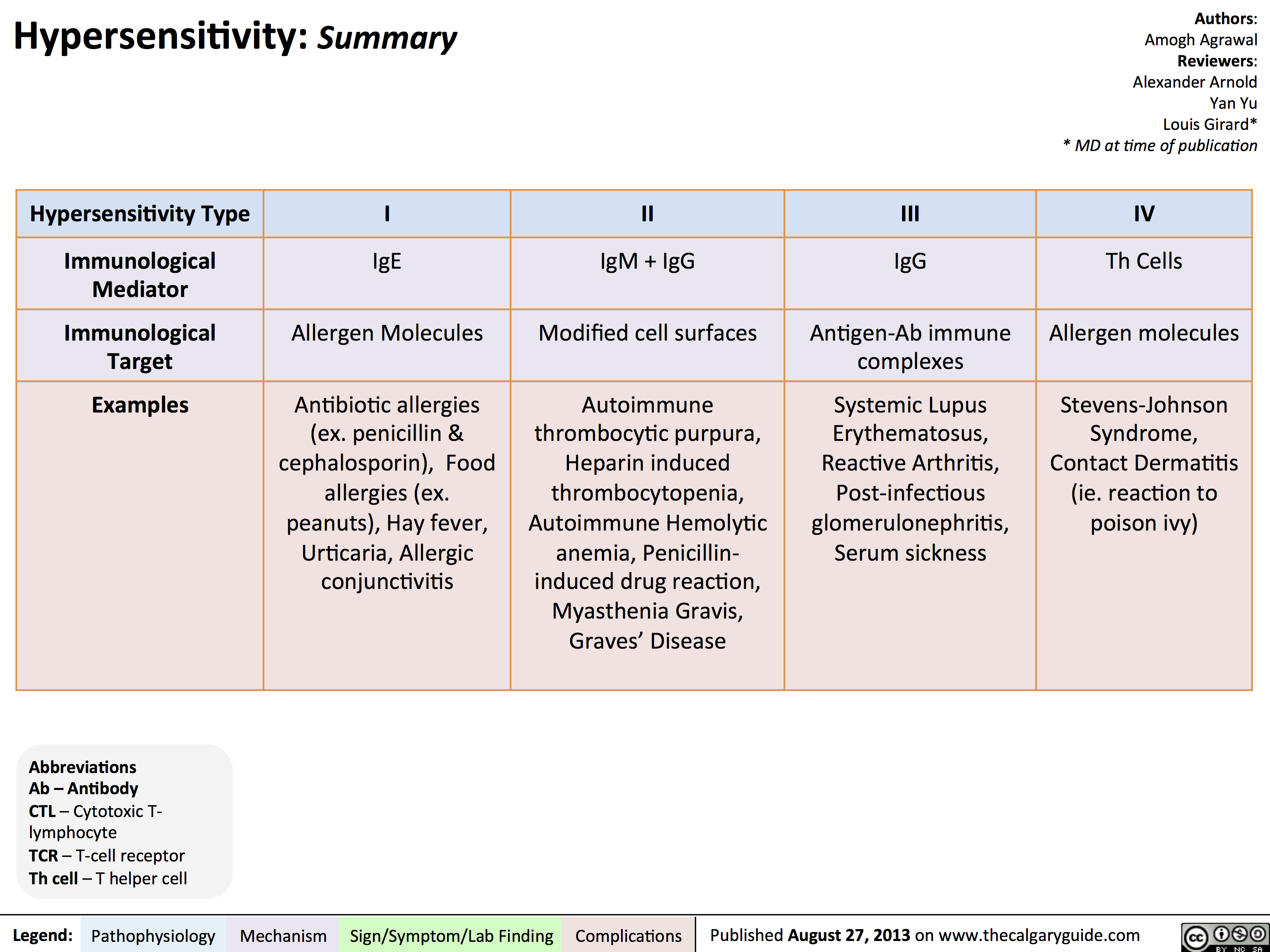
Hypersensitivity Summary
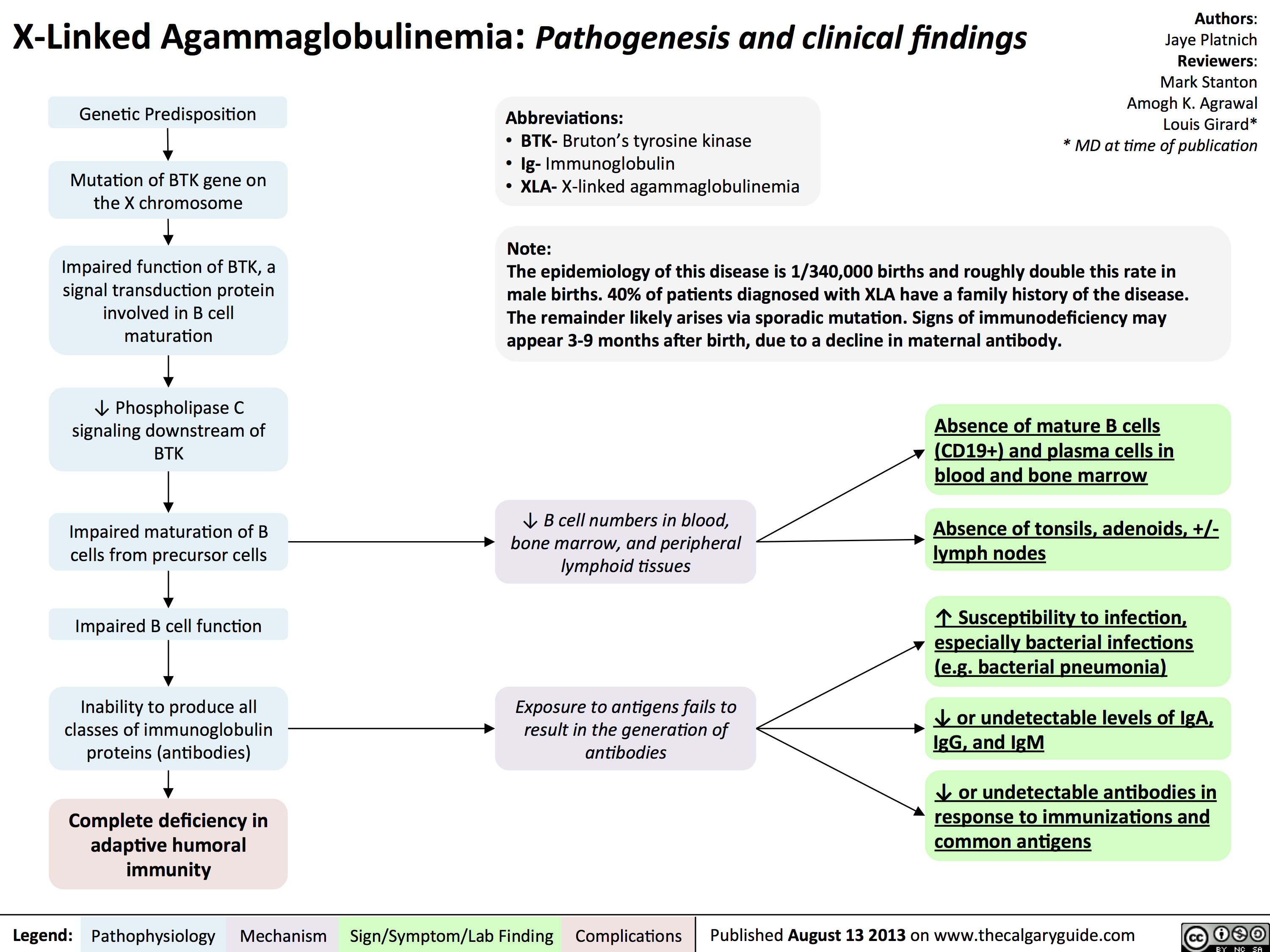
Agammaglobulinemia: Pathogenesis and clinical findings
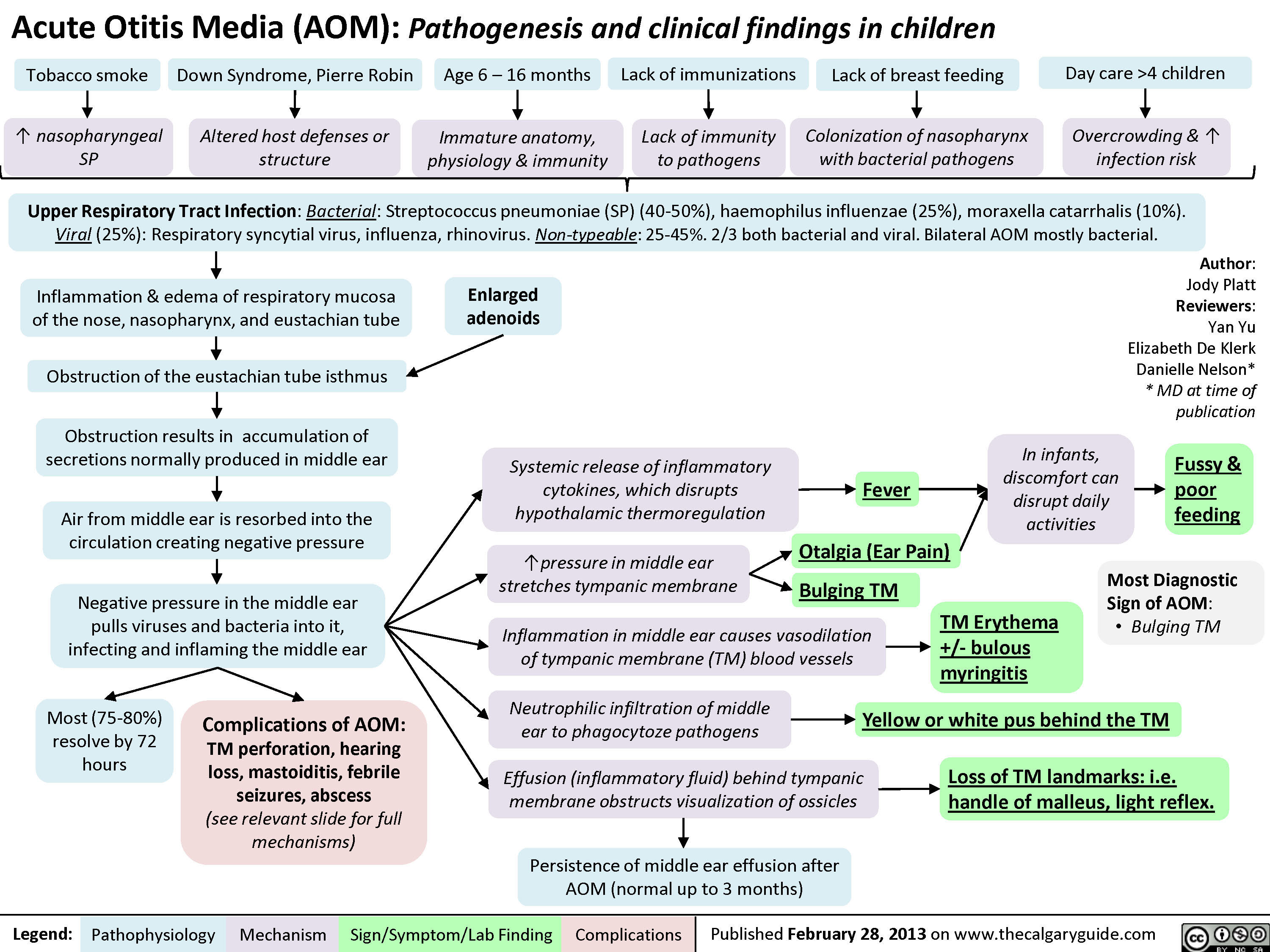
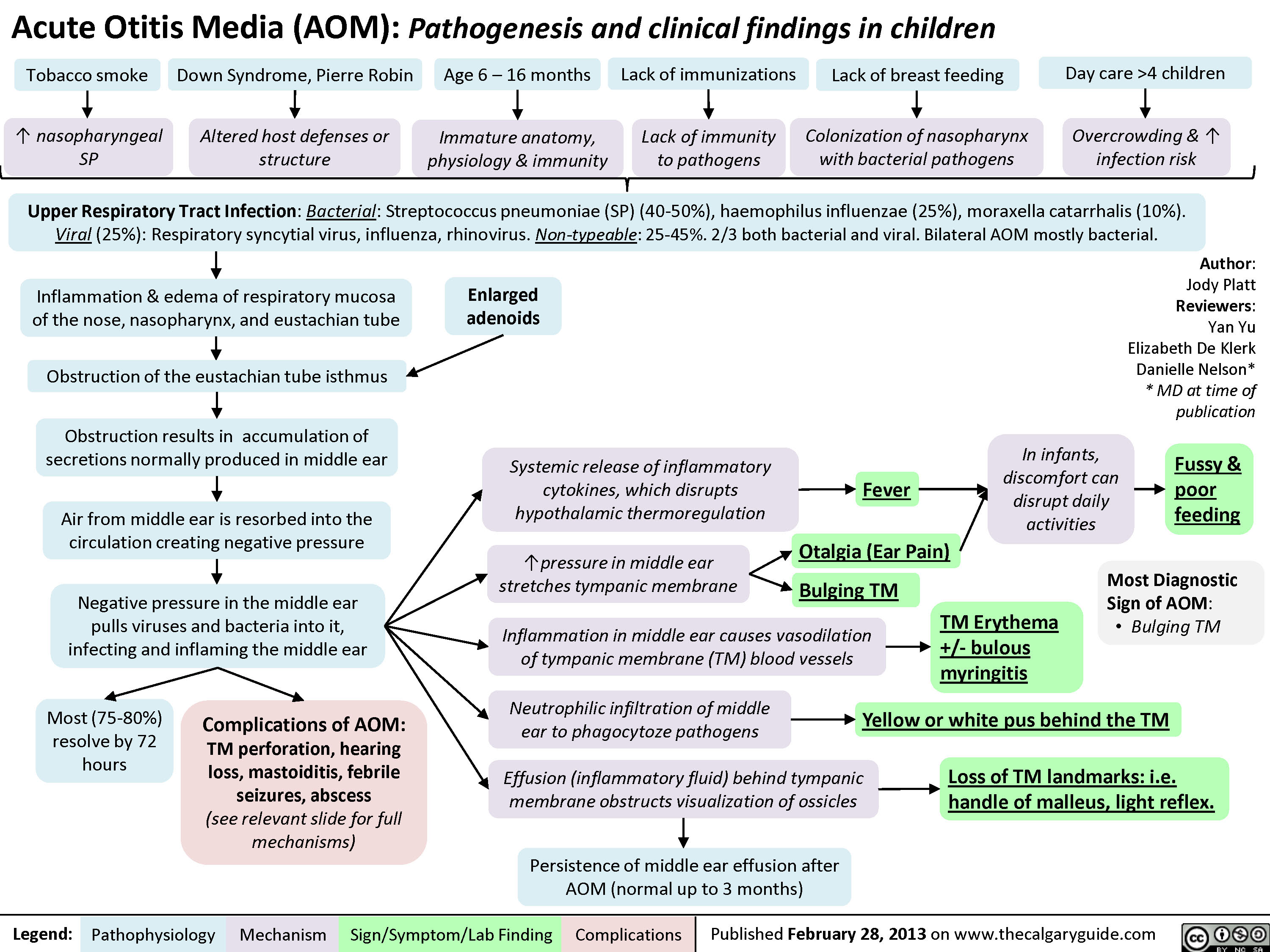
Acute Otitis Media: Pathogenesis and Clinical Findings (in Children)
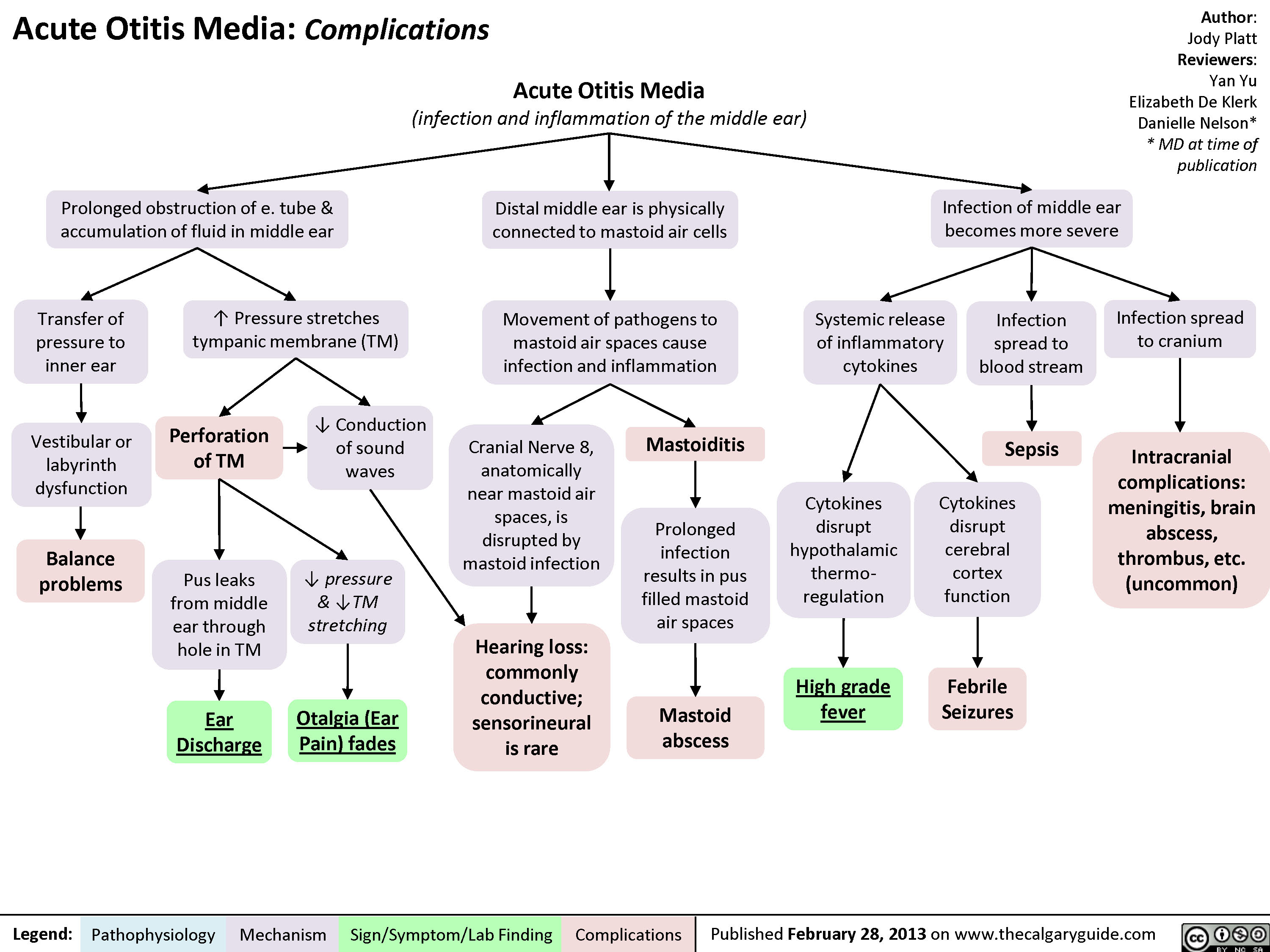
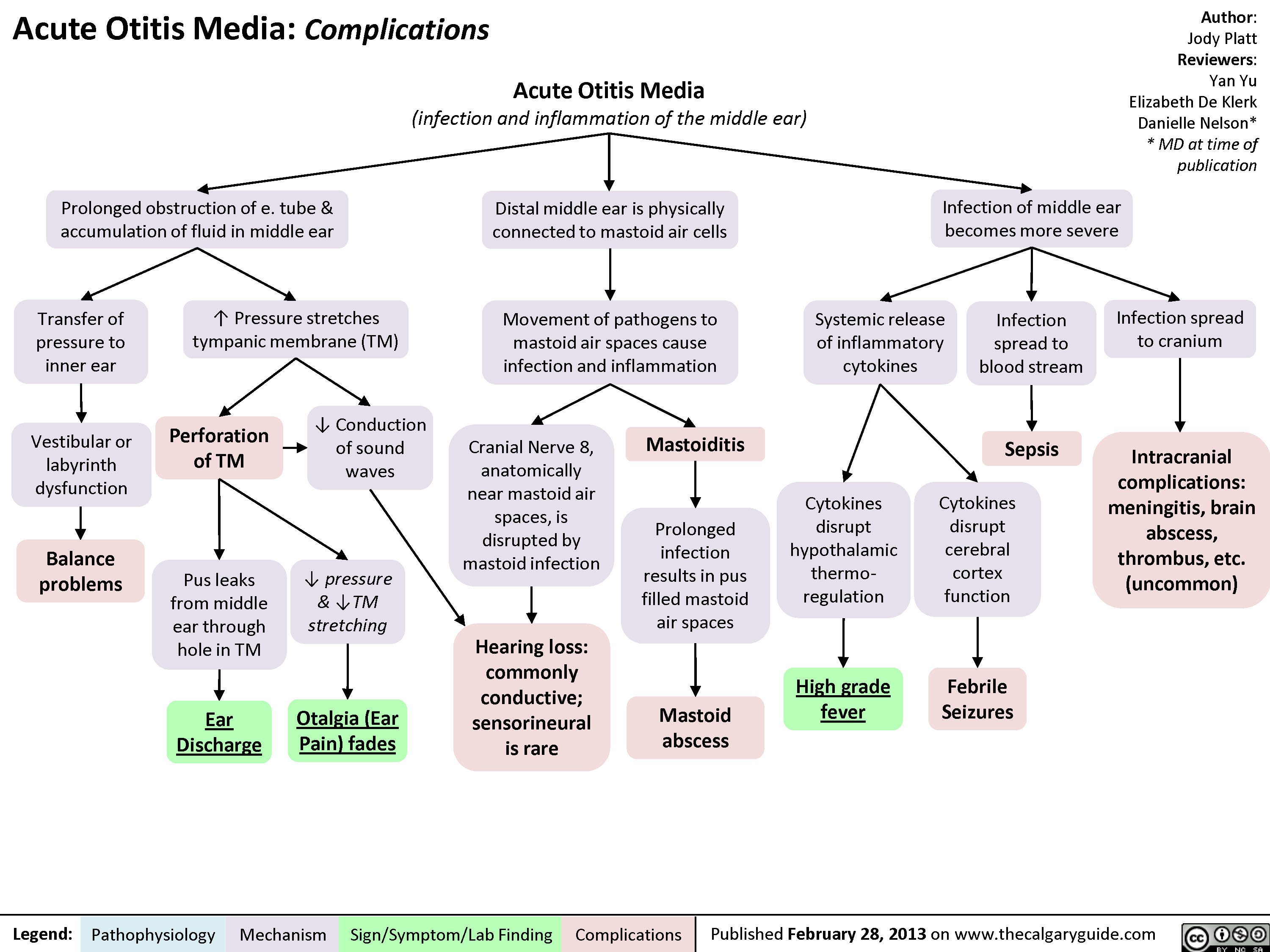
Acute Otitis Media: Complications
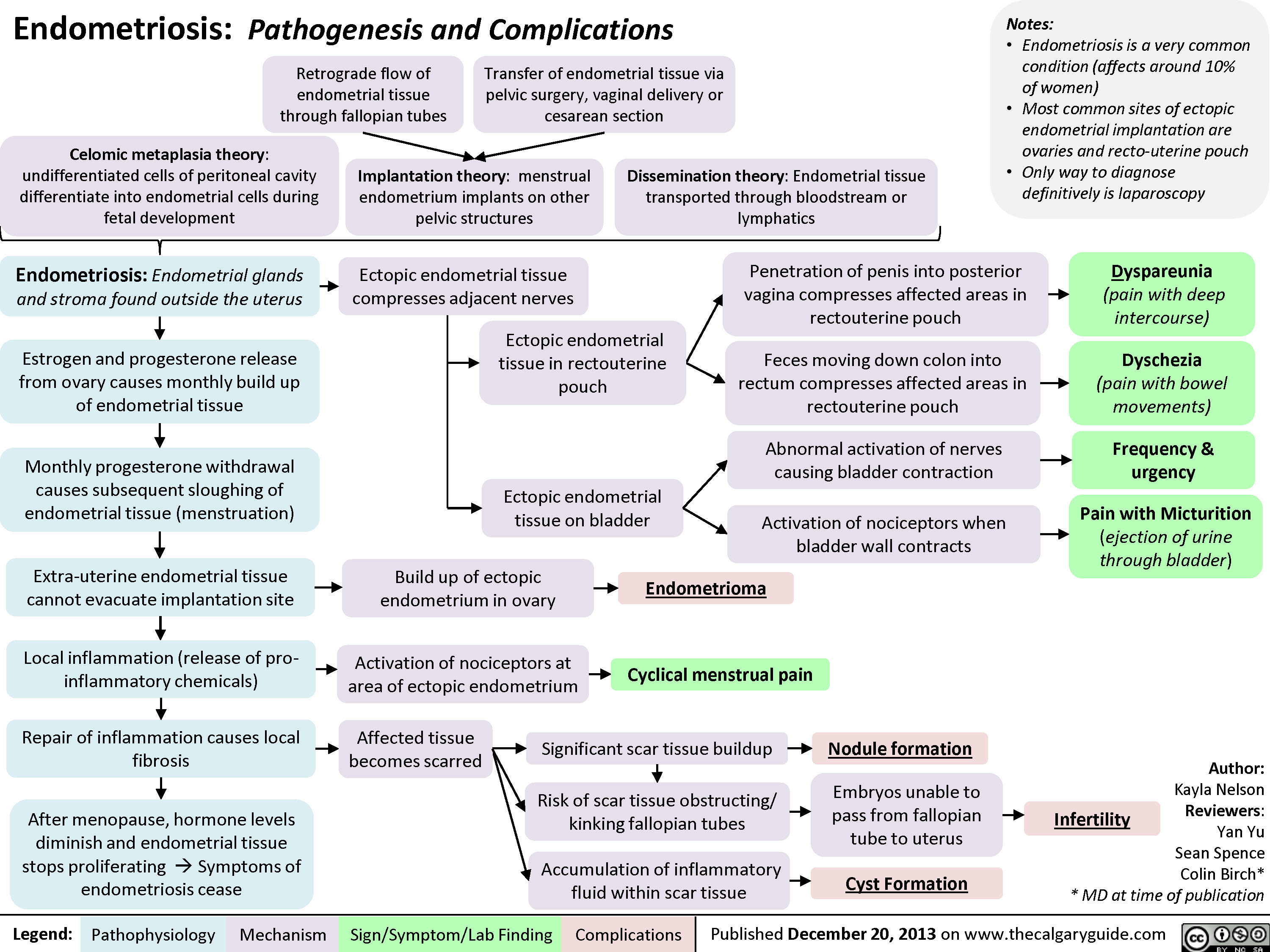
Endometriosis: Pathogenesis and Complications
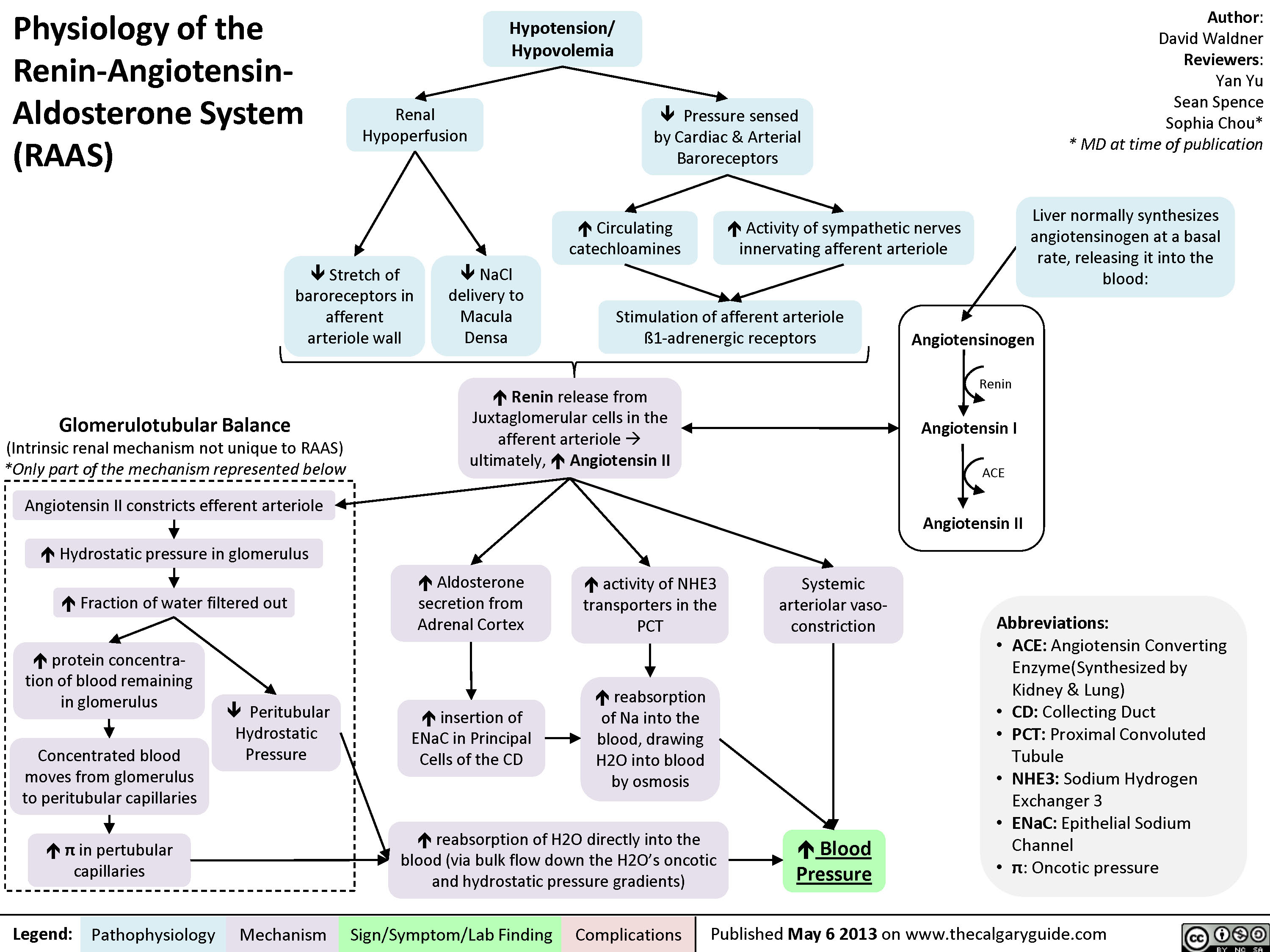
Physiology of the Renin-Angiotensin-Aldosterone System (RAAS)
Hypokalemia: Clinical Findings
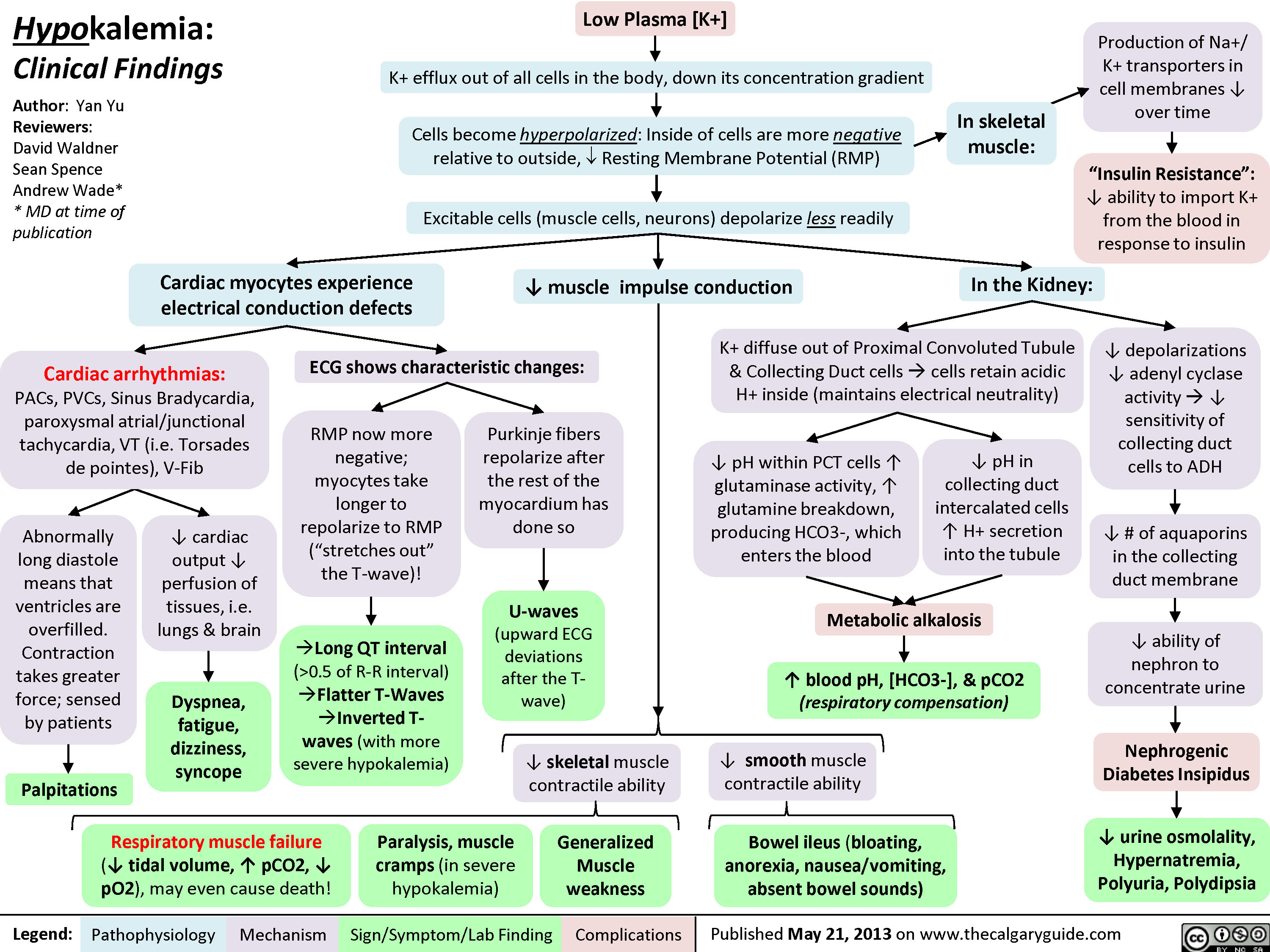 0.5 of R-R interval)?Flatter T-Waves ?Inverted T-waves (with more severe hypokalemia)Purkinje fibers repolarize after the rest of the myocardium has done soU-waves (upward ECG deviations after the T-wave)Cells become hyperpolarized: Inside of cells are more negative relative to outside, ? Resting Membrane Potential (RMP)In the Kidney:Generalized Muscle weaknessK+ diffuse out of Proximal Convoluted Tubule & Collecting Duct cells ? cells retain acidic H+ inside (maintains electrical neutrality)? pH within PCT cells ? glutaminase activity, ? glutamine breakdown, producing HCO3-, which enters the blood? blood pH, [HCO3-], & pCO2 (respiratory compensation)Low Plasma [K+]Abnormally long diastole means that ventricles are overfilled. Contraction takes greater force; sensed by patientsDyspnea, fatigue, dizziness, syncope? cardiac output ? perfusion of tissues, i.e. lungs & brainCardiac arrhythmias: PACs, PVCs, Sinus Bradycardia, paroxysmal atrial/junctional tachycardia, VT (i.e. Torsades de pointes), V-Fib? smooth muscle contractile abilityBowel ileus (bloating, anorexia, nausea/vomiting, absent bowel sounds)? pH in collecting duct intercalated cells ? H+ secretion into the tubuleMetabolic alkalosisParalysis, muscle cramps (in severe hypokalemia)Respiratory muscle failure (? tidal volume, ? pCO2, ? pO2), may even cause death!? depolarizations ? adenyl cyclase activity ? ? sensitivity of collecting duct cells to ADH? ability of nephron to concentrate urineNephrogenic Diabetes Insipidus? urine osmolality, Hypernatremia, Polyuria, Polydipsia? # of aquaporins in the collecting duct membrane"Insulin Resistance": ? ability to import K+ from the blood in response to insulinIn skeletal muscle:
117 kB / 307 word" title="Yu, Yan - Hypokalemia clinical findings - FINAL.pptx
Production of Na+/ K+ transporters in cell membranes ? over timeHypokalemia: Clinical FindingsAuthor: Yan YuReviewers:David WaldnerSean SpenceAndrew Wade** MD at time of publicationLegend:Published May 21, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsPalpitationsExcitable cells (muscle cells, neurons) depolarize less readilyK+ efflux out of all cells in the body, down its concentration gradientCardiac myocytes experience electrical conduction defects? muscle impulse conductionECG shows characteristic changes:? skeletal muscle contractile abilityRMP now more negative; myocytes take longer to repolarize to RMP("stretches out" the T-wave)! Long QT interval (>0.5 of R-R interval)?Flatter T-Waves ?Inverted T-waves (with more severe hypokalemia)Purkinje fibers repolarize after the rest of the myocardium has done soU-waves (upward ECG deviations after the T-wave)Cells become hyperpolarized: Inside of cells are more negative relative to outside, ? Resting Membrane Potential (RMP)In the Kidney:Generalized Muscle weaknessK+ diffuse out of Proximal Convoluted Tubule & Collecting Duct cells ? cells retain acidic H+ inside (maintains electrical neutrality)? pH within PCT cells ? glutaminase activity, ? glutamine breakdown, producing HCO3-, which enters the blood? blood pH, [HCO3-], & pCO2 (respiratory compensation)Low Plasma [K+]Abnormally long diastole means that ventricles are overfilled. Contraction takes greater force; sensed by patientsDyspnea, fatigue, dizziness, syncope? cardiac output ? perfusion of tissues, i.e. lungs & brainCardiac arrhythmias: PACs, PVCs, Sinus Bradycardia, paroxysmal atrial/junctional tachycardia, VT (i.e. Torsades de pointes), V-Fib? smooth muscle contractile abilityBowel ileus (bloating, anorexia, nausea/vomiting, absent bowel sounds)? pH in collecting duct intercalated cells ? H+ secretion into the tubuleMetabolic alkalosisParalysis, muscle cramps (in severe hypokalemia)Respiratory muscle failure (? tidal volume, ? pCO2, ? pO2), may even cause death!? depolarizations ? adenyl cyclase activity ? ? sensitivity of collecting duct cells to ADH? ability of nephron to concentrate urineNephrogenic Diabetes Insipidus? urine osmolality, Hypernatremia, Polyuria, Polydipsia? # of aquaporins in the collecting duct membrane"Insulin Resistance": ? ability to import K+ from the blood in response to insulinIn skeletal muscle:
117 kB / 307 word" />
0.5 of R-R interval)?Flatter T-Waves ?Inverted T-waves (with more severe hypokalemia)Purkinje fibers repolarize after the rest of the myocardium has done soU-waves (upward ECG deviations after the T-wave)Cells become hyperpolarized: Inside of cells are more negative relative to outside, ? Resting Membrane Potential (RMP)In the Kidney:Generalized Muscle weaknessK+ diffuse out of Proximal Convoluted Tubule & Collecting Duct cells ? cells retain acidic H+ inside (maintains electrical neutrality)? pH within PCT cells ? glutaminase activity, ? glutamine breakdown, producing HCO3-, which enters the blood? blood pH, [HCO3-], & pCO2 (respiratory compensation)Low Plasma [K+]Abnormally long diastole means that ventricles are overfilled. Contraction takes greater force; sensed by patientsDyspnea, fatigue, dizziness, syncope? cardiac output ? perfusion of tissues, i.e. lungs & brainCardiac arrhythmias: PACs, PVCs, Sinus Bradycardia, paroxysmal atrial/junctional tachycardia, VT (i.e. Torsades de pointes), V-Fib? smooth muscle contractile abilityBowel ileus (bloating, anorexia, nausea/vomiting, absent bowel sounds)? pH in collecting duct intercalated cells ? H+ secretion into the tubuleMetabolic alkalosisParalysis, muscle cramps (in severe hypokalemia)Respiratory muscle failure (? tidal volume, ? pCO2, ? pO2), may even cause death!? depolarizations ? adenyl cyclase activity ? ? sensitivity of collecting duct cells to ADH? ability of nephron to concentrate urineNephrogenic Diabetes Insipidus? urine osmolality, Hypernatremia, Polyuria, Polydipsia? # of aquaporins in the collecting duct membrane"Insulin Resistance": ? ability to import K+ from the blood in response to insulinIn skeletal muscle:
117 kB / 307 word" title="Yu, Yan - Hypokalemia clinical findings - FINAL.pptx
Production of Na+/ K+ transporters in cell membranes ? over timeHypokalemia: Clinical FindingsAuthor: Yan YuReviewers:David WaldnerSean SpenceAndrew Wade** MD at time of publicationLegend:Published May 21, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsPalpitationsExcitable cells (muscle cells, neurons) depolarize less readilyK+ efflux out of all cells in the body, down its concentration gradientCardiac myocytes experience electrical conduction defects? muscle impulse conductionECG shows characteristic changes:? skeletal muscle contractile abilityRMP now more negative; myocytes take longer to repolarize to RMP("stretches out" the T-wave)! Long QT interval (>0.5 of R-R interval)?Flatter T-Waves ?Inverted T-waves (with more severe hypokalemia)Purkinje fibers repolarize after the rest of the myocardium has done soU-waves (upward ECG deviations after the T-wave)Cells become hyperpolarized: Inside of cells are more negative relative to outside, ? Resting Membrane Potential (RMP)In the Kidney:Generalized Muscle weaknessK+ diffuse out of Proximal Convoluted Tubule & Collecting Duct cells ? cells retain acidic H+ inside (maintains electrical neutrality)? pH within PCT cells ? glutaminase activity, ? glutamine breakdown, producing HCO3-, which enters the blood? blood pH, [HCO3-], & pCO2 (respiratory compensation)Low Plasma [K+]Abnormally long diastole means that ventricles are overfilled. Contraction takes greater force; sensed by patientsDyspnea, fatigue, dizziness, syncope? cardiac output ? perfusion of tissues, i.e. lungs & brainCardiac arrhythmias: PACs, PVCs, Sinus Bradycardia, paroxysmal atrial/junctional tachycardia, VT (i.e. Torsades de pointes), V-Fib? smooth muscle contractile abilityBowel ileus (bloating, anorexia, nausea/vomiting, absent bowel sounds)? pH in collecting duct intercalated cells ? H+ secretion into the tubuleMetabolic alkalosisParalysis, muscle cramps (in severe hypokalemia)Respiratory muscle failure (? tidal volume, ? pCO2, ? pO2), may even cause death!? depolarizations ? adenyl cyclase activity ? ? sensitivity of collecting duct cells to ADH? ability of nephron to concentrate urineNephrogenic Diabetes Insipidus? urine osmolality, Hypernatremia, Polyuria, Polydipsia? # of aquaporins in the collecting duct membrane"Insulin Resistance": ? ability to import K+ from the blood in response to insulinIn skeletal muscle:
117 kB / 307 word" />
Hyperkalemia: Clinical Findings
![Yu, Yan - Hyperkalemia clinical findings - Published.pptx
Hyperkalemia: Clinical FindingsAuthor: Yan YuReviewers:Alexander ArnoldDavid WaldnerSean SpenceAndrew Wade** MD at time of publicationLegend:Published September 9, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsPalpitationsNotes: Symptoms usually manifest when plasma [K+] > 7.0 mmol/L, but can occur at lower [K+]s when hyperkalemia is acute.ECG changes can, but don't necessarily, correlate with a particular [K+].Initially: Excitable cells (muscle cells, neurons) undergo action potentials more readily? [K+ ] gradient between cells and the blood (K+ tends to stay inside cells, less K+ diffuses out)In the Heart:In Skeletal Muscle:[K+] >5.5 mmol/L :faster myocardial repolarization(](http://calgaryguide.ucalgary.ca/wp-content/uploads/2014/09/hyperkalemiaclinicalfindings.jpg) 6.5 mmol/L:? atrial conduction; slow signal transmission from SA to AV nodeCells become slightly depolarized: Resting Membrane Potential (RMP) is brought closer to thresholdIn the Kidney:Muscle weakness and even paralysis (respiratory muscle weakness is rare)? reabsorption of Na+ from Cortical Collecting Duct (CCD)CCD lumen remains more positively chargedMetabolic Acidosis(normal anion gap)Over time (when patients become symptomatic): Chronic membrane depolarization desensitizes voltage-gated Na+ channels (slows their opening) ? ? membrane excitability ? ? action potential generation[K+] > 7.0 mmol/L:? ventricular conductionBradycardiaProlonged, abnormal QRSAV blocks[K+] > 9.0 mmol/L:more conduction abnormalitiesPEA with bizarre wide-QRS rhythmV-fibAsystole? urinary H+ secretion by alpha-intercalated cellsHIGH Plasma [K+] (potassium ion concentration)Dyspnea, fatigue, dizziness, syncope? cardiac output ? ? perfusion of tissues, i.e. lungs & brainCardiac arrhythmias: Conduction blocks (AV block, Bundle branch blocks), VT , V-Fib, Bradycardia, Asystole.?? PR interval ?P-wave flattens, eventually disappearsIf severe, QRS & T-waves fuse:Sine-WavesThe higher the [K+], the slower the voltage-gated Na+ channels open, reflected by distinctive ECG changes:If the K+ is due to ? aldosterone effect ? principal cell dysfunctionHigh pH ? glutamate deamination, which normally produces NH4+? NH4+ reaches the thick ascending limb to be converted to NH3Less NH3 diffuses into the collecting duct to be converted to NH4+ through binding with H+ ? ? NH4+ and therefore ? H+ is excretedK+ moves into proximal tubule cells, causing H+ to diffuse out ? Intracellular alkalosis Irregular force and rhythm of cardiac muscle contraction is sensed by the patient? contraction impulse is conductedDefective electrical conduction through cardiac myocytesMore acid (H=) is retained in the body
118 kB / 357 words" title="Yu, Yan - Hyperkalemia clinical findings - Published.pptx
Hyperkalemia: Clinical FindingsAuthor: Yan YuReviewers:Alexander ArnoldDavid WaldnerSean SpenceAndrew Wade** MD at time of publicationLegend:Published September 9, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsPalpitationsNotes: Symptoms usually manifest when plasma [K+] > 7.0 mmol/L, but can occur at lower [K+]s when hyperkalemia is acute.ECG changes can, but don't necessarily, correlate with a particular [K+].Initially: Excitable cells (muscle cells, neurons) undergo action potentials more readily? [K+ ] gradient between cells and the blood (K+ tends to stay inside cells, less K+ diffuses out)In the Heart:In Skeletal Muscle:[K+] >5.5 mmol/L :faster myocardial repolarization("squeezes up" T-wave)Tall, peaked T-Waves Short QT interval (<0.5 of RR interval)[K+] > 6.5 mmol/L:? atrial conduction; slow signal transmission from SA to AV nodeCells become slightly depolarized: Resting Membrane Potential (RMP) is brought closer to thresholdIn the Kidney:Muscle weakness and even paralysis (respiratory muscle weakness is rare)? reabsorption of Na+ from Cortical Collecting Duct (CCD)CCD lumen remains more positively chargedMetabolic Acidosis(normal anion gap)Over time (when patients become symptomatic): Chronic membrane depolarization desensitizes voltage-gated Na+ channels (slows their opening) ? ? membrane excitability ? ? action potential generation[K+] > 7.0 mmol/L:? ventricular conductionBradycardiaProlonged, abnormal QRSAV blocks[K+] > 9.0 mmol/L:more conduction abnormalitiesPEA with bizarre wide-QRS rhythmV-fibAsystole? urinary H+ secretion by alpha-intercalated cellsHIGH Plasma [K+] (potassium ion concentration)Dyspnea, fatigue, dizziness, syncope? cardiac output ? ? perfusion of tissues, i.e. lungs & brainCardiac arrhythmias: Conduction blocks (AV block, Bundle branch blocks), VT , V-Fib, Bradycardia, Asystole.?? PR interval ?P-wave flattens, eventually disappearsIf severe, QRS & T-waves fuse:Sine-WavesThe higher the [K+], the slower the voltage-gated Na+ channels open, reflected by distinctive ECG changes:If the K+ is due to ? aldosterone effect ? principal cell dysfunctionHigh pH ? glutamate deamination, which normally produces NH4+? NH4+ reaches the thick ascending limb to be converted to NH3Less NH3 diffuses into the collecting duct to be converted to NH4+ through binding with H+ ? ? NH4+ and therefore ? H+ is excretedK+ moves into proximal tubule cells, causing H+ to diffuse out ? Intracellular alkalosis Irregular force and rhythm of cardiac muscle contraction is sensed by the patient? contraction impulse is conductedDefective electrical conduction through cardiac myocytesMore acid (H=) is retained in the body
118 kB / 357 words" />
6.5 mmol/L:? atrial conduction; slow signal transmission from SA to AV nodeCells become slightly depolarized: Resting Membrane Potential (RMP) is brought closer to thresholdIn the Kidney:Muscle weakness and even paralysis (respiratory muscle weakness is rare)? reabsorption of Na+ from Cortical Collecting Duct (CCD)CCD lumen remains more positively chargedMetabolic Acidosis(normal anion gap)Over time (when patients become symptomatic): Chronic membrane depolarization desensitizes voltage-gated Na+ channels (slows their opening) ? ? membrane excitability ? ? action potential generation[K+] > 7.0 mmol/L:? ventricular conductionBradycardiaProlonged, abnormal QRSAV blocks[K+] > 9.0 mmol/L:more conduction abnormalitiesPEA with bizarre wide-QRS rhythmV-fibAsystole? urinary H+ secretion by alpha-intercalated cellsHIGH Plasma [K+] (potassium ion concentration)Dyspnea, fatigue, dizziness, syncope? cardiac output ? ? perfusion of tissues, i.e. lungs & brainCardiac arrhythmias: Conduction blocks (AV block, Bundle branch blocks), VT , V-Fib, Bradycardia, Asystole.?? PR interval ?P-wave flattens, eventually disappearsIf severe, QRS & T-waves fuse:Sine-WavesThe higher the [K+], the slower the voltage-gated Na+ channels open, reflected by distinctive ECG changes:If the K+ is due to ? aldosterone effect ? principal cell dysfunctionHigh pH ? glutamate deamination, which normally produces NH4+? NH4+ reaches the thick ascending limb to be converted to NH3Less NH3 diffuses into the collecting duct to be converted to NH4+ through binding with H+ ? ? NH4+ and therefore ? H+ is excretedK+ moves into proximal tubule cells, causing H+ to diffuse out ? Intracellular alkalosis Irregular force and rhythm of cardiac muscle contraction is sensed by the patient? contraction impulse is conductedDefective electrical conduction through cardiac myocytesMore acid (H=) is retained in the body
118 kB / 357 words" title="Yu, Yan - Hyperkalemia clinical findings - Published.pptx
Hyperkalemia: Clinical FindingsAuthor: Yan YuReviewers:Alexander ArnoldDavid WaldnerSean SpenceAndrew Wade** MD at time of publicationLegend:Published September 9, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsPalpitationsNotes: Symptoms usually manifest when plasma [K+] > 7.0 mmol/L, but can occur at lower [K+]s when hyperkalemia is acute.ECG changes can, but don't necessarily, correlate with a particular [K+].Initially: Excitable cells (muscle cells, neurons) undergo action potentials more readily? [K+ ] gradient between cells and the blood (K+ tends to stay inside cells, less K+ diffuses out)In the Heart:In Skeletal Muscle:[K+] >5.5 mmol/L :faster myocardial repolarization("squeezes up" T-wave)Tall, peaked T-Waves Short QT interval (<0.5 of RR interval)[K+] > 6.5 mmol/L:? atrial conduction; slow signal transmission from SA to AV nodeCells become slightly depolarized: Resting Membrane Potential (RMP) is brought closer to thresholdIn the Kidney:Muscle weakness and even paralysis (respiratory muscle weakness is rare)? reabsorption of Na+ from Cortical Collecting Duct (CCD)CCD lumen remains more positively chargedMetabolic Acidosis(normal anion gap)Over time (when patients become symptomatic): Chronic membrane depolarization desensitizes voltage-gated Na+ channels (slows their opening) ? ? membrane excitability ? ? action potential generation[K+] > 7.0 mmol/L:? ventricular conductionBradycardiaProlonged, abnormal QRSAV blocks[K+] > 9.0 mmol/L:more conduction abnormalitiesPEA with bizarre wide-QRS rhythmV-fibAsystole? urinary H+ secretion by alpha-intercalated cellsHIGH Plasma [K+] (potassium ion concentration)Dyspnea, fatigue, dizziness, syncope? cardiac output ? ? perfusion of tissues, i.e. lungs & brainCardiac arrhythmias: Conduction blocks (AV block, Bundle branch blocks), VT , V-Fib, Bradycardia, Asystole.?? PR interval ?P-wave flattens, eventually disappearsIf severe, QRS & T-waves fuse:Sine-WavesThe higher the [K+], the slower the voltage-gated Na+ channels open, reflected by distinctive ECG changes:If the K+ is due to ? aldosterone effect ? principal cell dysfunctionHigh pH ? glutamate deamination, which normally produces NH4+? NH4+ reaches the thick ascending limb to be converted to NH3Less NH3 diffuses into the collecting duct to be converted to NH4+ through binding with H+ ? ? NH4+ and therefore ? H+ is excretedK+ moves into proximal tubule cells, causing H+ to diffuse out ? Intracellular alkalosis Irregular force and rhythm of cardiac muscle contraction is sensed by the patient? contraction impulse is conductedDefective electrical conduction through cardiac myocytesMore acid (H=) is retained in the body
118 kB / 357 words" />
Hypocalcemia: Clinical Findings
![Yu, Yan - Hypocalcemia - Clinical Findings - FINAL.pptx
Hypocalcemia: Clinical FindingsAuthor: Yan YuReviewers:David WaldnerSean SpenceGreg Kline** MD at time of publicationLegend:Published May 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsHypocalcemia(serum [Ca2+] <2.1mmol/L)Altered sensory ability of peripheral nervesLess Ca2+ outside cells, with no change in + charges inside cellsPeripheral paraesthesia? Neuronal](http://calgaryguide.ucalgary.ca/wp-content/uploads/2014/09/Hypocalcemia-Clinical-Findings.jpg "Yu, Yan - Hypocalcemia - Clinical Findings - FINAL.pptx
Hypocalcemia: Clinical FindingsAuthor: Yan YuReviewers:David WaldnerSean SpenceGreg Kline** MD at time of publicationLegend:Published May 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsHypocalcemia(serum [Ca2+] <2.1mmol/L)Altered sensory ability of peripheral nervesLess Ca2+ outside cells, with no change in + charges inside cellsPeripheral paraesthesia? Neuronal")
Hypercalcemia: Clinical Findings
Nephrotic Syndrome: Pathogenesis and Clinical Findings
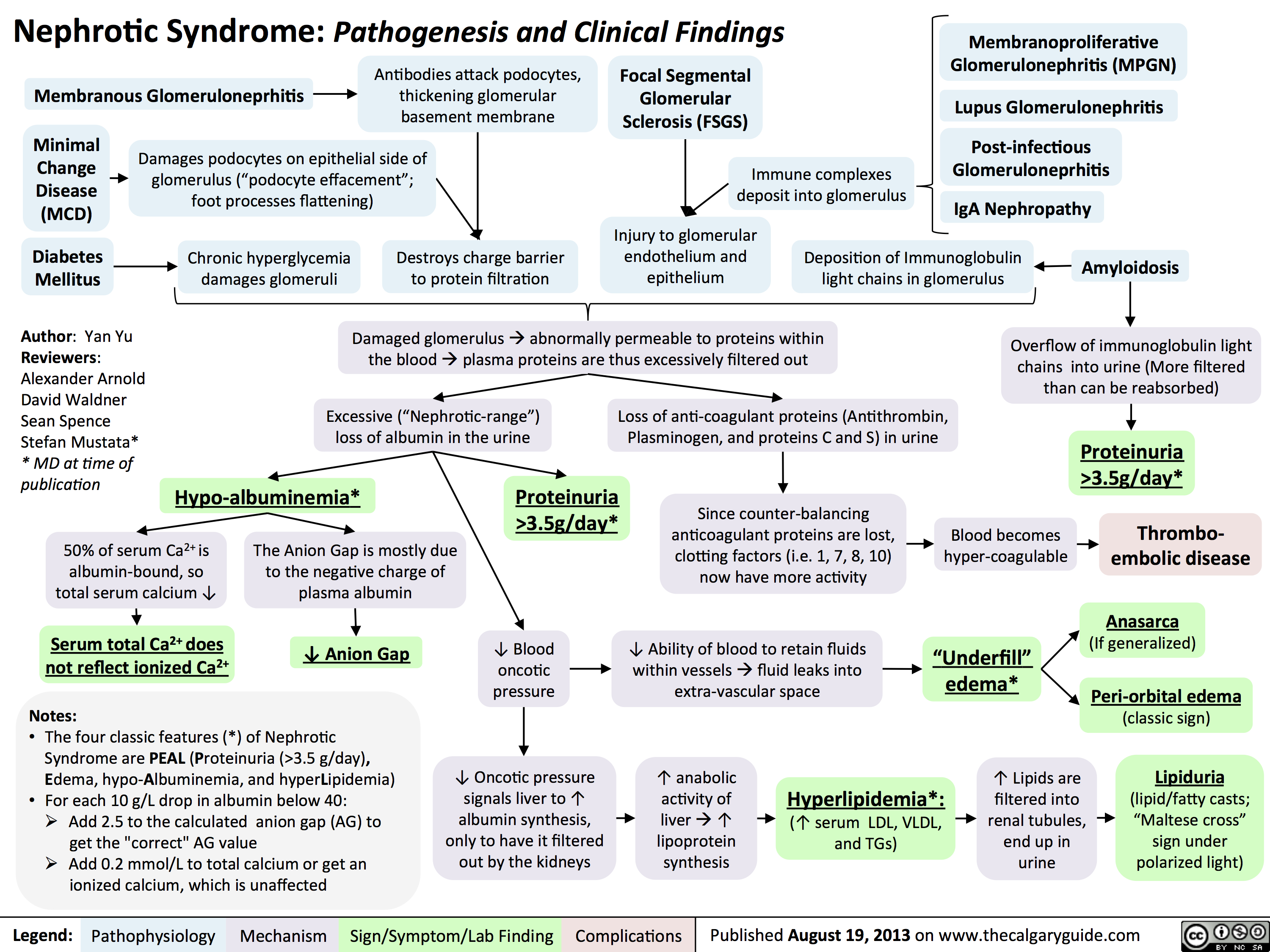 3.5g/day*? Ability of blood to retain fluids within vessels ? fluid leaks into extra-vascular spaceInjury to glomerular endothelium and epitheliumImmune complexes deposit into glomerulusDamaged glomerulus ? abnormally permeable to proteins within the blood ? plasma proteins are thus excessively filtered out? Oncotic pressure signals liver to ? albumin synthesis, only to have it filtered out by the kidneys? anabolic activity of liver ? ? lipoprotein synthesisHyperlipidemia*:(? serum LDL, VLDL, and TGs)Lipiduria(lipid/fatty casts; "Maltese cross" sign under polarized light)Since counter-balancing anticoagulant proteins are lost, clotting factors (i.e. 1, 7, 8, 10) now have more activityThrombo-embolic diseaseBlood becomes hyper-coagulable? Lipids are filtered into renal tubules, end up in urineMembranoproliferative Glomerulonephritis (MPGN)Lupus Glomerulonephritis Post-infectious GlomeruloneprhitisIgA NephropathyDamages podocytes on epithelial side of glomerulus ("podocyte effacement"; foot processes flattening)Diabetes MellitusChronic hyperglycemia damages glomeruliDeposition of Immunoglobulin light chains in glomerulusAmyloidosisAnasarca(If generalized)Peri-orbital edema (classic sign)Focal Segmental Glomerular Sclerosis (FSGS)Membranous GlomeruloneprhitisAntibodies attack podocytes, thickening glomerular basement membraneOverflow of immunoglobulin light chains into urine (More filtered than can be reabsorbed)Proteinuria >3.5g/day*The Anion Gap is mostly due to the negative charge of plasma albumin? Anion GapNotes: The four classic features (*) of Nephrotic Syndrome are PEAL (Proteinuria (>3.5 g/day), Edema, hypo-Albuminemia, and hyperLipidemia)For each 10 g/L drop in albumin below 40:Add 2.5 to the calculated anion gap (AG) to get the "correct" AG valueAdd 0.2 mmol/L to total calcium or get an ionized calcium, which is unaffected50% of serum Ca2+ is albumin-bound, so total serum calcium ? Serum total Ca2+ does not reflect ionized Ca2+ ? Blood oncotic pressure" title="Destroys charge barrier to protein filtrationNephrotic Syndrome: Pathogenesis and Clinical FindingsAuthor: Yan YuReviewers:Alexander ArnoldDavid WaldnerSean SpenceStefan Mustata** MD at time of publicationLegend:Published August 19, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsExcessive ("Nephrotic-range") loss of albumin in the urineHypo-albuminemia*Loss of anti-coagulant proteins (Antithrombin, Plasminogen, and proteins C and S) in urineMinimal Change Disease (MCD)"Underfill" edema*Proteinuria >3.5g/day*? Ability of blood to retain fluids within vessels ? fluid leaks into extra-vascular spaceInjury to glomerular endothelium and epitheliumImmune complexes deposit into glomerulusDamaged glomerulus ? abnormally permeable to proteins within the blood ? plasma proteins are thus excessively filtered out? Oncotic pressure signals liver to ? albumin synthesis, only to have it filtered out by the kidneys? anabolic activity of liver ? ? lipoprotein synthesisHyperlipidemia*:(? serum LDL, VLDL, and TGs)Lipiduria(lipid/fatty casts; "Maltese cross" sign under polarized light)Since counter-balancing anticoagulant proteins are lost, clotting factors (i.e. 1, 7, 8, 10) now have more activityThrombo-embolic diseaseBlood becomes hyper-coagulable? Lipids are filtered into renal tubules, end up in urineMembranoproliferative Glomerulonephritis (MPGN)Lupus Glomerulonephritis Post-infectious GlomeruloneprhitisIgA NephropathyDamages podocytes on epithelial side of glomerulus ("podocyte effacement"; foot processes flattening)Diabetes MellitusChronic hyperglycemia damages glomeruliDeposition of Immunoglobulin light chains in glomerulusAmyloidosisAnasarca(If generalized)Peri-orbital edema (classic sign)Focal Segmental Glomerular Sclerosis (FSGS)Membranous GlomeruloneprhitisAntibodies attack podocytes, thickening glomerular basement membraneOverflow of immunoglobulin light chains into urine (More filtered than can be reabsorbed)Proteinuria >3.5g/day*The Anion Gap is mostly due to the negative charge of plasma albumin? Anion GapNotes: The four classic features (*) of Nephrotic Syndrome are PEAL (Proteinuria (>3.5 g/day), Edema, hypo-Albuminemia, and hyperLipidemia)For each 10 g/L drop in albumin below 40:Add 2.5 to the calculated anion gap (AG) to get the "correct" AG valueAdd 0.2 mmol/L to total calcium or get an ionized calcium, which is unaffected50% of serum Ca2+ is albumin-bound, so total serum calcium ? Serum total Ca2+ does not reflect ionized Ca2+ ? Blood oncotic pressure" />
3.5g/day*? Ability of blood to retain fluids within vessels ? fluid leaks into extra-vascular spaceInjury to glomerular endothelium and epitheliumImmune complexes deposit into glomerulusDamaged glomerulus ? abnormally permeable to proteins within the blood ? plasma proteins are thus excessively filtered out? Oncotic pressure signals liver to ? albumin synthesis, only to have it filtered out by the kidneys? anabolic activity of liver ? ? lipoprotein synthesisHyperlipidemia*:(? serum LDL, VLDL, and TGs)Lipiduria(lipid/fatty casts; "Maltese cross" sign under polarized light)Since counter-balancing anticoagulant proteins are lost, clotting factors (i.e. 1, 7, 8, 10) now have more activityThrombo-embolic diseaseBlood becomes hyper-coagulable? Lipids are filtered into renal tubules, end up in urineMembranoproliferative Glomerulonephritis (MPGN)Lupus Glomerulonephritis Post-infectious GlomeruloneprhitisIgA NephropathyDamages podocytes on epithelial side of glomerulus ("podocyte effacement"; foot processes flattening)Diabetes MellitusChronic hyperglycemia damages glomeruliDeposition of Immunoglobulin light chains in glomerulusAmyloidosisAnasarca(If generalized)Peri-orbital edema (classic sign)Focal Segmental Glomerular Sclerosis (FSGS)Membranous GlomeruloneprhitisAntibodies attack podocytes, thickening glomerular basement membraneOverflow of immunoglobulin light chains into urine (More filtered than can be reabsorbed)Proteinuria >3.5g/day*The Anion Gap is mostly due to the negative charge of plasma albumin? Anion GapNotes: The four classic features (*) of Nephrotic Syndrome are PEAL (Proteinuria (>3.5 g/day), Edema, hypo-Albuminemia, and hyperLipidemia)For each 10 g/L drop in albumin below 40:Add 2.5 to the calculated anion gap (AG) to get the "correct" AG valueAdd 0.2 mmol/L to total calcium or get an ionized calcium, which is unaffected50% of serum Ca2+ is albumin-bound, so total serum calcium ? Serum total Ca2+ does not reflect ionized Ca2+ ? Blood oncotic pressure" title="Destroys charge barrier to protein filtrationNephrotic Syndrome: Pathogenesis and Clinical FindingsAuthor: Yan YuReviewers:Alexander ArnoldDavid WaldnerSean SpenceStefan Mustata** MD at time of publicationLegend:Published August 19, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsExcessive ("Nephrotic-range") loss of albumin in the urineHypo-albuminemia*Loss of anti-coagulant proteins (Antithrombin, Plasminogen, and proteins C and S) in urineMinimal Change Disease (MCD)"Underfill" edema*Proteinuria >3.5g/day*? Ability of blood to retain fluids within vessels ? fluid leaks into extra-vascular spaceInjury to glomerular endothelium and epitheliumImmune complexes deposit into glomerulusDamaged glomerulus ? abnormally permeable to proteins within the blood ? plasma proteins are thus excessively filtered out? Oncotic pressure signals liver to ? albumin synthesis, only to have it filtered out by the kidneys? anabolic activity of liver ? ? lipoprotein synthesisHyperlipidemia*:(? serum LDL, VLDL, and TGs)Lipiduria(lipid/fatty casts; "Maltese cross" sign under polarized light)Since counter-balancing anticoagulant proteins are lost, clotting factors (i.e. 1, 7, 8, 10) now have more activityThrombo-embolic diseaseBlood becomes hyper-coagulable? Lipids are filtered into renal tubules, end up in urineMembranoproliferative Glomerulonephritis (MPGN)Lupus Glomerulonephritis Post-infectious GlomeruloneprhitisIgA NephropathyDamages podocytes on epithelial side of glomerulus ("podocyte effacement"; foot processes flattening)Diabetes MellitusChronic hyperglycemia damages glomeruliDeposition of Immunoglobulin light chains in glomerulusAmyloidosisAnasarca(If generalized)Peri-orbital edema (classic sign)Focal Segmental Glomerular Sclerosis (FSGS)Membranous GlomeruloneprhitisAntibodies attack podocytes, thickening glomerular basement membraneOverflow of immunoglobulin light chains into urine (More filtered than can be reabsorbed)Proteinuria >3.5g/day*The Anion Gap is mostly due to the negative charge of plasma albumin? Anion GapNotes: The four classic features (*) of Nephrotic Syndrome are PEAL (Proteinuria (>3.5 g/day), Edema, hypo-Albuminemia, and hyperLipidemia)For each 10 g/L drop in albumin below 40:Add 2.5 to the calculated anion gap (AG) to get the "correct" AG valueAdd 0.2 mmol/L to total calcium or get an ionized calcium, which is unaffected50% of serum Ca2+ is albumin-bound, so total serum calcium ? Serum total Ca2+ does not reflect ionized Ca2+ ? Blood oncotic pressure" />
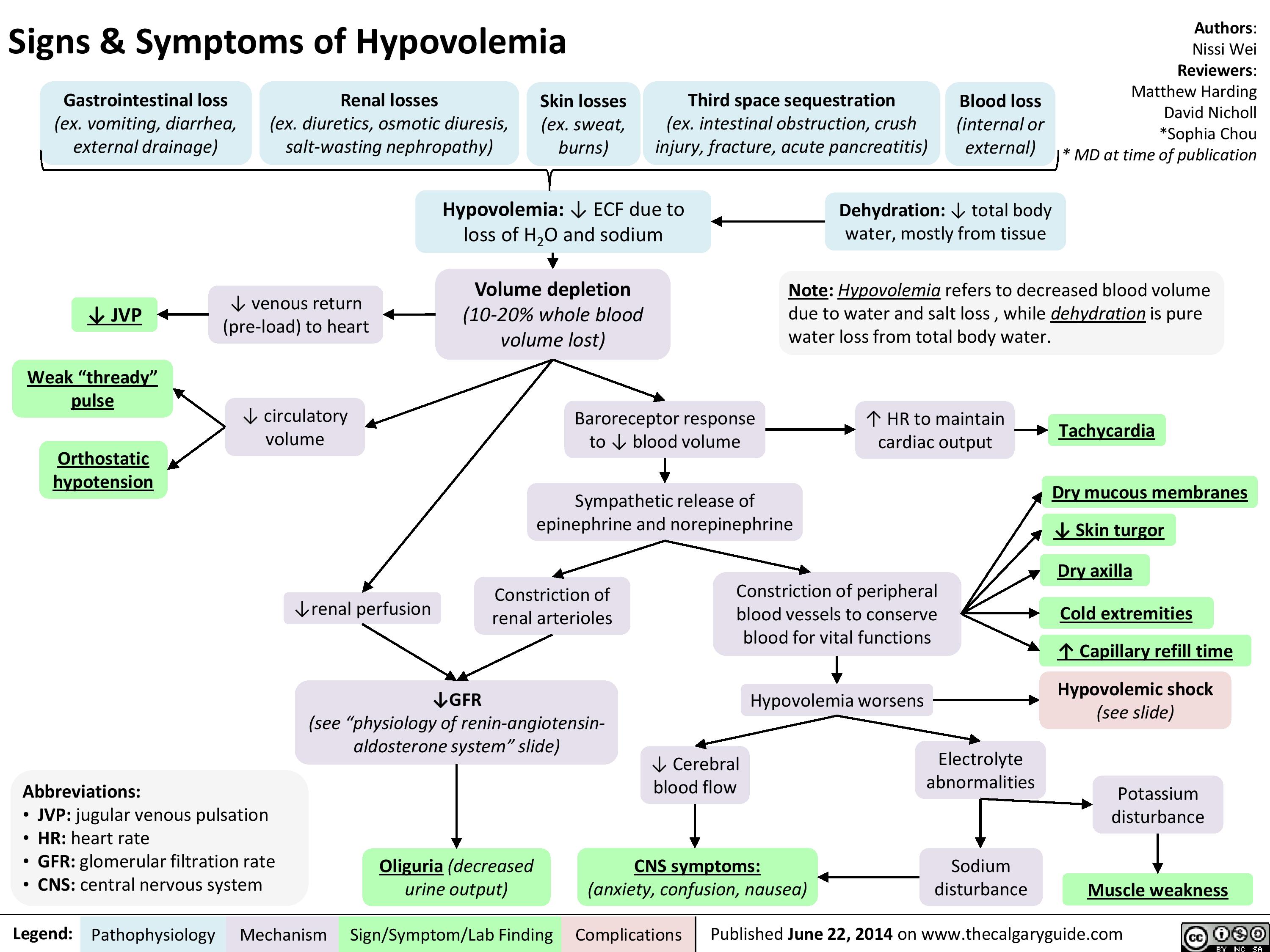
Signs and Symptoms of Hypovolemia
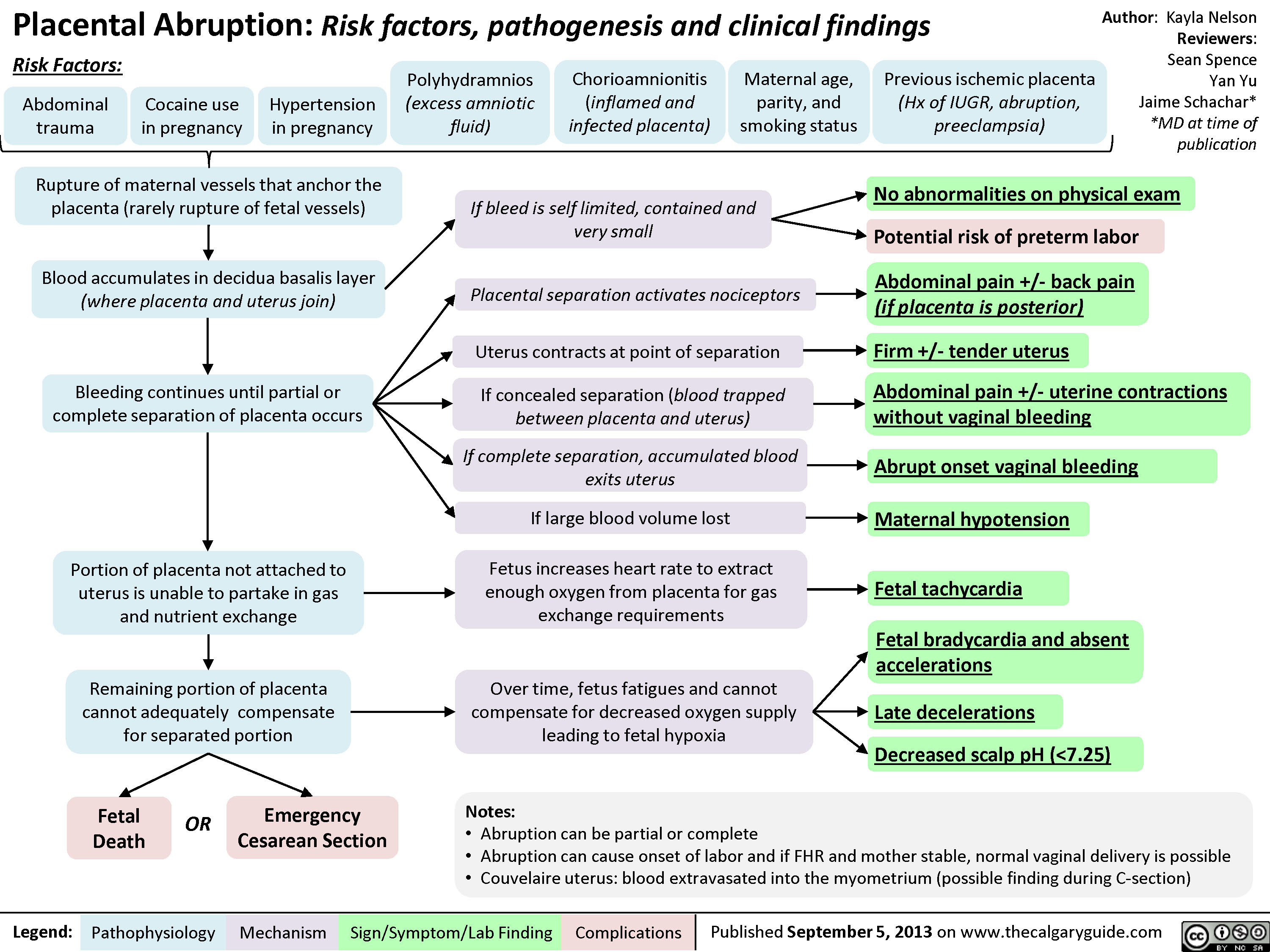
Placental Abruption
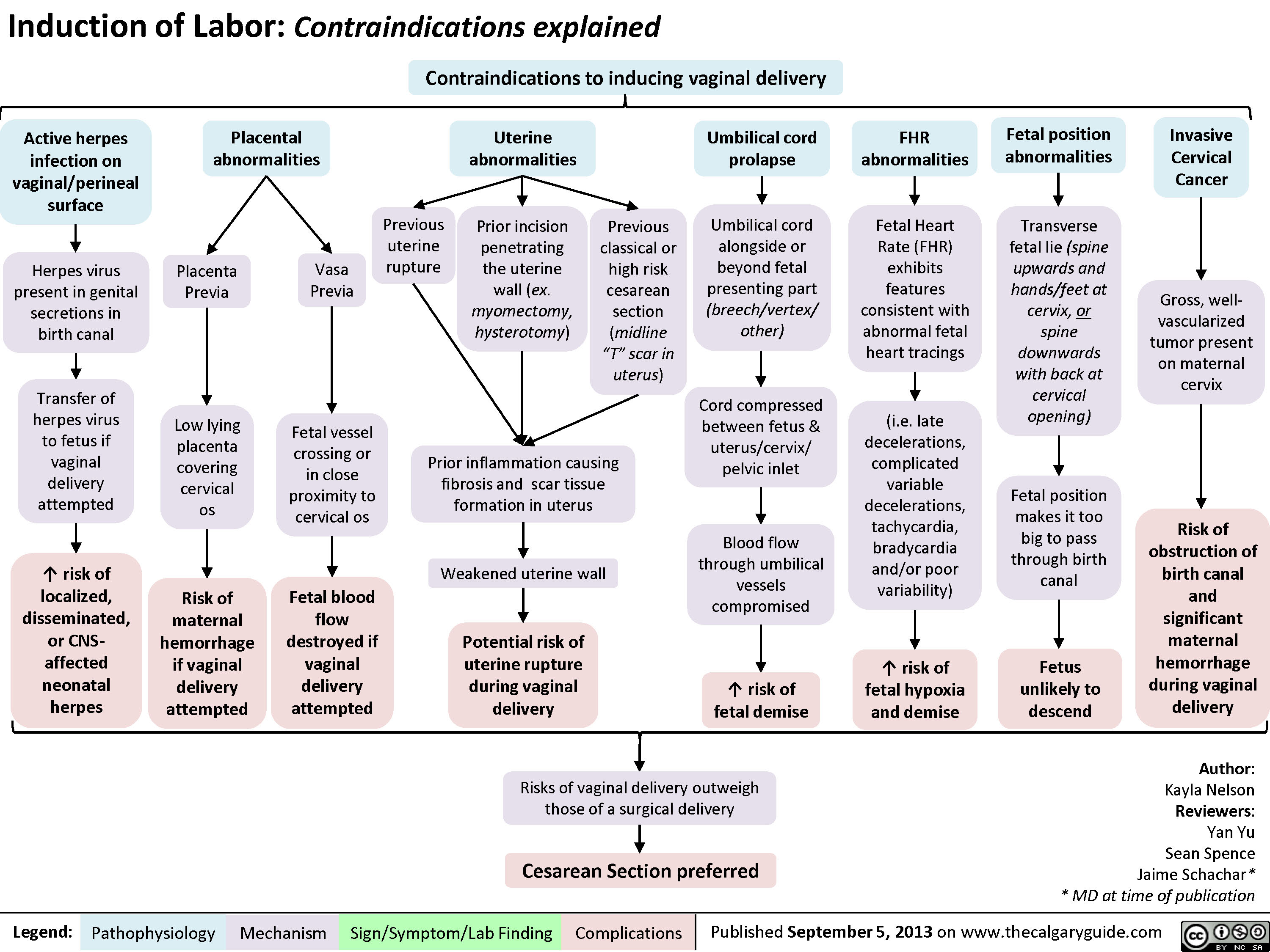
Contraindications to Inducing Vaginal Delivery
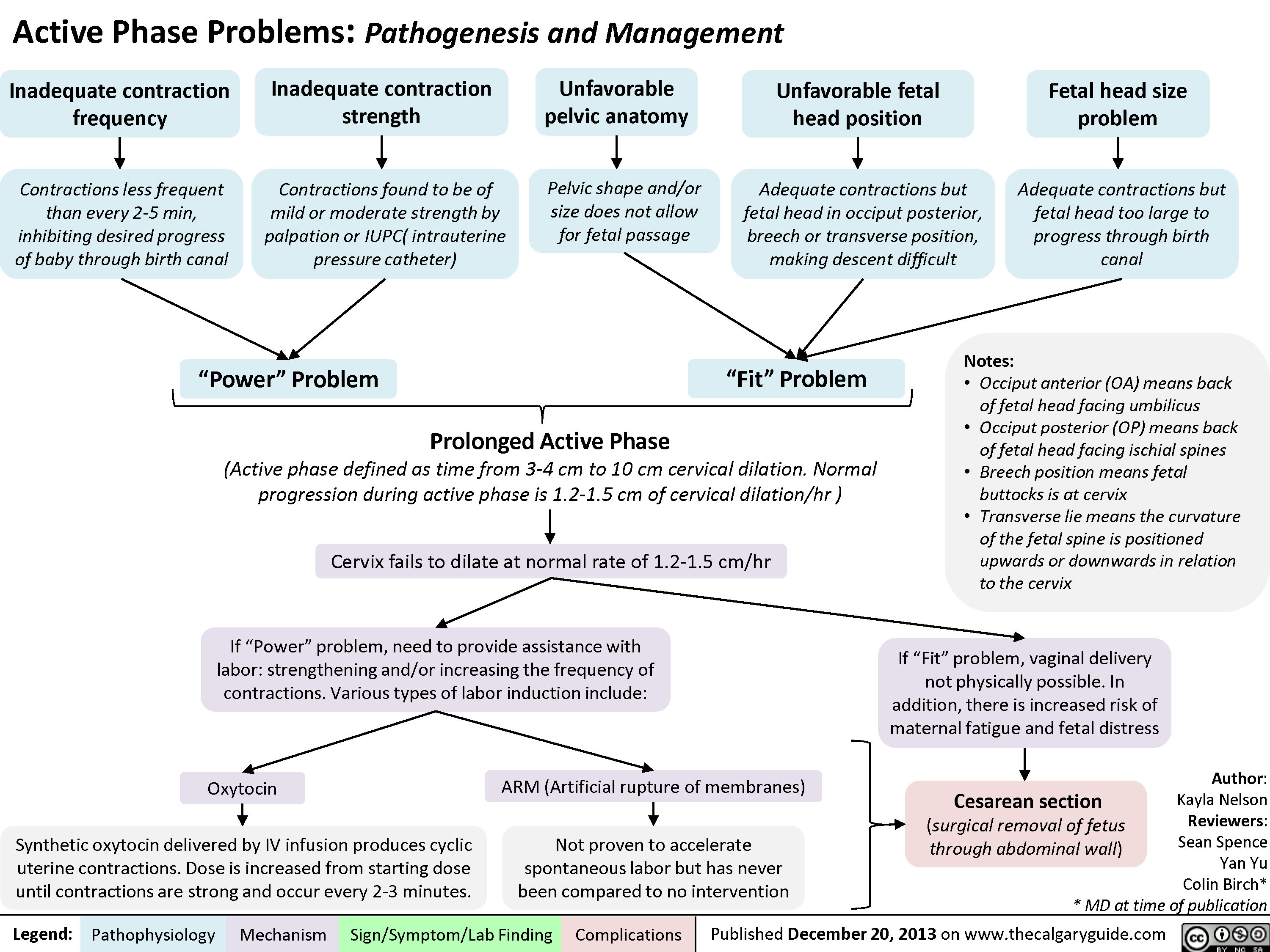
Active Phase Problems: Pathogenesis and Management
Normal Signs of Placental Detachment

Methods to Improve Fetal Oxygenation
 pattern (i.e. variable decelerations, mild tachycardia, mild ? in HR variability)? Mechanical stress on the fetus, to allow better perfusion of fetusImproved perfusion of maternal organs, including the uterus/fetusNote: if these methods do not restore normal FHR, perform scalp stimulation and scalp pH to better assess fetal hypoxia)Normal FHR pattern
91 kB / 187 words")
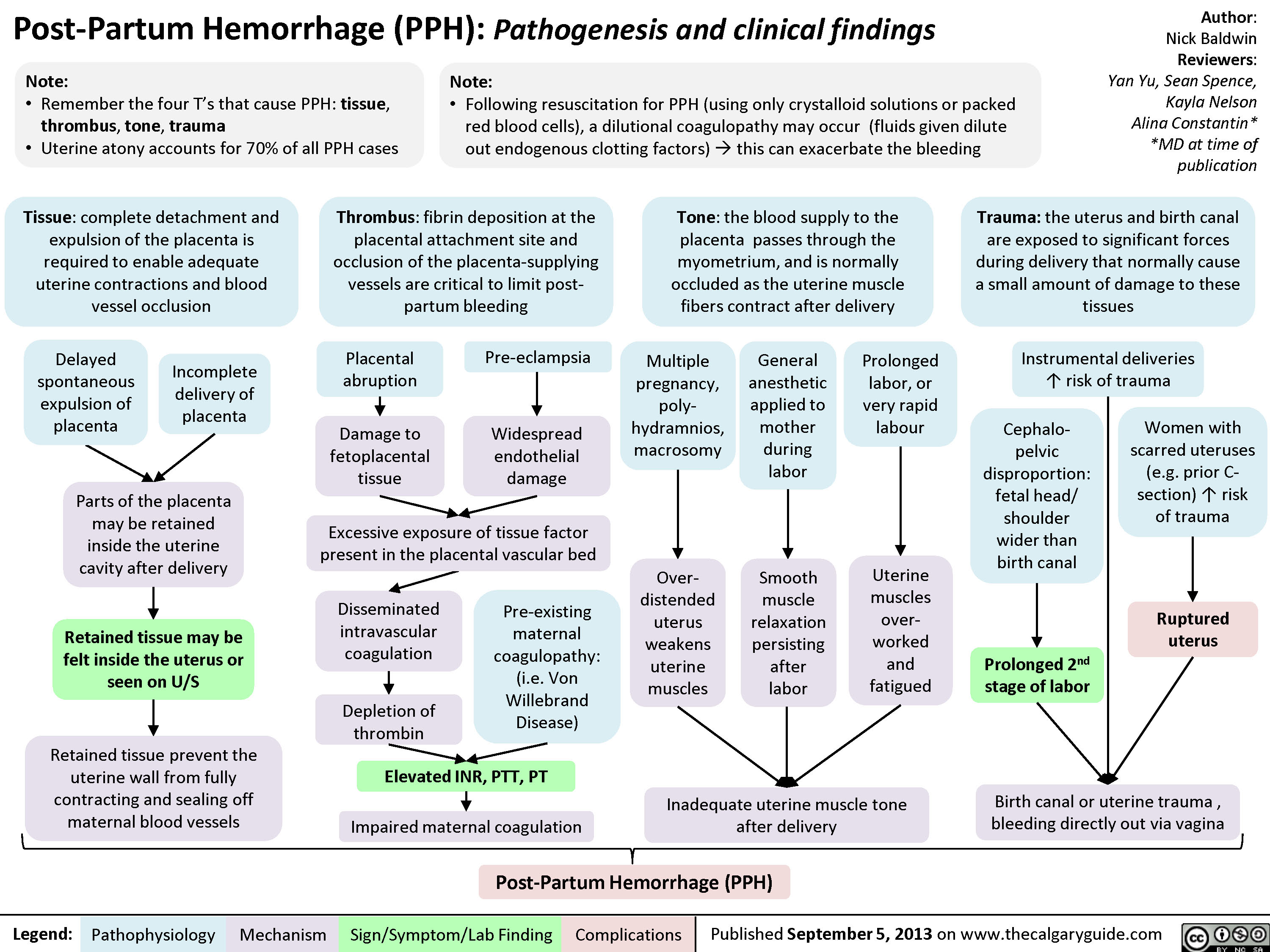
Post-Partum Hemorrhage
Upper Urinary Tract infection (UUTI): Pathogenesis and Clinical Findings

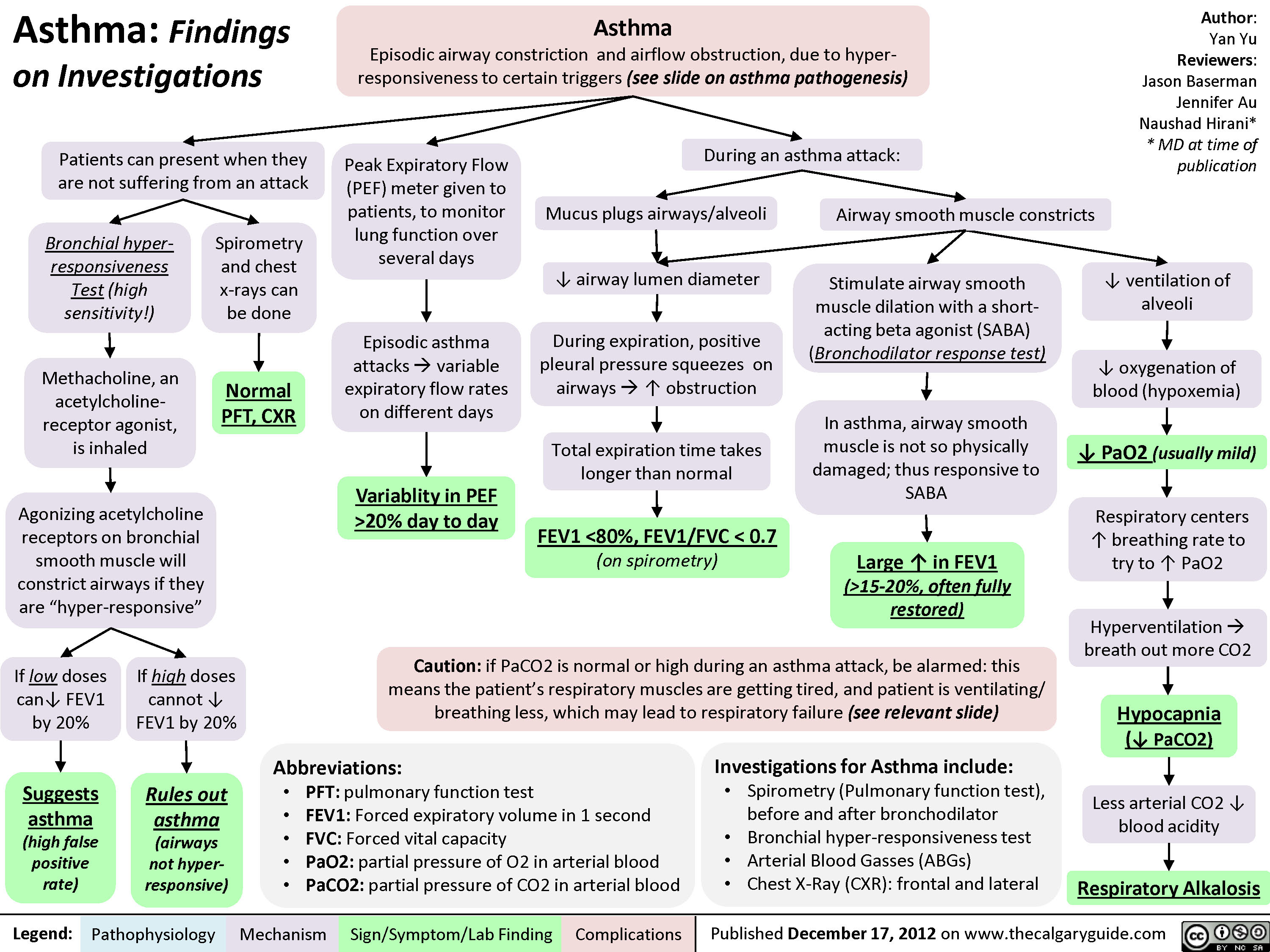
Asthma: Findings on Investigations
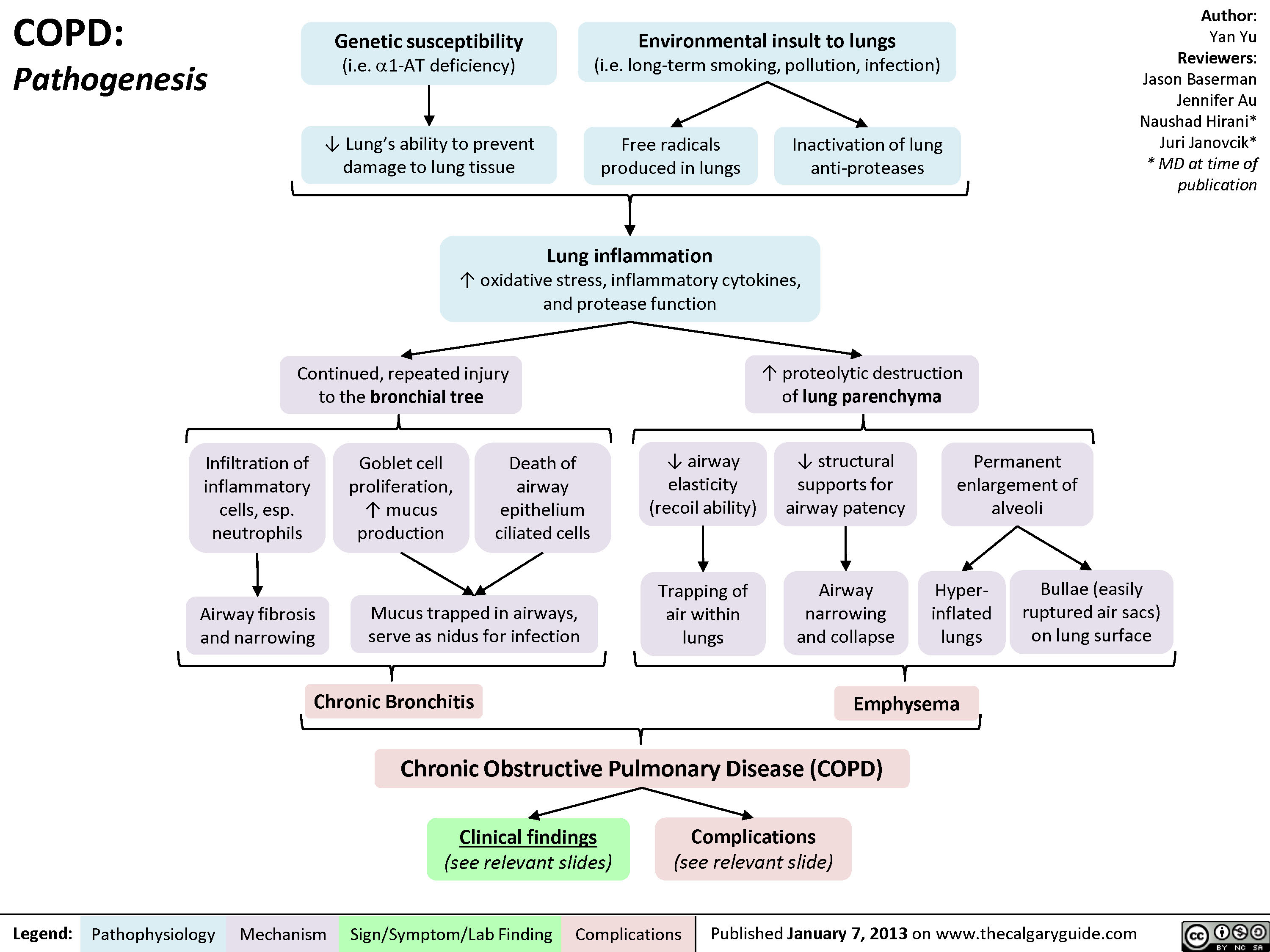
COPD: Pathogenesis
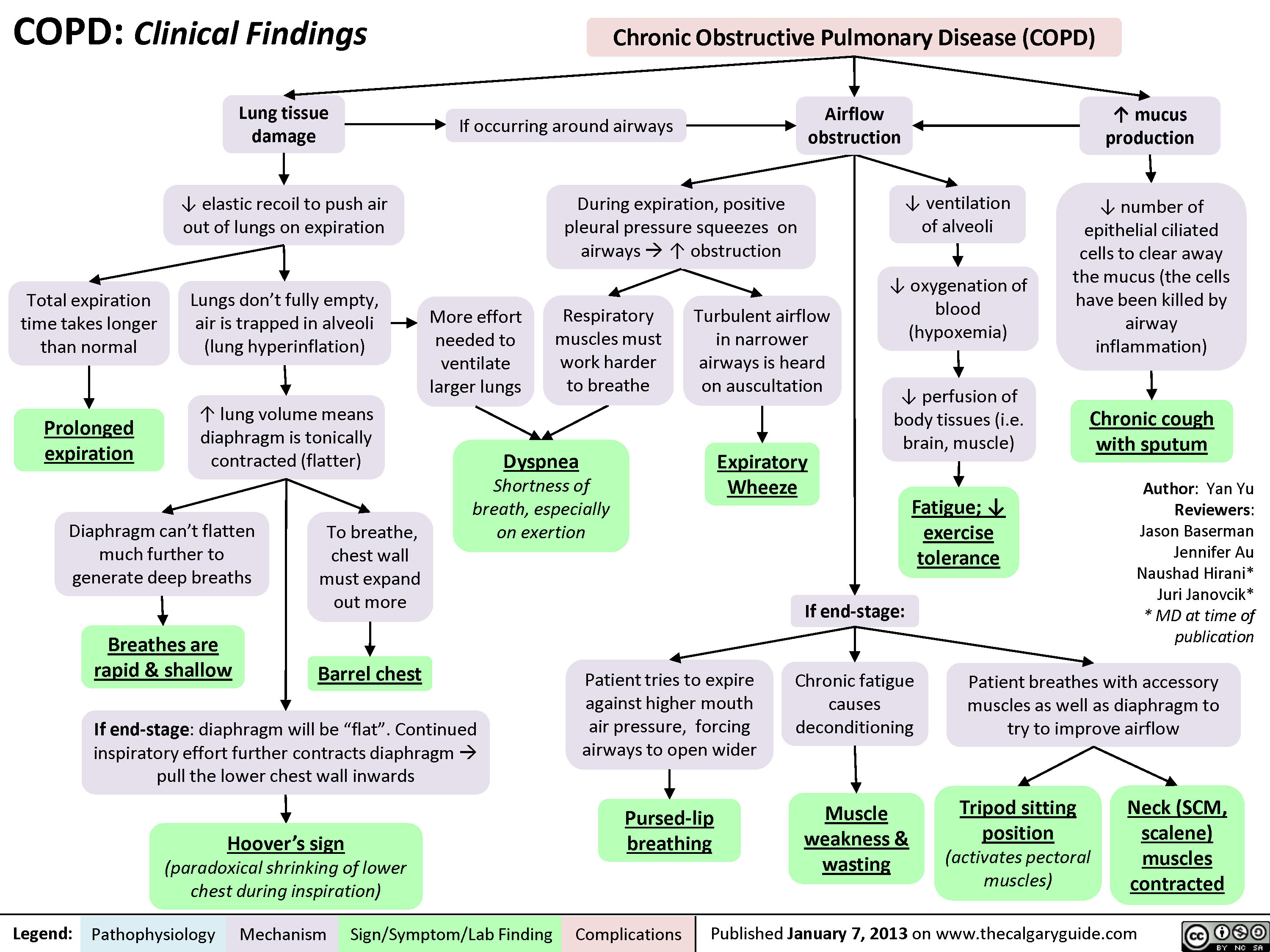
COPD: Clinical Findings
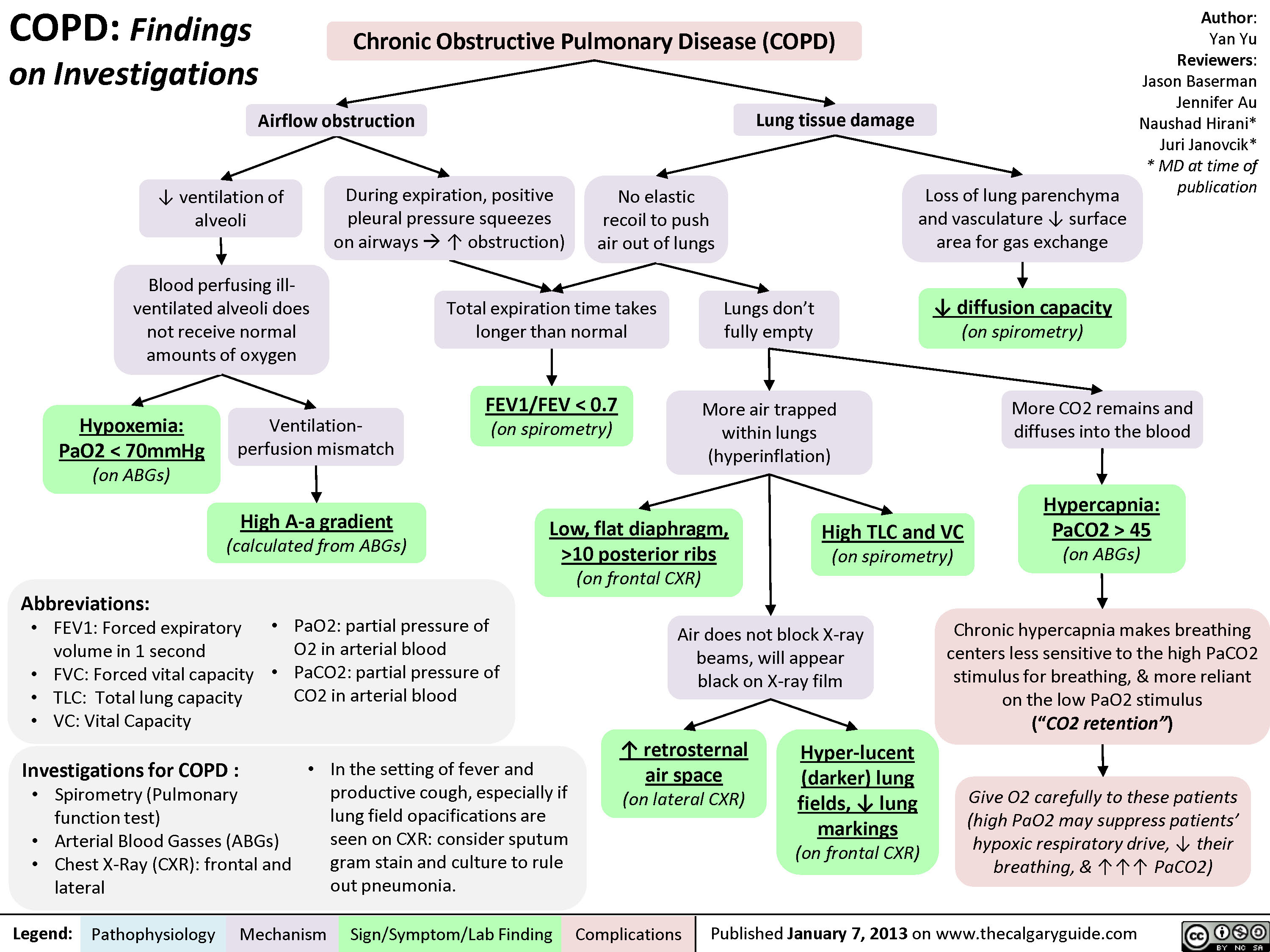
COPD: Findings on Investigations
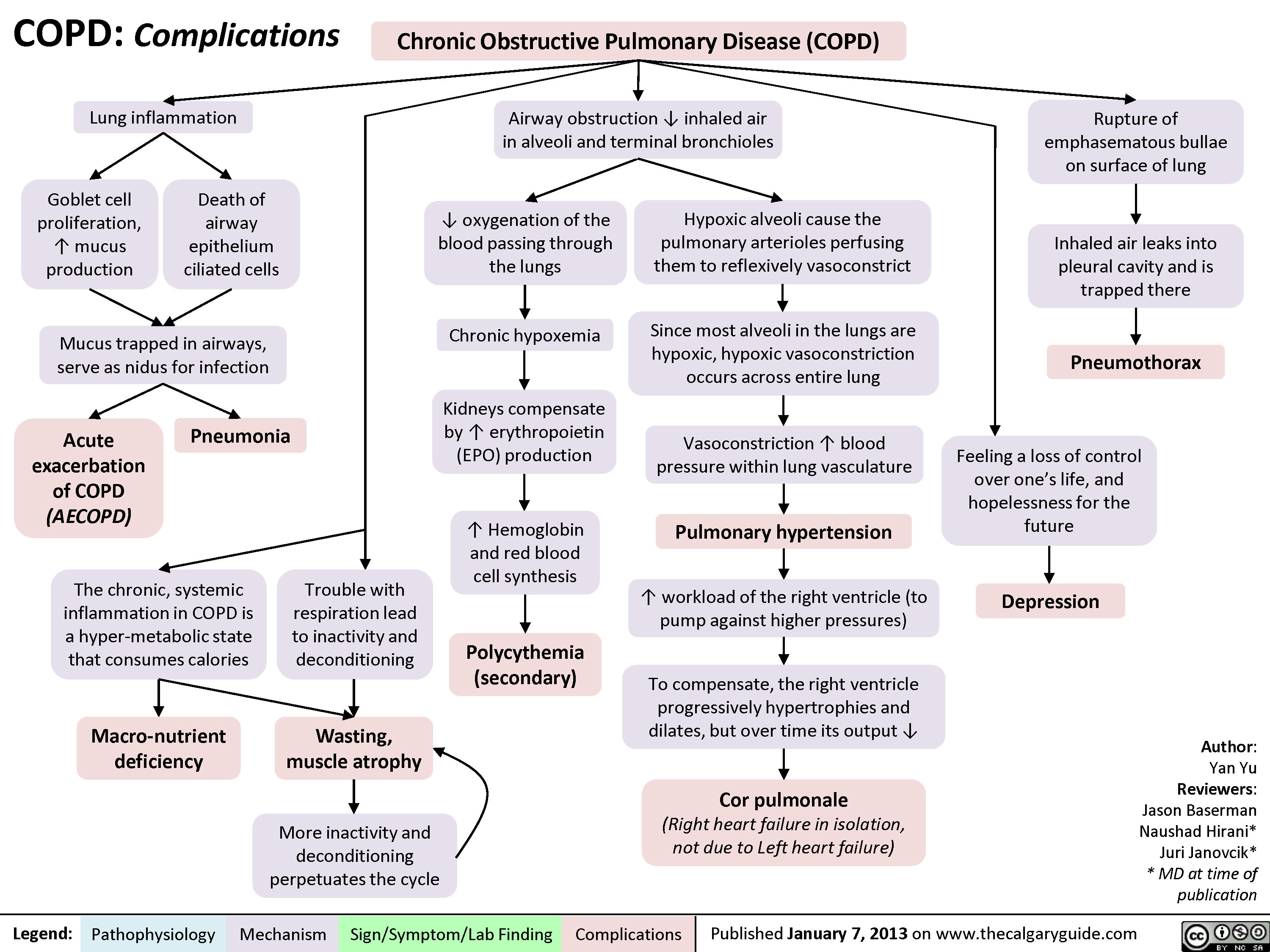
COPD: Complications
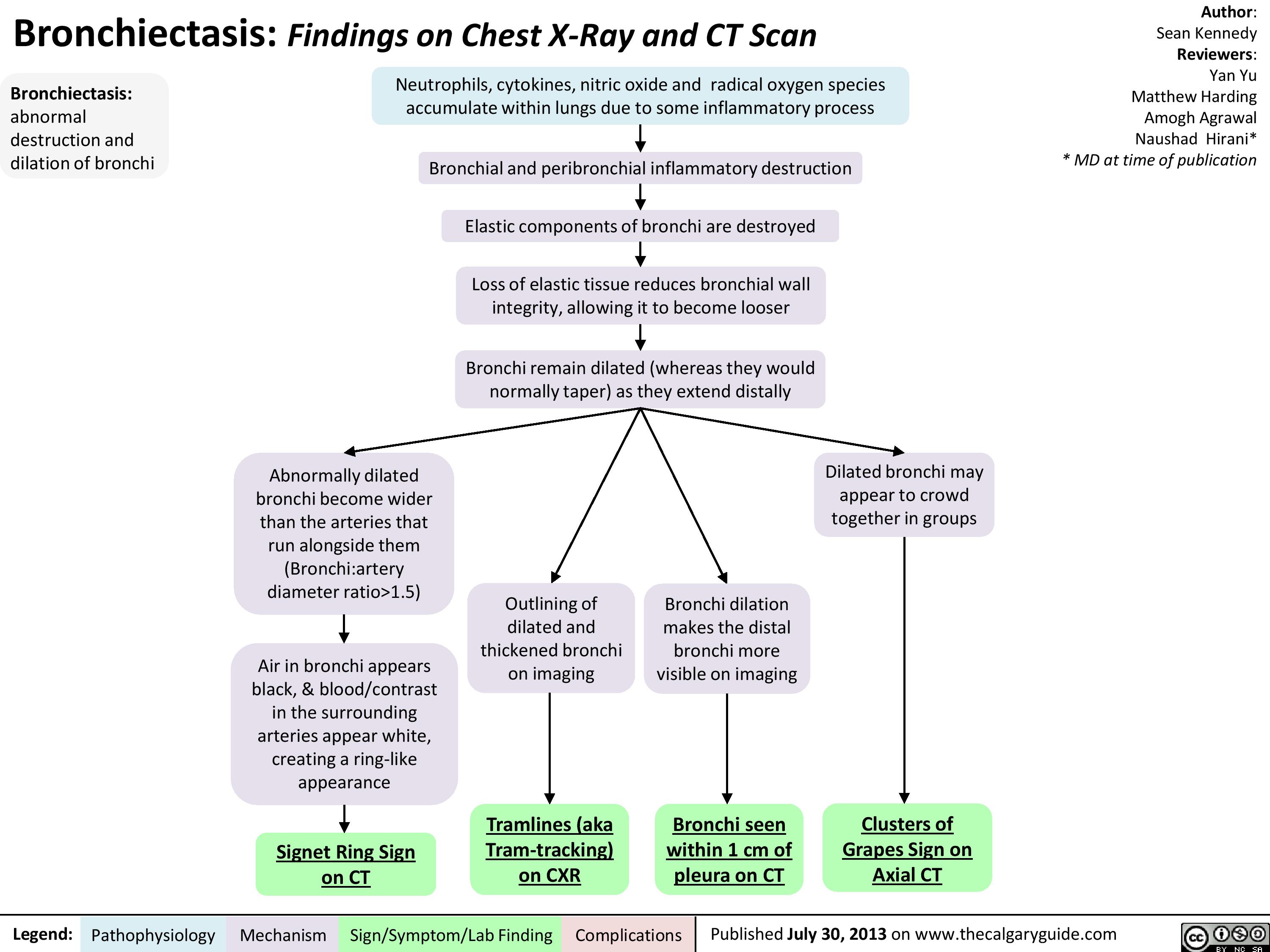
Bronchiectasis: Findings on Chest X-Ray and CT Scan
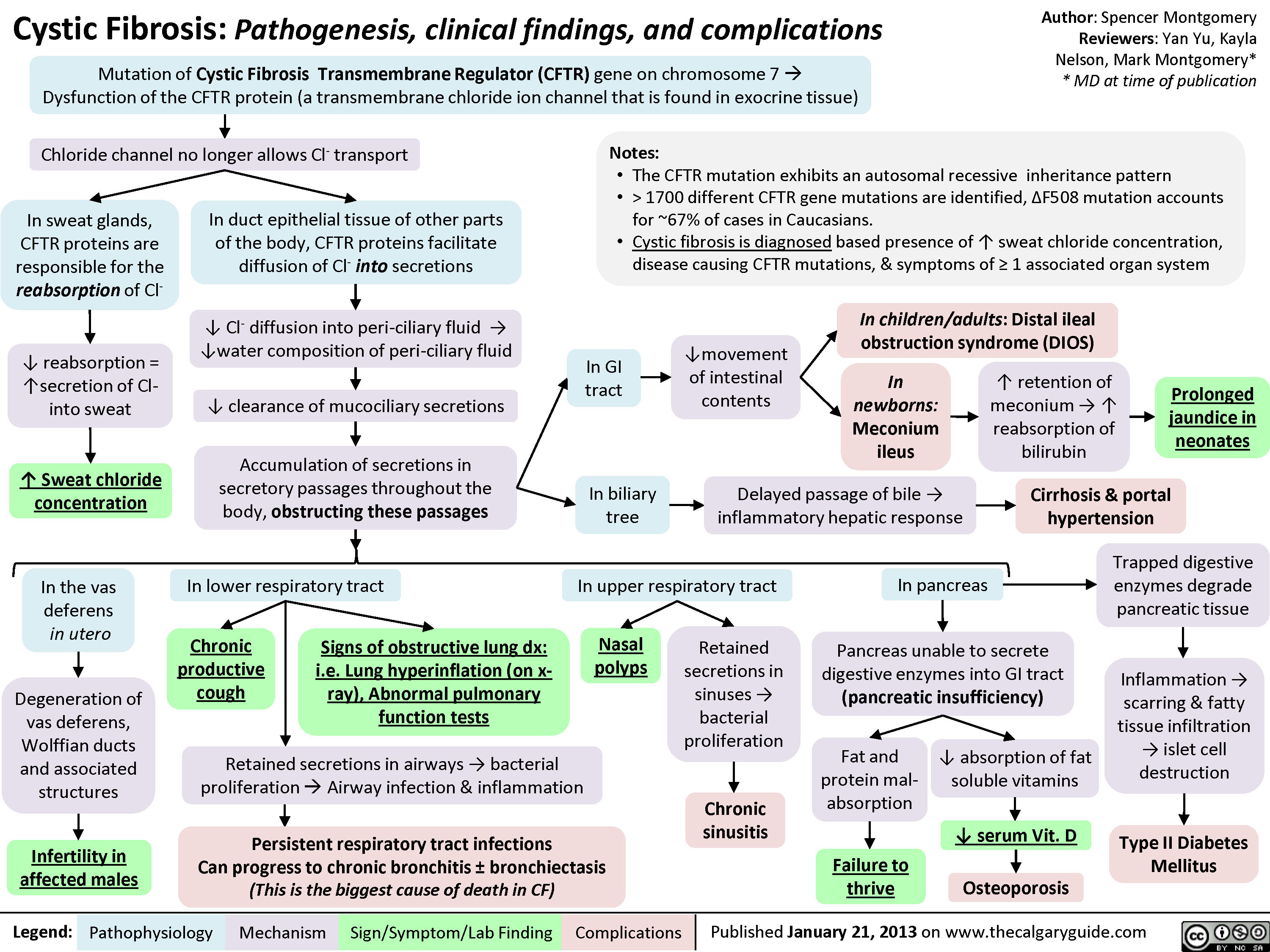
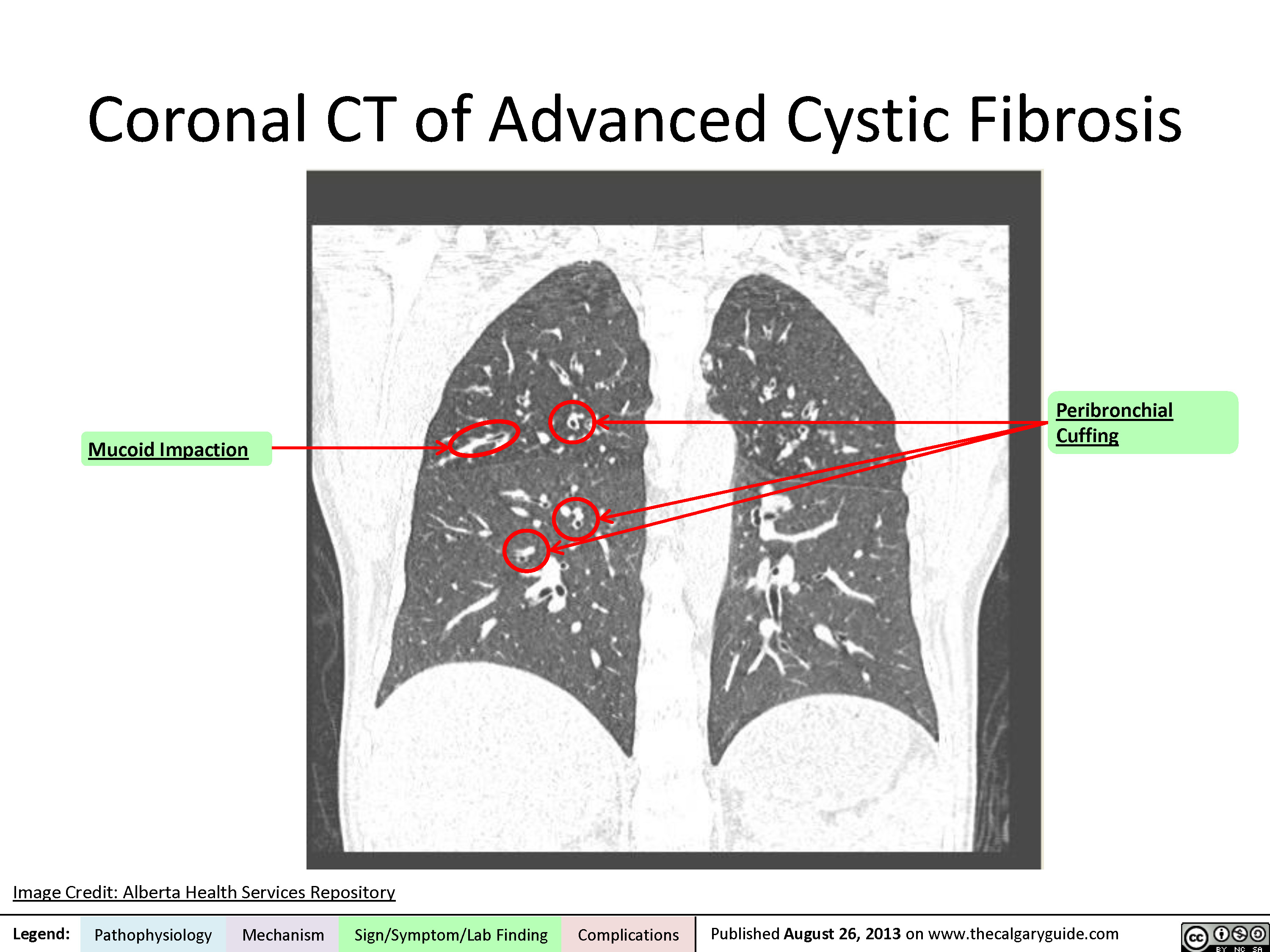
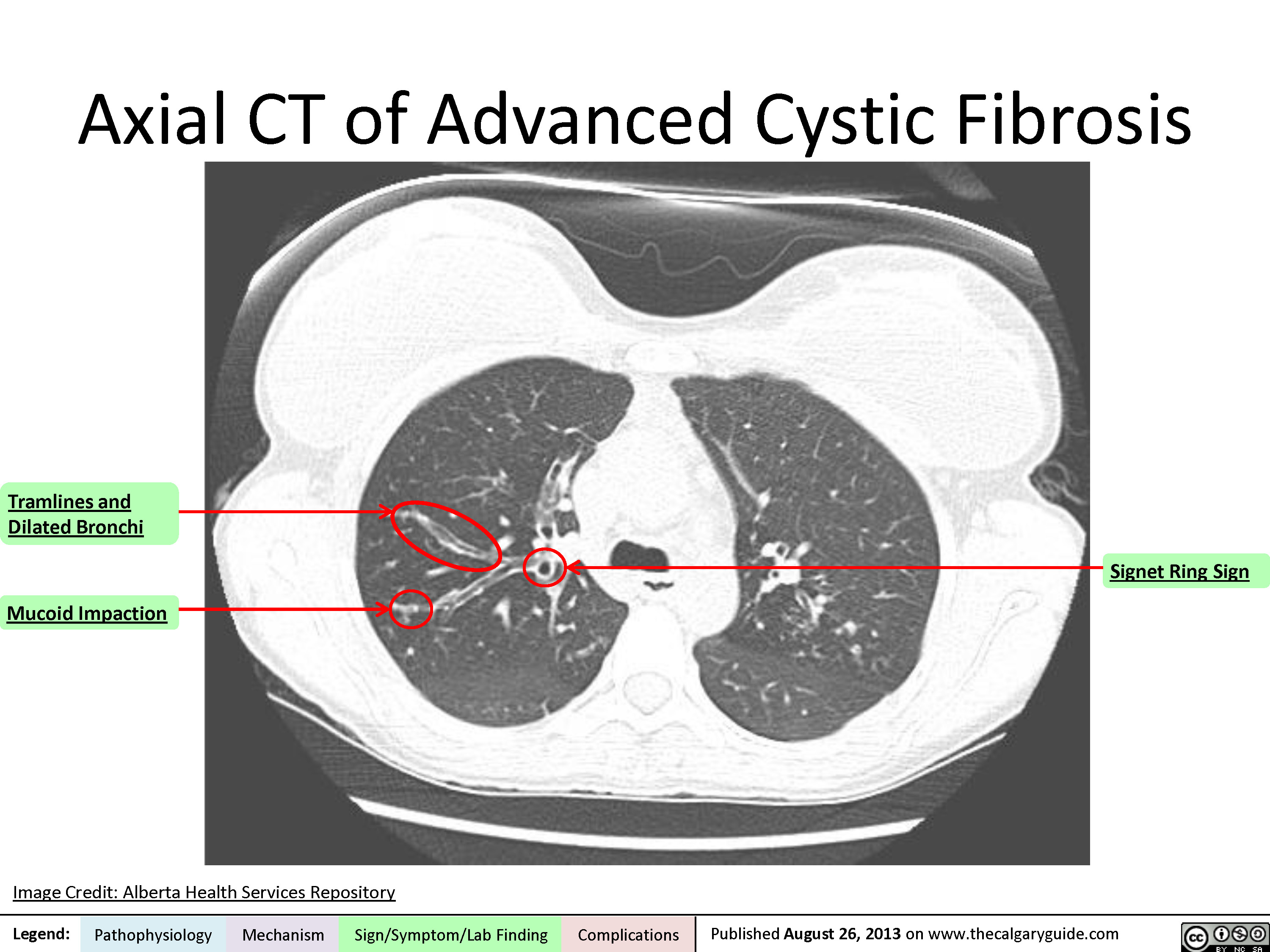
Cystic Fibrosis
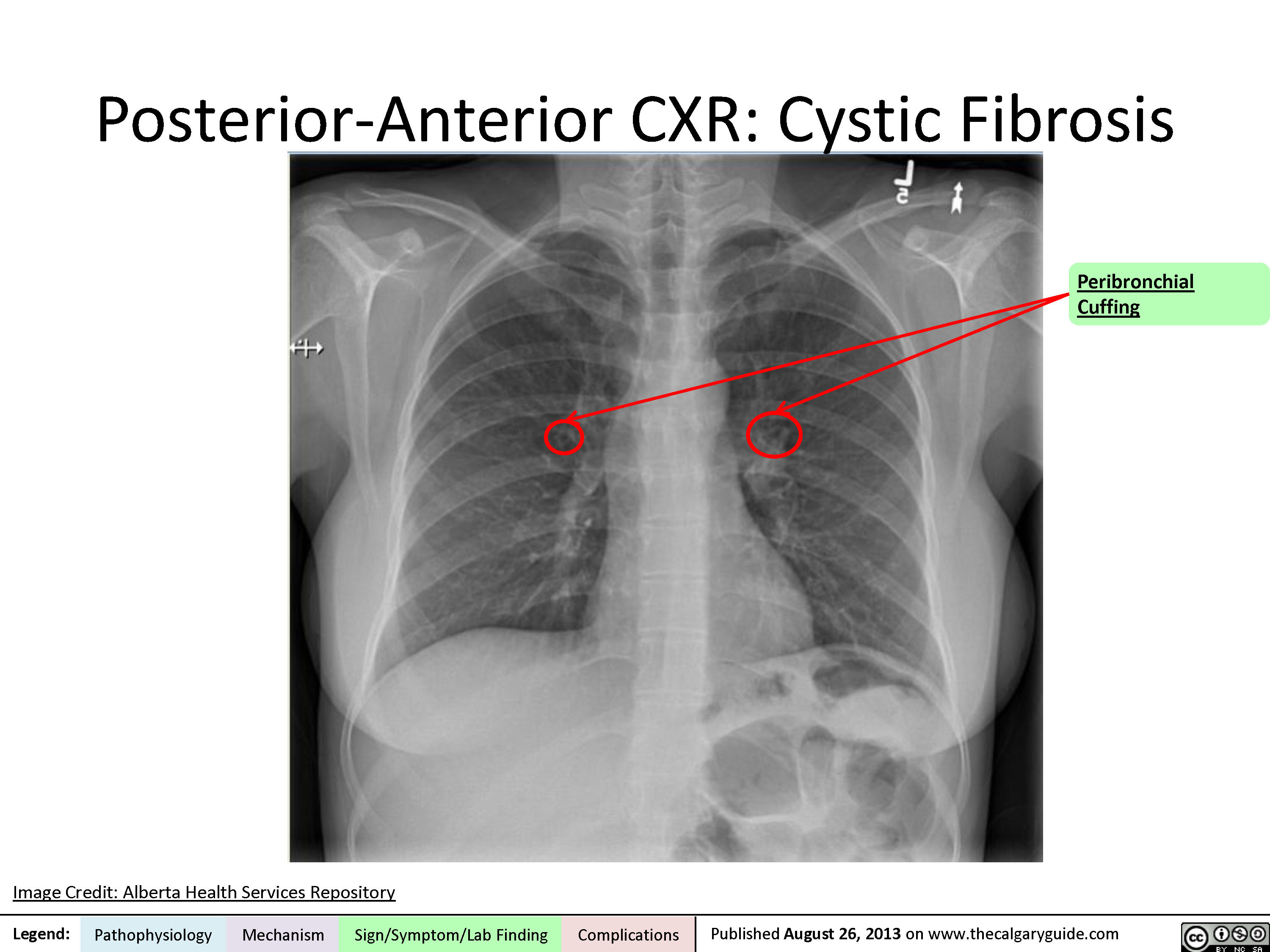
Posterior-Anterior Chest X-Ray
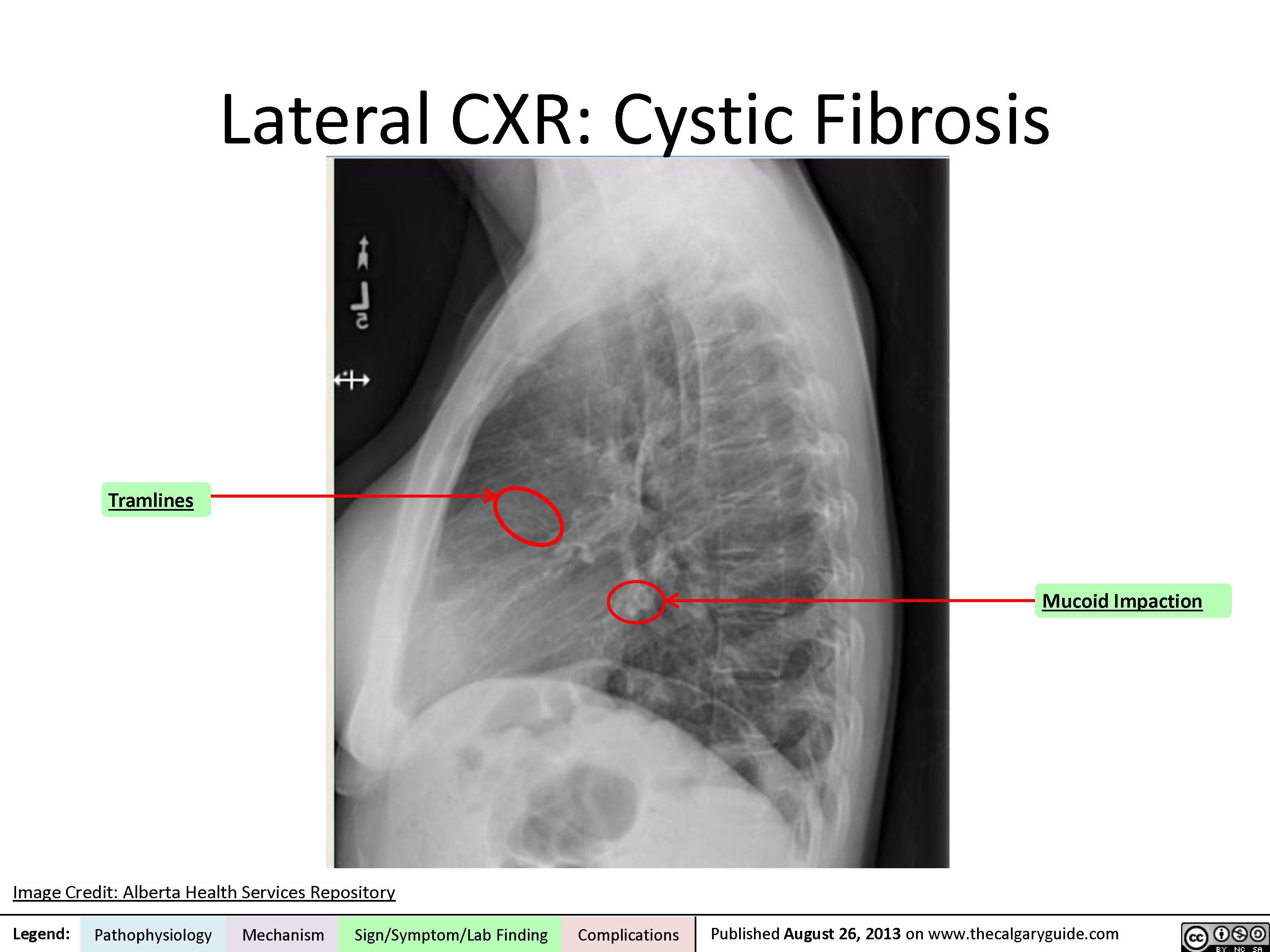
Lateral Chest X-Ray
Coronal CT
Axial CT
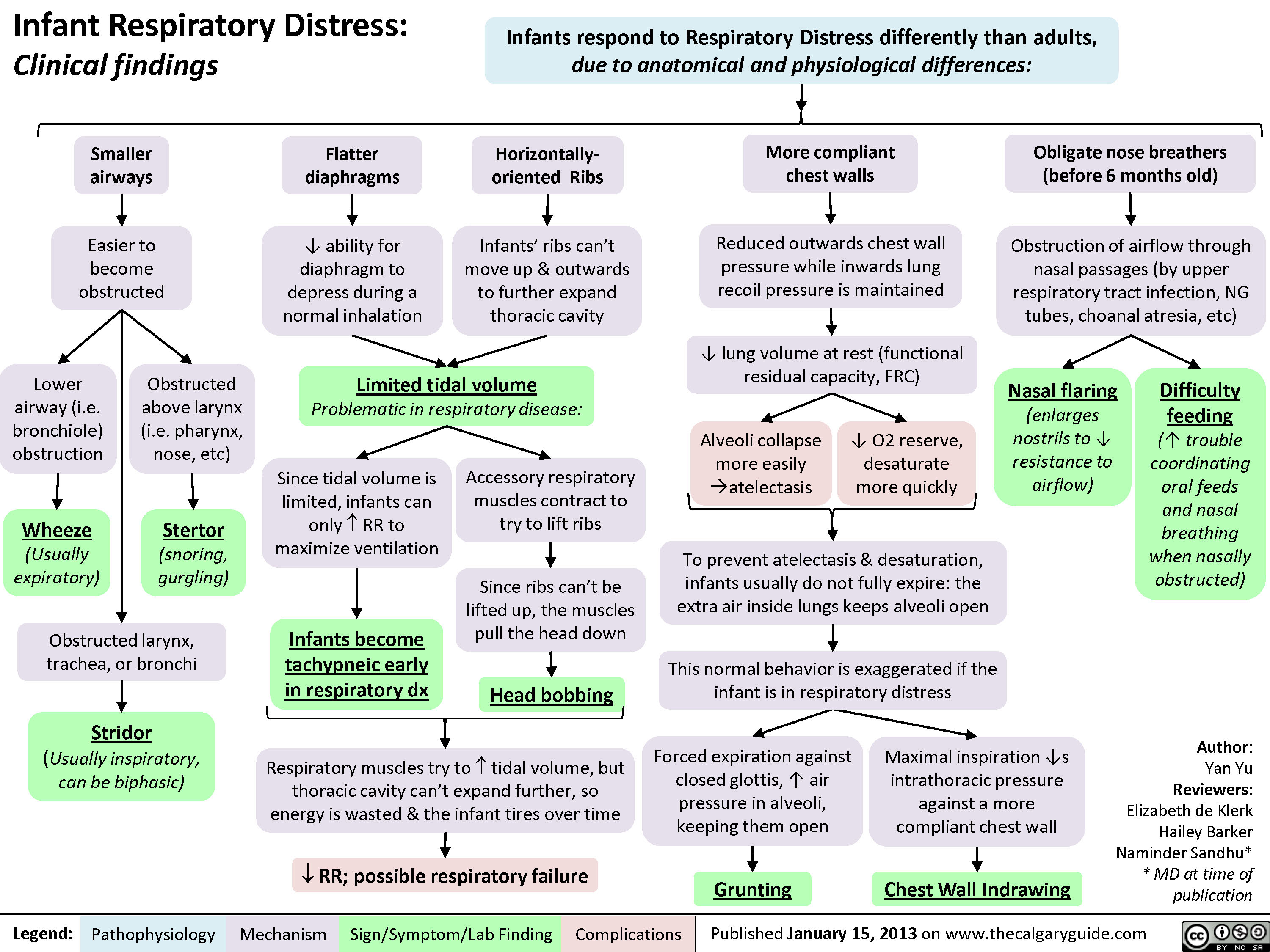
Infant Respiratory Distress: Clinical findings
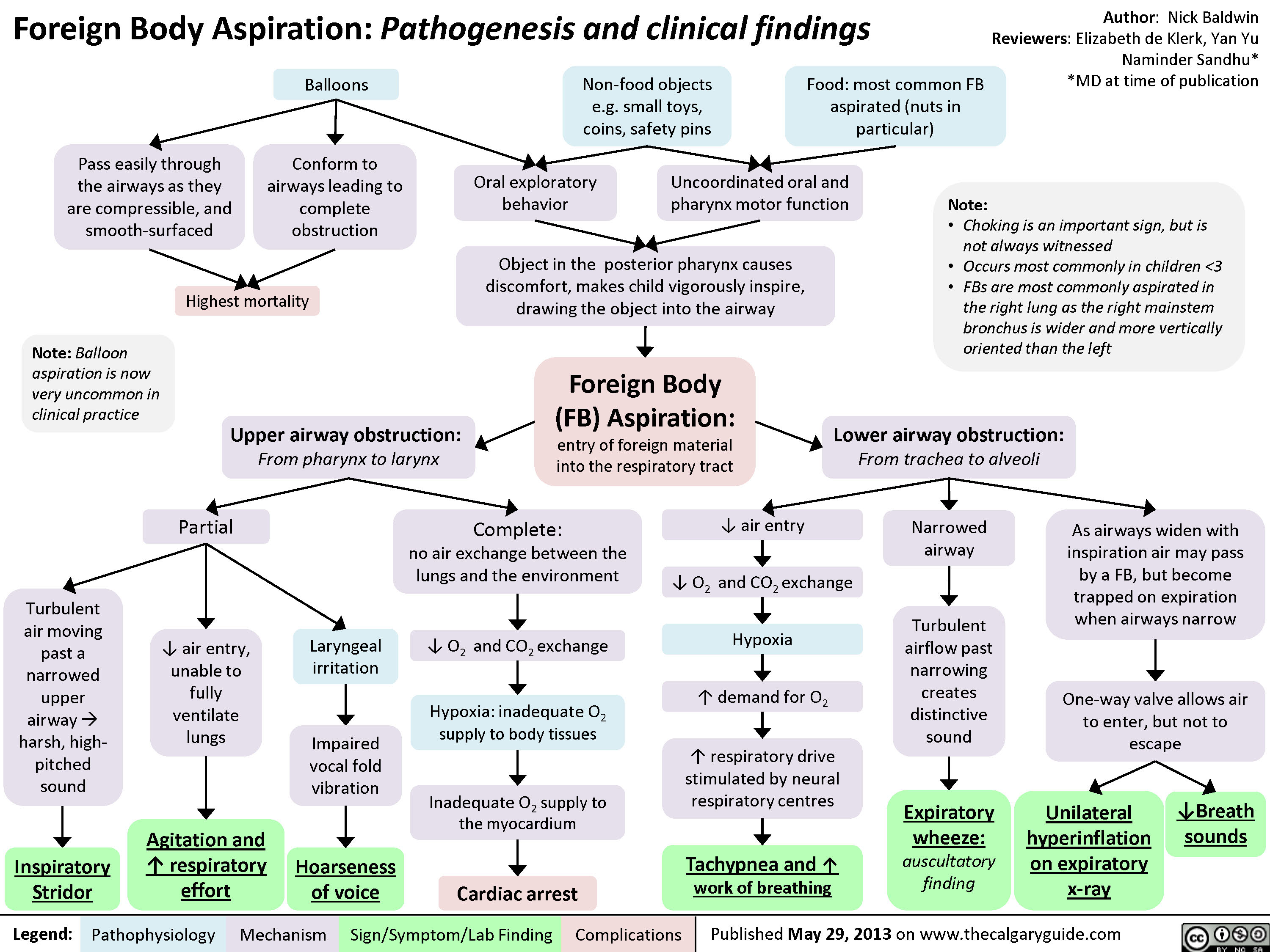
Foreign Body Aspiration
Types of Burns - Summary of Causes and Clinical Findings

Deep Partial Thickness Burns: Pathogenesis and Clinical Findings

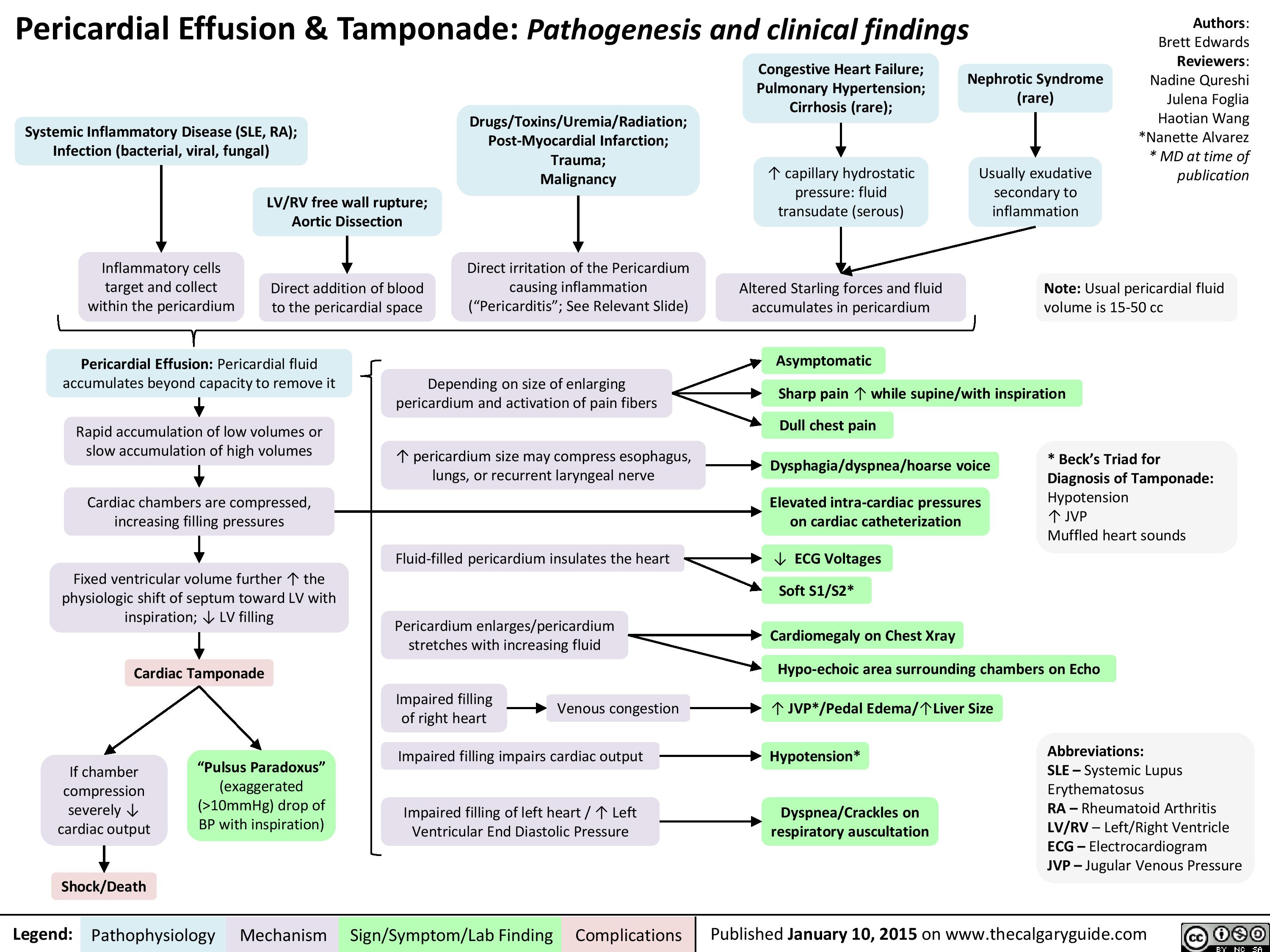
Pericardial Effusion and Tamponade: Pathogenesis and Clinical Findings
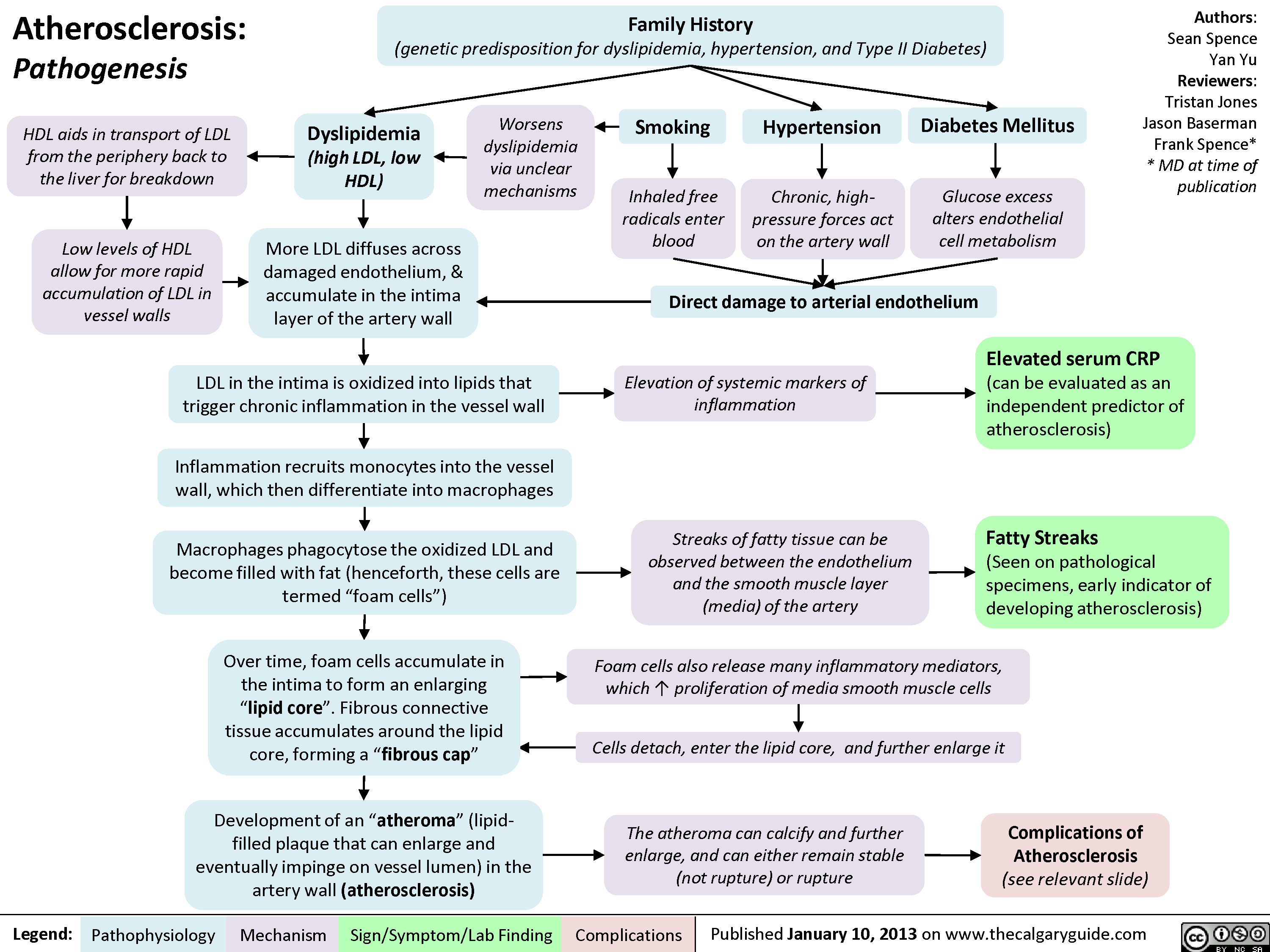
Atherosclerosis - Pathogenesis
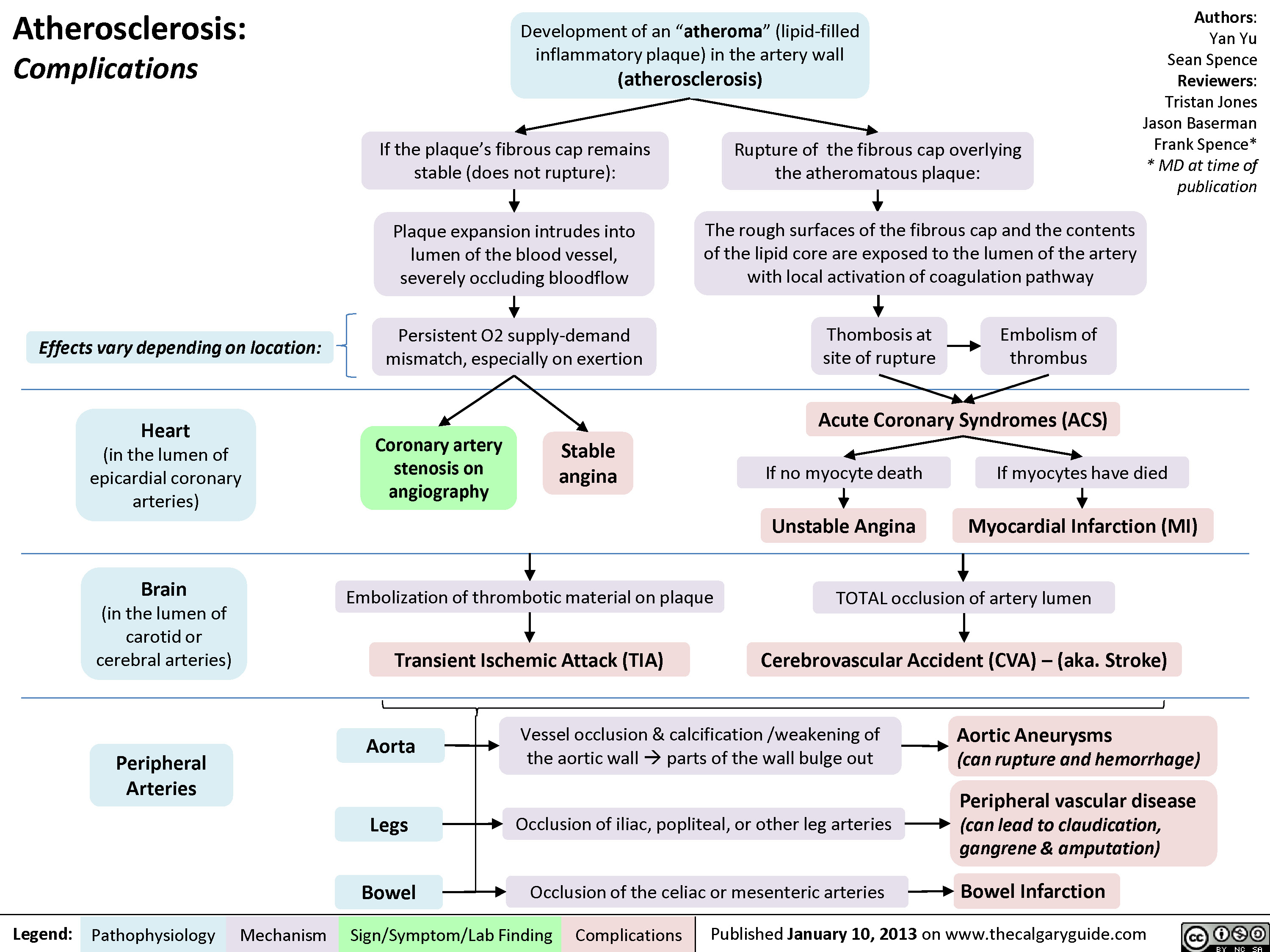
Atherosclerosis - Complications
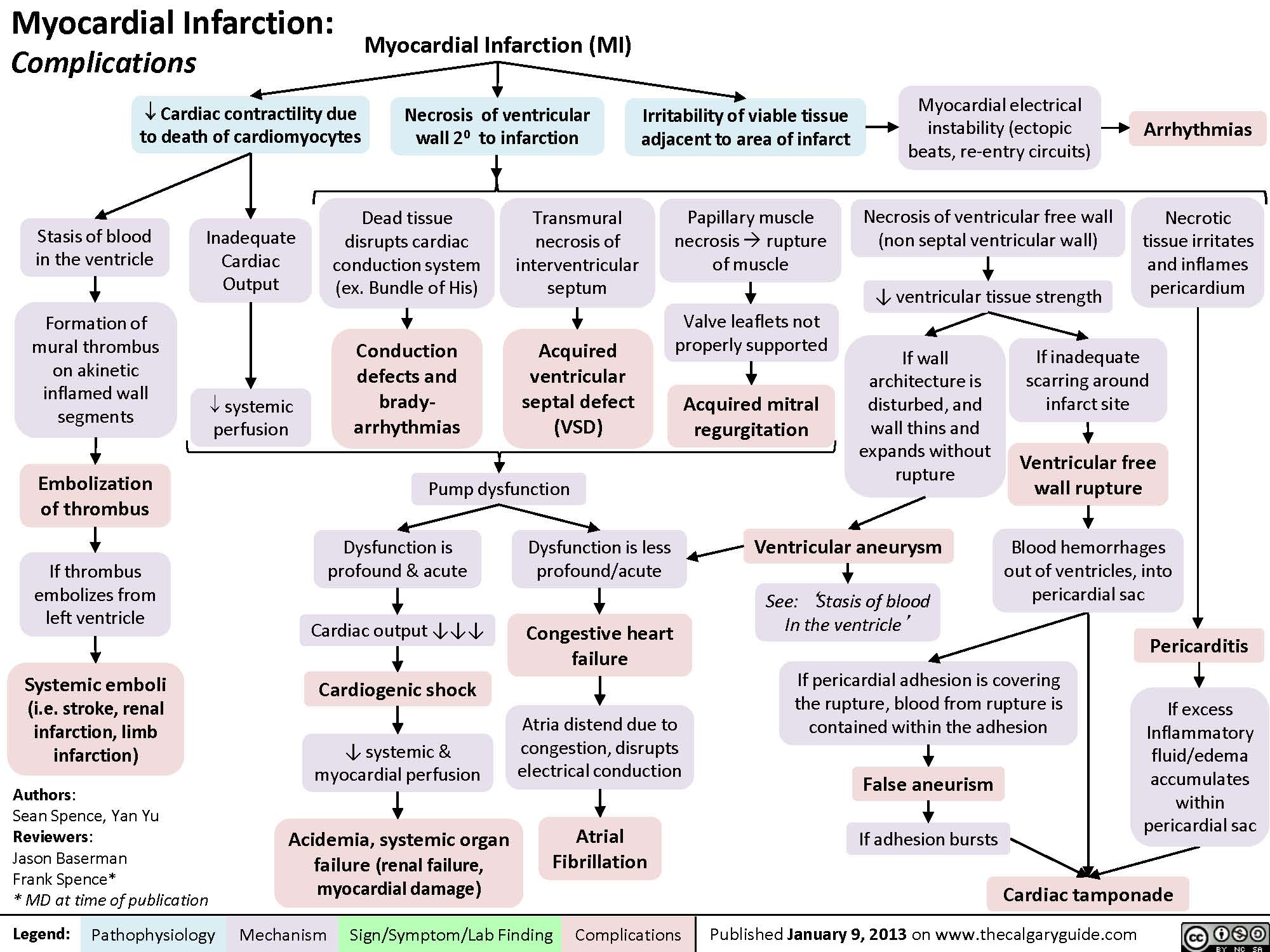
Complications of Myocardial Infarction
myocardial-infarction-findings-on-investigations
Acute, trans-mural myocardial ischemiaIschemia of sub-endocardial myocardiumMyocardial infarctionNote: Both types of ST-segment changes are non-specific: they can indicate Myocardial Infarctions , but can also be false positives (i.e. caused by left ventricular hypertrophy, bundle branch blocks, and other non-myocardial ischemic causes)If ischemia progresses to tissue infarctionPathologic Q-waves (localizes to site of ischemia)Tissue necrosis ? Local myocardial inflammation2-4 hours after MI: troponin proteins released into blood3-8 hours after MI:Creatinine-kinase MB-isozymes released into blood? serum Cardiac Troponins: cTnT, cTnI(Sensitive and most specific serum marker for myocardial necrosis)Relatively faster clearance from circulation? serum CK-MB(less sensitive and specific for myocardial necrosis than Troponins)ST-segment depression(non-localizing)Inflammatory cytokines can spread systemicallyStimulation of neutrophil and monocyte migration towards area of inflammation? WBC count (on CBC)? C-Reactive Protein (CRP)Dead, damaged cardiac myocytes release inner contents into the bloodRelatively slower clearance from circulationSerum CK-MB levels normalize within 3 daysSerum Troponin levels normalize within 14 daysNote: Measuring both CK-MB and Troponins gives a timeline to the MI. For instance, if CK-MB is normal but Troponins are high, it means the MI happened >3 days but <14 days ago.ST-segment elevation(localizes to site of ischemia)Legend:Published January 30, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplications
104 kB / 212 words")
myocardial-infarction-findings-on-physical-exam
 Diastolic compliance (necrotic myocardium does not relax as well to accommodate blood)Necrosis of papillary muscles:S4(4th heart sound)? Force of ventricular contractionsMitral valve regurgitationBlood")
MI Findings on History
Dilated Cardiomyopathy
Myocarditis
Restrictive Cardiomyopathy
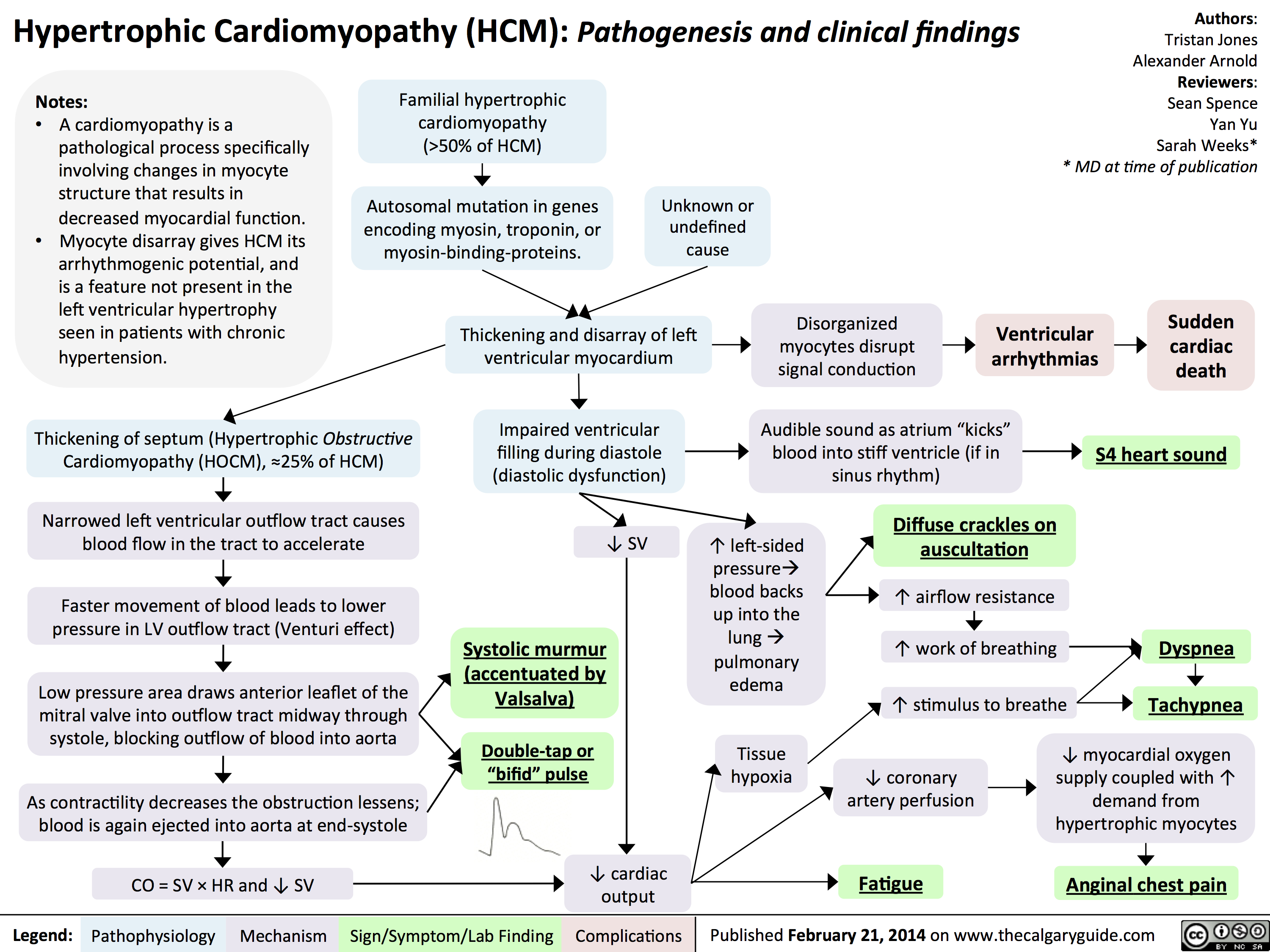
Hypertrophic Cardiomyopathy
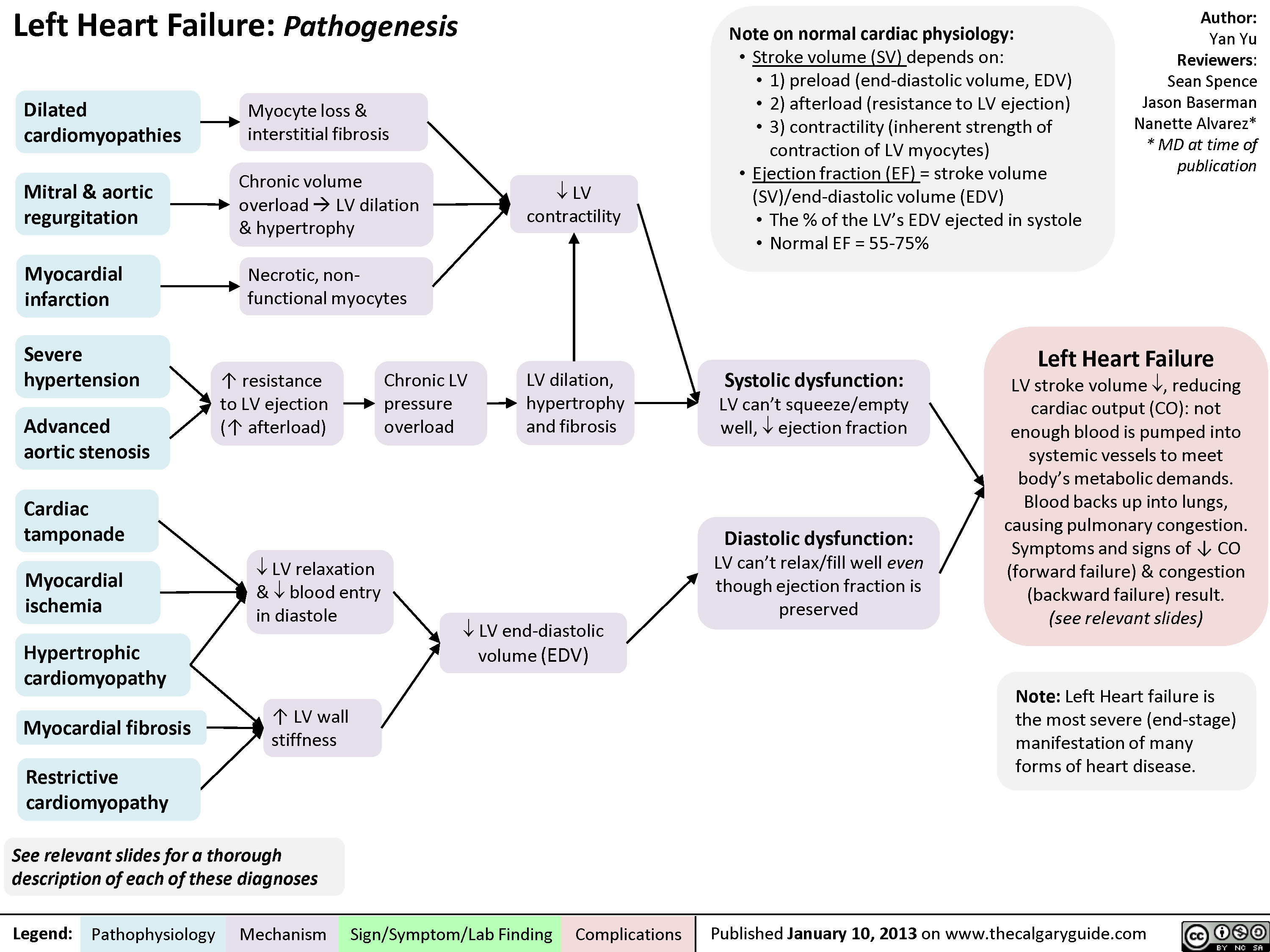
Left Heart Failure - Pathogenesis
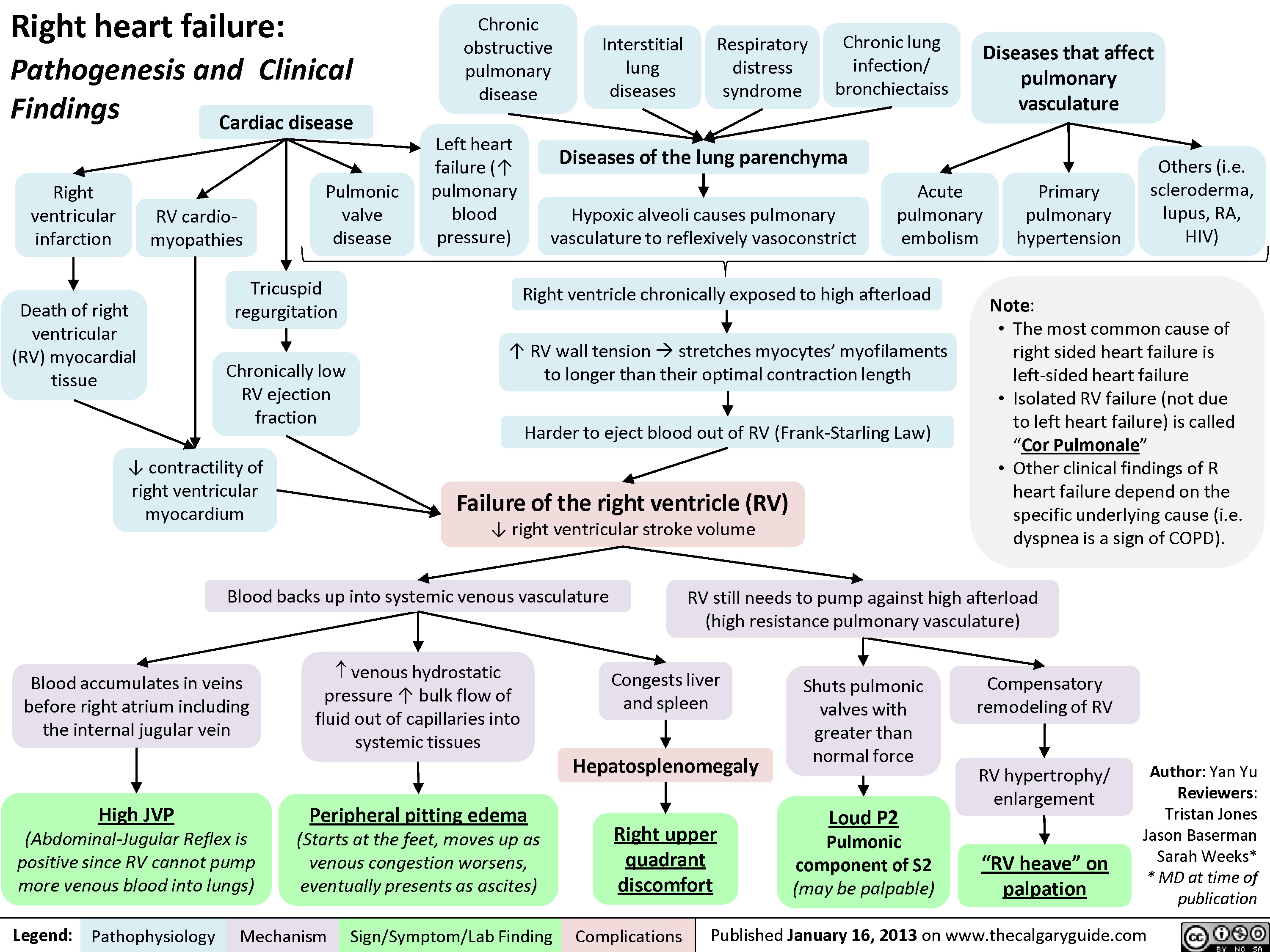
Right Heart Failure
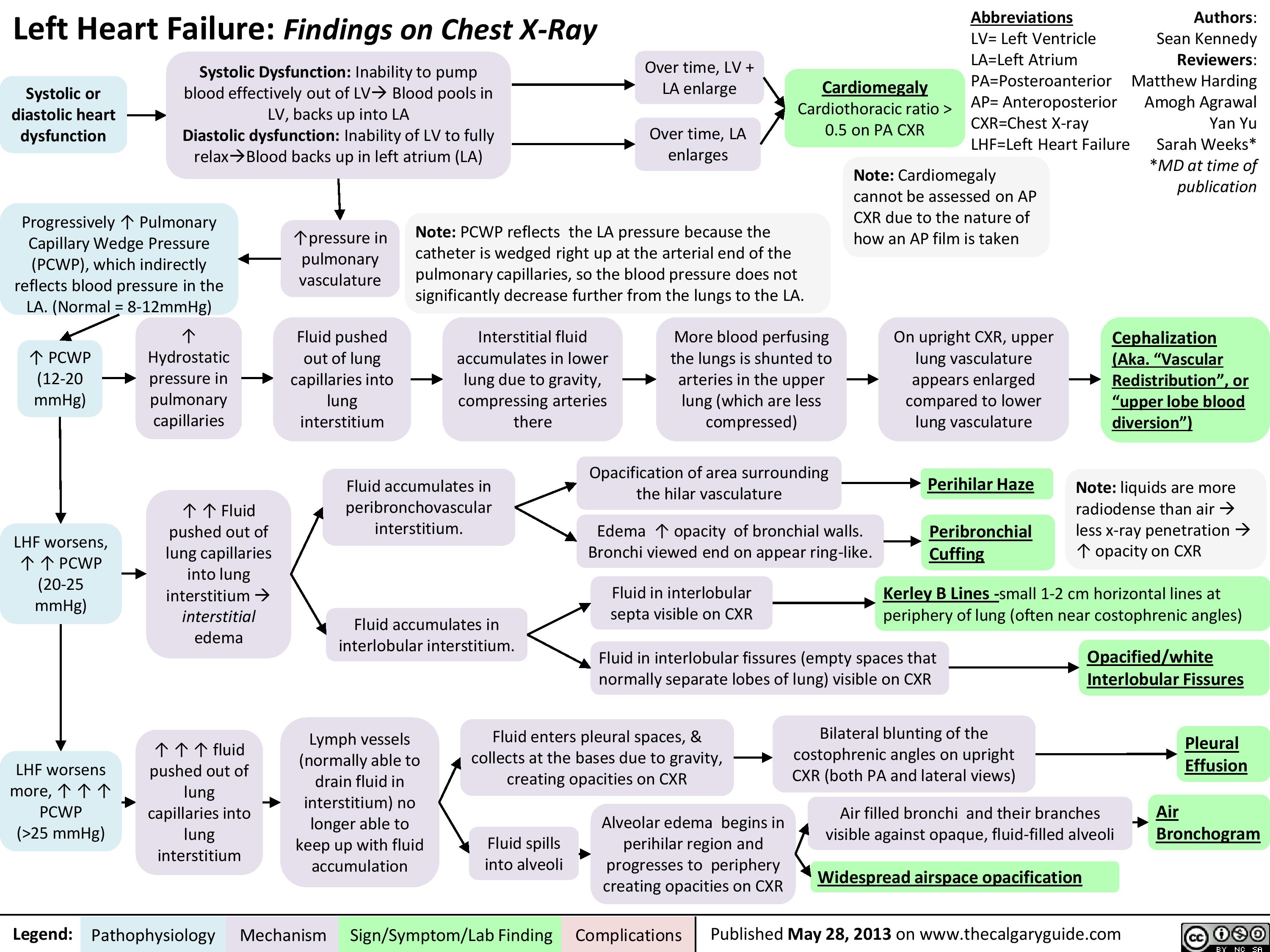
Left Heart Failure
Left Heart Failure - Physical Exam Findings
Left Heart Failure - Findings on History
pericarditis
Aortic Dissection
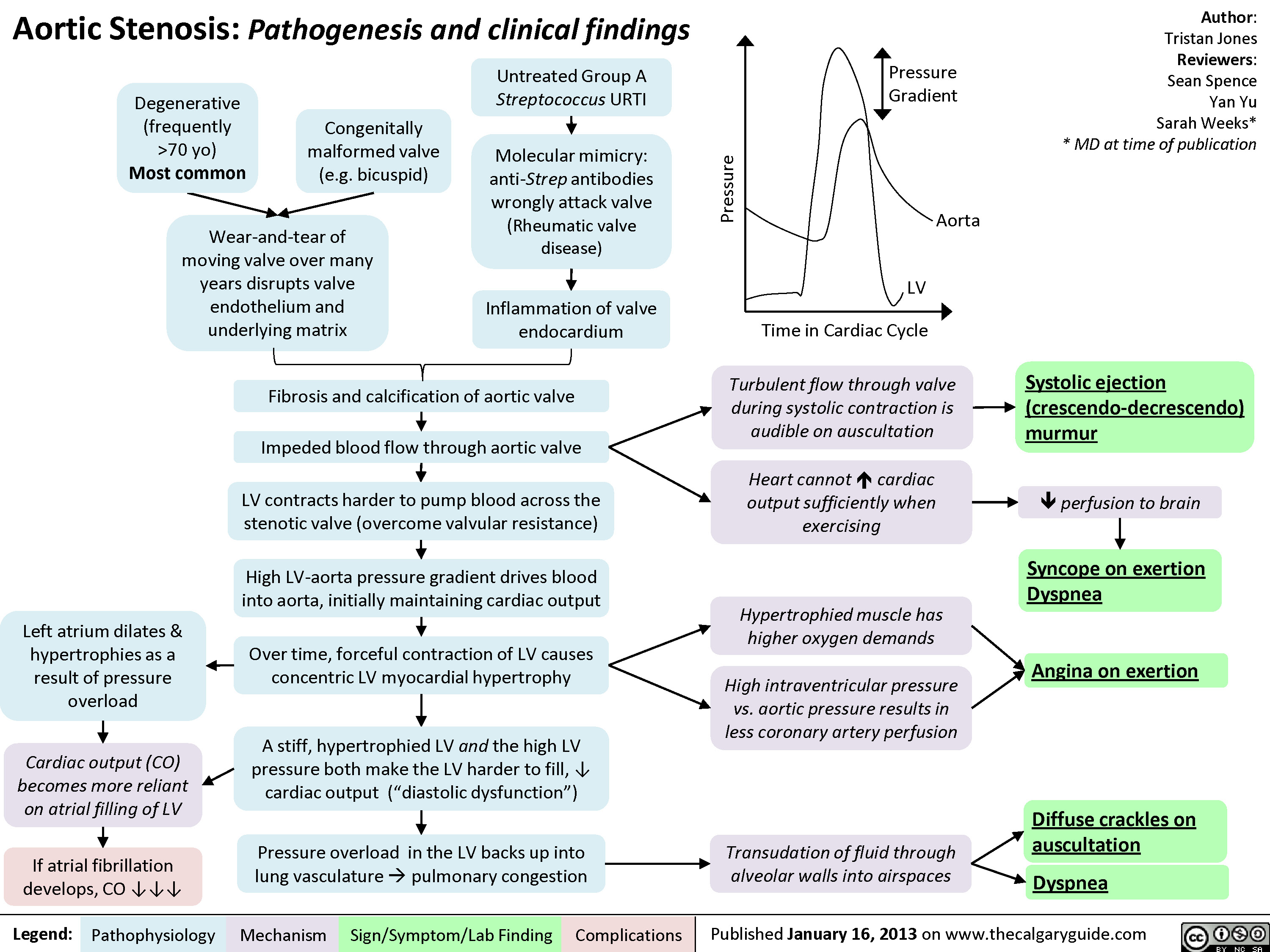
Aortic Stenosis - Pathogenesis and Clinical Findings
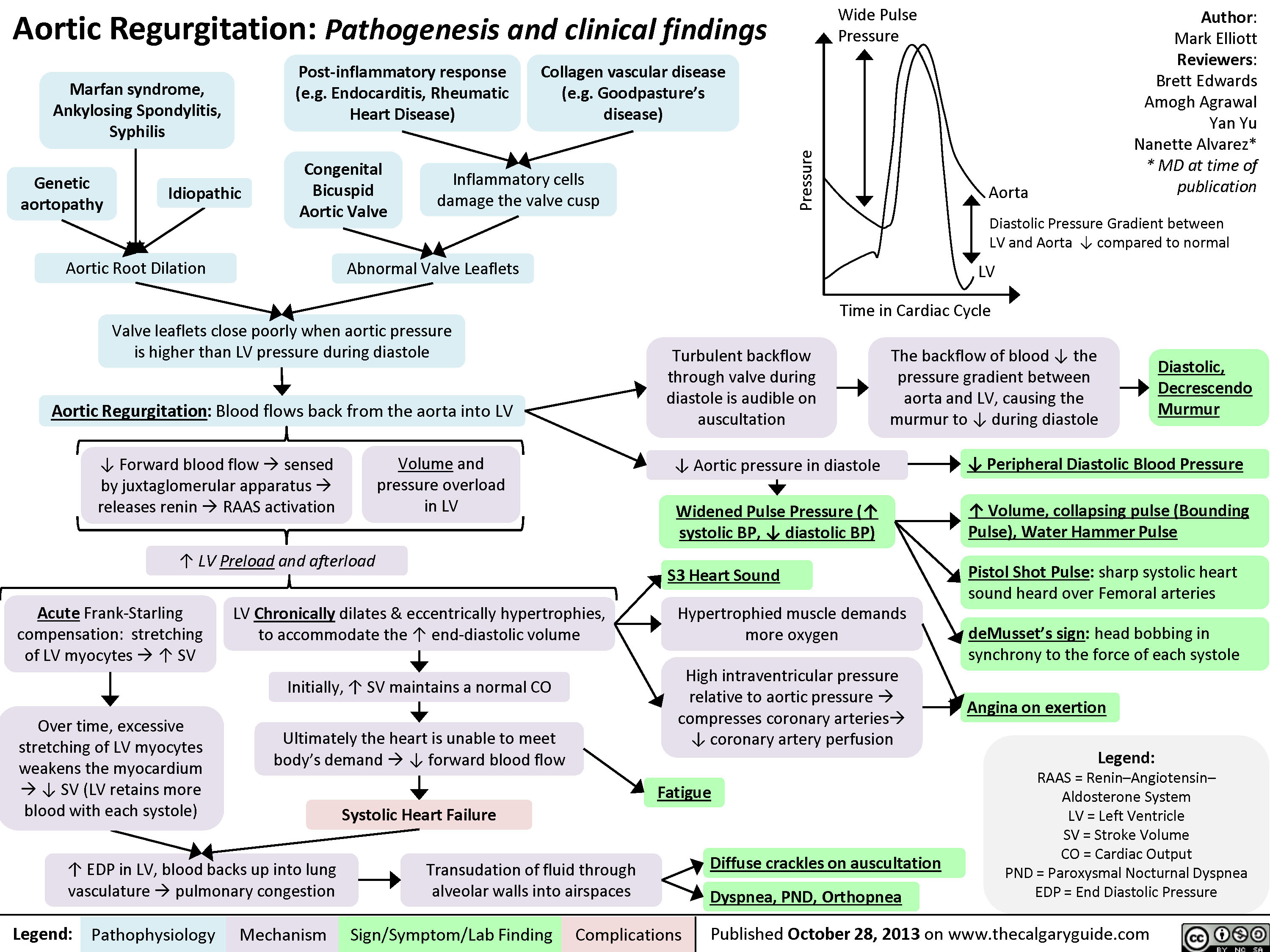
Aortic Regurgitation
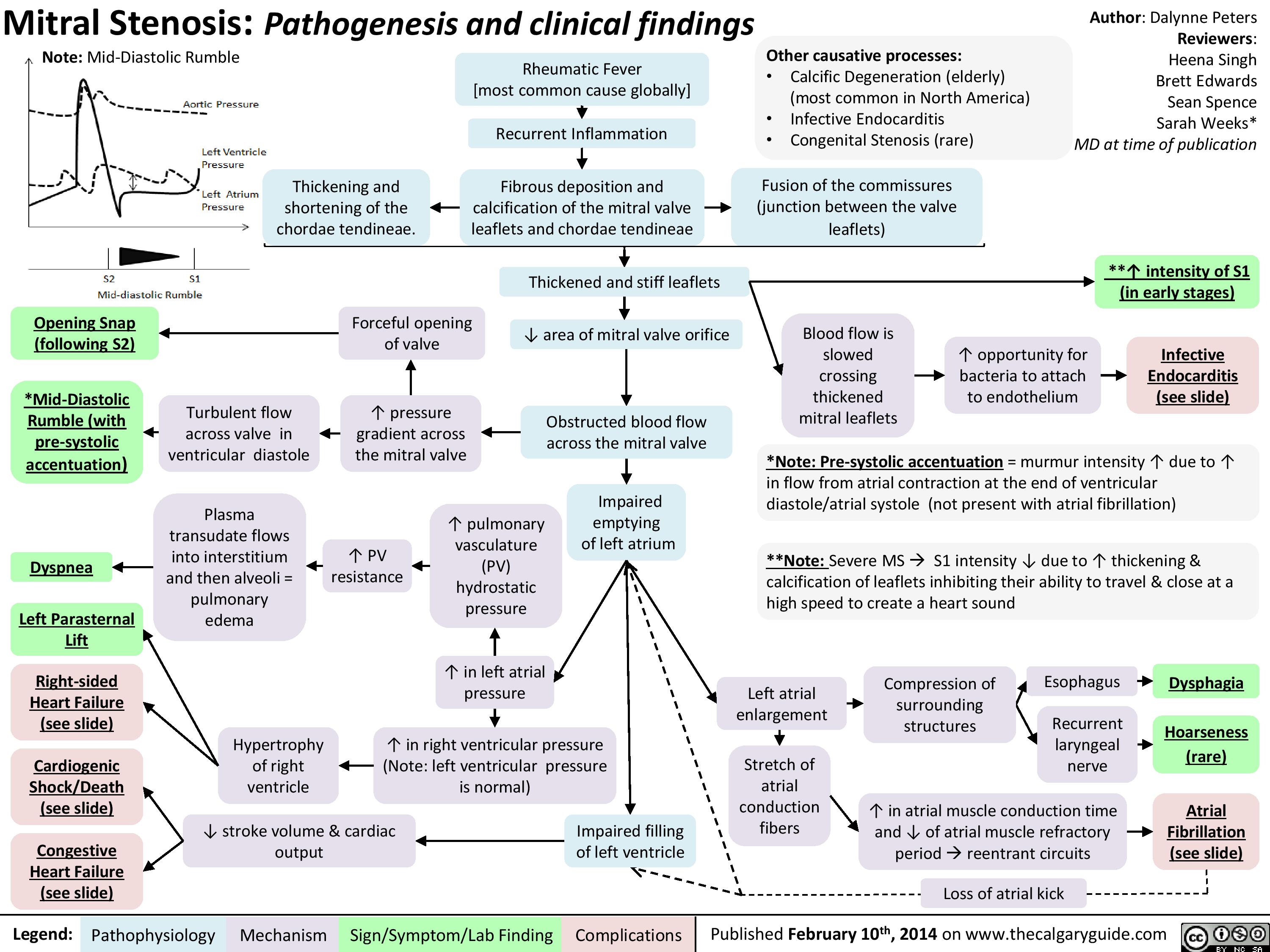
Mitral Stenosis
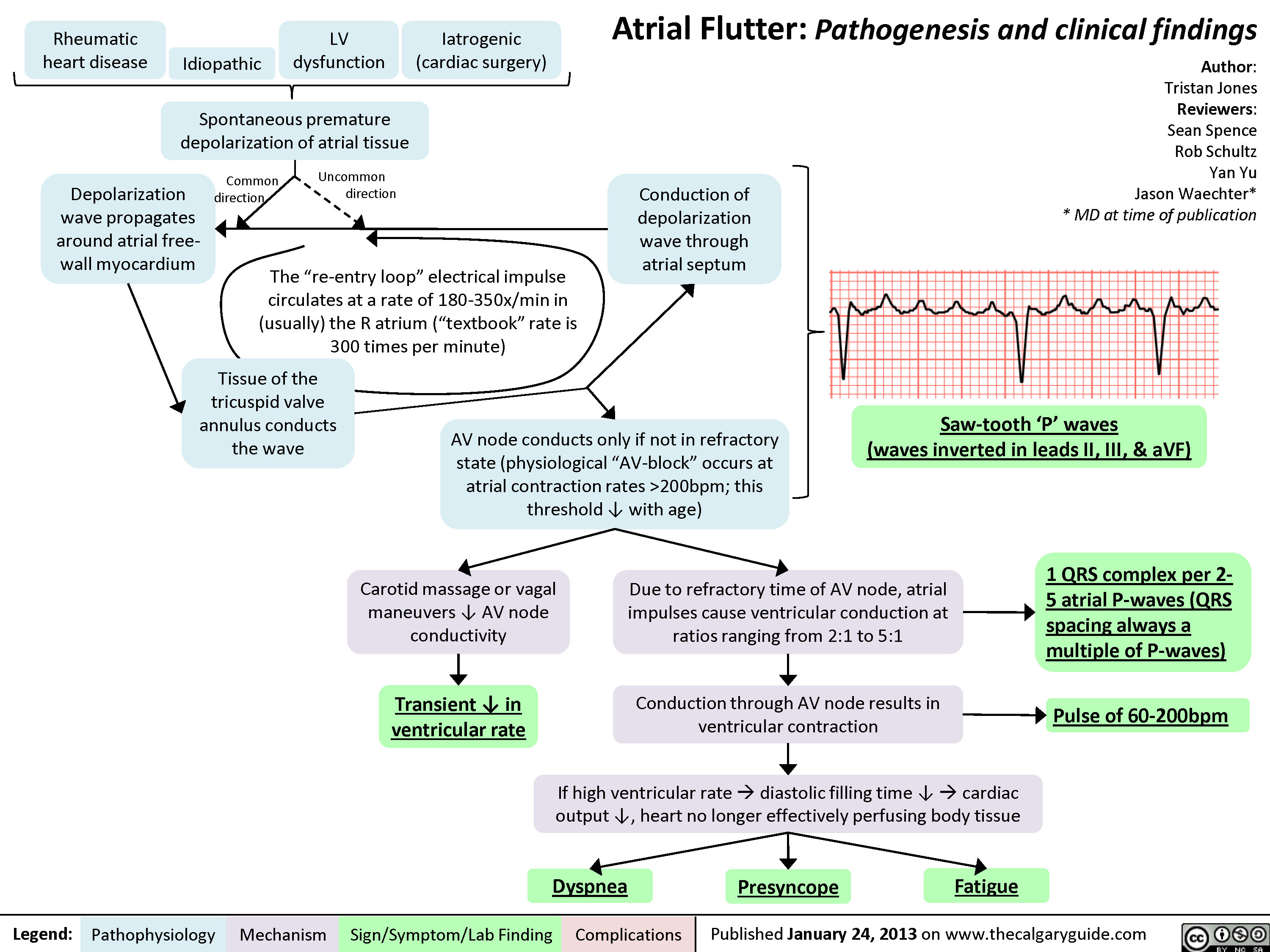
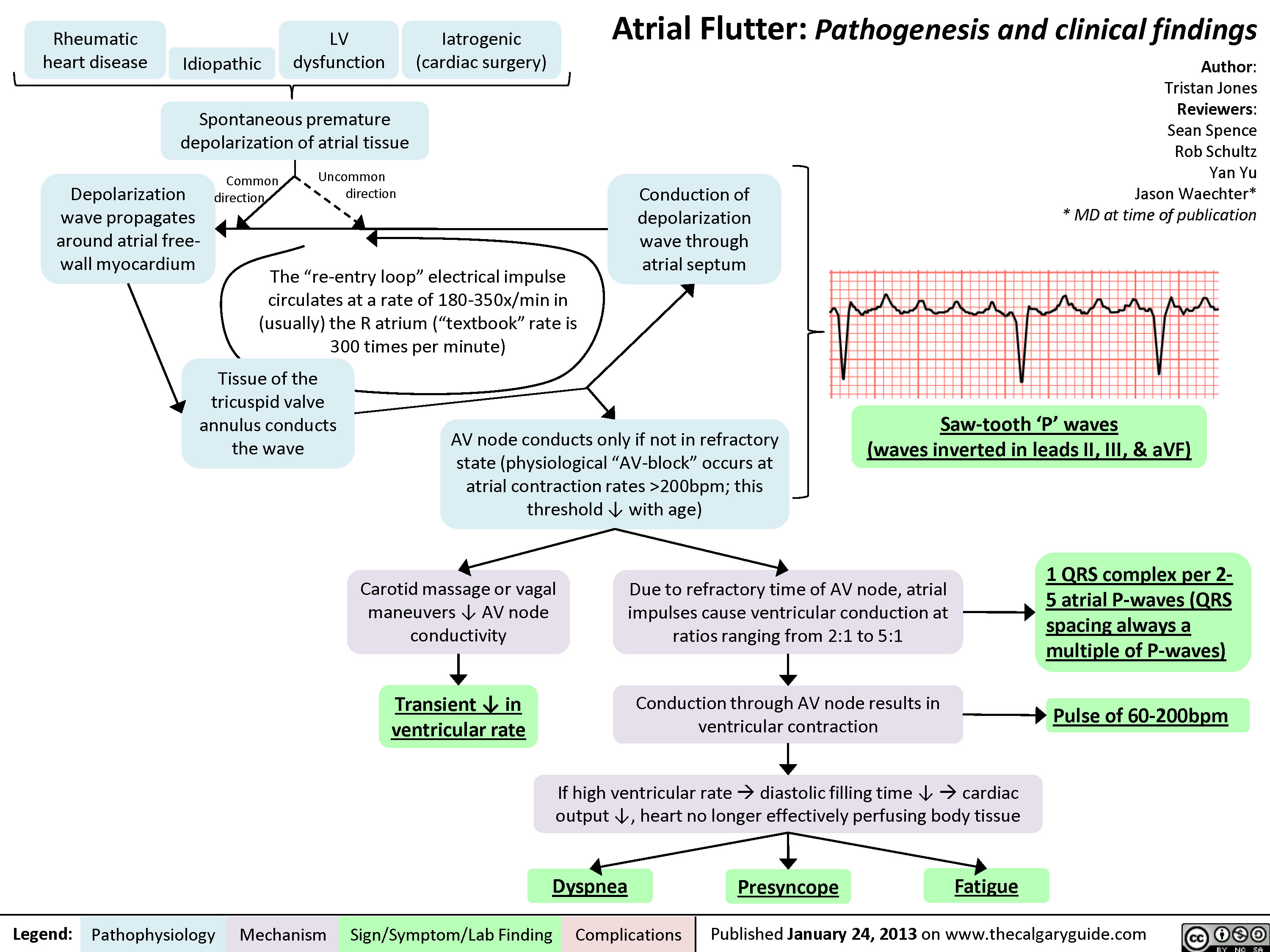
Atrial Flutter
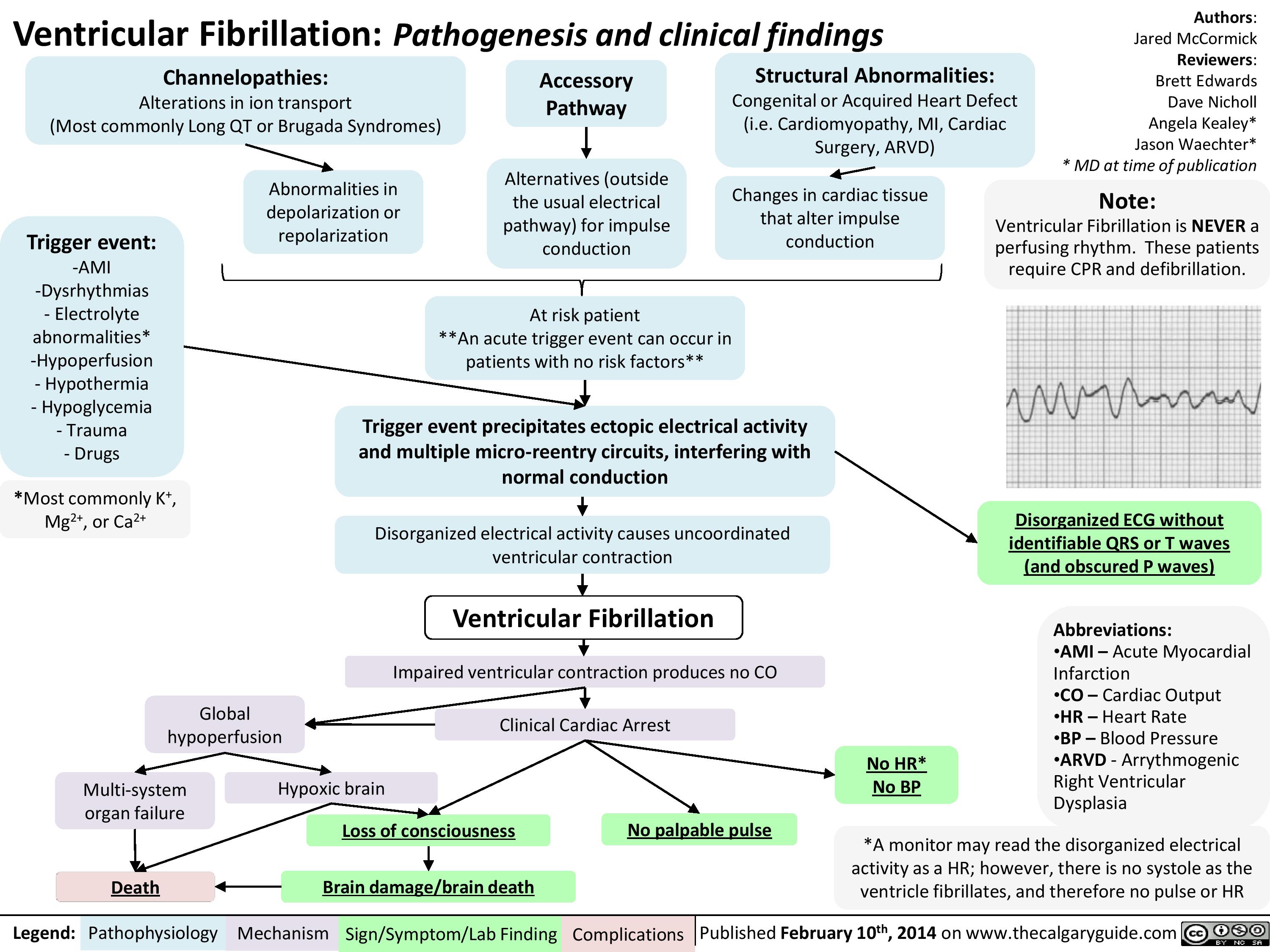
Ventricular fibrillation
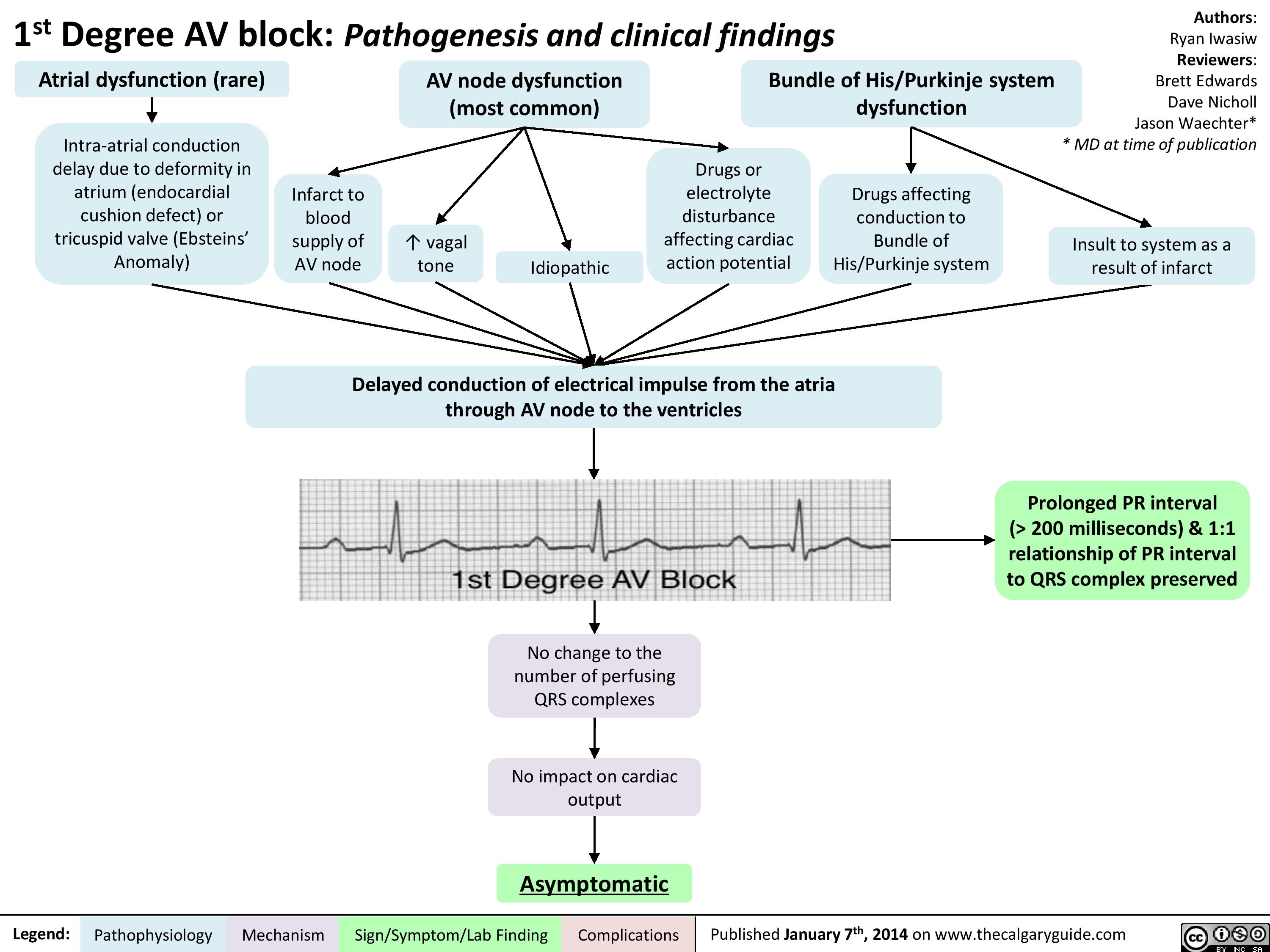
1st Degree AV block
Second Degree Heart Block - Mobitz Type II - Pathogenesis and clinical findings

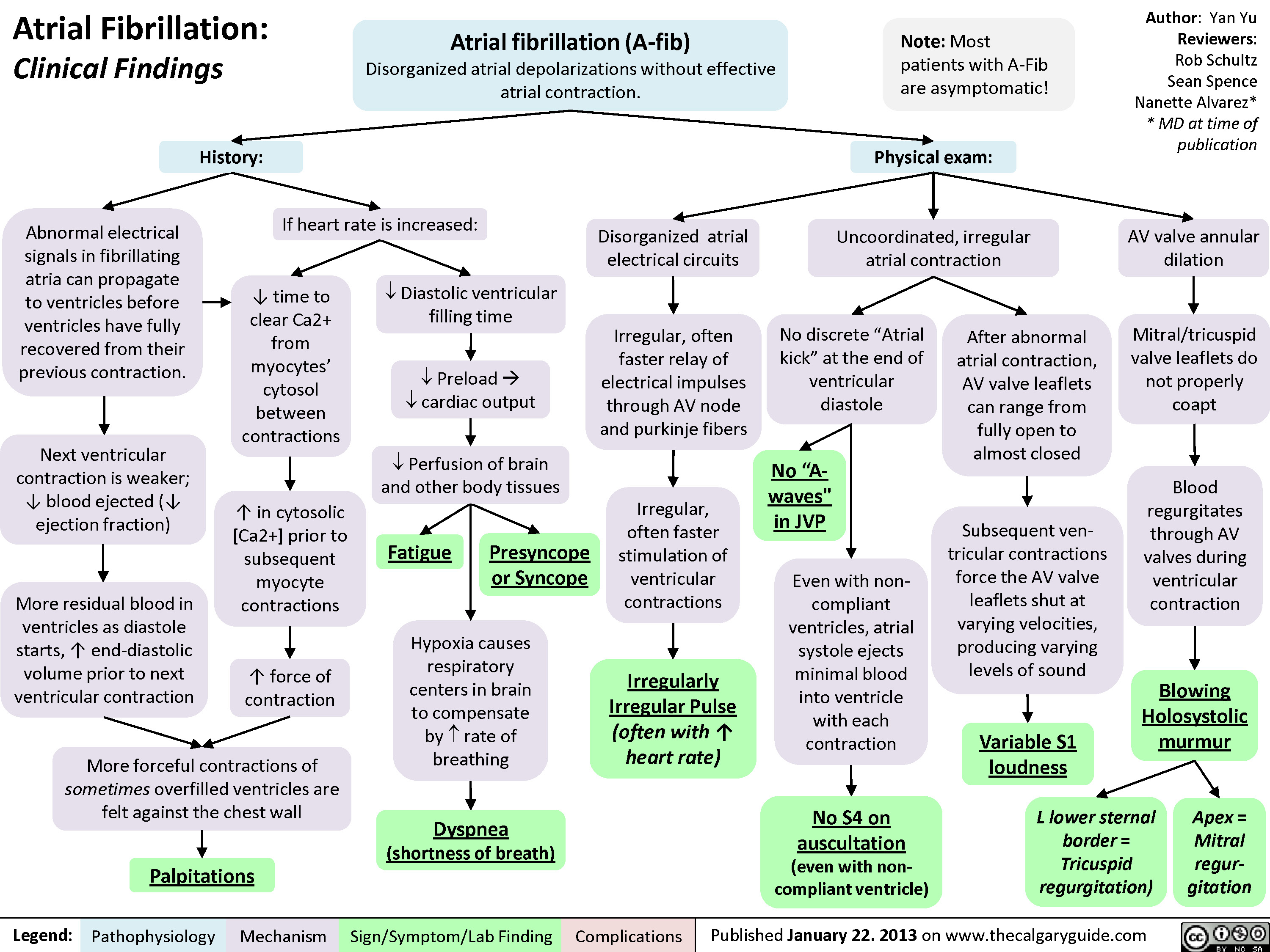
Atrial Fibrillation - Clinical Findings
atrial-fibrillation-complications

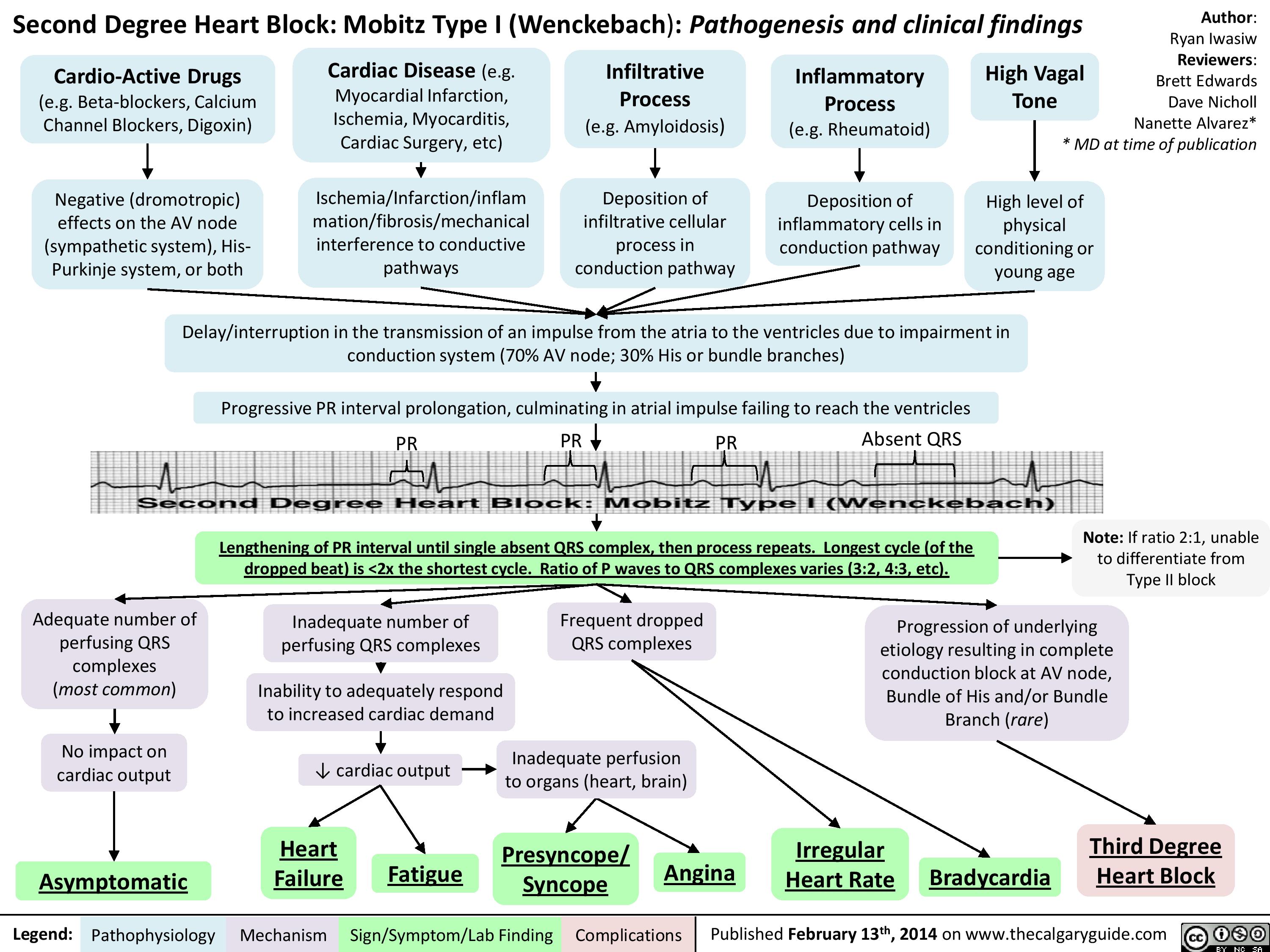
Second Degree Heart Block - Mobitz Type I (Wenckebach) - Pathogenesis and Clinical Findings
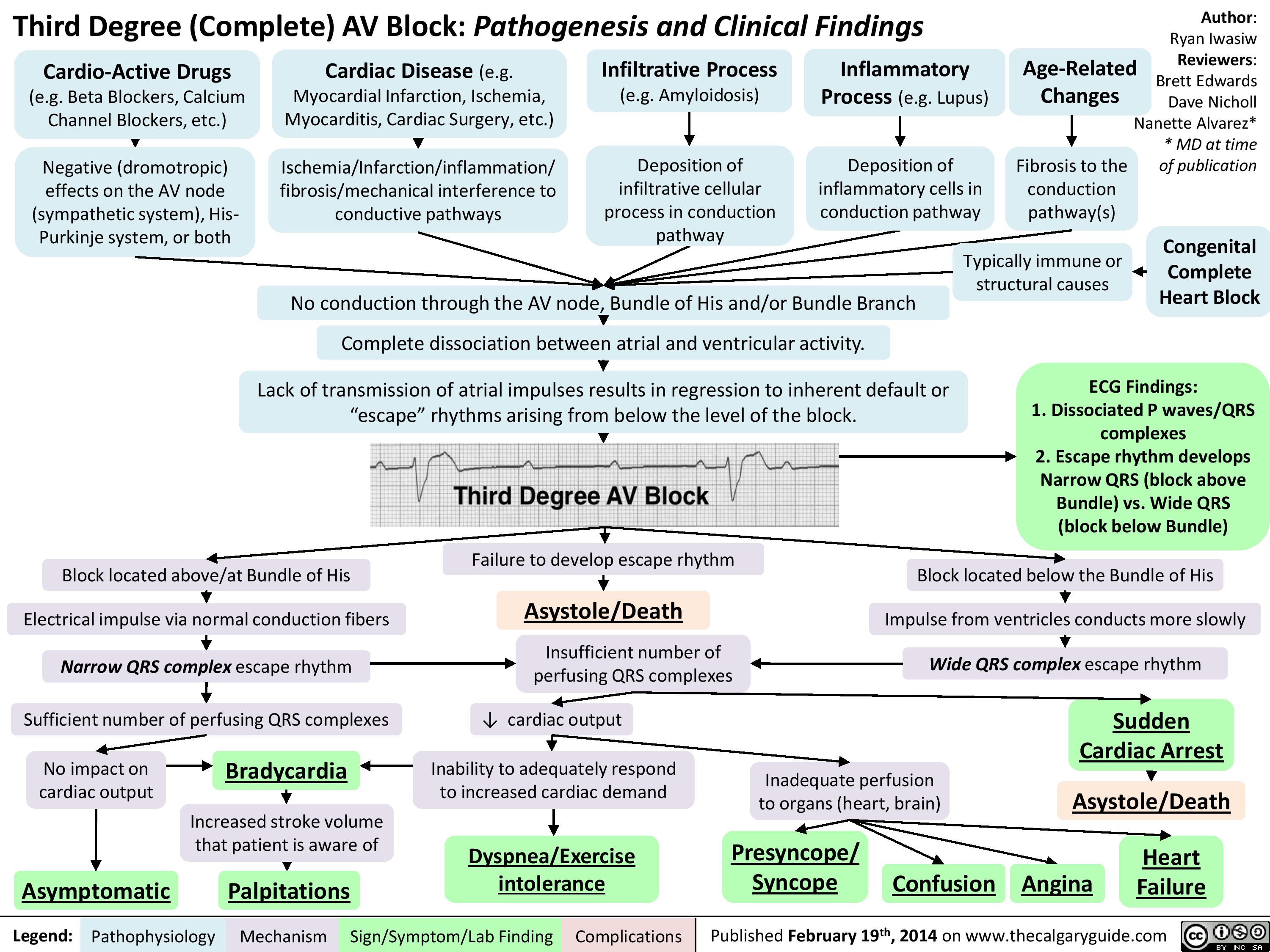
Third Degree (Complete) AV Block - Pathogenesis and Clinical Findings
Atrial Flutter (1)
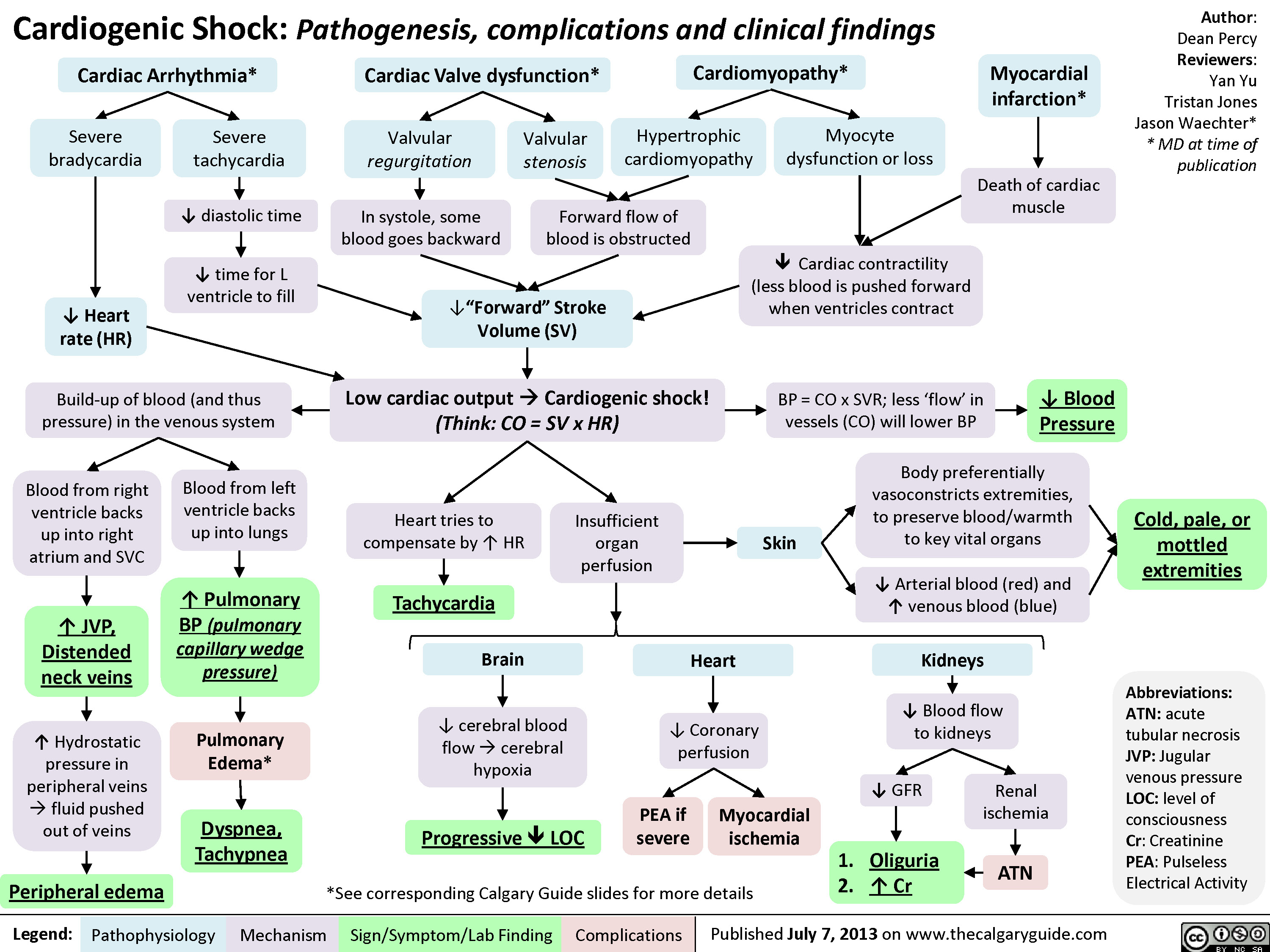
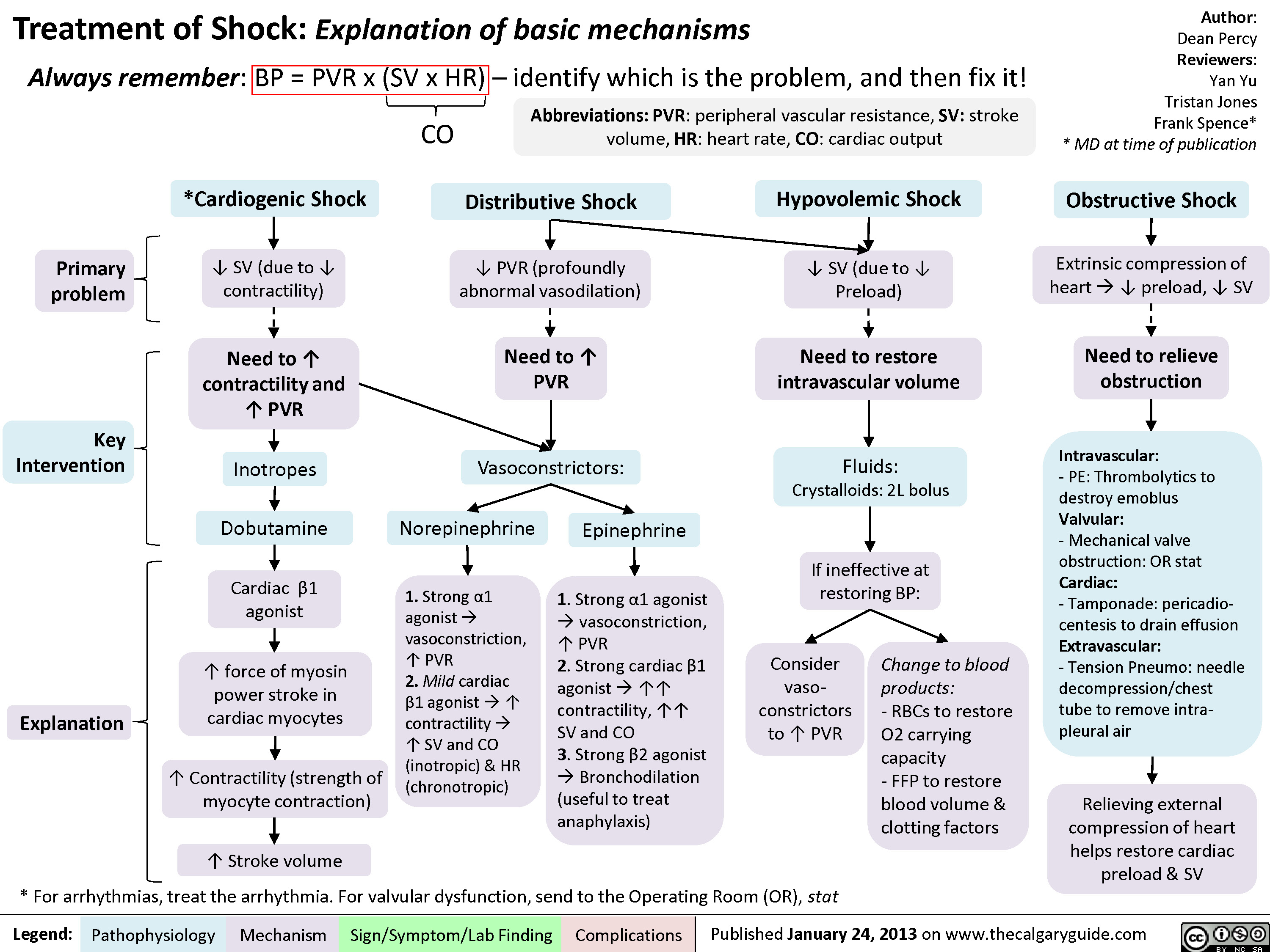
Cardiogenic Shock
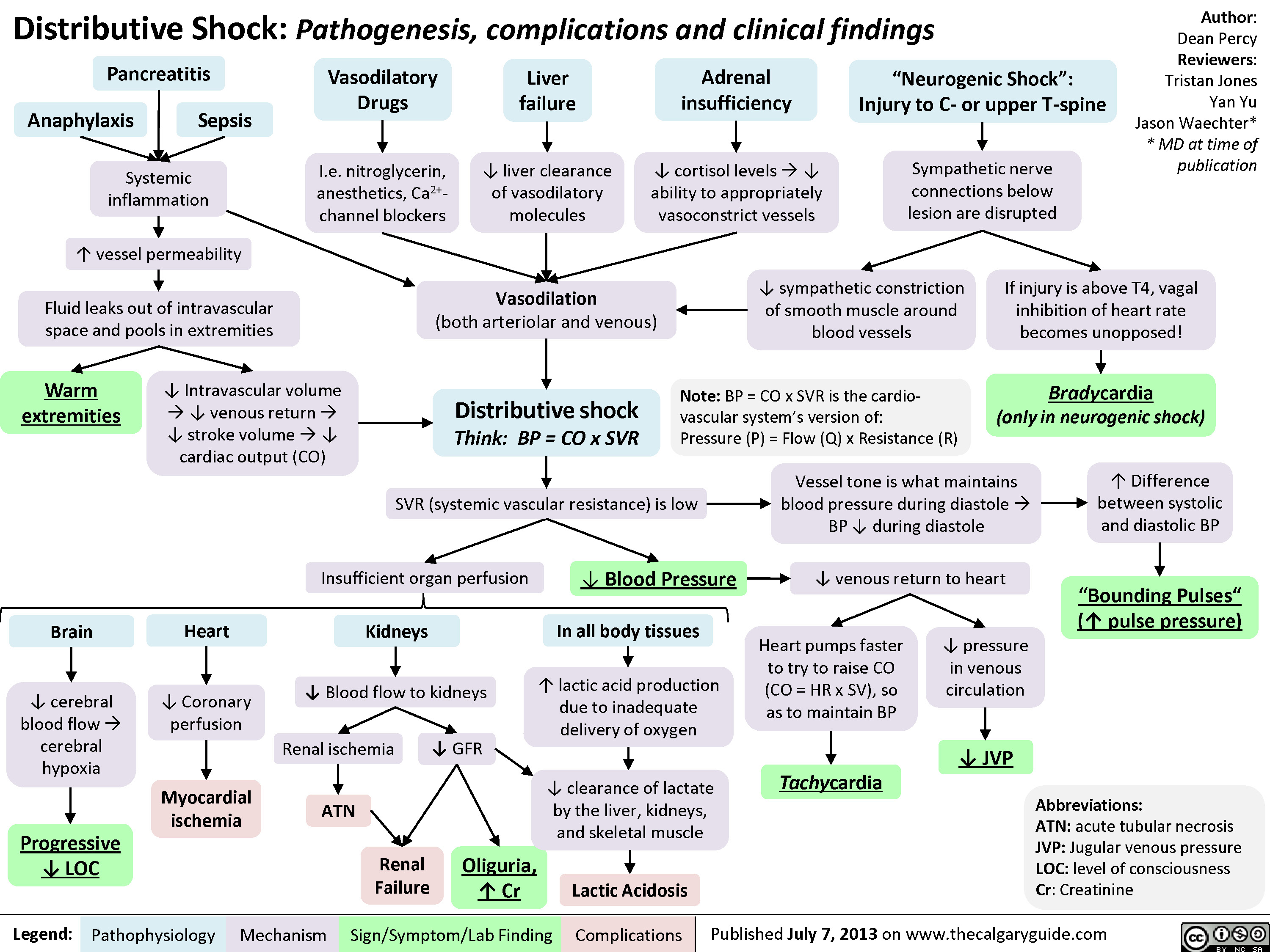
Distributive Shock
Obstructive Shock

Drugs used to treat shock
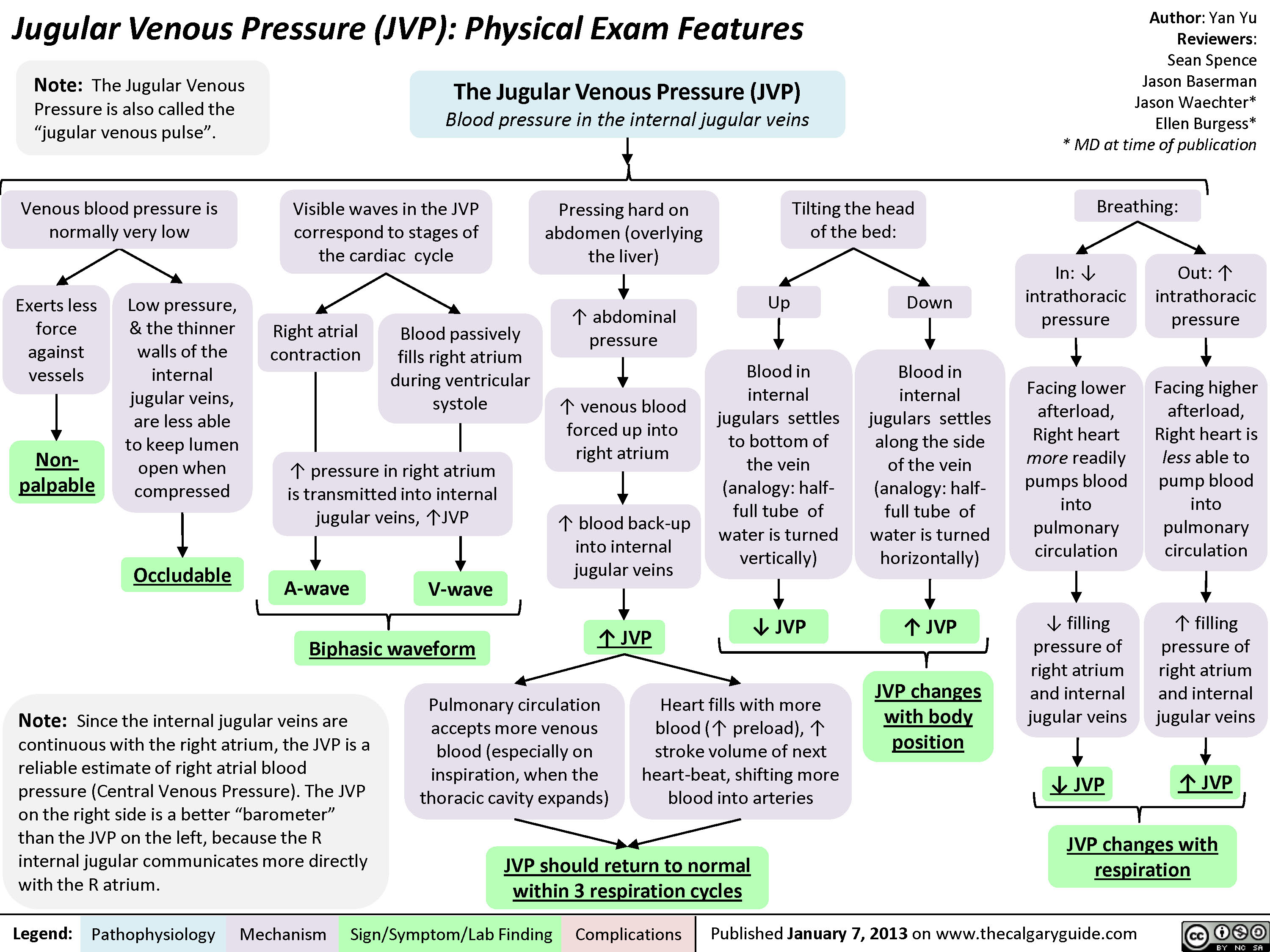
JVP-Physical Exam Features
jvp-kussmals-sign-explained
: Kussmal's Sign explainedExcessive pericardial fluid compresses heart walls on all sidesLegend:Published January 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsAuthor: Yan YuReviewers:Sean SpenceJason BasermanJason Waechter** MD at time of publication? Right ventricle wall complianceConstrictive pericarditisRight ventricle prevented from fully expanding ? ability of the right ventricle to accommodate higher venous returnBackup of venous blood into right atrium and preceding internal jugular veinsRestrictive cardiomyopathyInflamed, fibrotic pericardium restricts expansion of heartRight ventricle myocardial infarct Cardiac tamponade (rare)InspirationMore venous blood tries to enter the low-pressure thoracic cavity via the right ventricle? pressure in thoracic cavity
JVP should return to normal within 3 respiration cyclesJugular Venous Pressure (JVP): Physical Exam FeaturesExerts less force against vesselsTilting the head of the bed:Low pressure, & the thinner walls of the internal jugular veins, are less able to keep lumen open when compressedLegend:Published January 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsAuthor: Yan YuReviewers:Sean SpenceJason BasermanJason Waechter** MD at time of publicationBlood in internal jugulars settles to bottom of the vein (analogy: half-full tube of water is turned vertically)Visible waves in the JVP correspond to stages of the cardiac cycleNon-palpableBiphasic waveform? JVP The Jugular Venous Pressure (JVP) Blood pressure in the internal jugular veinsV-waveA-waveRight atrial contractionBlood passively fills right atrium during ventricular systole? JVP? JVPIn: ? intrathoracic pressurePressing hard on abdomen (overlying the liver), or doing a valsalvaFacing lower afterload, Right heart more readily pumps blood into pulmonary circulation? abdominal pressure? venous blood forced up into right atriumVenous blood pressure is normally very lowOccludableNote: Since the internal jugular veins are continuous with the right atrium, the JVP is a reliable estimate of right atrial blood pressure (Central Venous Pressure). The JVP on the right side is a better")
Pulsus Paradoxus
Pulsus ParadoxusThrombi in the pulmonary arteries ? blood filling pulmonary vasculatureLegend:Published January 21, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsAuthor: Yan YuReviewers:Sean SpenceLaura CraigNanette Alvarez** MD at time of publication? ? ? forward blood flow from lungs into left heartWith cardiac pathology external to myocardium(Cardiac tamponade, or rarely with constrictive pericarditis)? Right heart filling, ? blood flow into lung vesselsMore blood returns to R heart ? more blood enters and pools in pulmonary vasculature? blood returns to the left heart, ? its fillingWith obstructive lung diseases (i.e. COPD)With vascular pathology (rare):InspirationNormally:? lung volume ? ? intra-vascular volume within pulmonary blood vessels ? ? lung capacitance for blood, ? R heart afterloadPulsus Paradoxus:Exaggerated ?in systolic BP on inspiration (>10mmHg)? left heart stroke volume/cardiac outputOn inspiration, ? ? ? blood enter lungs and pools within pulmonary vasculature? ? ? left heart stroke volume/cardiac outputAbnormally:On inspiration, as pulmonary intra-vasculature volume expands and blood pools within, flow into the left heart ? ? ? Pulmonary embolism? venous return to R heartVena cava obstructionBy thrombi, or external compression by masses/ fibrosis (from obesity, pregnancy) As ? blood fills R heart on inspiration, external constraints on myocardium ? cardiac expansion, interventricular septum is pushed into LVThere is no room in the pericardial sac for the LV to expand and maintain normal end diastolic volume (i.e. ? LV filling)
98 kB / 233 words")
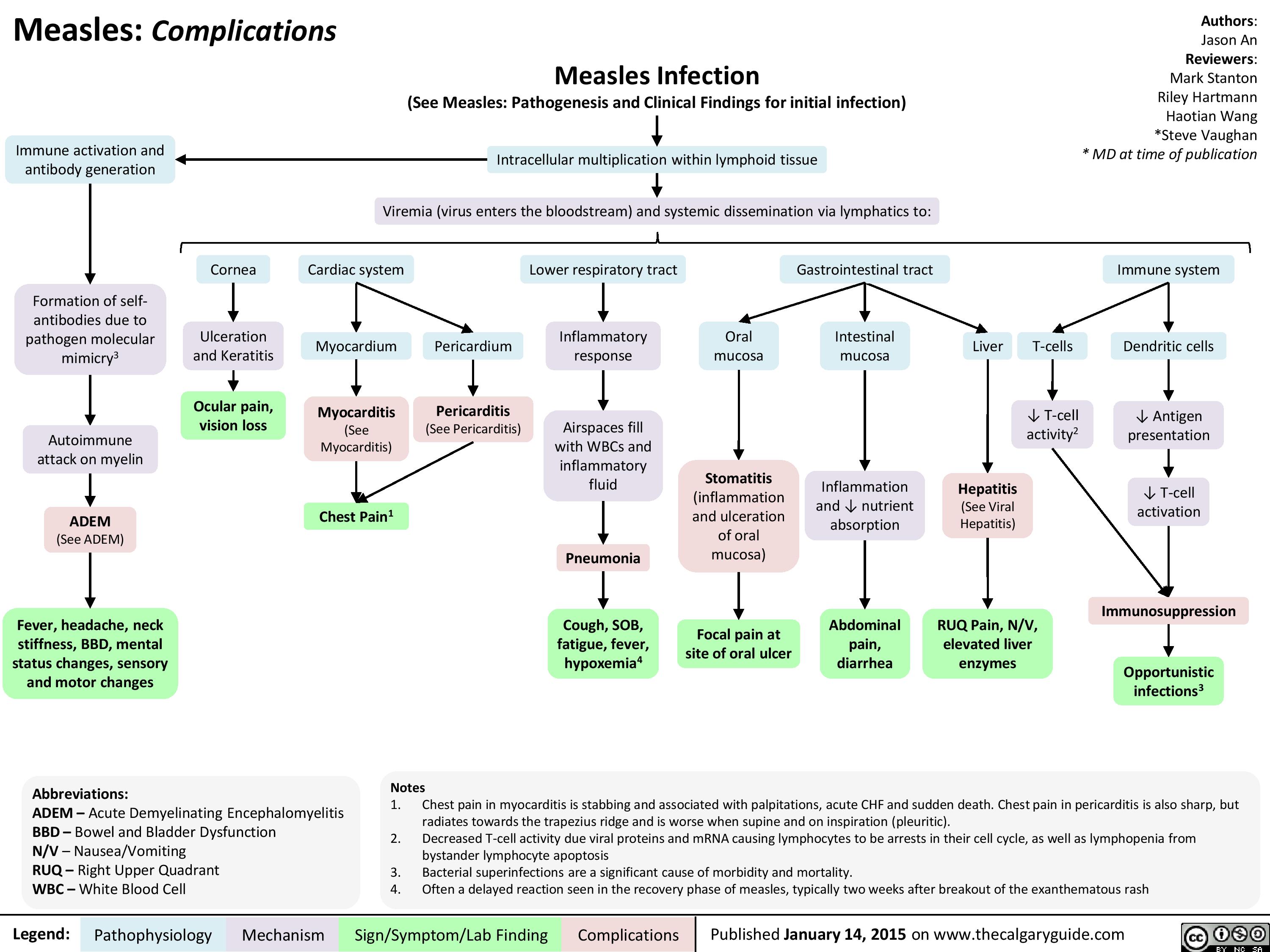
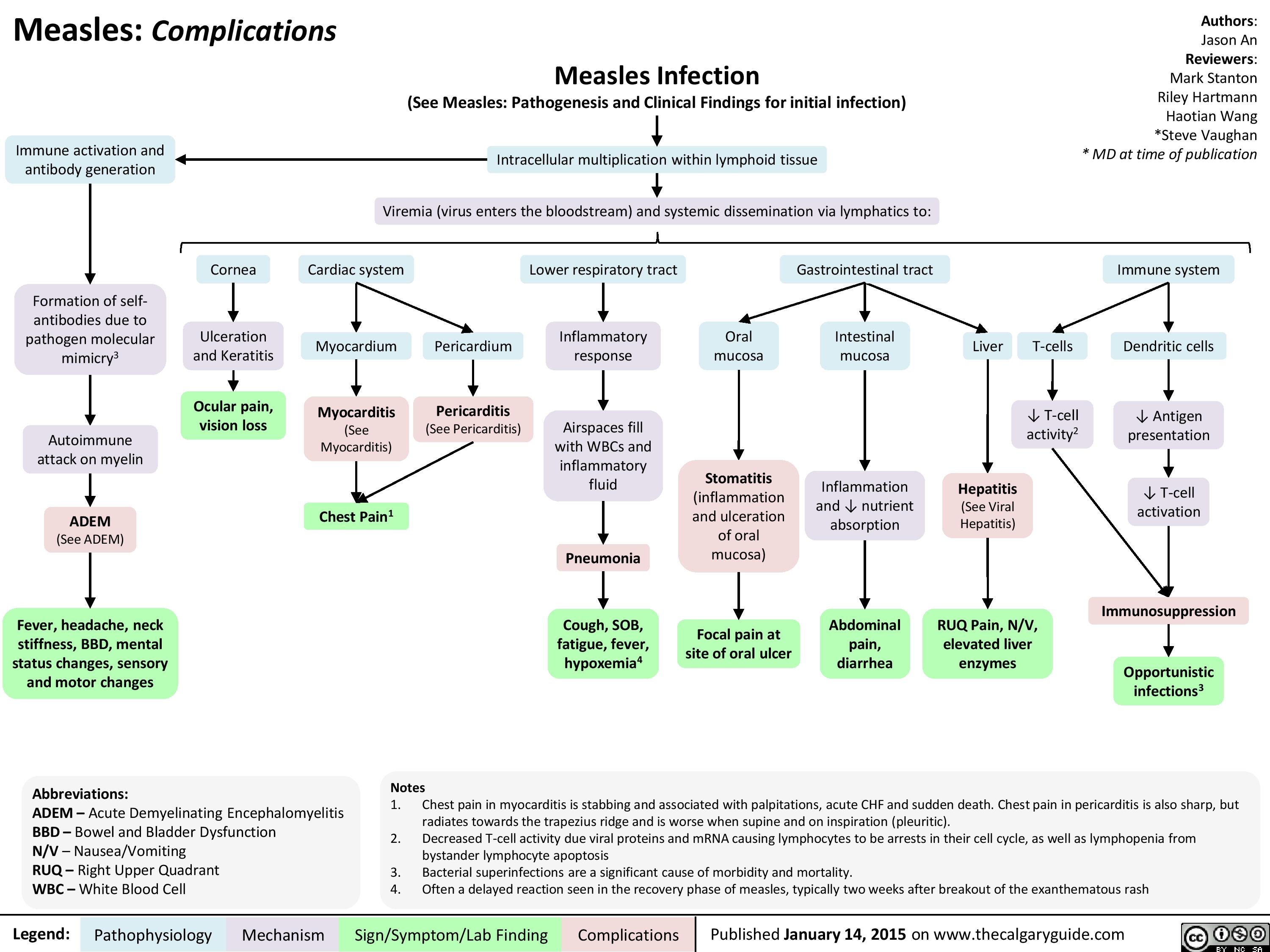
Complications of Measles Pathogenesis and Clinical Findings
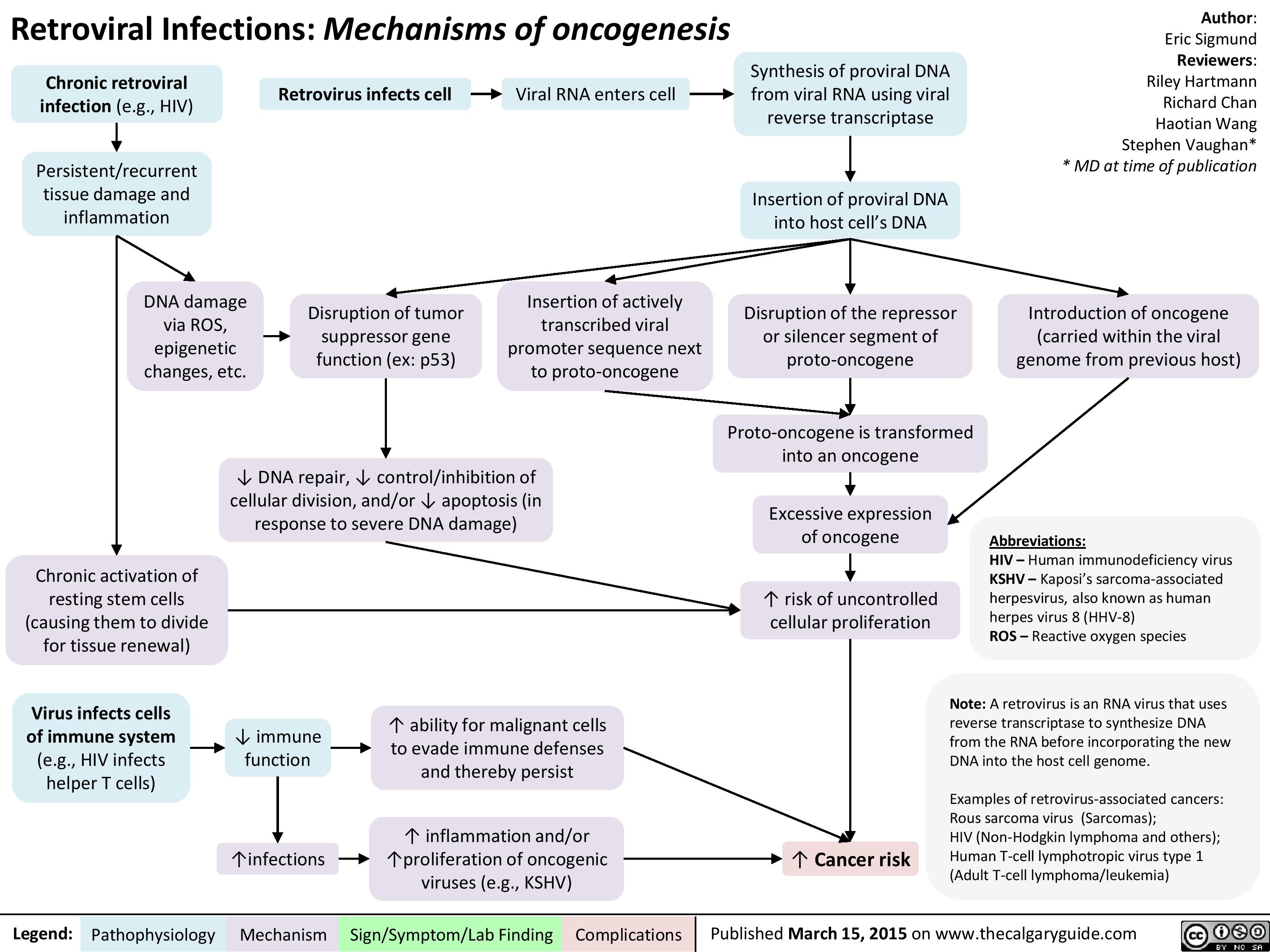
Retroviral Infections Mechanisms of oncogenesis
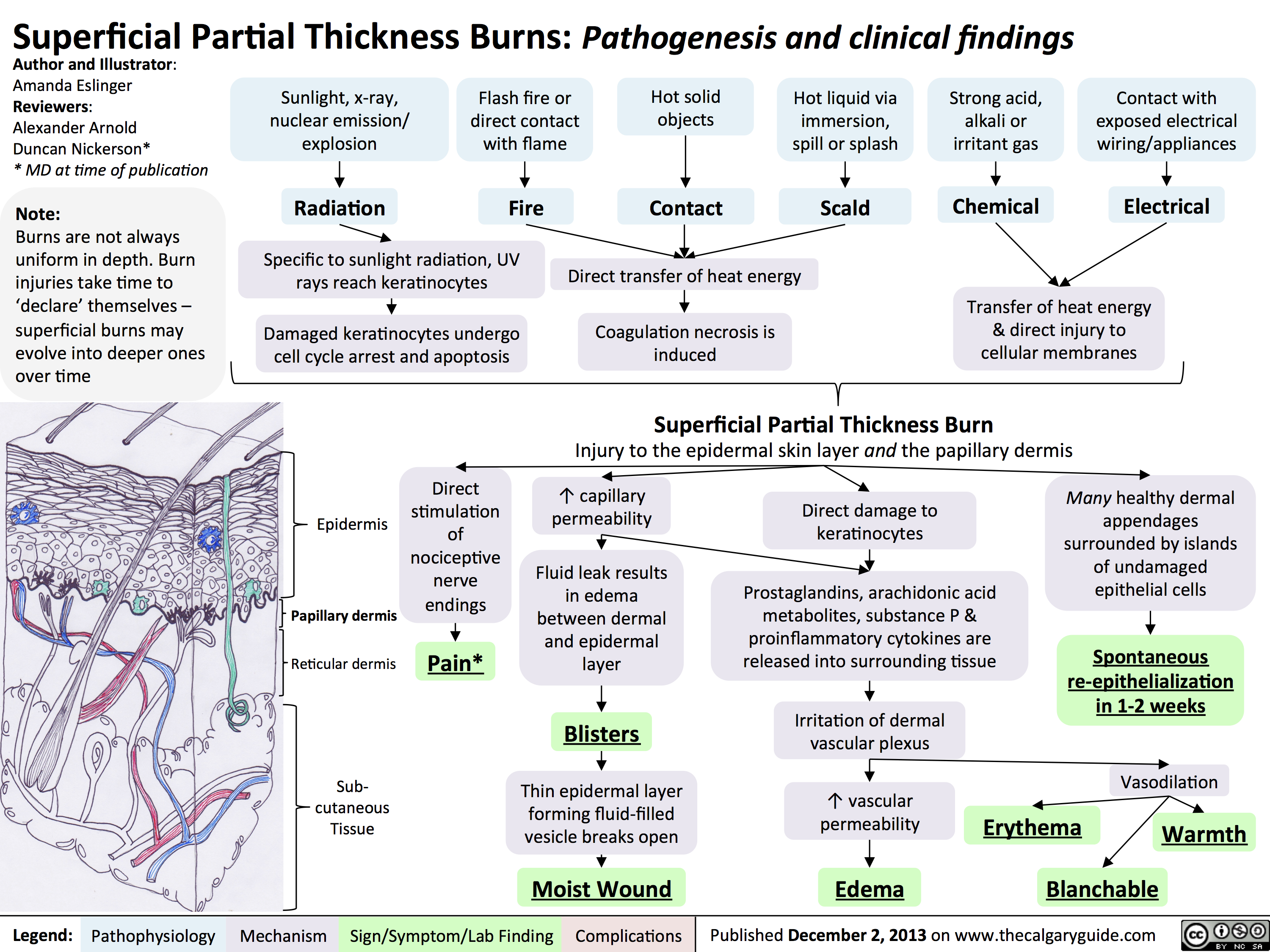
Superficial Partial Thickness Burns - Pathogenesis and Clinical Findings
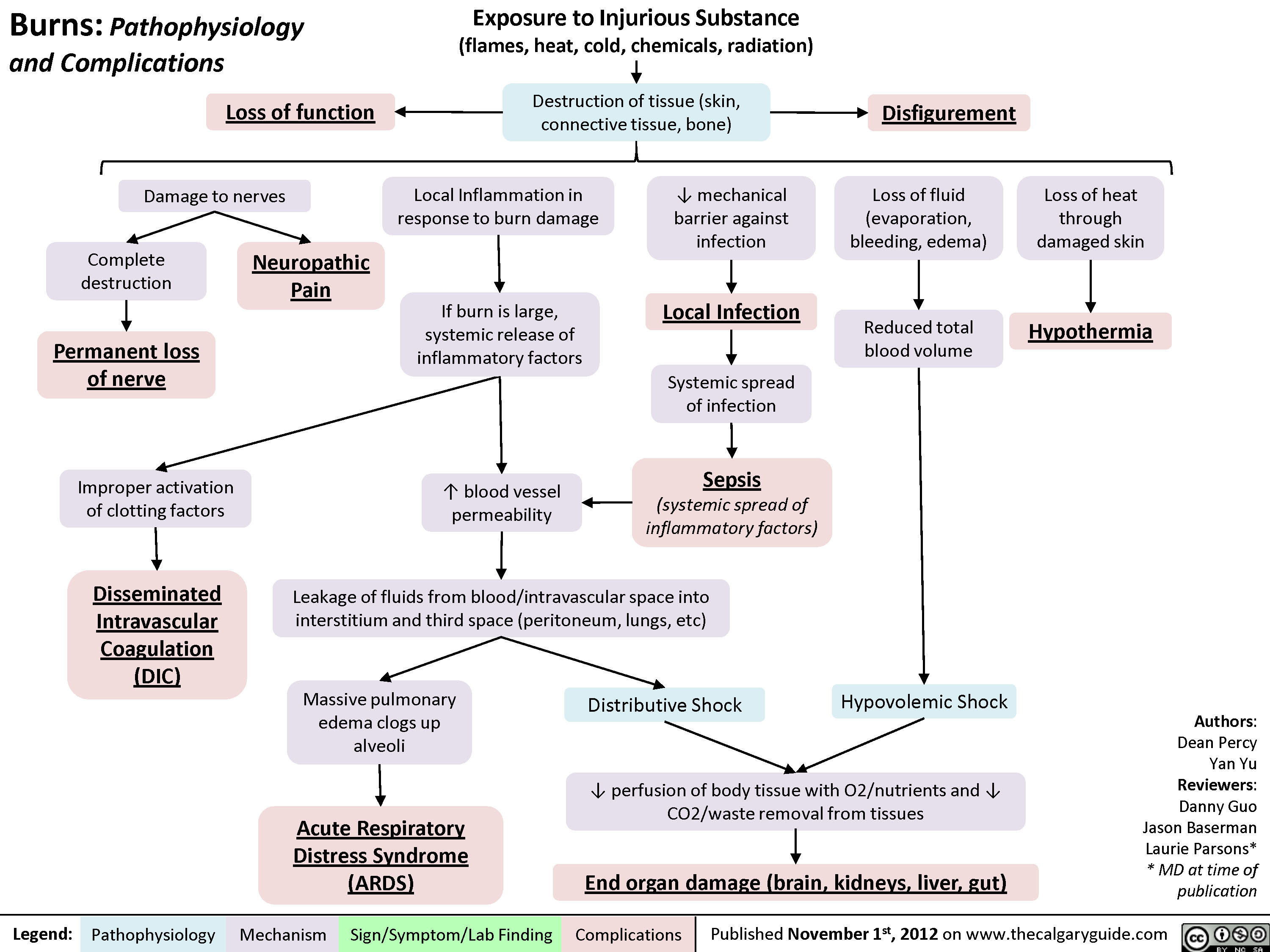
Complications of Burns
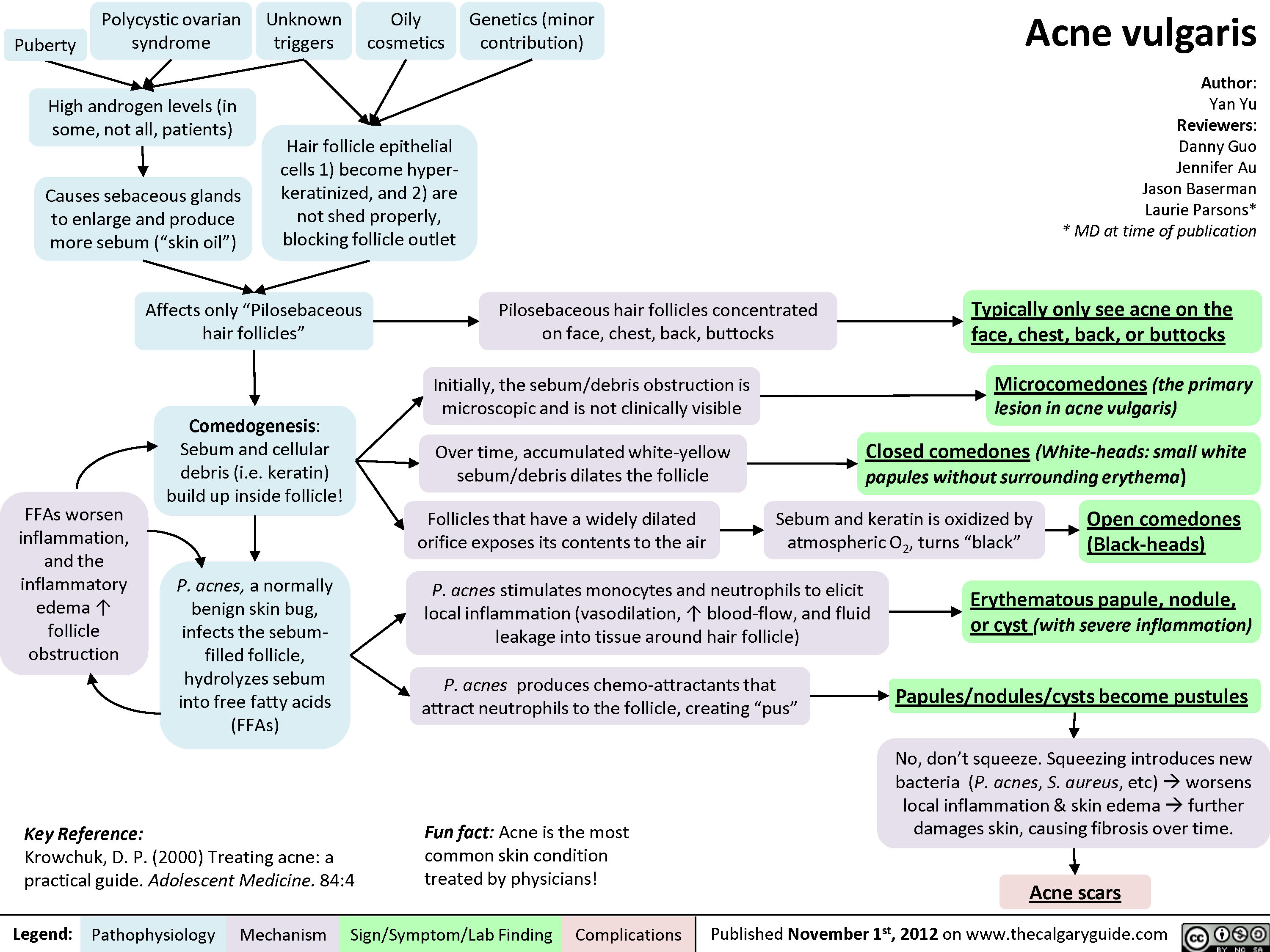
Acne Vulgaris
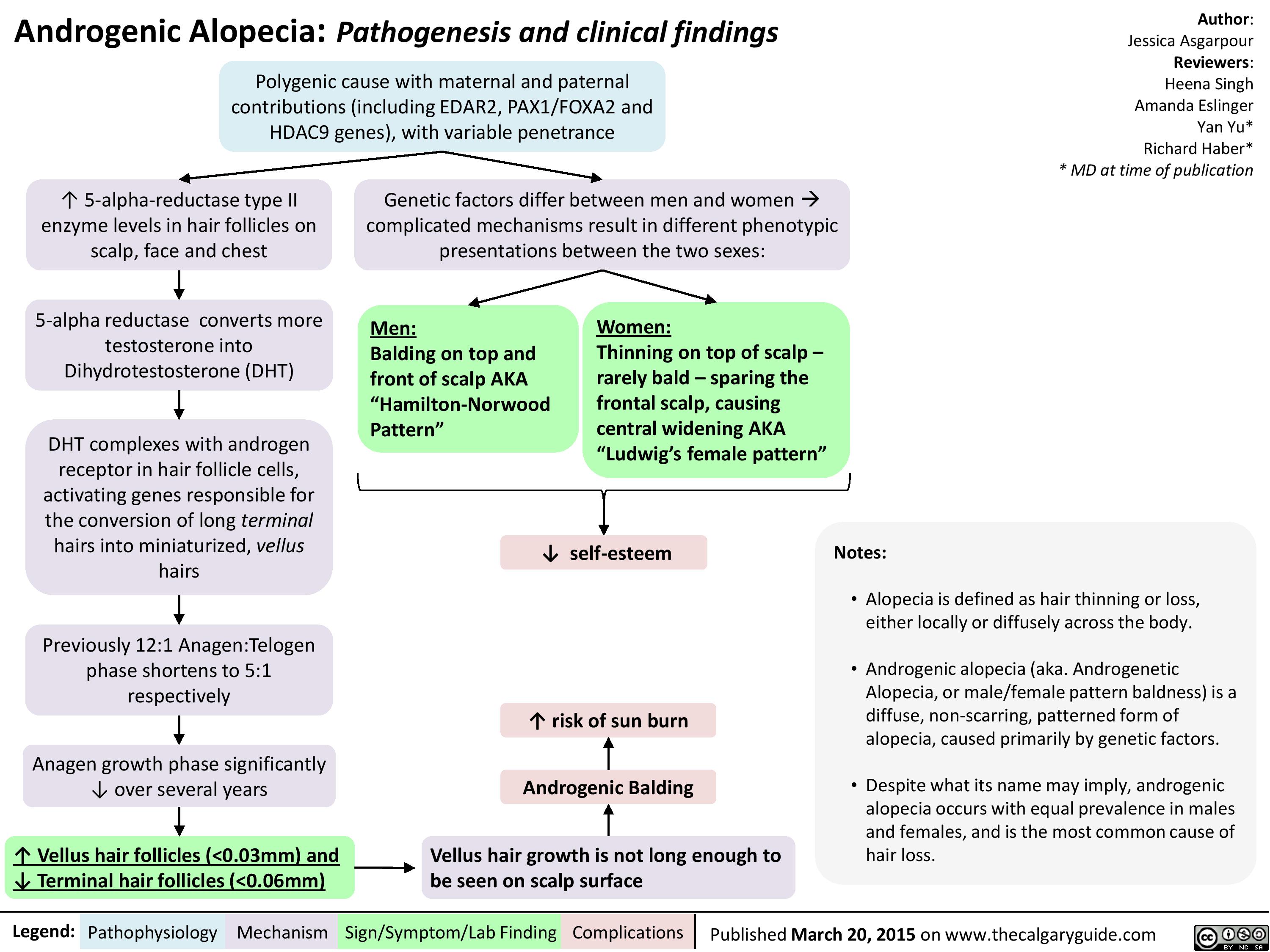
Androgenic Alopecia
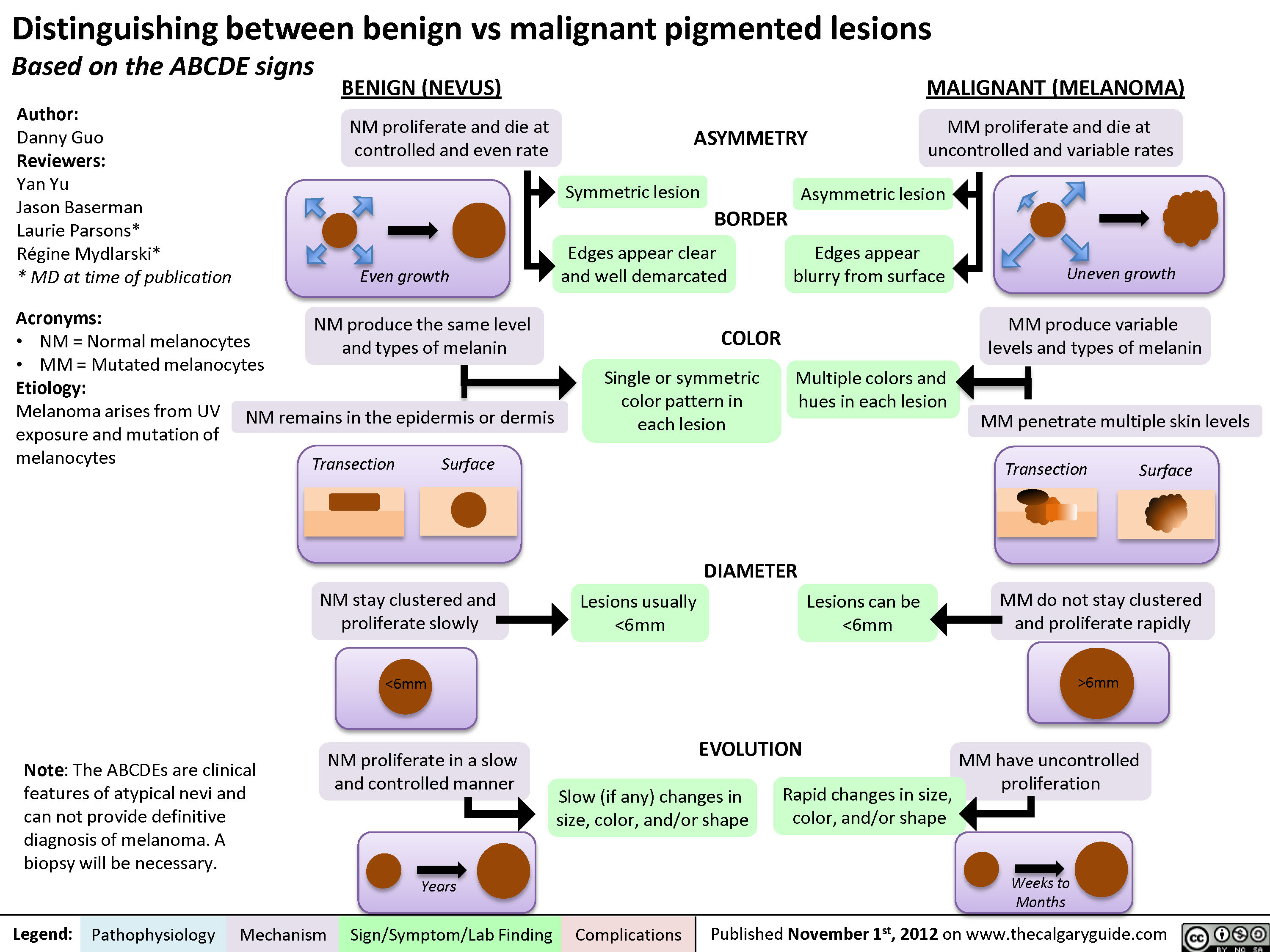
Distinguishing between Benign and Malignant Pigmented Lesions
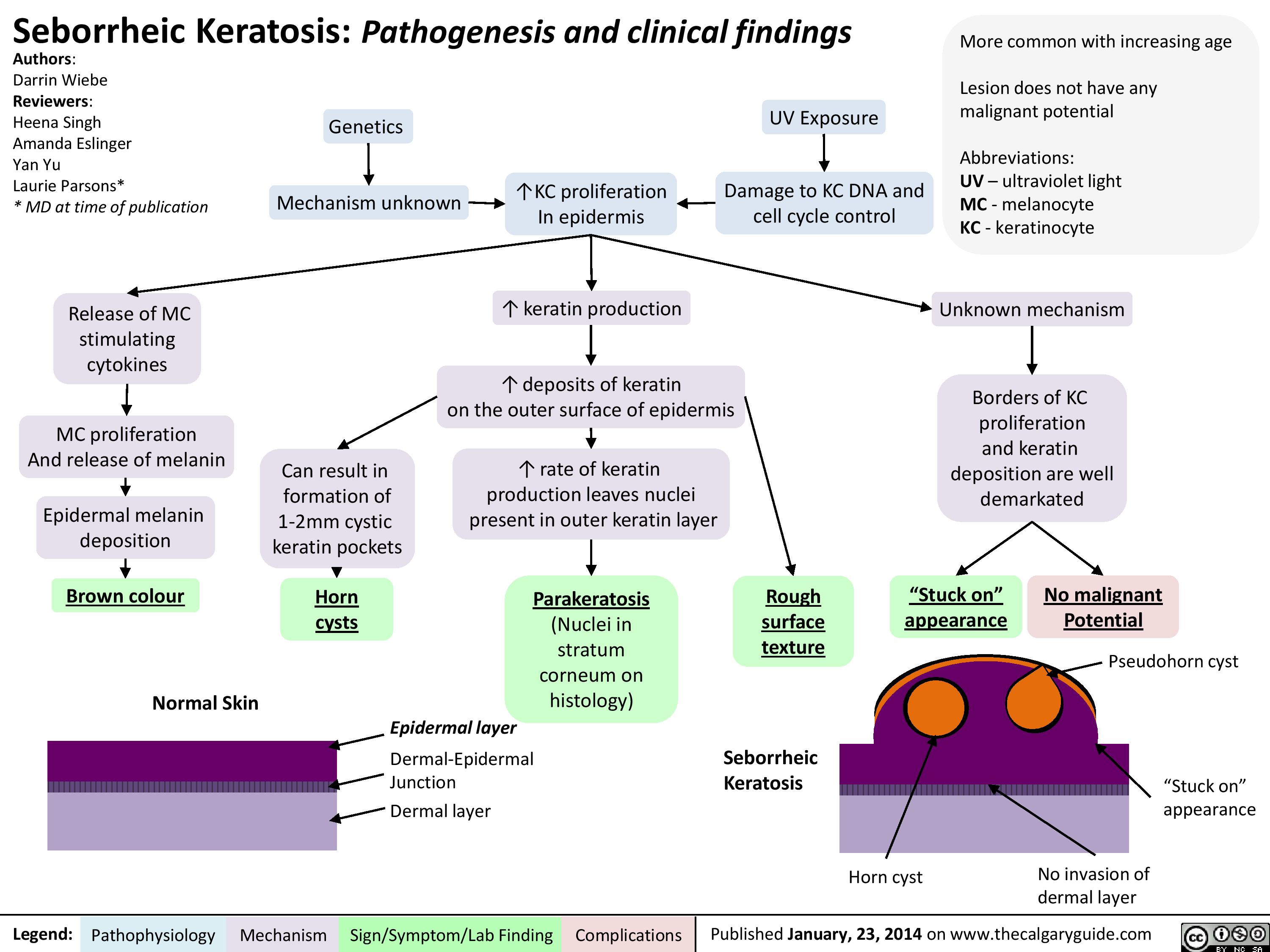
Seborrheic Keratosis
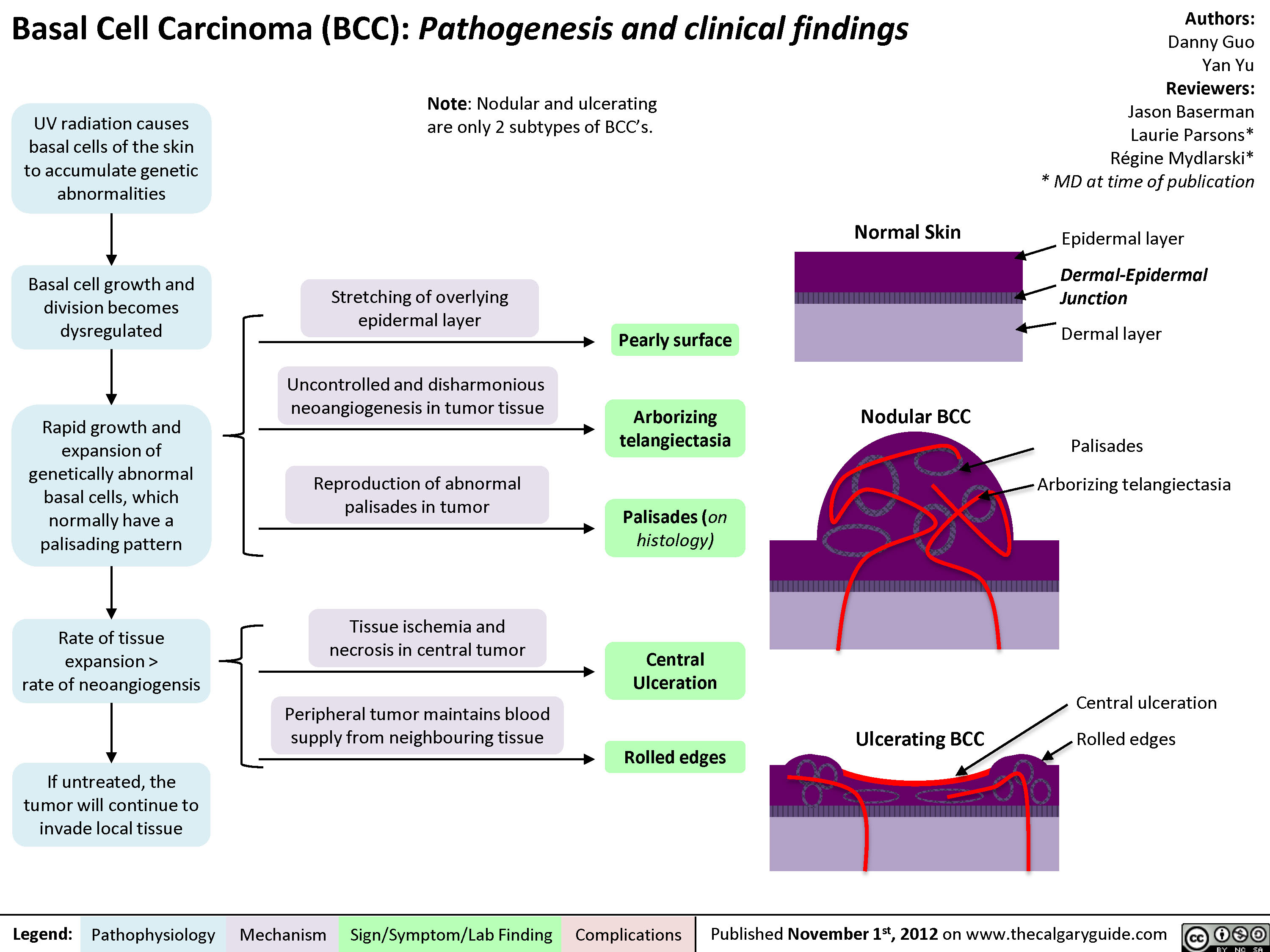
Basal Cell Carcinoma (BCC)
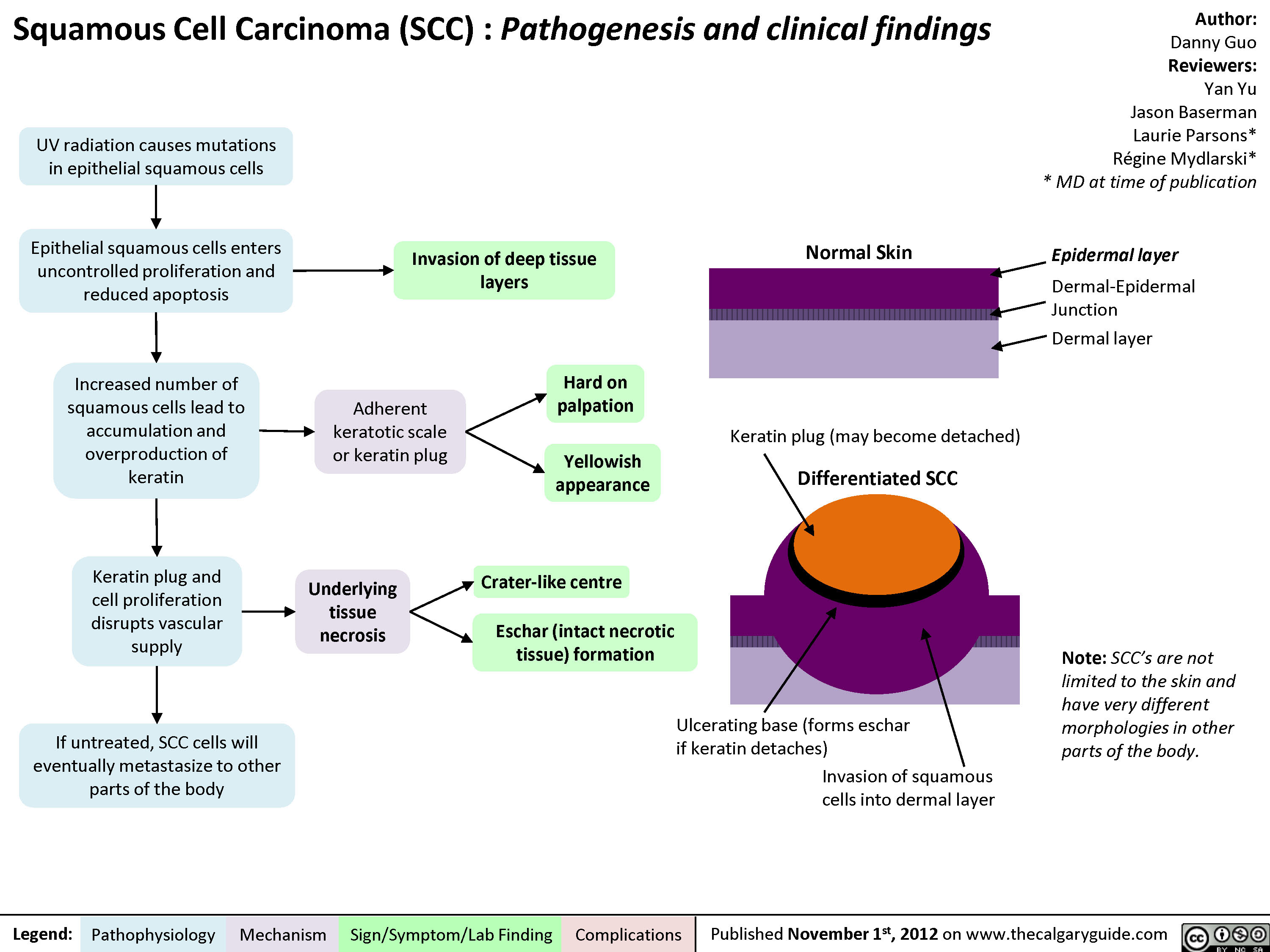
Squamous Cell Carcinoma (SCC)
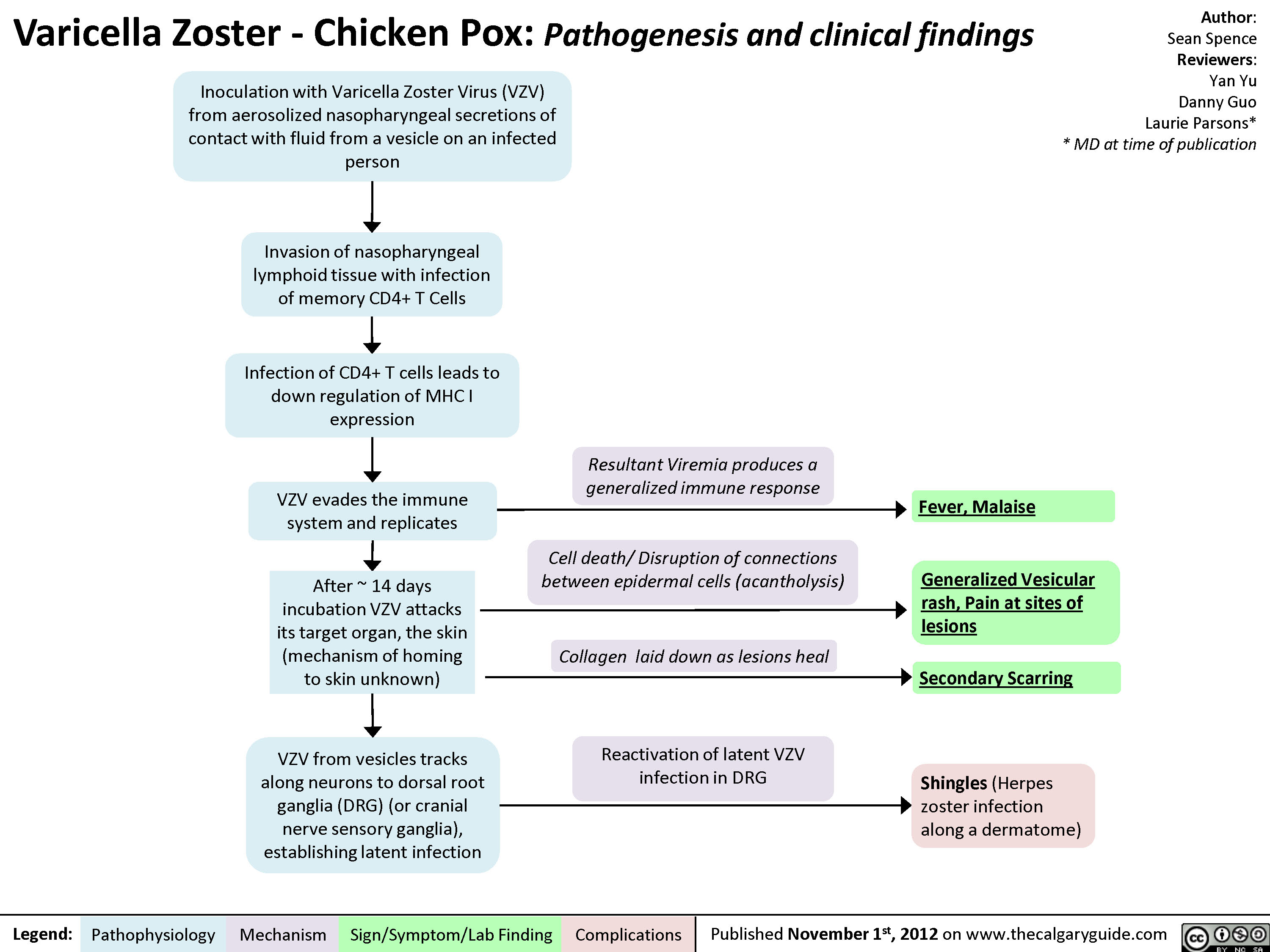
Varicella Zoster (Chicken Pox)
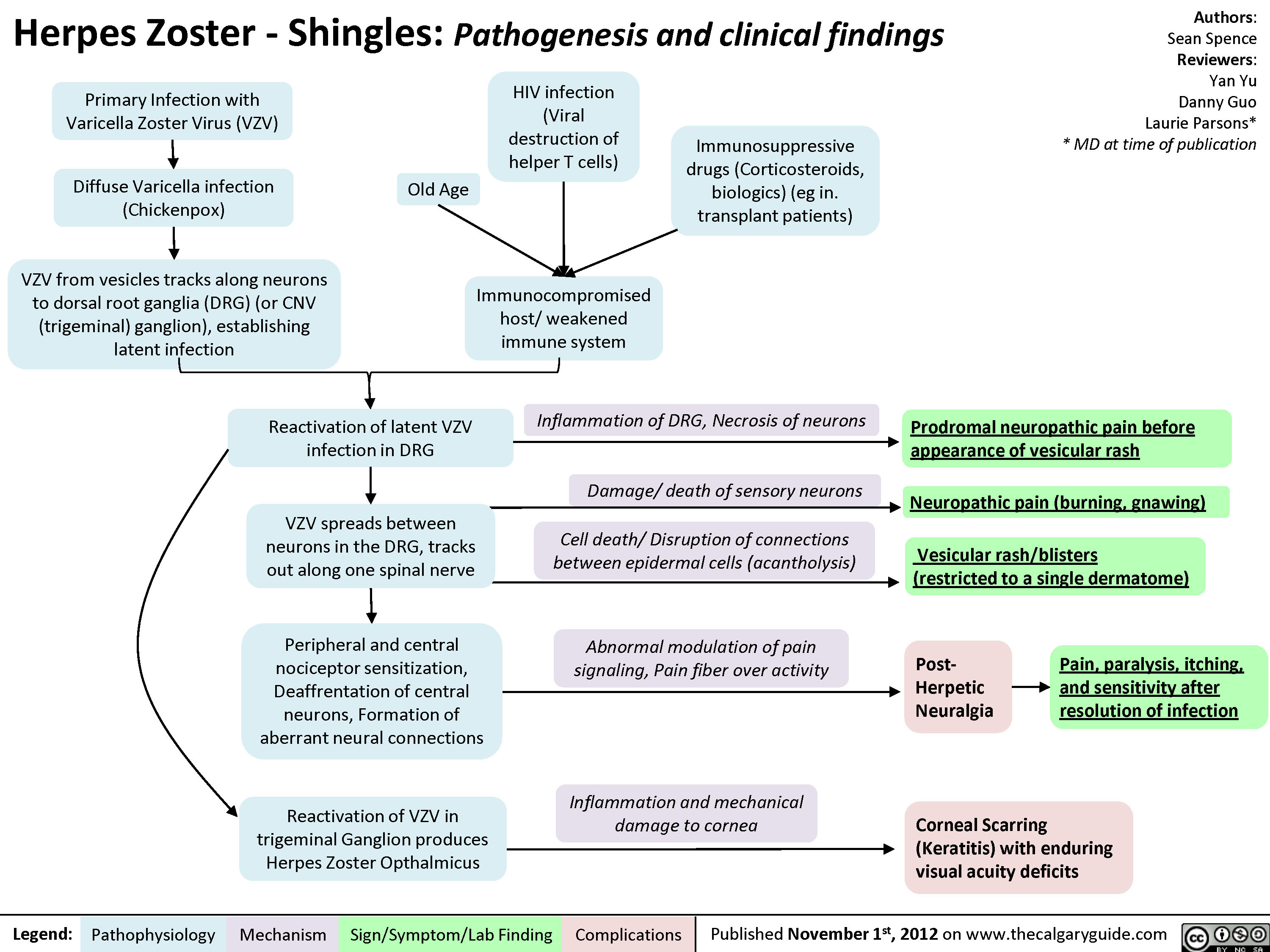
Herpes Zoster (Shingles)
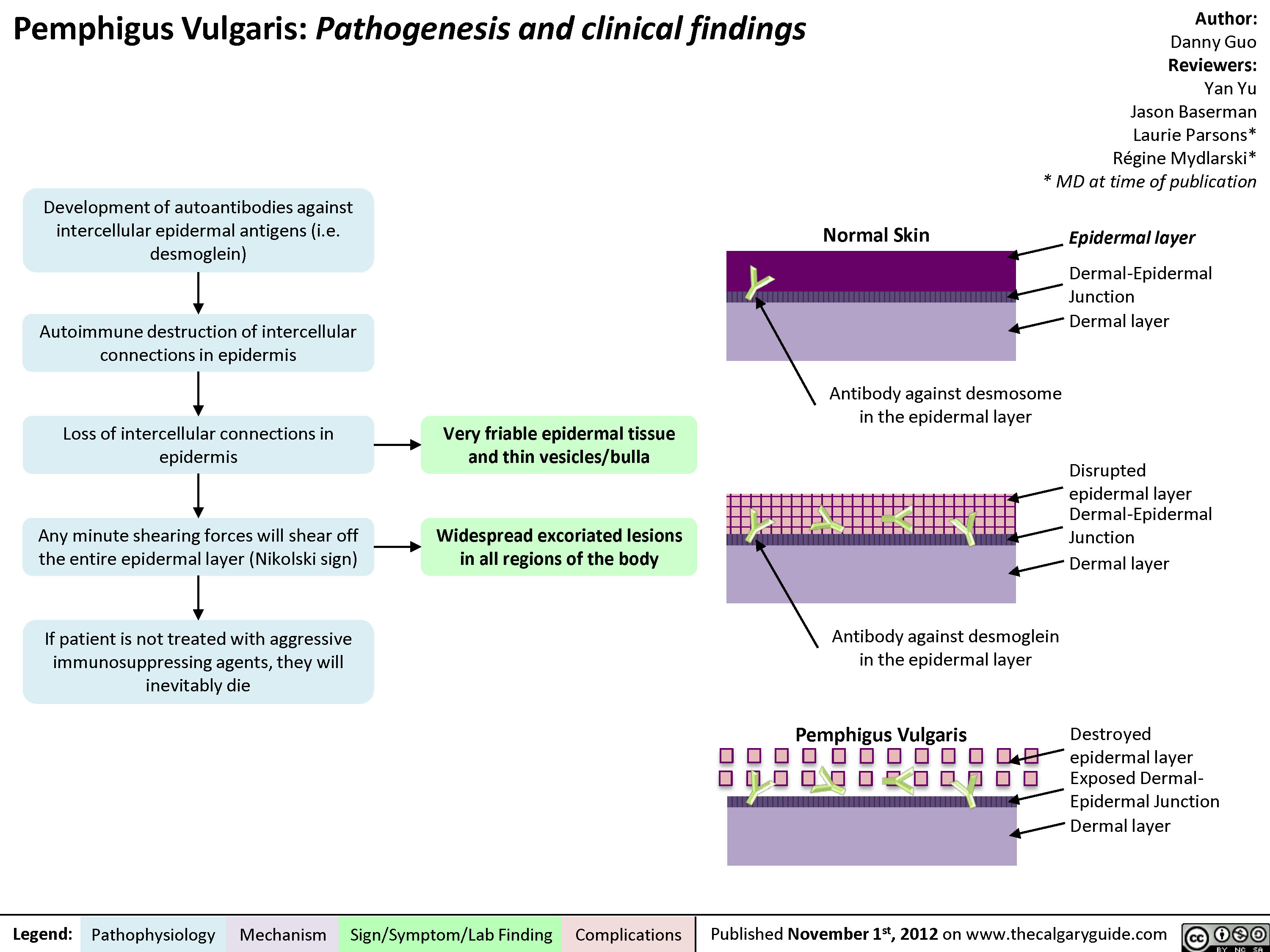
Pemphigus Vulgaris
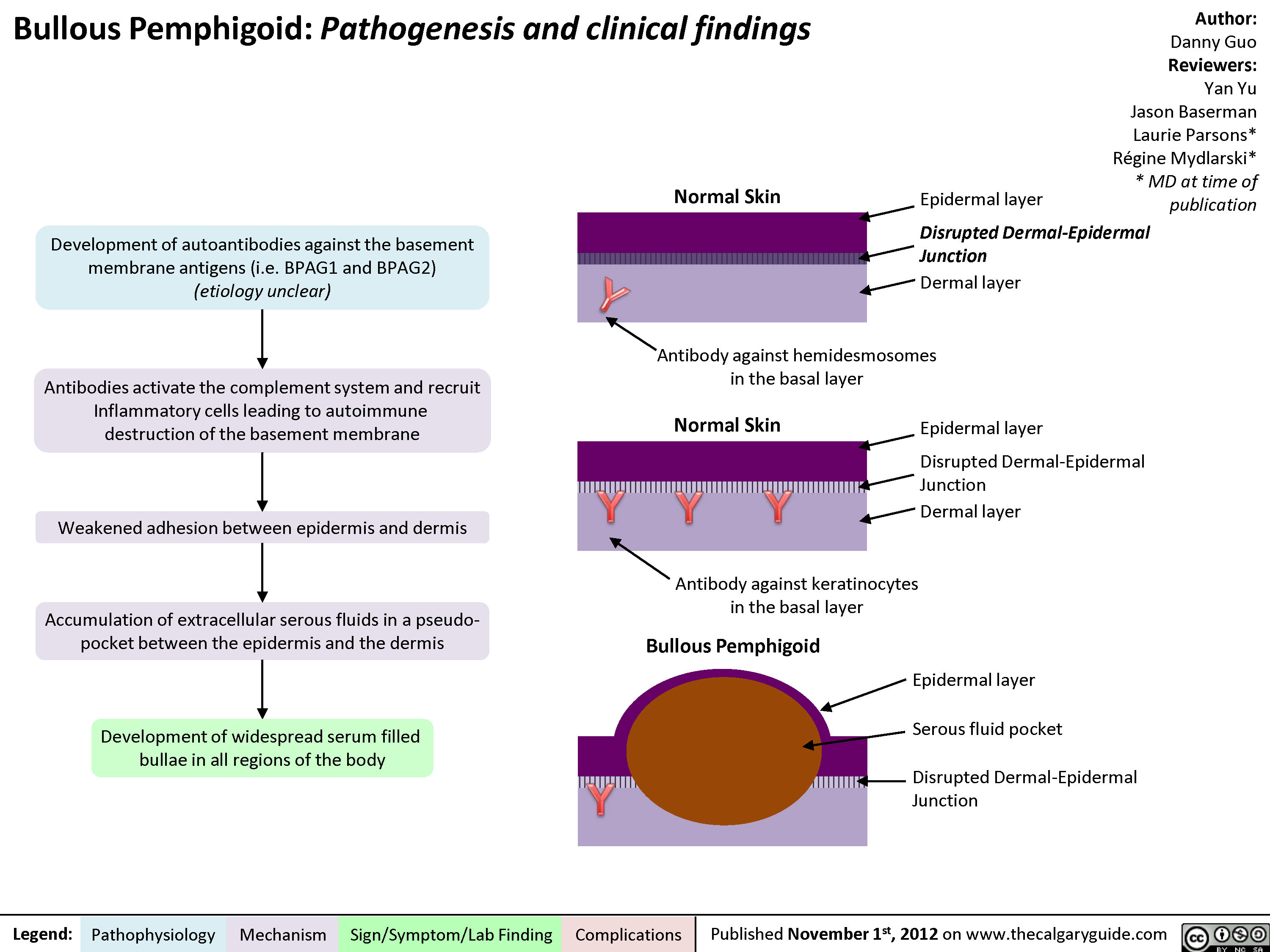
Bullous Pemphigoid
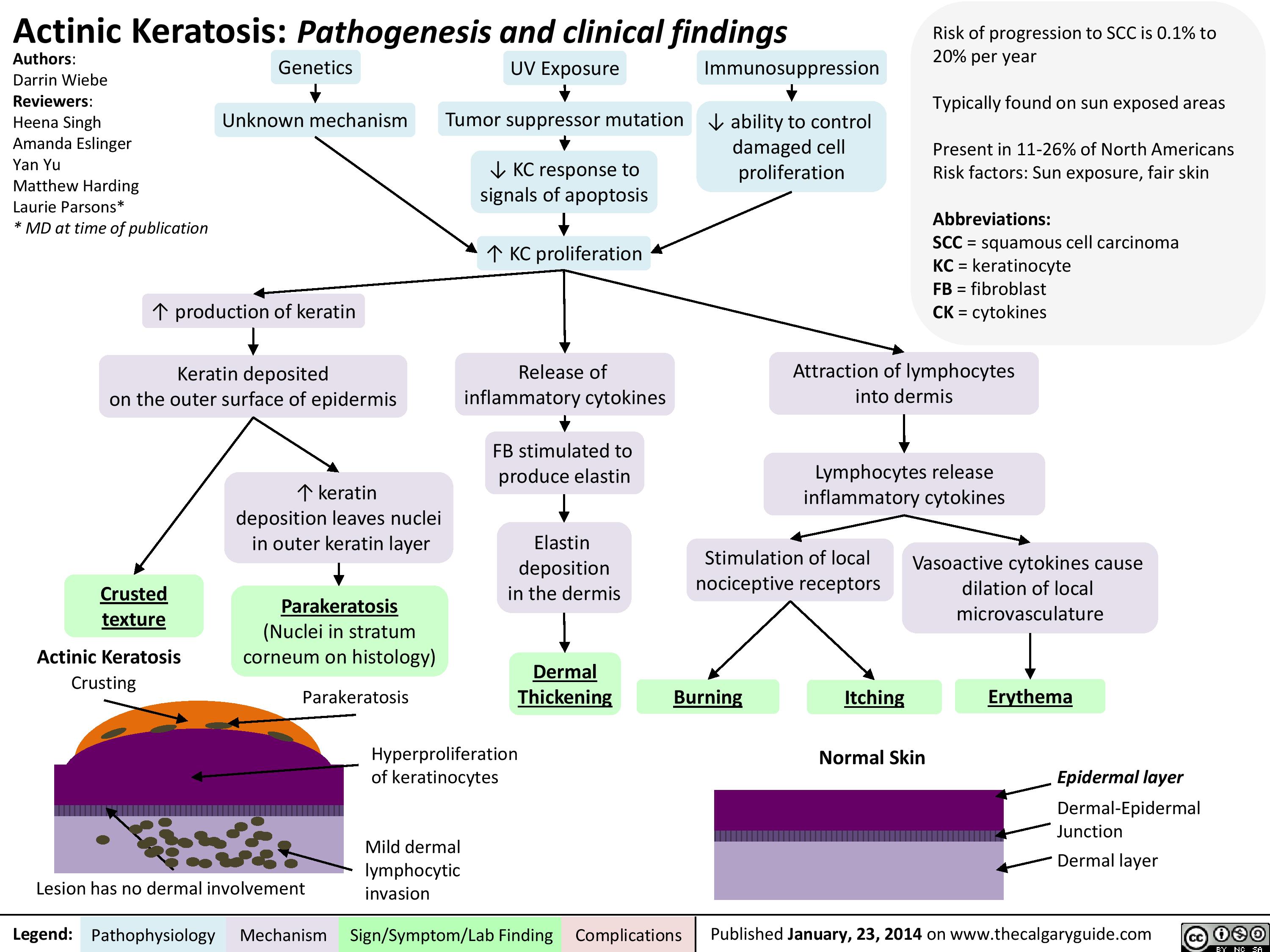
Actinic Keratosis
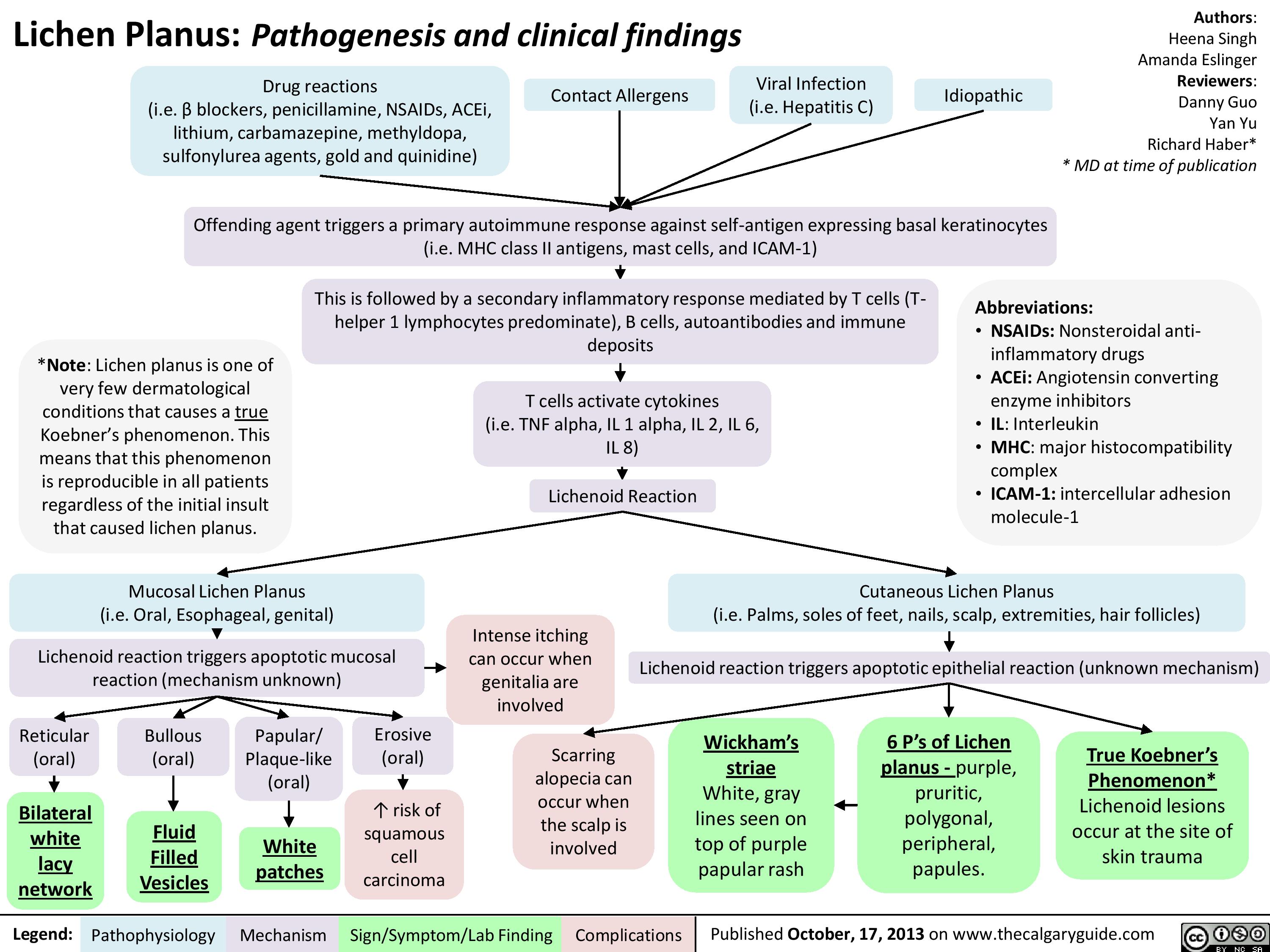
Lichen Planus
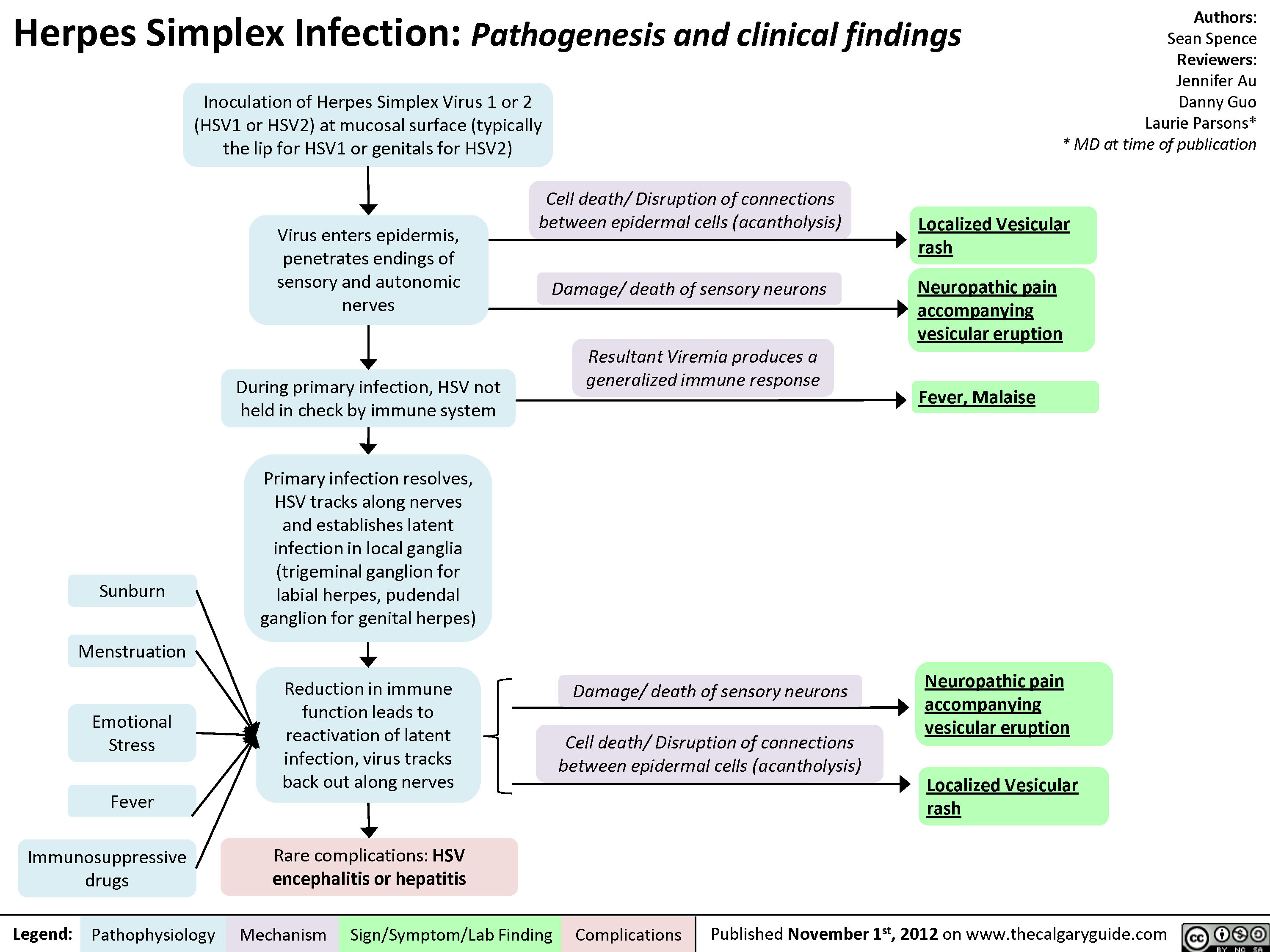
Herpes Simplex Virus (HSV)
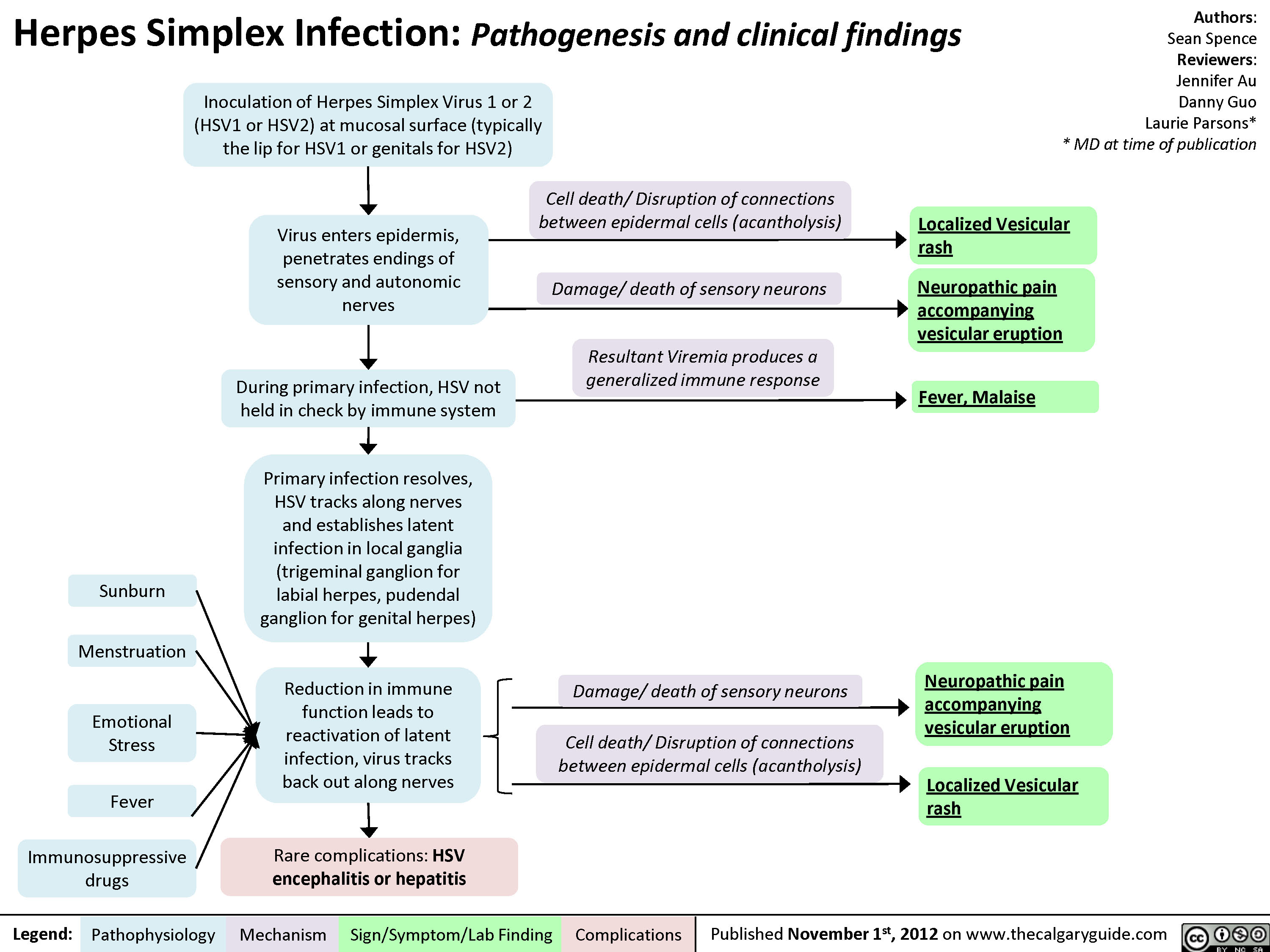
Herpes Simplex Virus (HSV)
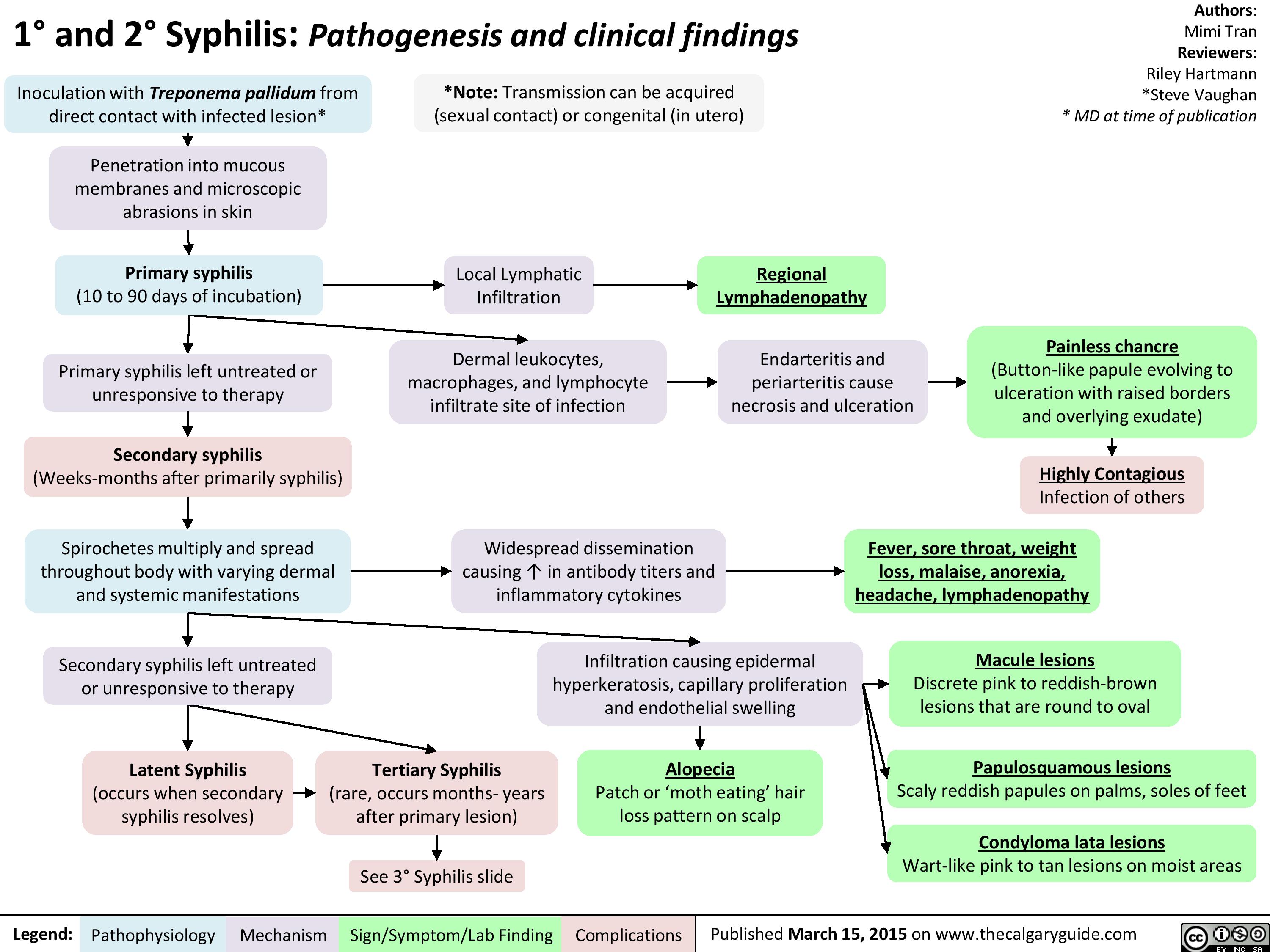
1-and-2-syphilis-pathogenesis-and-clinical-findings
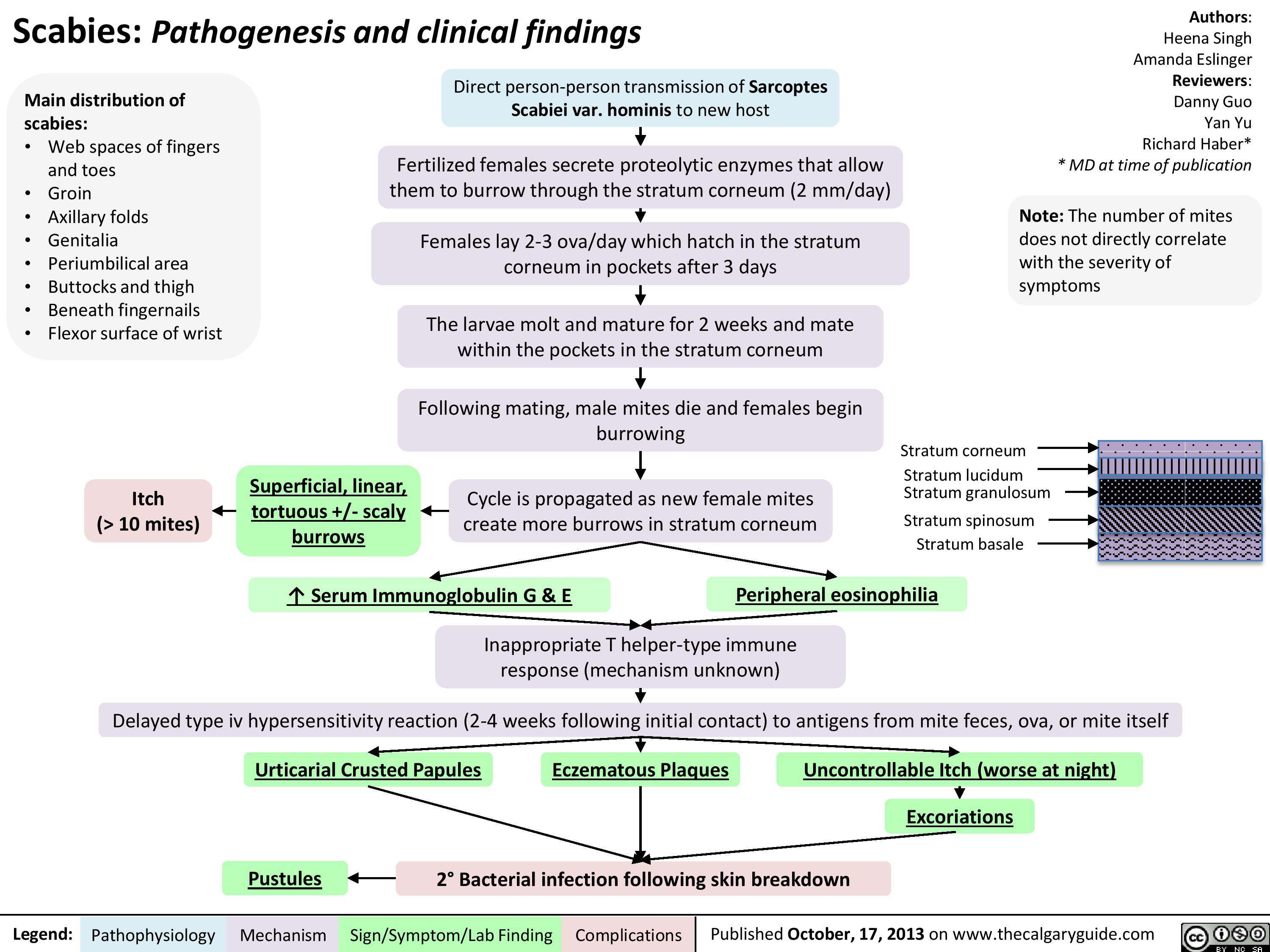
Scabies
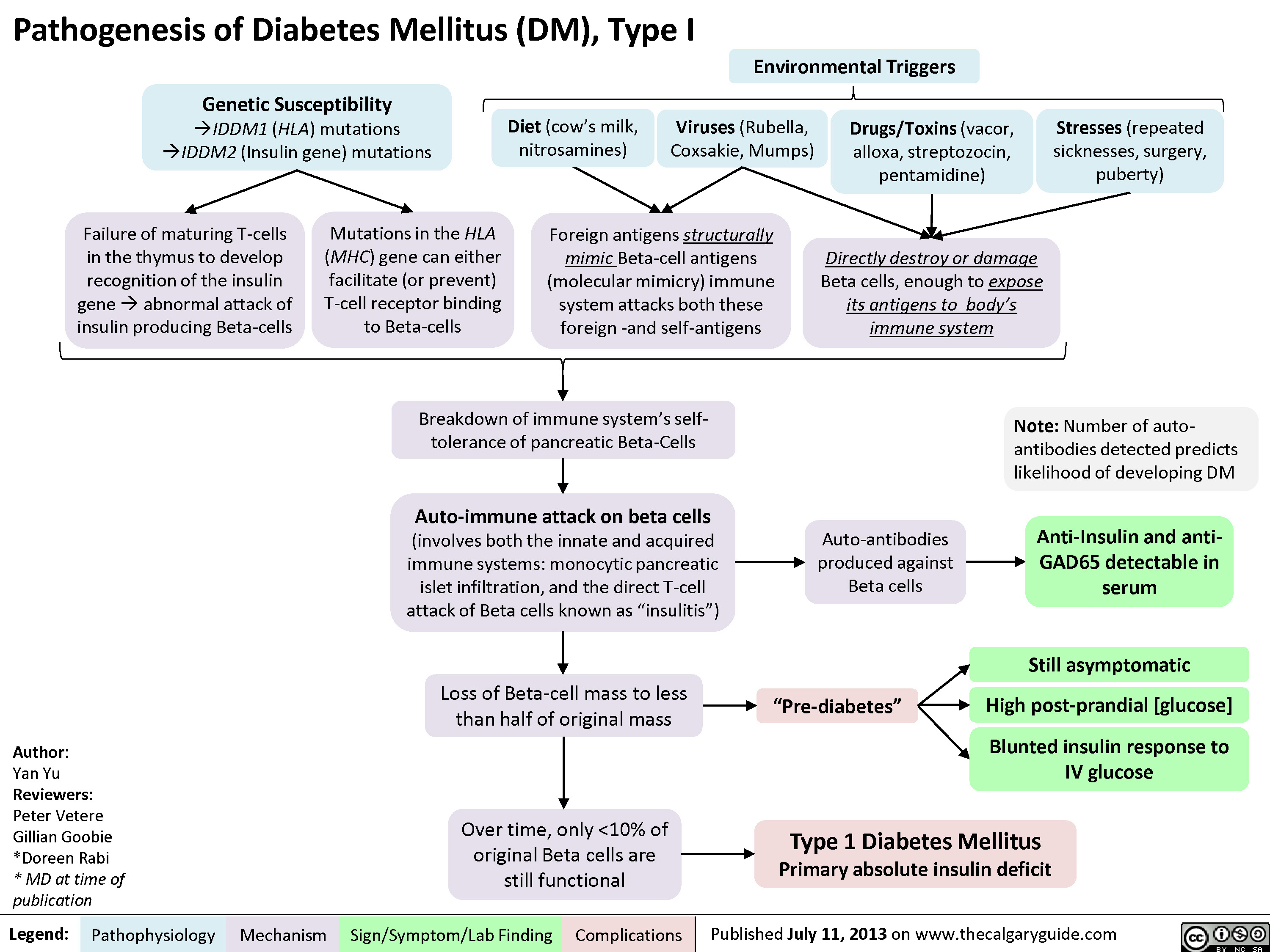
DM I pathogenesis
Pathogenesis of Diabetes mellitus DM), Type II

Diabetic Ketoacidosis

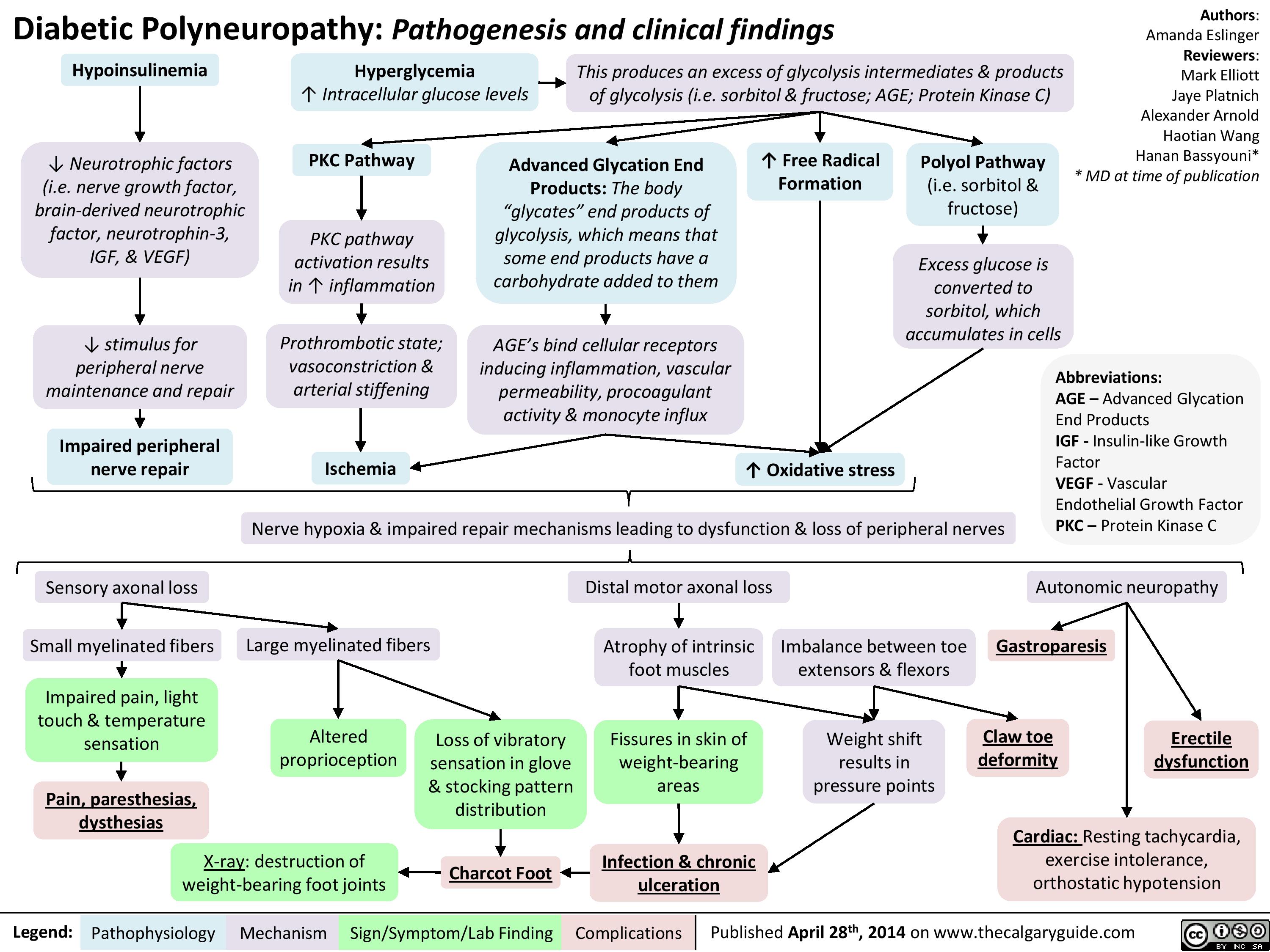
Diabetic Polyneuropathy
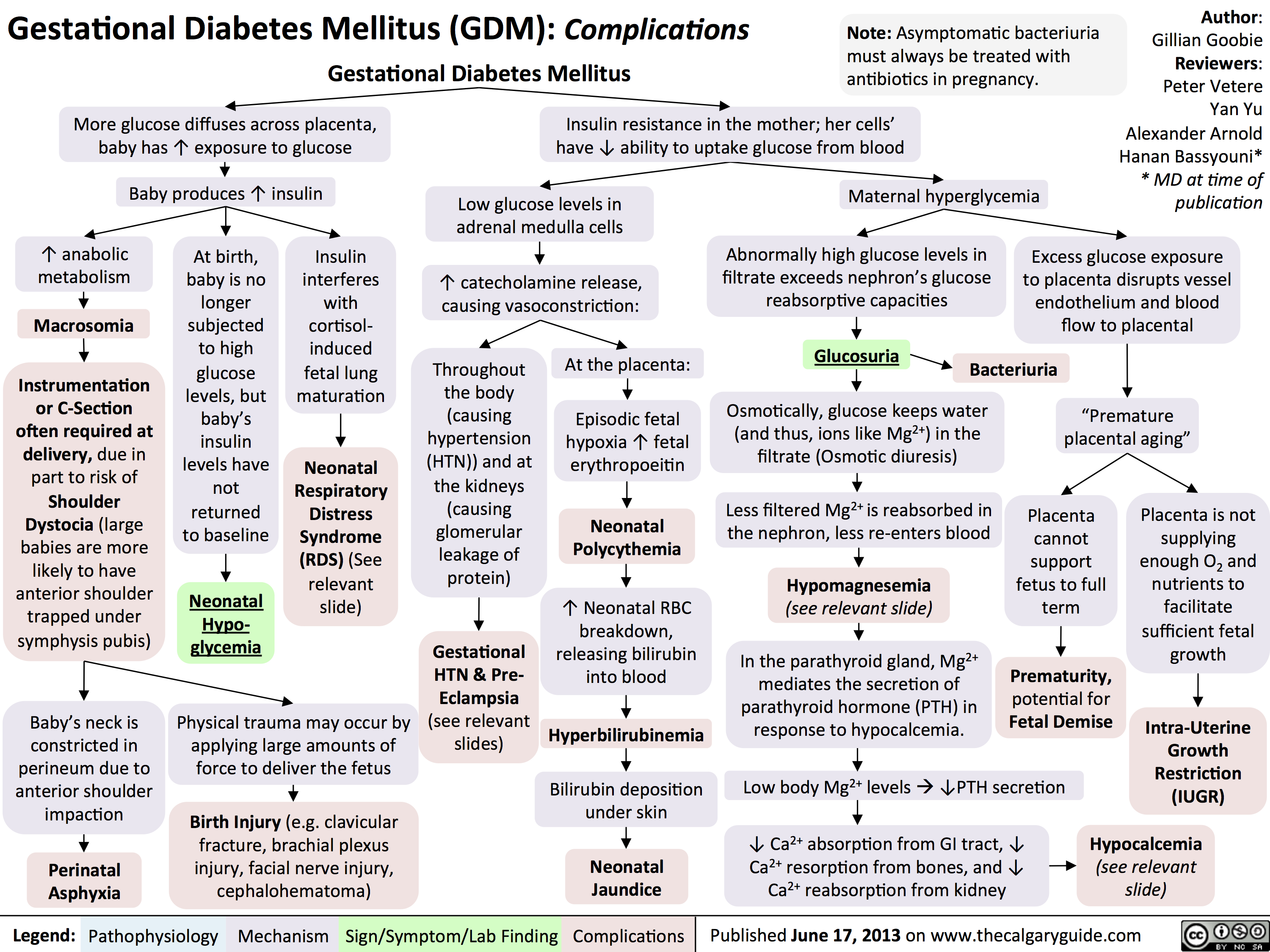
GDM Complications
Hypoglycemia - Pathogenesis

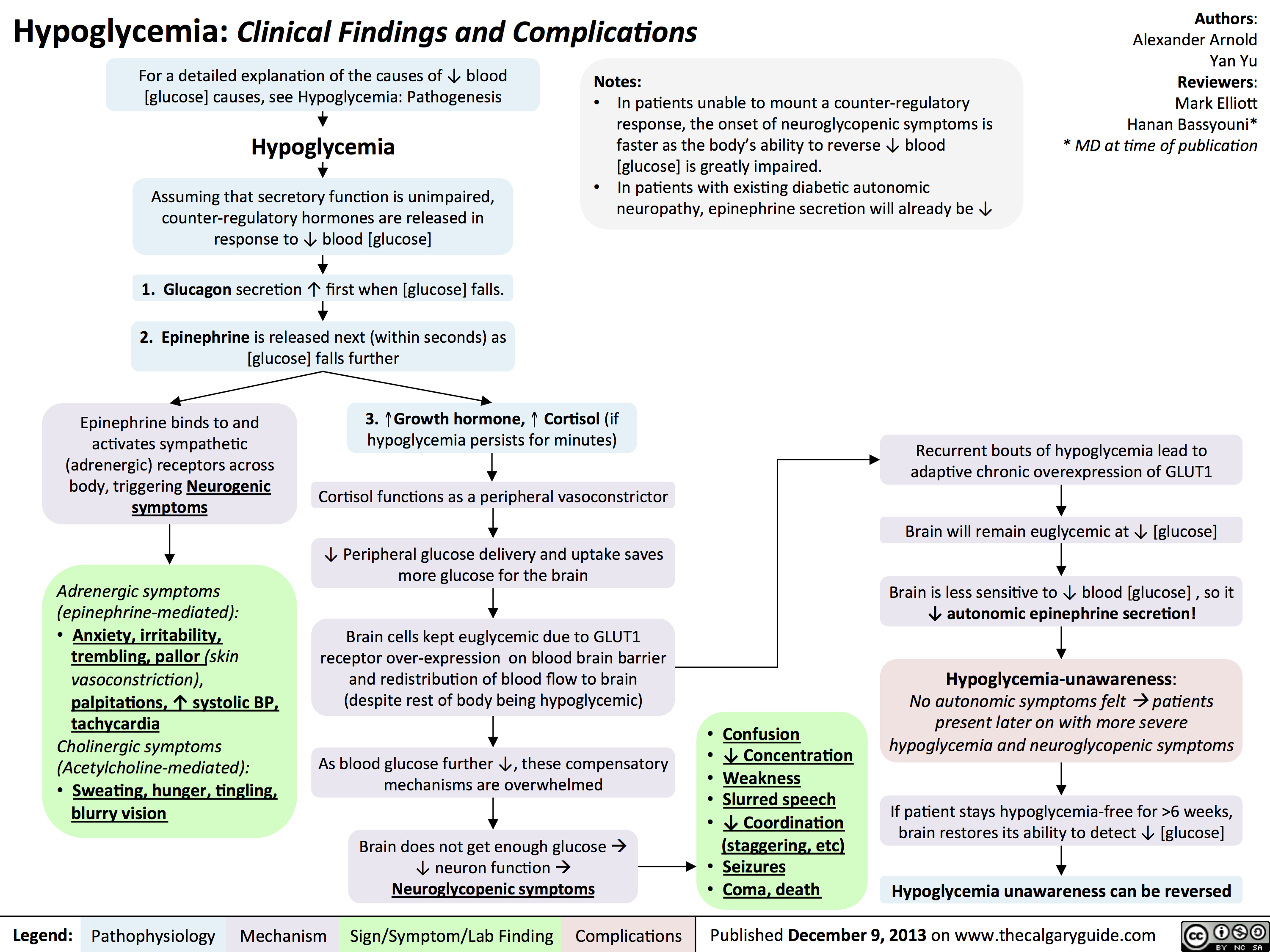
Hypoglycemia - Clinical Findings and Complications
Diabetic Hypoglycemia
![Yu, Yan - Diabetic Hypoglycemia - Clinical Findings - FINAL.pptx
? Epinephrine(Released within seconds as [glucose] falls further) Growth hormone, ? Cortisol (if hypoglycemia persists for minutes)Glucagon should ? when [glucose] falls. But here, glucagon release is inhibited by 1) diabetic auto-immune destruction of Alpha cells & 2) the high insulin.43210Plasma Glucose concentration (mmol/L)Liver should ? glycogenolysis & gluconeogenesisPeripheral vaso-constrictionPlasma [glucose] stays lowActivation of sympathetic (adrenergic) receptors across body, triggering Neurogenic symptomsPlasma [glucose] ?Excess subcutaneous insulin or insulin-secretagogue ?? [insulin] in the bloodOver time: [insulin] in the DM patient depends only on how much was injected or how much secretagogue was consumed; not on the body's physiological state.[Insulin] stays high in excessively-treated DM patientsPlasma [glucose] normally ?, but...High insulin transports plasma glucose into cells!In pts with existing diabetic autonomic neuropathy, epi-nephrine secretion will already be ?Brain does not get enough glucose, ? neuron function ? Neuroglycopenic symptomsTx: glucose intake![Glucose] returns to normalIf no glucose intake:Hypoglycemia-unawareness: No autonomic Sx felt so hypoglycemia not treated early ? pts present later on with more severe hypoglycemia and neuroglycopenic sxBrain cells kept chronically euglycemic due to GLUT1 receptor over-expression (despite rest of body being hypoglycemic)With many hypoglycemic events over time:Brain feels no need to ? glucose, so it ? autonomic epinephrine secretion!This is the normal sequence of hormone responses to ?ing plasma glucose levels.But this normal hormonal response will be blunted over time if there is 1) continued hypoglycemia dampening the sympathetic nervous system, and 2) long-standing diabetic neuropathy! (To be explained later in this flow chart)Abbreviations: [ ] = concentrationTx = TreatmentDM = Diabetes mellitusDiabetic Hypoglycemia: Pathogenesis and Clinical FindingsConfusionCan't concentrateWeaknessSlurred speech? coordination (staggering, etc)SeizuresComa, deathAdrenergic symptoms (epinephrine-mediated):Anxiety, irritability, trembling, pallor (skin vasoconstriction), palpitations, ? systolic BP, tachycardia Cholinergic symptoms(Acetylcholine-mediated):Sweating, hunger, tingling, blurry visionNote: In pts w/out DM, endogenous insulin secretion normally stops when blood [glucose] drops to <4mmol/LAuthor: Yan YuReviewers: Peter Vetere, Gillian Goobie, Hanan Bassyouni** MD at time of publicationLegend:Published June 14, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsMany hypoglycemic events over time blunt epinephrine secretion further.Hypoglycemia unawareness can be reversedIf pt stays hypoglycemia-free for >6 weeks, brain restores its ability to detect low glucose levels? peripheral glucose delivery and uptake (saving more glucose for the brain)Lack of glucagon effect reinforces hypoglycemia
124 kB / 361 words](http://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/Diabetic-Hypoglycemia-Clinical-Findings.jpg "Yu, Yan - Diabetic Hypoglycemia - Clinical Findings - FINAL.pptx
? Epinephrine(Released within seconds as [glucose] falls further) Growth hormone, ? Cortisol (if hypoglycemia persists for minutes)Glucagon should ? when [glucose] falls. But here, glucagon release is inhibited by 1) diabetic auto-immune destruction of Alpha cells & 2) the high insulin.43210Plasma Glucose concentration (mmol/L)Liver should ? glycogenolysis & gluconeogenesisPeripheral vaso-constrictionPlasma [glucose] stays lowActivation of sympathetic (adrenergic) receptors across body, triggering Neurogenic symptomsPlasma [glucose] ?Excess subcutaneous insulin or insulin-secretagogue ?? [insulin] in the bloodOver time: [insulin] in the DM patient depends only on how much was injected or how much secretagogue was consumed; not on the body's physiological state.[Insulin] stays high in excessively-treated DM patientsPlasma [glucose] normally ?, but...High insulin transports plasma glucose into cells!In pts with existing diabetic autonomic neuropathy, epi-nephrine secretion will already be ?Brain does not get enough glucose, ? neuron function ? Neuroglycopenic symptomsTx: glucose intake![Glucose] returns to normalIf no glucose intake:Hypoglycemia-unawareness: No autonomic Sx felt so hypoglycemia not treated early ? pts present later on with more severe hypoglycemia and neuroglycopenic sxBrain cells kept chronically euglycemic due to GLUT1 receptor over-expression (despite rest of body being hypoglycemic)With many hypoglycemic events over time:Brain feels no need to ? glucose, so it ? autonomic epinephrine secretion!This is the normal sequence of hormone responses to ?ing plasma glucose levels.But this normal hormonal response will be blunted over time if there is 1) continued hypoglycemia dampening the sympathetic nervous system, and 2) long-standing diabetic neuropathy! (To be explained later in this flow chart)Abbreviations: [ ] = concentrationTx = TreatmentDM = Diabetes mellitusDiabetic Hypoglycemia: Pathogenesis and Clinical FindingsConfusionCan't concentrateWeaknessSlurred speech? coordination (staggering, etc)SeizuresComa, deathAdrenergic symptoms (epinephrine-mediated):Anxiety, irritability, trembling, pallor (skin vasoconstriction), palpitations, ? systolic BP, tachycardia Cholinergic symptoms(Acetylcholine-mediated):Sweating, hunger, tingling, blurry visionNote: In pts w/out DM, endogenous insulin secretion normally stops when blood [glucose] drops to <4mmol/LAuthor: Yan YuReviewers: Peter Vetere, Gillian Goobie, Hanan Bassyouni** MD at time of publicationLegend:Published June 14, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsMany hypoglycemic events over time blunt epinephrine secretion further.Hypoglycemia unawareness can be reversedIf pt stays hypoglycemia-free for >6 weeks, brain restores its ability to detect low glucose levels? peripheral glucose delivery and uptake (saving more glucose for the brain)Lack of glucagon effect reinforces hypoglycemia
124 kB / 361 words")
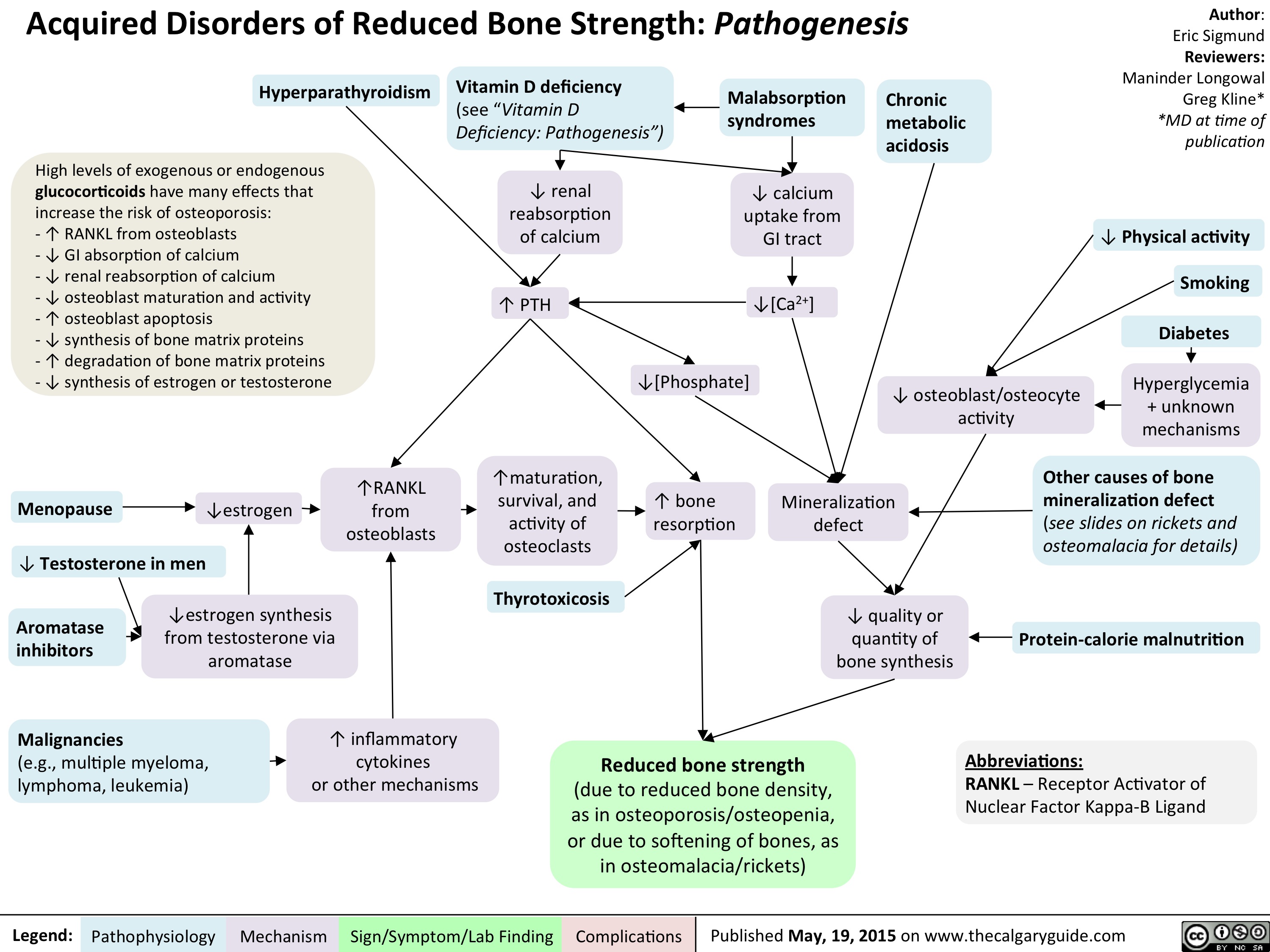
Acquired Disorders of Reduced Bone Strength - Pathogenesis
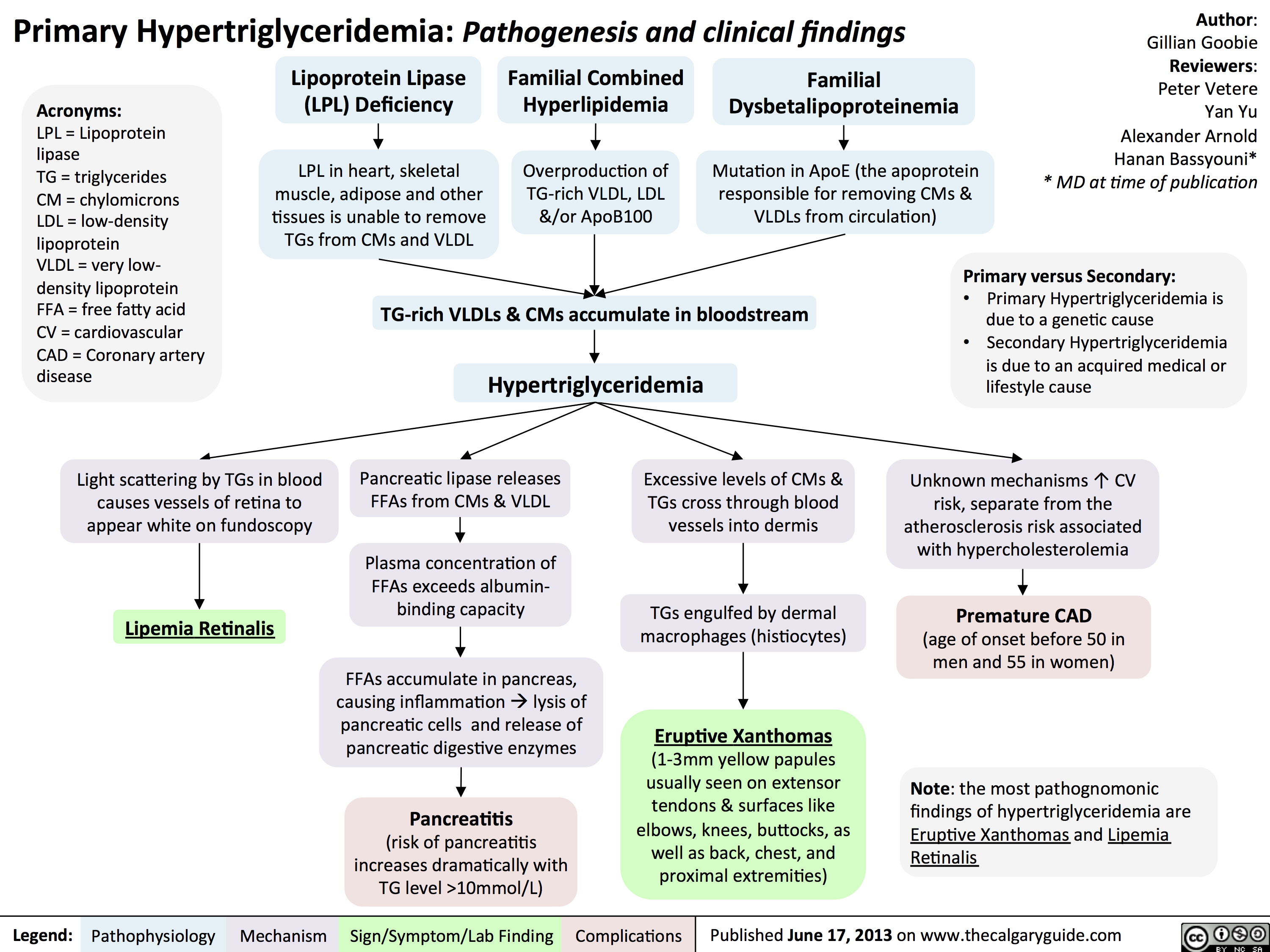
Primary Hypertriglyceridemia
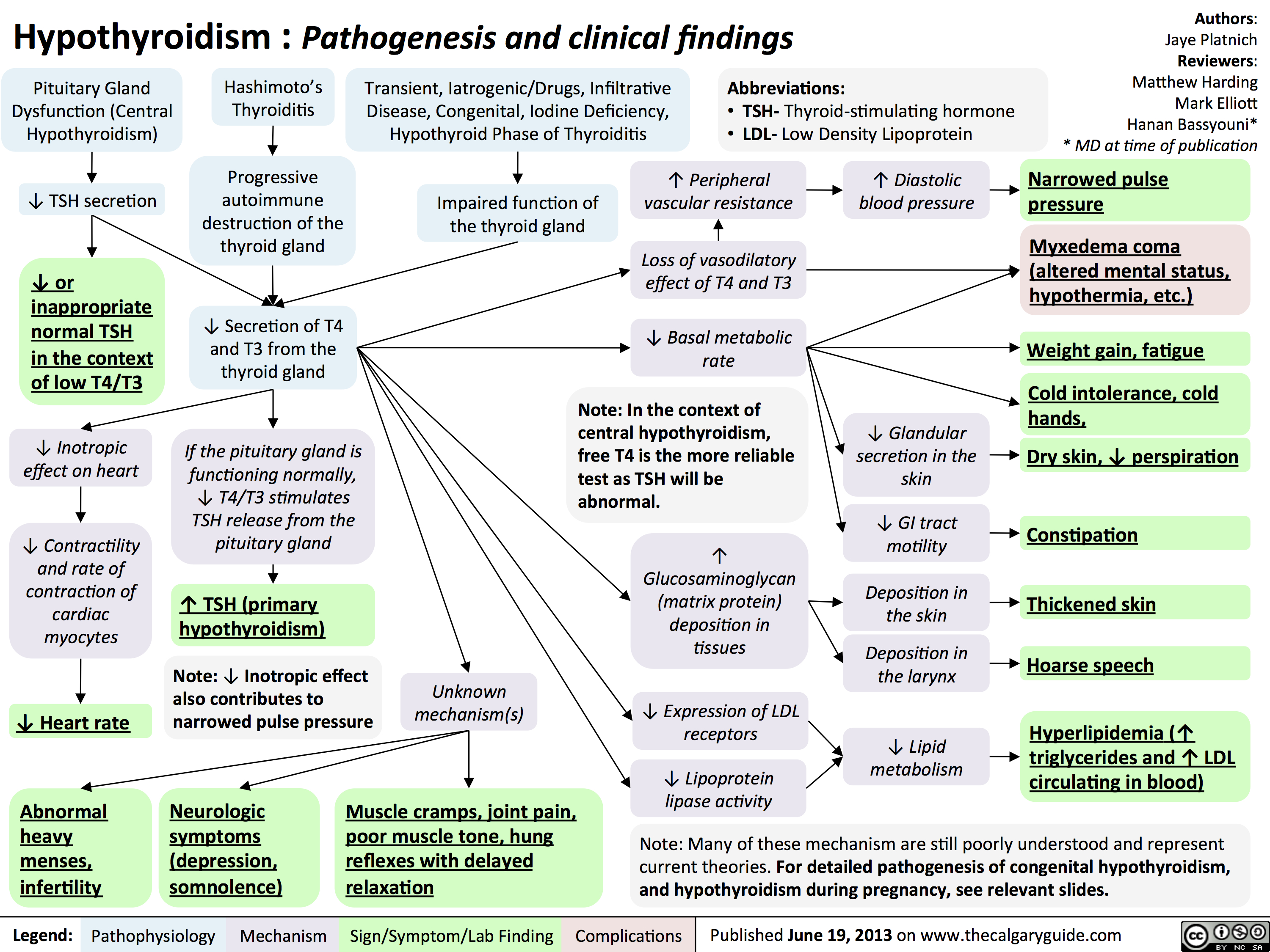
Hypothyroidism
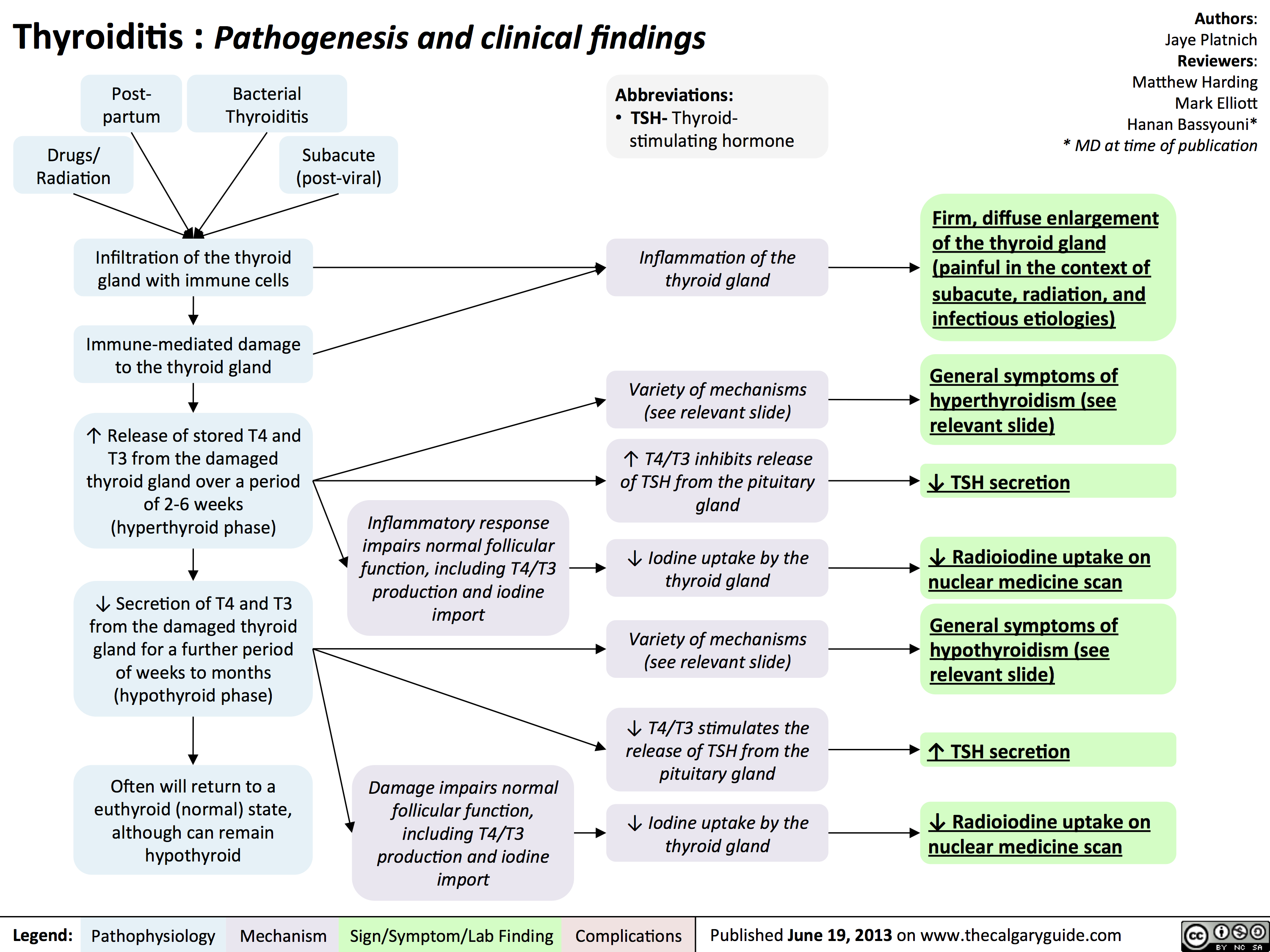
Hashimoto
Thyroiditis
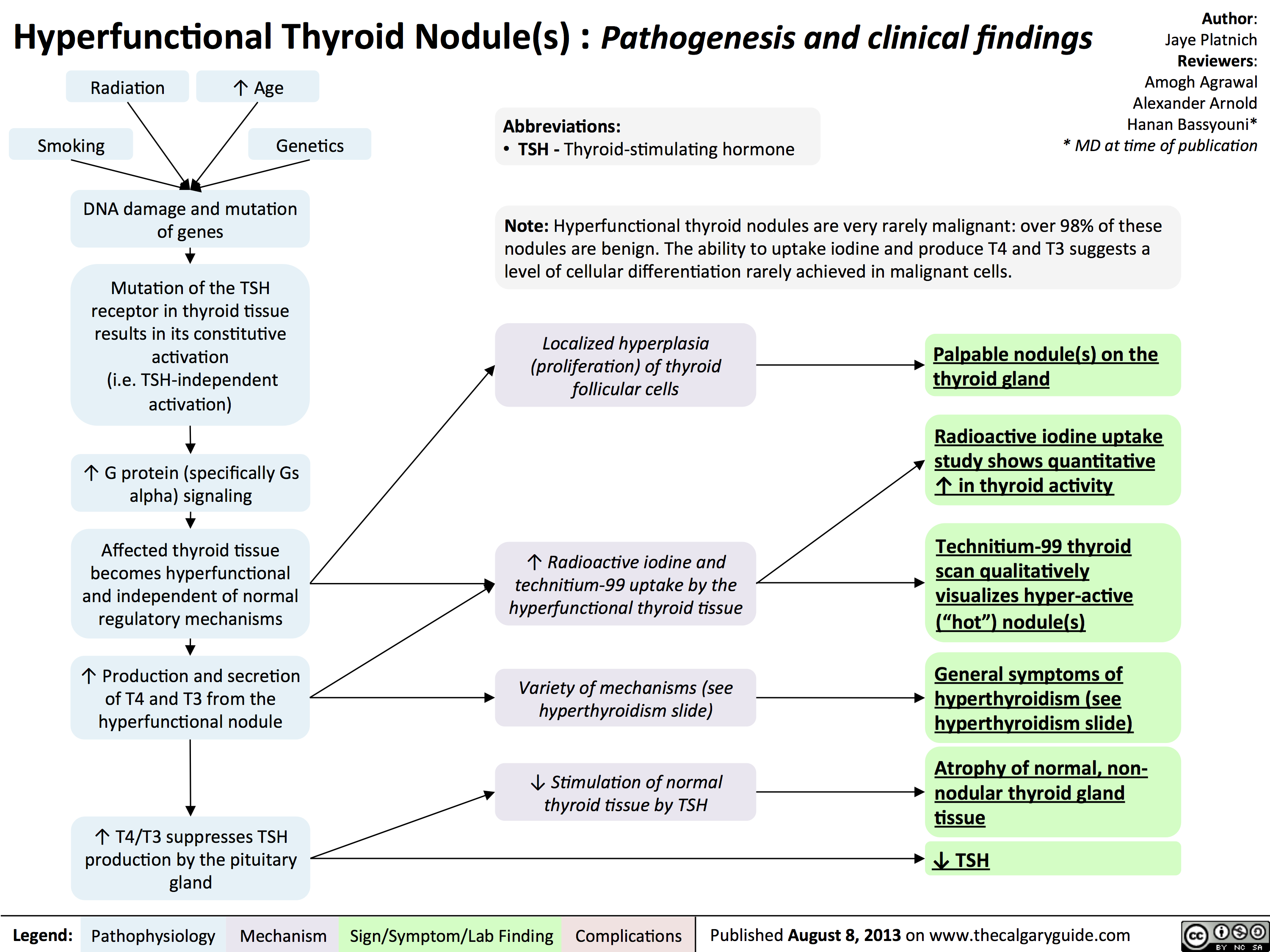
Hyperfunctional
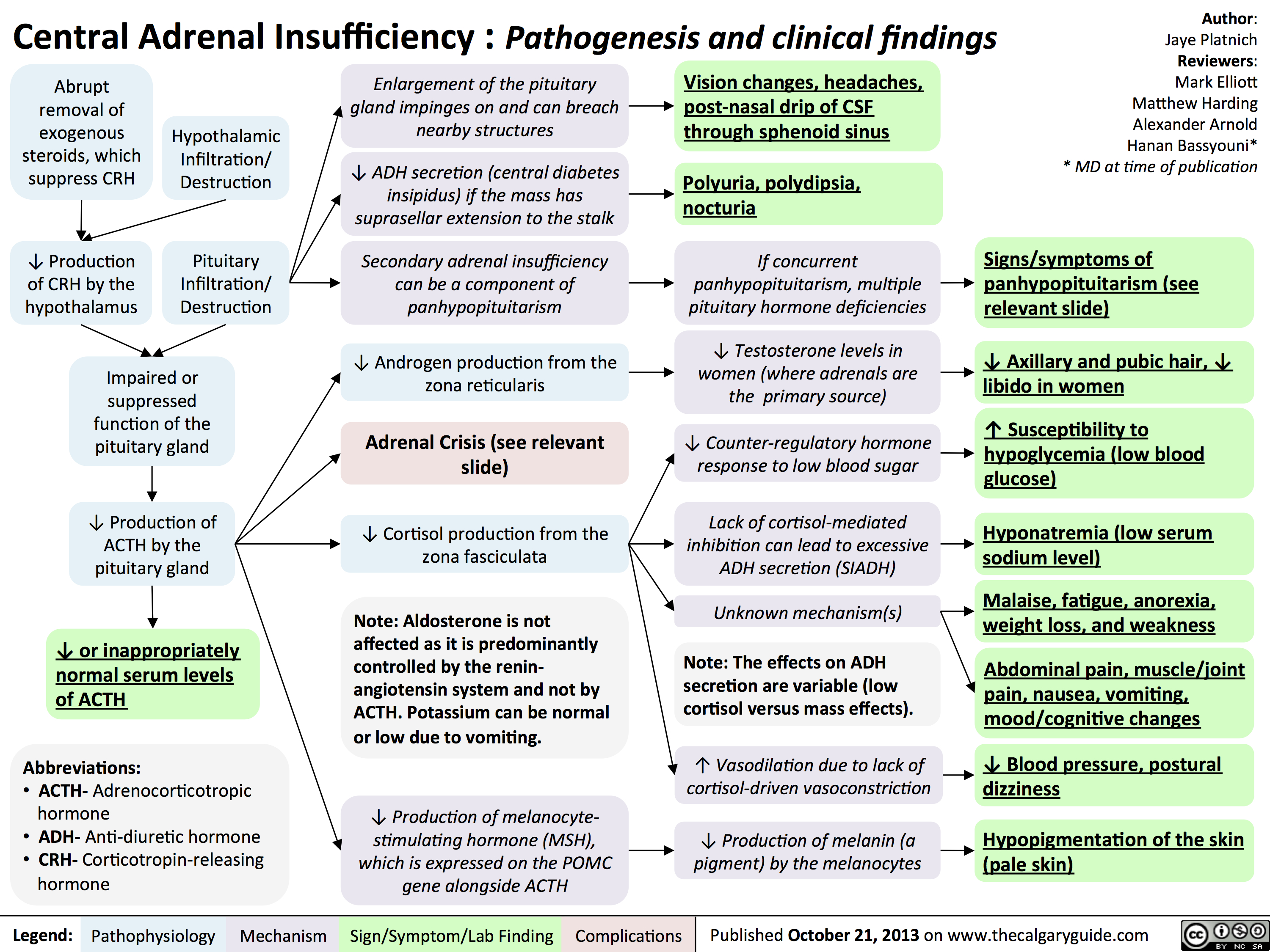
Central Adrenal Insufficiency - Pathogenesis and Clinical Findings
Clinical Findings of Androgen Deficiency
![Yu, Yan - Androgen Deficiency - FINAL.pptx
Hypogonadism in Males:Clinical Findings of Androgen Deficiency? secretion volume from seminal vesicle and prostateAuthor: Yan YuReviewers:Peter VetereGillian GoobieHanan Bassyouni** MD at time of publicationLegend:Published June 18, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplications? effect of testosterone on the brain? Libido(sensitive, but less specific)? [testosterone] : [estrogen] ratio at the male breast? ejaculate volume(a sensitive and specific sign)Gynecomastia (palpable breast tissue, not fat, directly under nipple)Fatigue,low mood, irrtabilityHot flashes, sweats(Can be nocturnal; occur only when hypogonadism is severe)Vasomotor neural response of unknown causeFewer spontaneous erections (i.e. in the morning)Lack of androgens (i.e. testosterone, DHT) in men past the age of pubertyIn advanced stages of the disease, after years of hypogonadism:(thus, less commonly seen)Low Bone Mass Density (BMD)Less testosterone to be converted into estrogen in bone? muscle bulk and strengthSmall, soft testicles(<4cm long on orchidometer)Lack of hormones to stimulate and maintain testicular hyperplasia/growthLoss of androgenic hair (on face, midline, and pubic area)Vertebral fracture (height loss), or other fragility fracturesIf sexual development is incomplete from puberty:Note: These clinical findings apply to many disorders, including:-Andropause-Hypopituitarism (suspect if other hormone abnormalities & Sx of mass lesion like visual field loss, diplopia, and headache exist)-Testicular Failure (if Hx of chemo, radiation, excess alcohol, and chronic liver disease)-Klinefelter's (if assoc. tall and eunuchoid stature, breast enlargement and cognitive deficiency - XXY)-Kallman's (if assoc. anosmia, and tall/eunuchoid stature)-Drugs (e.g. ketoconazole, anabolic steroids, spironolactone, digoxin, marijuana)Testosterone's inhibitory effect on estrogen is not enough to prevent breast growthDeficiency in testosterone during puberty delays fusion of epiphysesTall, eunuchoid statureNote: any disease involving an increase in aromatase activity (hyperthyroidism, cirrhosis, HCG-secreting tumors) will also cause relative estrogen excess & subsequent gynecomastia.
111 kB / 272 words](http://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/Clinical-Findings-of-Androgen-Deficiency.jpg "Yu, Yan - Androgen Deficiency - FINAL.pptx
Hypogonadism in Males:Clinical Findings of Androgen Deficiency? secretion volume from seminal vesicle and prostateAuthor: Yan YuReviewers:Peter VetereGillian GoobieHanan Bassyouni** MD at time of publicationLegend:Published June 18, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplications? effect of testosterone on the brain? Libido(sensitive, but less specific)? [testosterone] : [estrogen] ratio at the male breast? ejaculate volume(a sensitive and specific sign)Gynecomastia (palpable breast tissue, not fat, directly under nipple)Fatigue,low mood, irrtabilityHot flashes, sweats(Can be nocturnal; occur only when hypogonadism is severe)Vasomotor neural response of unknown causeFewer spontaneous erections (i.e. in the morning)Lack of androgens (i.e. testosterone, DHT) in men past the age of pubertyIn advanced stages of the disease, after years of hypogonadism:(thus, less commonly seen)Low Bone Mass Density (BMD)Less testosterone to be converted into estrogen in bone? muscle bulk and strengthSmall, soft testicles(<4cm long on orchidometer)Lack of hormones to stimulate and maintain testicular hyperplasia/growthLoss of androgenic hair (on face, midline, and pubic area)Vertebral fracture (height loss), or other fragility fracturesIf sexual development is incomplete from puberty:Note: These clinical findings apply to many disorders, including:-Andropause-Hypopituitarism (suspect if other hormone abnormalities & Sx of mass lesion like visual field loss, diplopia, and headache exist)-Testicular Failure (if Hx of chemo, radiation, excess alcohol, and chronic liver disease)-Klinefelter's (if assoc. tall and eunuchoid stature, breast enlargement and cognitive deficiency - XXY)-Kallman's (if assoc. anosmia, and tall/eunuchoid stature)-Drugs (e.g. ketoconazole, anabolic steroids, spironolactone, digoxin, marijuana)Testosterone's inhibitory effect on estrogen is not enough to prevent breast growthDeficiency in testosterone during puberty delays fusion of epiphysesTall, eunuchoid statureNote: any disease involving an increase in aromatase activity (hyperthyroidism, cirrhosis, HCG-secreting tumors) will also cause relative estrogen excess & subsequent gynecomastia.
111 kB / 272 words")
Hypocalcemia - Clinical Findings
![Yu, Yan - Hypocalcemia - Clinical Findings - FINAL.pptx
Hypocalcemia: Clinical FindingsAuthor: Yan YuReviewers:David WaldnerSean SpenceGreg Kline** MD at time of publicationLegend:Published May 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsHypocalcemia(serum [Ca2+] <2.1mmol/L)Altered sensory ability of peripheral nervesLess Ca2+ outside cells, with no change in + charges inside cellsPeripheral paraesthesia? Neuronal](http://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/Hypocalcemia-Clinical-Findings.jpg "Yu, Yan - Hypocalcemia - Clinical Findings - FINAL.pptx
Hypocalcemia: Clinical FindingsAuthor: Yan YuReviewers:David WaldnerSean SpenceGreg Kline** MD at time of publicationLegend:Published May 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsHypocalcemia(serum [Ca2+] <2.1mmol/L)Altered sensory ability of peripheral nervesLess Ca2+ outside cells, with no change in + charges inside cellsPeripheral paraesthesia? Neuronal")
Hypercalcemia - Clinical Findings
![Yu, Yan - Hypercalcemia - Clinical Findings - FINAL.pptx
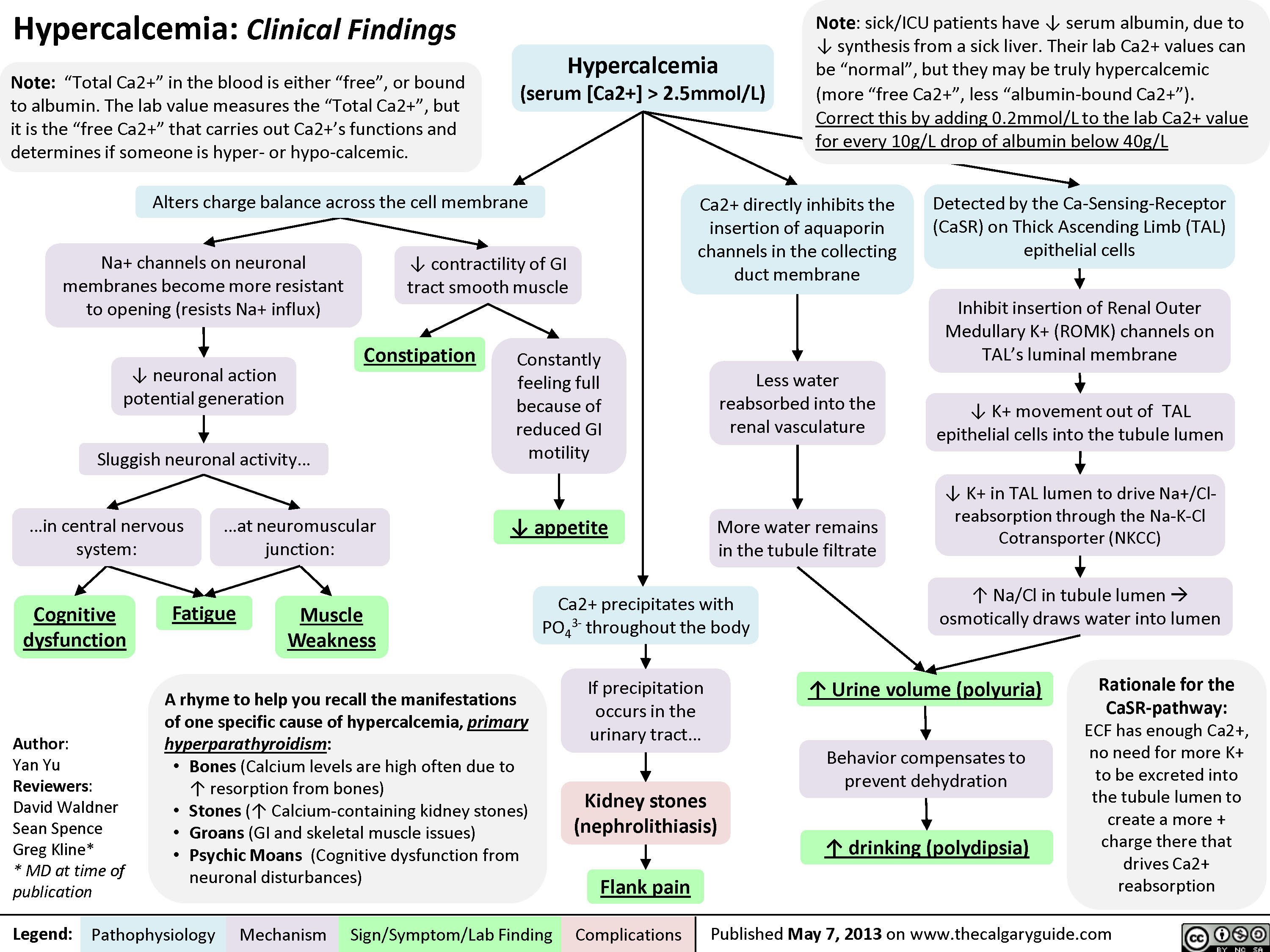
Hypercalcemia: Clinical FindingsAuthor: Yan YuReviewers:David WaldnerSean SpenceGreg Kline** MD at time of publicationLegend:Published May 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsHypercalcemia(serum [Ca2+] > 2.5mmol/L)Na+ channels on neuronal membranes become more resistant to opening (resists Na+ influx)Cognitive dysfunctionIf precipitation occurs in the urinary tract...Fatigue? contractility of GI tract smooth muscle? K+ movement out of TAL epithelial cells into the tubule lumen Alters charge balance across the cell membraneCa2+ precipitates with PO43- throughout the bodyDetected by the Ca-Sensing-Receptor (CaSR) on Thick Ascending Limb (TAL) epithelial cells? neuronal action potential generationSluggish neuronal activity...? appetiteConstipationFlank painInhibit insertion of Renal Outer Medullary K+ (ROMK) channels on TAL's luminal membrane? K+ in TAL lumen to drive Na+/Cl- reabsorption through the Na-K-Cl Cotransporter (NKCC)? Na/Cl in tubule lumen ? osmotically draws water into lumen? drinking (polydipsia)? Urine volume (polyuria)Rationale for the CaSR-pathway: ECF has enough Ca2+, no need for more K+ to be excreted into the tubule lumen to create a more + charge there that drives Ca2+ reabsorptionBehavior compensates to prevent dehydrationKidney stones (nephrolithiasis)Constantly feeling full because of reduced GI motilityCa2+ directly inhibits the insertion of aquaporin channels in the collecting duct membraneLess water reabsorbed into the renal vasculatureMore water remains in the tubule filtrateMuscle Weakness...in central nervous system:...at neuromuscular junction:A rhyme to help you recall the manifestations of one specific cause of hypercalcemia, primary hyperparathyroidism:Bones (Calcium levels are high often due to ? resorption from bones)Stones (? Calcium-containing kidney stones)Groans (GI and skeletal muscle issues) Psychic Moans (Cognitive dysfunction from neuronal disturbances)Note: sick/ICU patients have ? serum albumin, due to ? synthesis from a sick liver. Their lab Ca2+ values can be](http://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/Hypercalcemia-Clinical-Findings.jpg "Yu, Yan - Hypercalcemia - Clinical Findings - FINAL.pptx
Hypercalcemia: Clinical FindingsAuthor: Yan YuReviewers:David WaldnerSean SpenceGreg Kline** MD at time of publicationLegend:Published May 7, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsHypercalcemia(serum [Ca2+] > 2.5mmol/L)Na+ channels on neuronal membranes become more resistant to opening (resists Na+ influx)Cognitive dysfunctionIf precipitation occurs in the urinary tract...Fatigue? contractility of GI tract smooth muscle? K+ movement out of TAL epithelial cells into the tubule lumen Alters charge balance across the cell membraneCa2+ precipitates with PO43- throughout the bodyDetected by the Ca-Sensing-Receptor (CaSR) on Thick Ascending Limb (TAL) epithelial cells? neuronal action potential generationSluggish neuronal activity...? appetiteConstipationFlank painInhibit insertion of Renal Outer Medullary K+ (ROMK) channels on TAL's luminal membrane? K+ in TAL lumen to drive Na+/Cl- reabsorption through the Na-K-Cl Cotransporter (NKCC)? Na/Cl in tubule lumen ? osmotically draws water into lumen? drinking (polydipsia)? Urine volume (polyuria)Rationale for the CaSR-pathway: ECF has enough Ca2+, no need for more K+ to be excreted into the tubule lumen to create a more + charge there that drives Ca2+ reabsorptionBehavior compensates to prevent dehydrationKidney stones (nephrolithiasis)Constantly feeling full because of reduced GI motilityCa2+ directly inhibits the insertion of aquaporin channels in the collecting duct membraneLess water reabsorbed into the renal vasculatureMore water remains in the tubule filtrateMuscle Weakness...in central nervous system:...at neuromuscular junction:A rhyme to help you recall the manifestations of one specific cause of hypercalcemia, primary hyperparathyroidism:Bones (Calcium levels are high often due to ? resorption from bones)Stones (? Calcium-containing kidney stones)Groans (GI and skeletal muscle issues) Psychic Moans (Cognitive dysfunction from neuronal disturbances)Note: sick/ICU patients have ? serum albumin, due to ? synthesis from a sick liver. Their lab Ca2+ values can be")
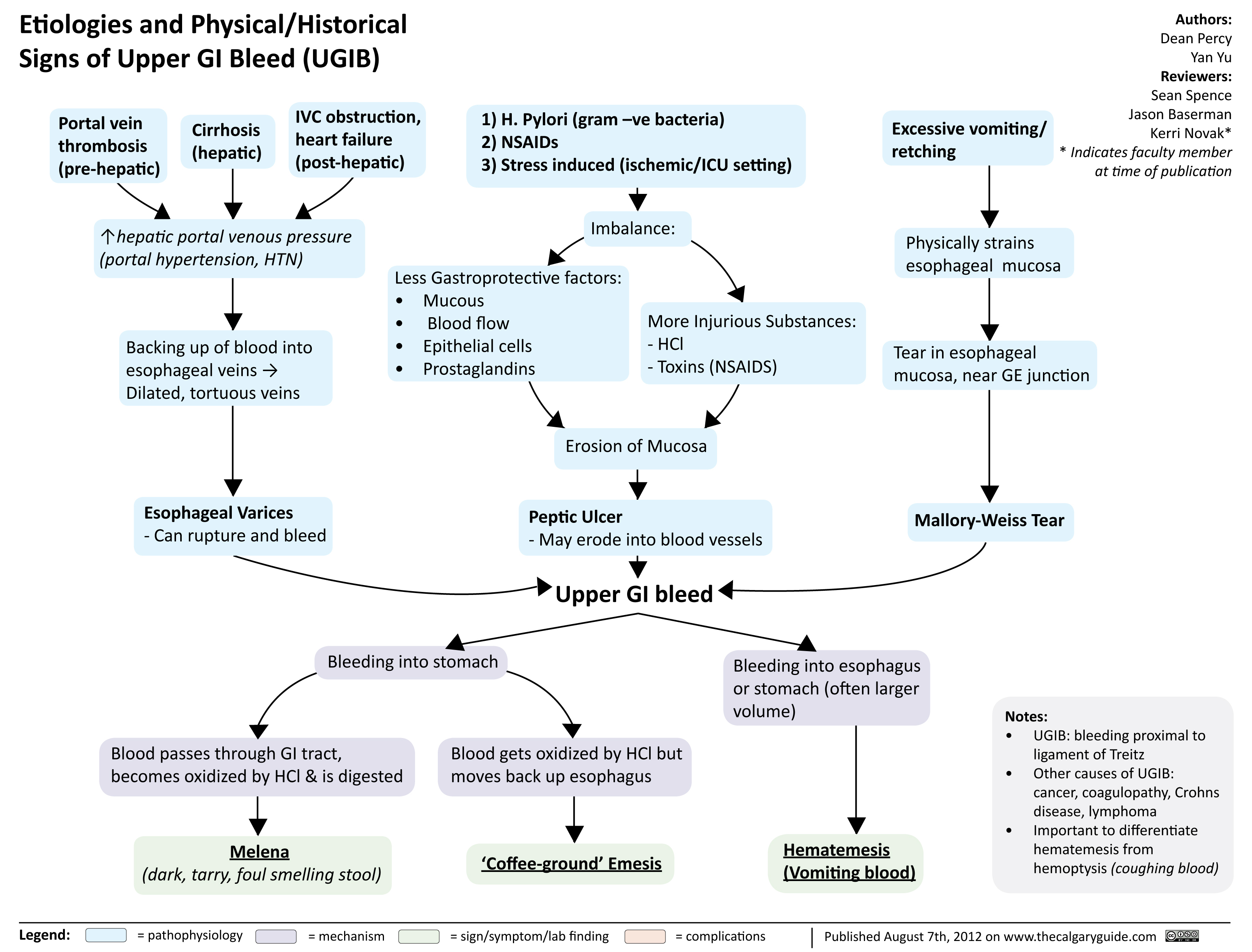
Etiologies and Physical Historical Signs of Upper GI Bleed
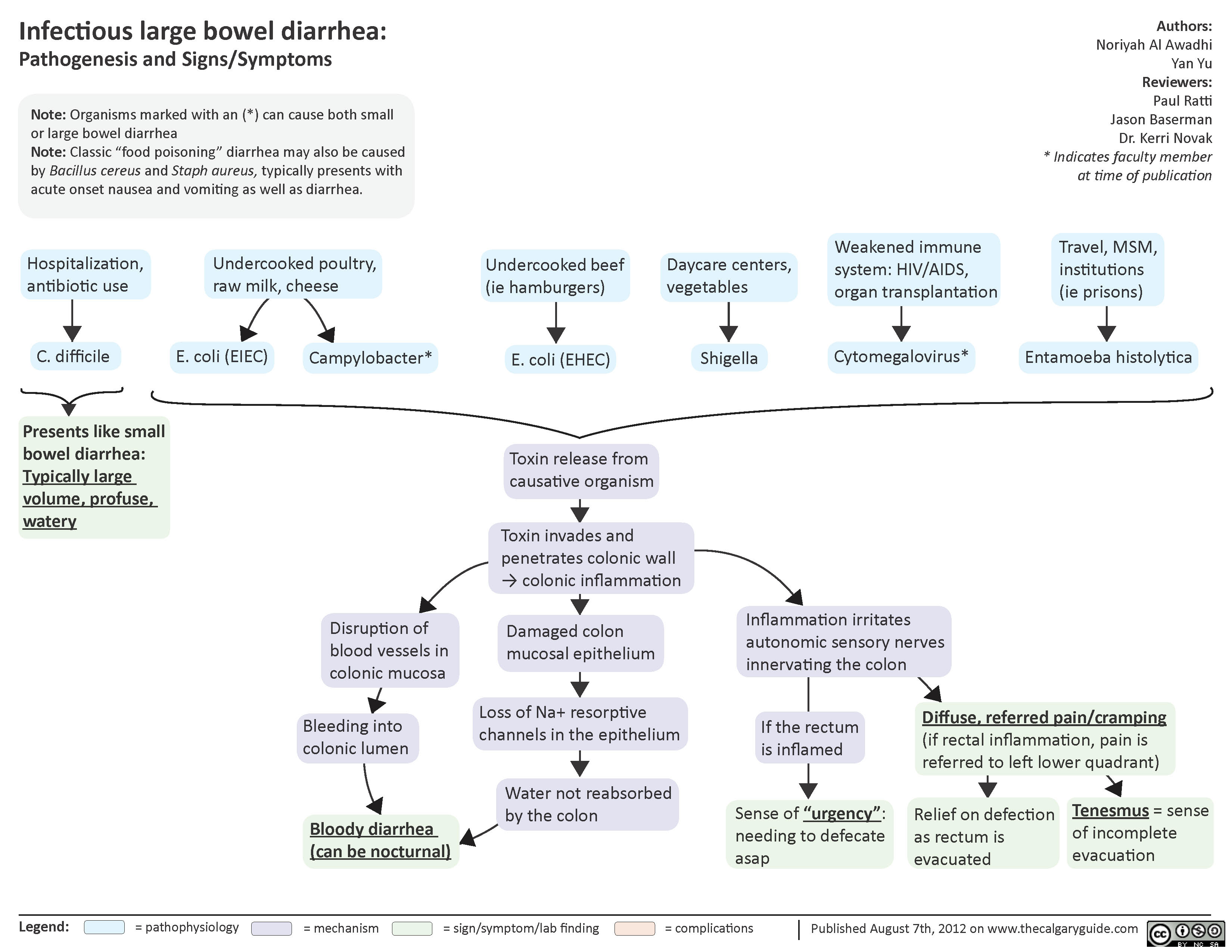
Infectious Large Bowel Diarrhea
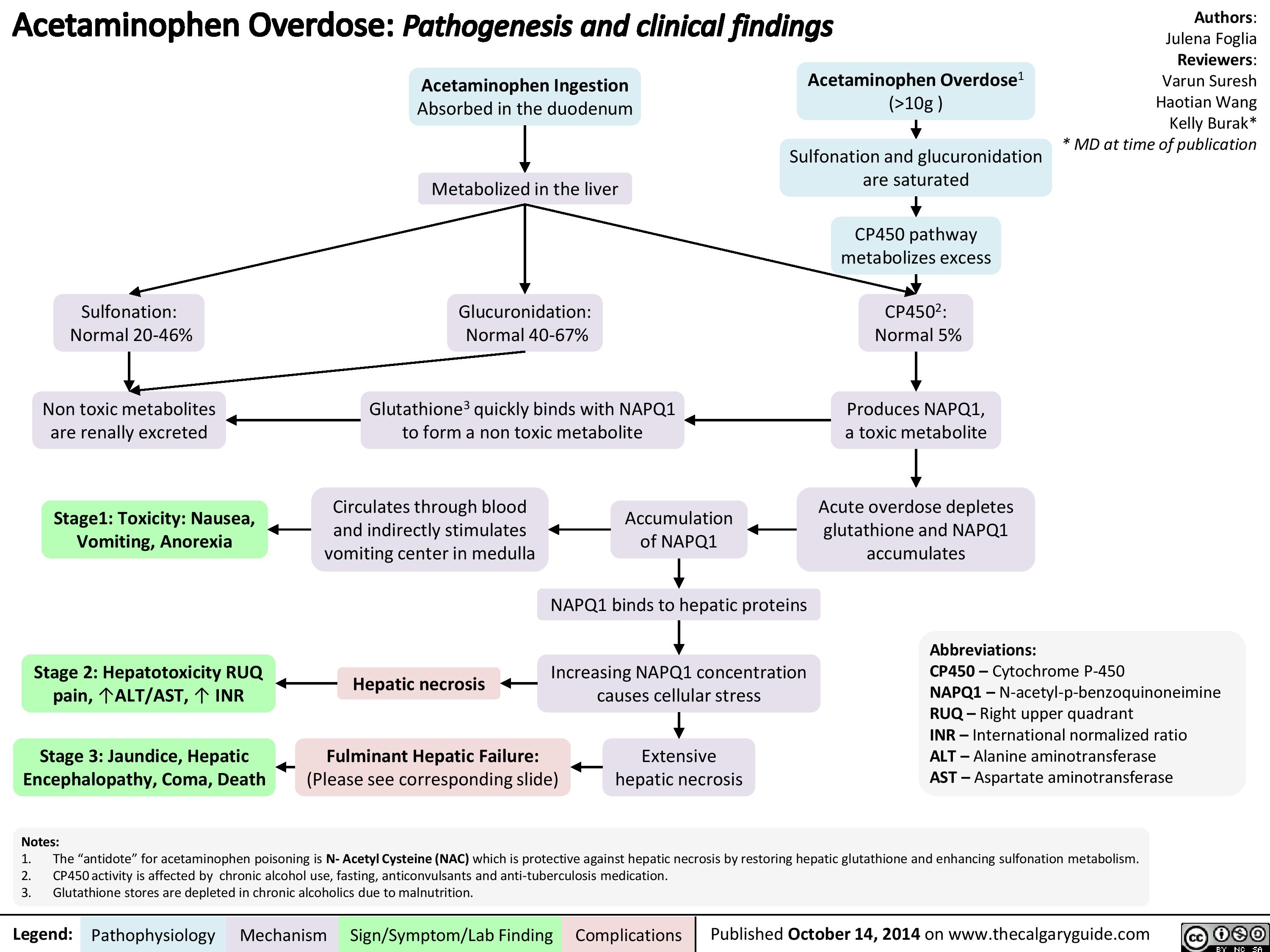
Acetaminophen Overdose
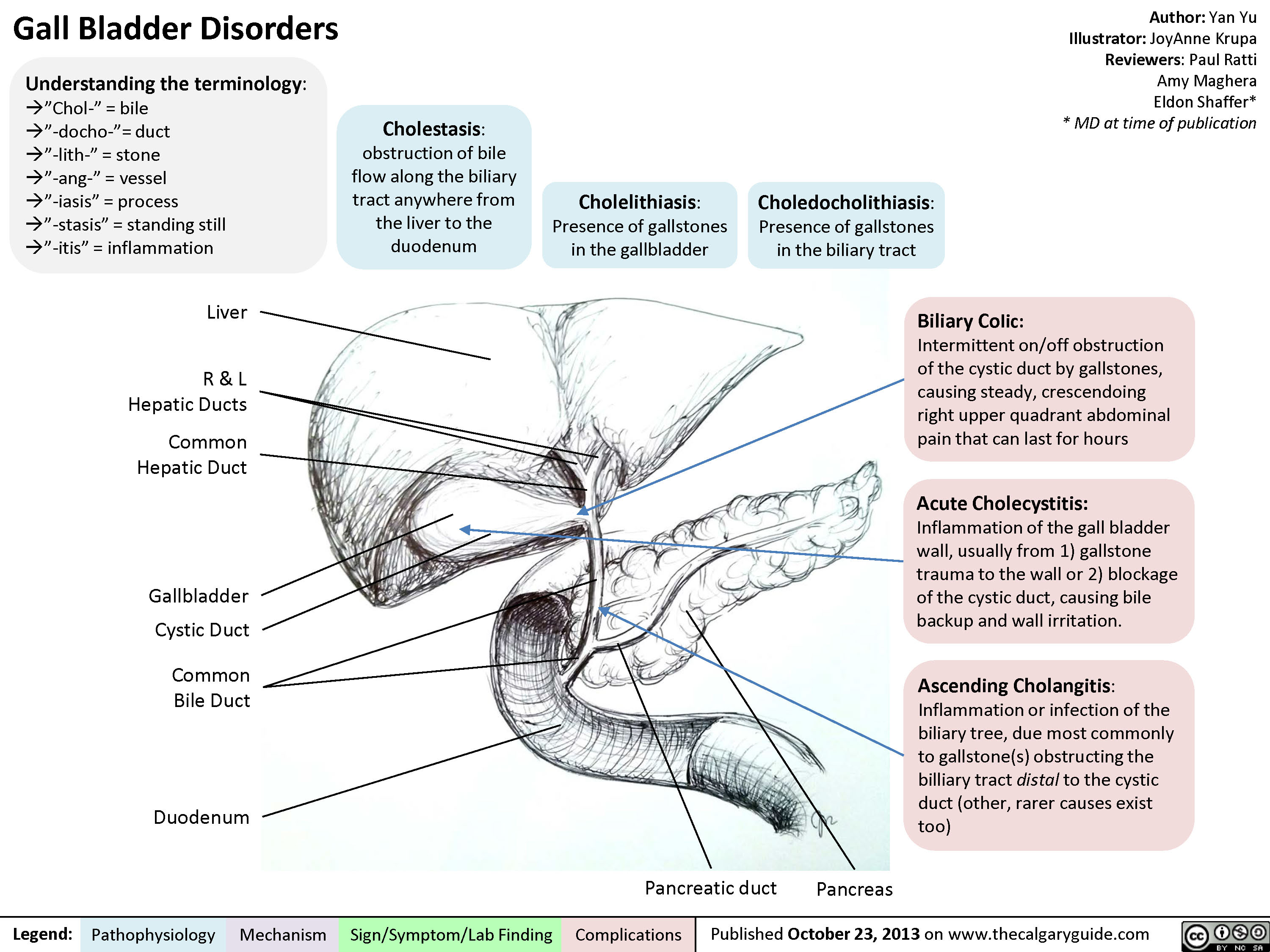
Gall Bladder Disorders
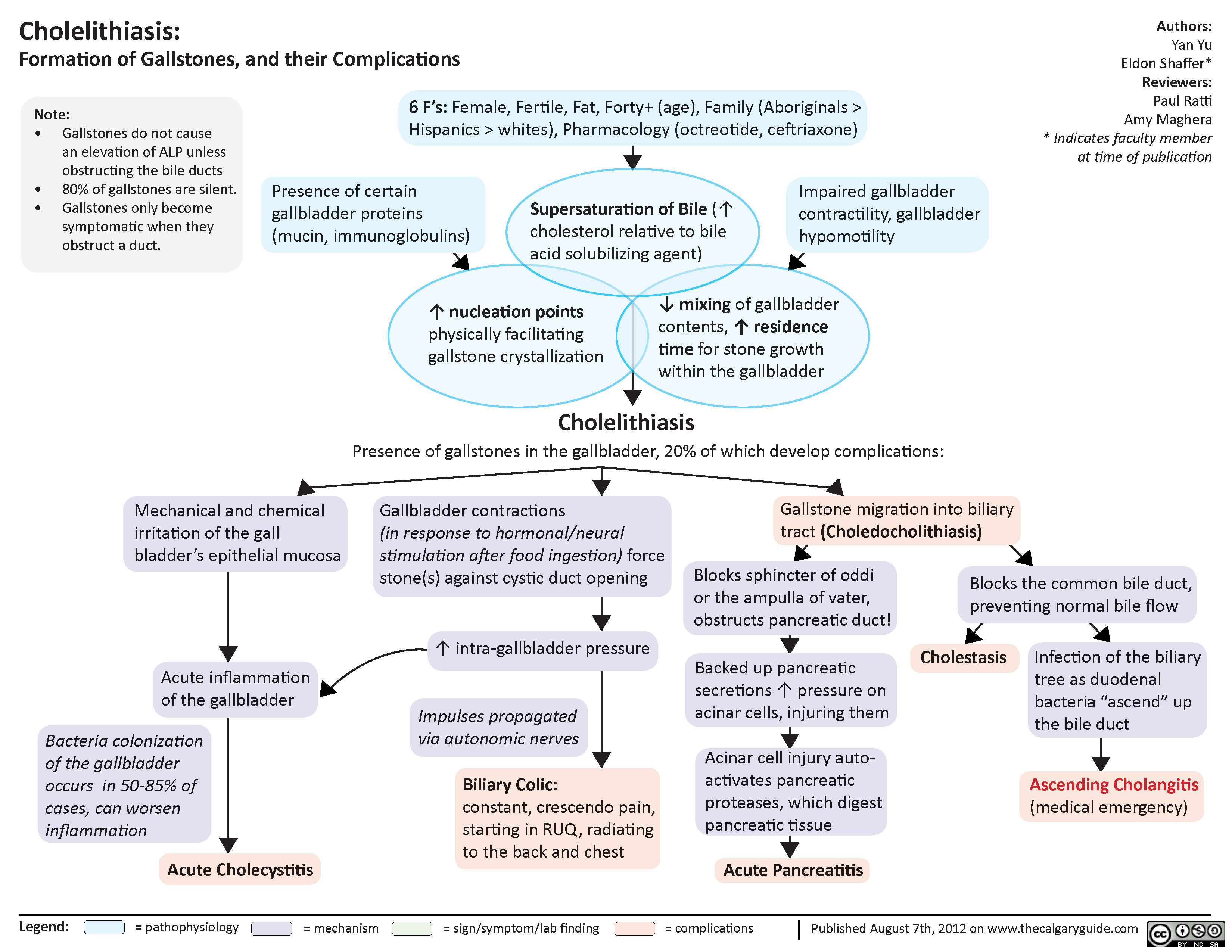
Cholelithiasis
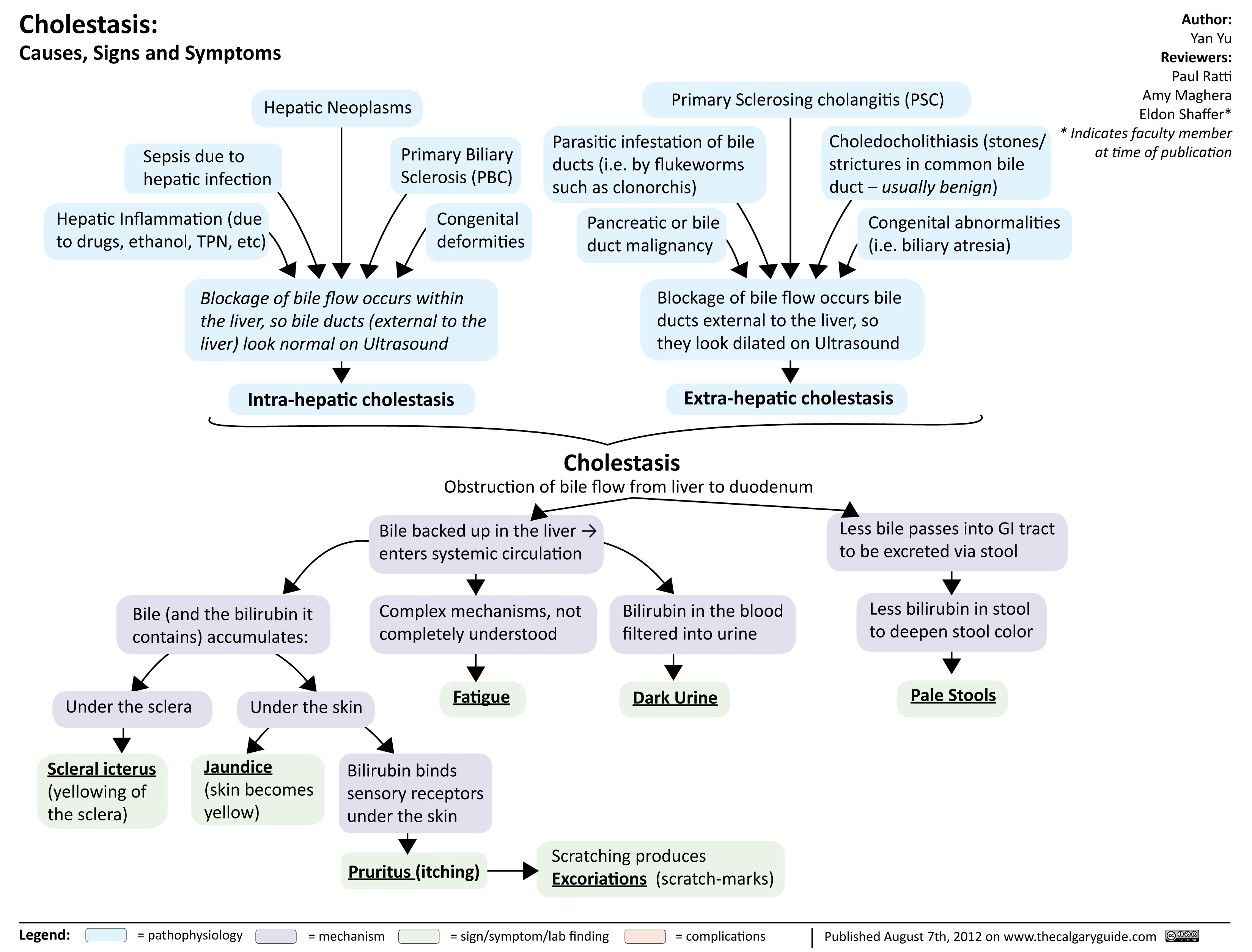
Cholestasis
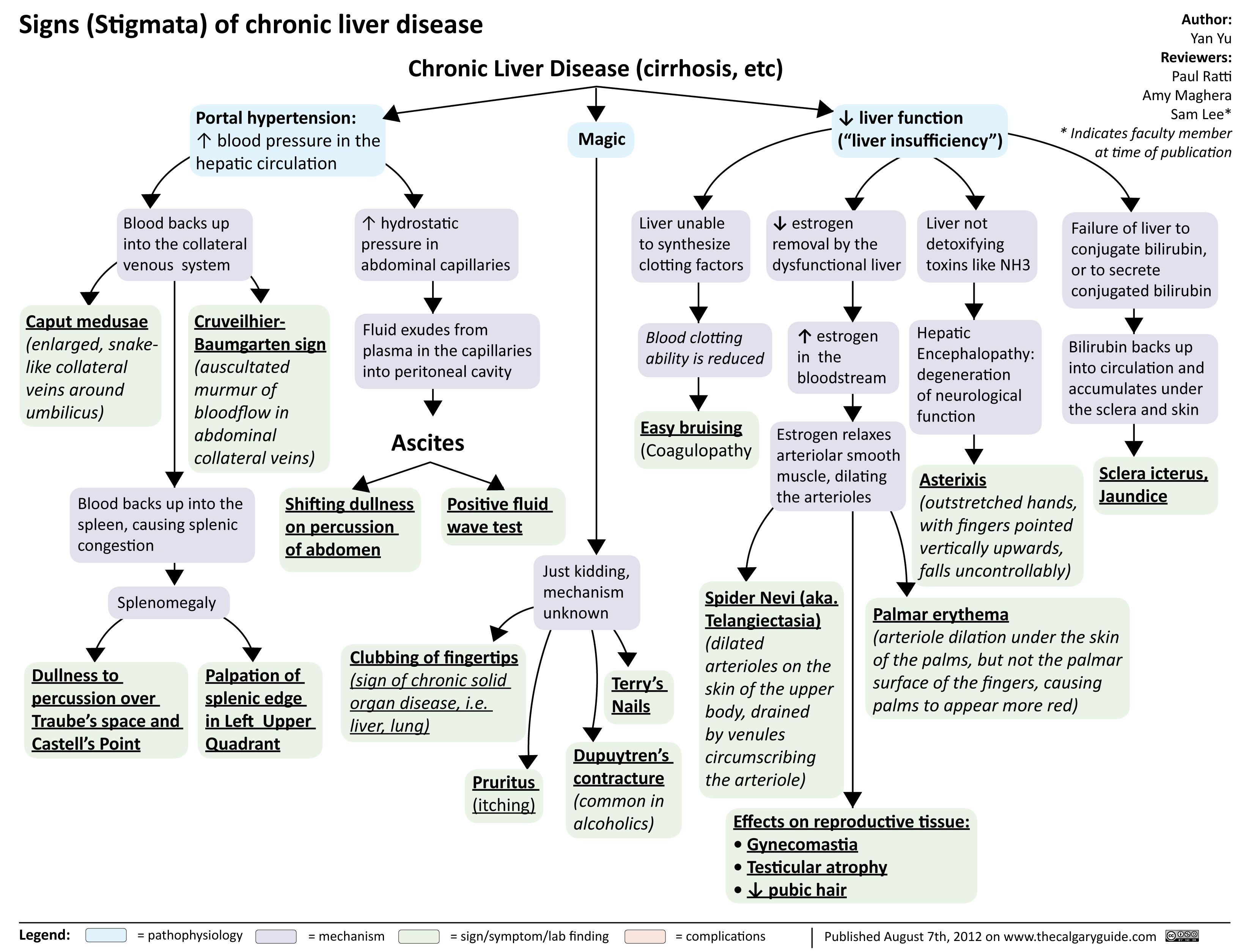
signs of chronic liver disease
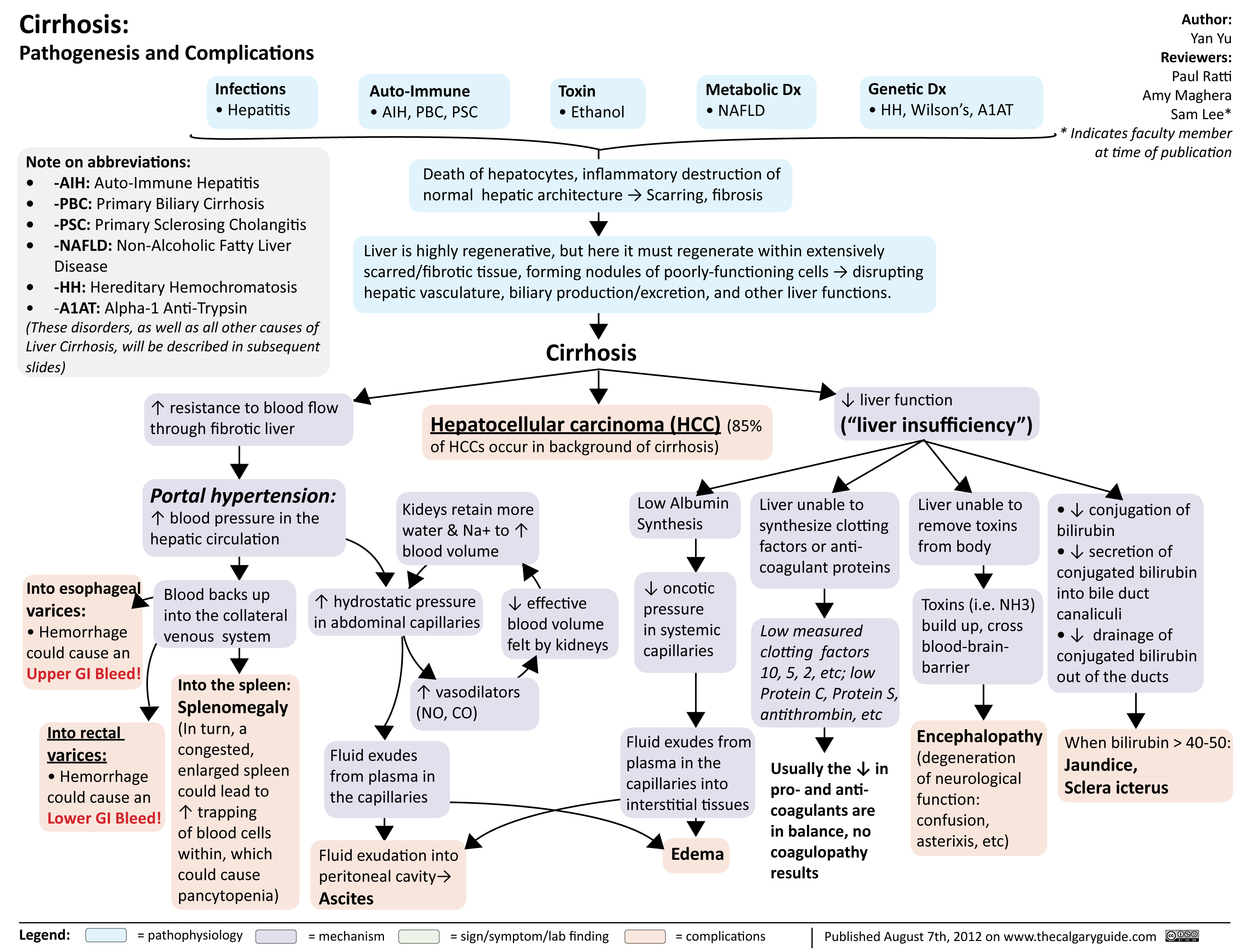
cirrhosis
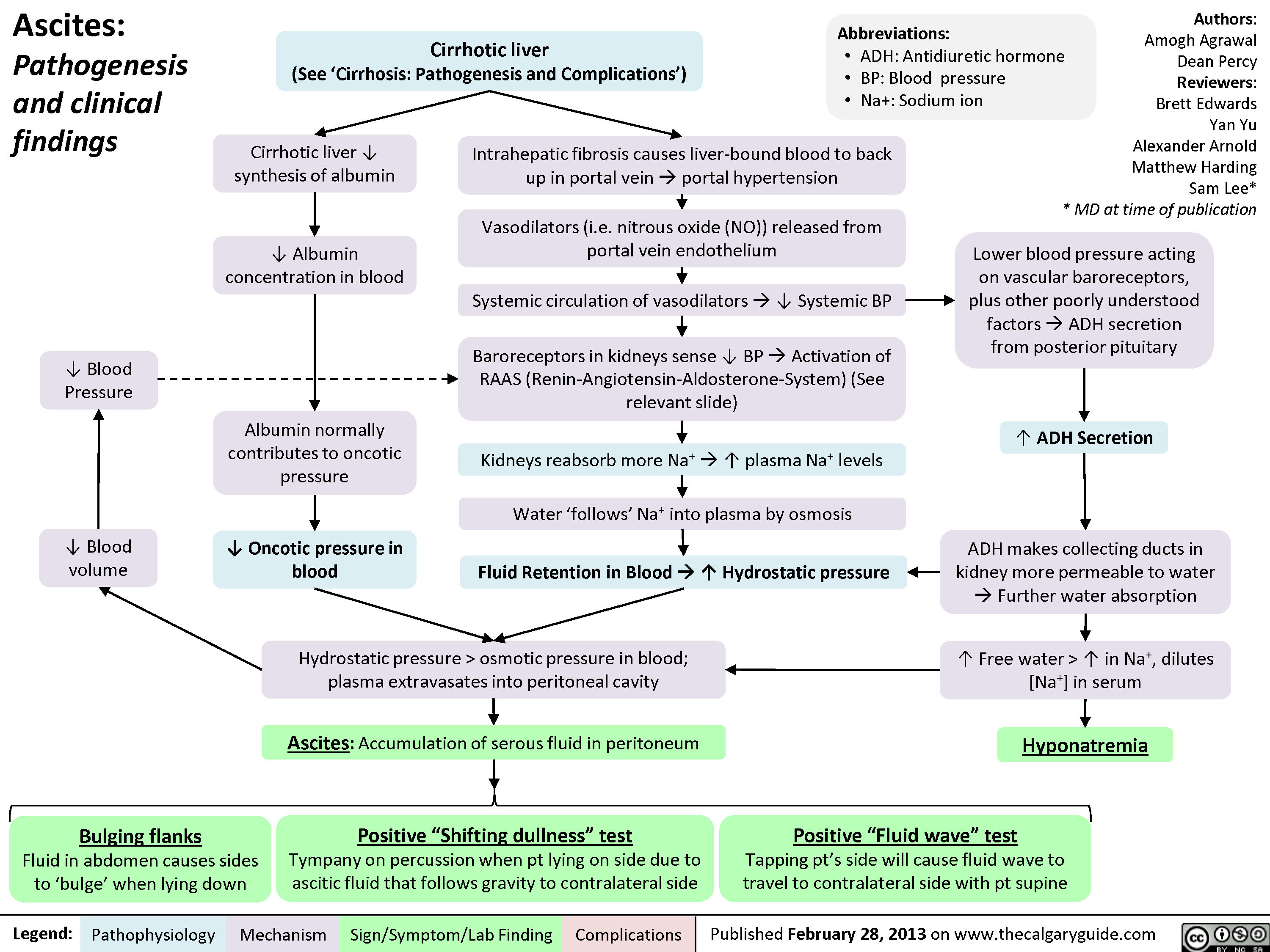
Ascites Clinical Findings
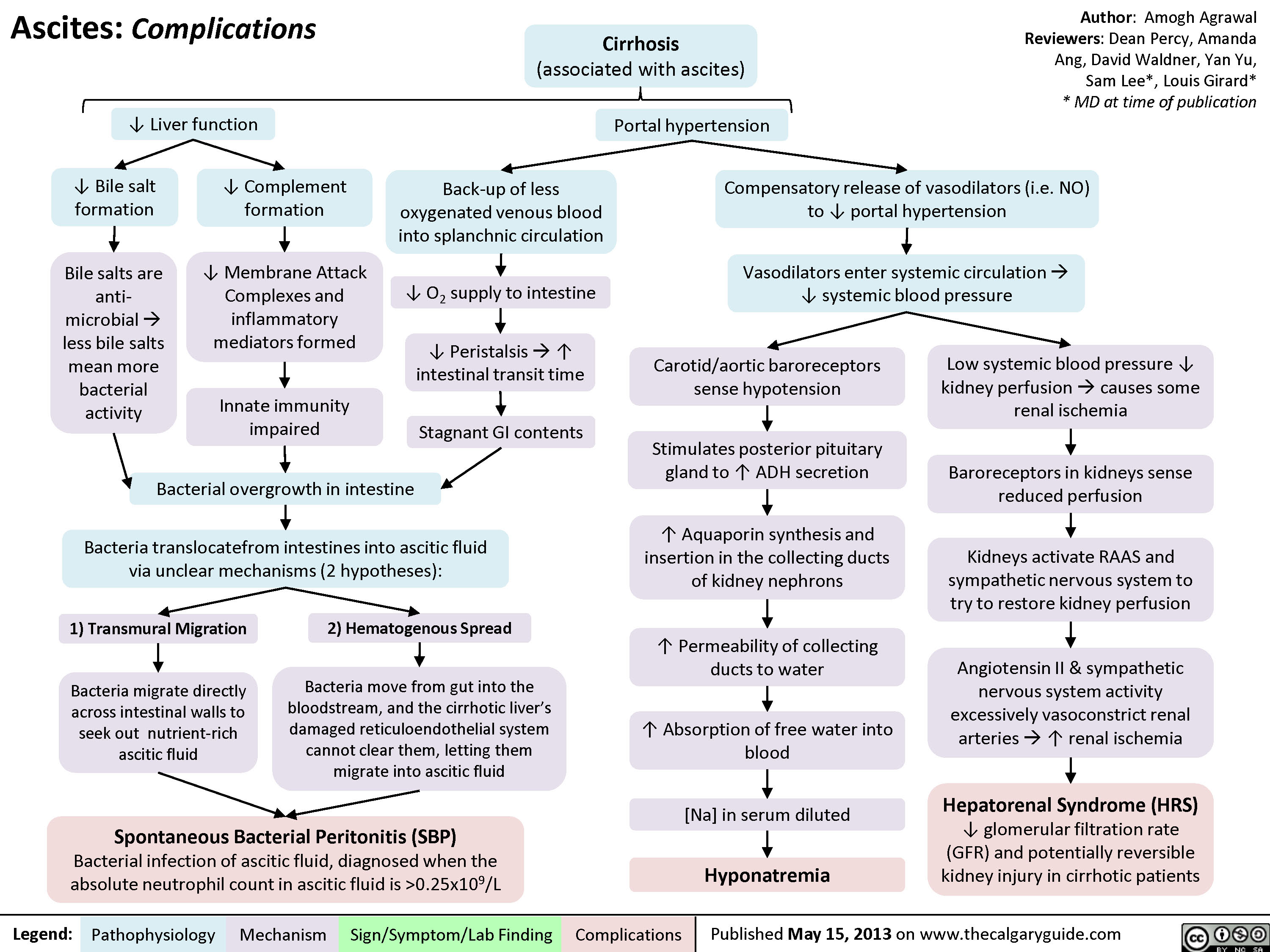
AscitesComplications
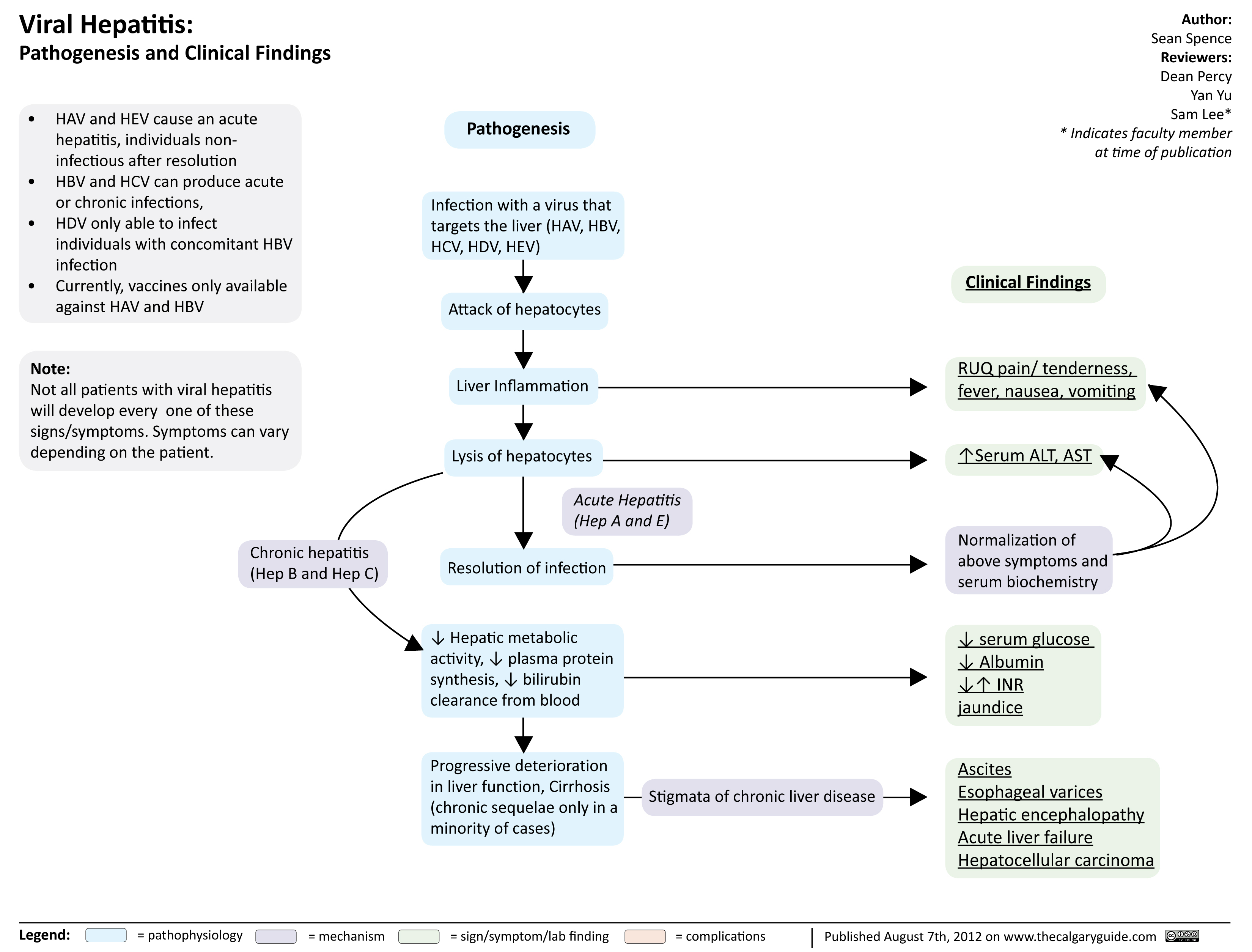
viral hepatits
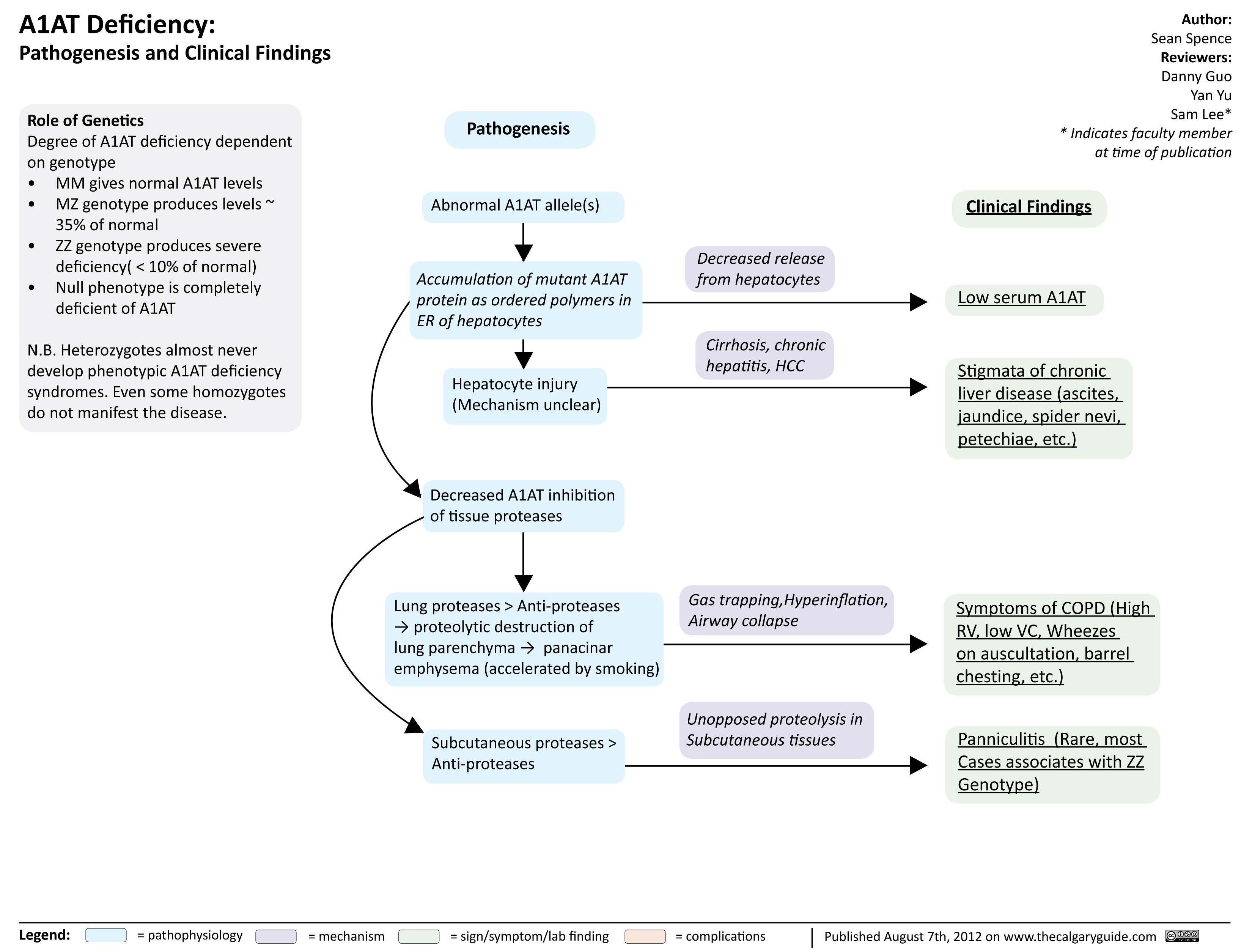
A1ATDeficiency
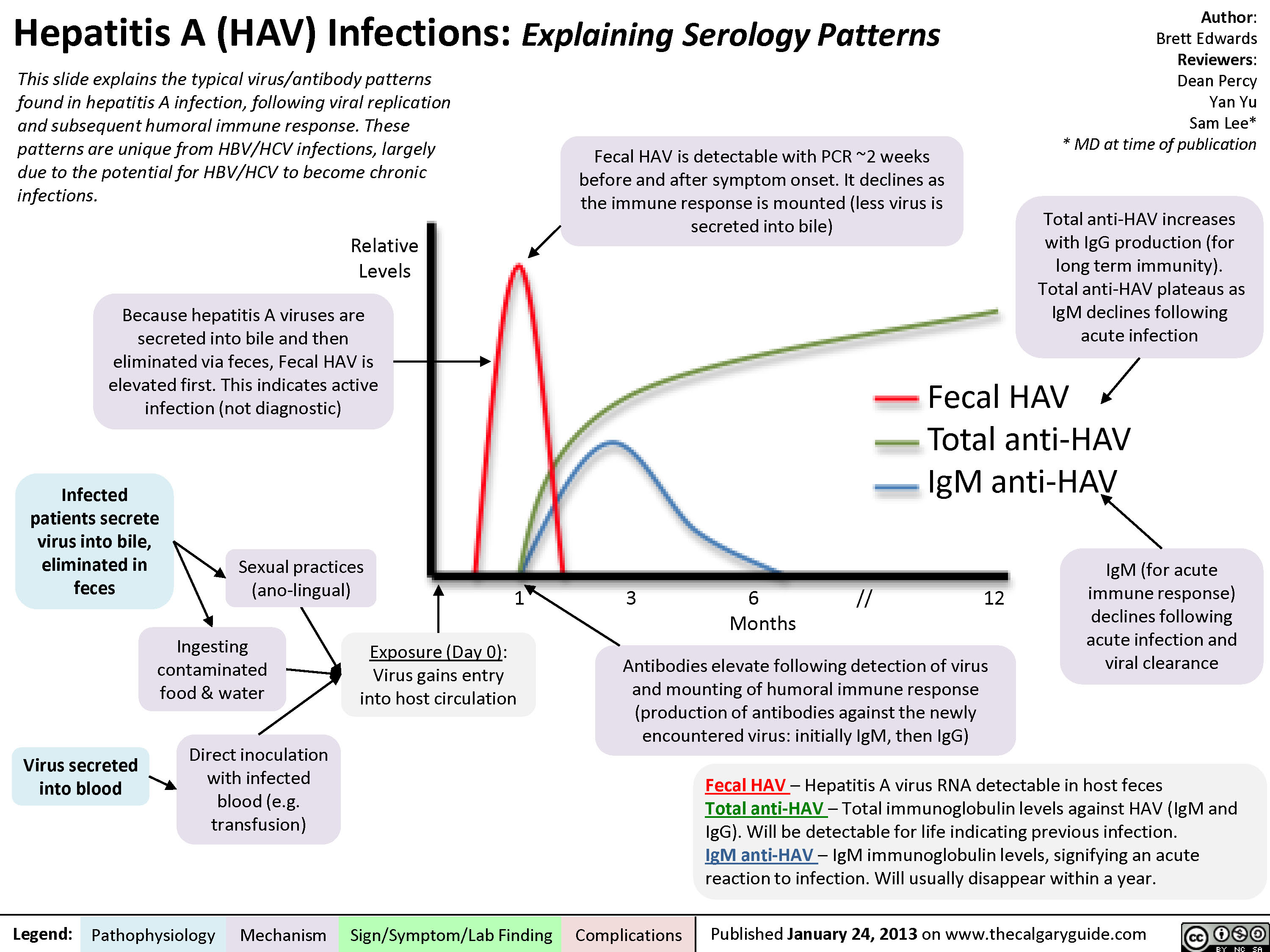
Hepatitis A (HAV) Infections
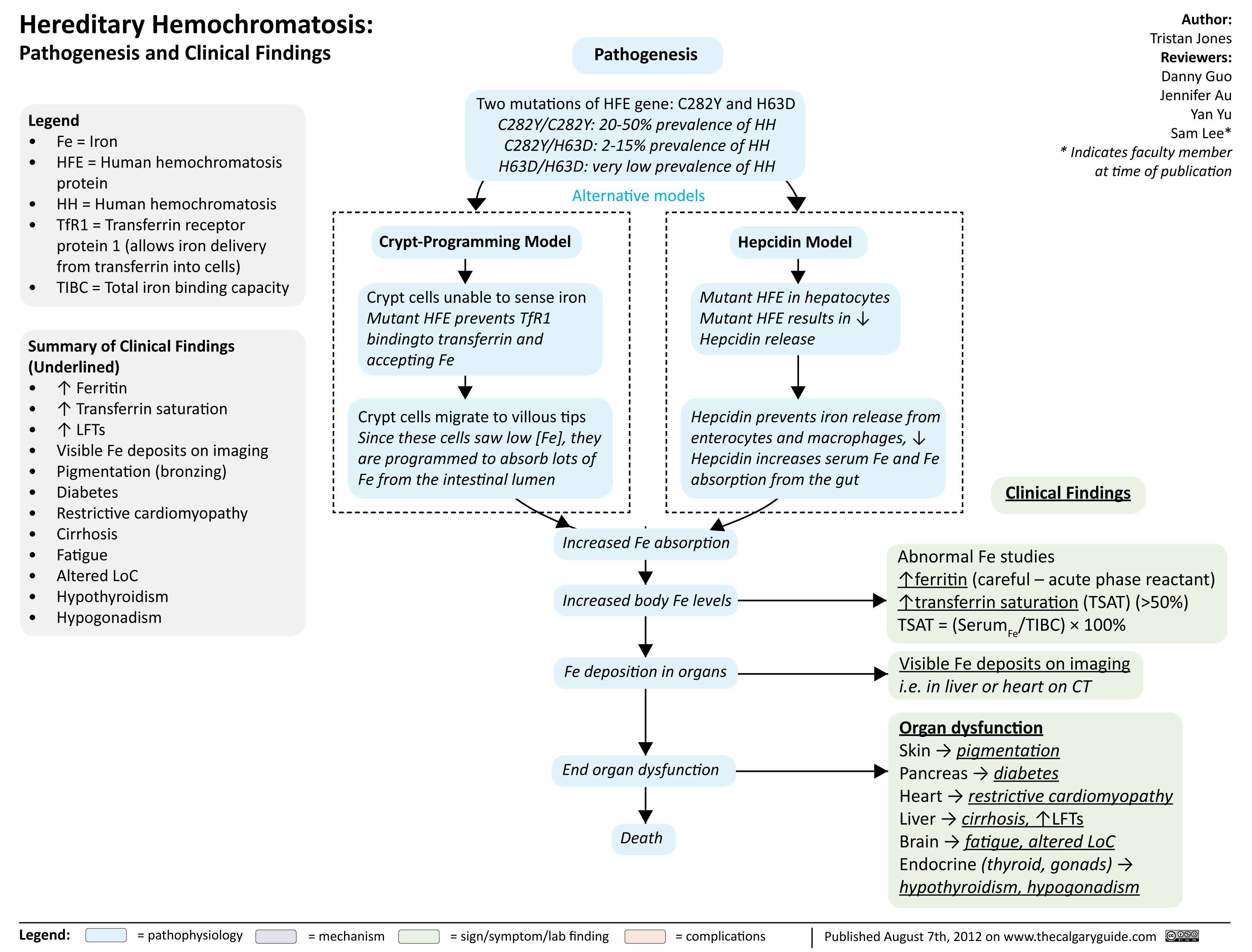
Hereditary hemochromatosis
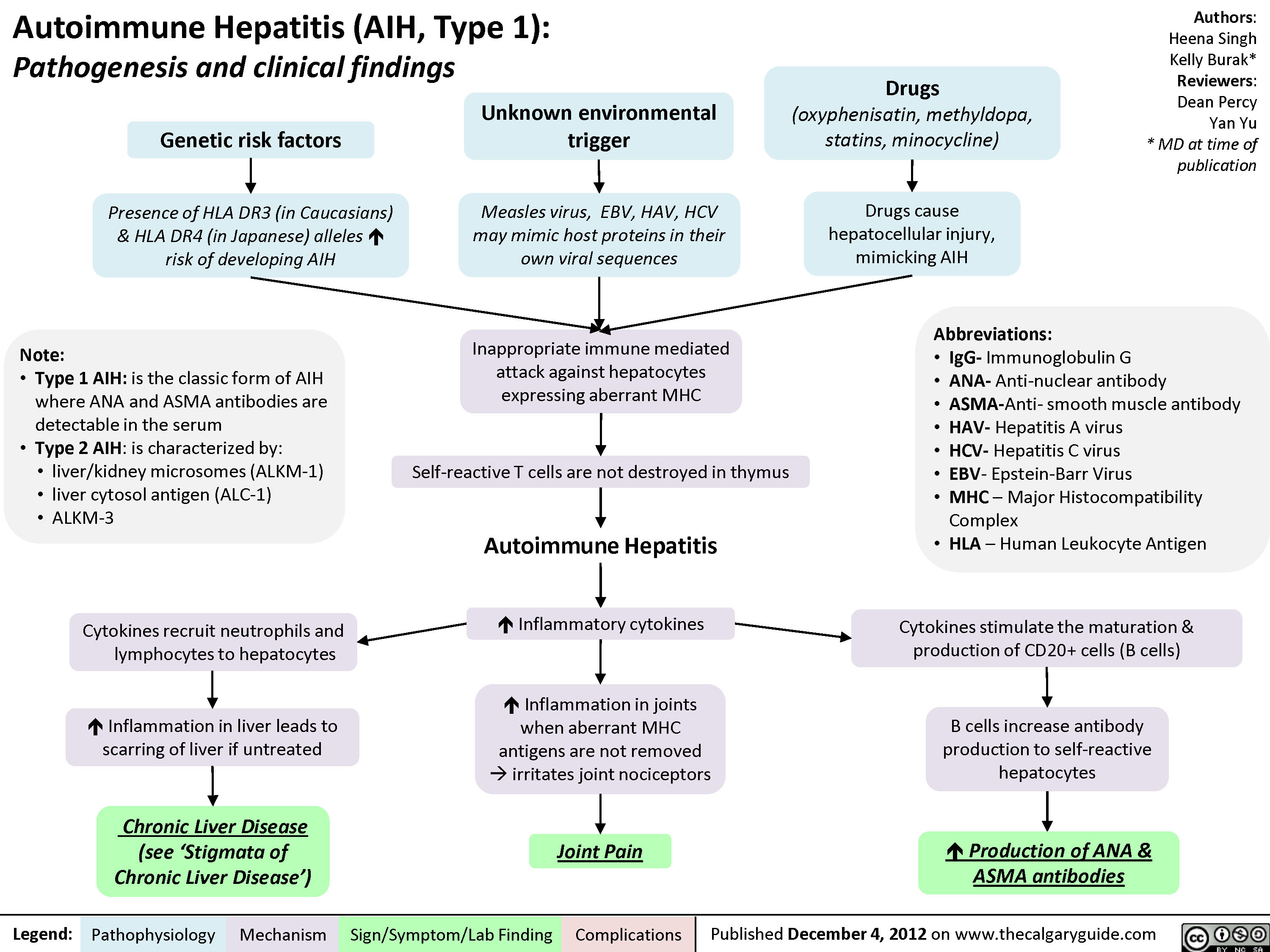
Auto-immune Hepatitis
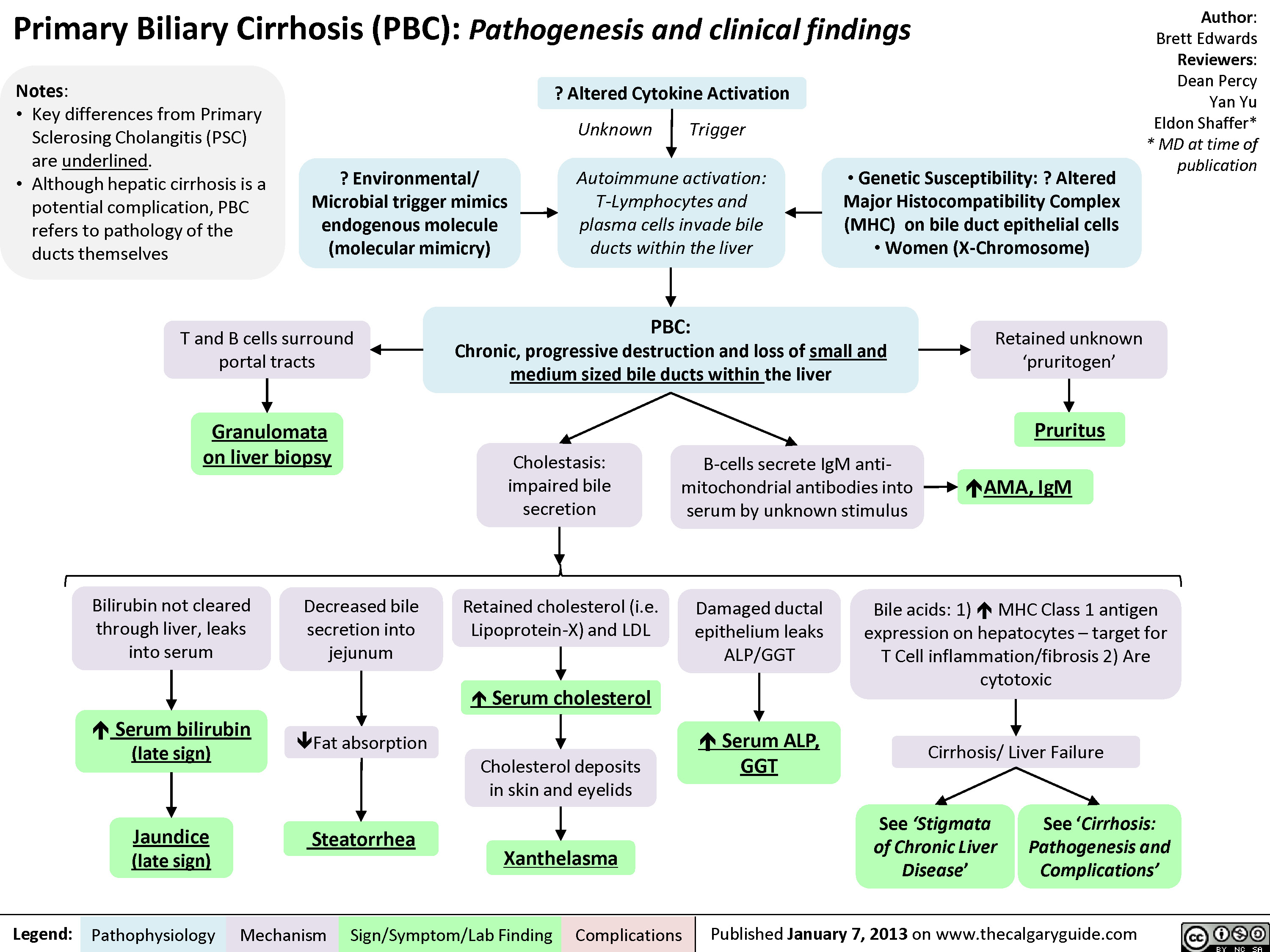
Primary Biliary Cirrhosis (PBC)
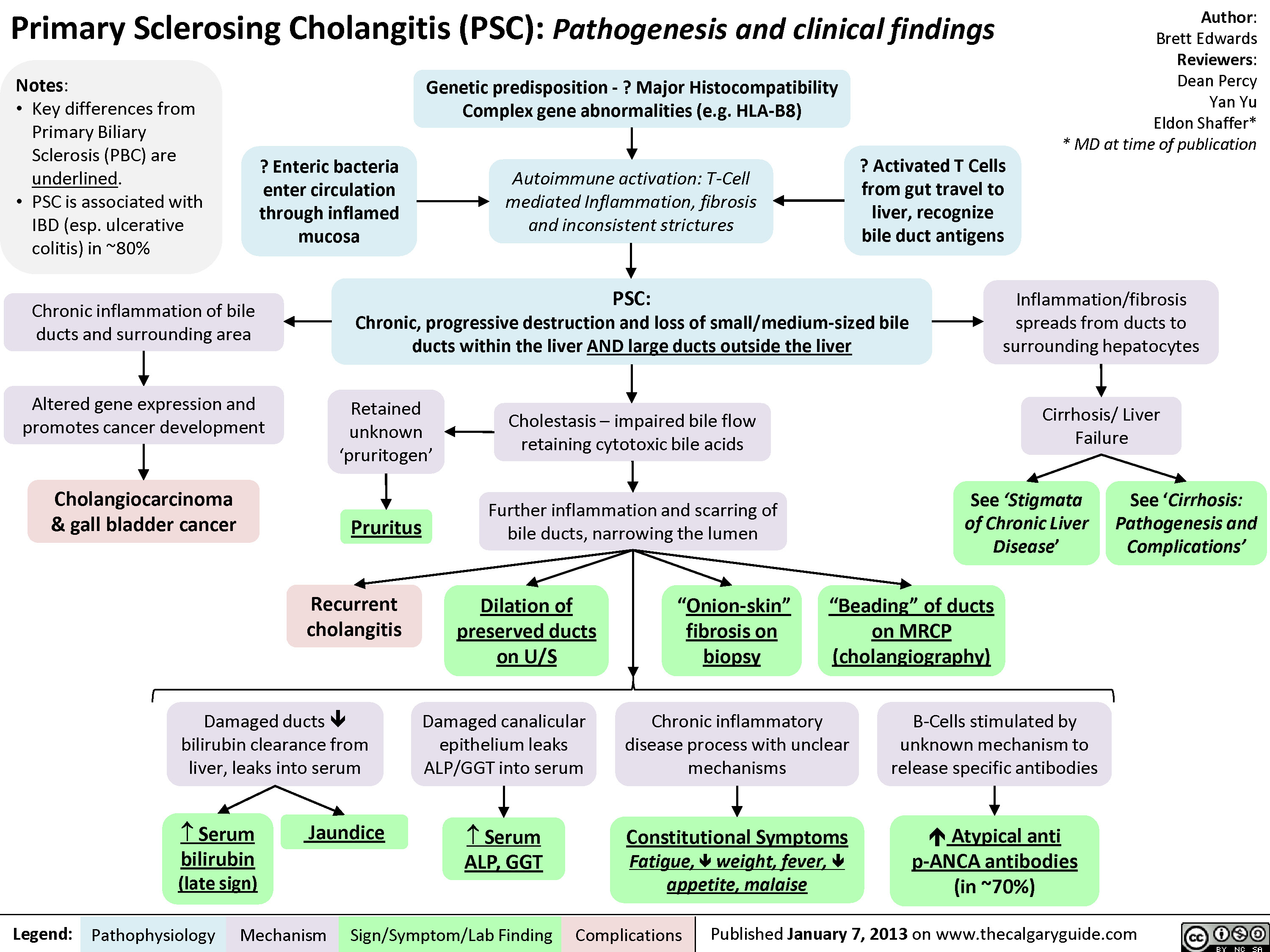
Primary Sclerosing Cholangitis (PSC)
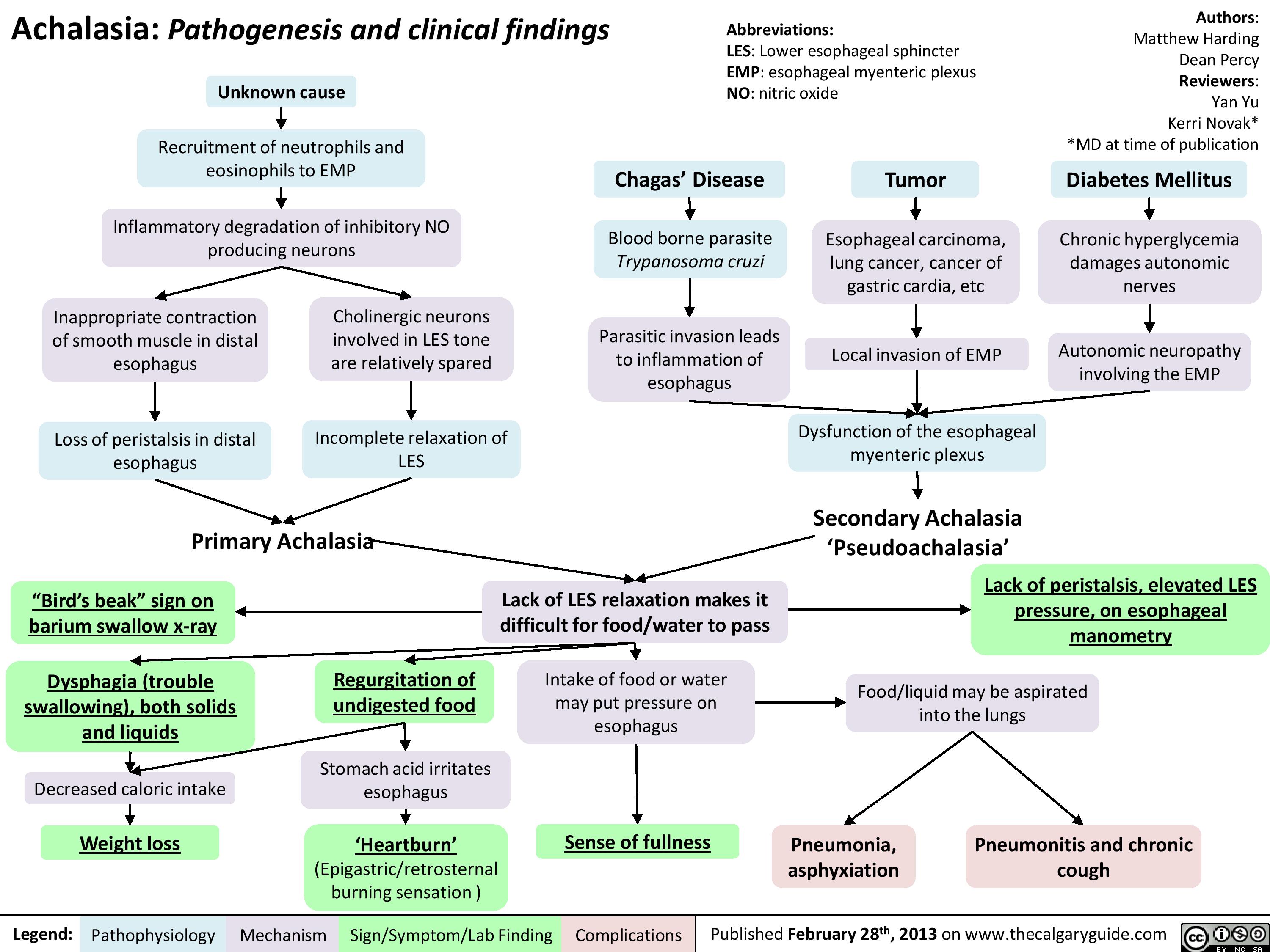
Achalasia Pathogenesis and clinical findings
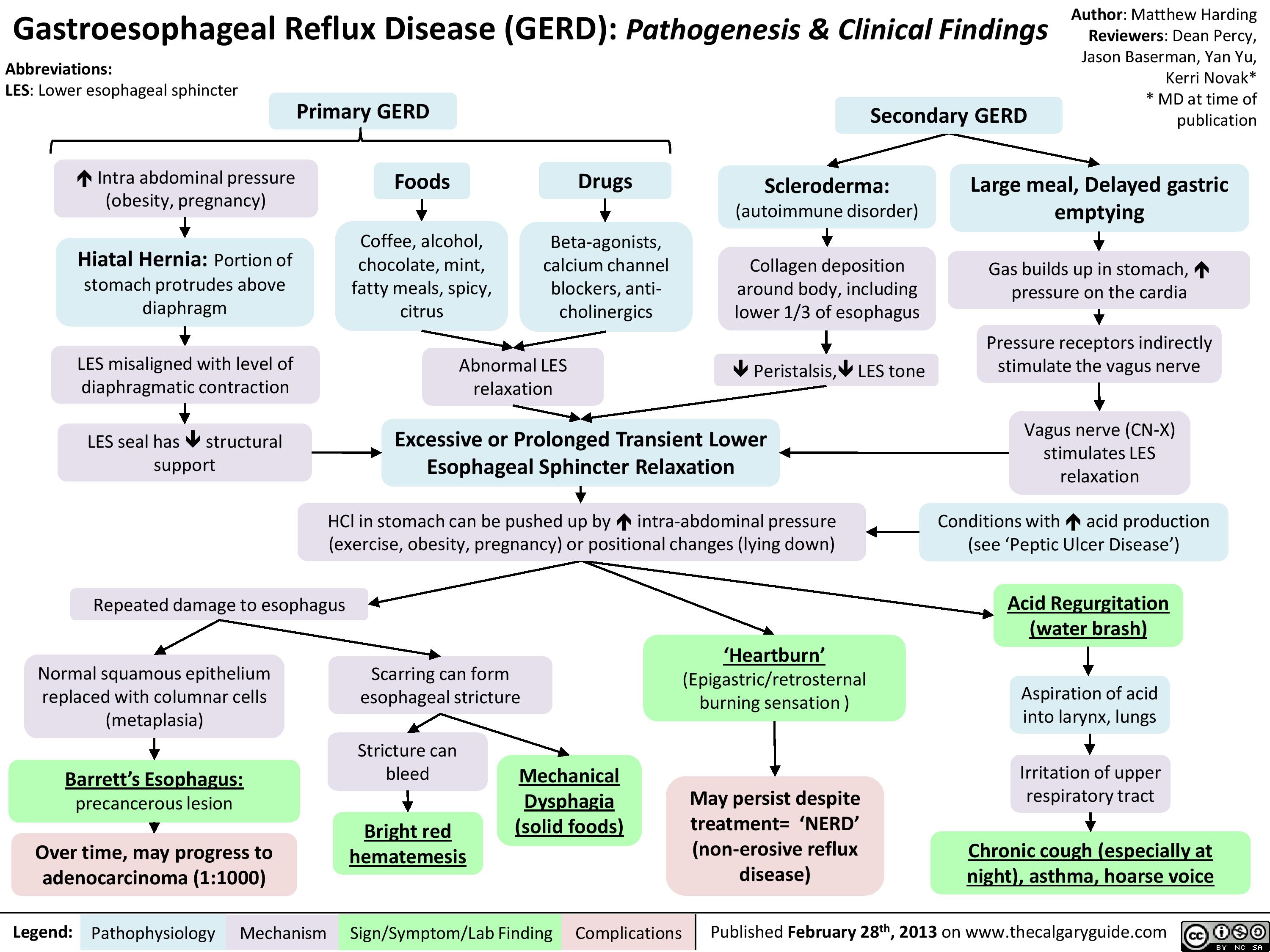
Gastroesophageal Reflux Disease (GERD) Pathogenesis and Clinical Findings
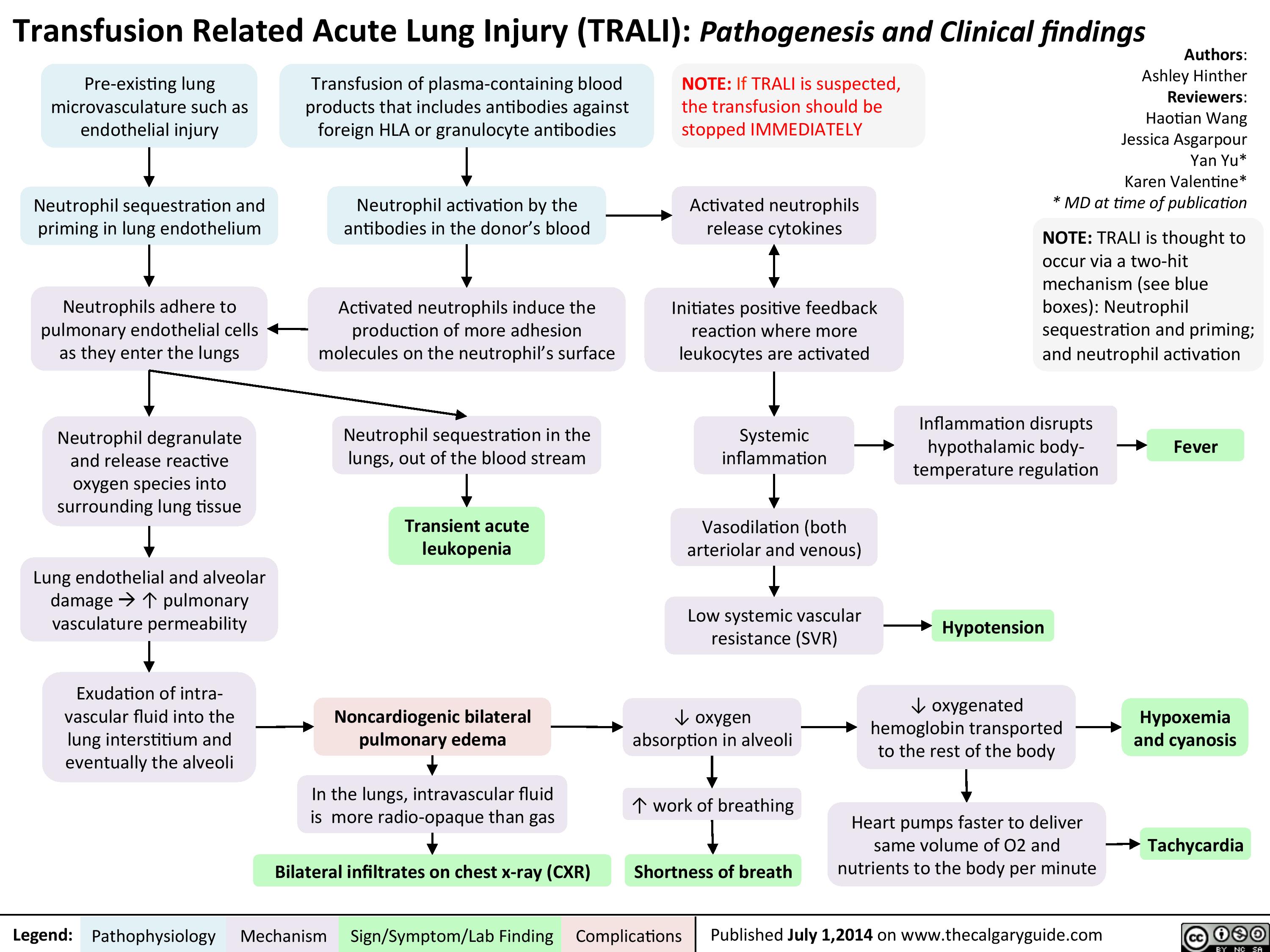
TRALI
Transfusion Associated Circulatory Overload (TACO)
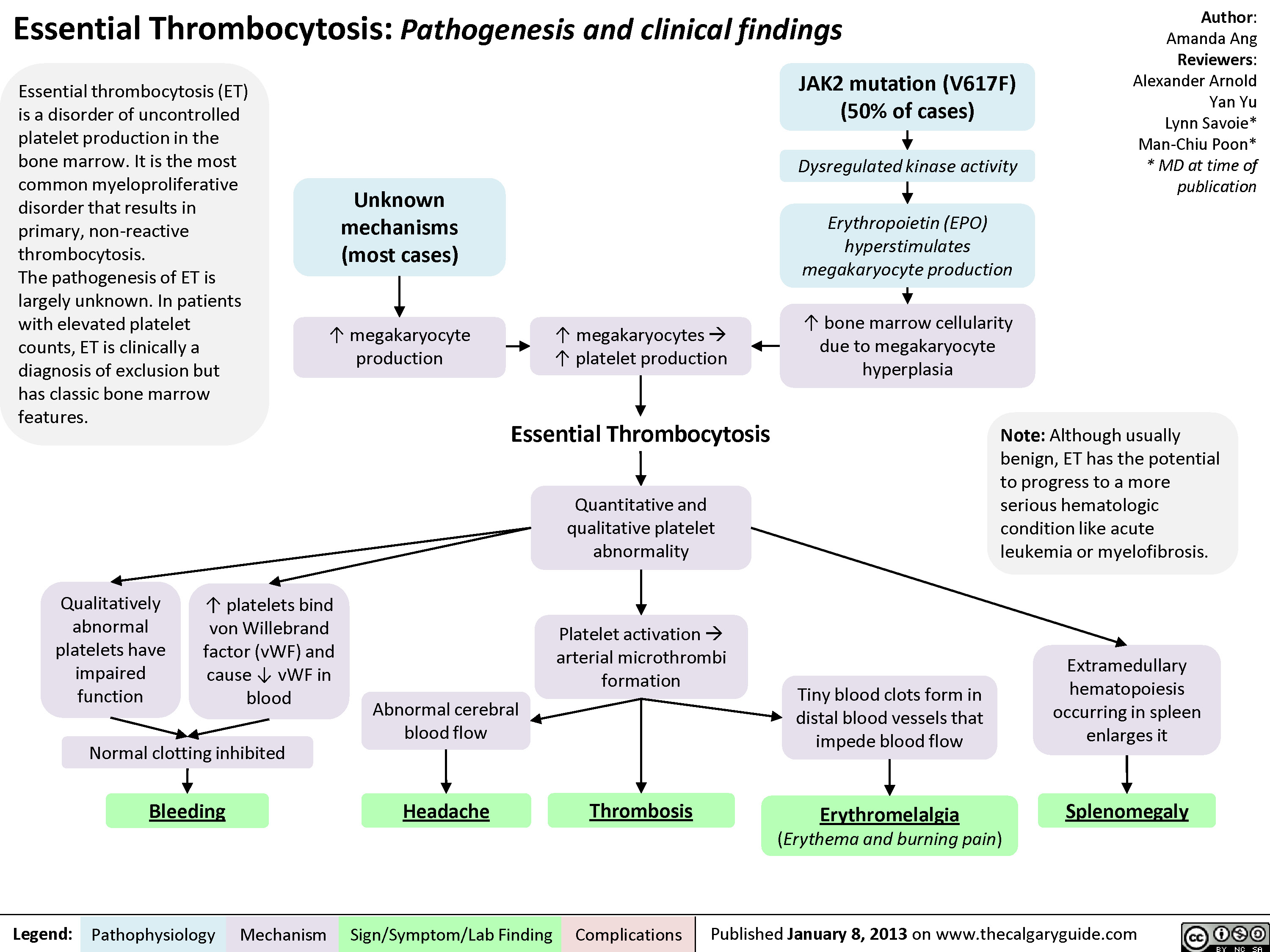
Essential Thrombocytosis (ET)
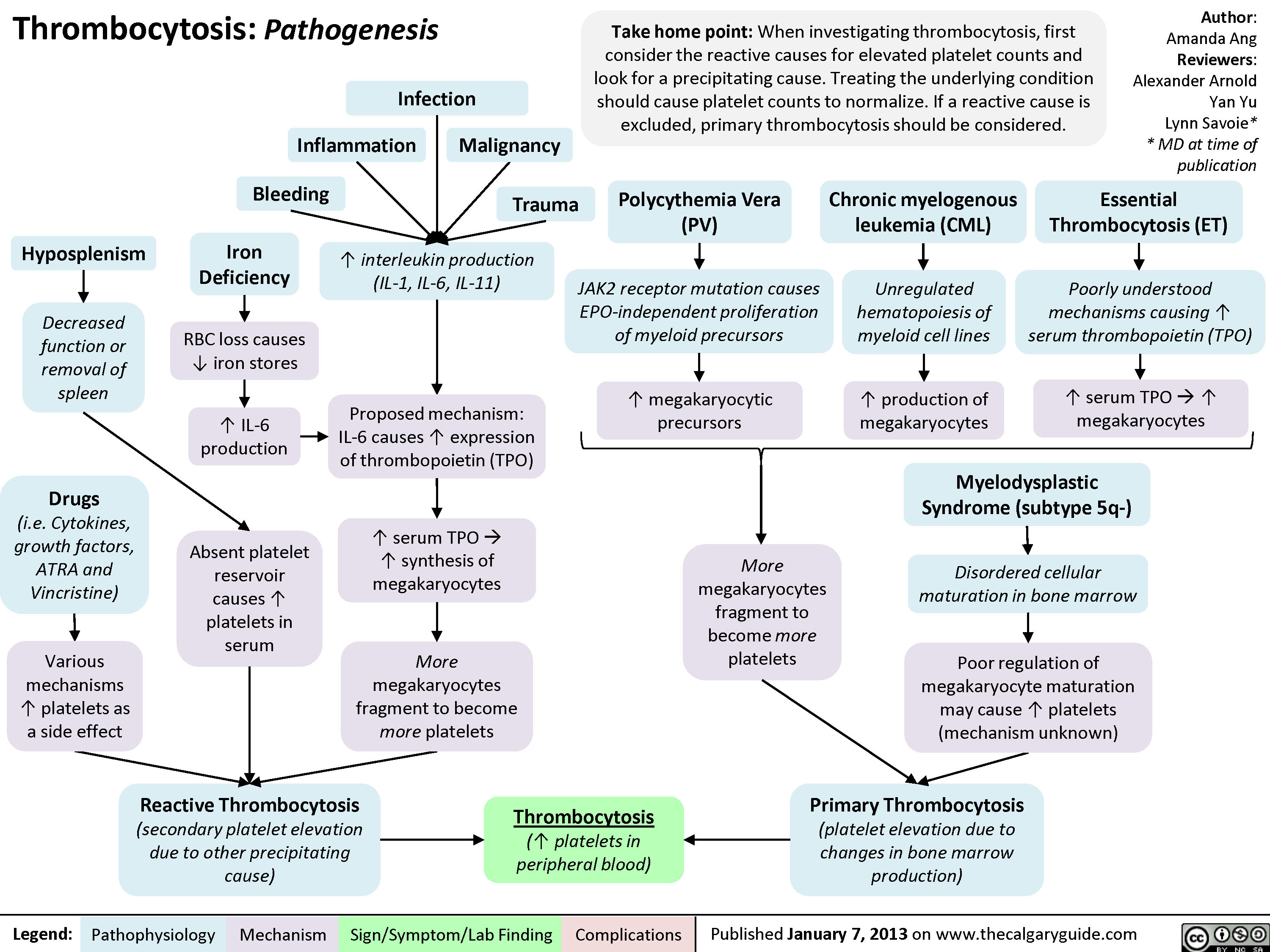
Pathogenesis of thrombocytosis
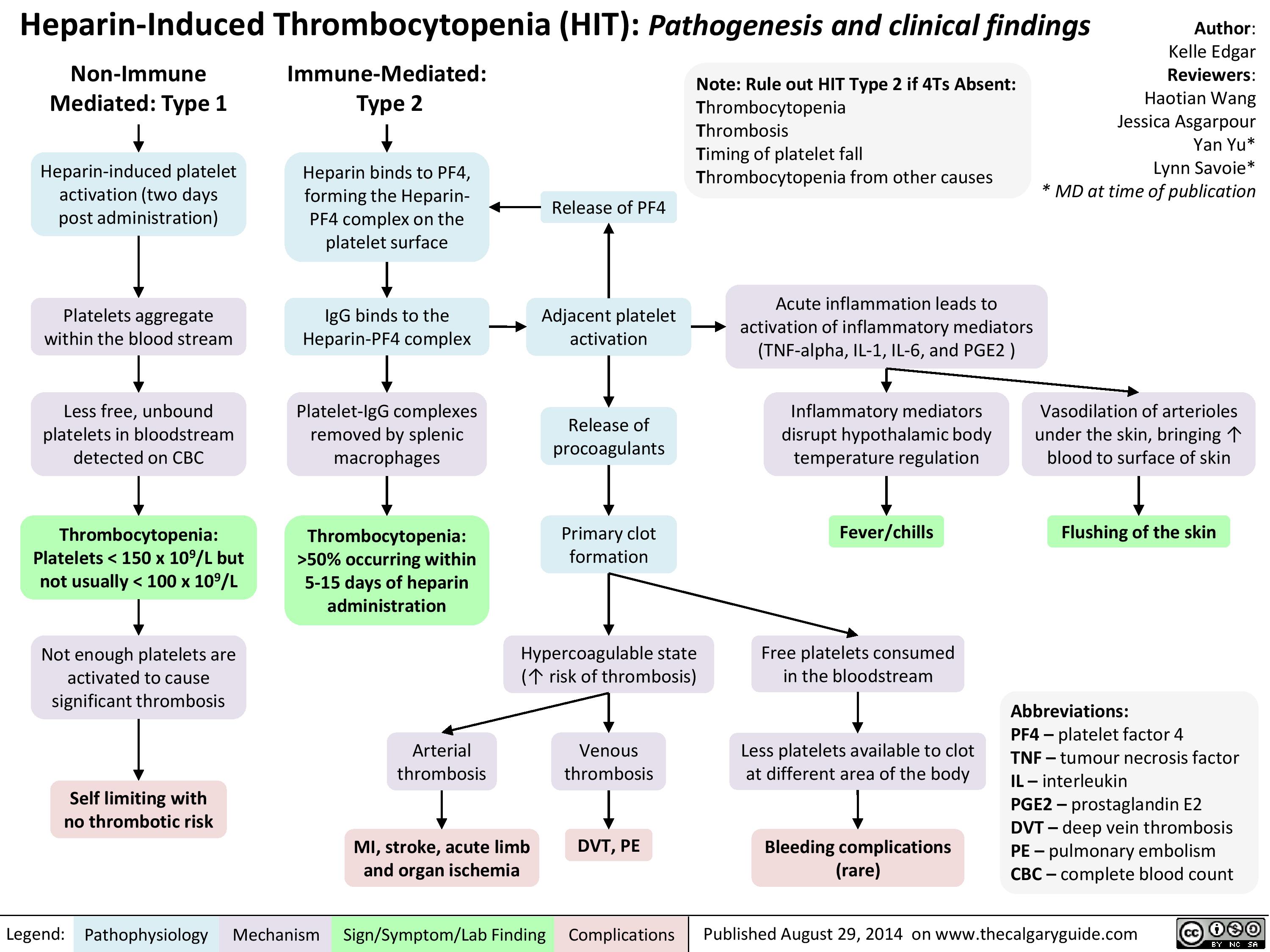
Heparin Induced Thrombocytopenia
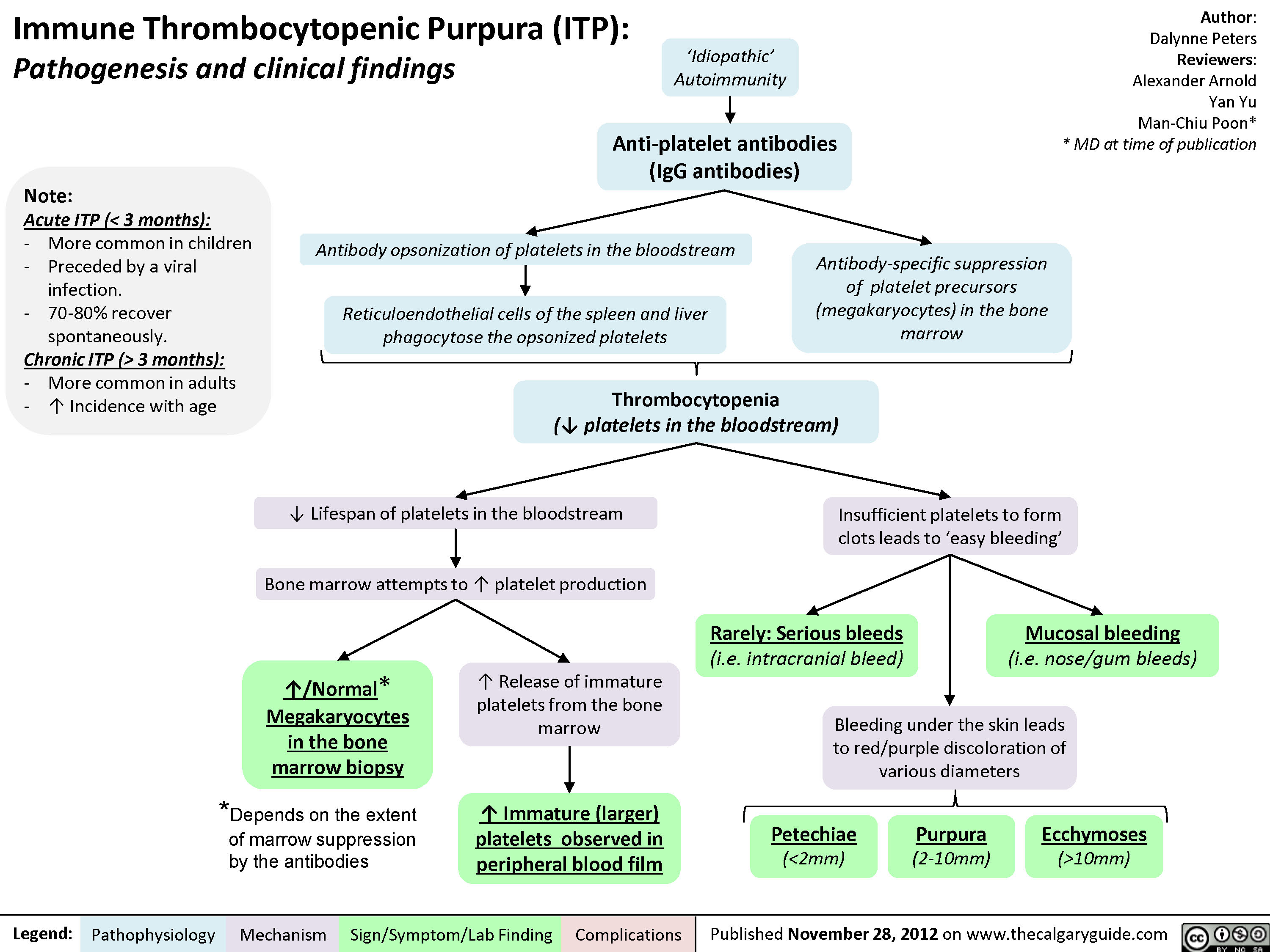
Immune thrombocytopenic purpura
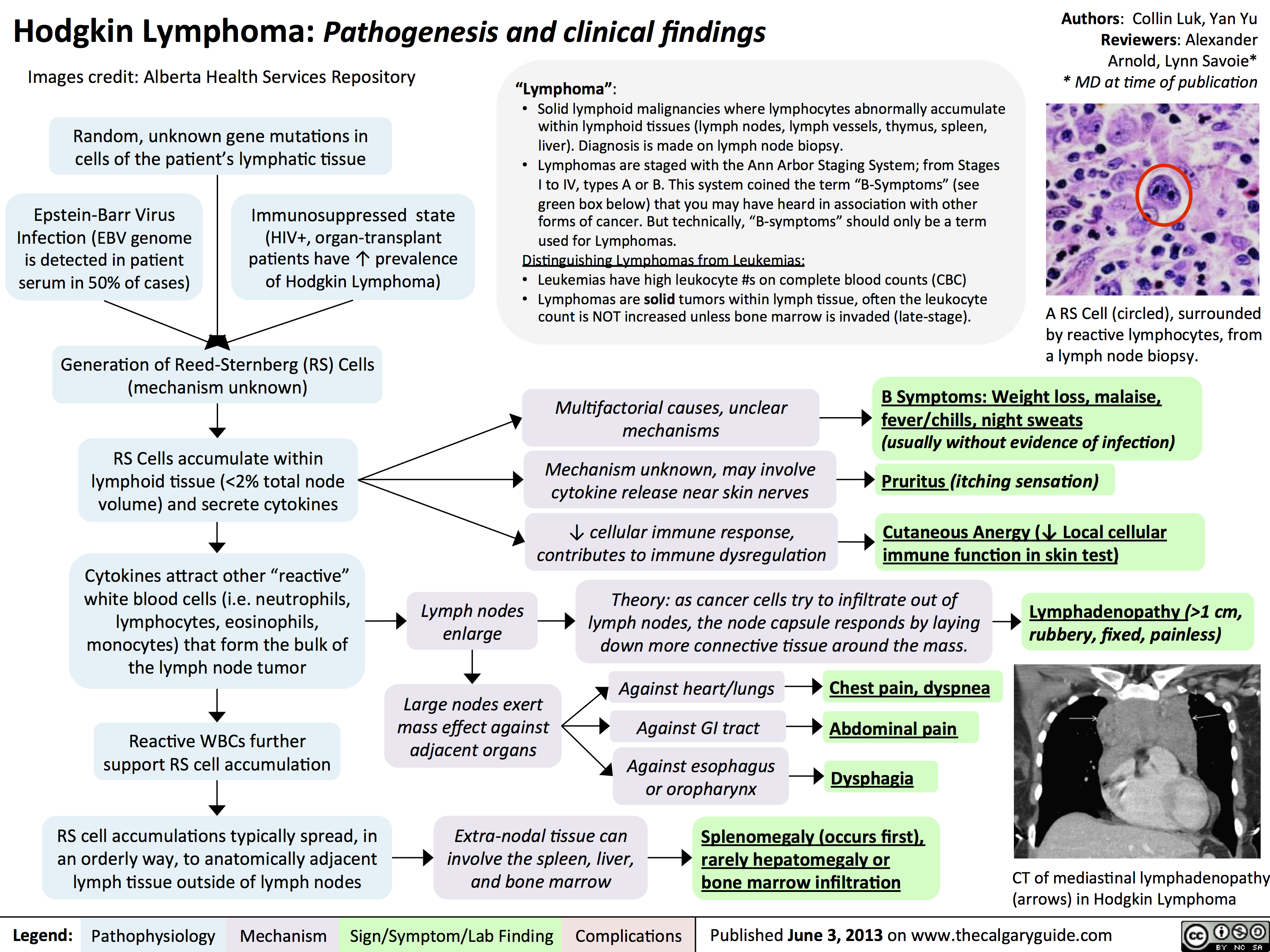
hodgkin lymphoma - pathogenesis and clinical findings
Clinical Features to Describe Abnormal Lymph Nodes

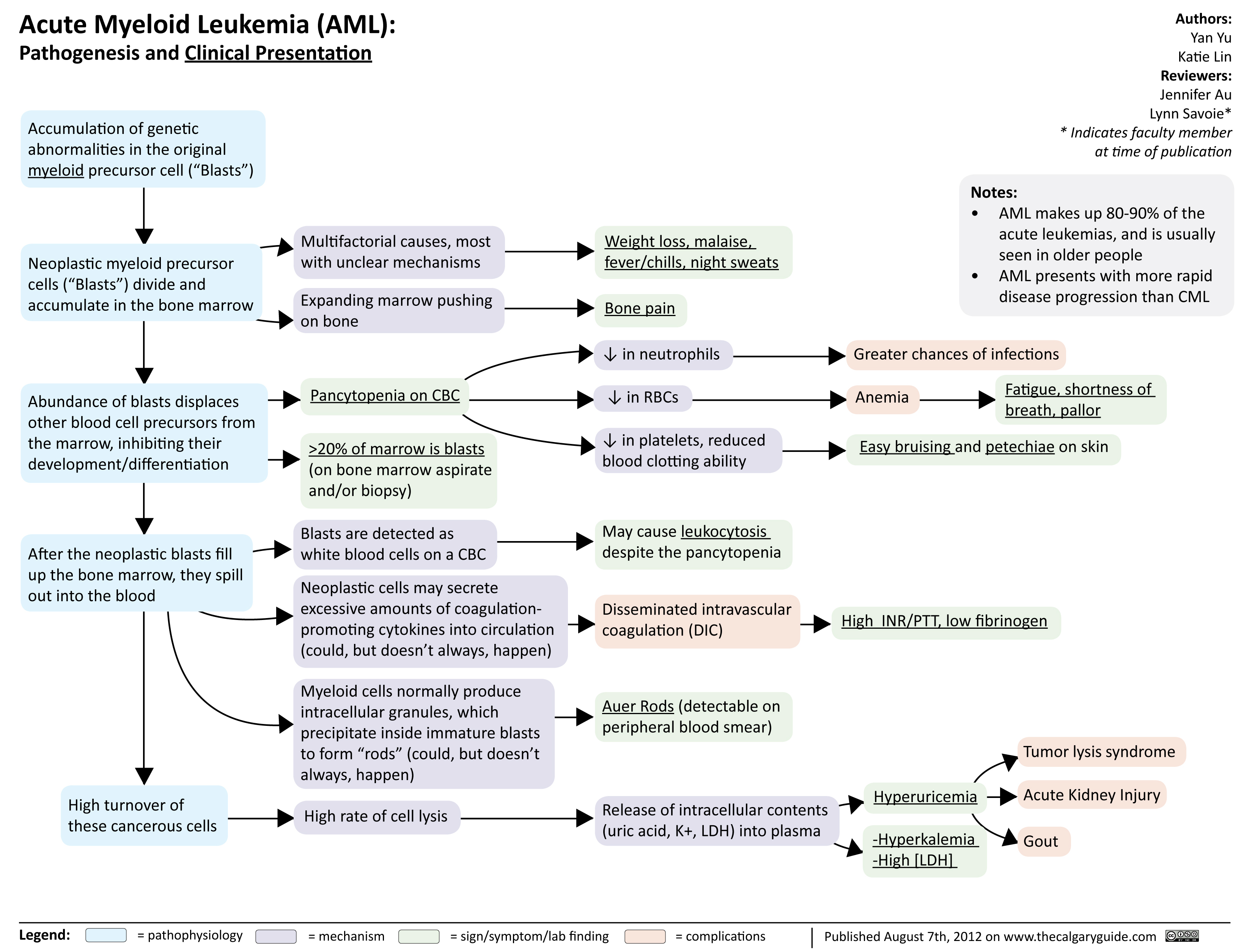
Acute Myeloid Leukemia
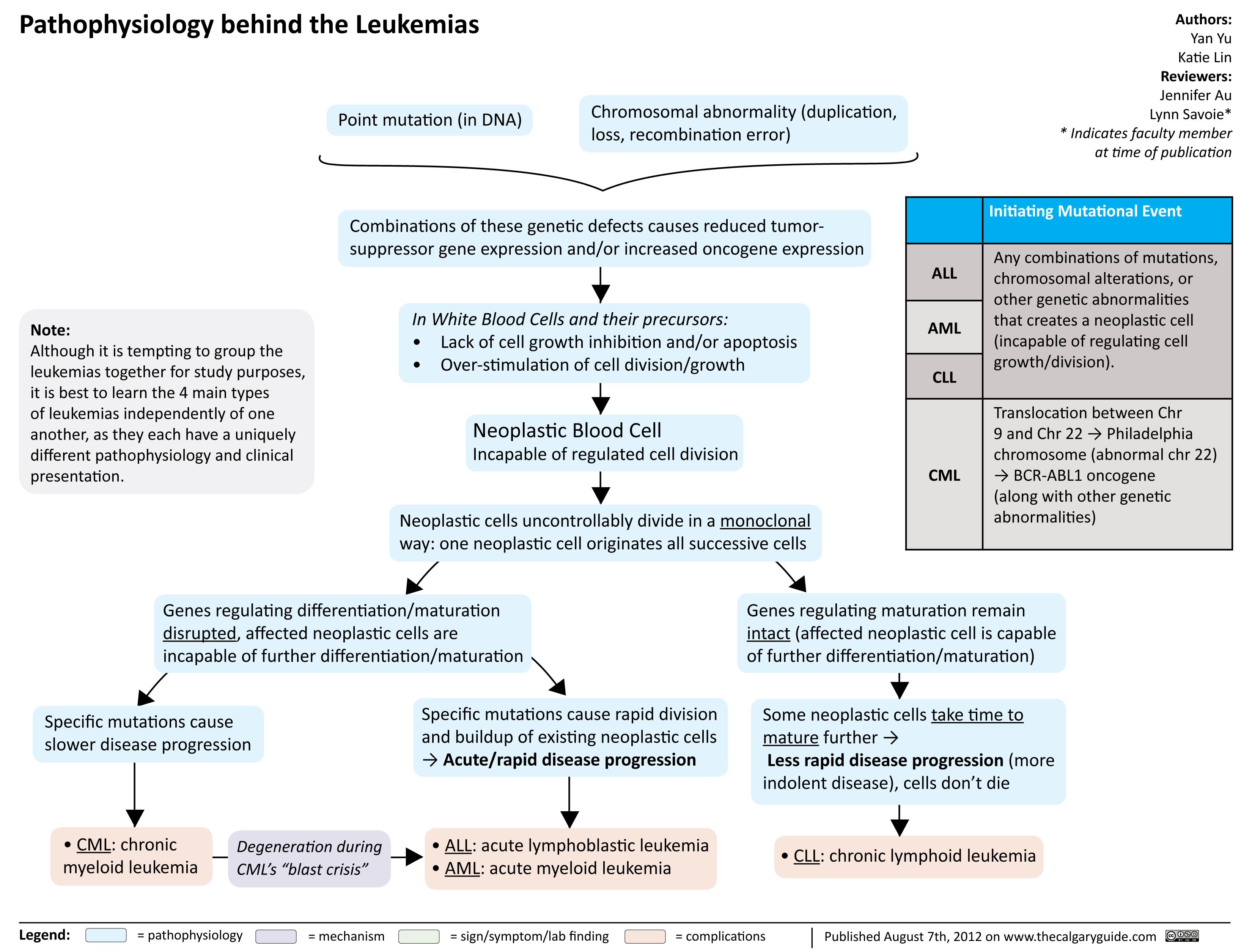
Pathophysiology behind the leukemias
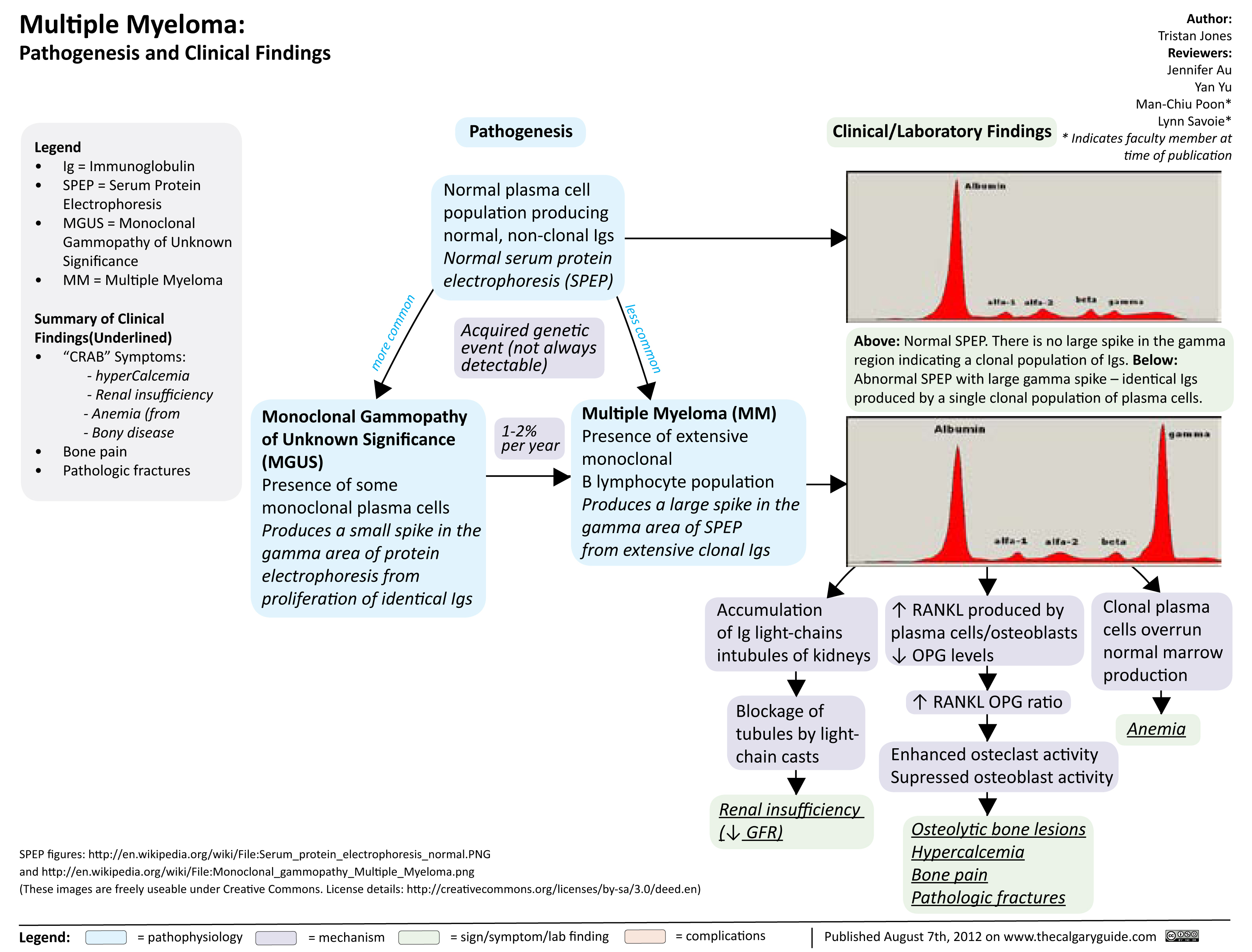
Multiple Myeloma
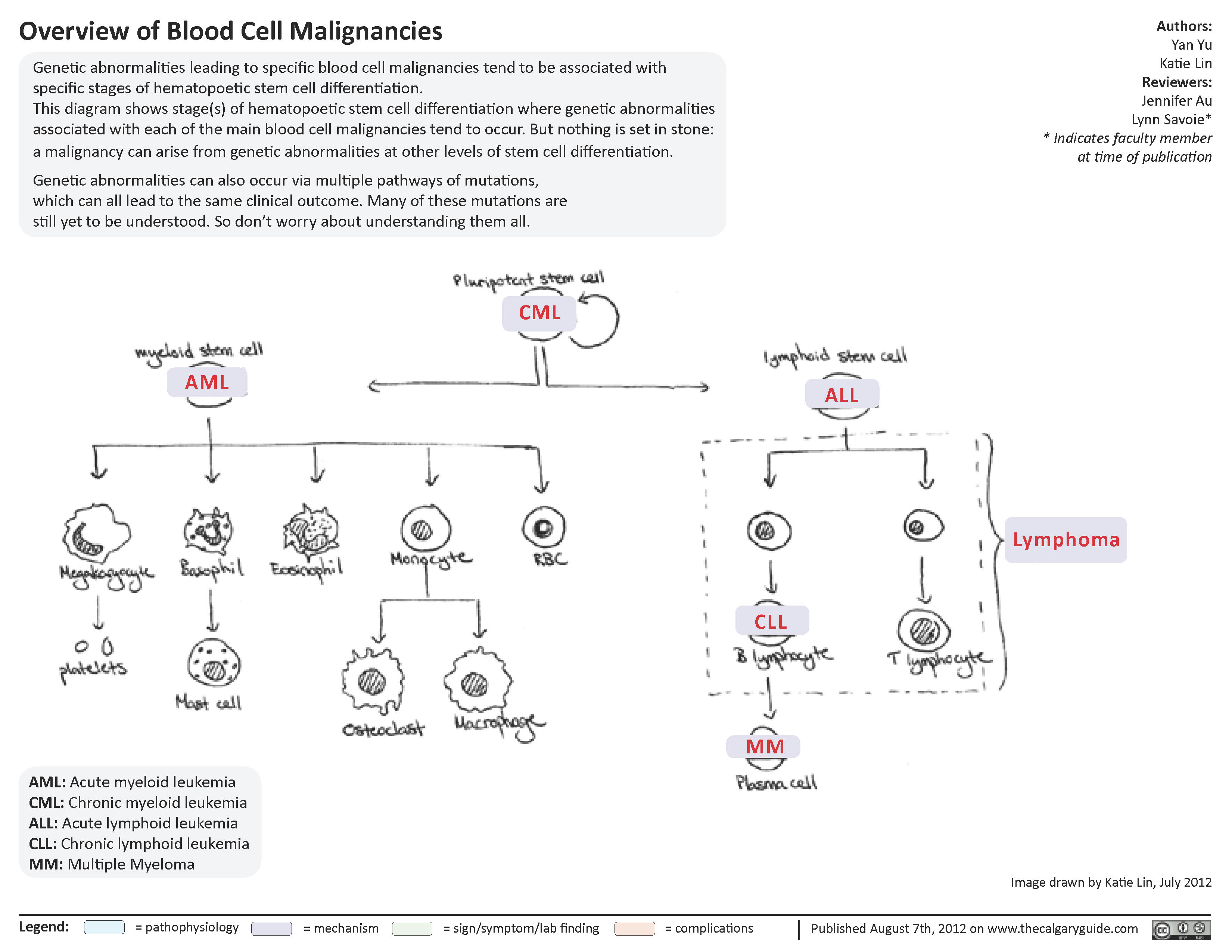
Overview of blood cell malignancies
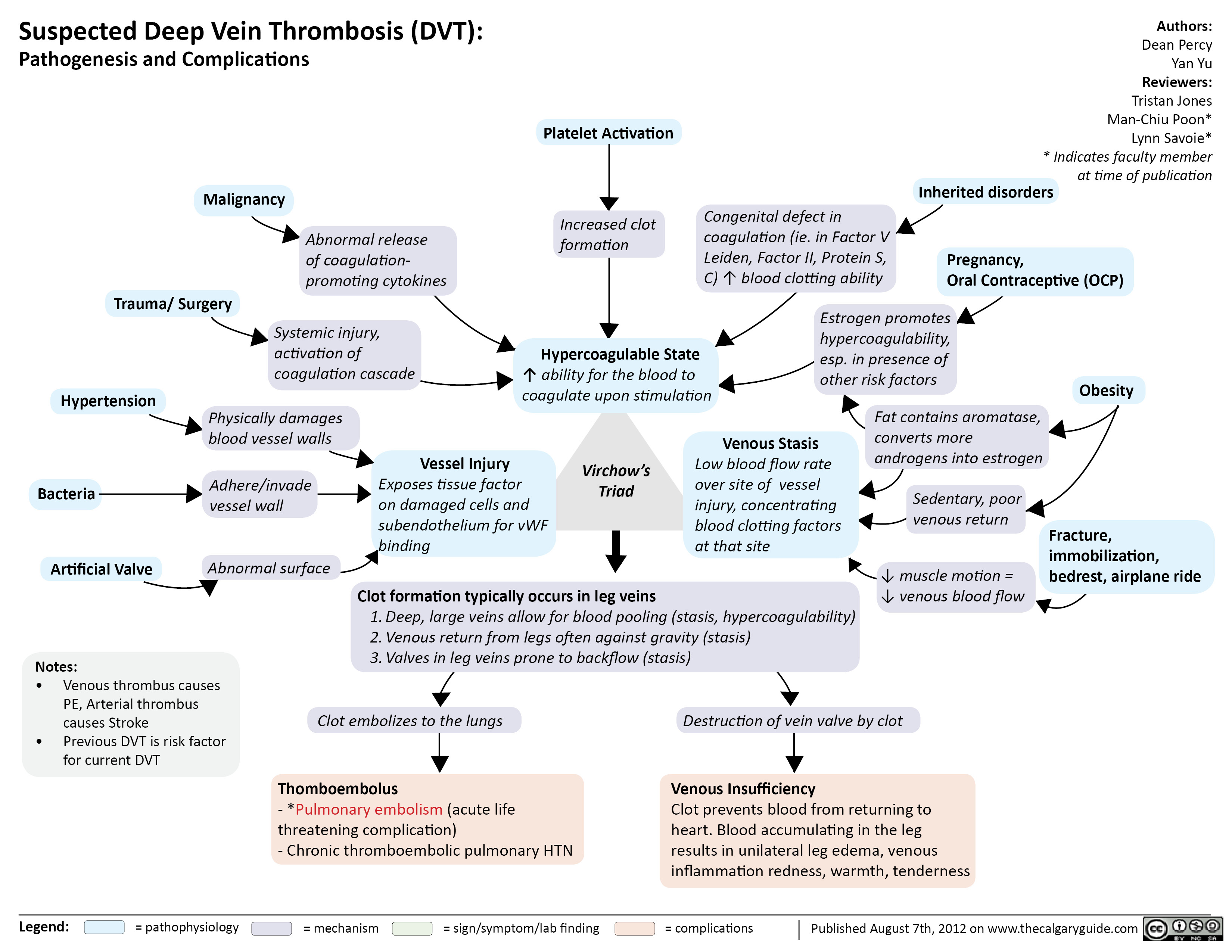
Suspected Deep Vein Thrombosis
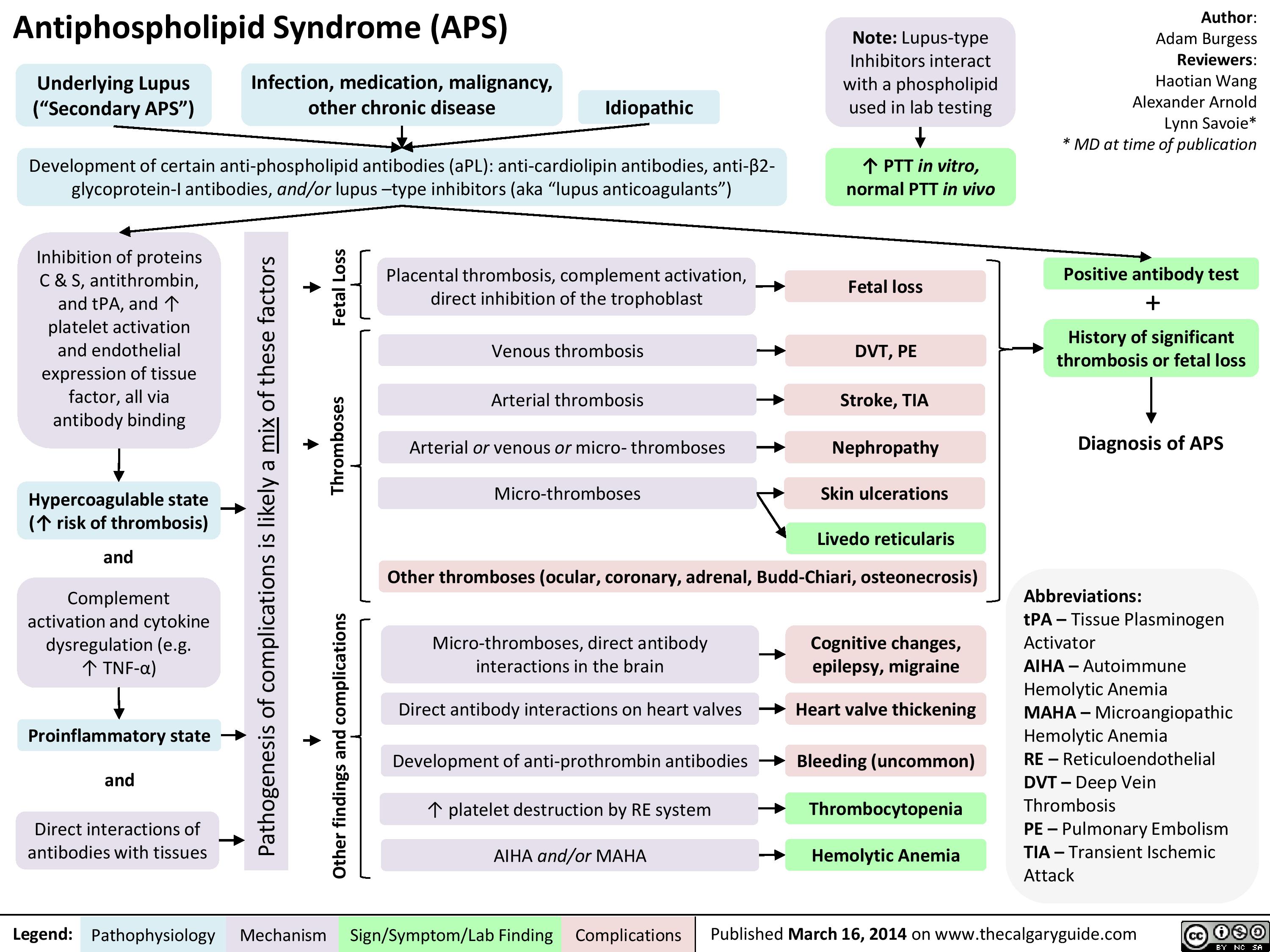
APS
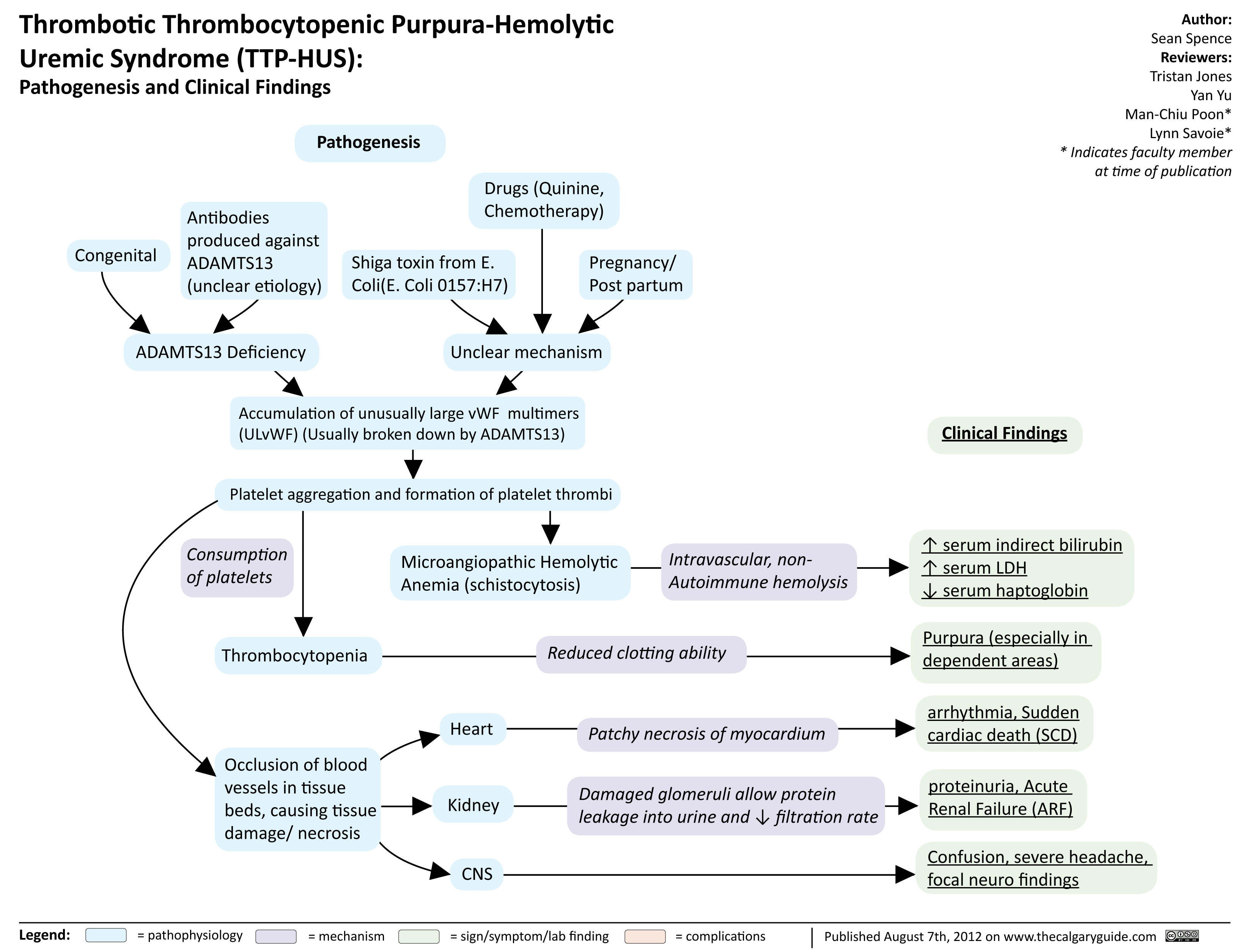
TTP HUS
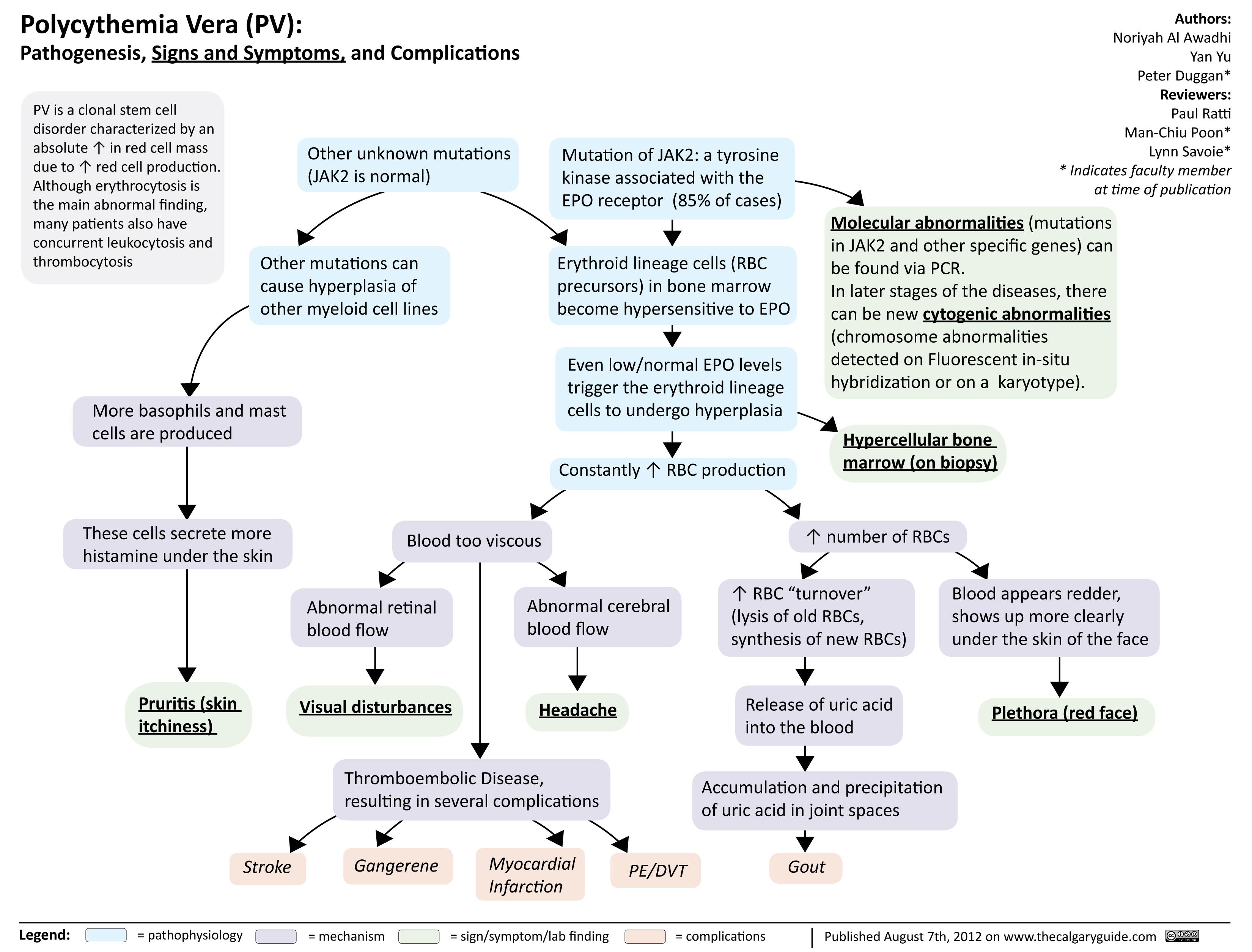
Polycythmia Vera
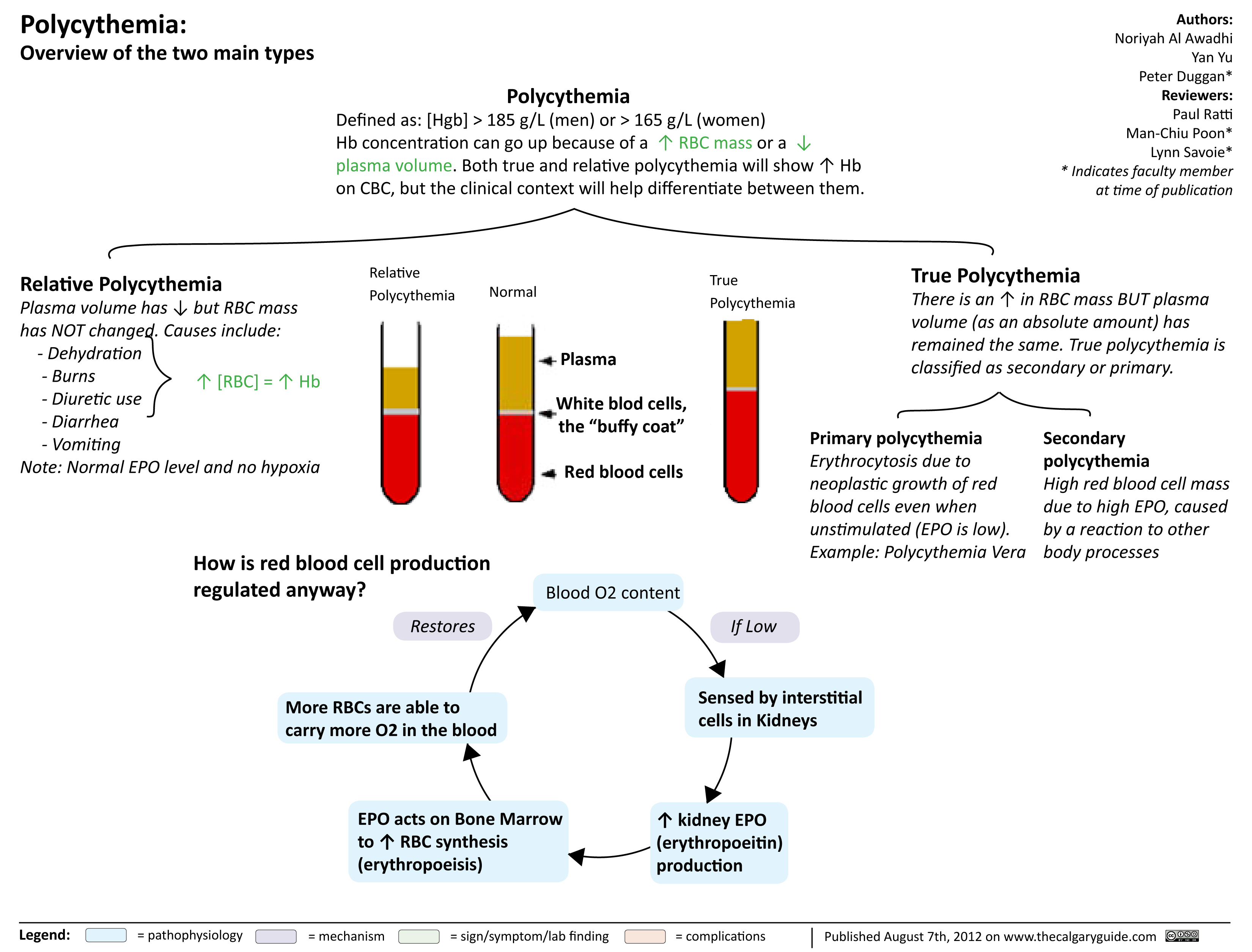
Polycythmia Overview
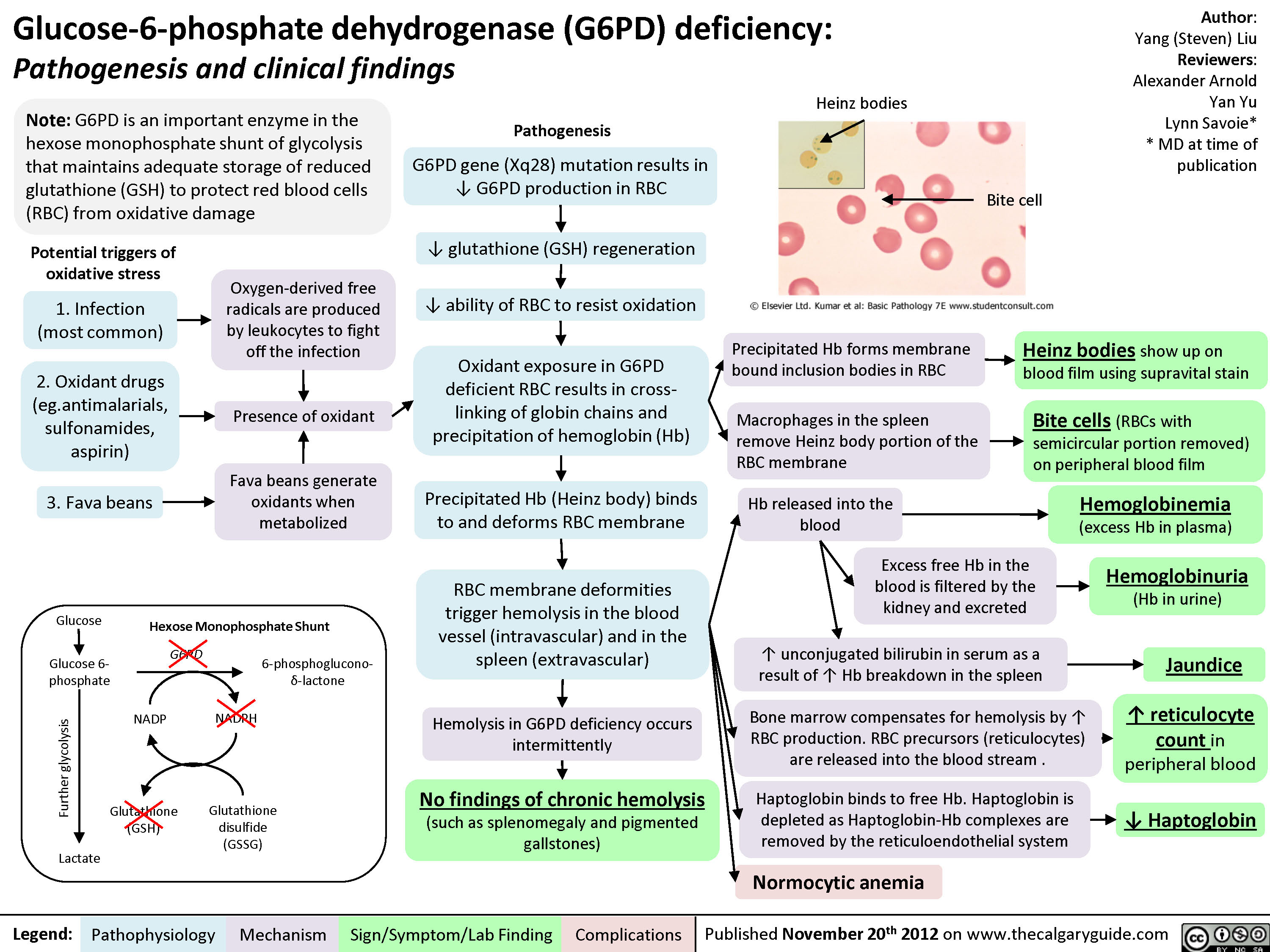
G6PD Deficiency
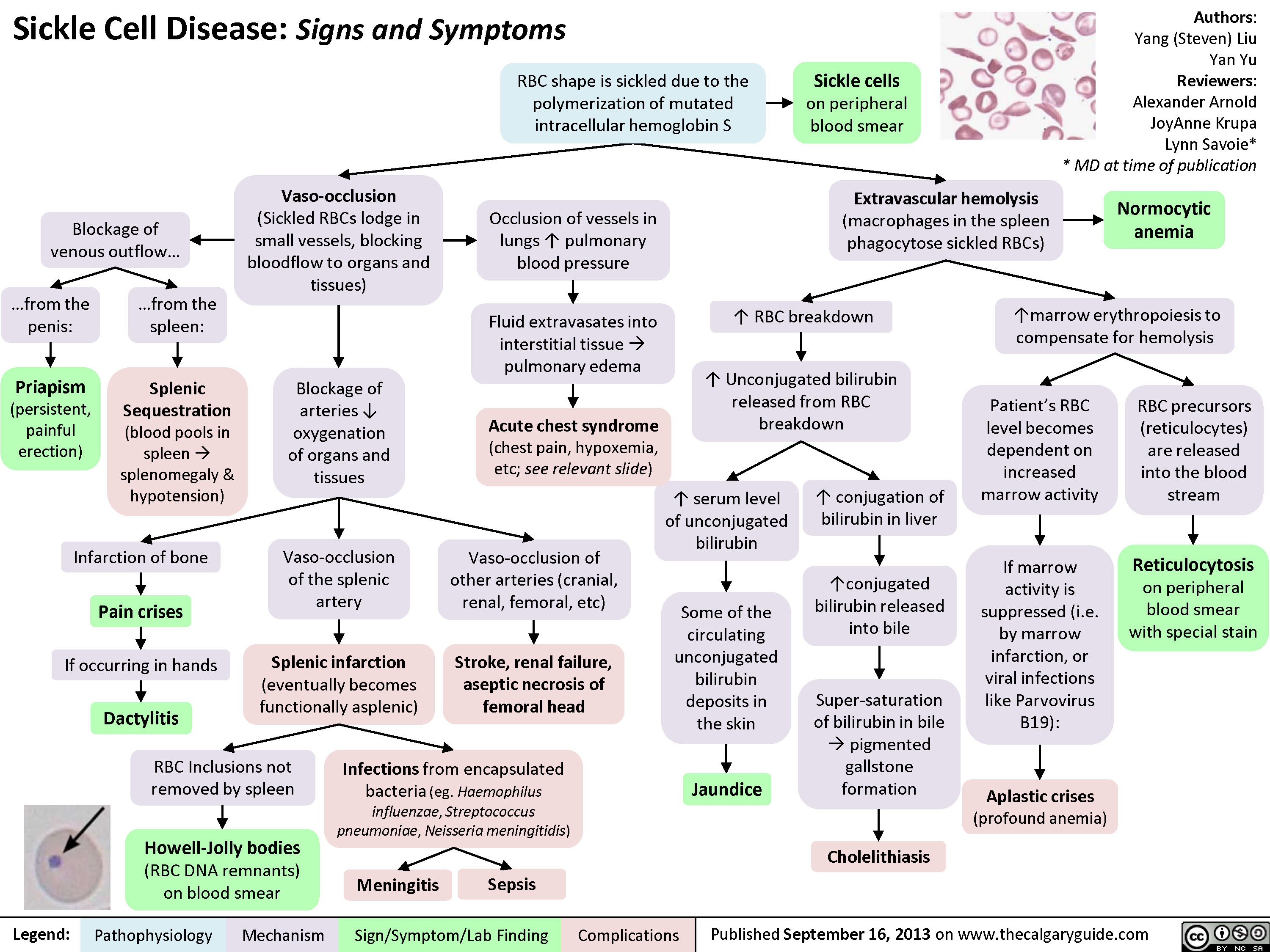
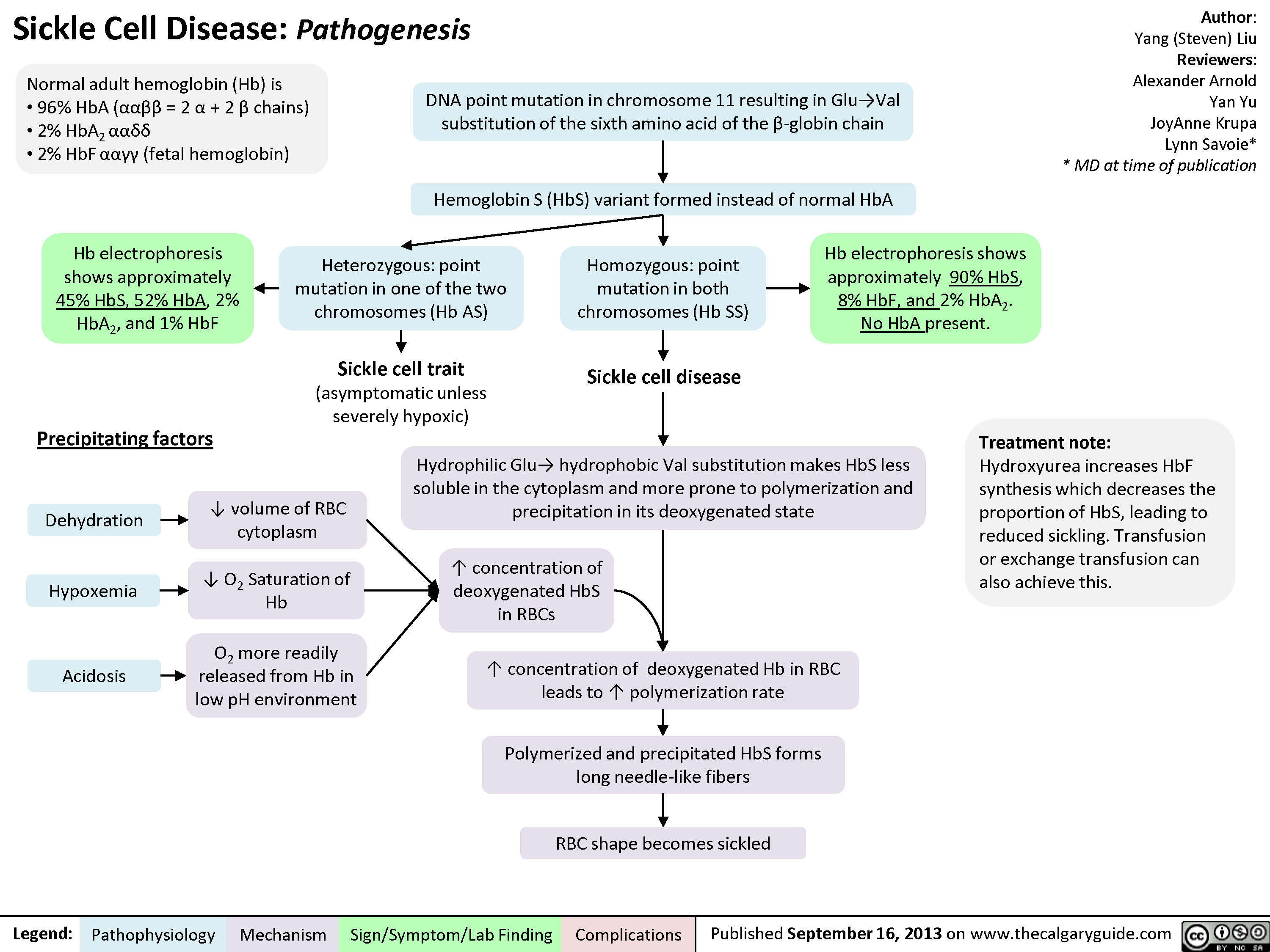
Sickle cell disease signs
Sickle cell disease
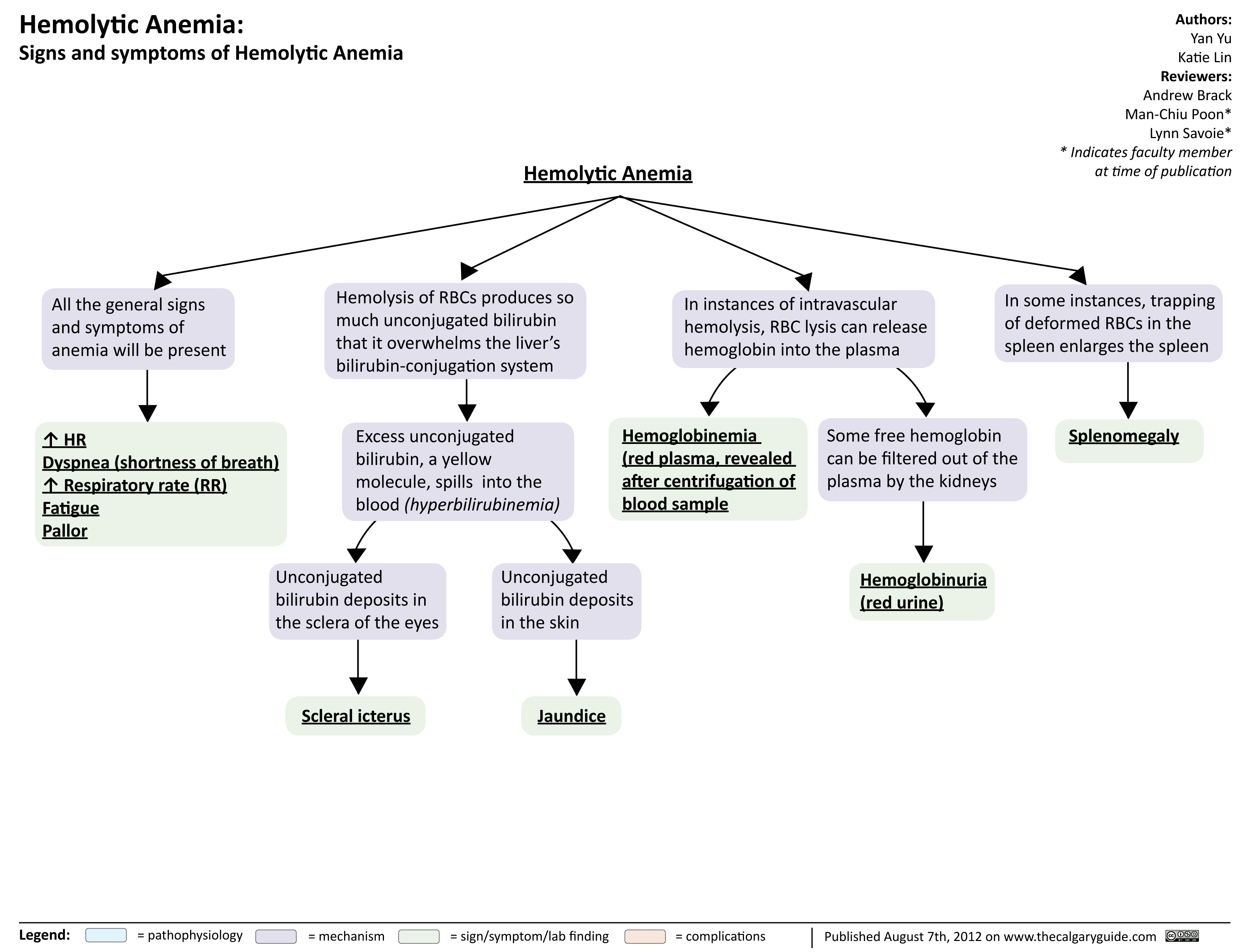
Hemolytic Anemia Signs and Symptoms
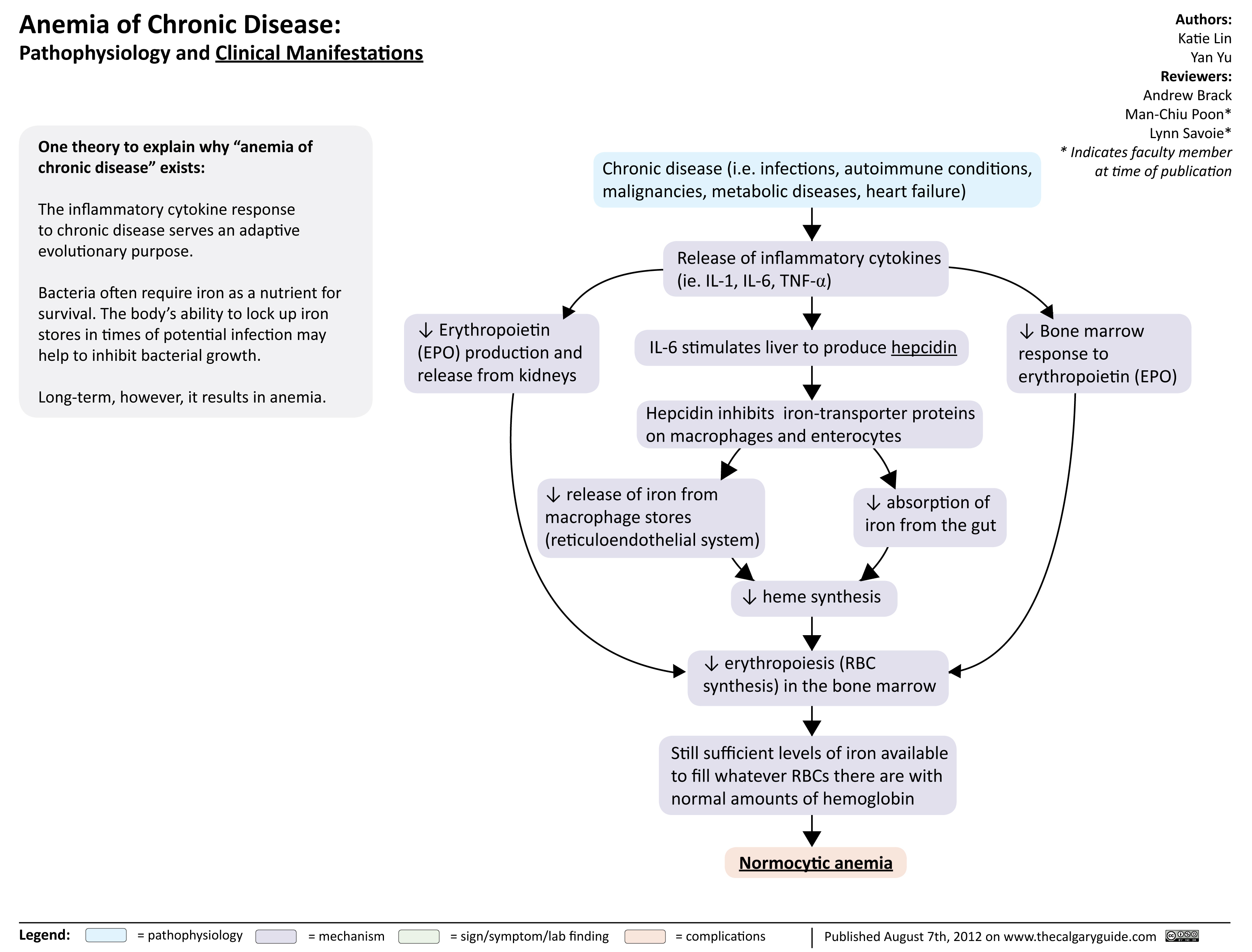
Anemia of Chronic Disease
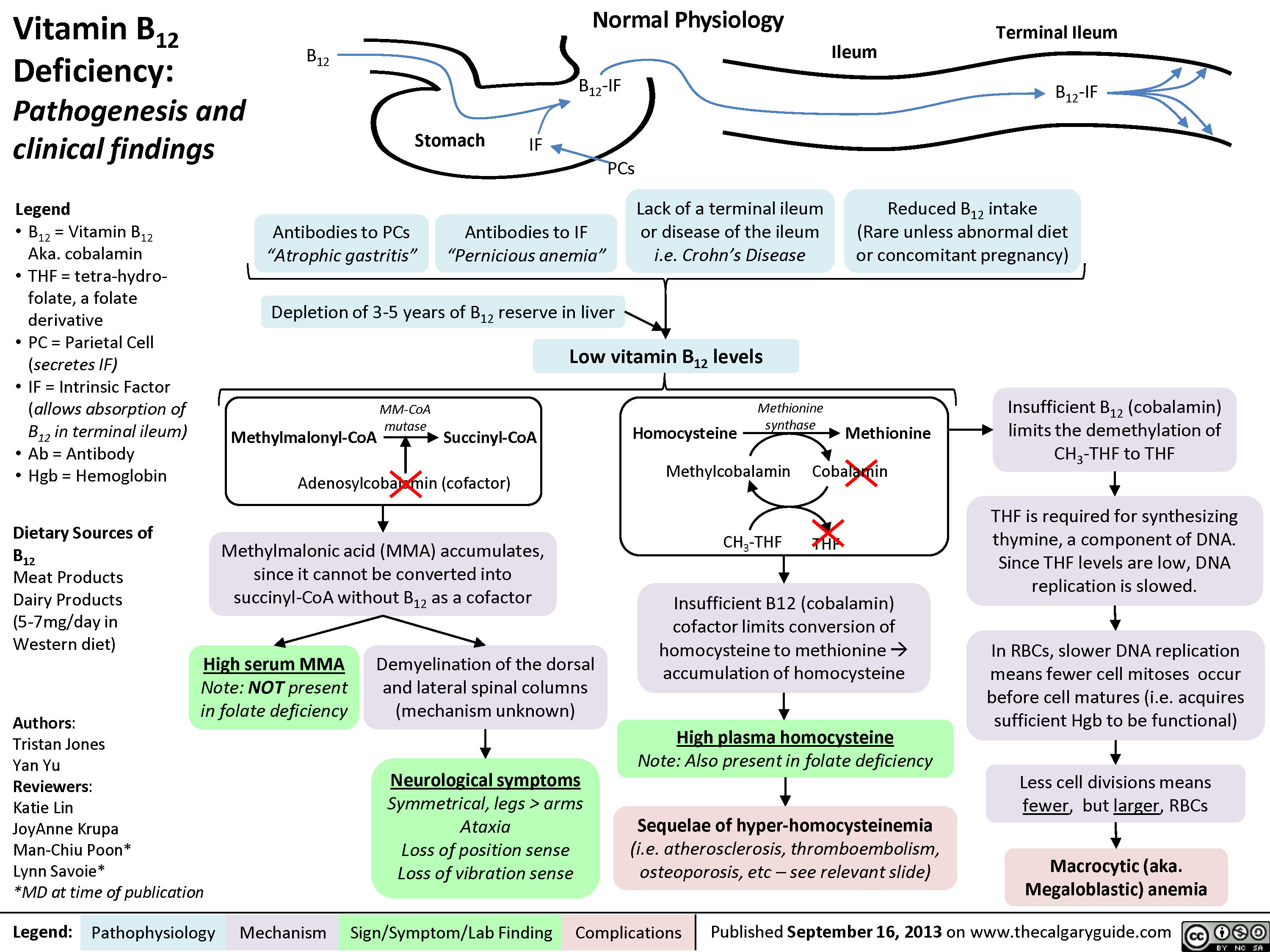
Vitamin B12 Deficiency
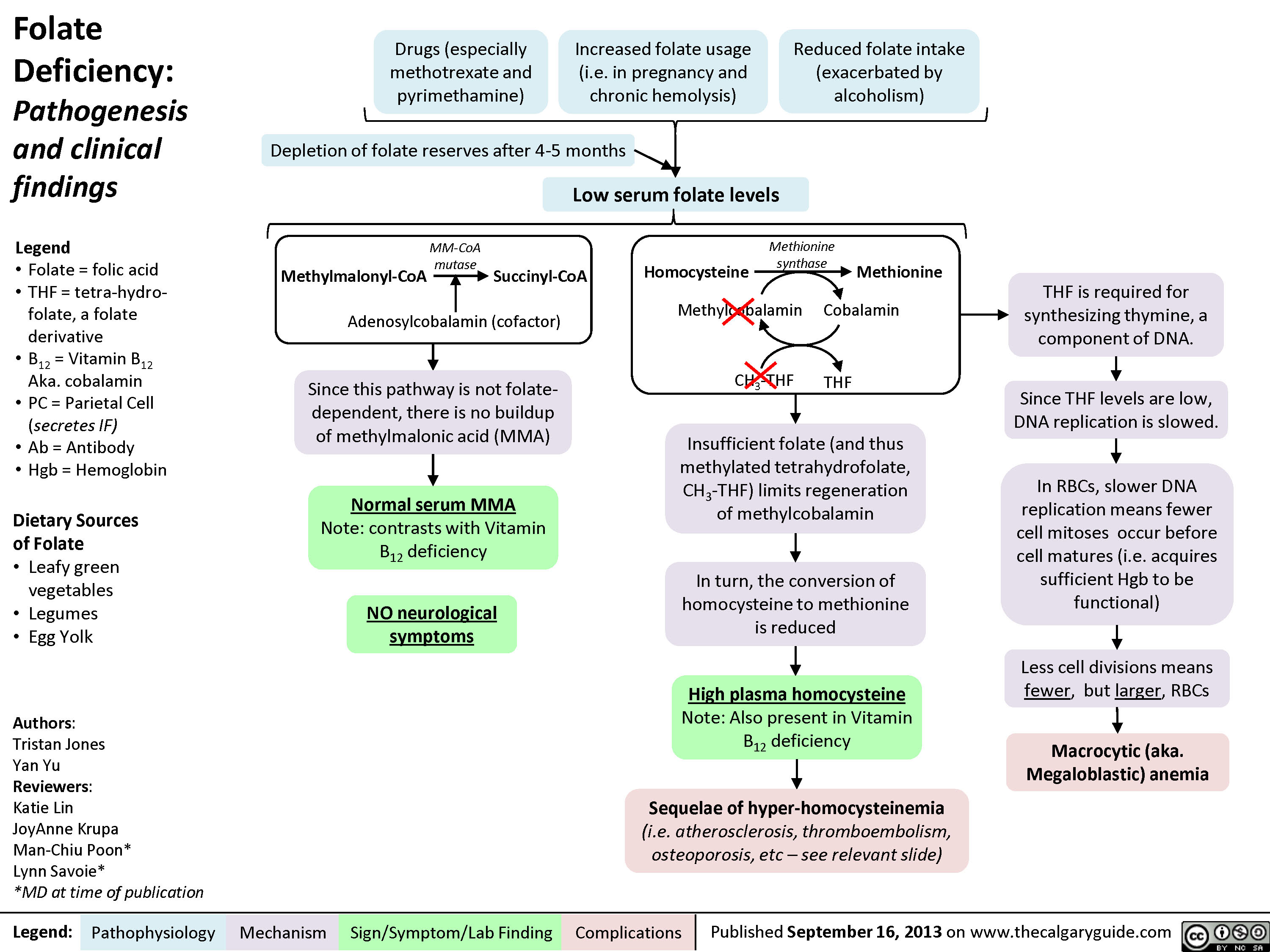
Folate Deficiency
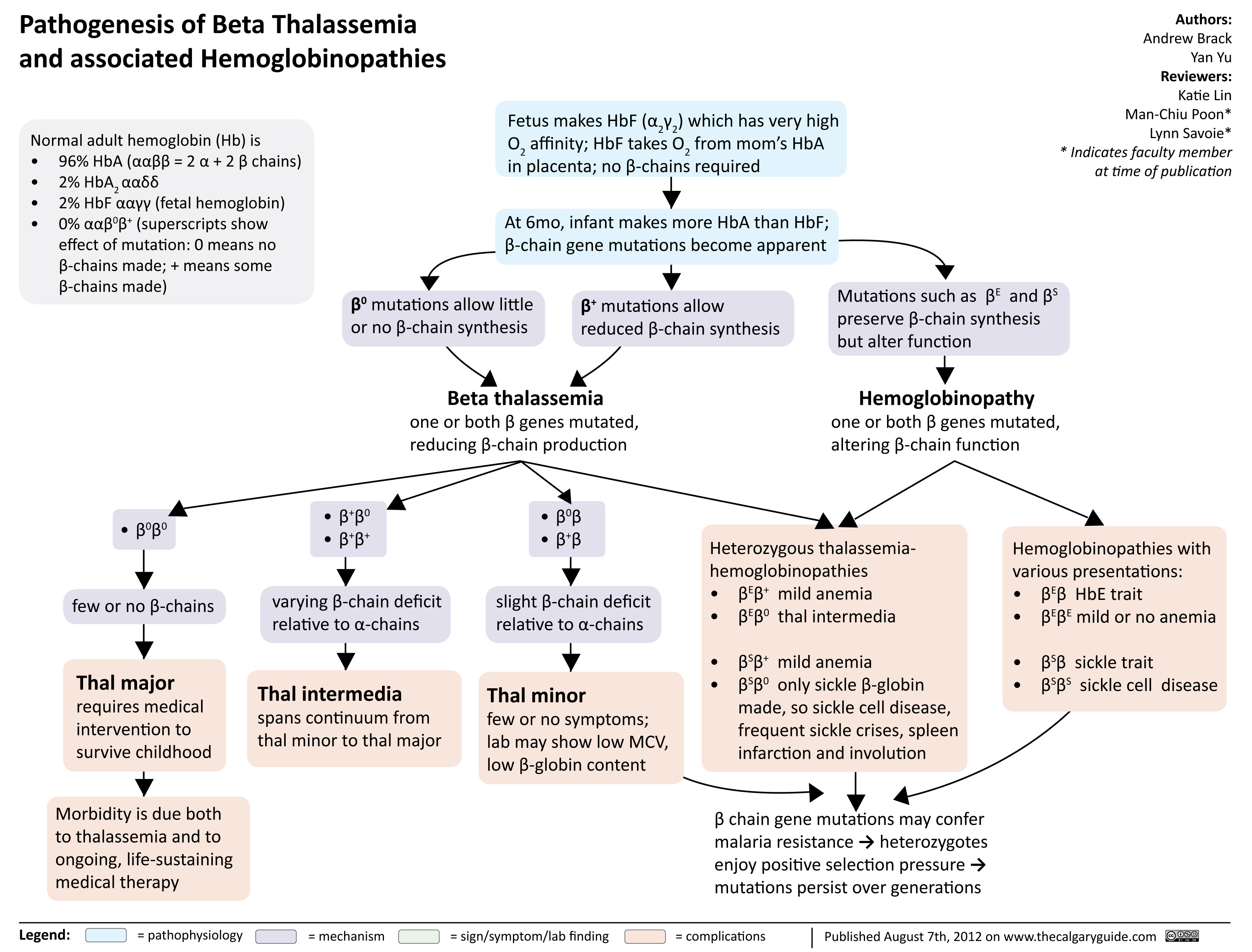
Pathogenesis of Beta Thalassemia
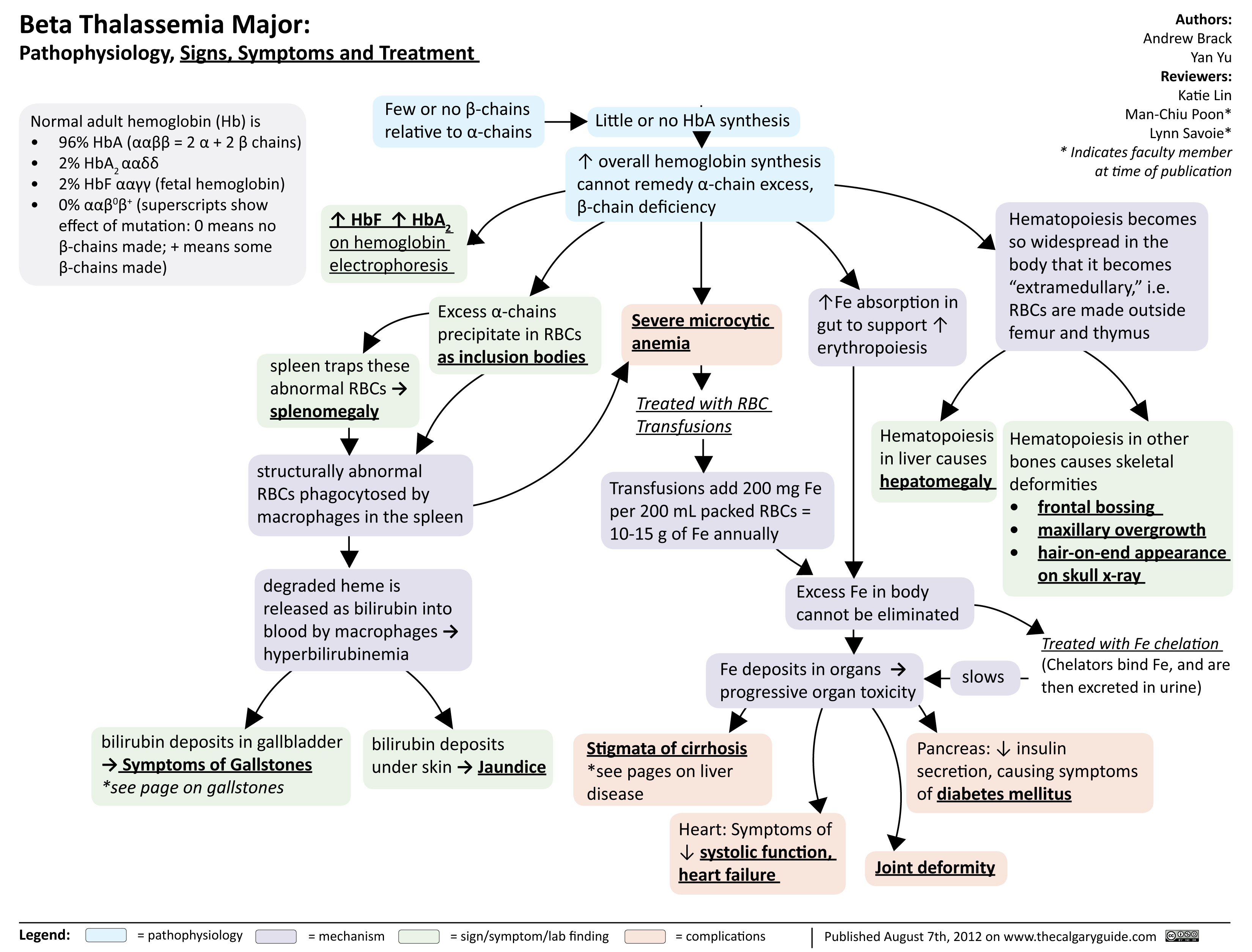
Beta Thalassemia Signs Symptoms Treatment
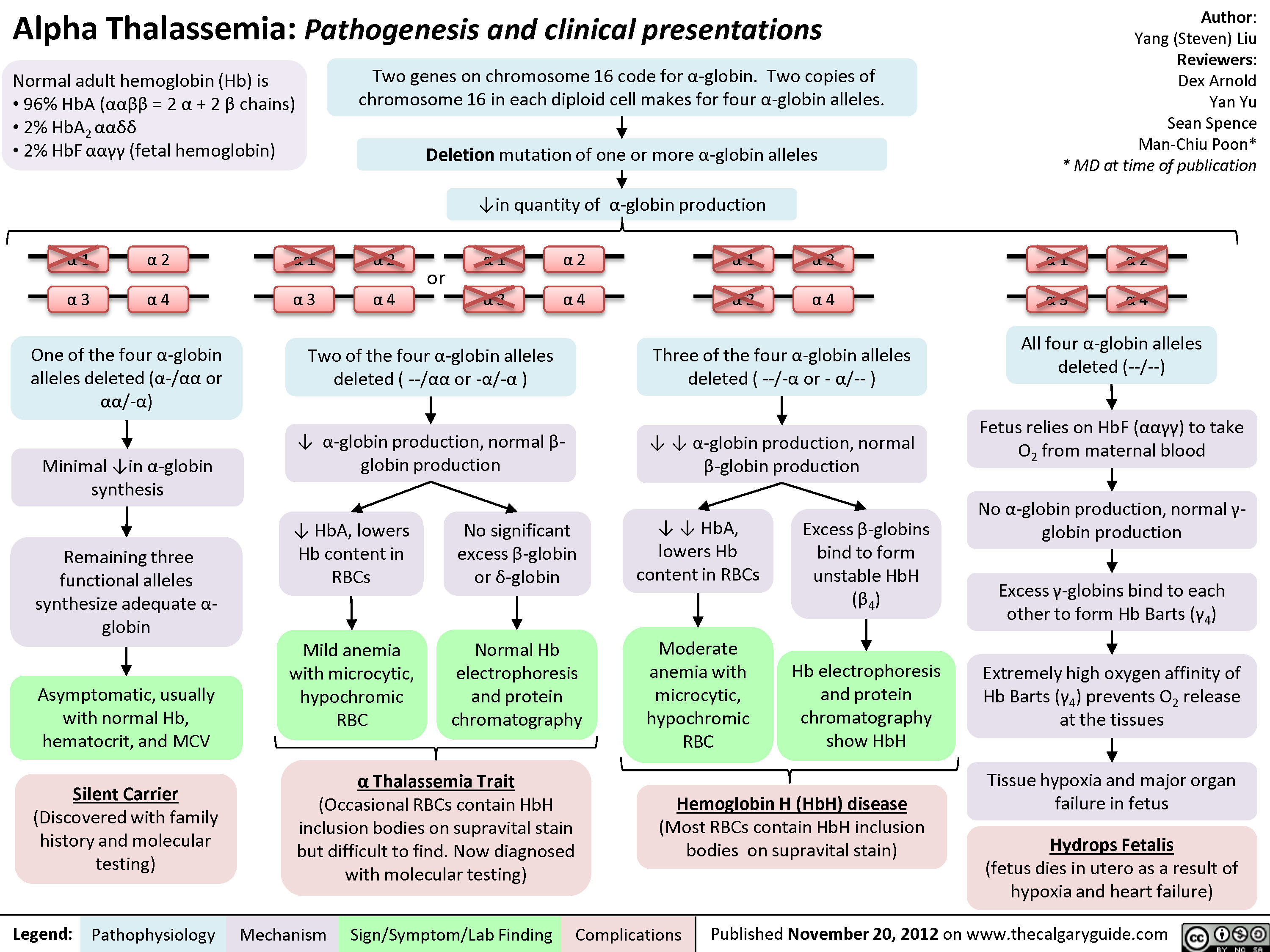
Alpha Thalassemia Pathogenesis
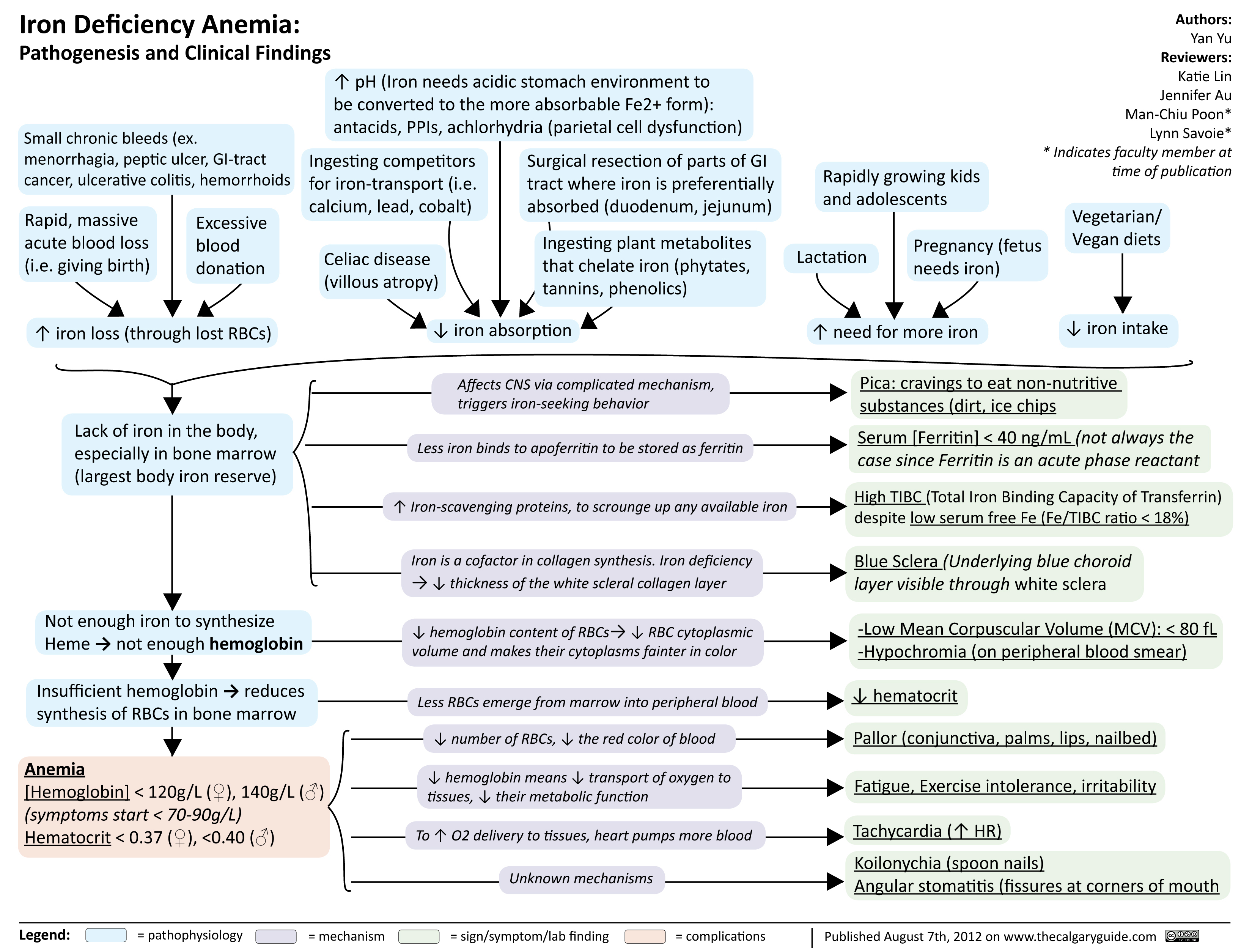
Iron Deficiency Anemia
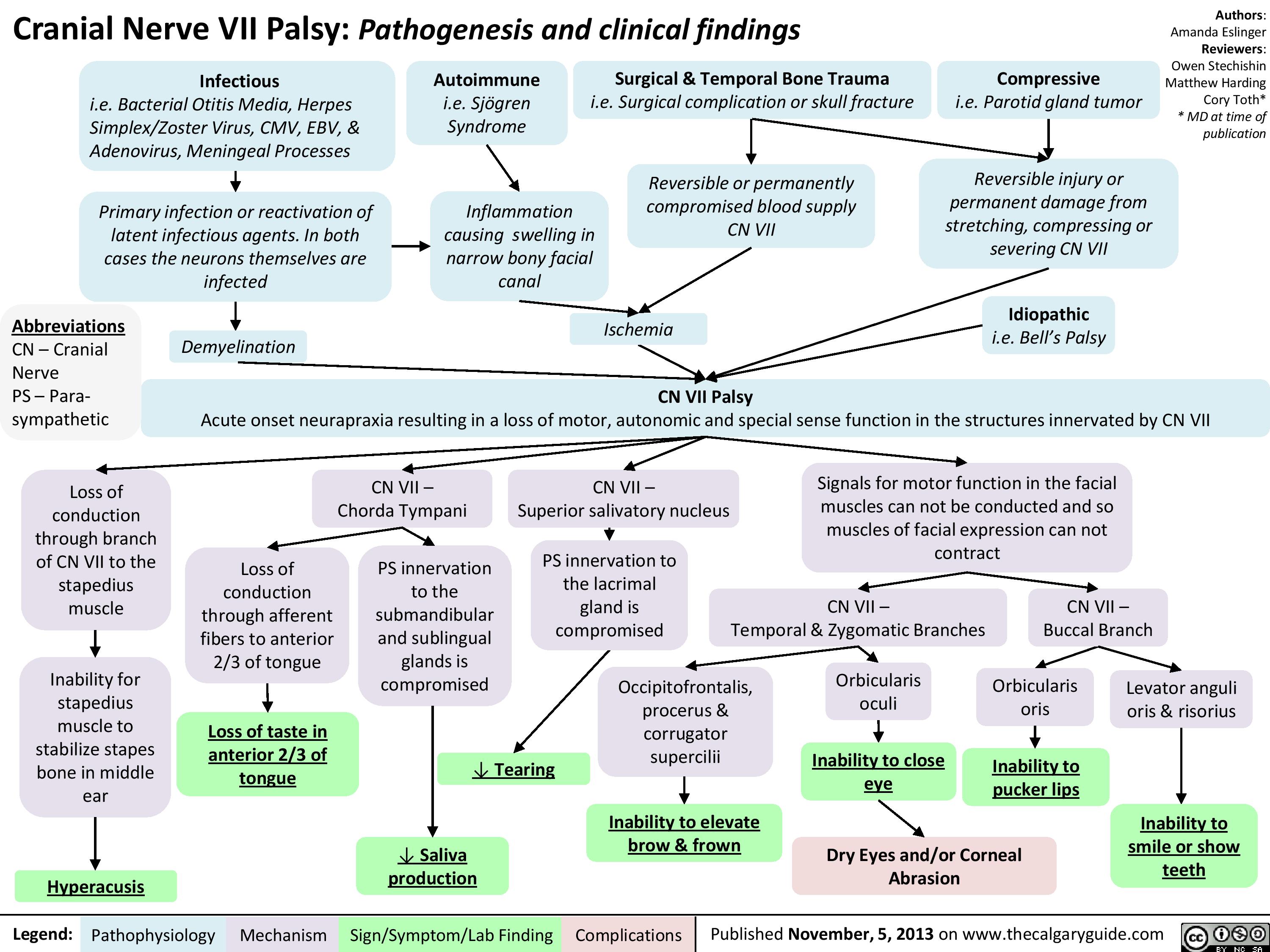
CNVII_Bells Palsy
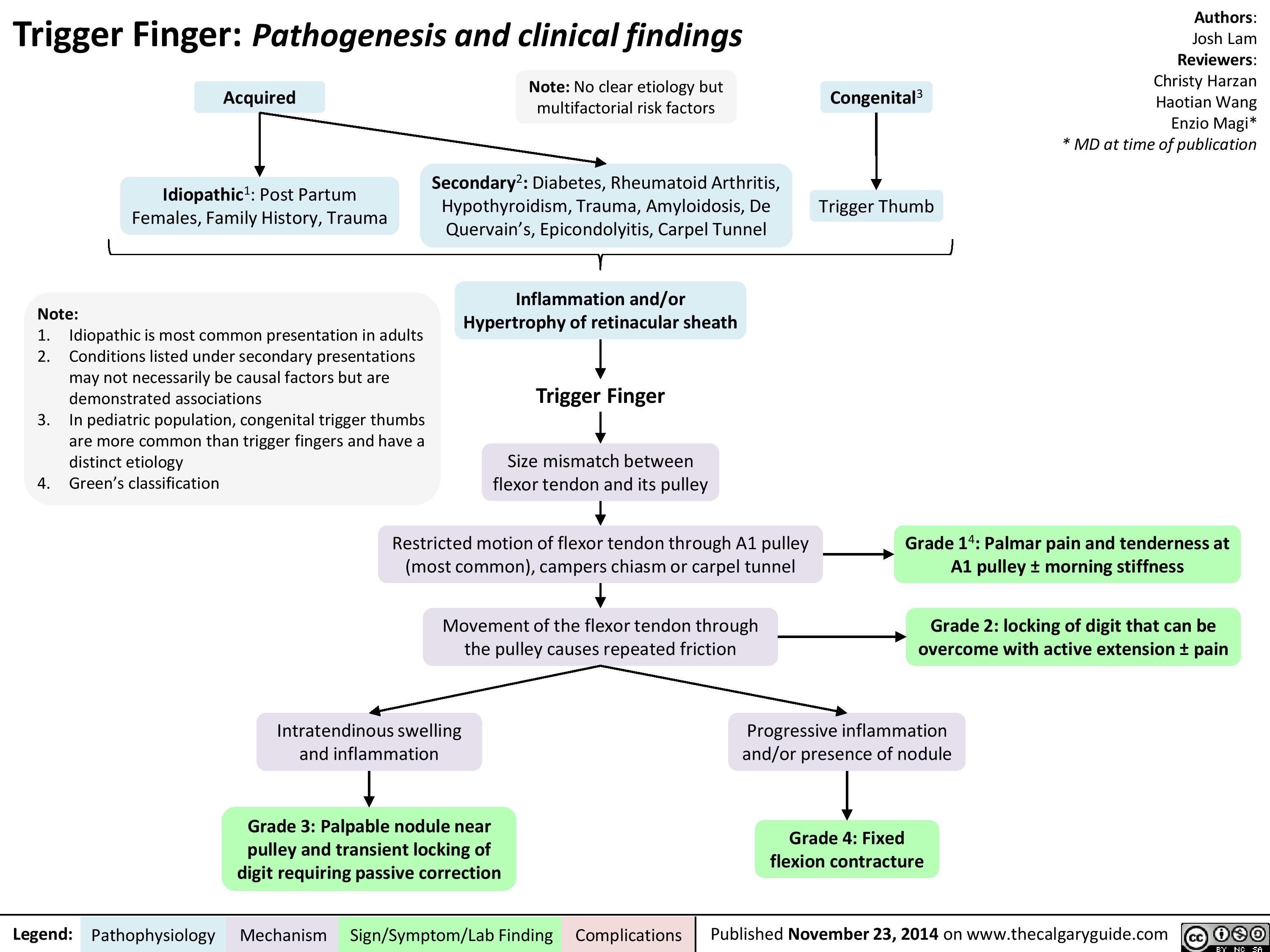
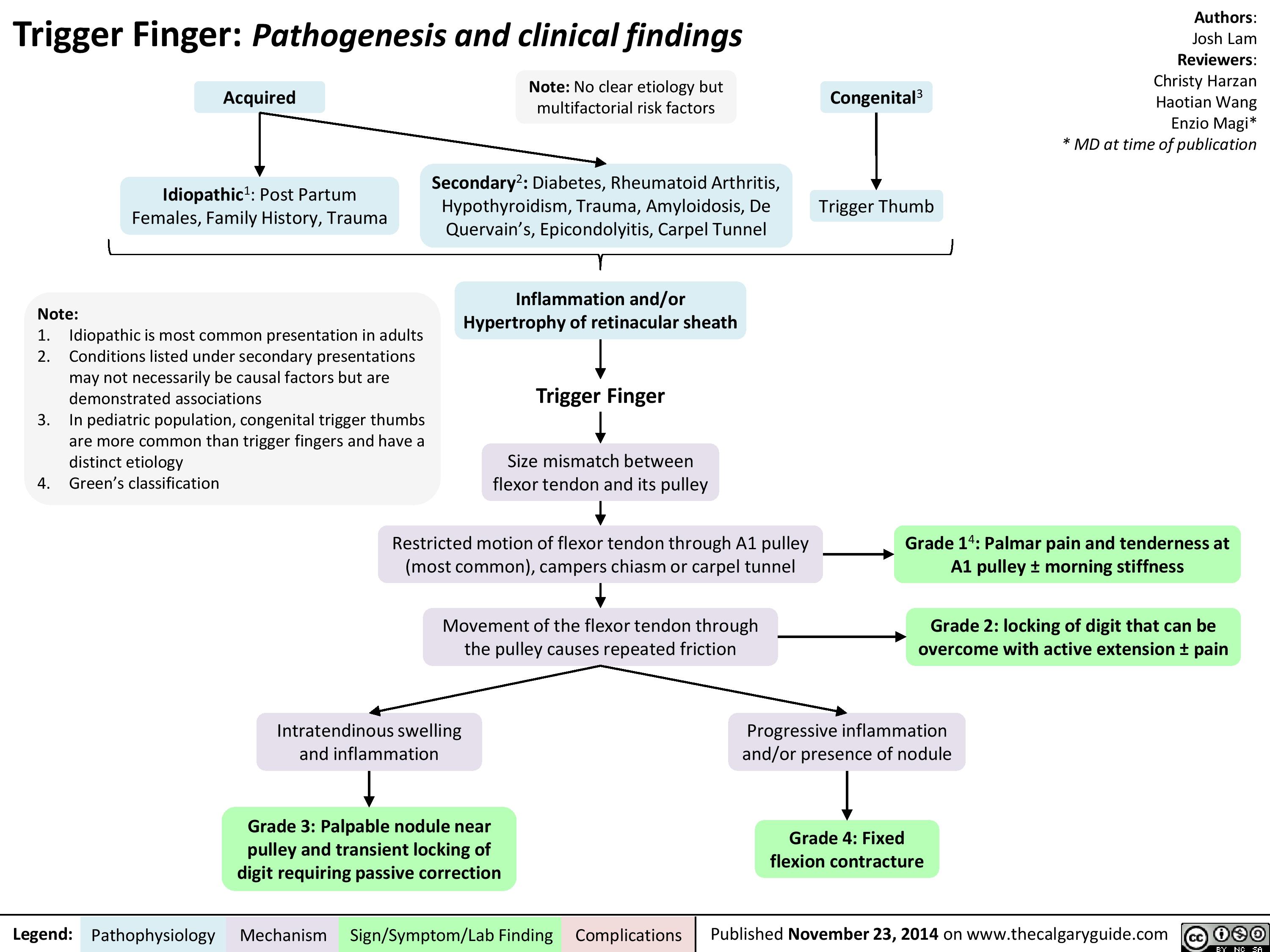
Trigger Finger
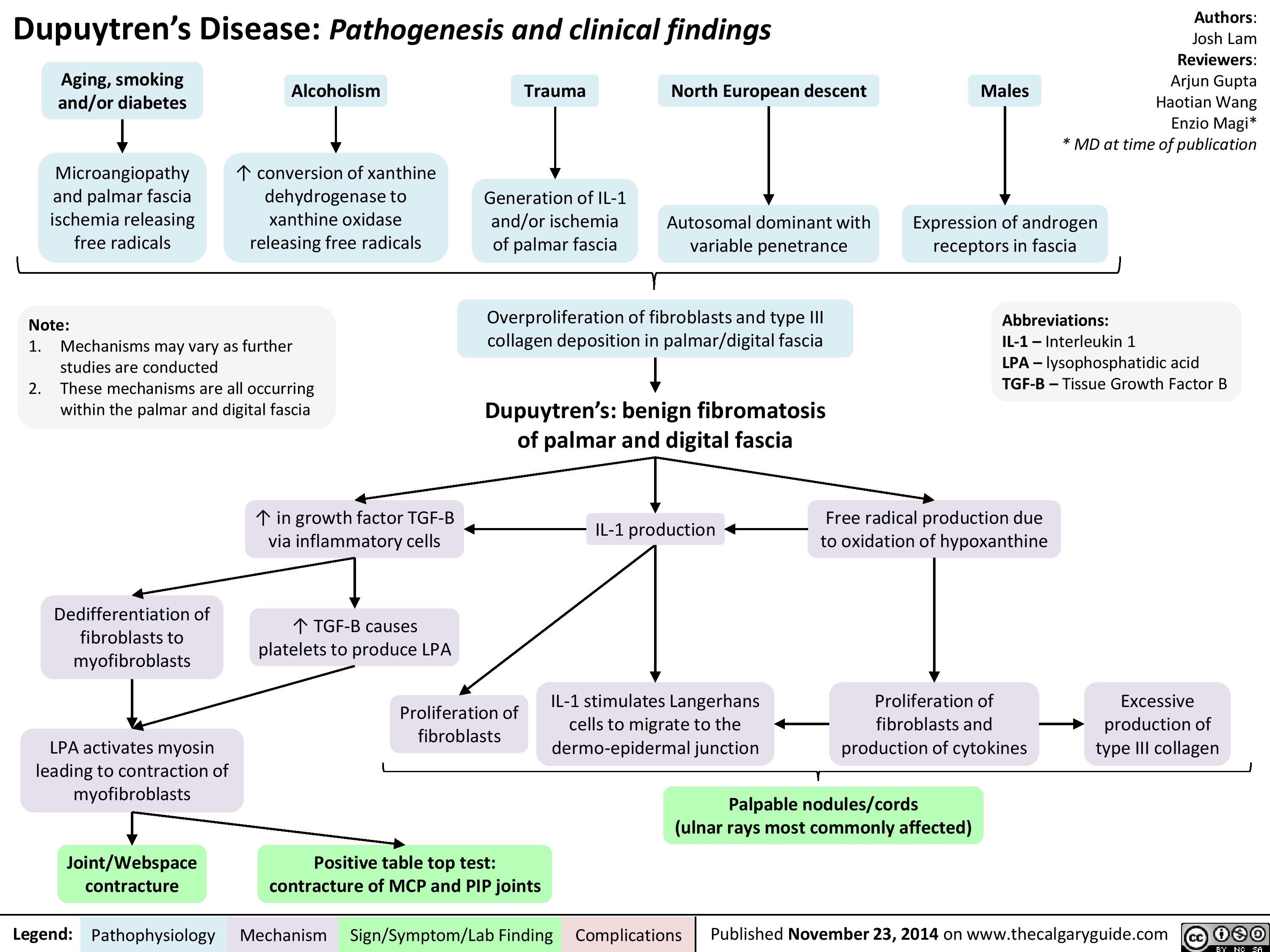
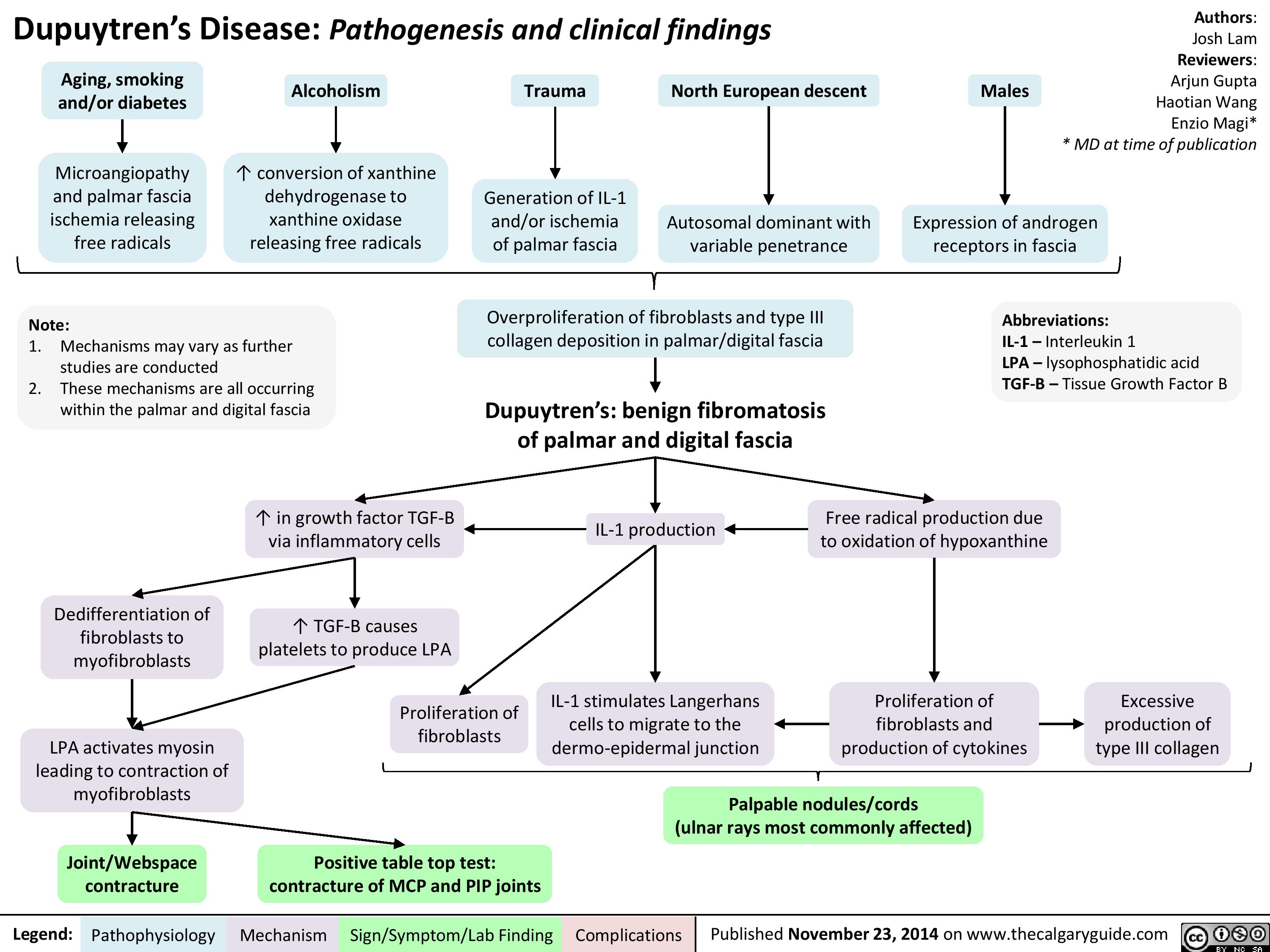
Dupuytren
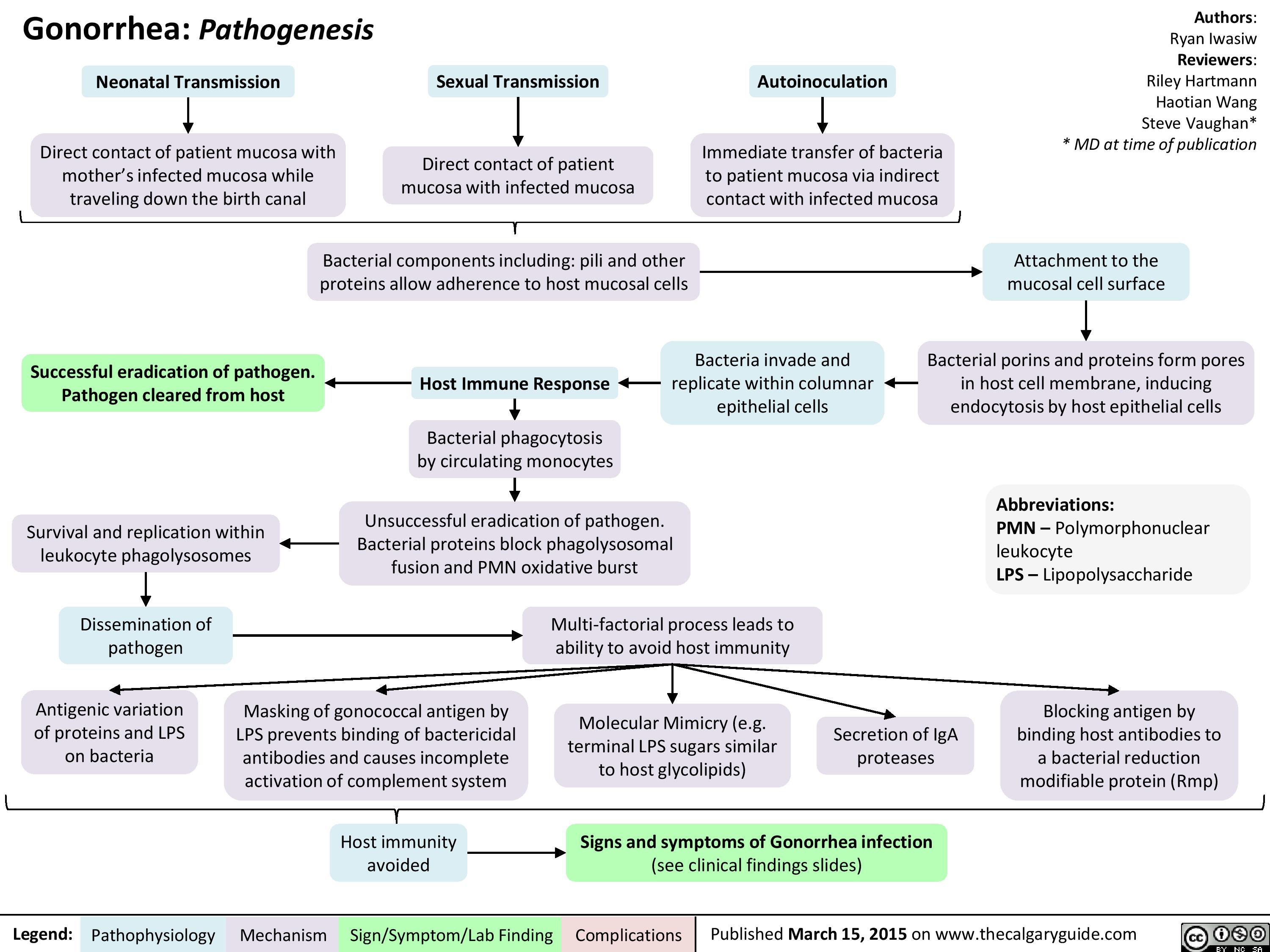
Gonorrhea Pathogenesis
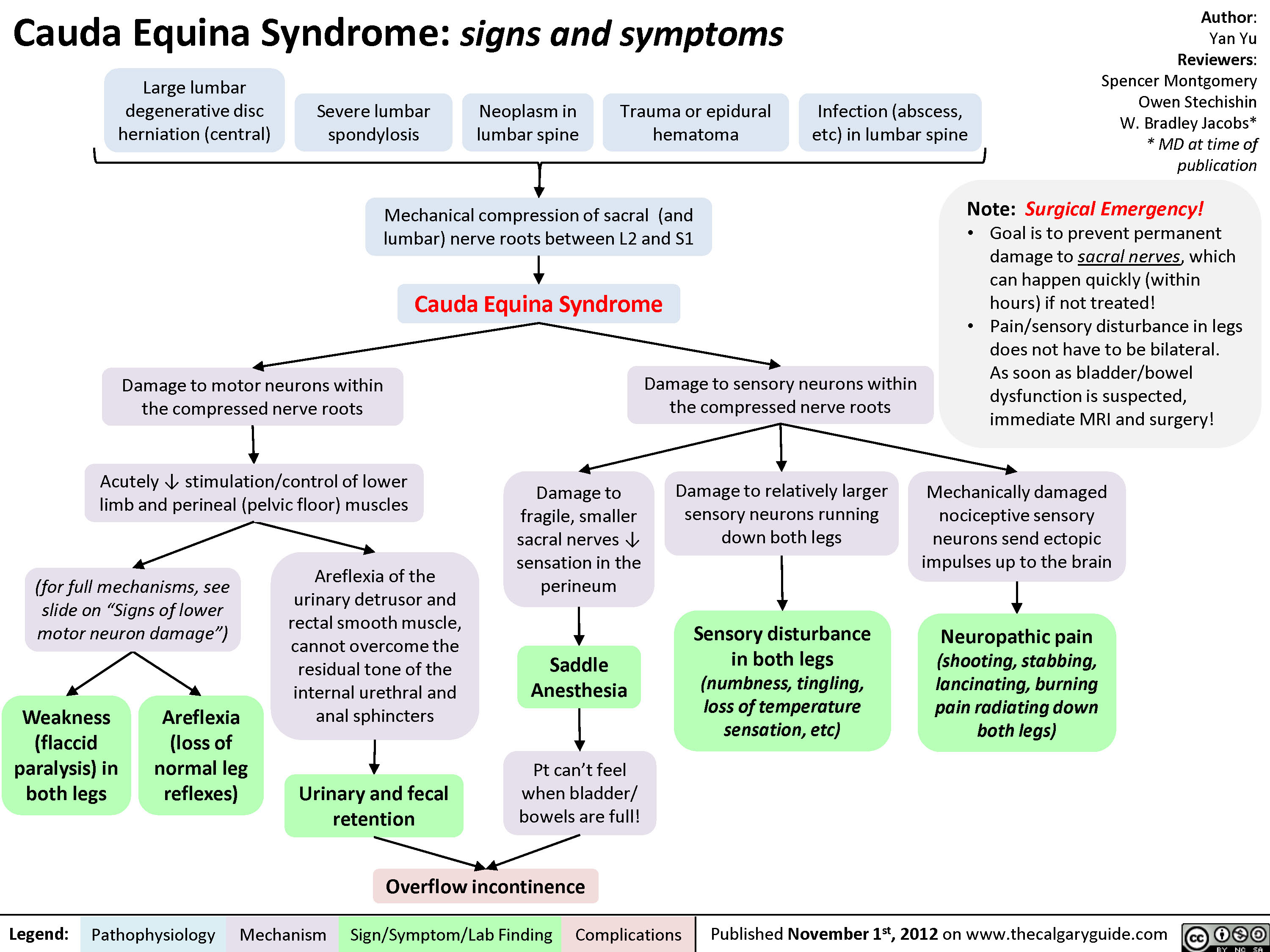
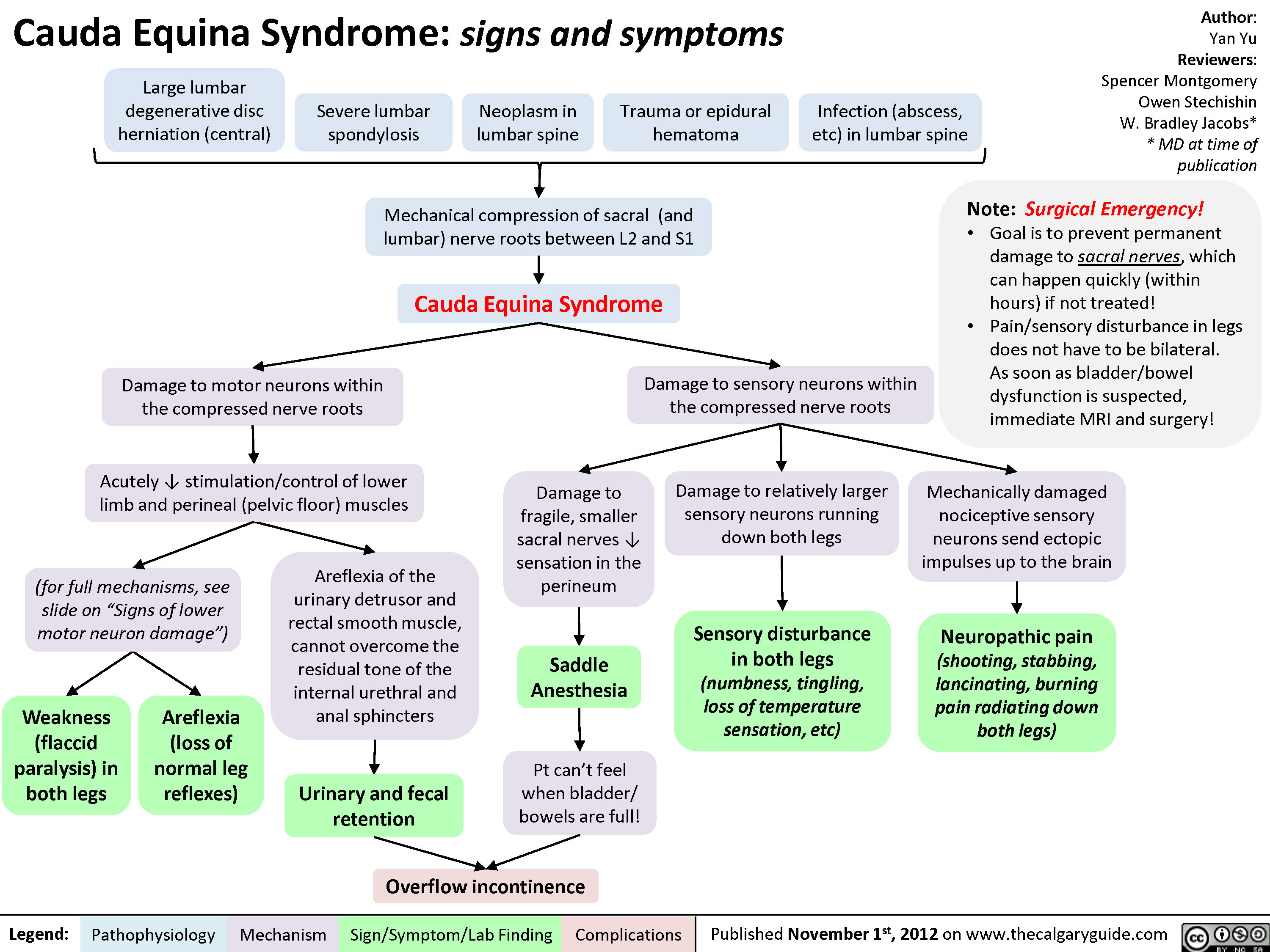
Cauda Equina Syndrome
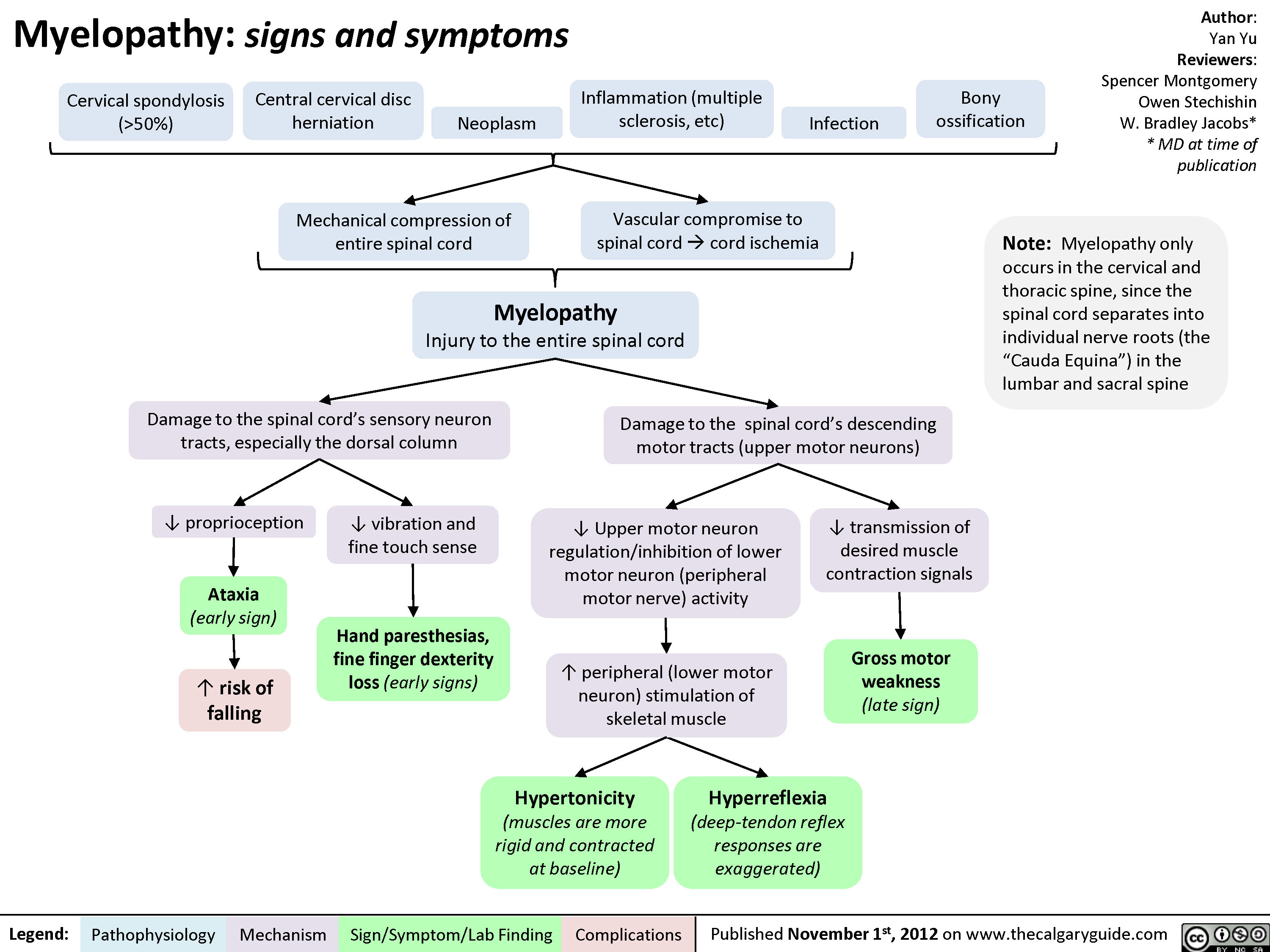
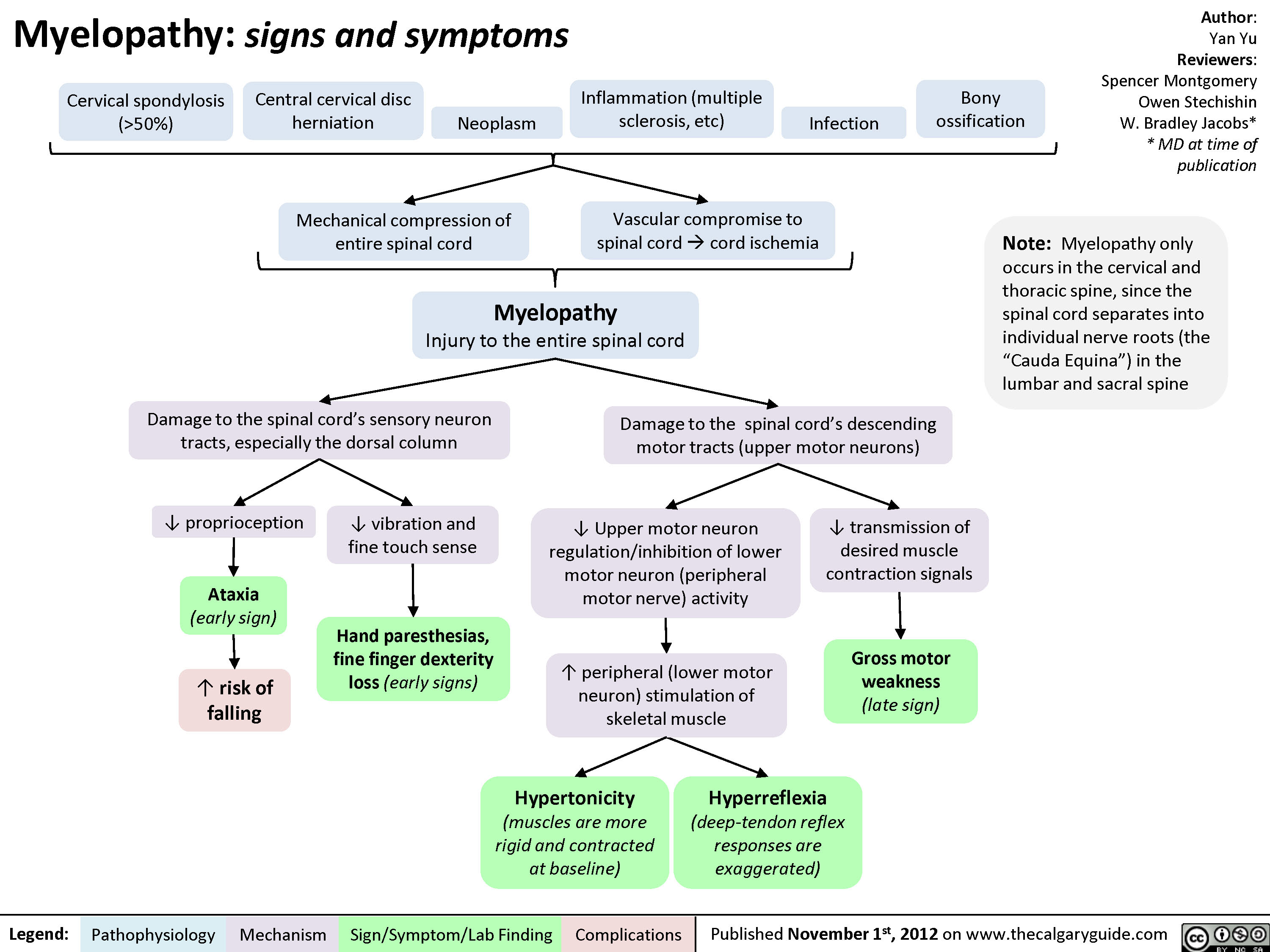
Myelopathy
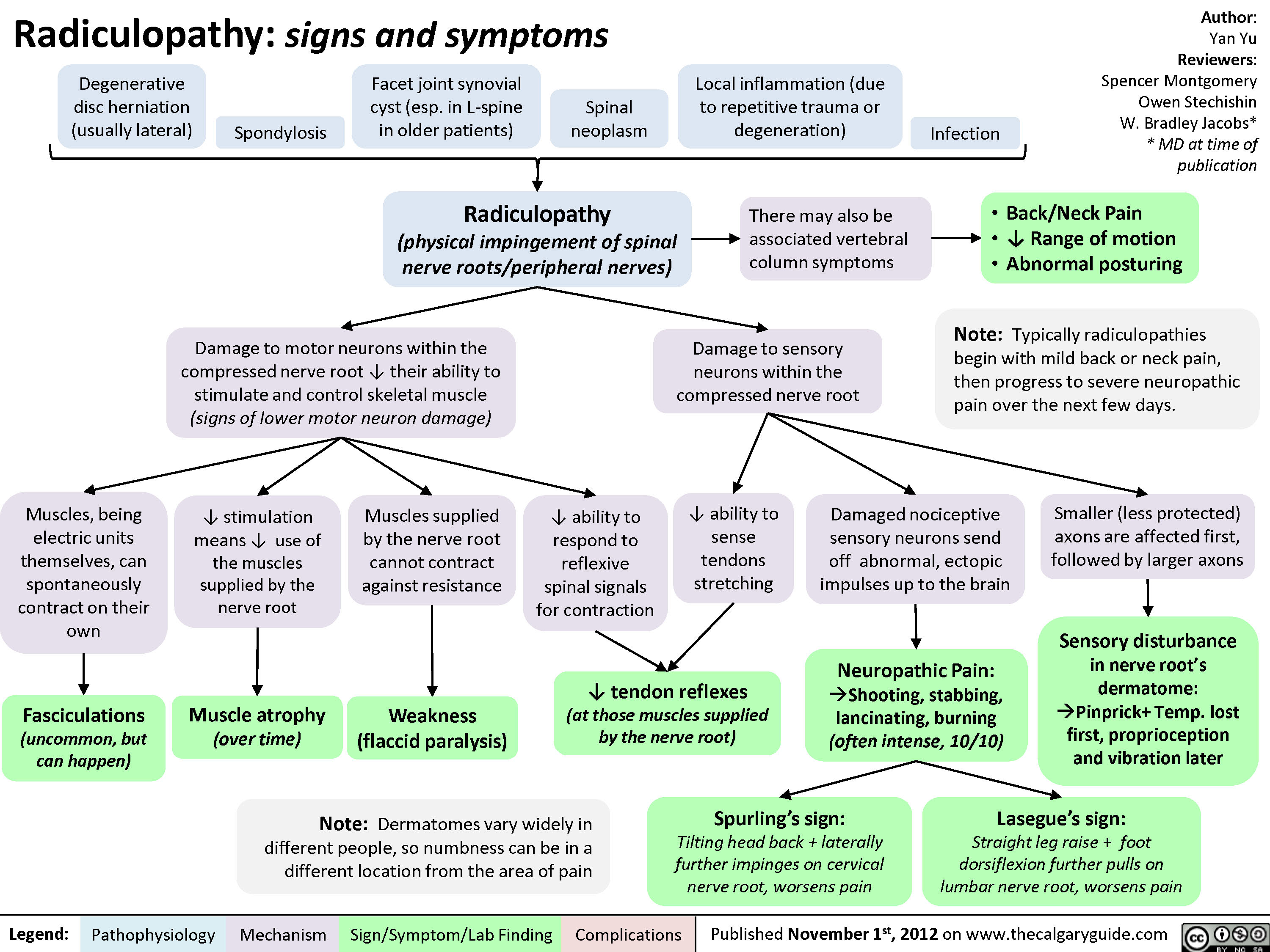
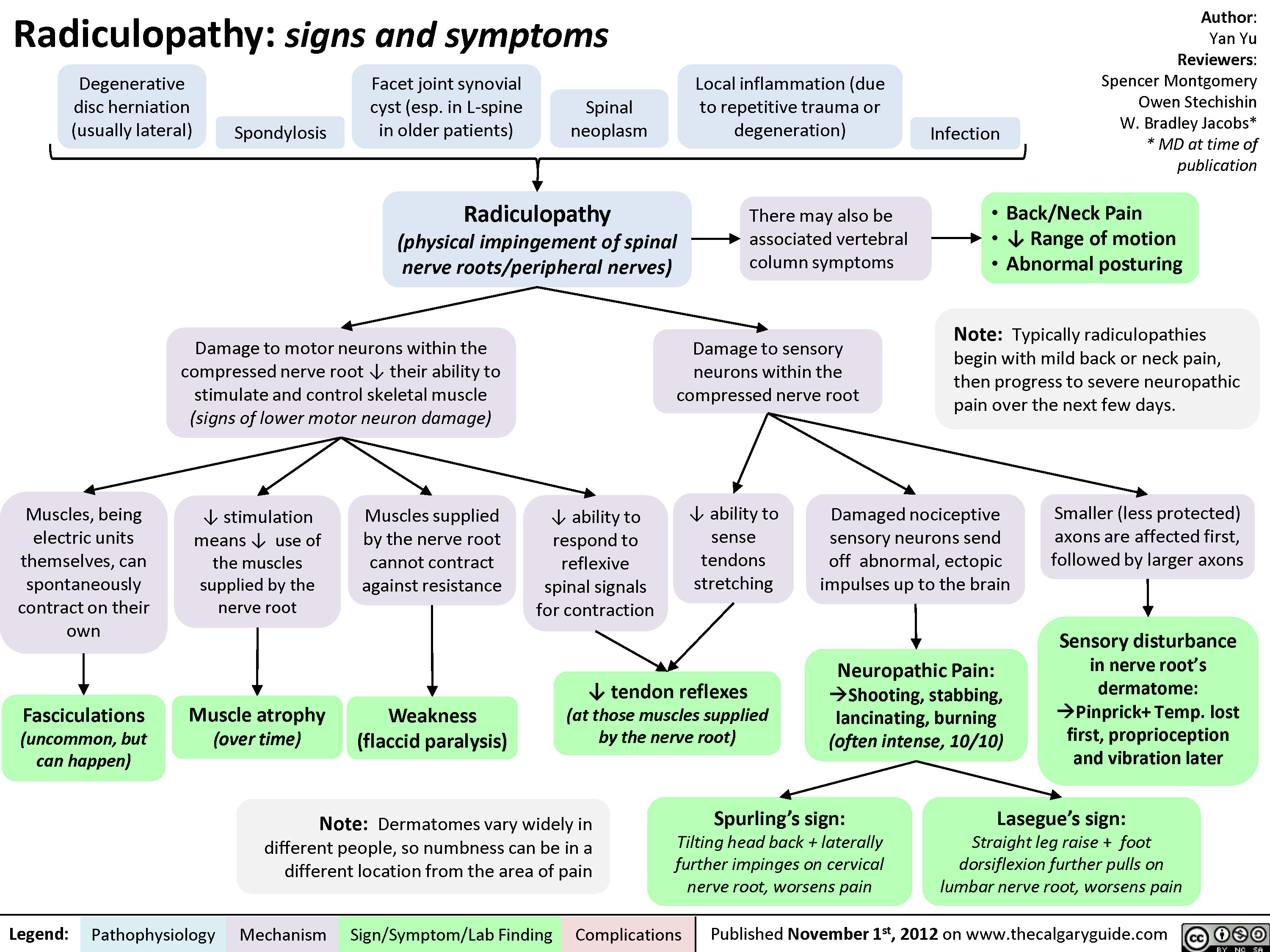
Radiculopathy
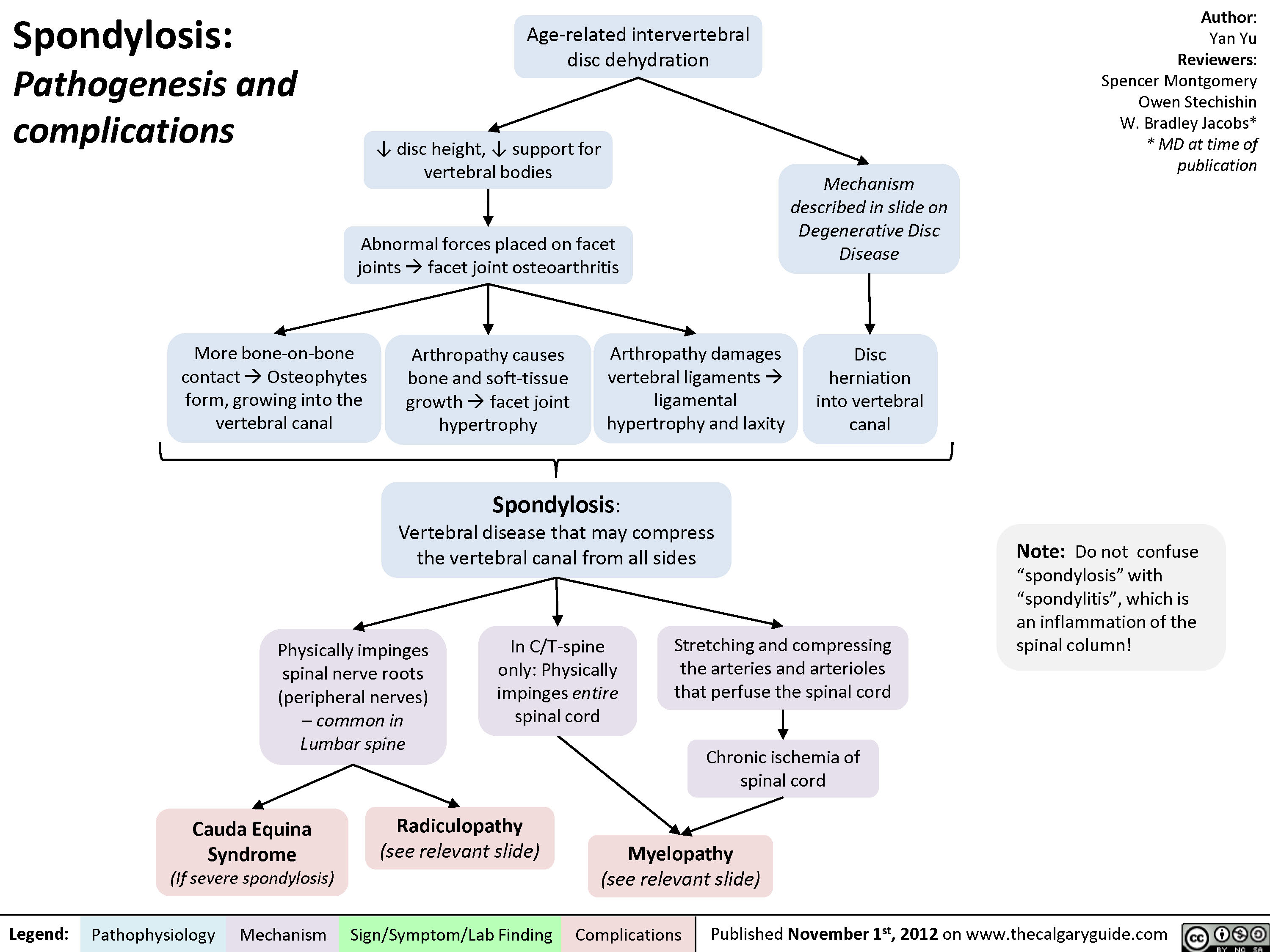
Spondylosis
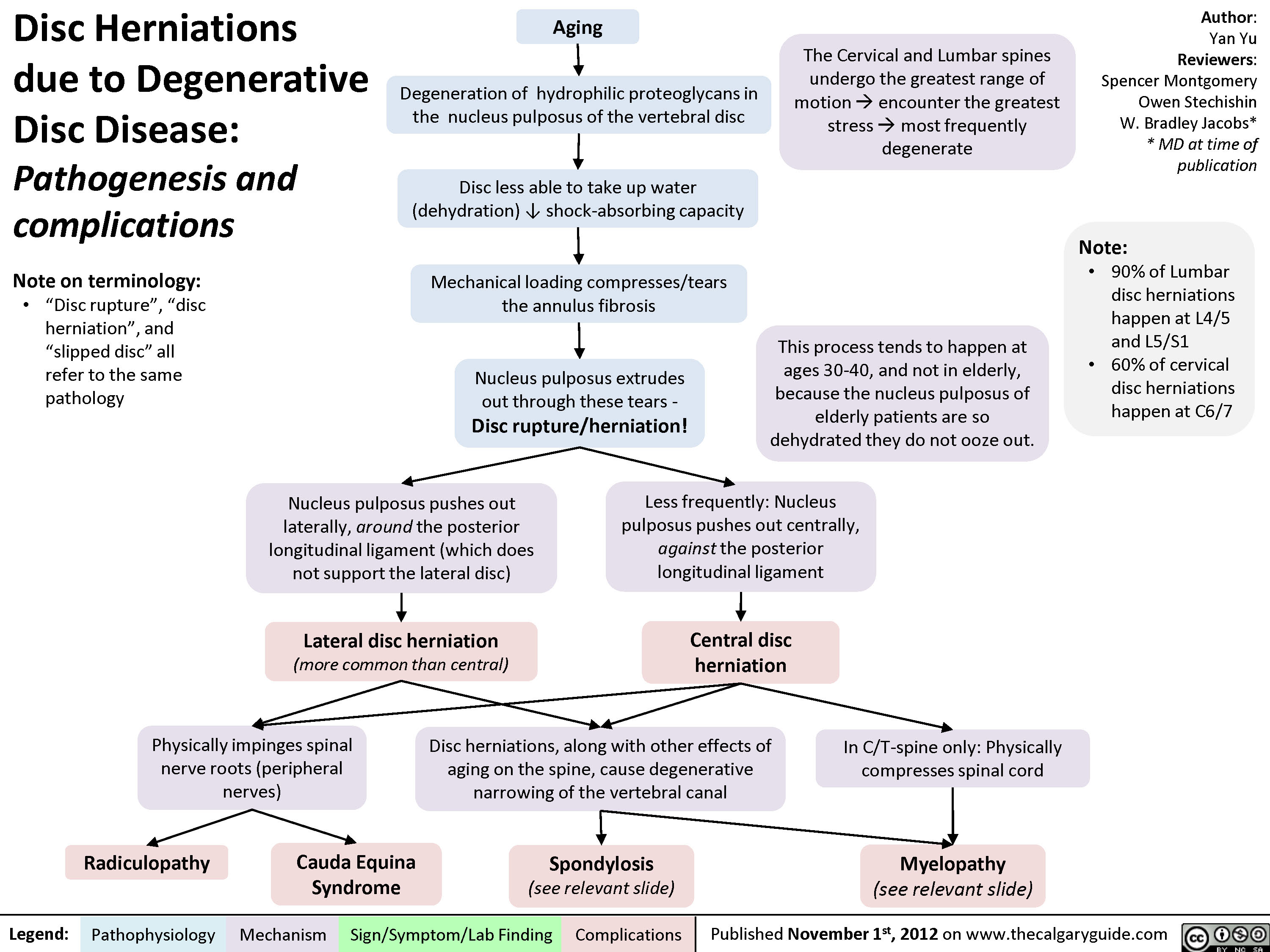
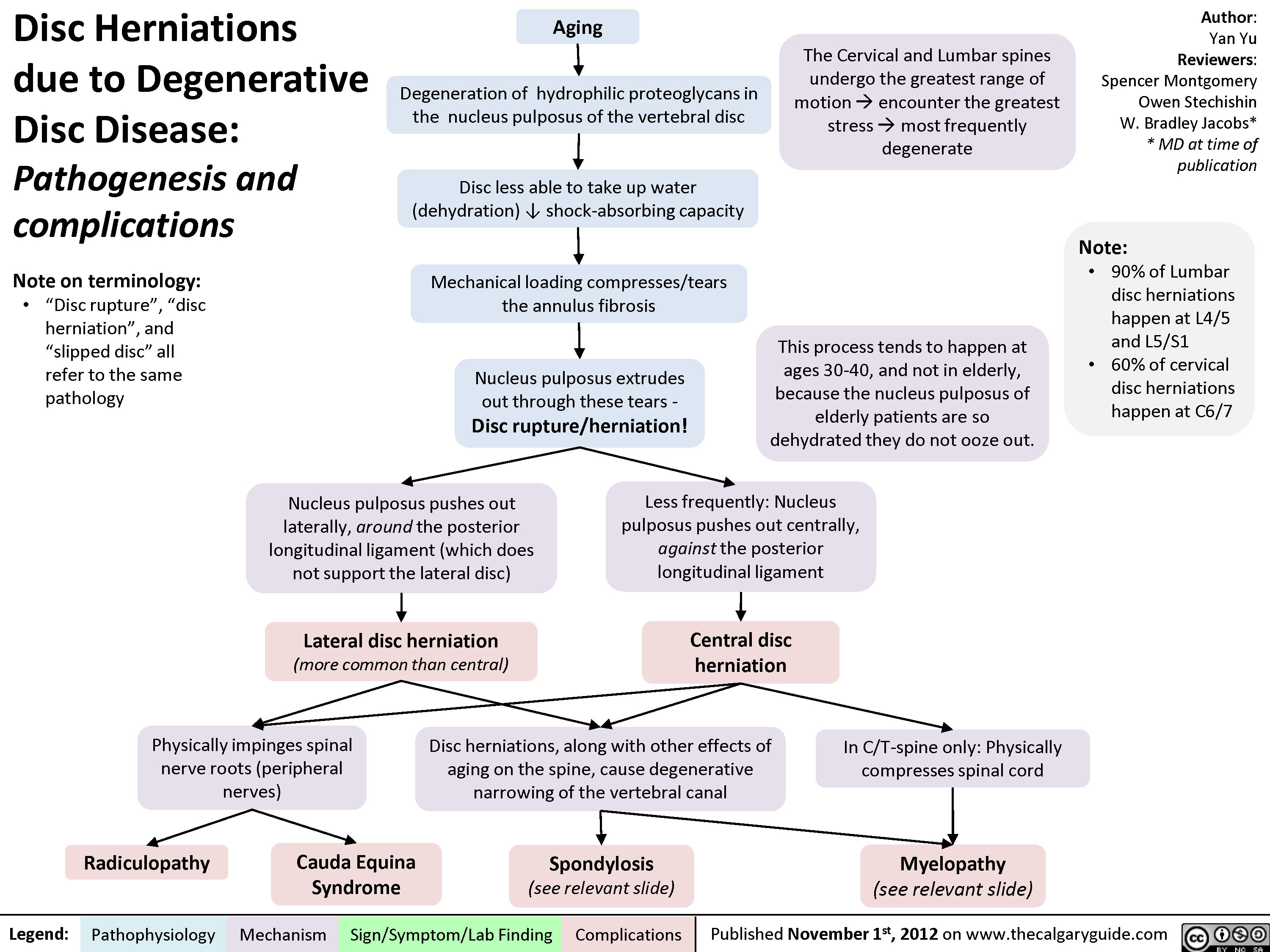
Disc Herniations
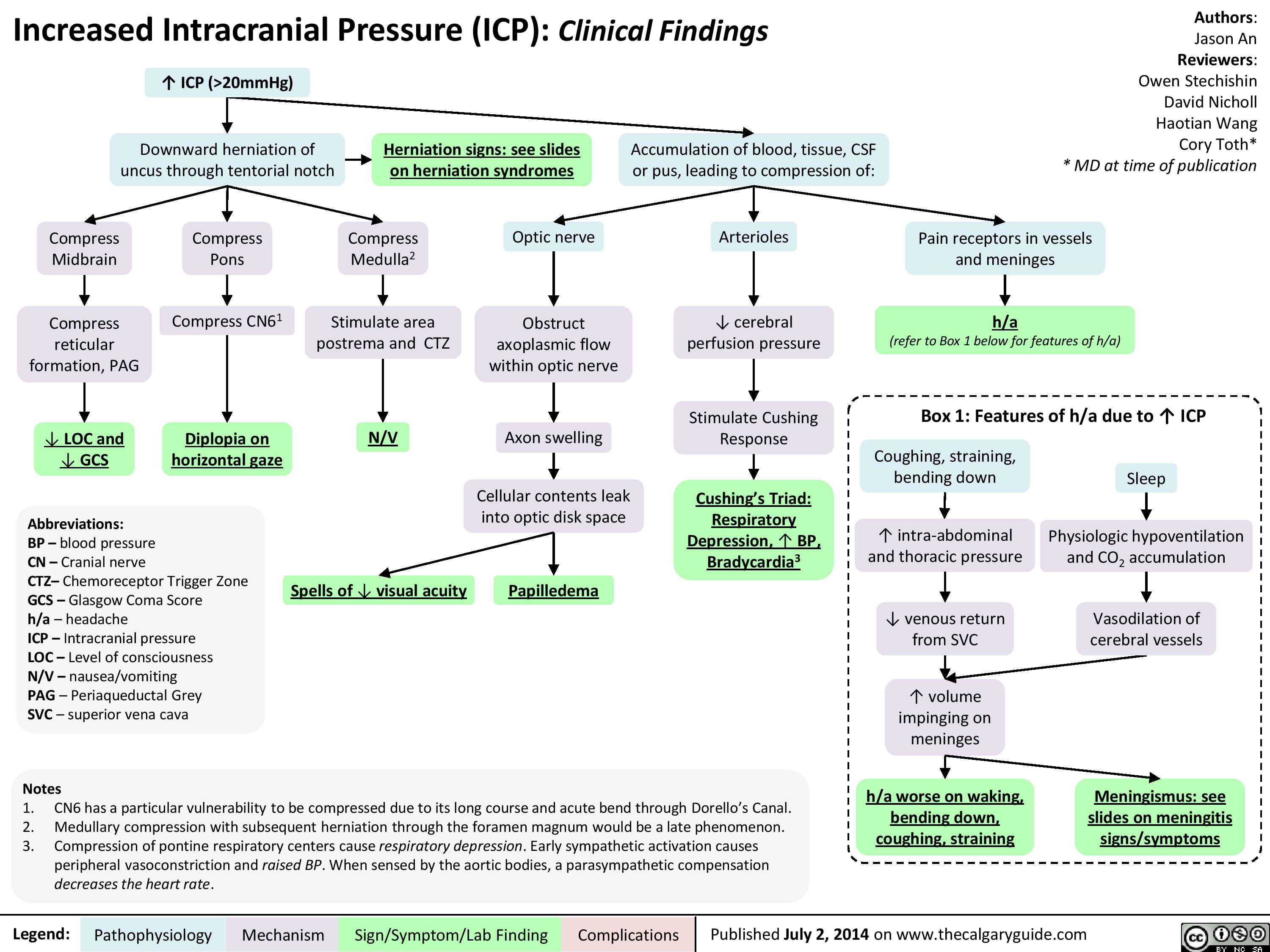
Presentation of increased ICP
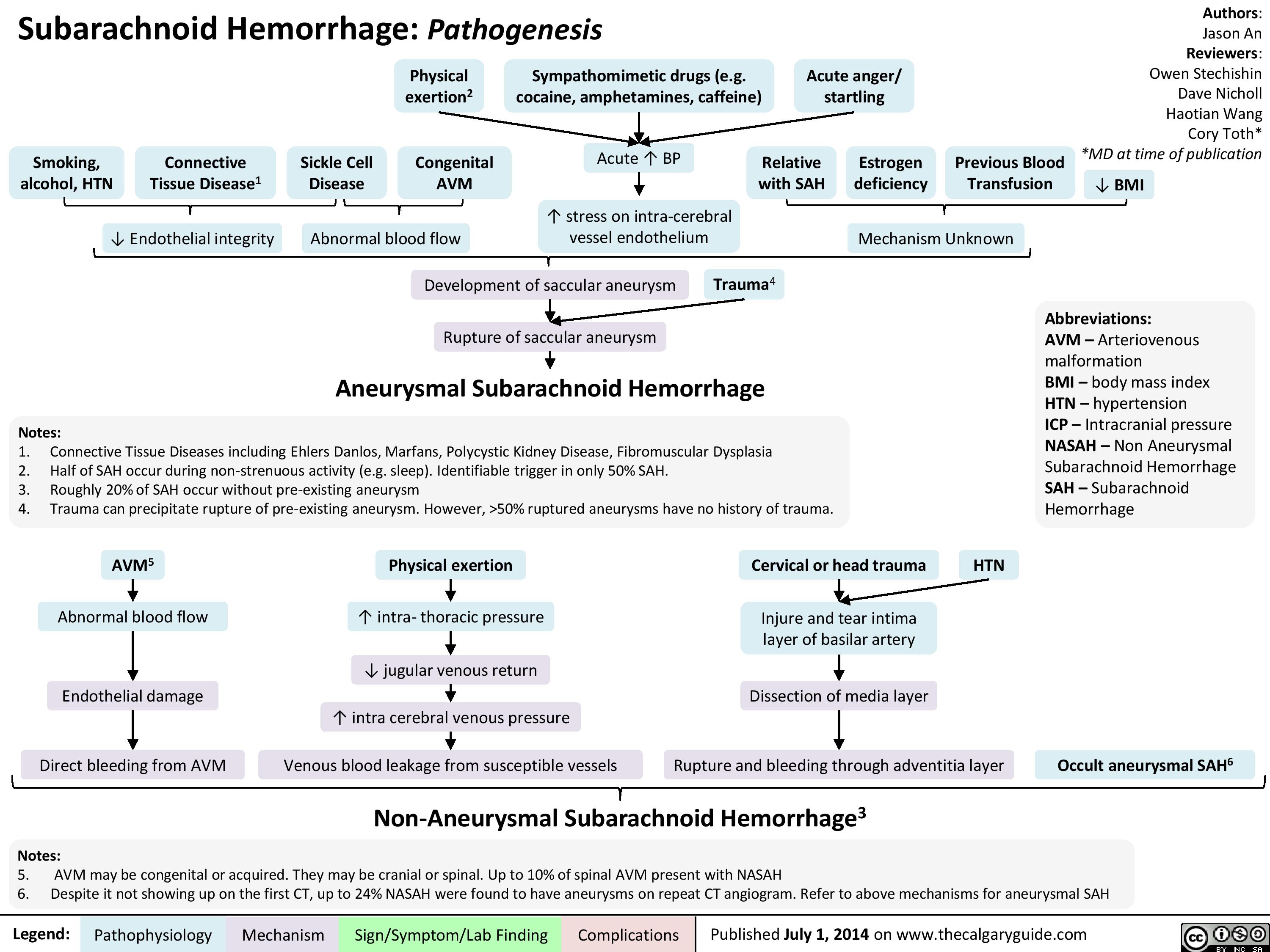
Pathogenesis of SAH
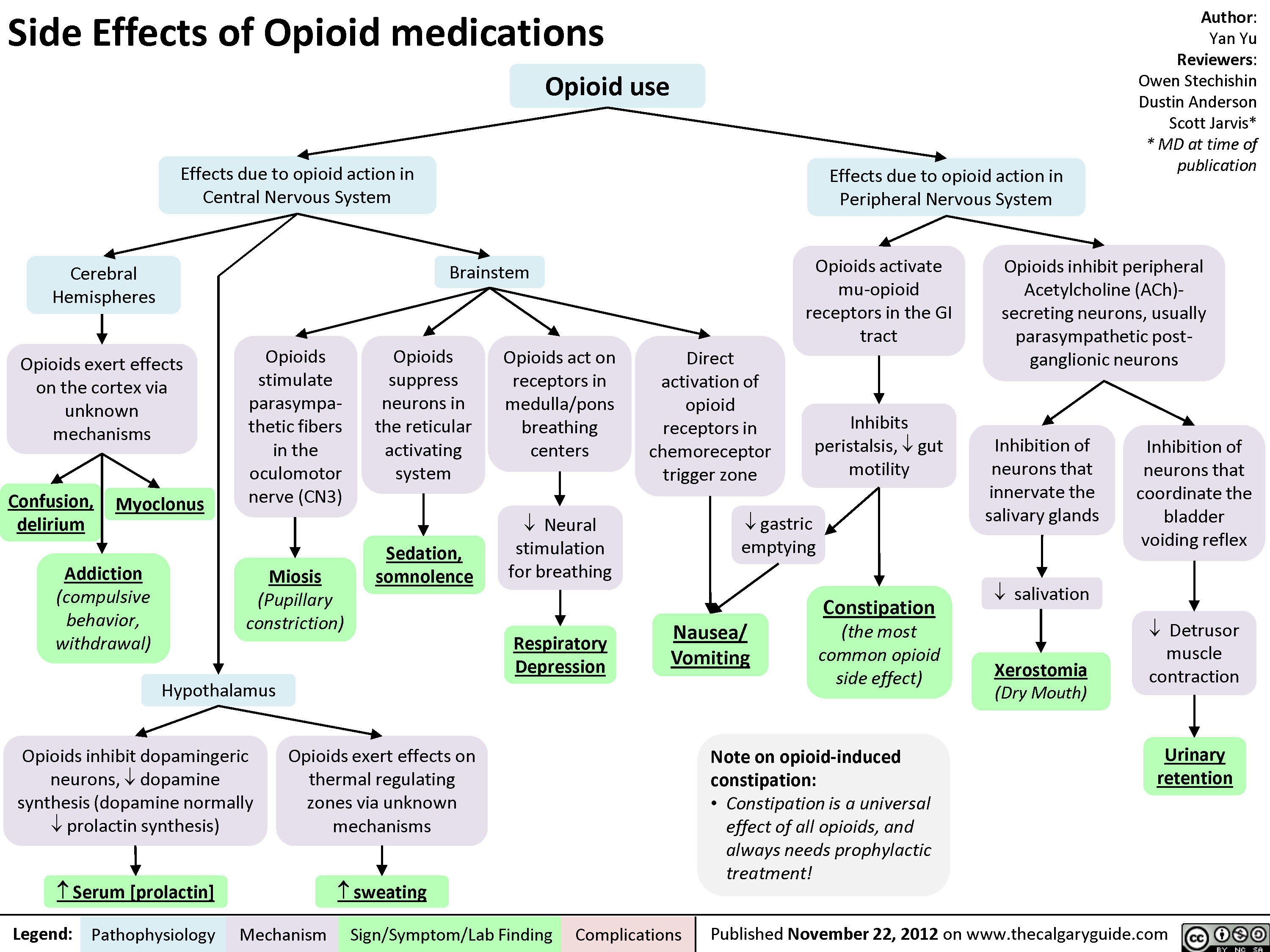
Side Effects of Opioid Medications
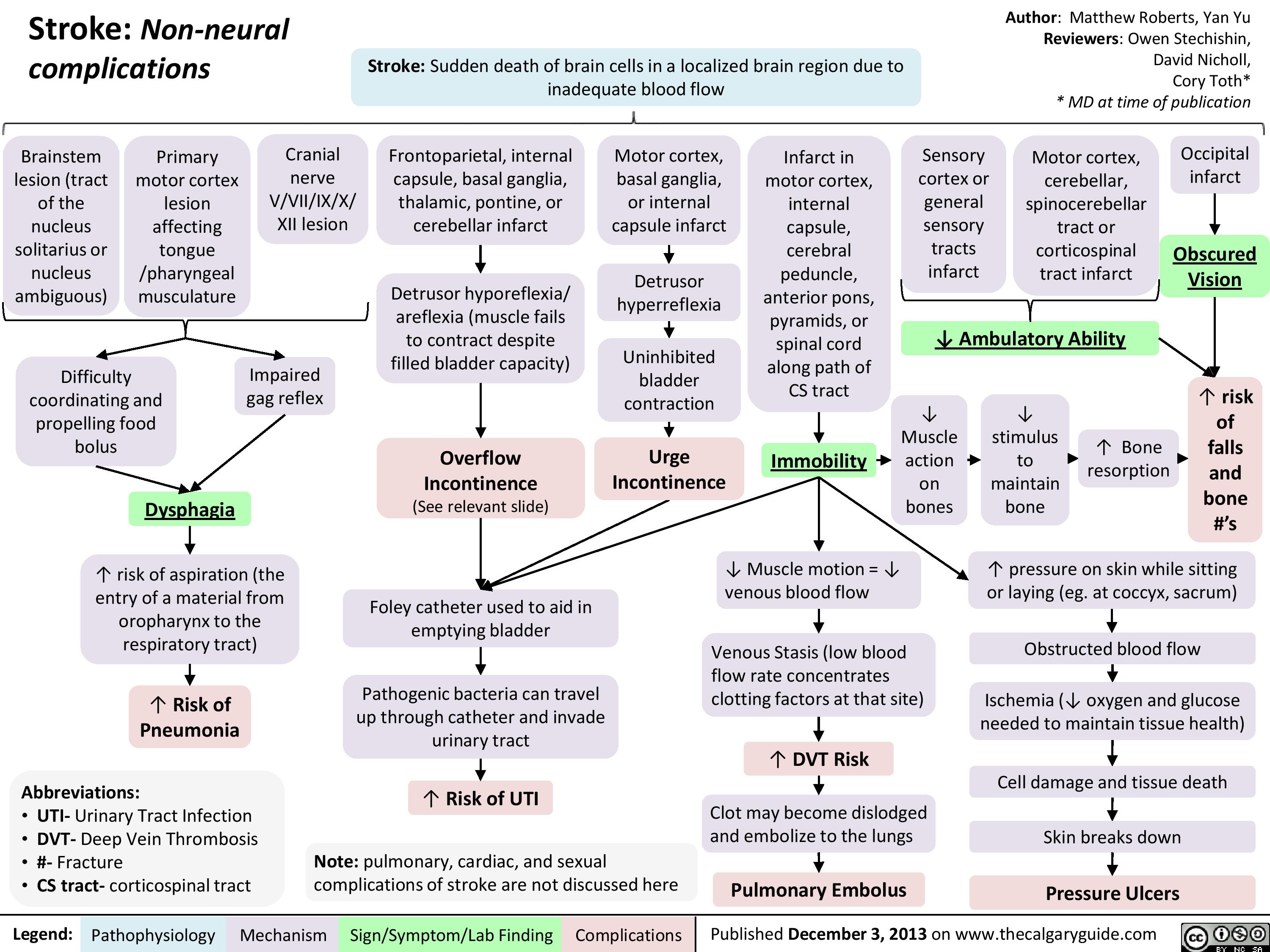
Non Neural Complications of Stroke
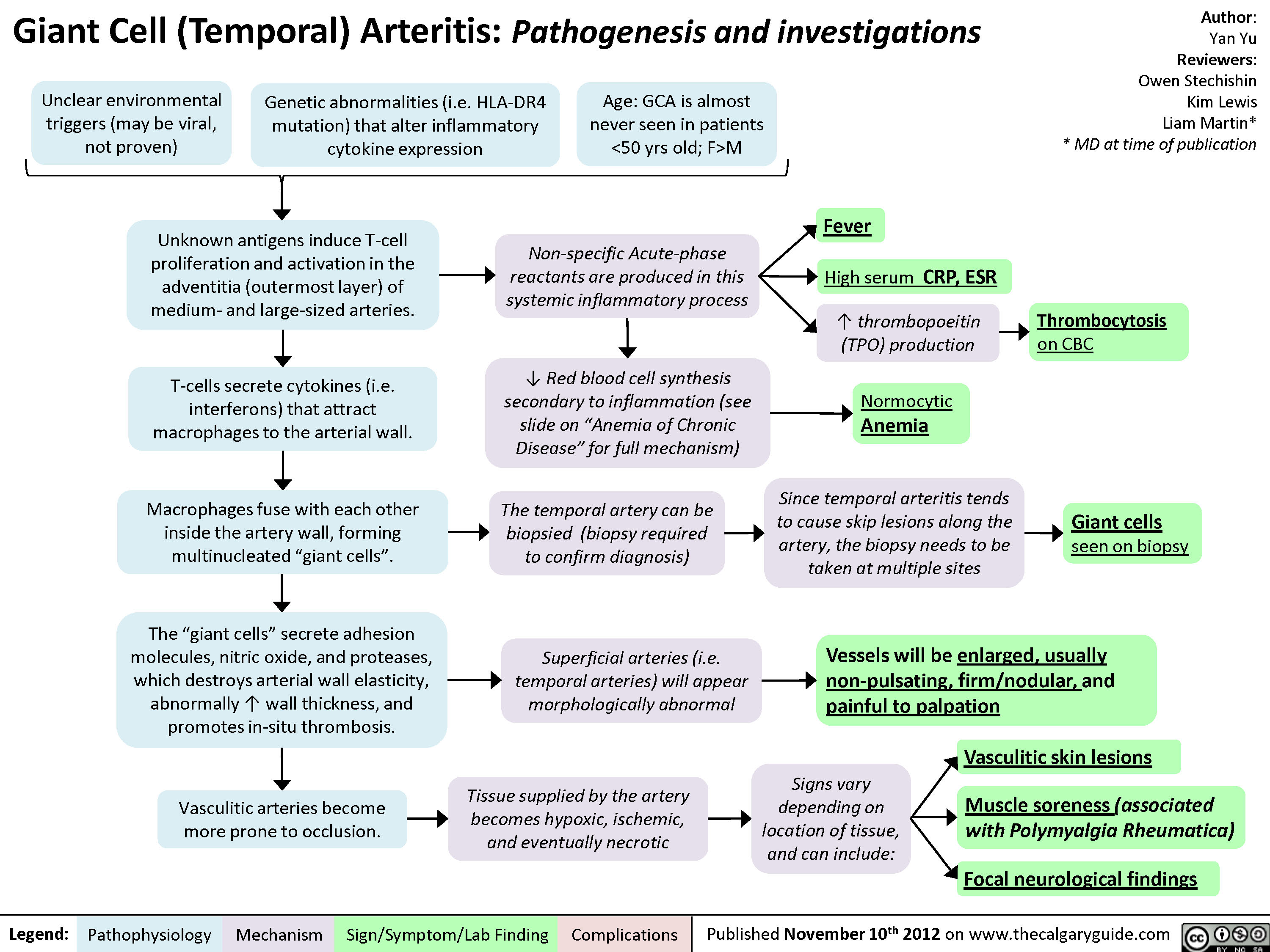
Giant Cell (Temporal) Arteritis - Pathogenesis and investigations
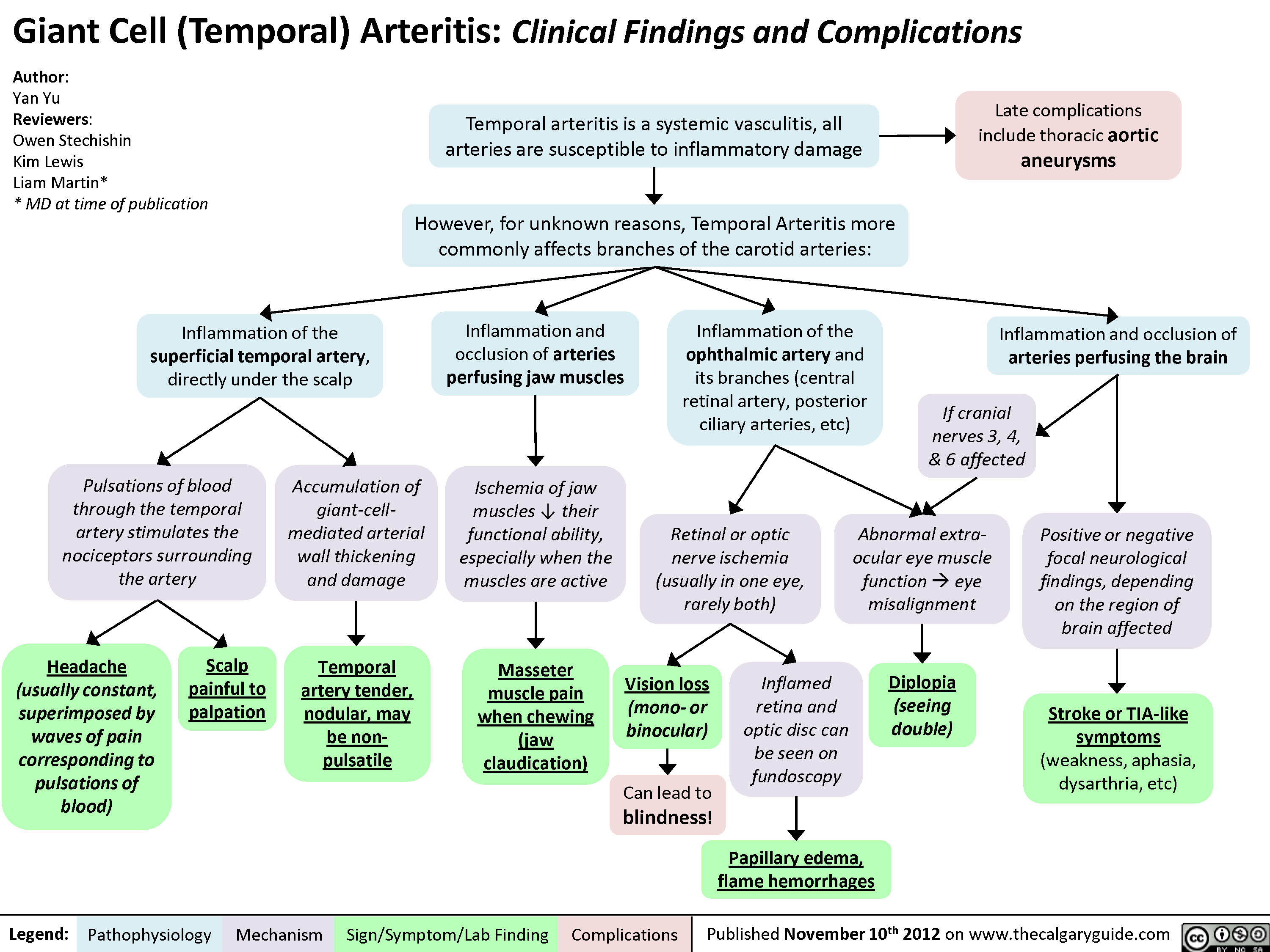
Giant Cell (Temporal) Arteritis - Clinical findings and Complications
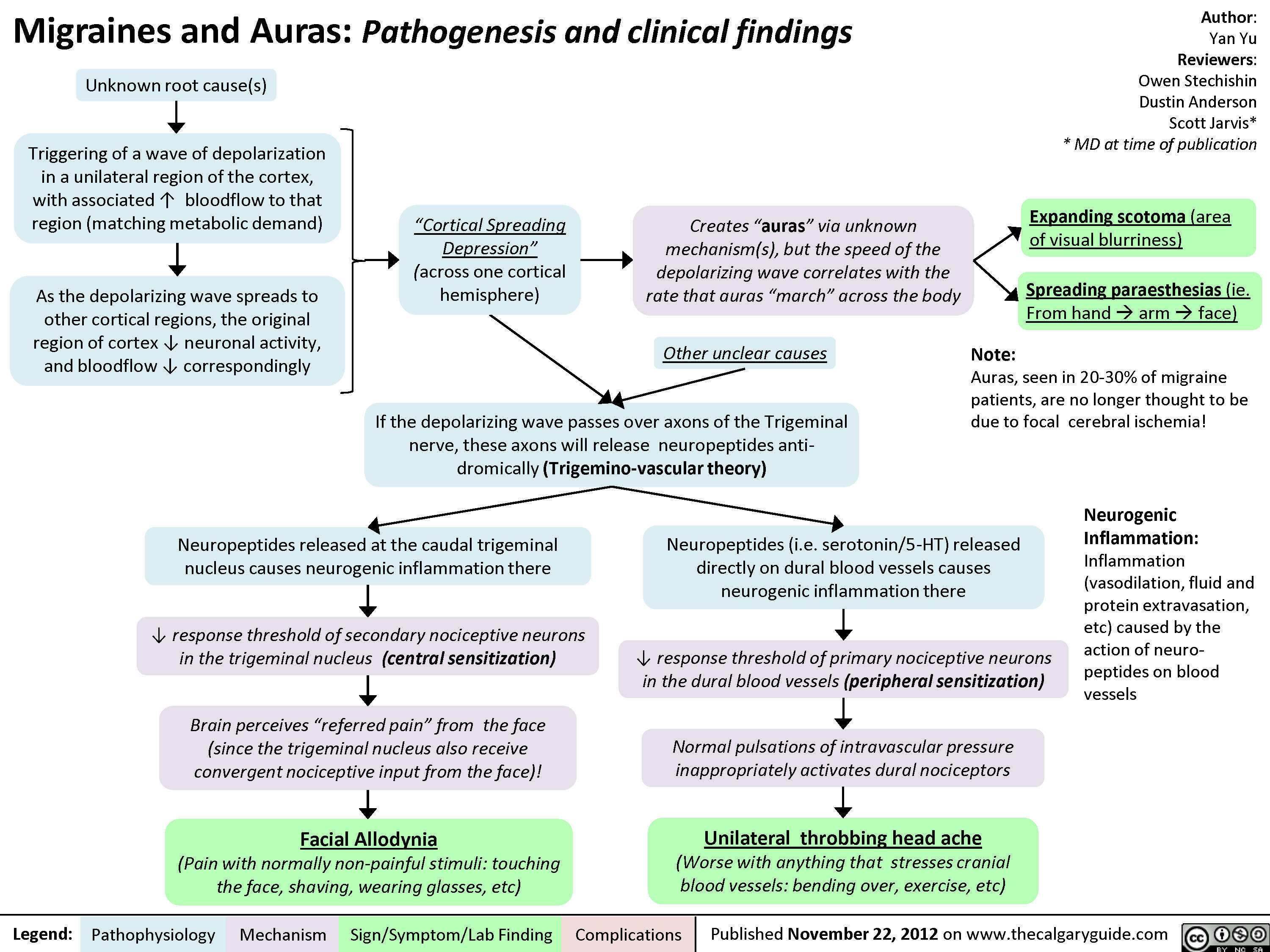
Migraines and Auras Pathogenesis and Clinical Findings
Pain Pathways in the Head

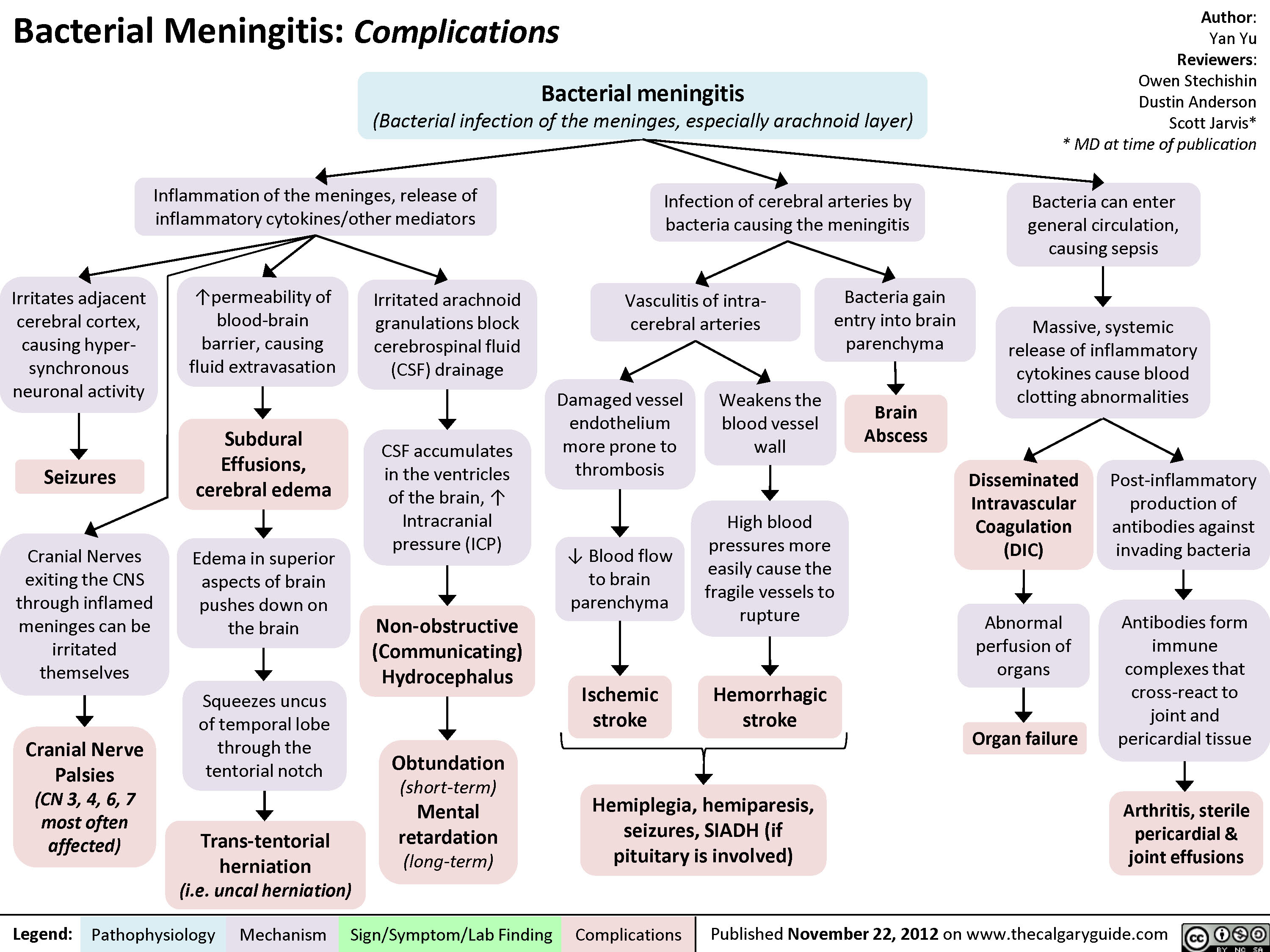
Bacterial Meningitis Complications
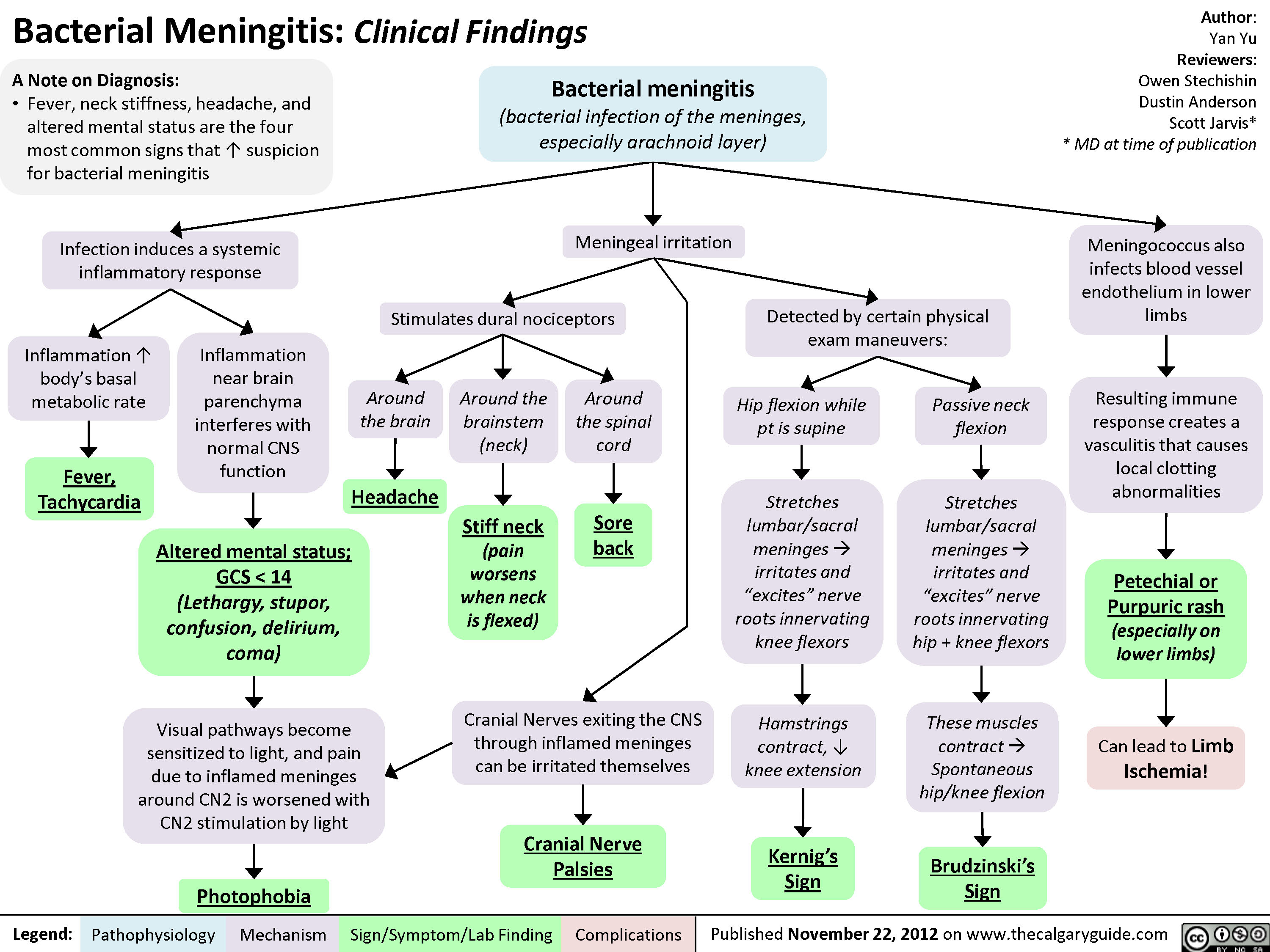
Bacterial Meningitis Clinical Findings
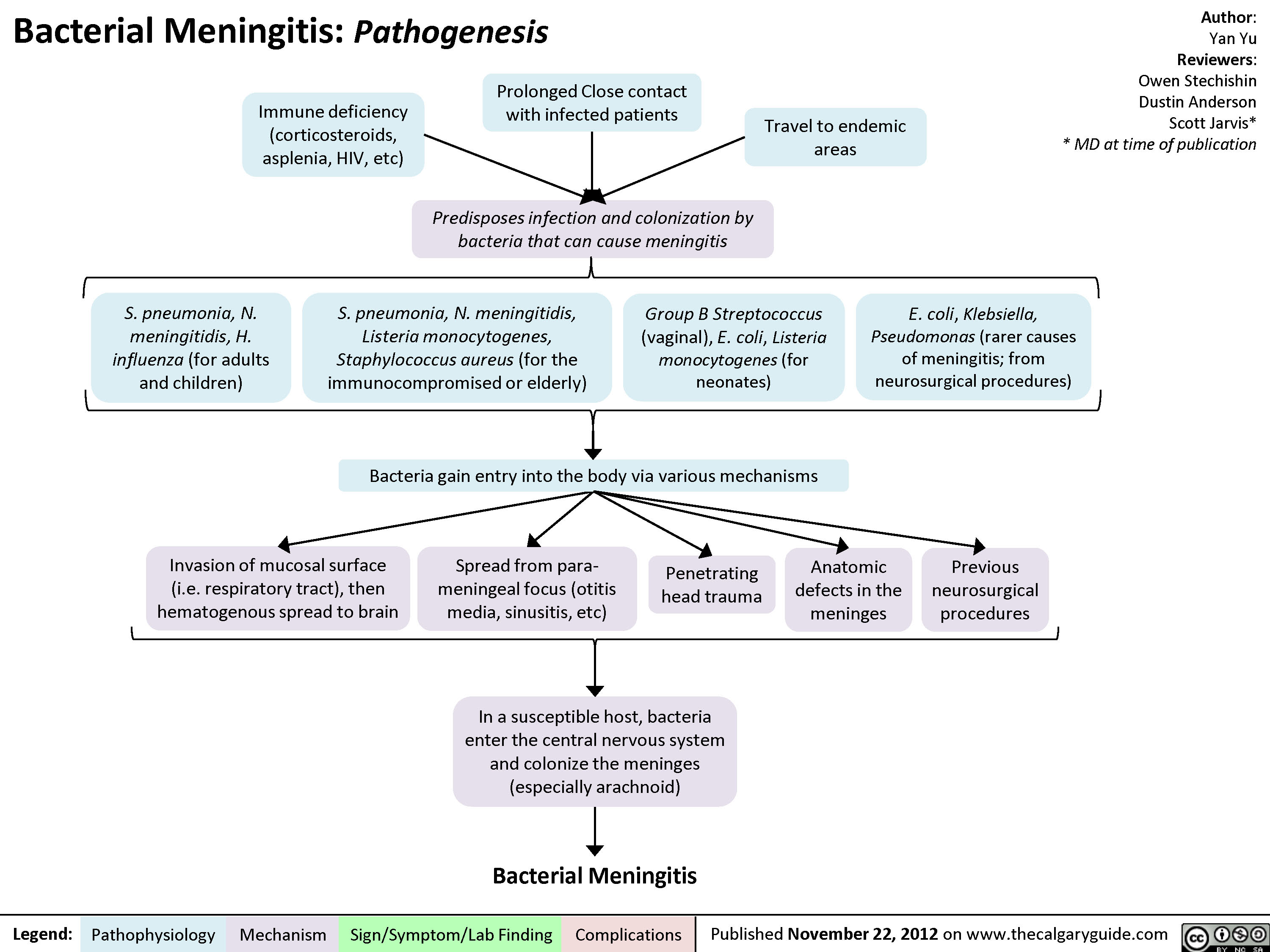
Bacterial Meningitis Pathogenesis
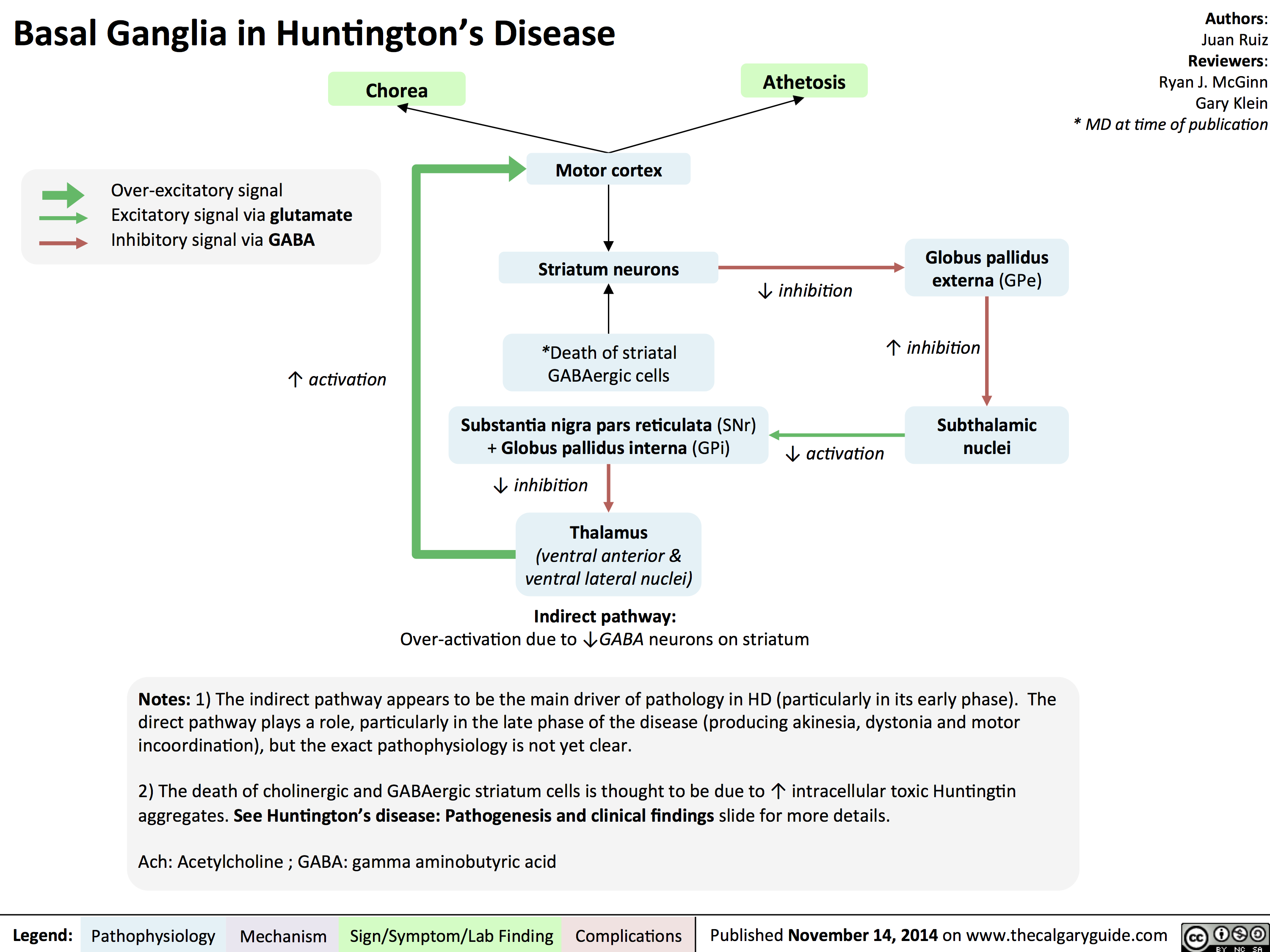
Basal Ganglia in Huntingtons Disease
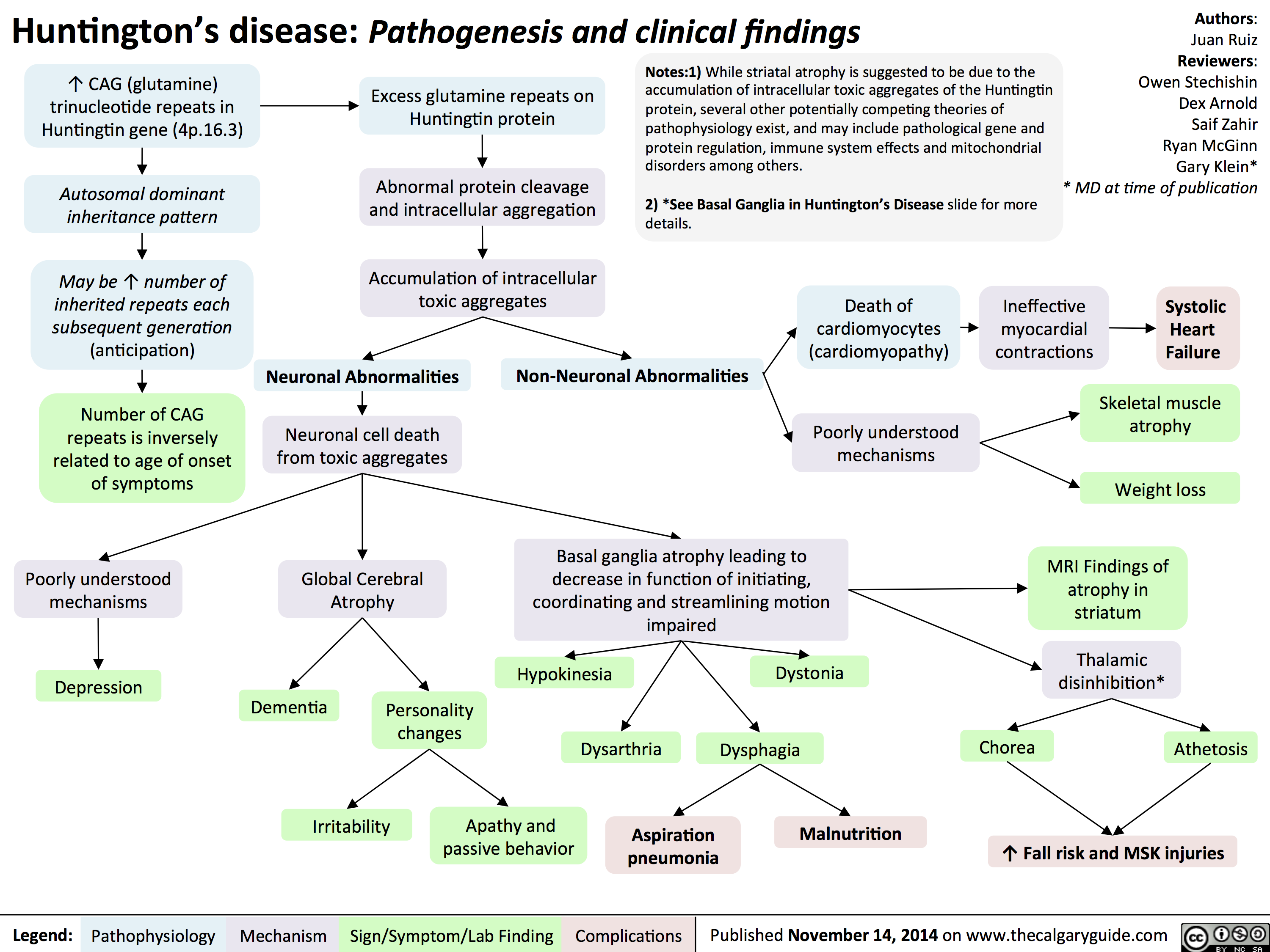
Huntingtons Disease Pathogenesis and Clinical Findings
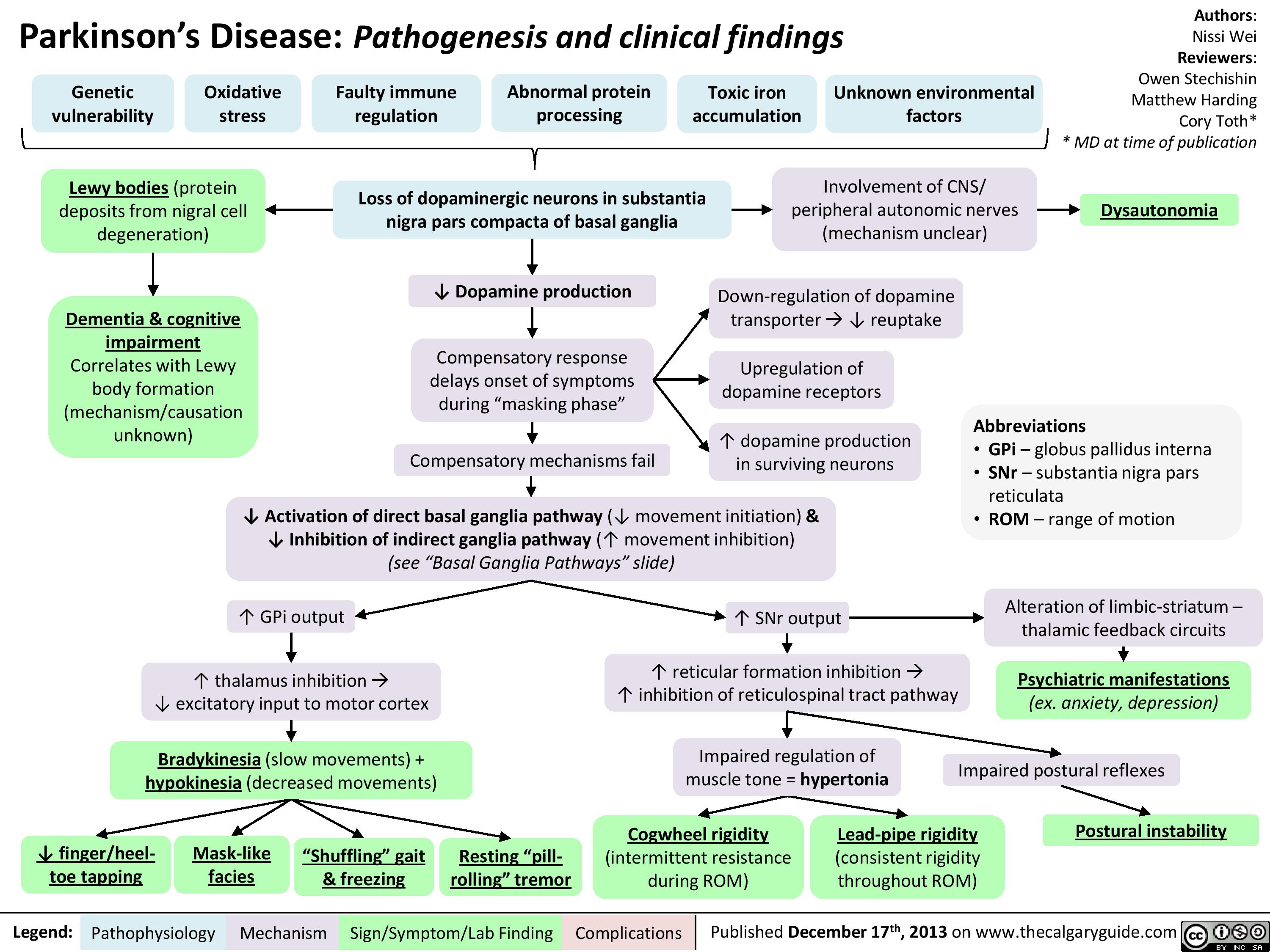
Parkinsons Disease
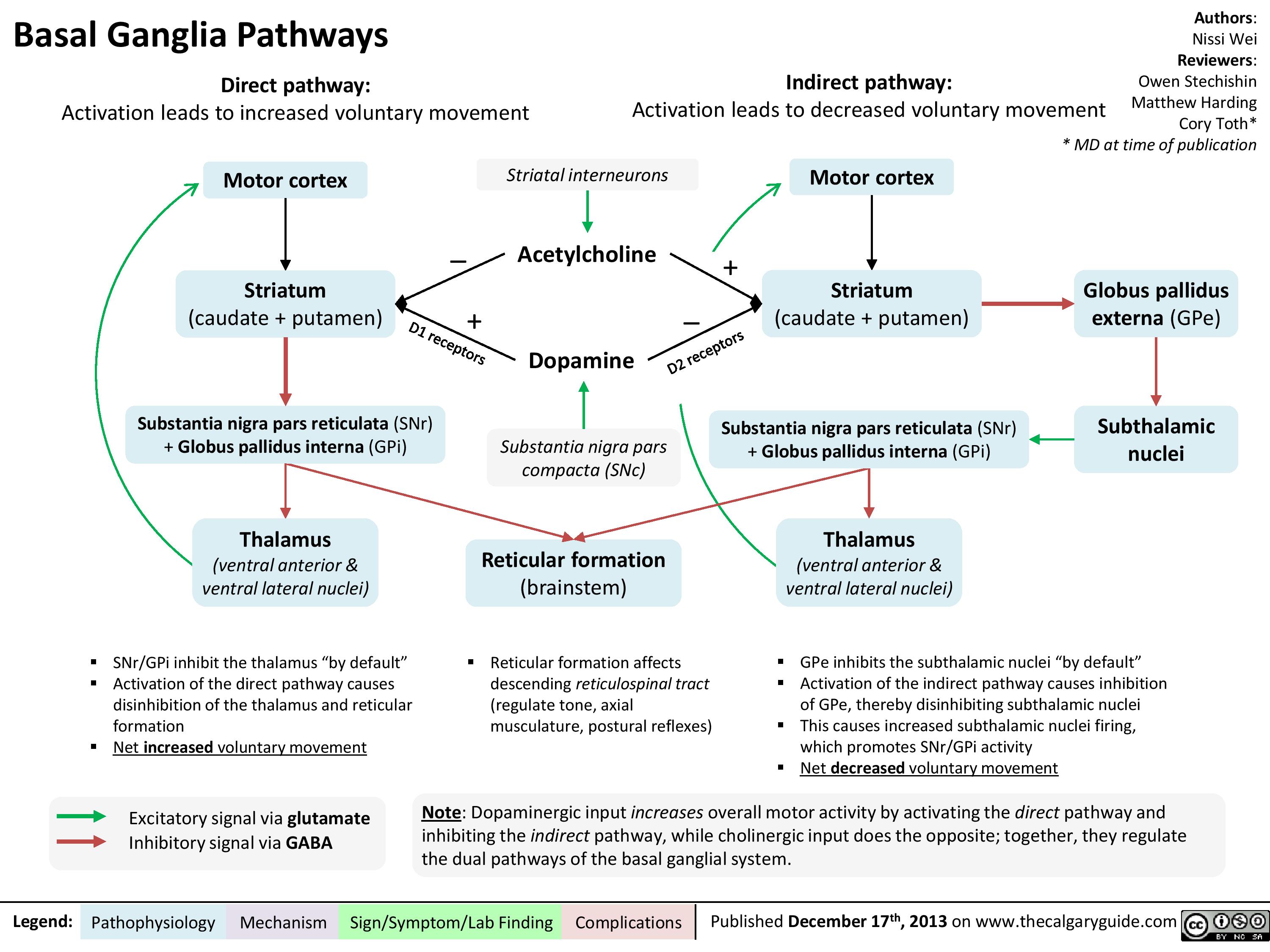
Basal ganglia pathways
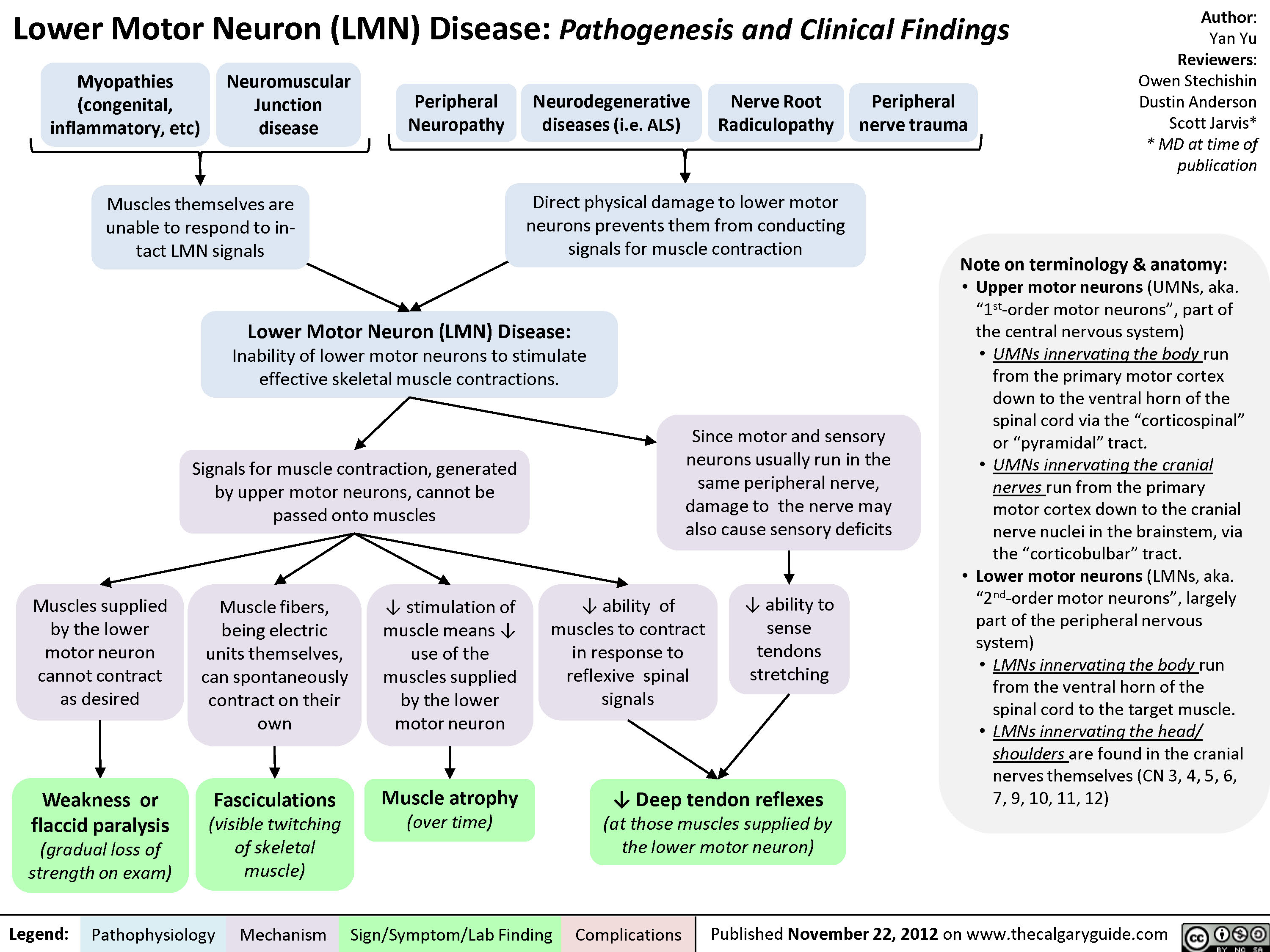
Lower Motor Neuron (UMN) Disease
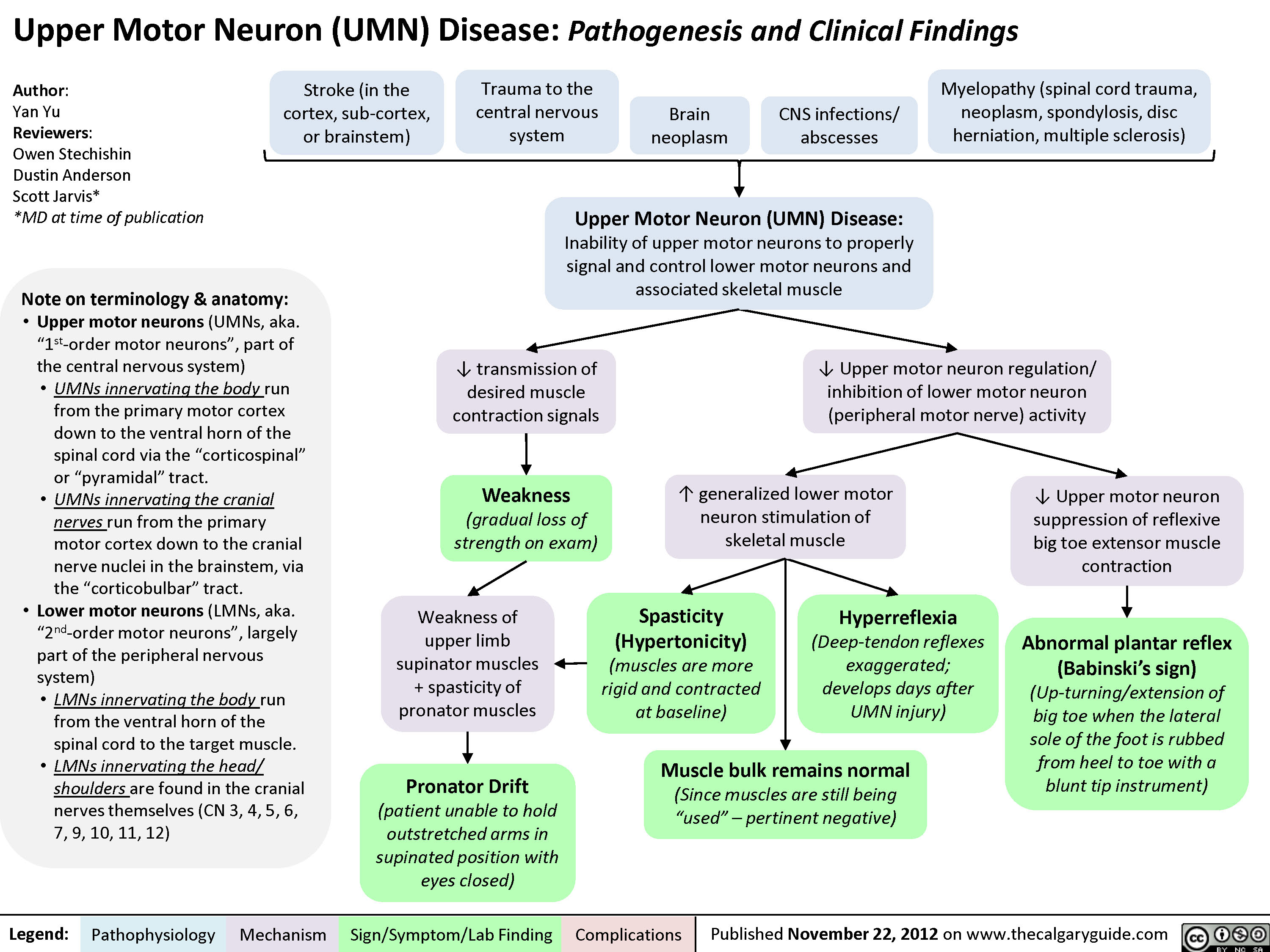
Upper Motor Neuron (UMN) Disease
Dupuytren
Trigger Finger
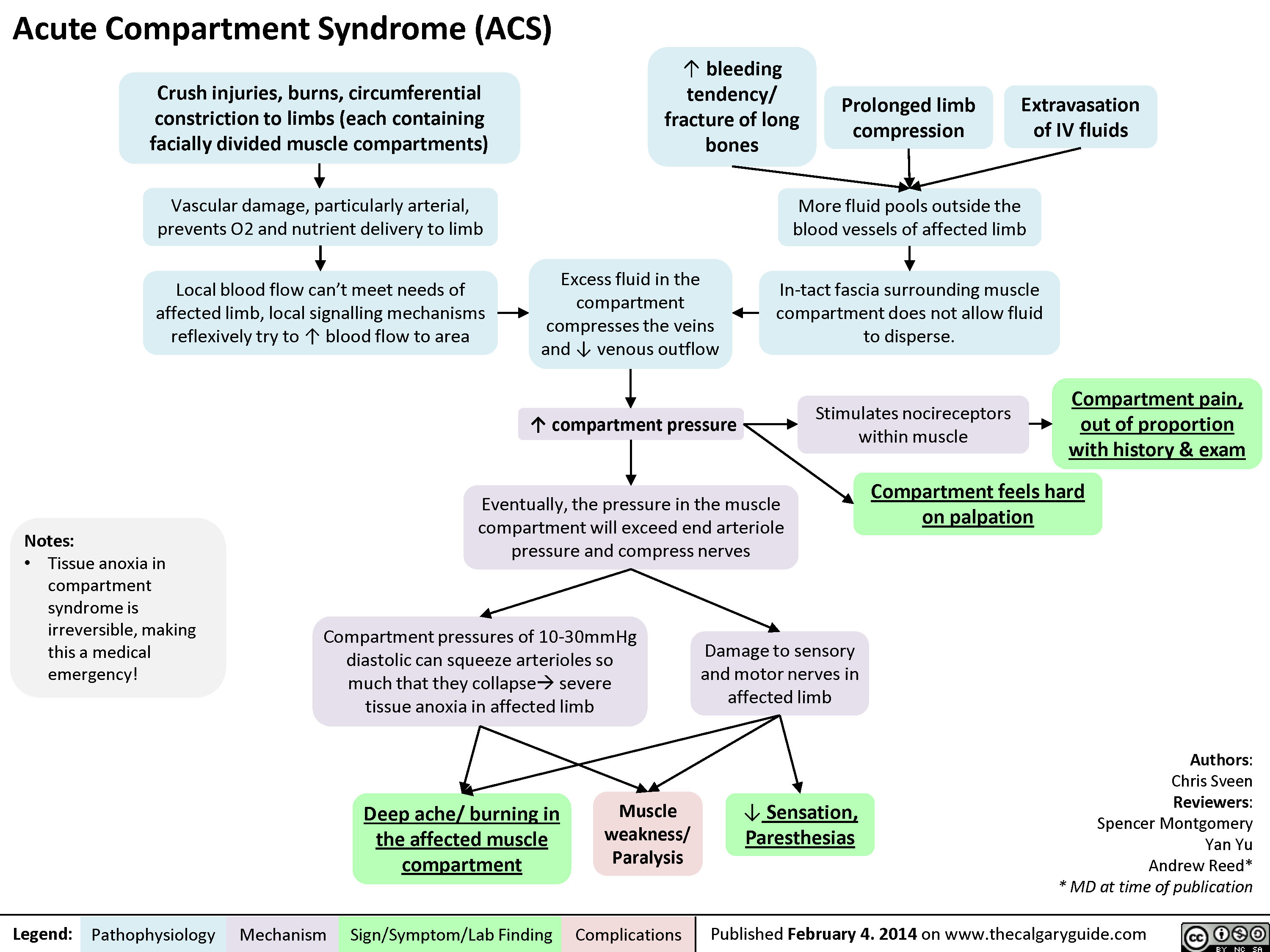
Acute Compartment Syndrome
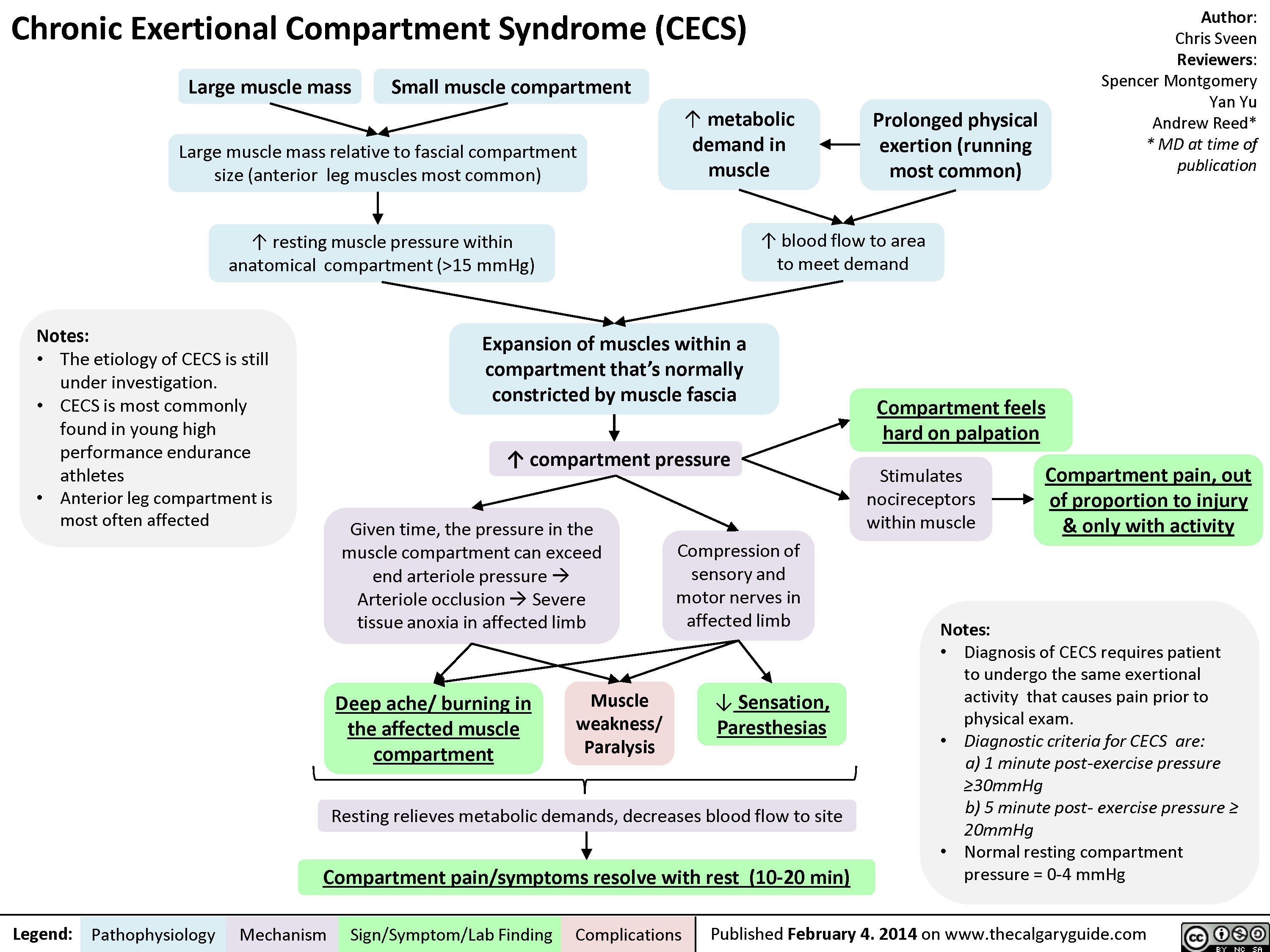
Chronic Exertional Compartment Syndrome
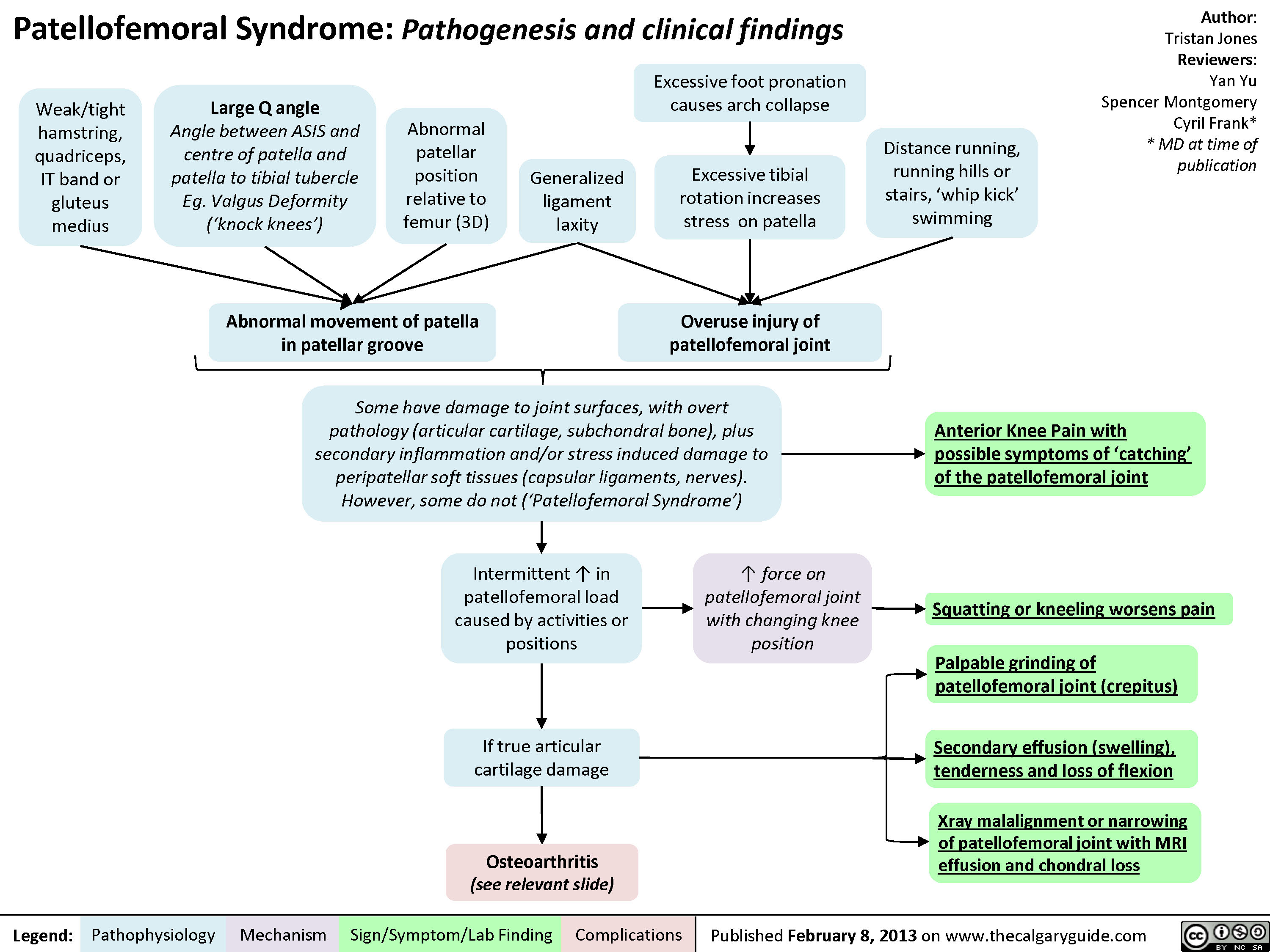
Patellofemoral Syndrome
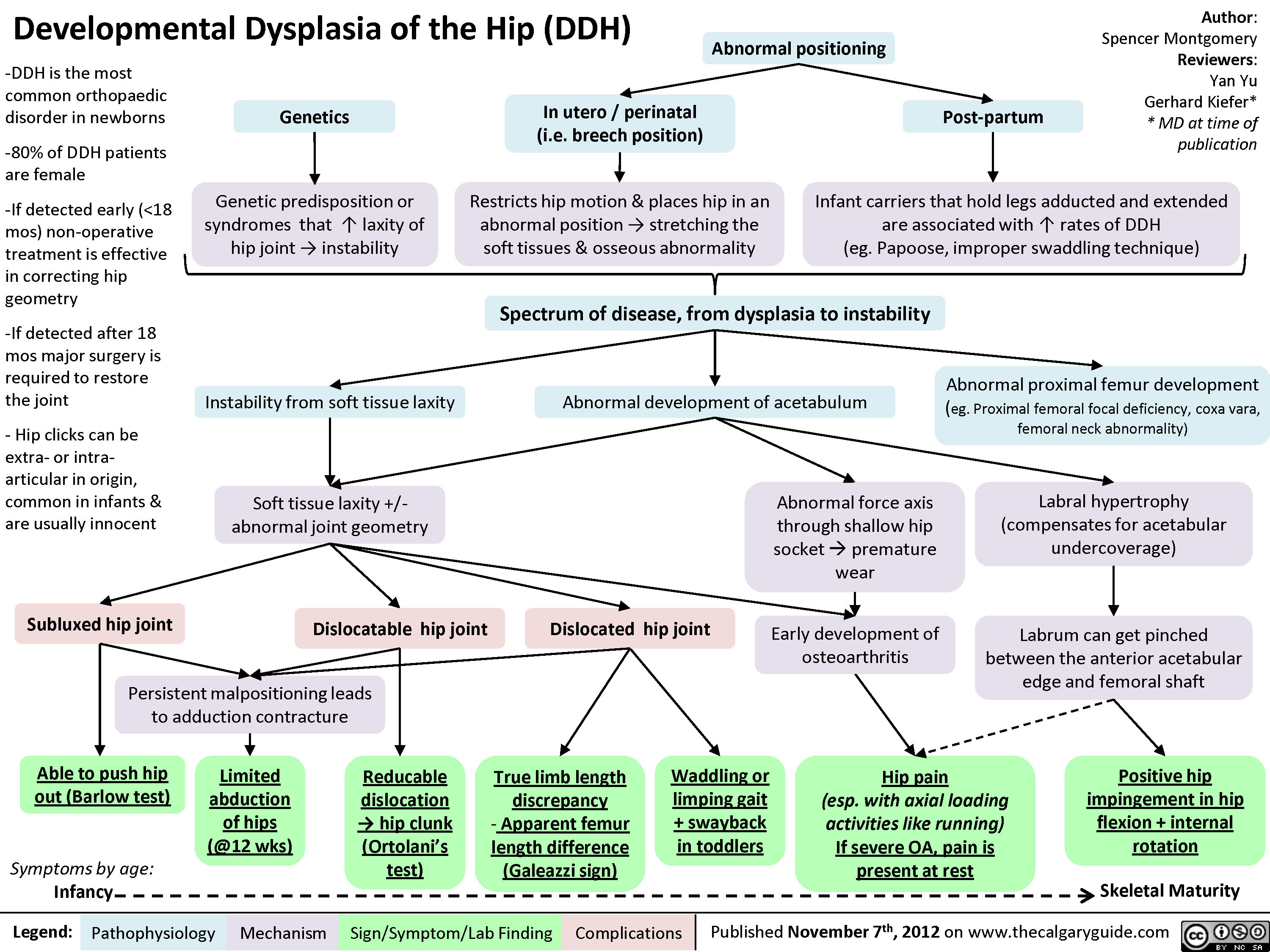
Developmental Dysplasia of the Hip (DDH)
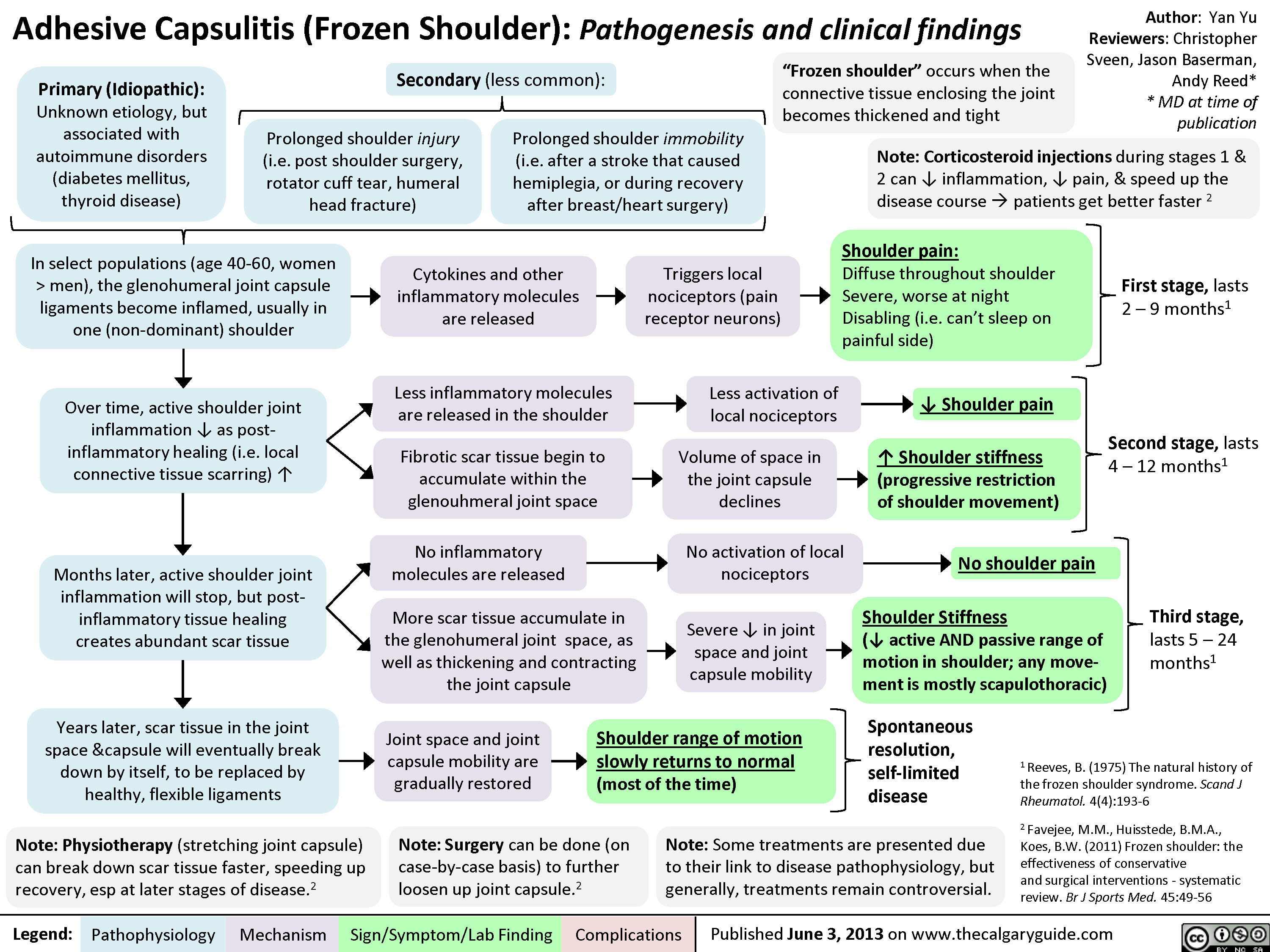
Adhesive Capsulitis
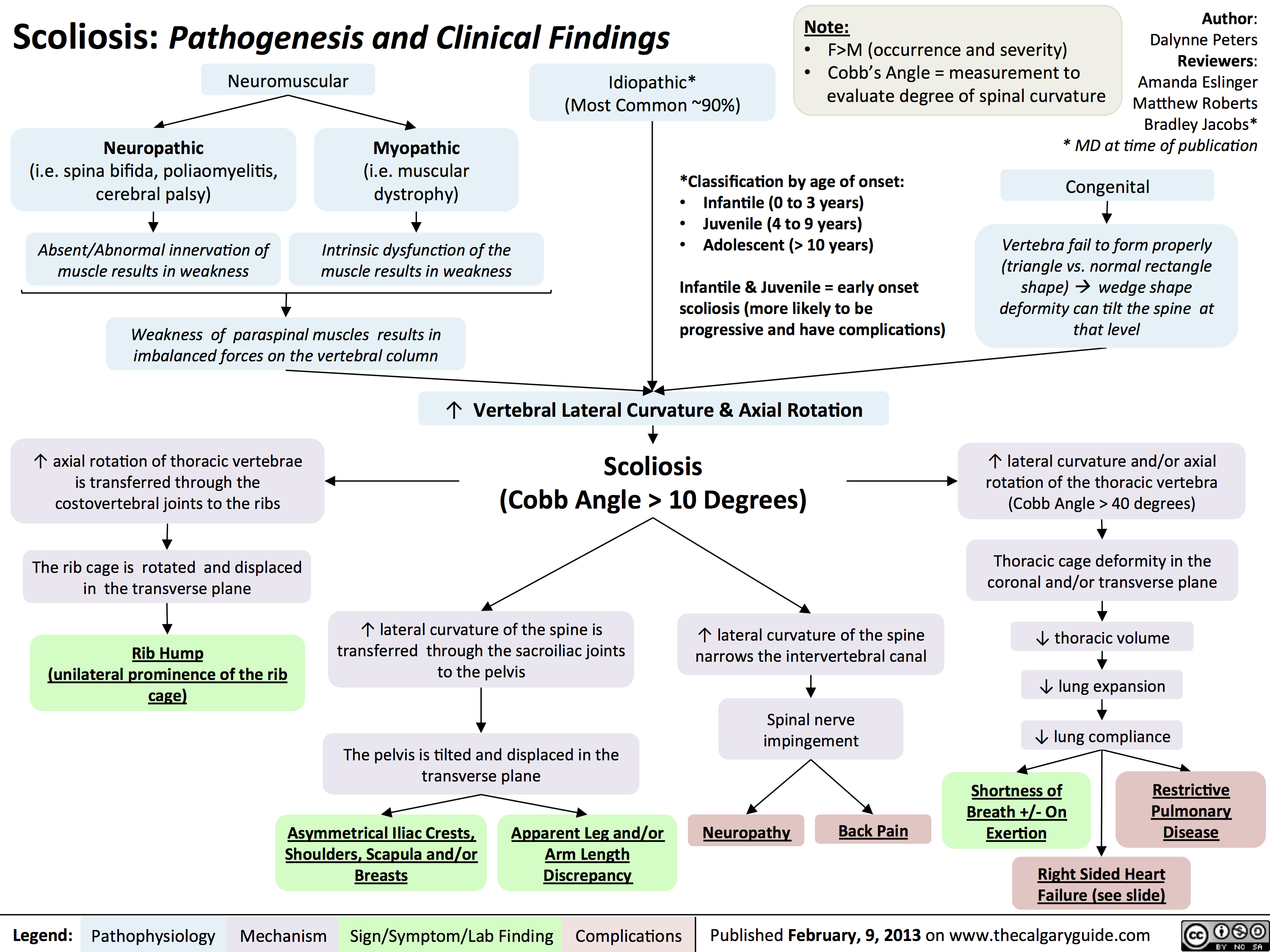
Scoliosis -Pathogenesis and Clinical Findings
Cauda Equina Syndrome
Myelopathy
Radiculopathy
Disc Herniations
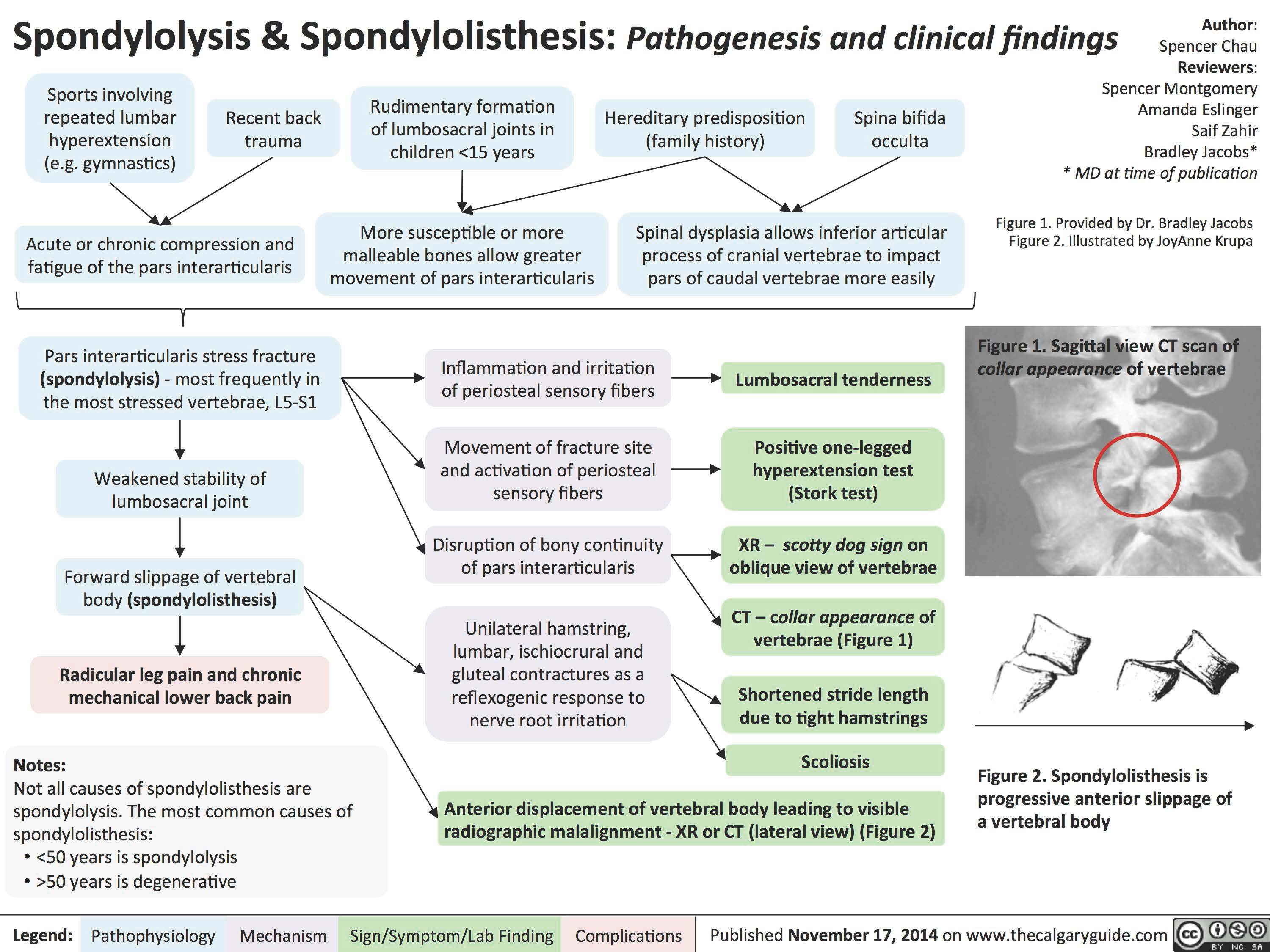
Spondylolysis _and_Spondylolisthesis Pathogenesis and Clinical Findings
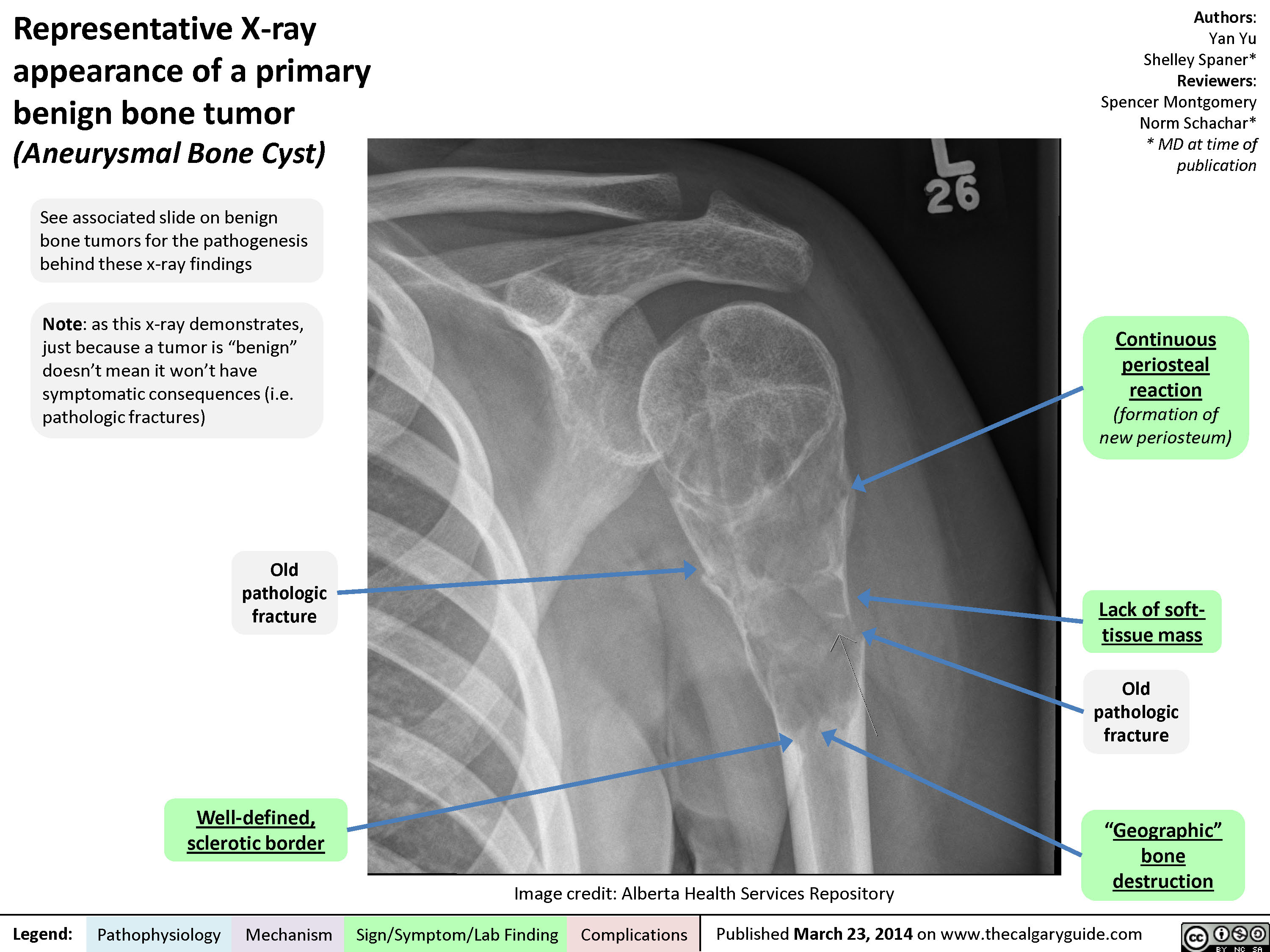
Representative X-ray appearance of a primary benign bone tumor
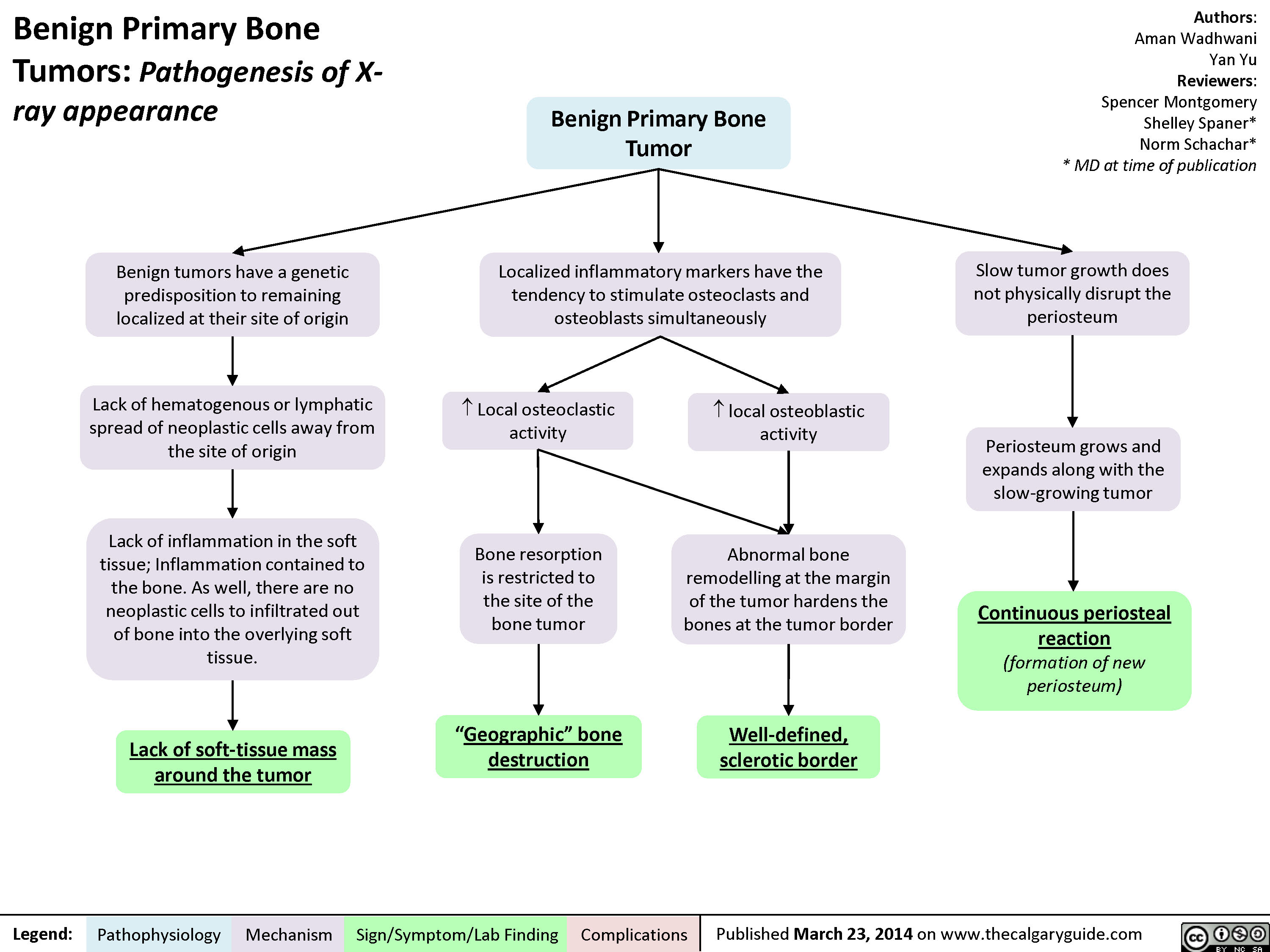
Benign Primary Bone Tumors - Pathogenesis of X-ray appearance
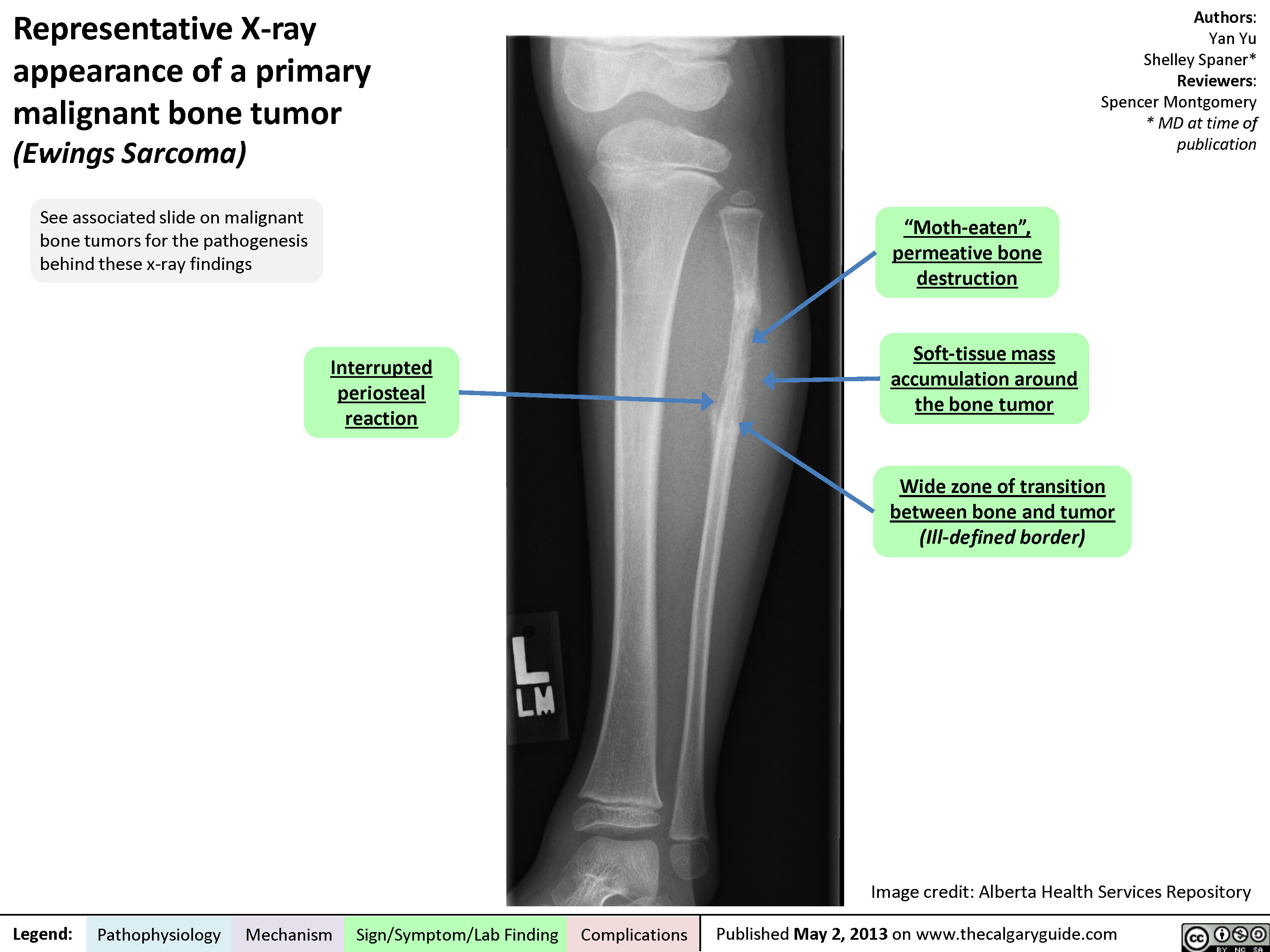
Representative X-ray appearance of a primary malignant bone tumor
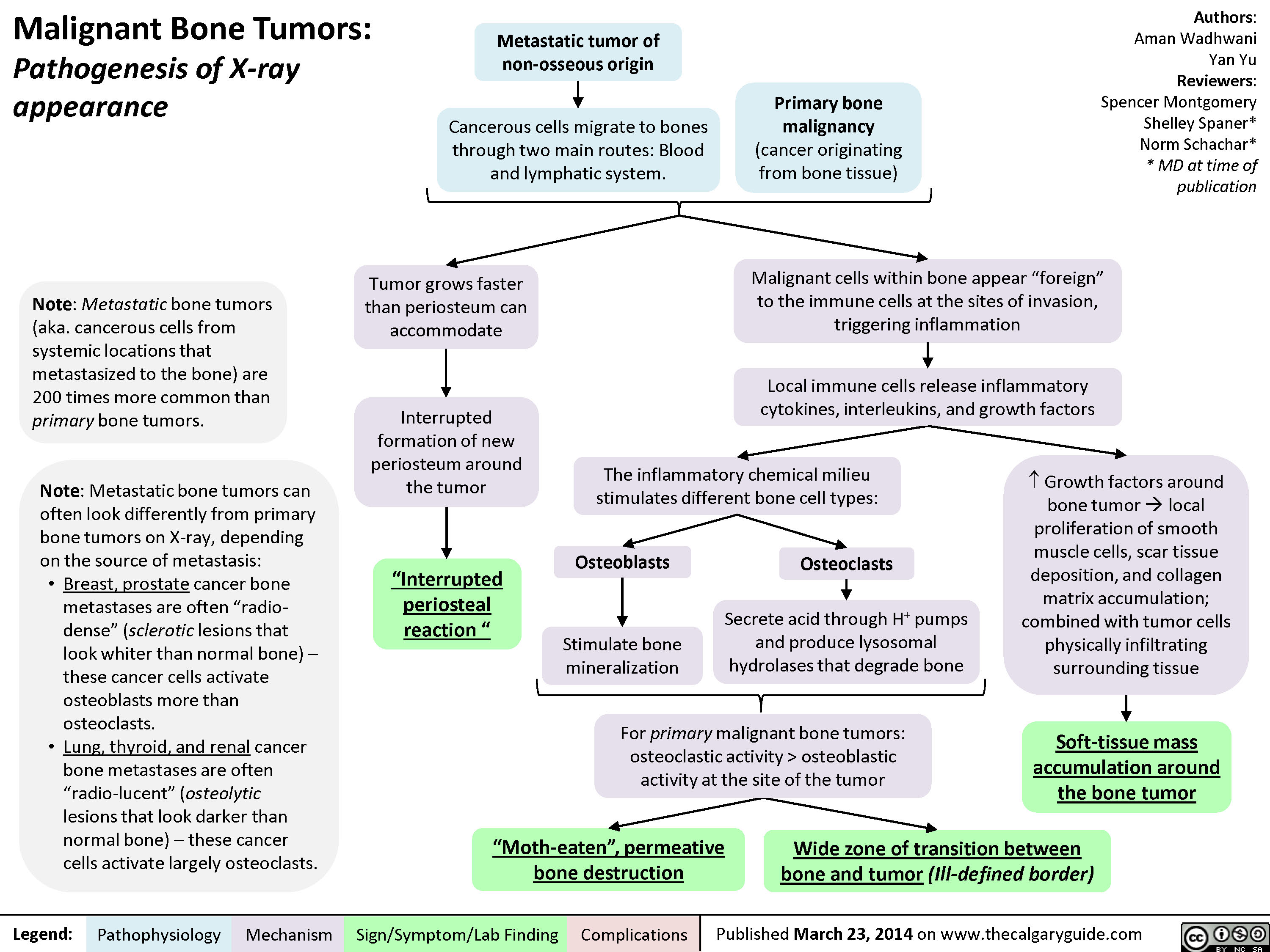
Malignant Bone Tumors - Pathogenesis of X-ray appearance
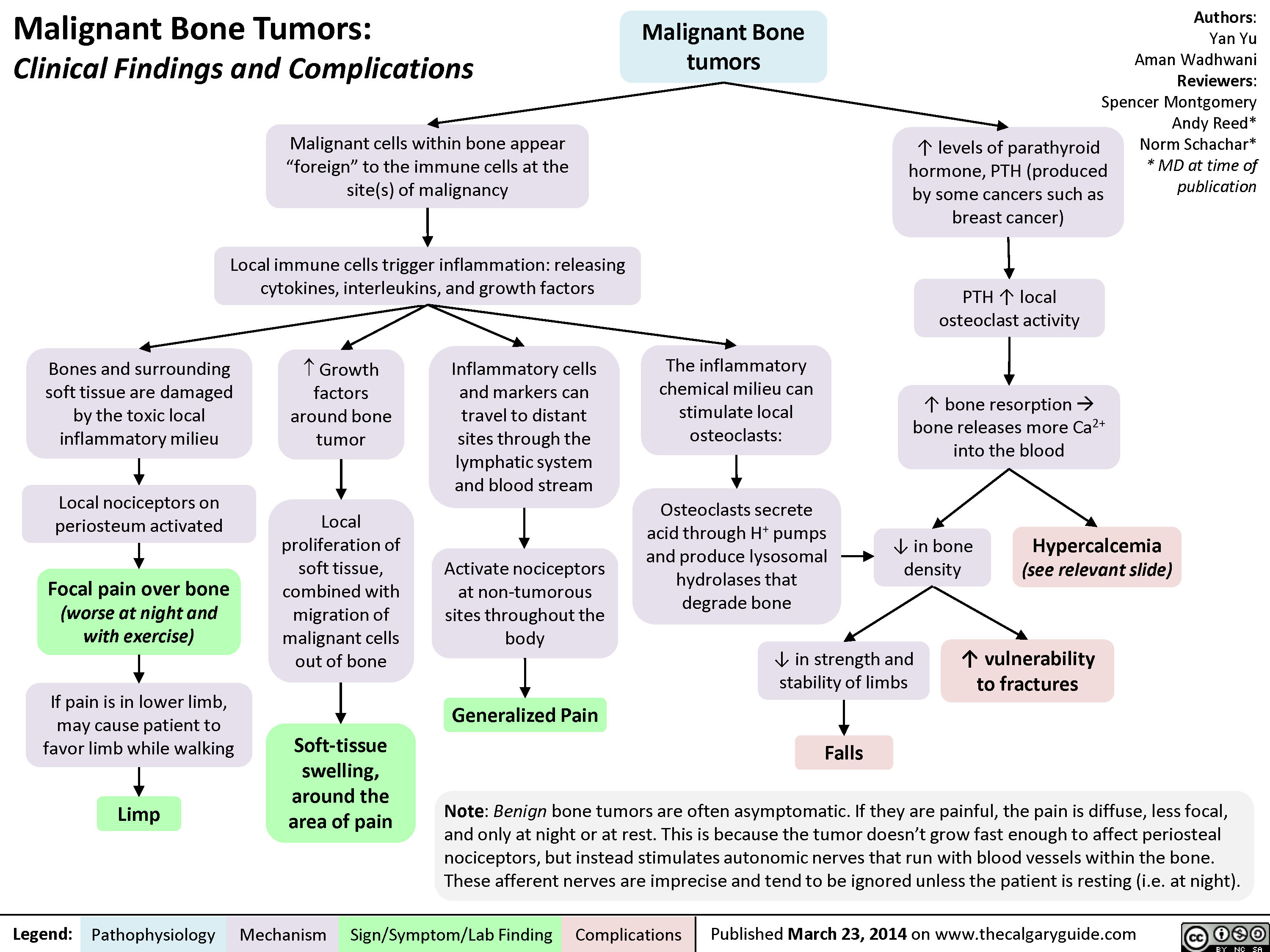
MSK tumors complications
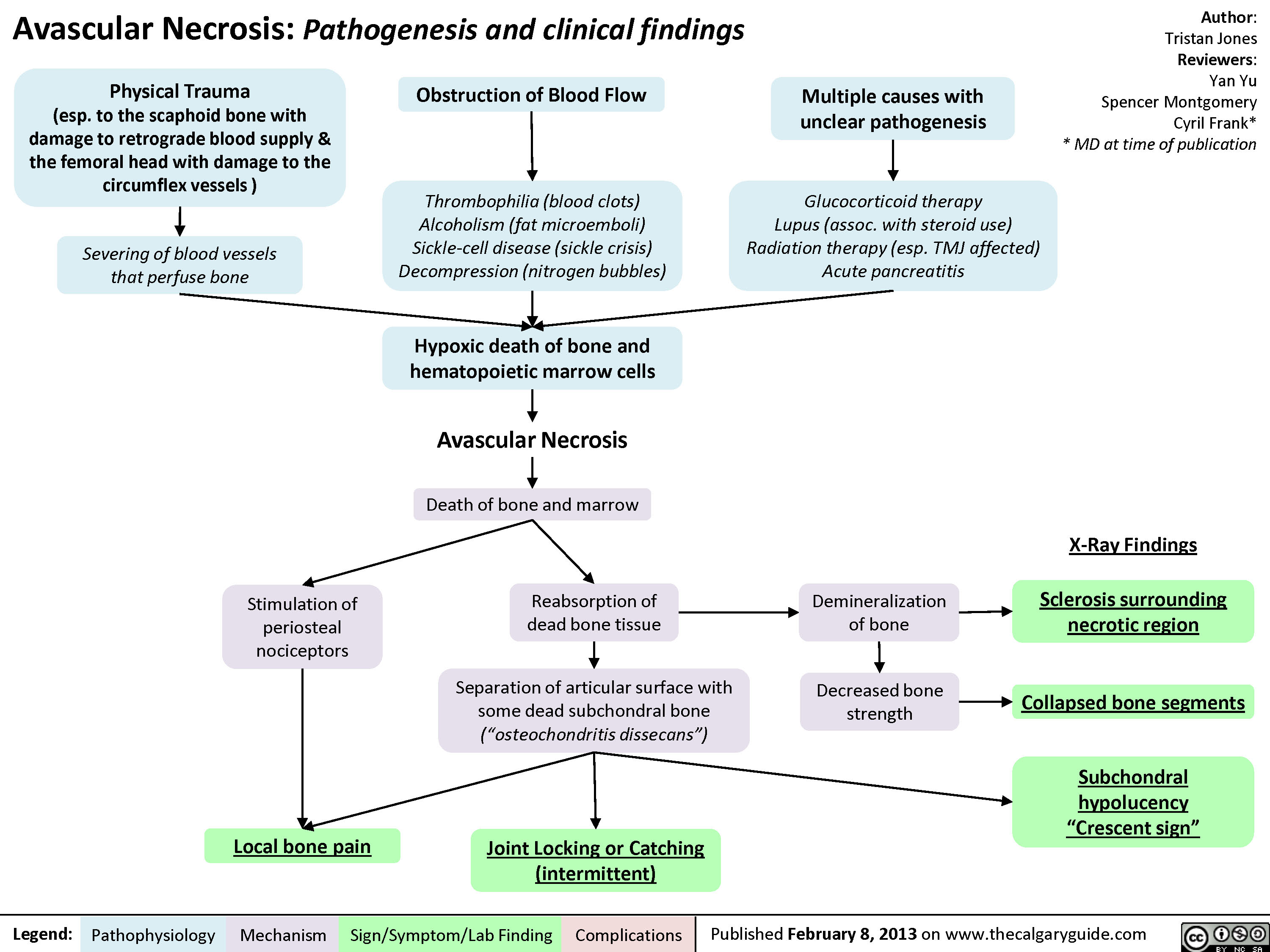
Avascular Necrosis - Pathogenesis and Clinical Findings
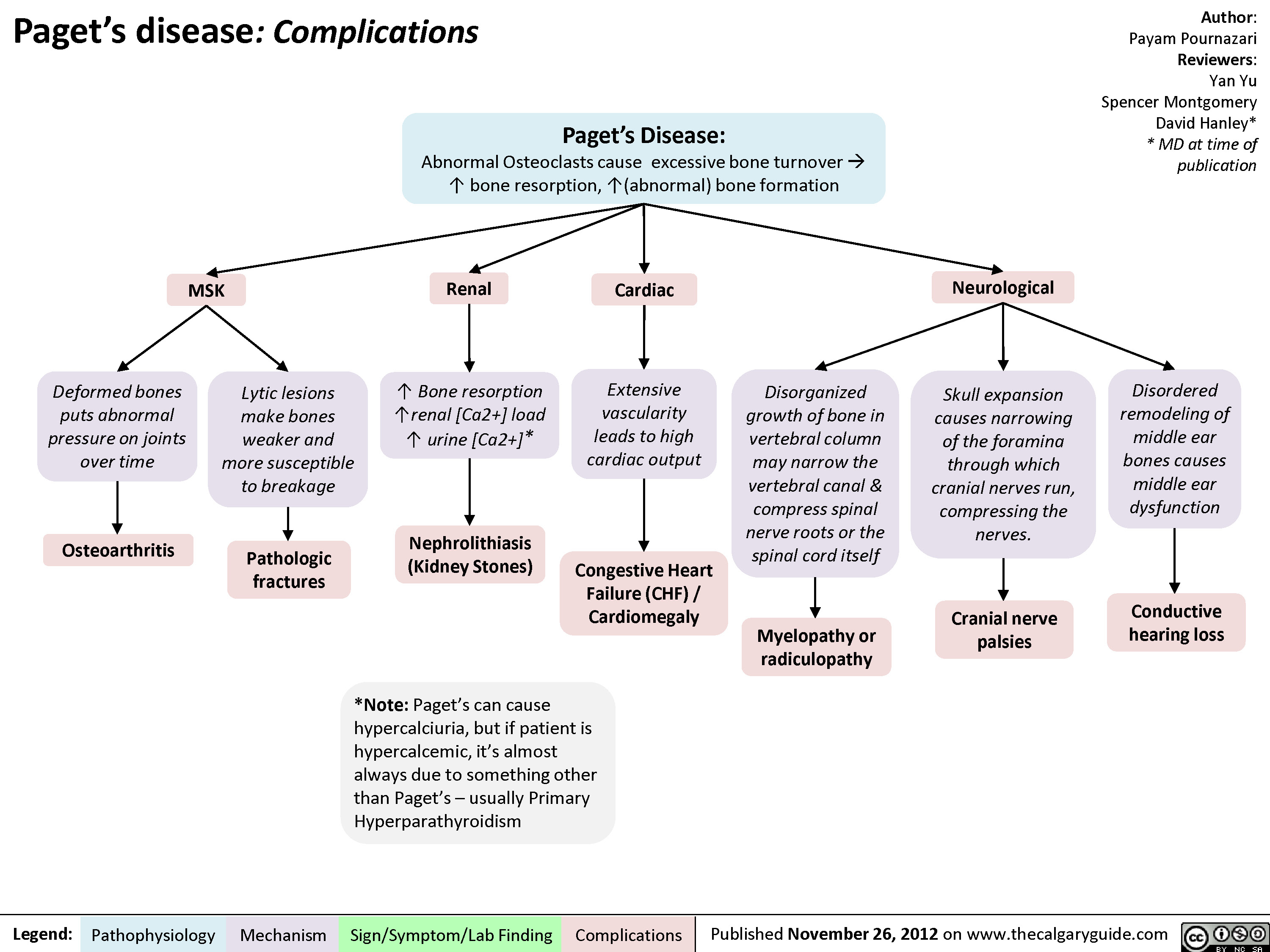
Pagets Disease Complications
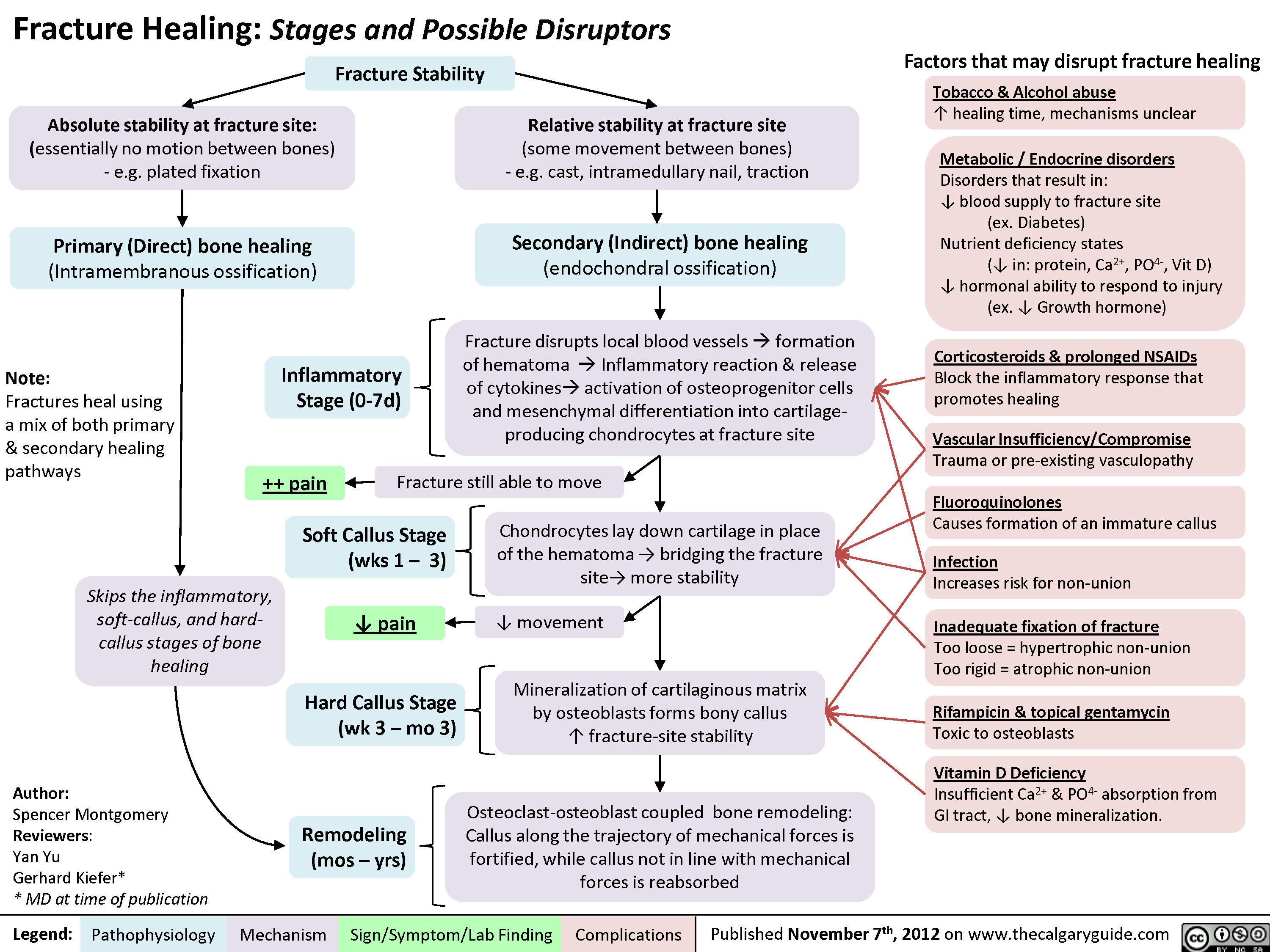
Fracture Healing (and disruptors of this process)
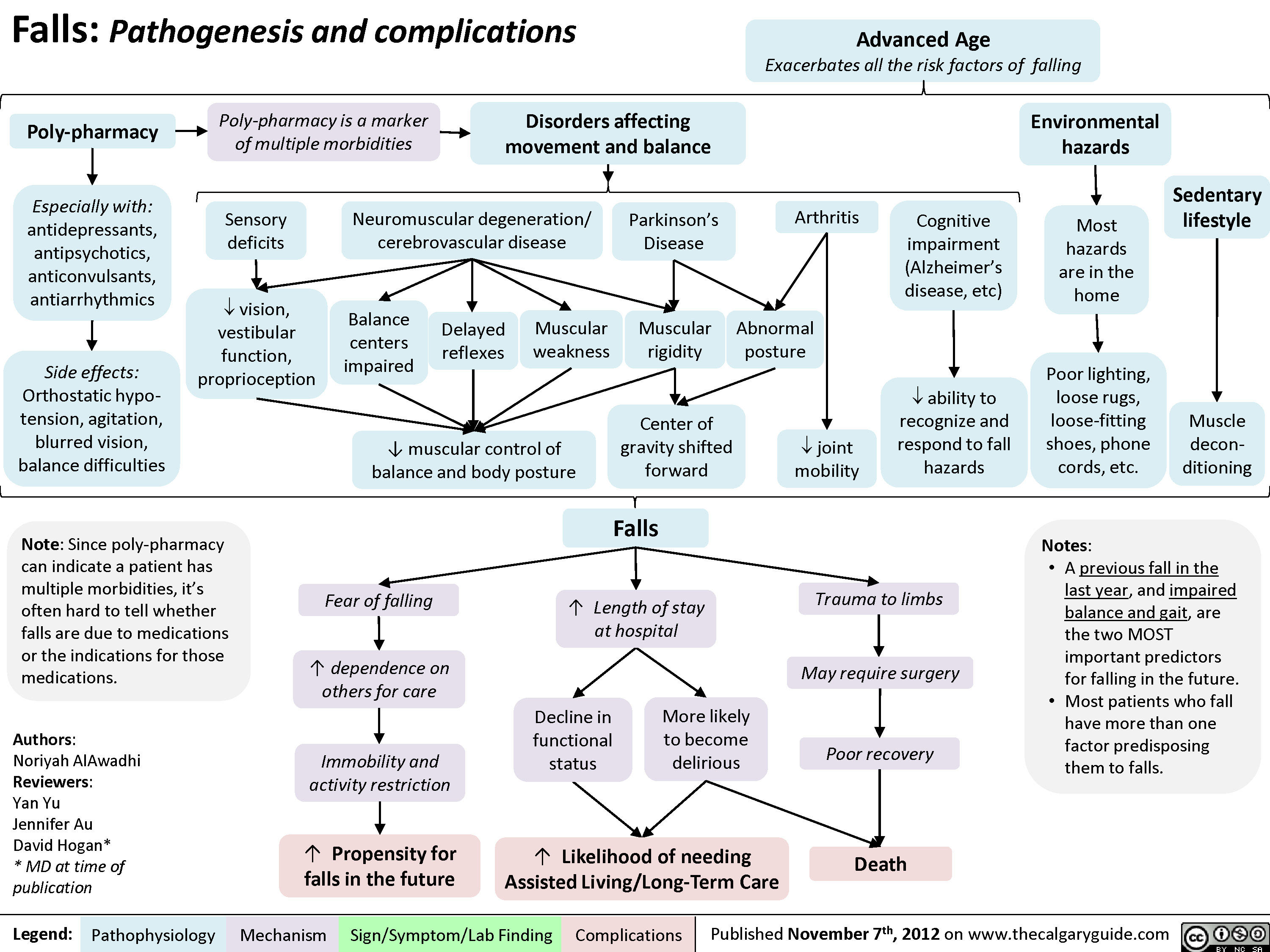
Falls
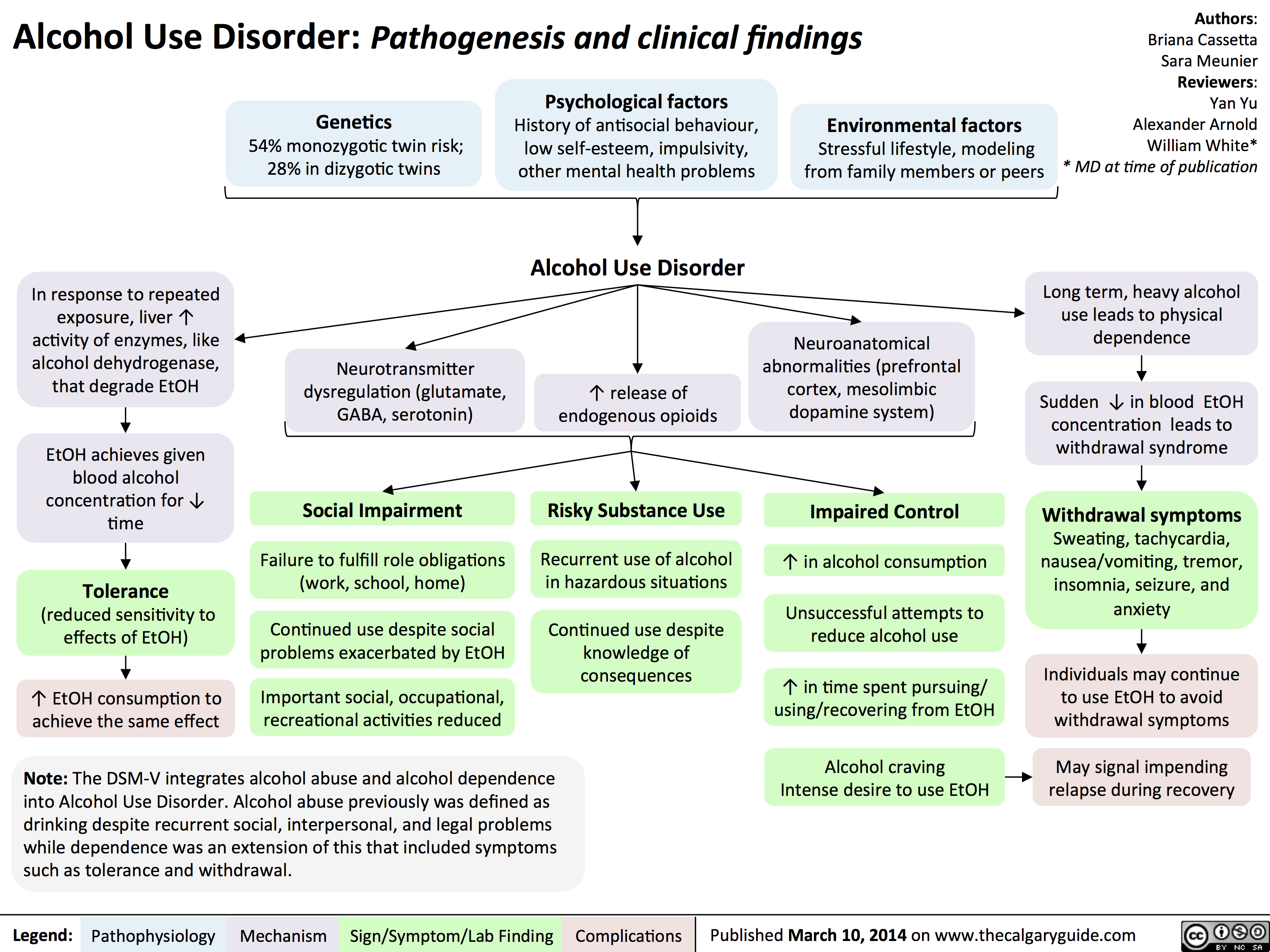
Alcohol Use Disorder
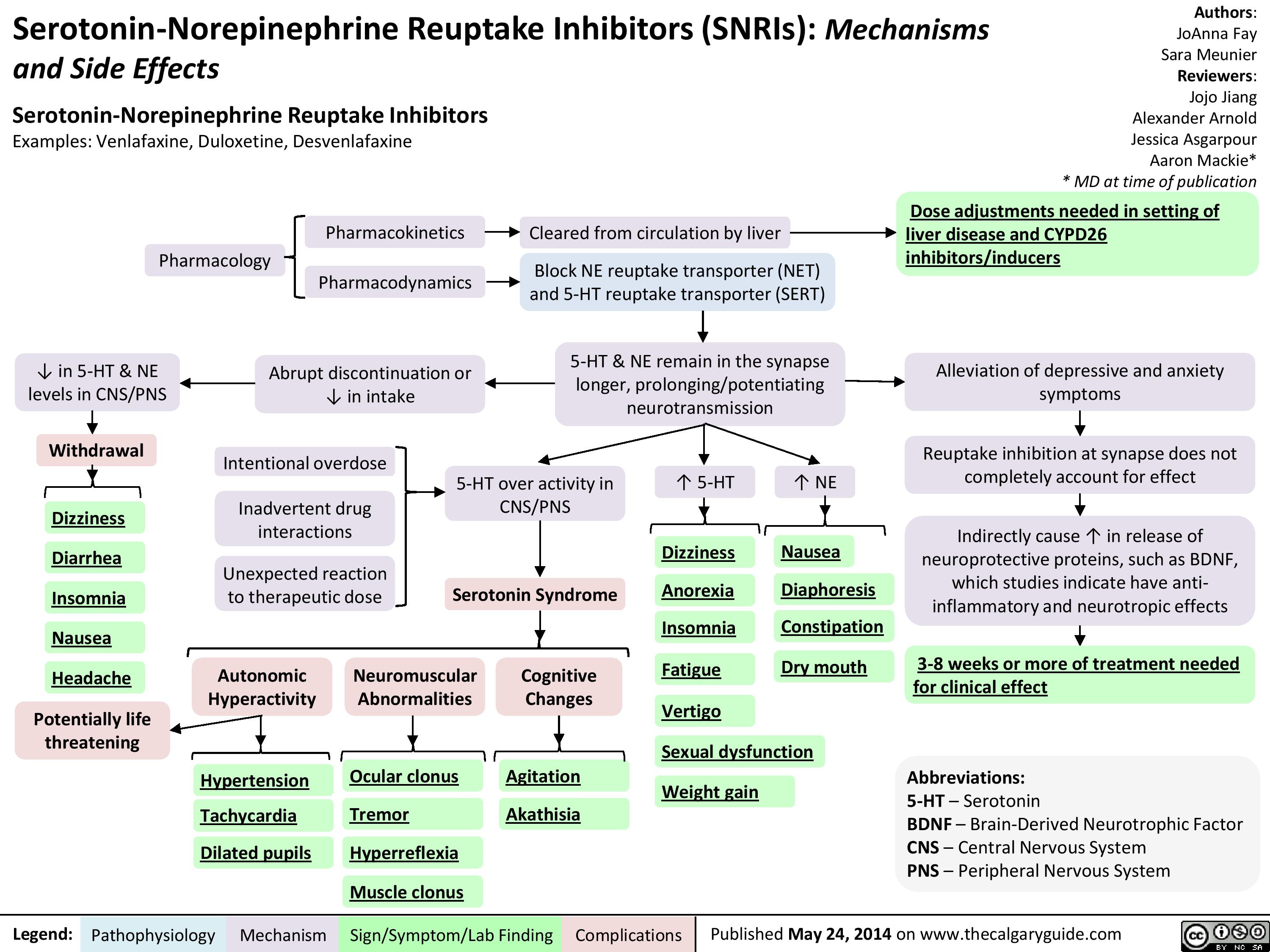
SNRIs
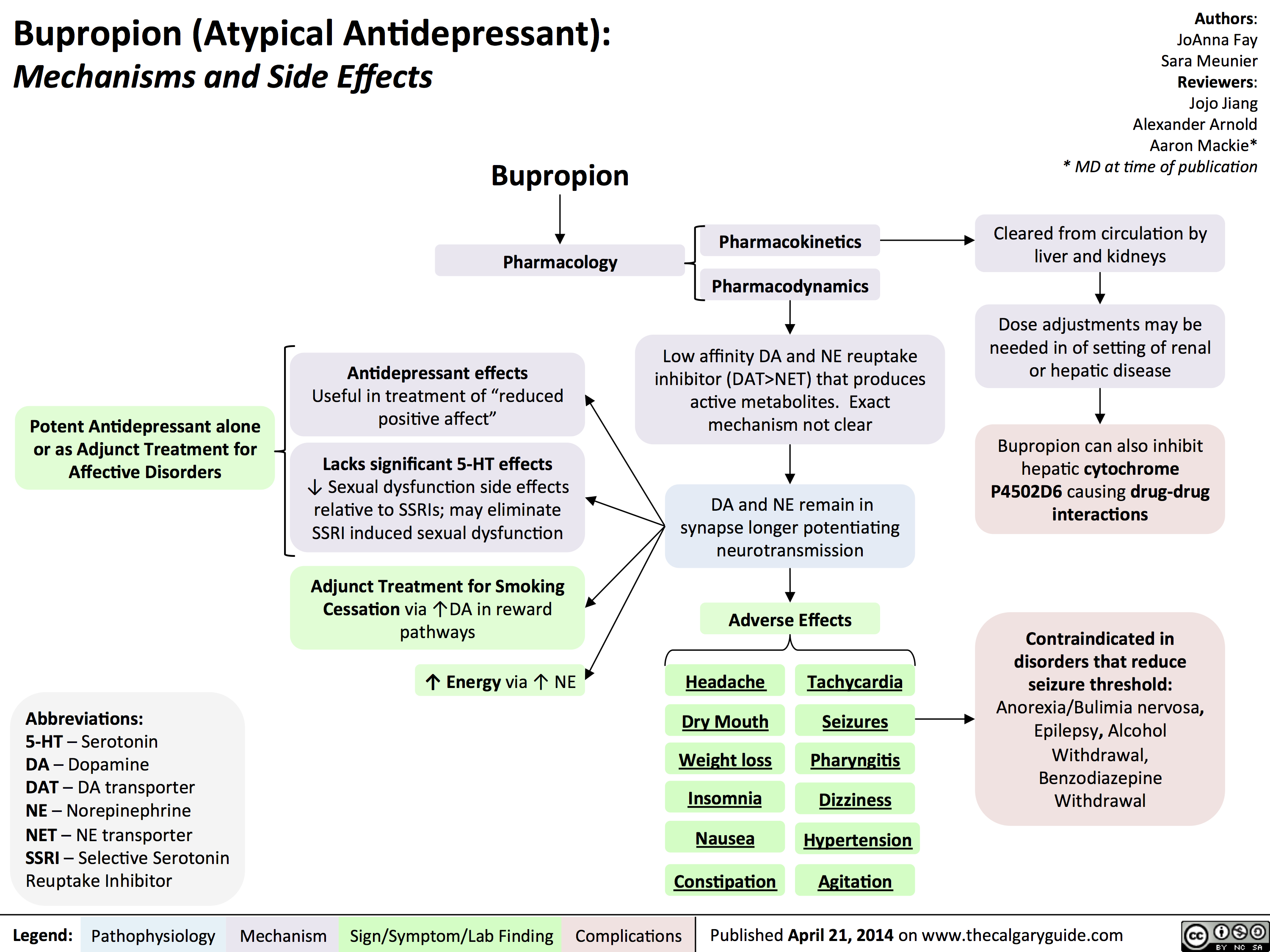
Bupropion
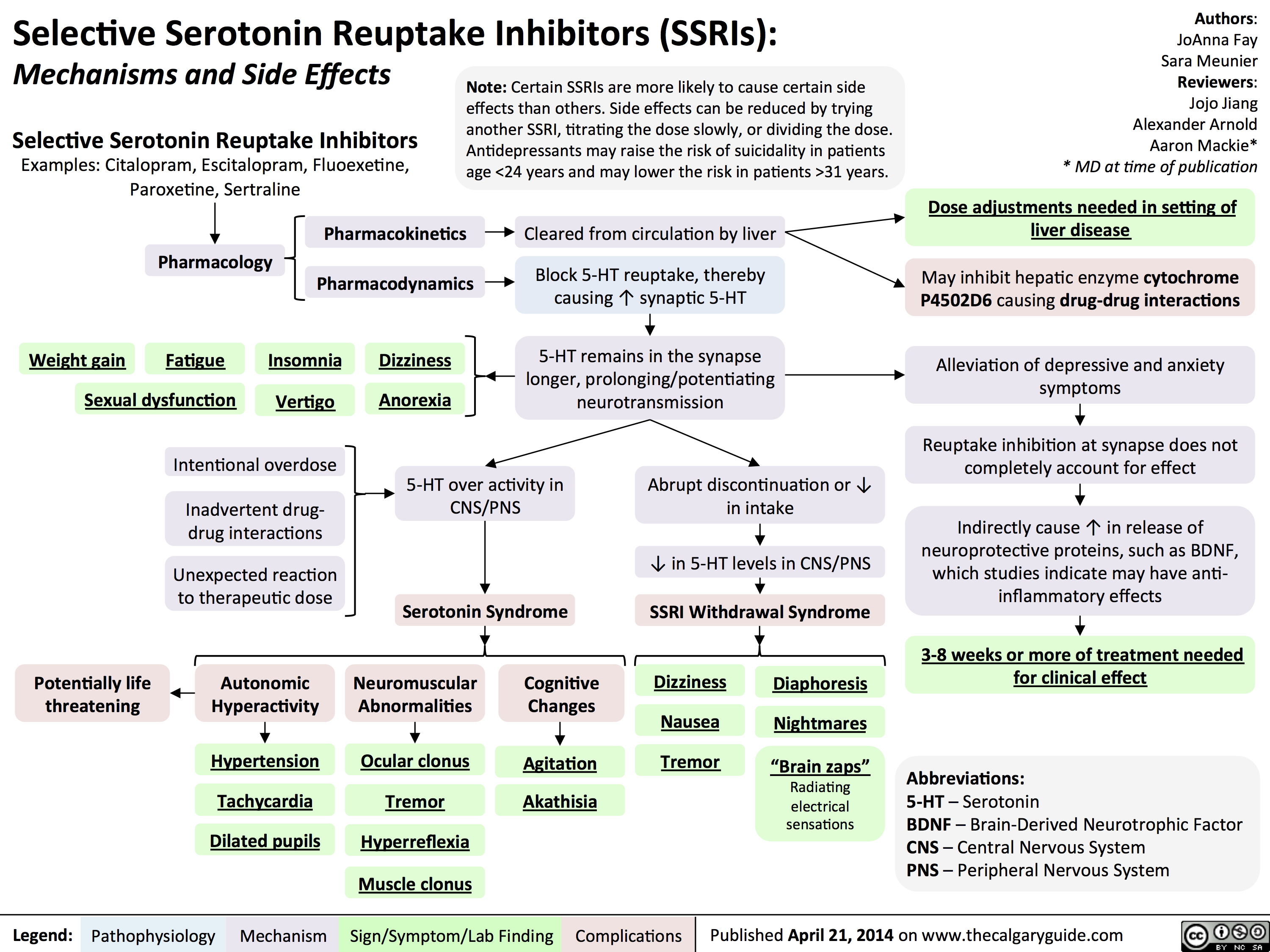
SSRIs
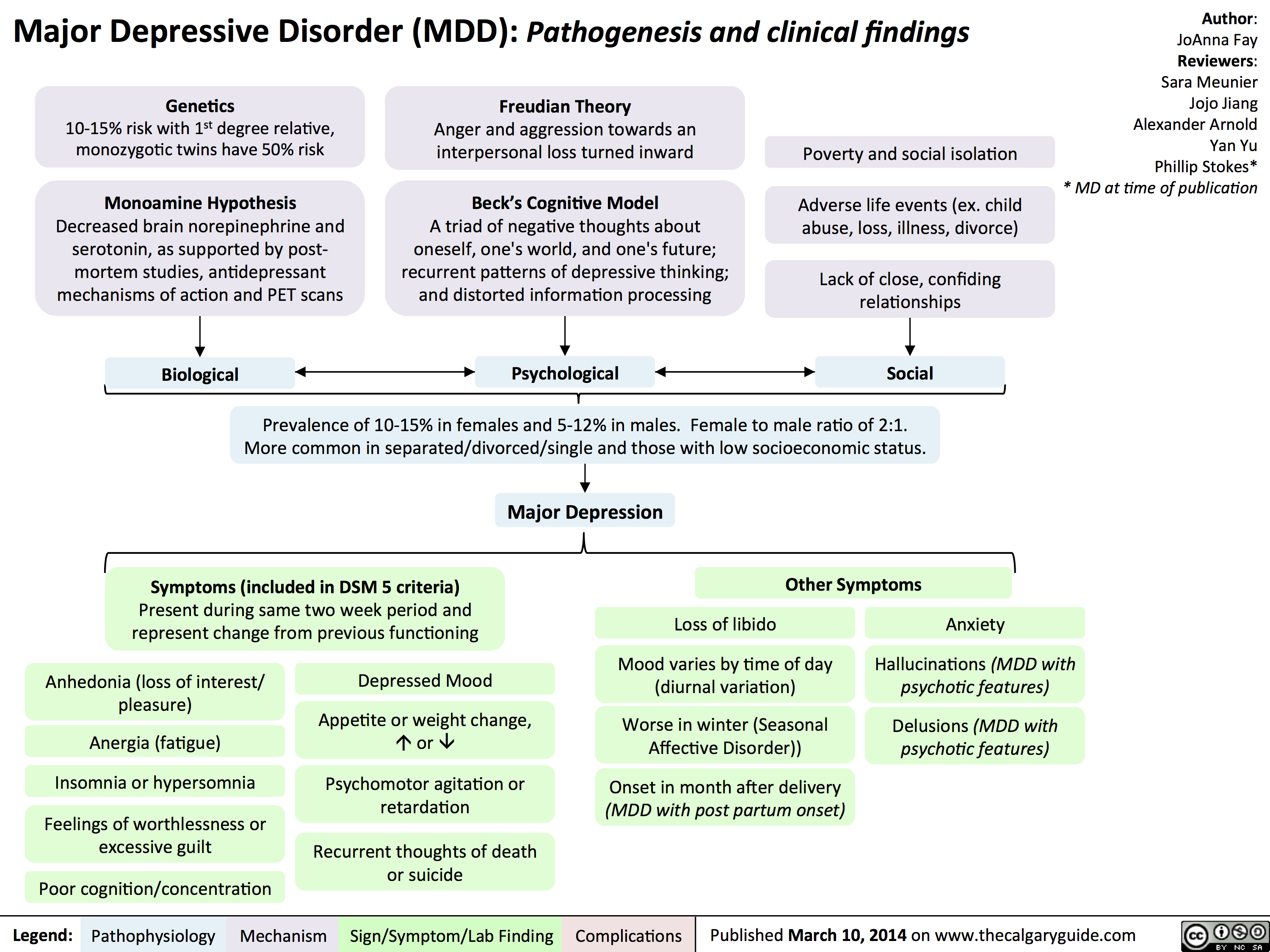
MDD
BipolarDisorder

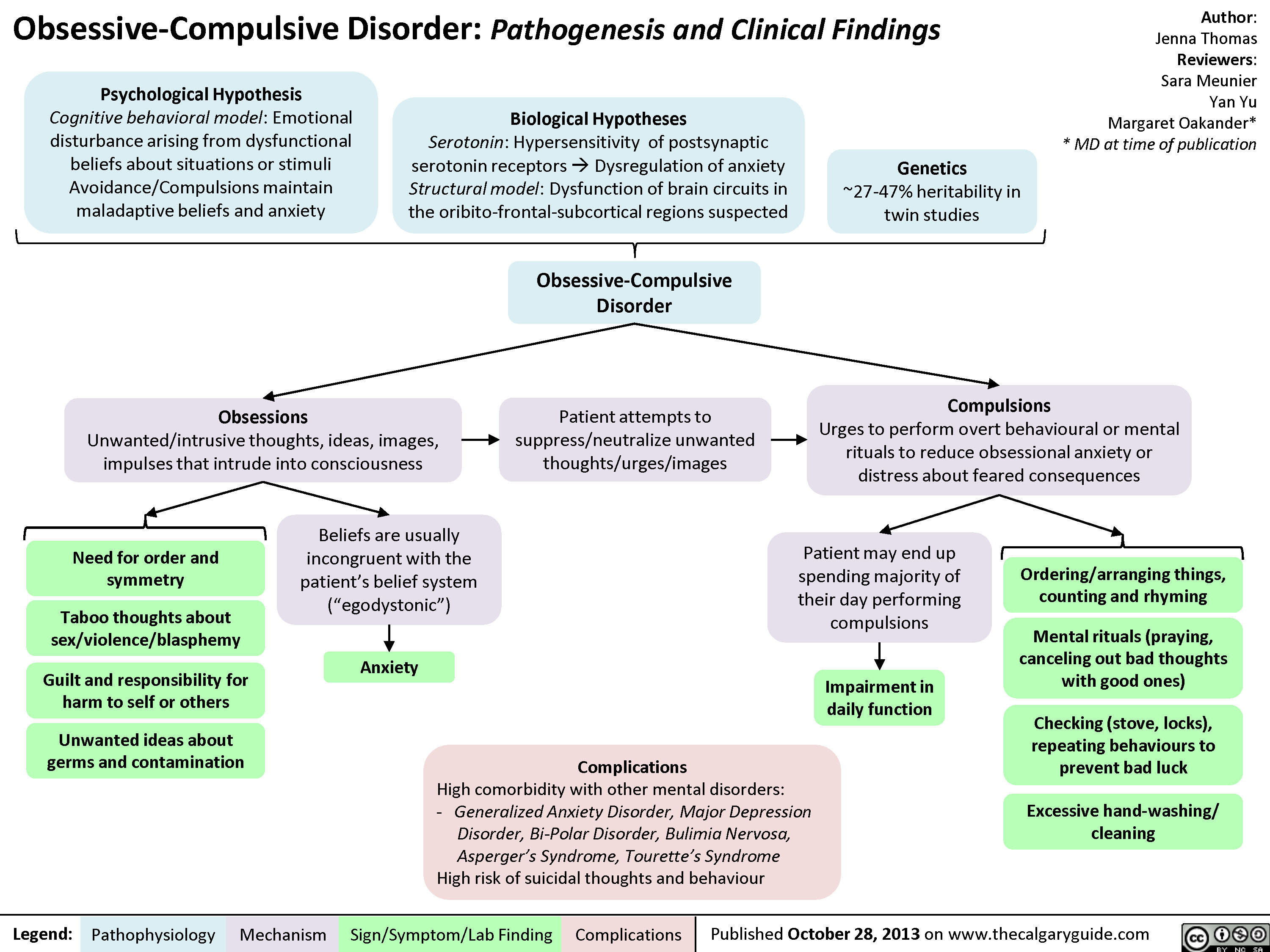
OCD
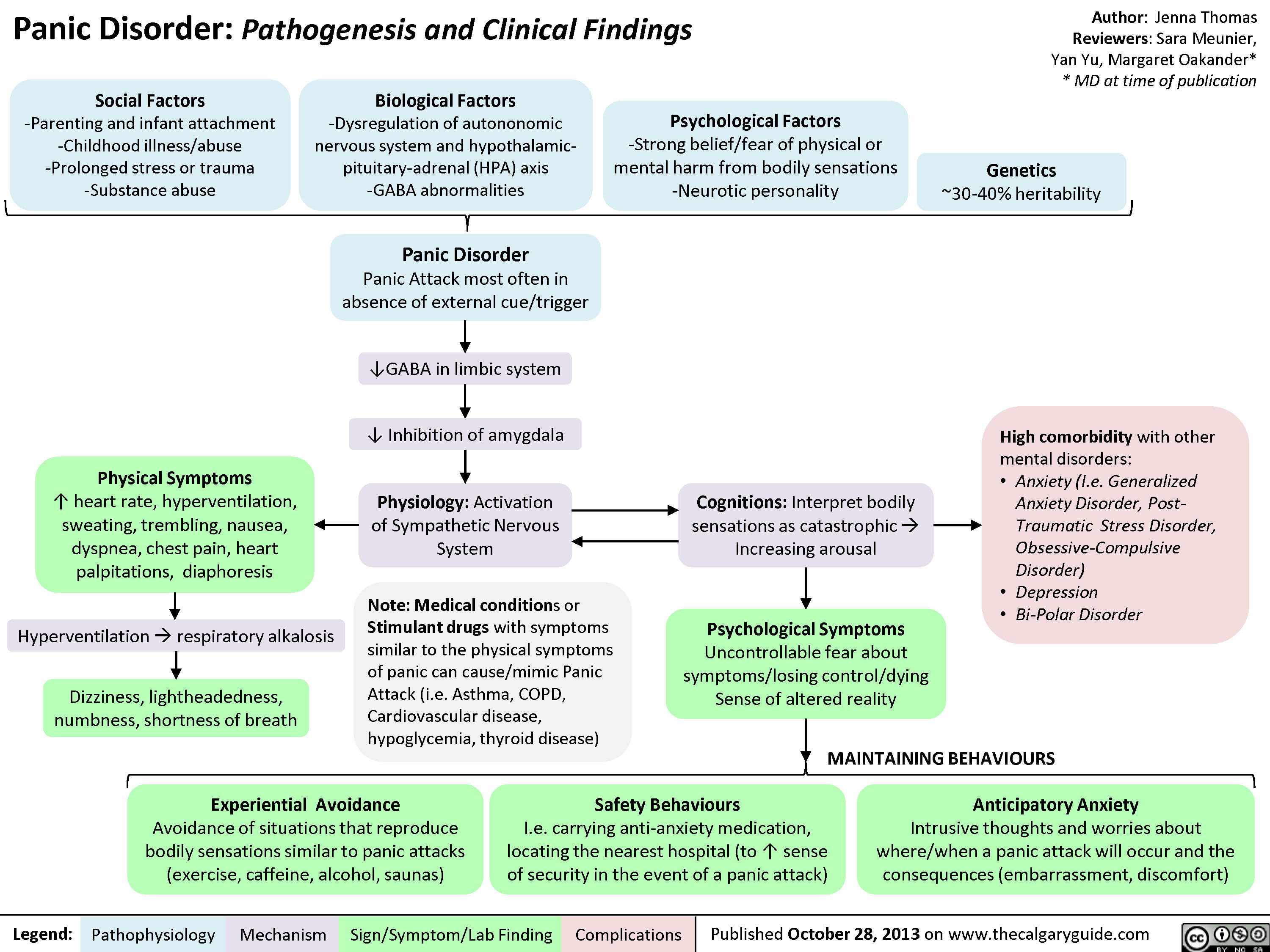
Panic Disorder
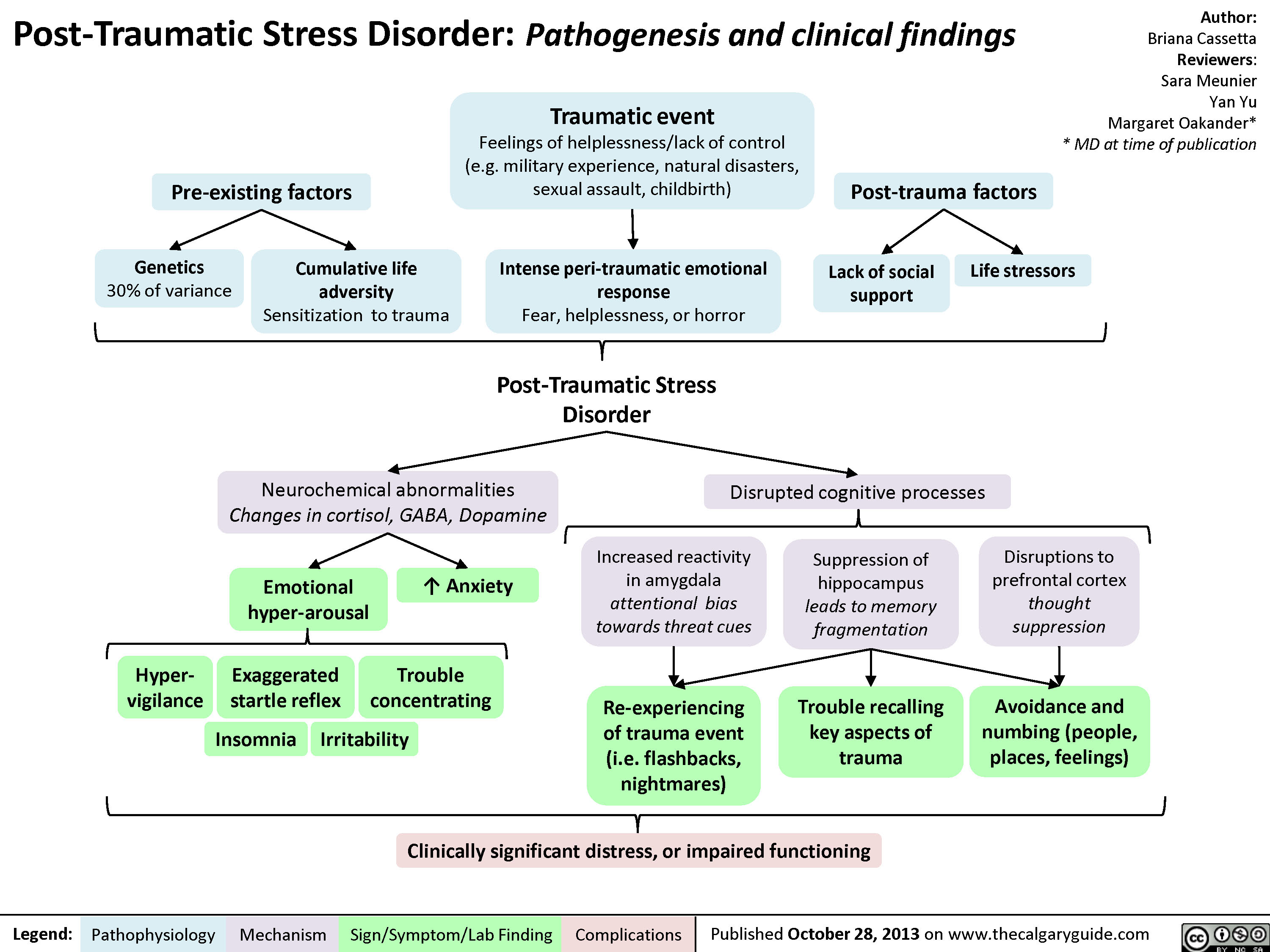
PTSD
Social Anxiety
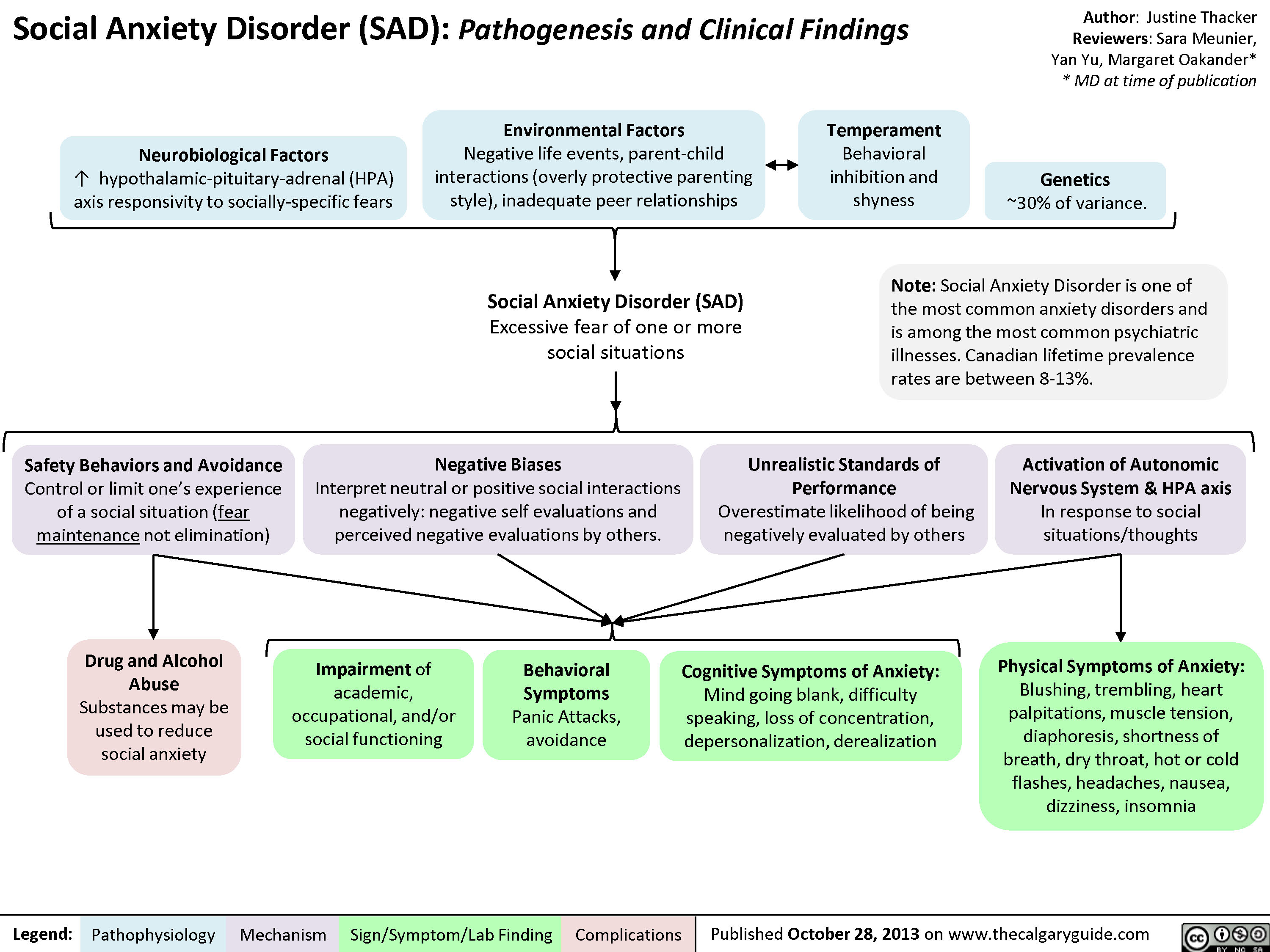
Pathogenesis of Anxiety Disorders
Sense of foreboding or apprehensionActivation of hypothalamus-pituitary-adrenal cortex axisPredisposition to anxiety: Imbalance and/or abnormal functioning of norepinephrine, serotonin, dopamine, and gamma-aminobutyric acid (GABA) Female gender (may be related to hormonal factors, less internal locus of control, greater reporting rates)Other biological theories (under investigation)Prefrontal Cortex modulation of amygdala impairedUnpleasant tensionAmygdala maladaptively activates fear response? Cortisol releaseChronic activation of stress hormones over time causes death of neurons in the hippocampusAnxiety Disorders:A maladaptive emotional state causing fear, worry, and excessive stress, characterized by:Perceived environmental threatHippocampus and Cingulate Gyrus abnormally process threatActivation of autonomic nervous system and adrenal medulla? Epinephrine releaseHippocampus shrinks in sizeAbility of hippocampus to normally integrate environmental stimuli is further compromisedMood dysregulationMemory impairmentStrong association between anxiety disorders and depressionMeasurable ? in Brain-Derived Neurotrophic factor (BDNF)BDNF value correlates with the degree of neuronal loss in the hippocampus
97 kB / 173 words")
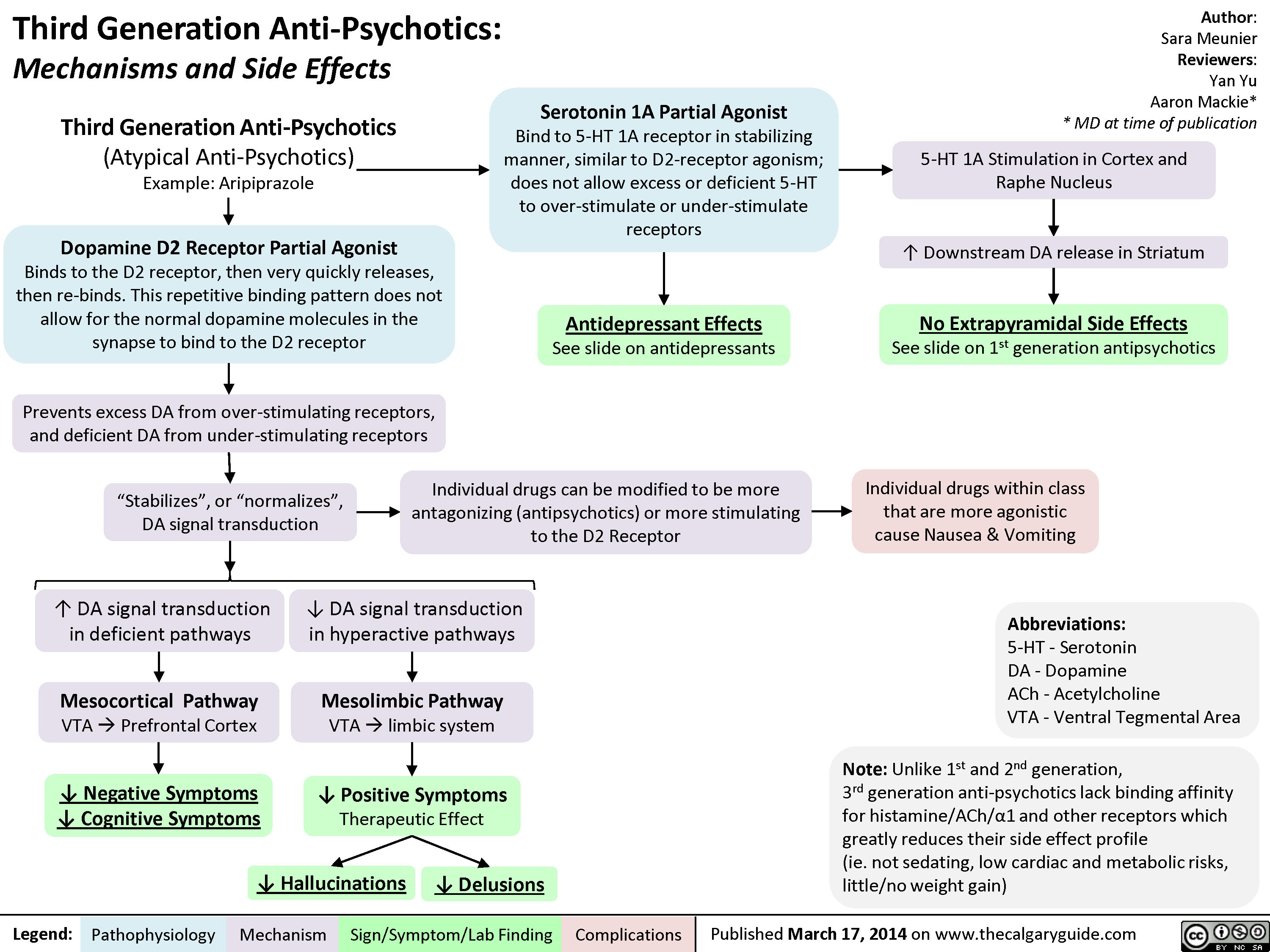
3rd gen anti-psychotics
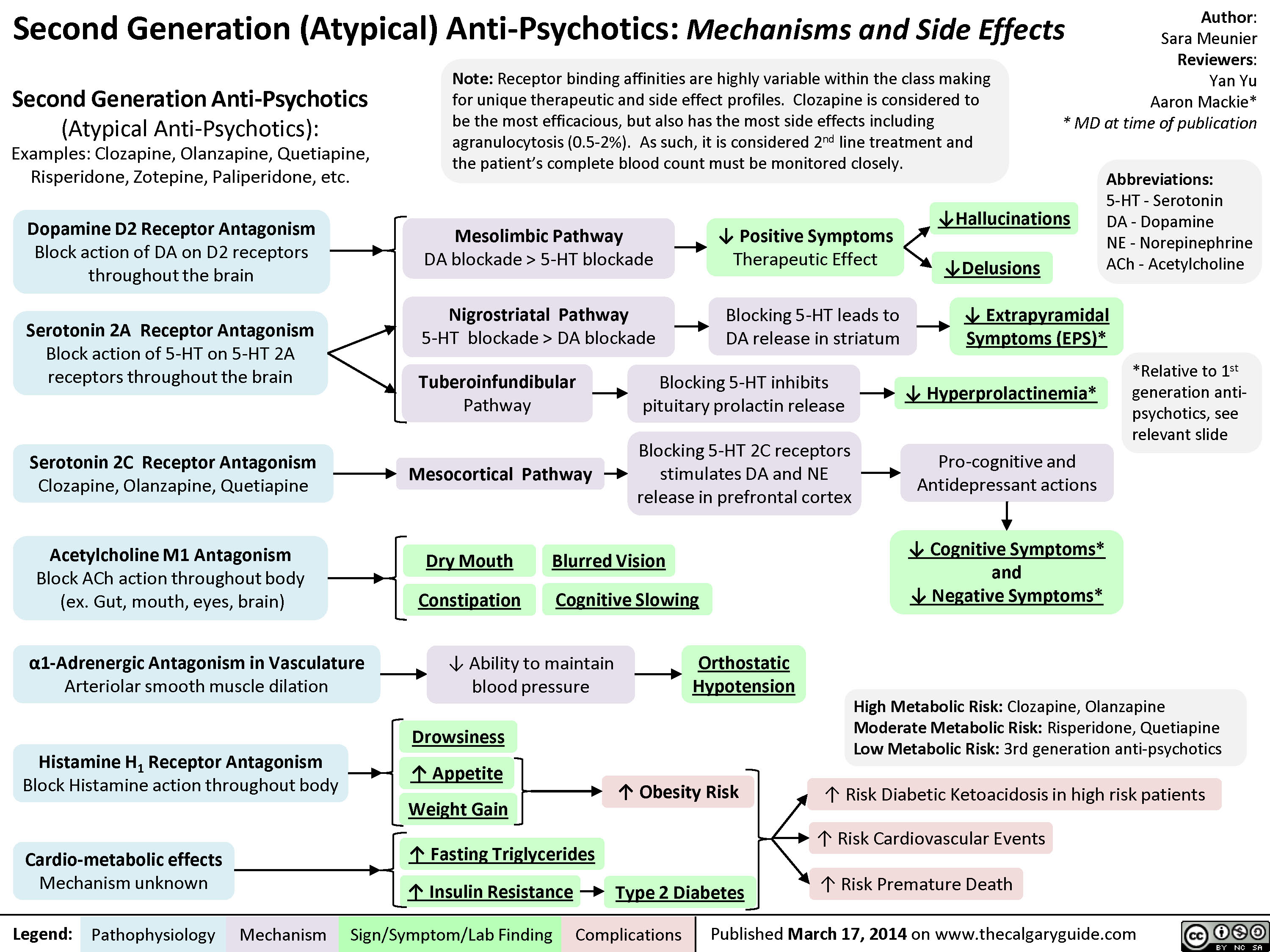
2nd generation antipsychotics
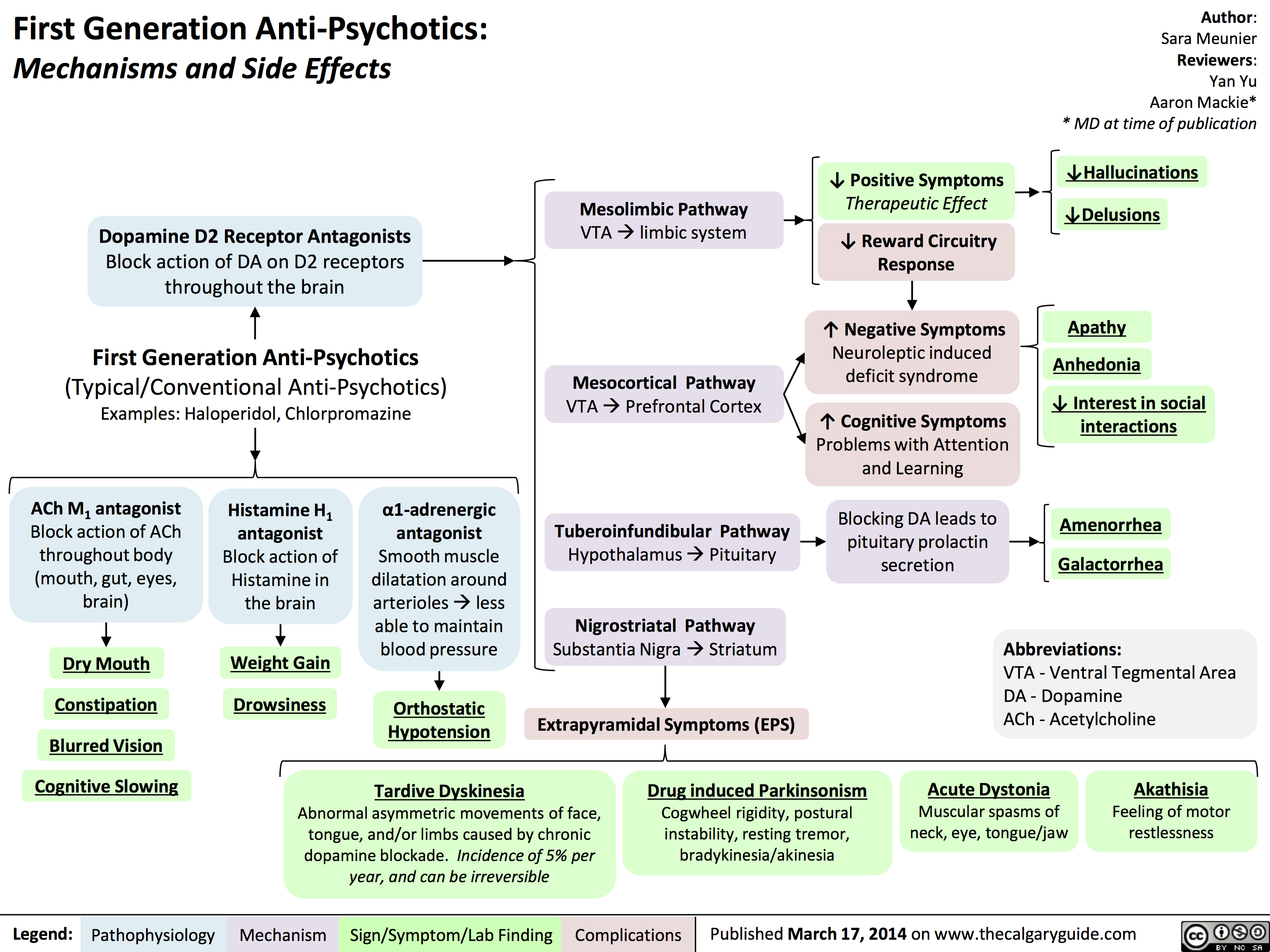
1st gen antipsychotics
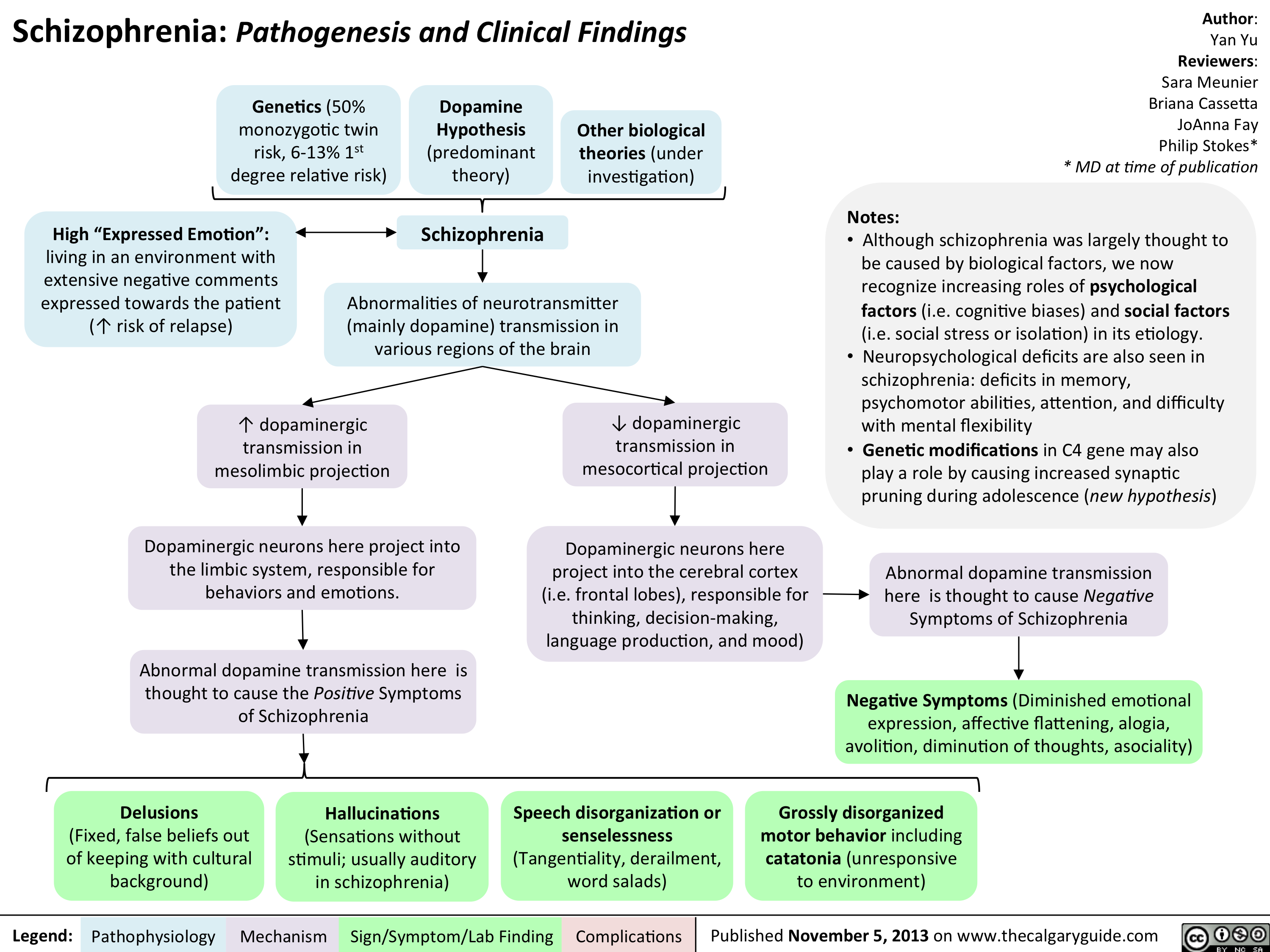
Schizophrenia Pathogenesis and Clinical Findings
? dopaminergic transmission in mesocortical projection? dopaminergic transmission in mesolimbic projection Author: Yan YuReviewers:Sara Meunier Briana CassettaJoAnna FayPhilip Stokes** MD at time of publicationLegend:Published November 5, 2013 on www.thecalgaryguide.comMechanismPathophysiologySign/Symptom/Lab FindingComplicationsGenetics (50% monozygotic twin risk, 6-13% 1st degree relative risk)Speech disorganization or senselessness (Tangentiality, derailment, word salads)Dopaminergic neurons here project into the limbic system, responsible for behaviors and emotions.SchizophreniaDopamine Hypothesis(predominant theory)Other biological theories (under investigation)High")
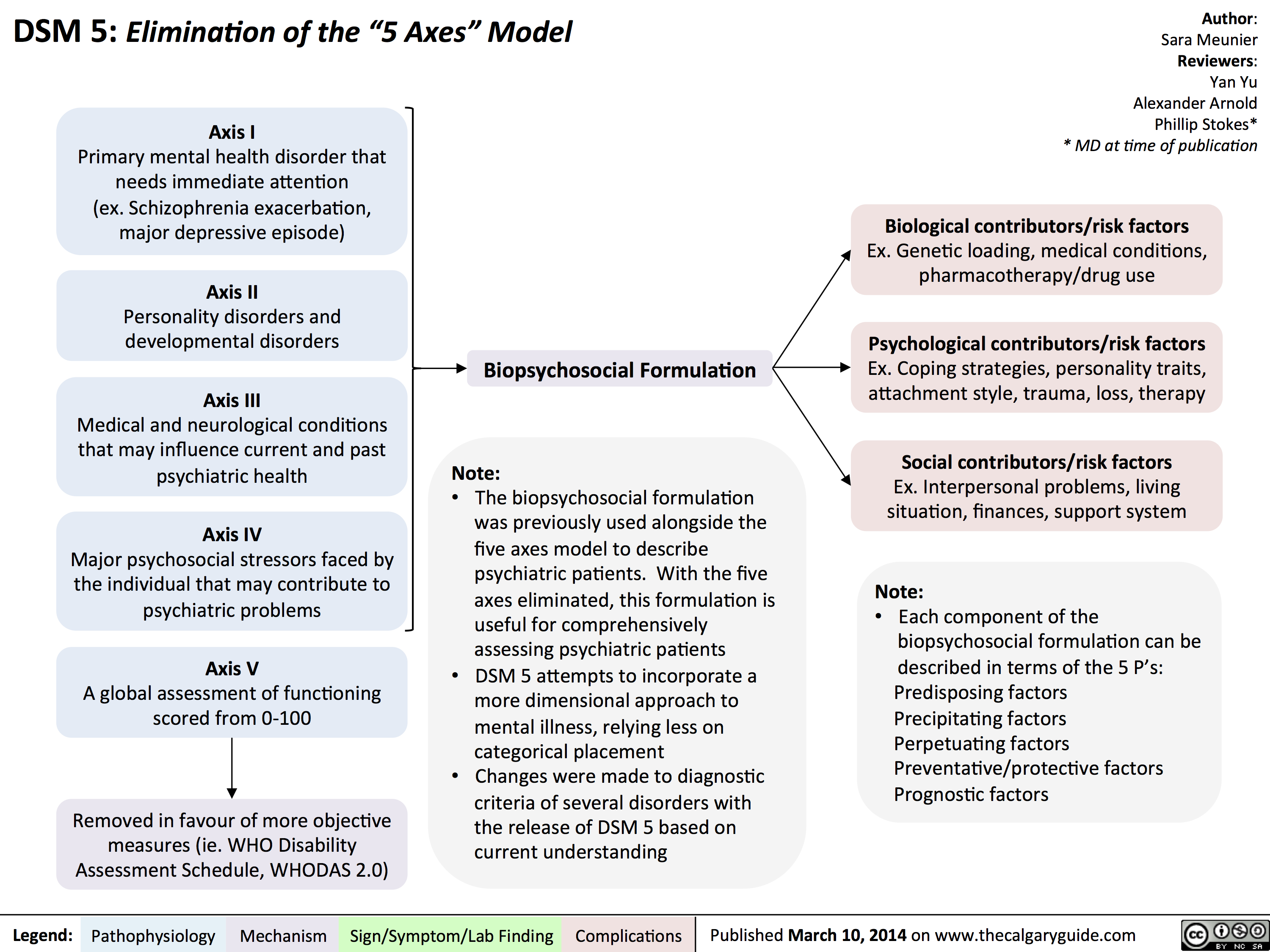
DSM - Axis to Formulation
Complications of Measles Pathogenesis and Clinical Findings
Kawasaki Disease

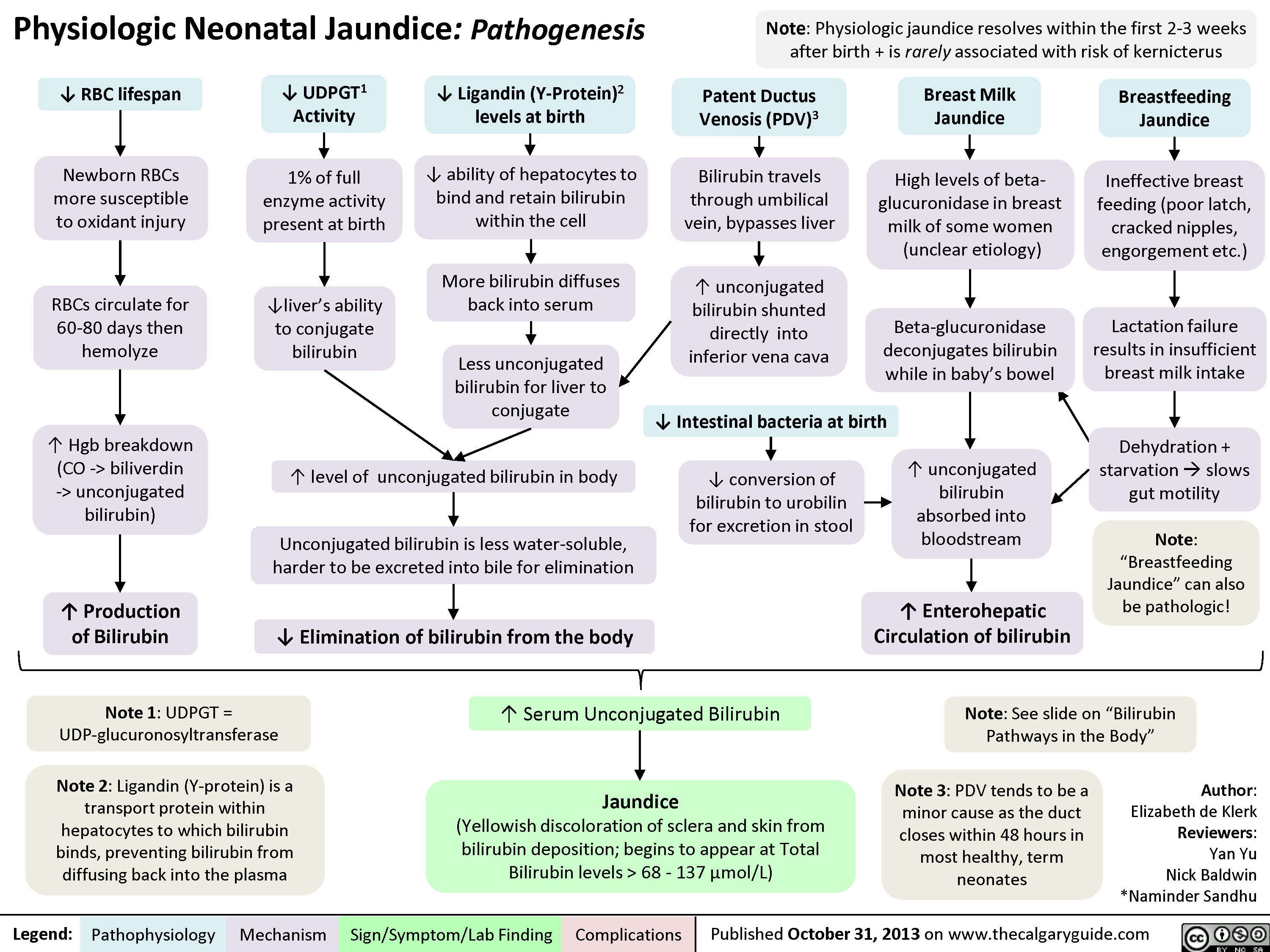
Physiologic Neonatal Jaundice
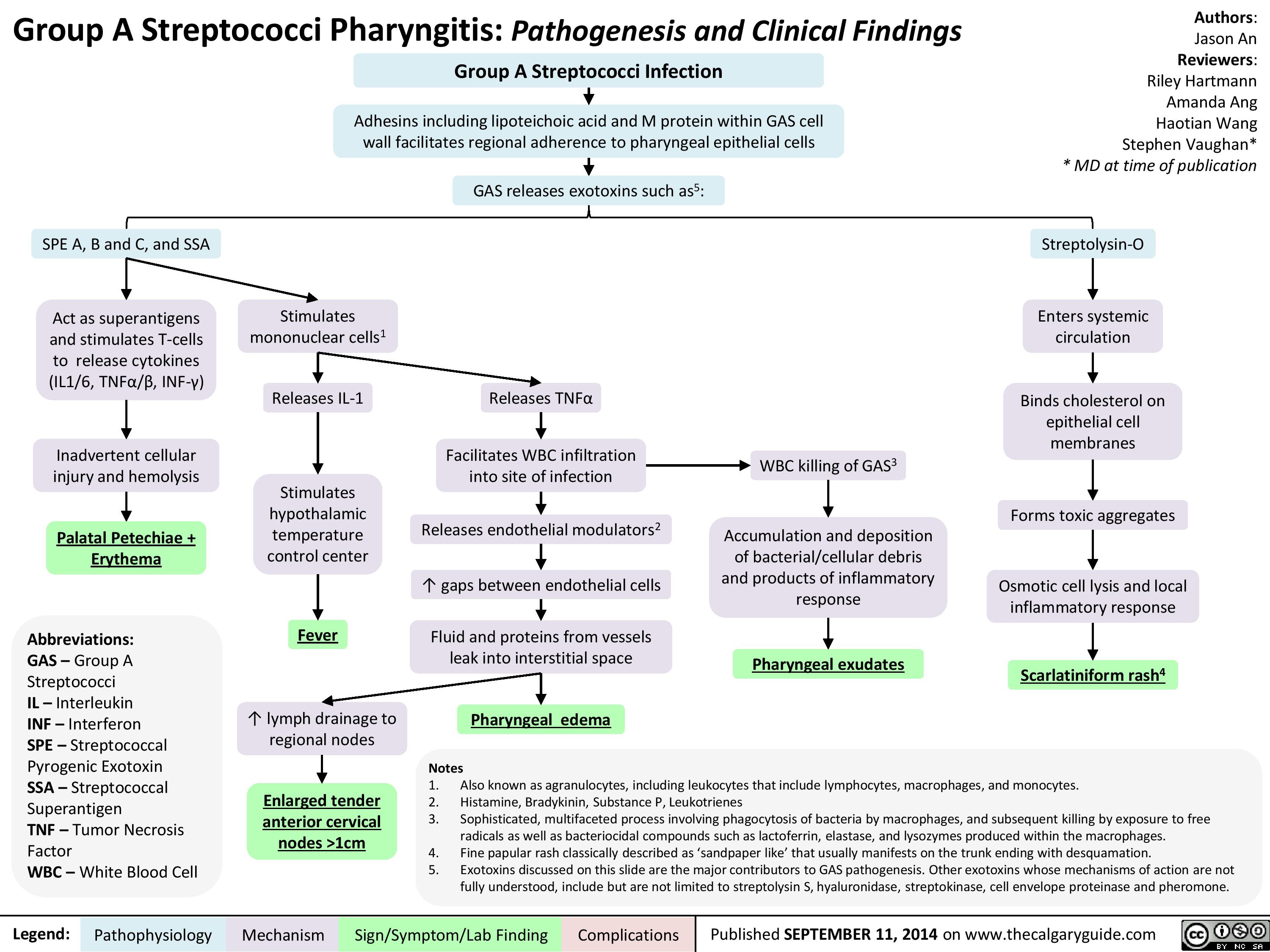
Group A Streptococci Pharyngitis Pathogenesis and Clinical Findings
AcuteOtitisComplications
Acute Otitis Media - Pathogenesis and Clinical Findings (in Children)
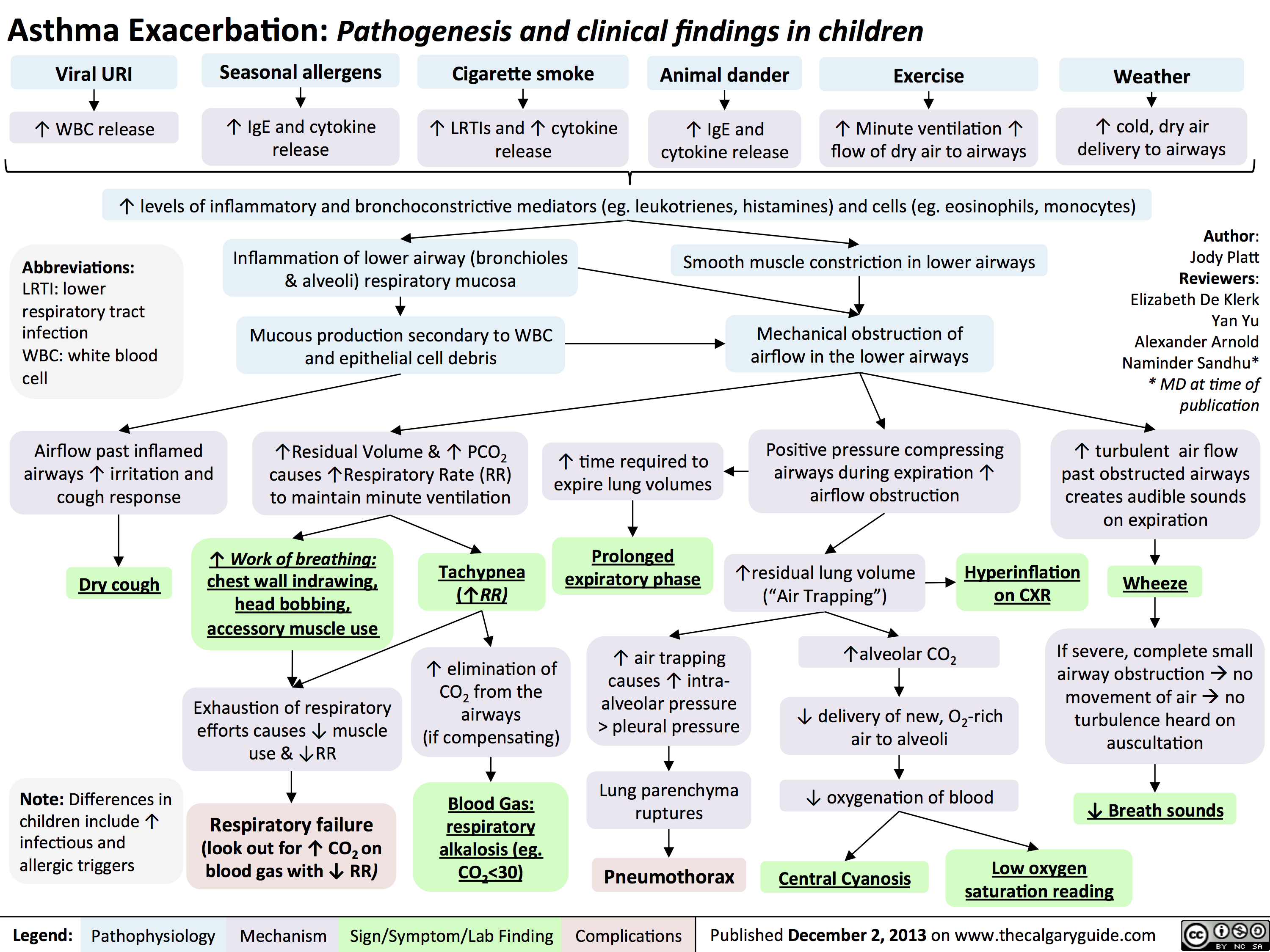
Asthma Exacerbation - Pathogenesis and Clinical Findings in Children
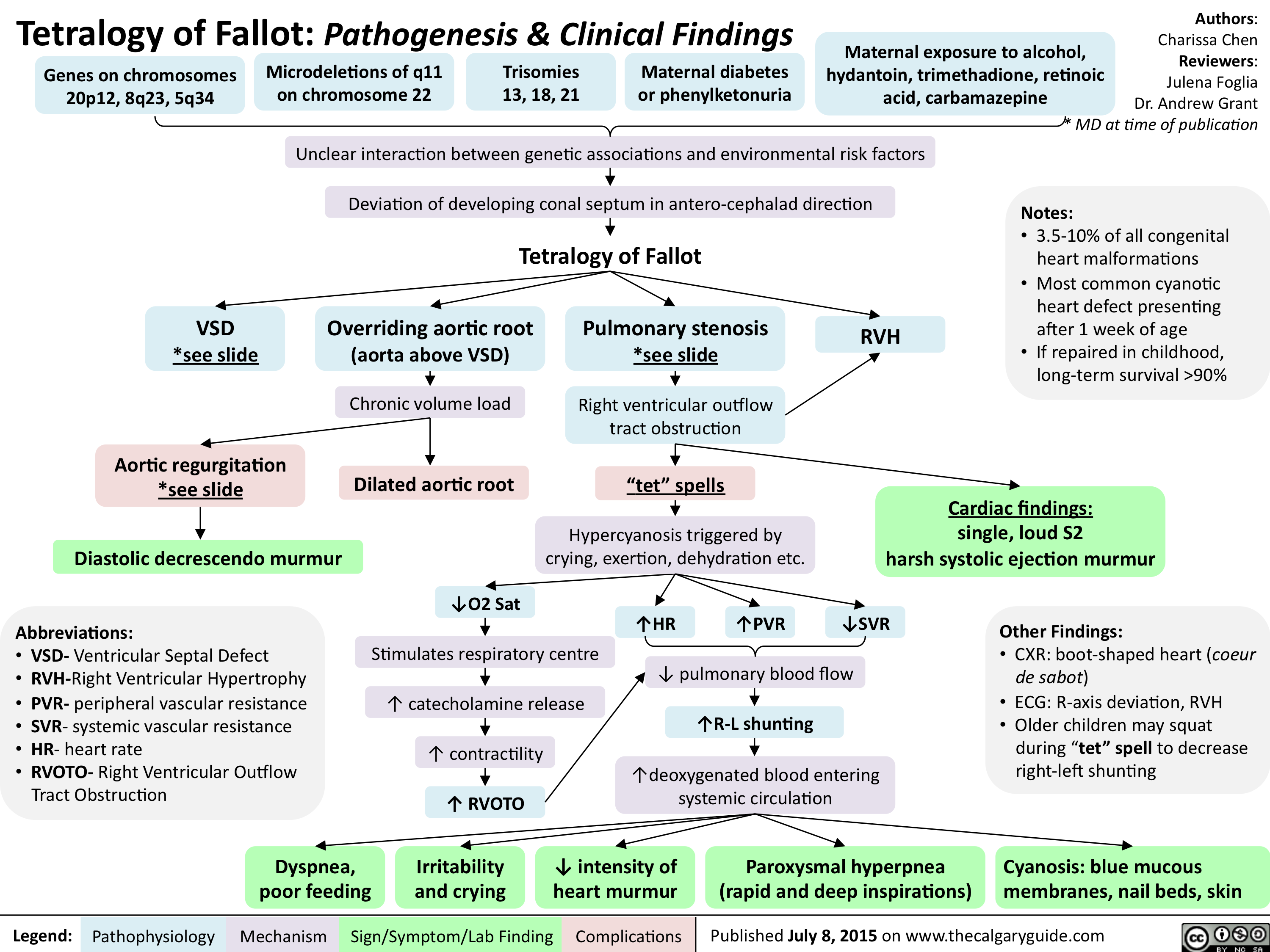
Tetralogy of Fallot-Pathogenesis & Clinical Findings
Transposition of the Great Arteries-Pathogenesis & clinical findings
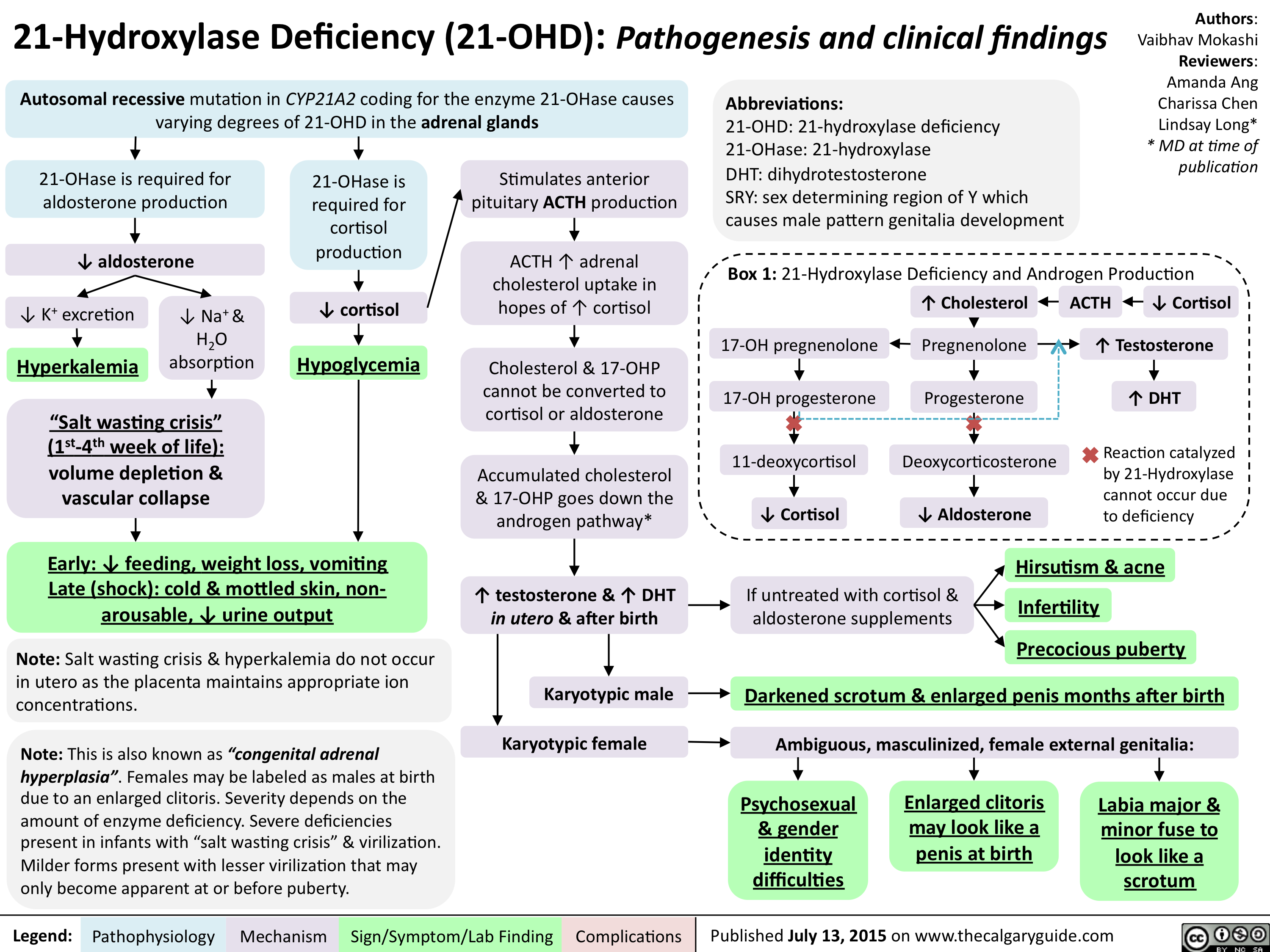
21-Hydroxylase Deficiency-Pathogenesis and clinical findings
Hallux Valgus pathogenesis and clinical findings - August 15 2015

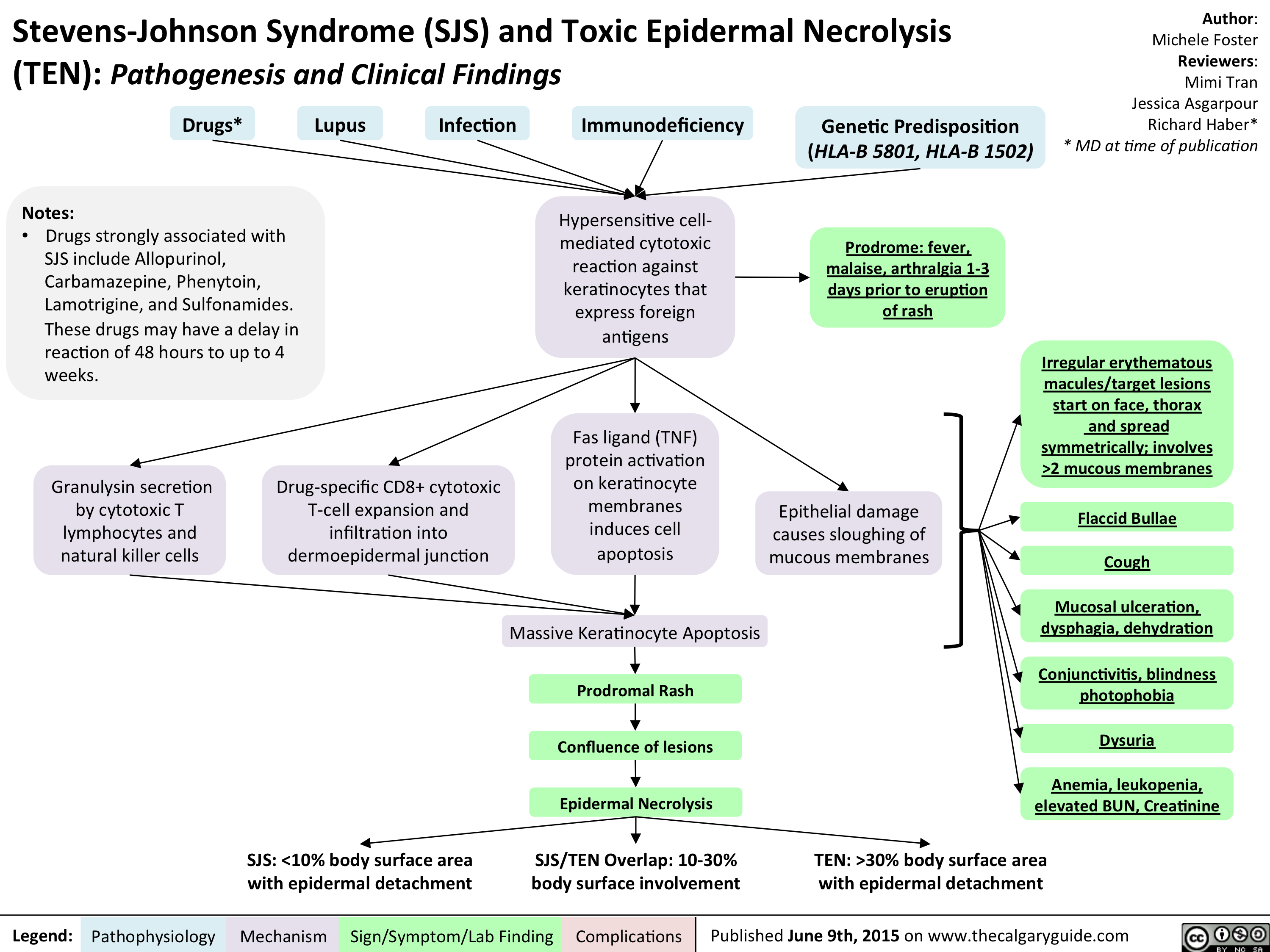
Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) - Pathogenesis and Clinical Findings
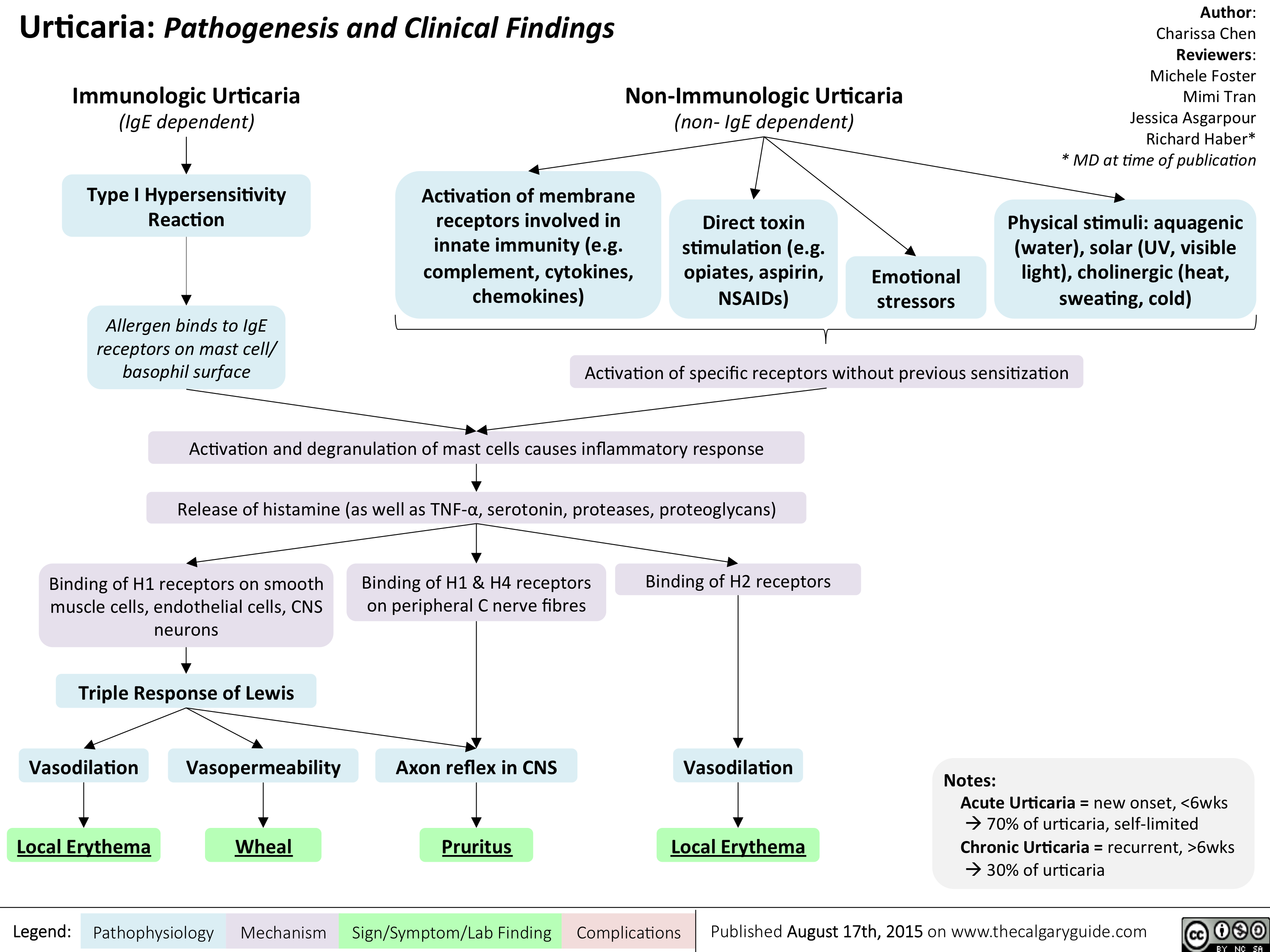
Urticaria- Pathogenesis and Clinical Findings
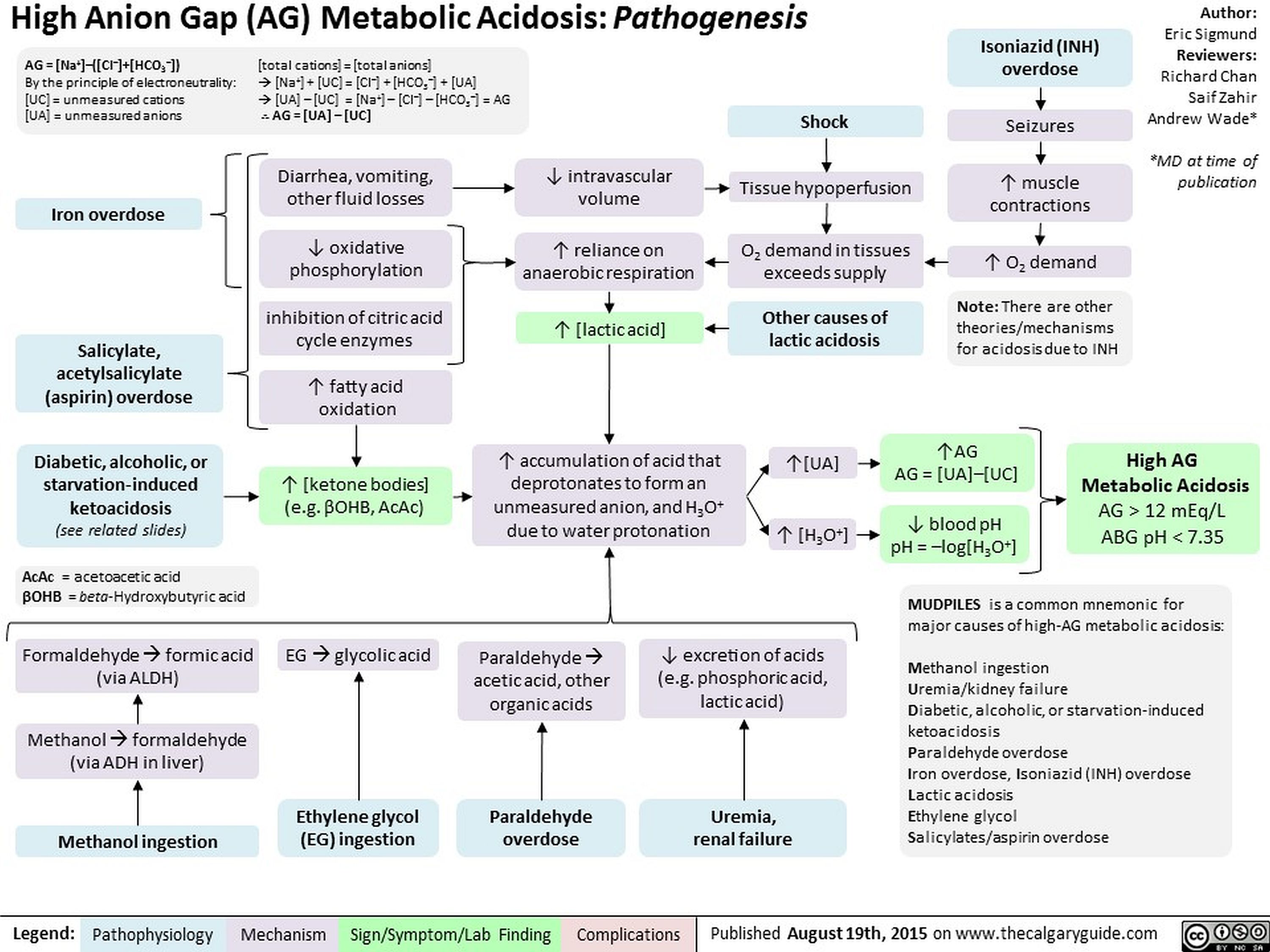
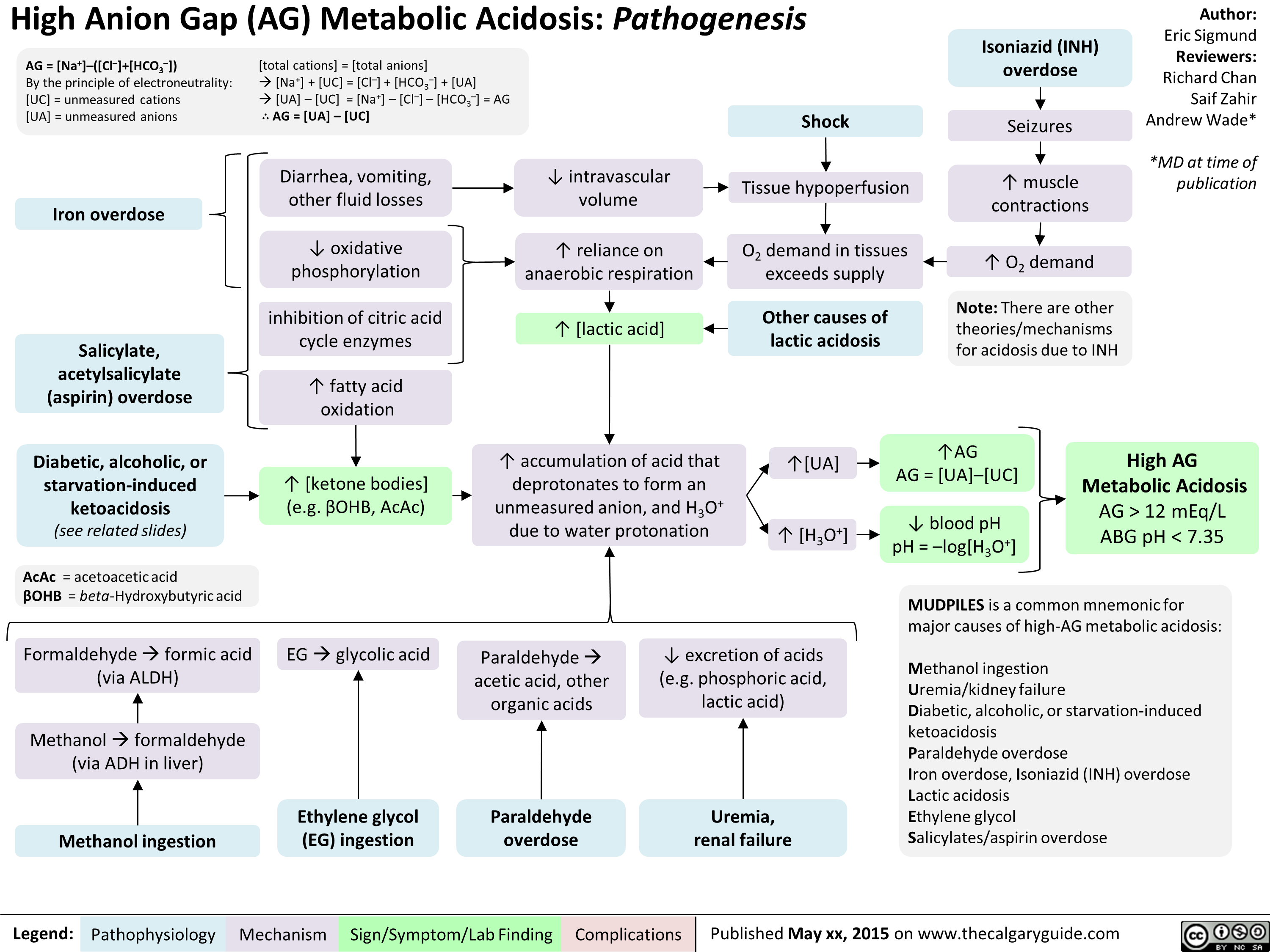
High Anion Gap Metabolic Acidosis Pathogenesis
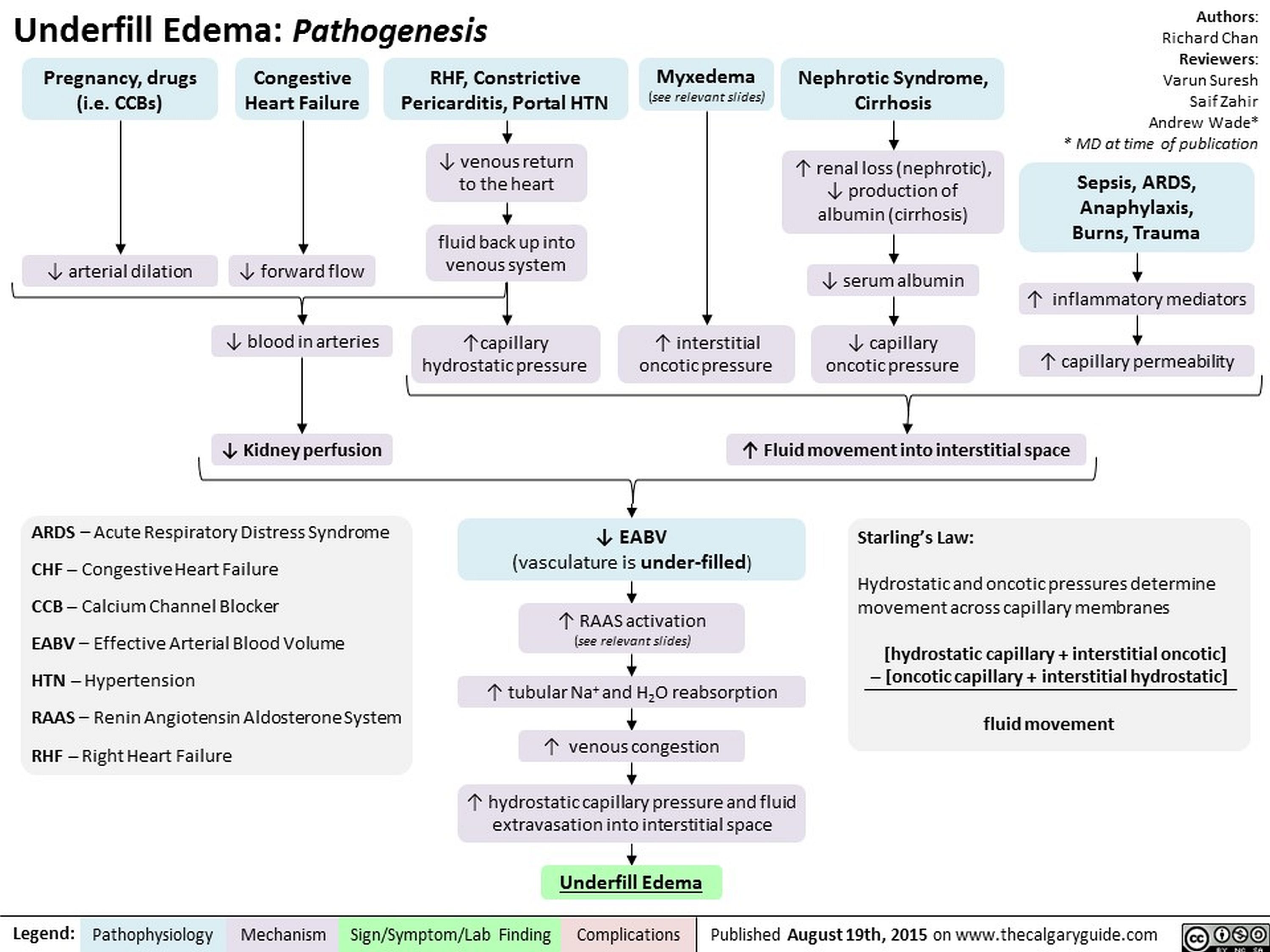
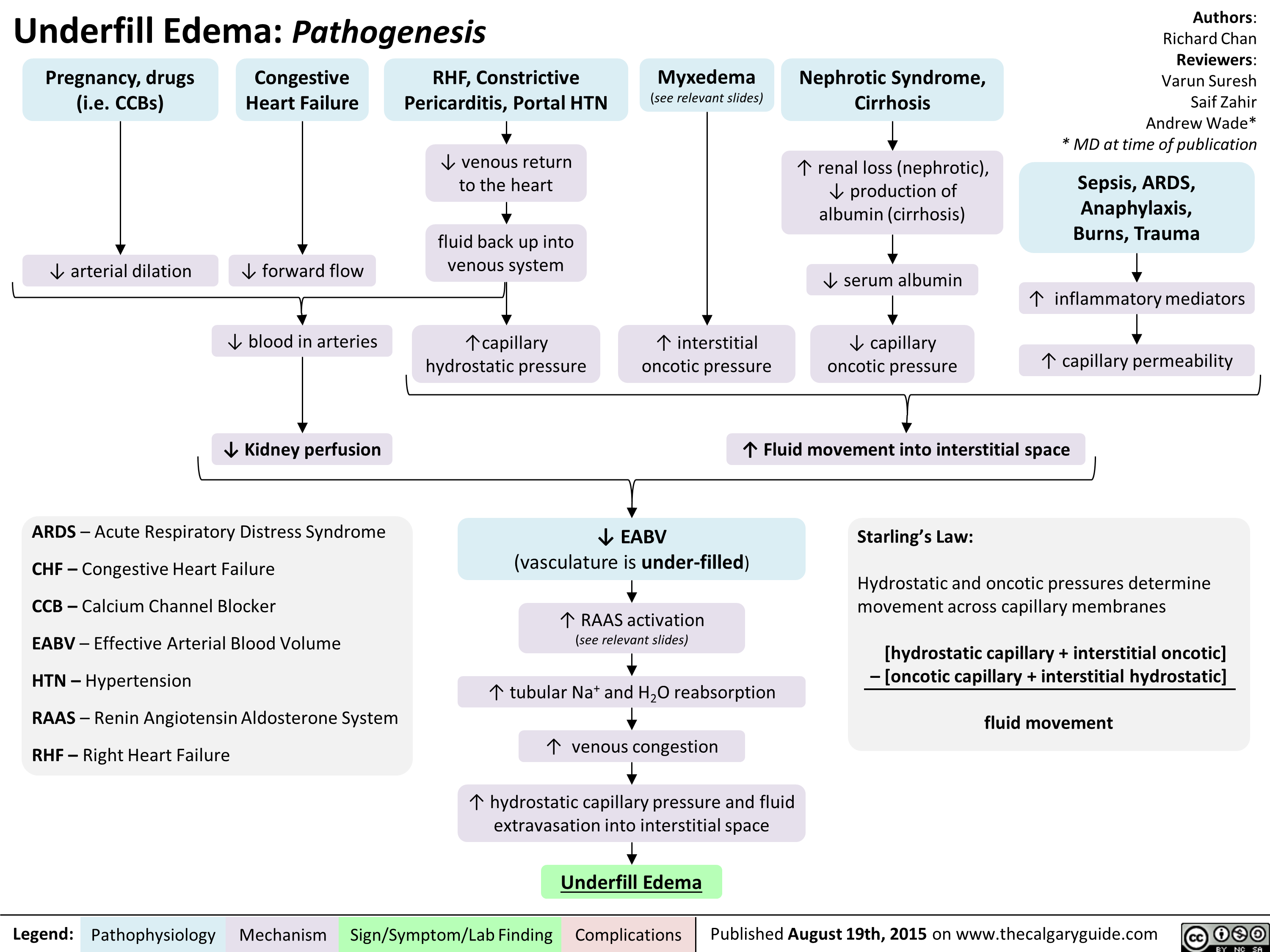
Underfill Edema Pathogenesis
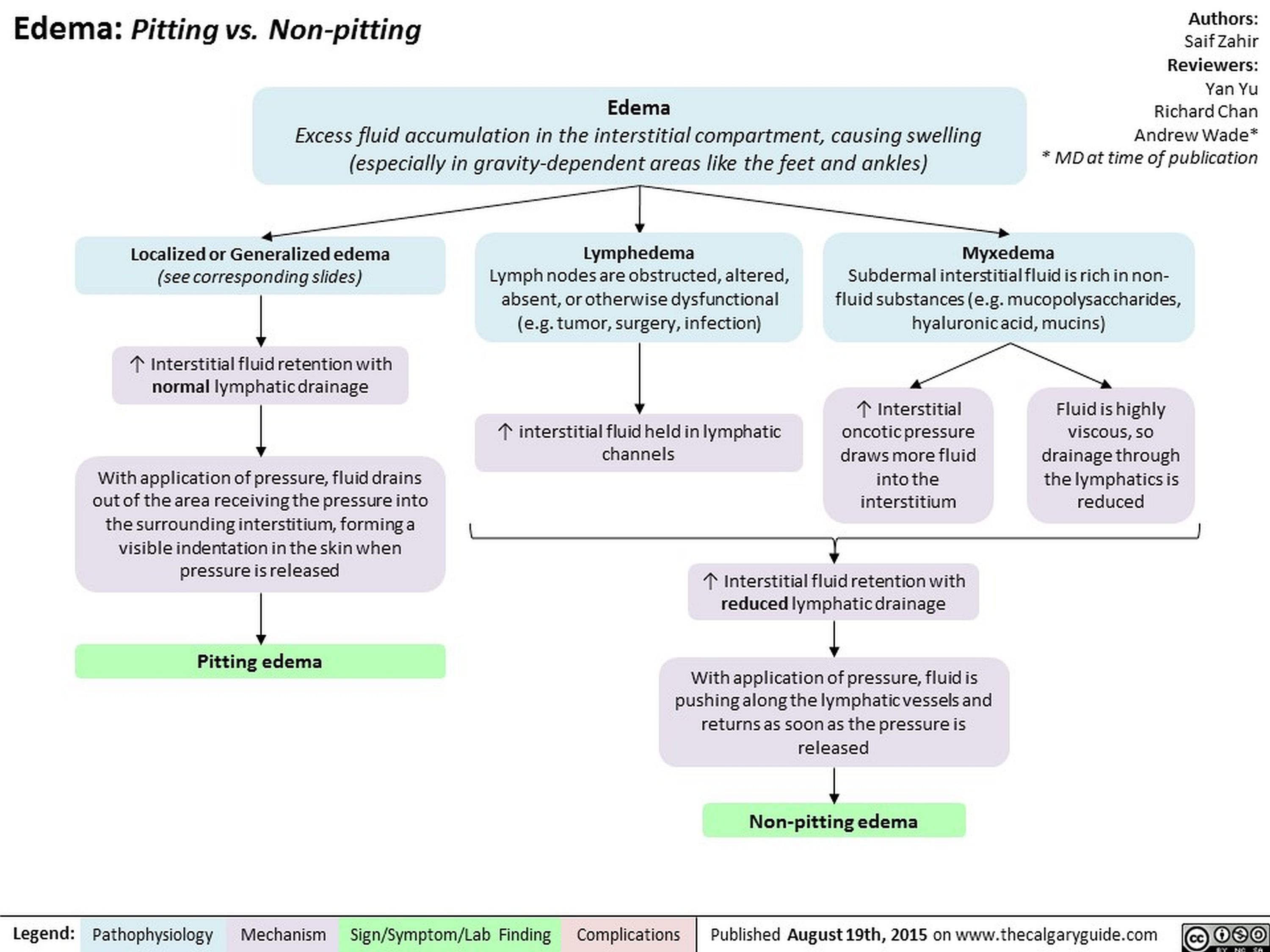
Edema Pitting vs Non-pitting
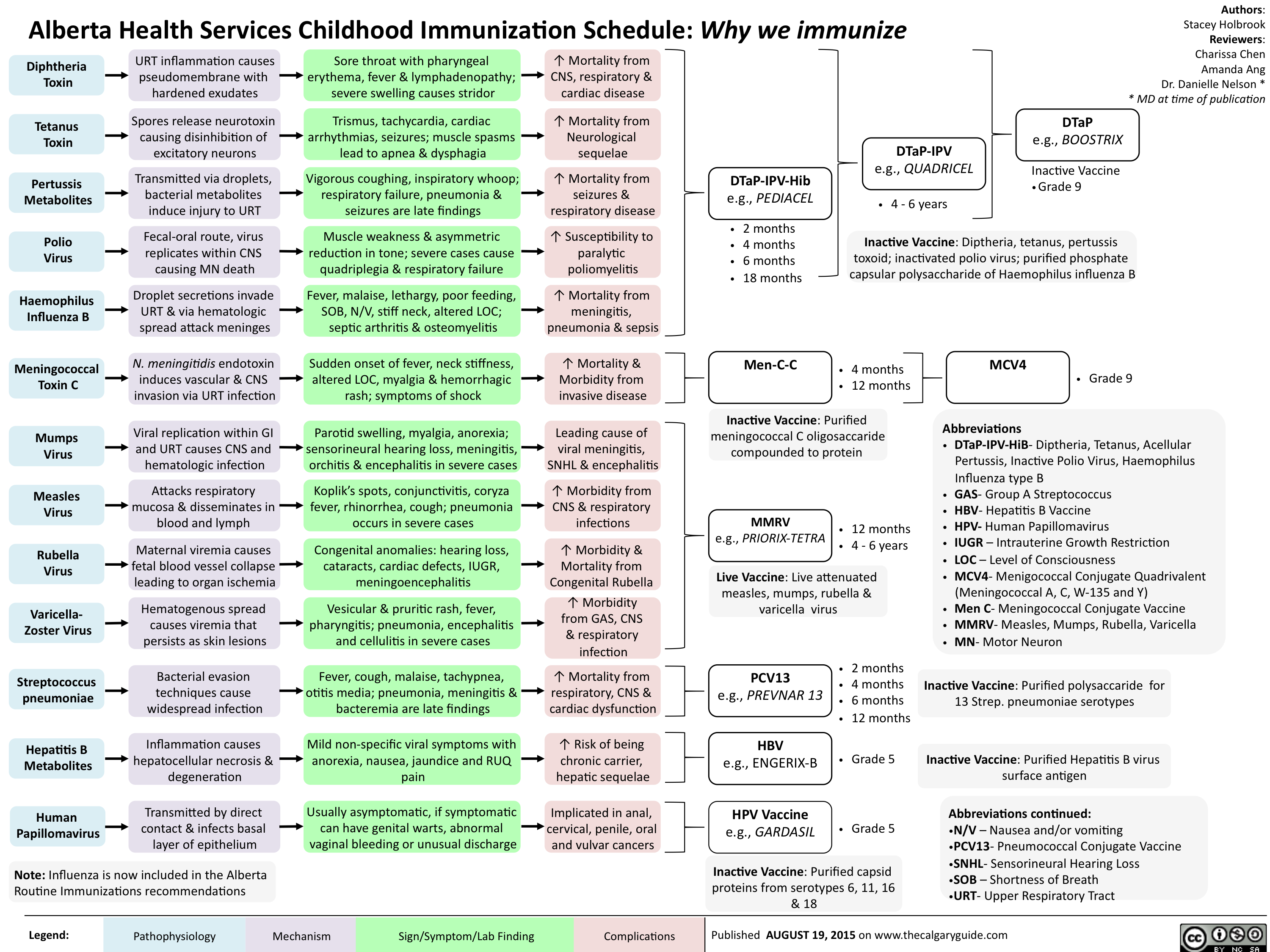
Childhood Immunization Schedule-Why we immunize
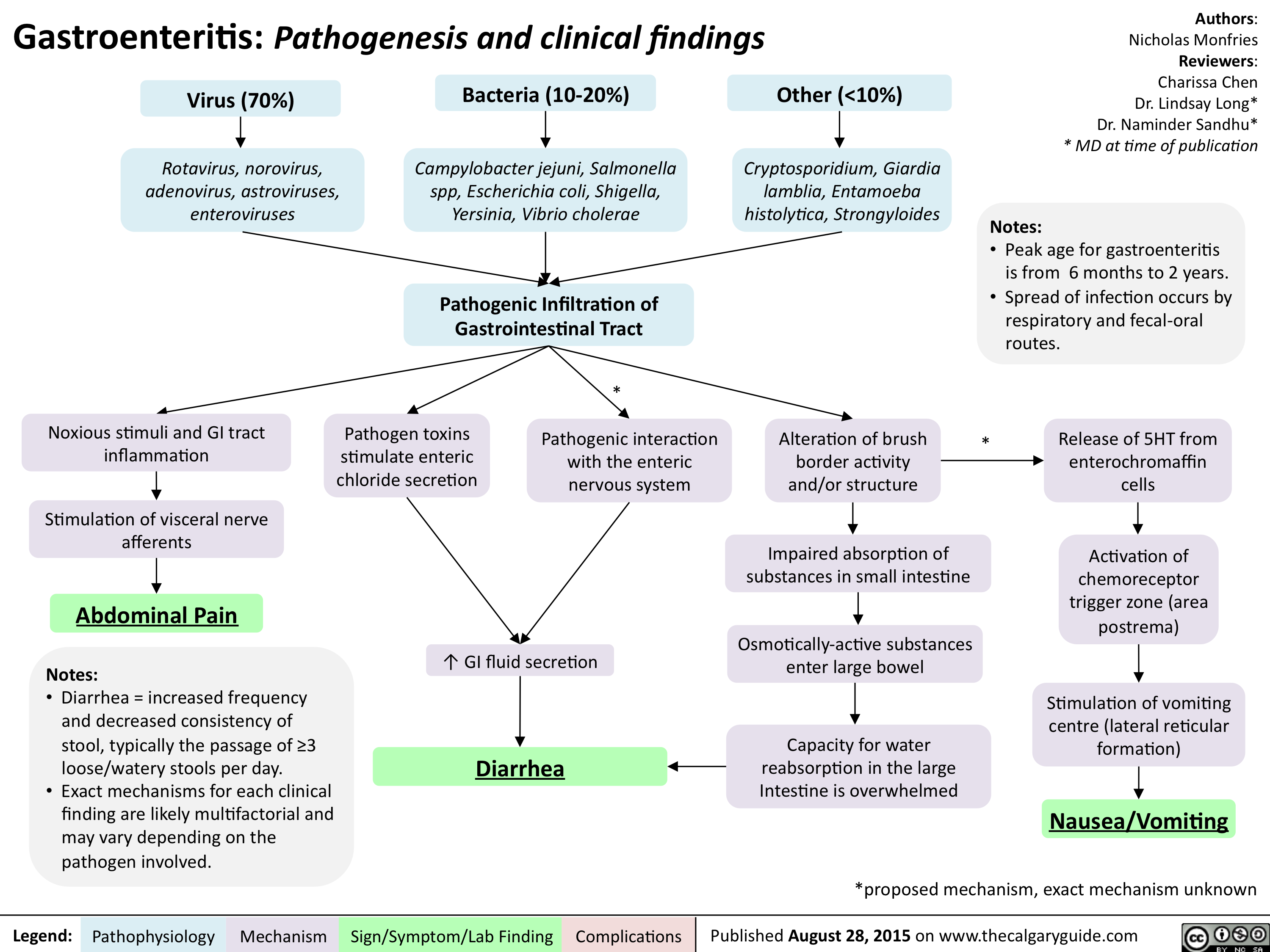
Gastroenteritis-Pathogenesis and clinical findings
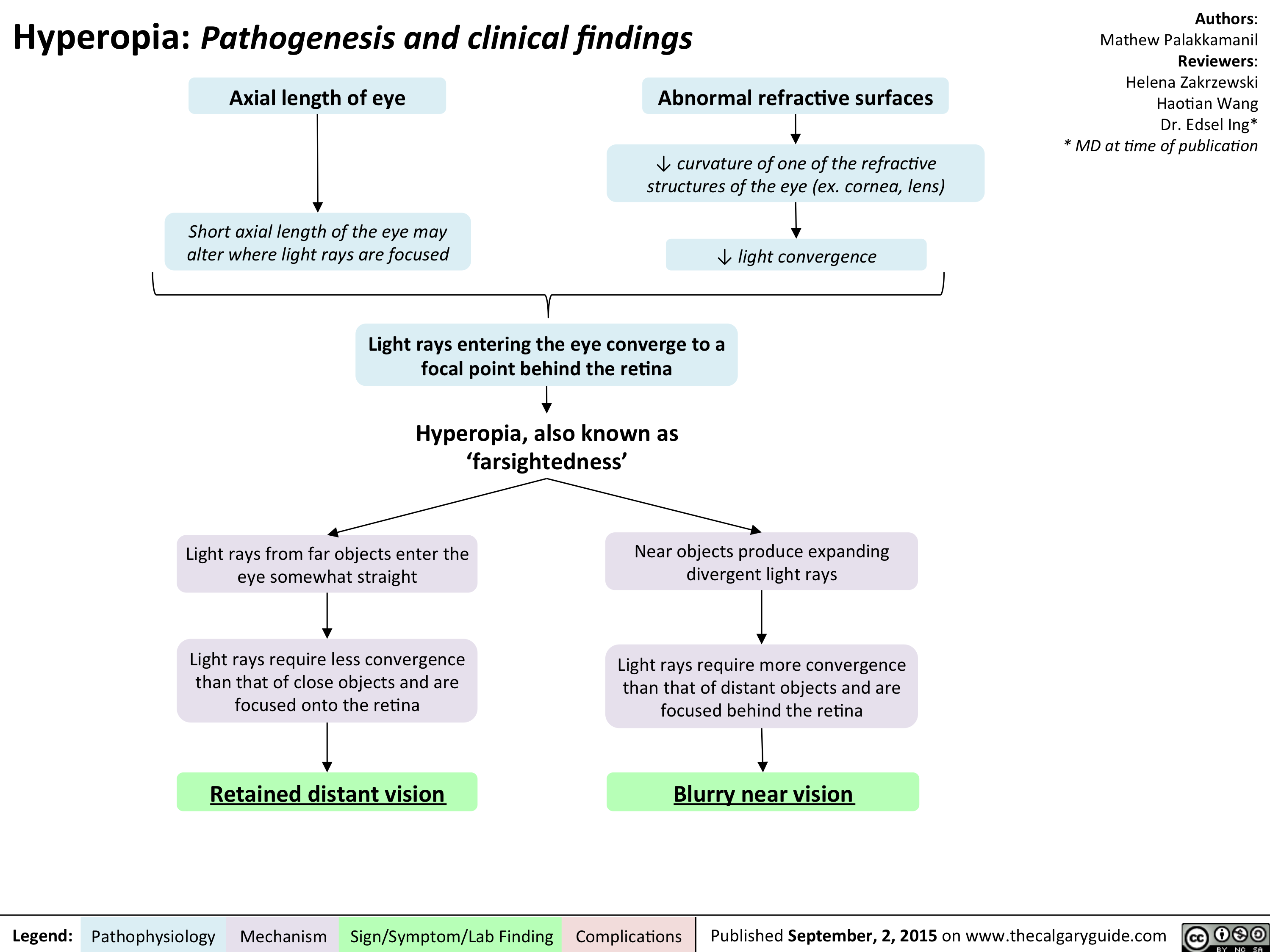
Hyperopia - Pathogenesis and Clinical Findings
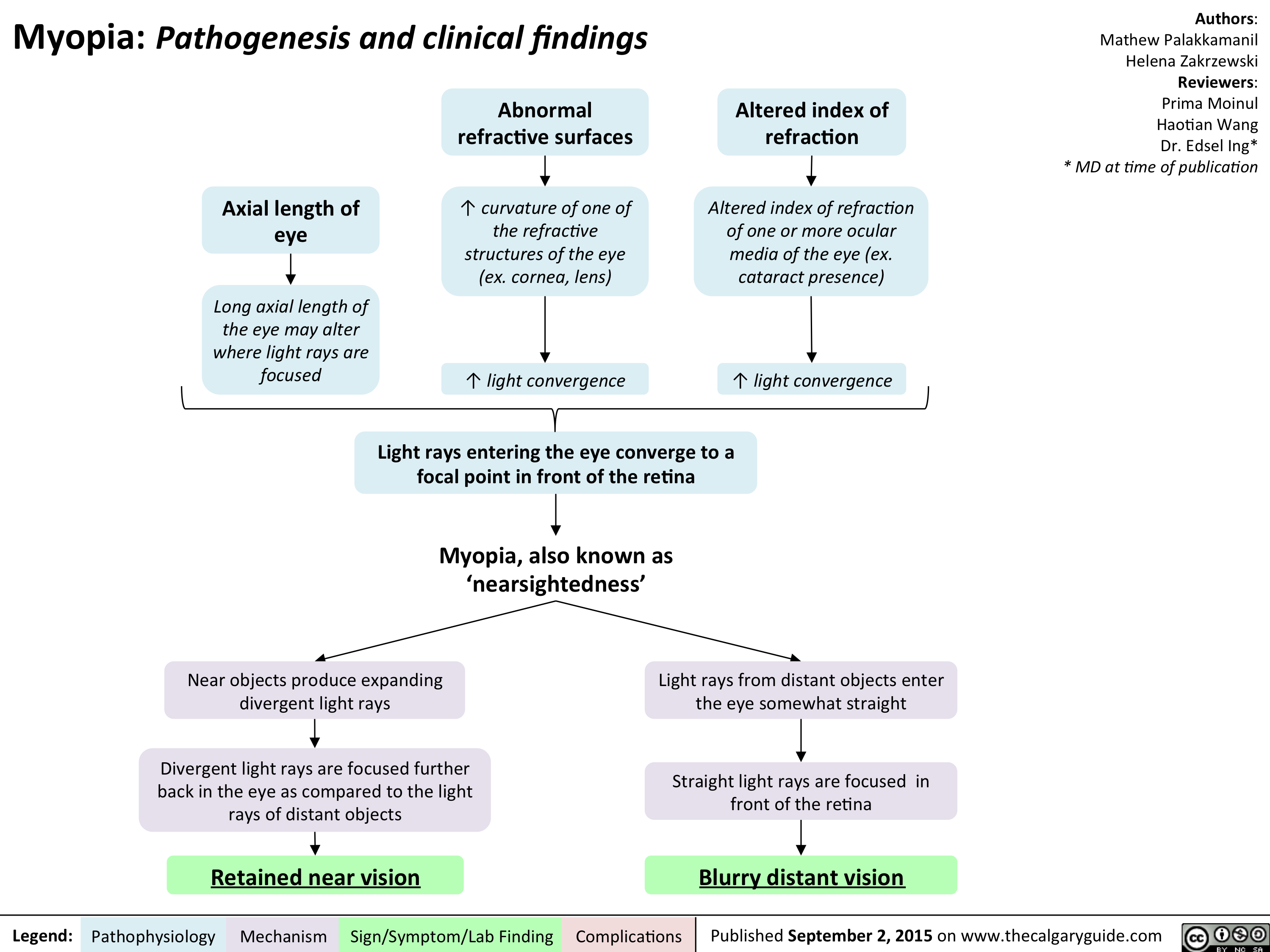
Myopia - Pathogenesis and clinical findings
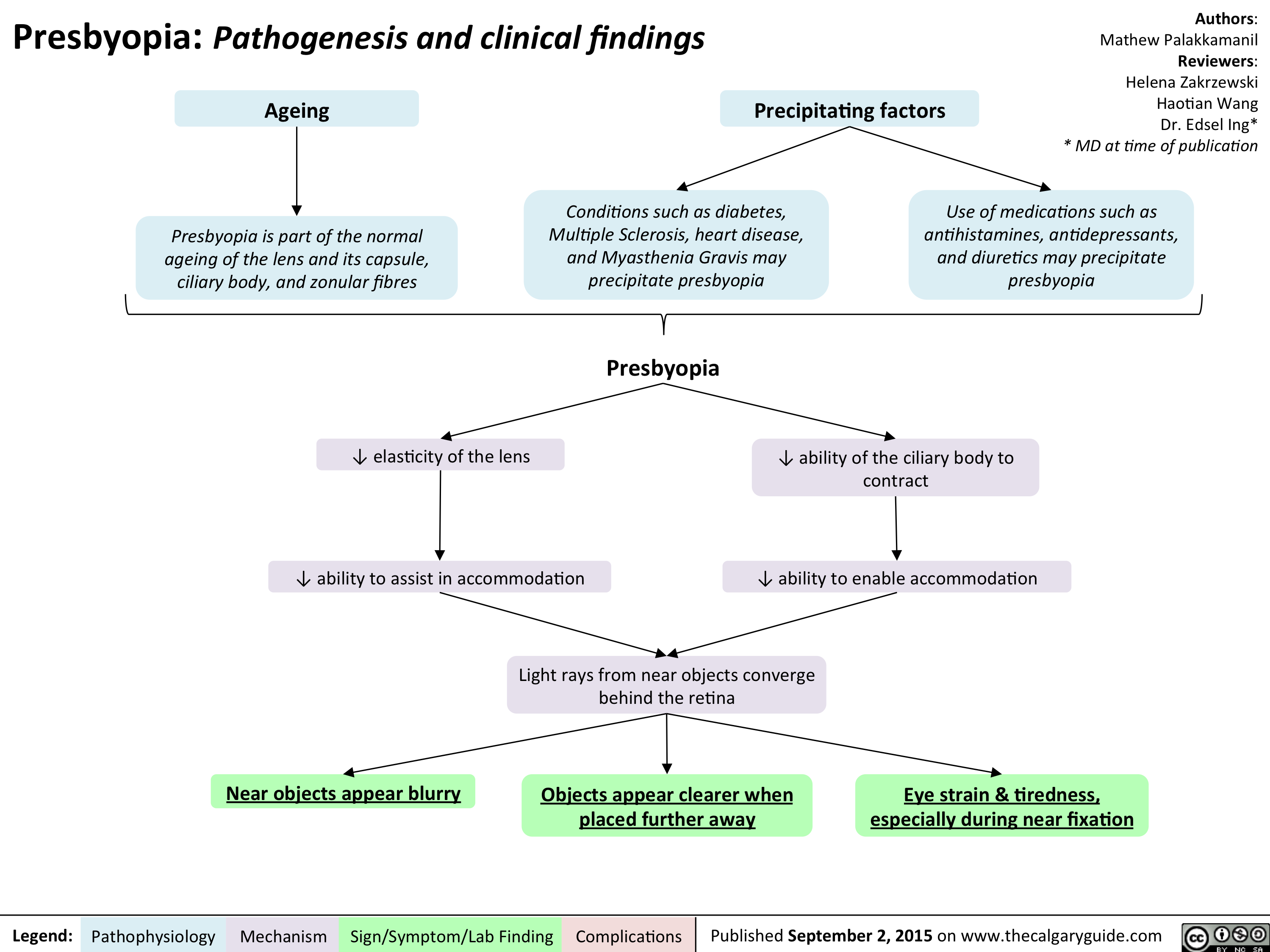
Presbyopia - Pathogenesis and clinical findings
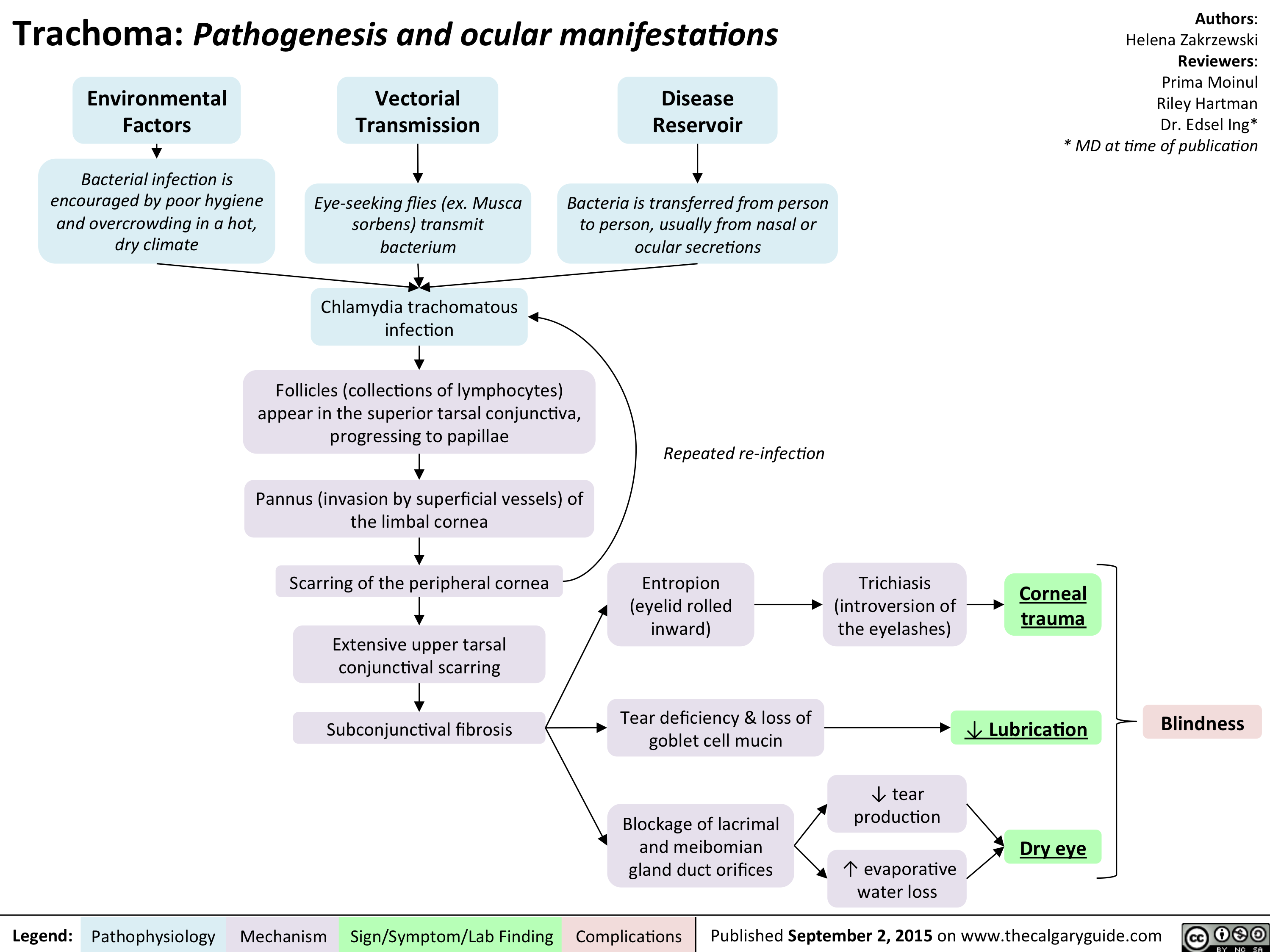
Trachoma - Pathogenesis and clinical findings
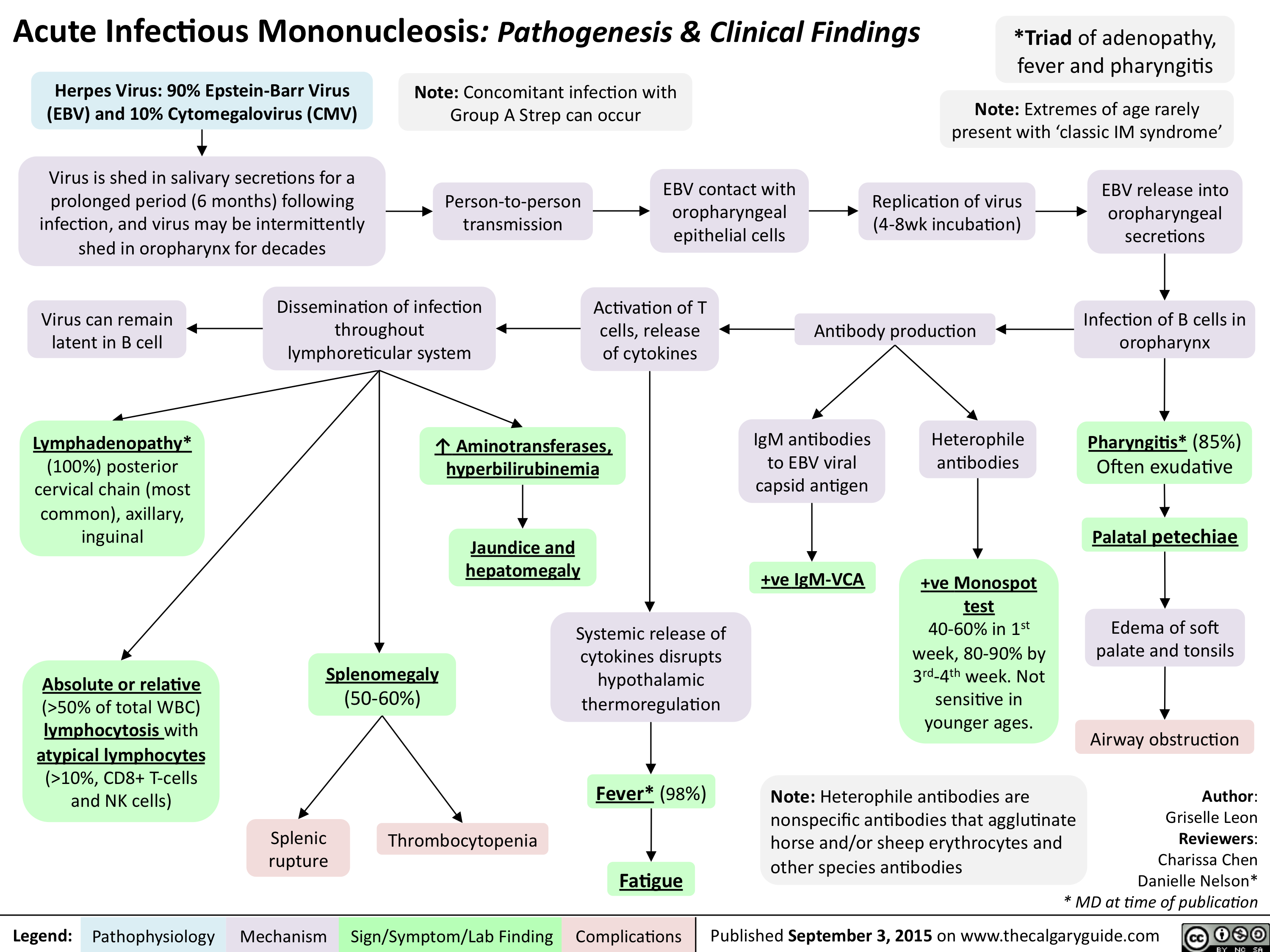
Acute Infectious Mononucleosis-Pathogenesis and clinical findings
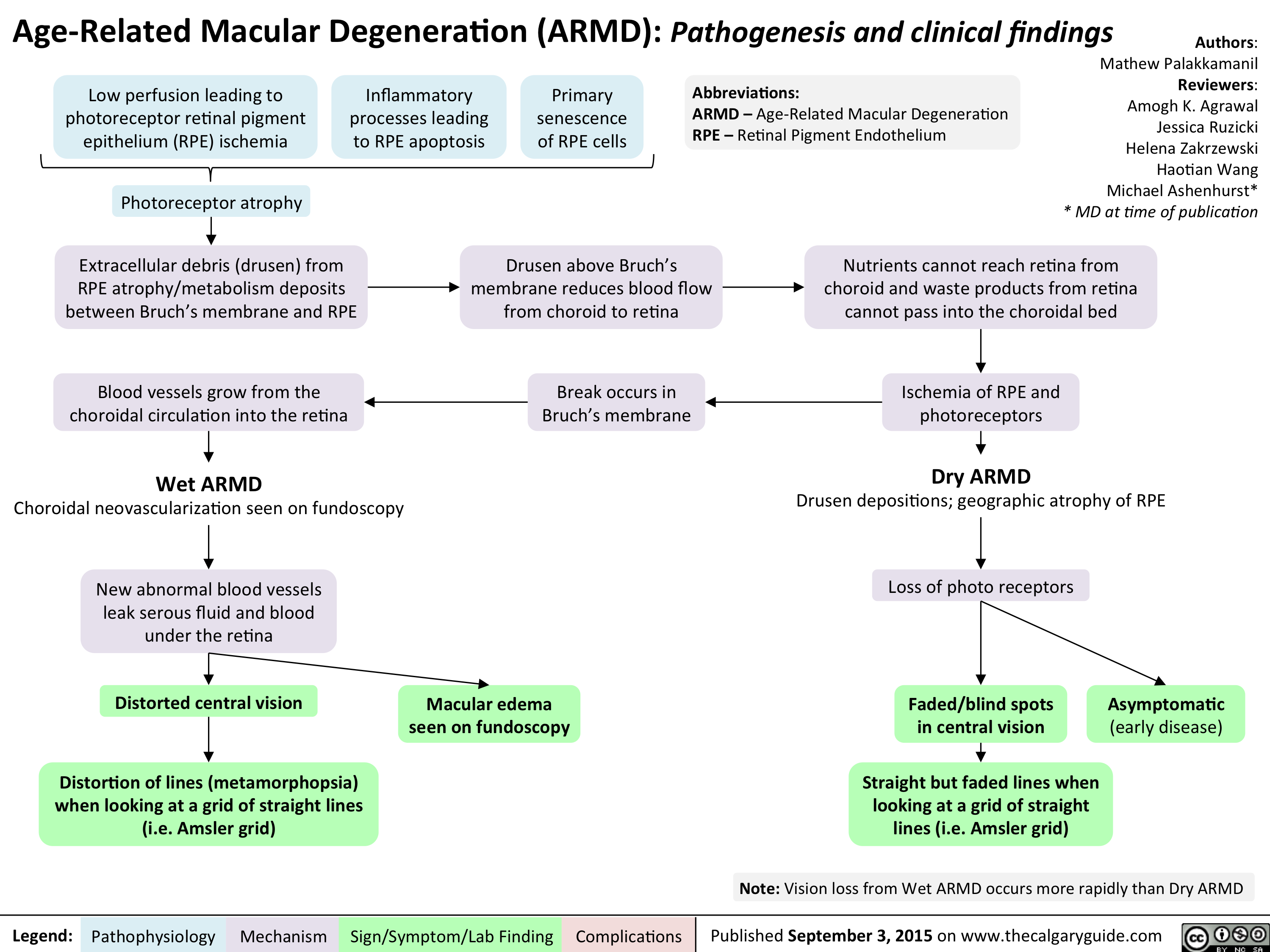
Age Related Macular Degeneration - Pathogenesis and clinical findings
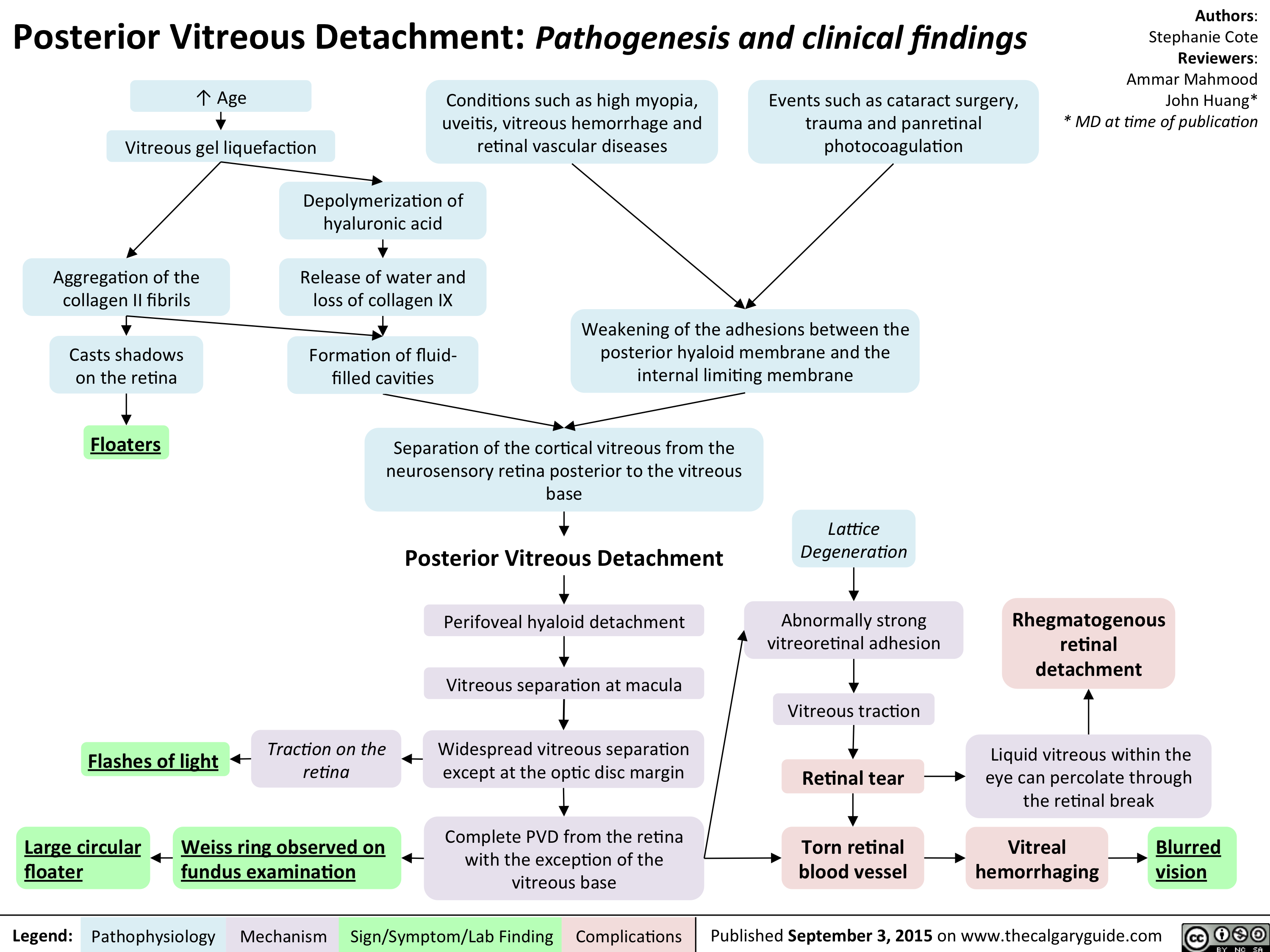
Posterior Vitreous Detachment - Pathogenesis and clinical findings
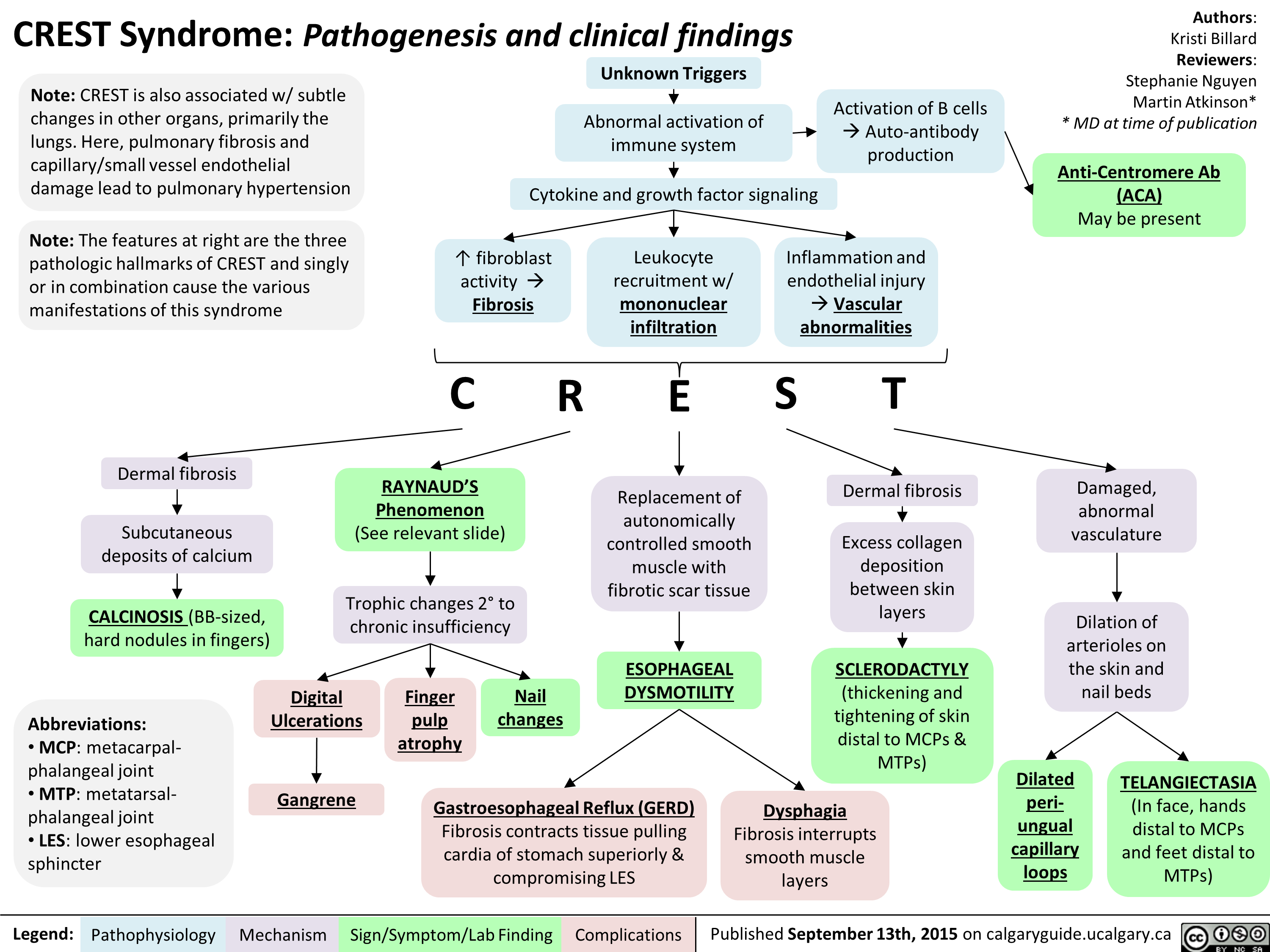
FINAL - CREST Syndrome Pathogenesis and clinical findings
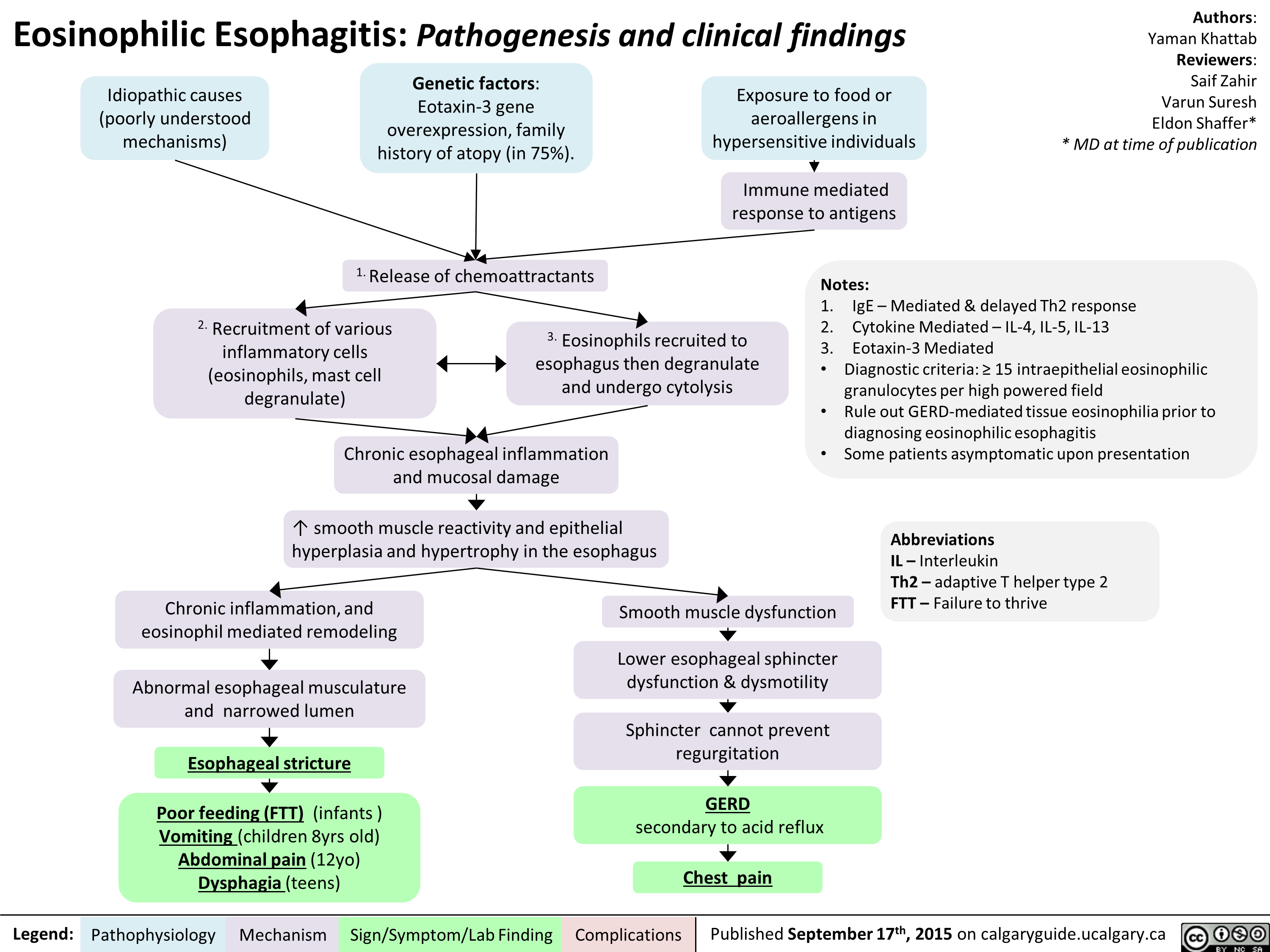
Eosinophillic Esophagitis -Kattab Yaman - Final For Publication
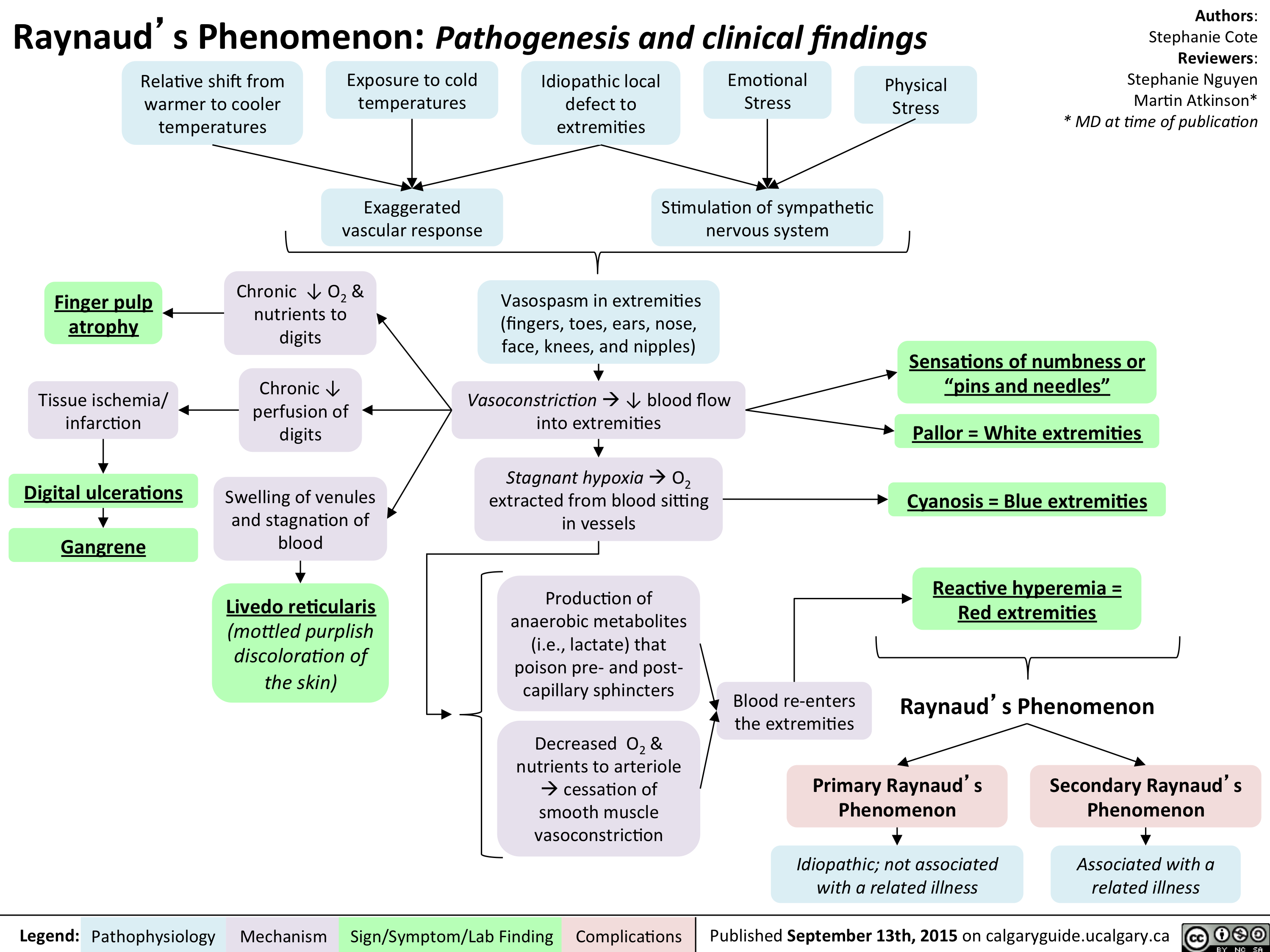
Raynaud Phenomenon Pathogenesis and Clinical Findings
Chan Richard - Underfill Edema - Final 210915
Pre-Renal Acute Kidney Injury Pathogenesis

High-AG Metabolic Acidosis Pathogenesis
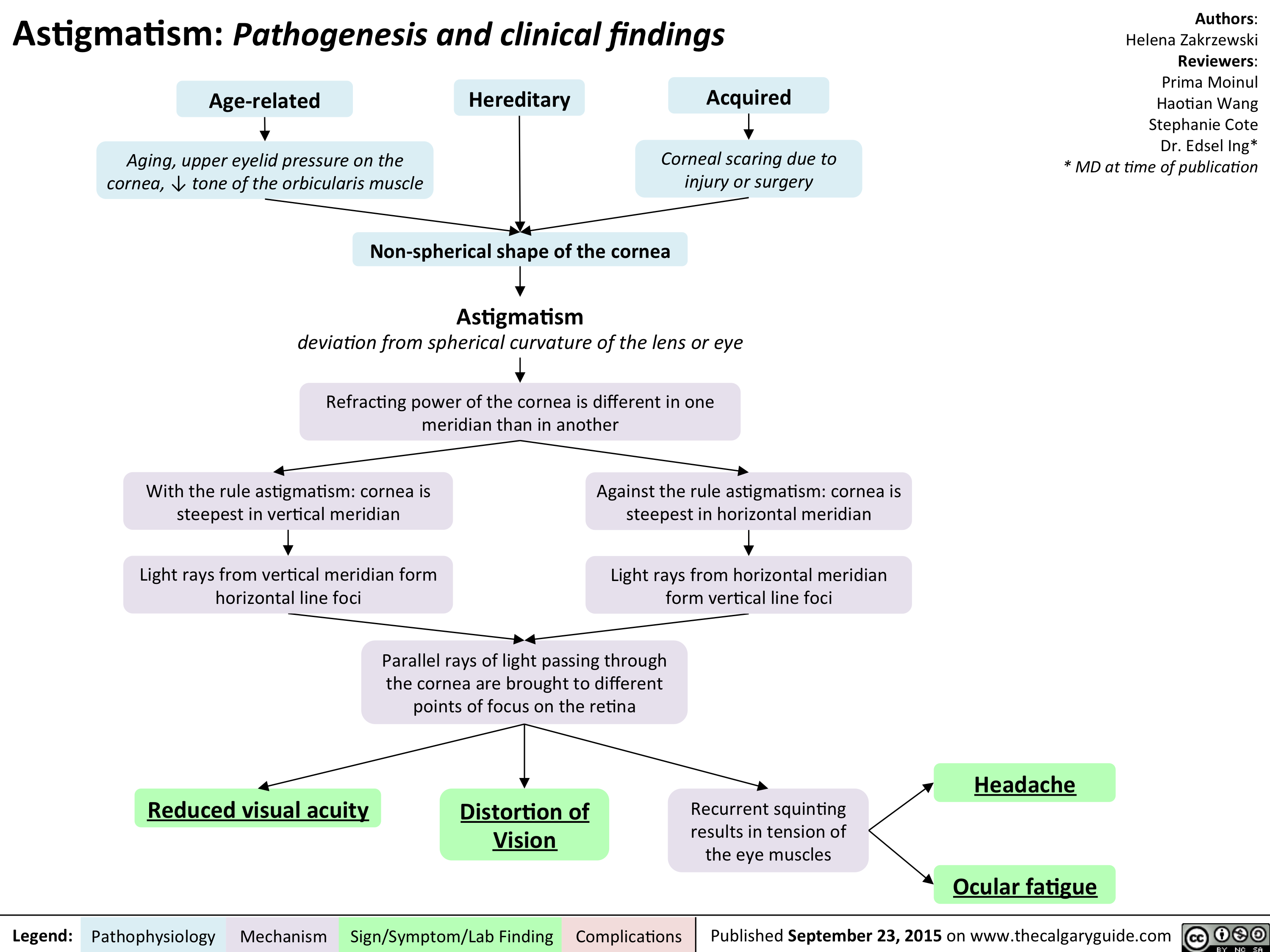
Astigmatism Pathogenesis and Clinical Findings
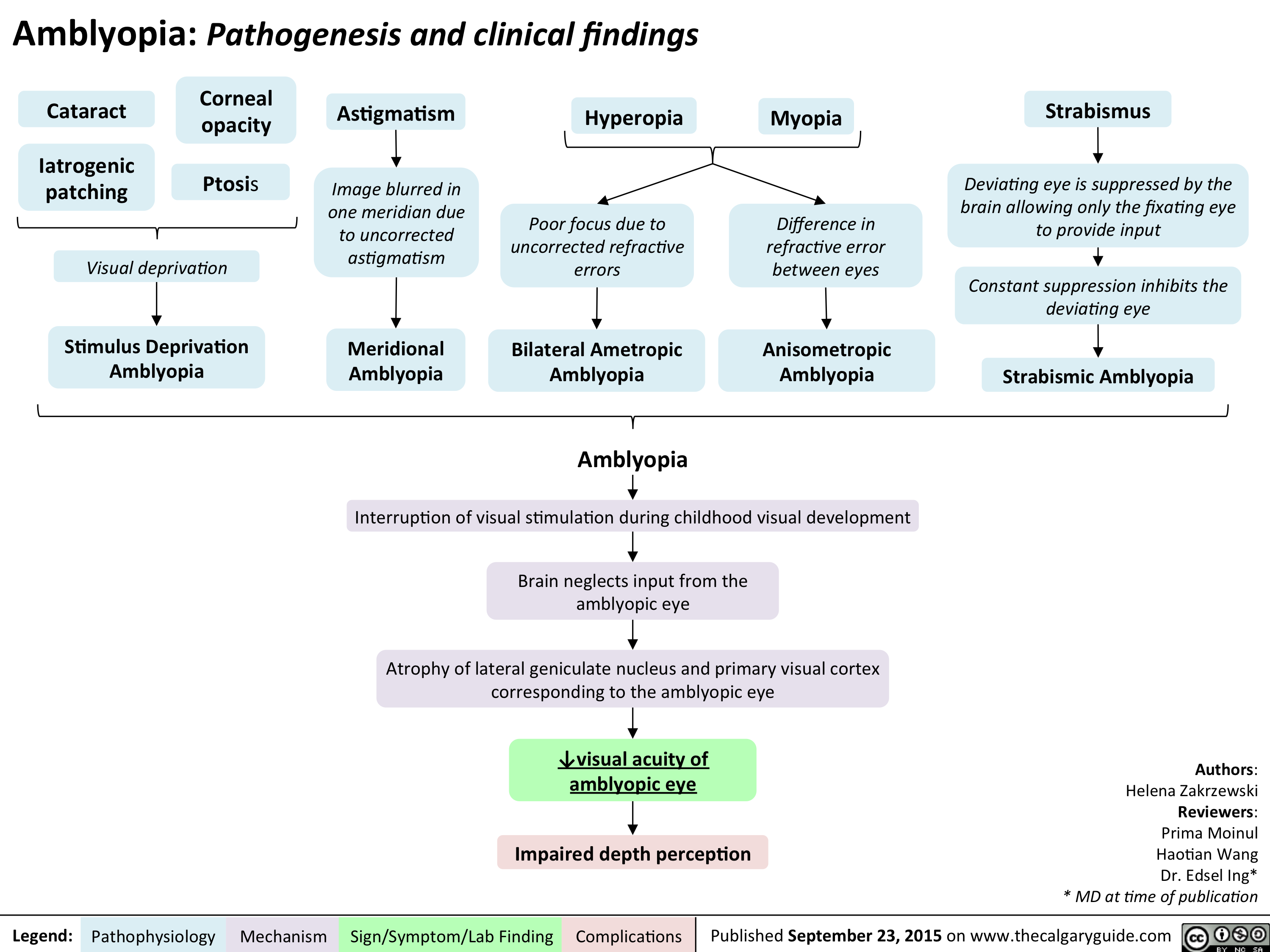
Amblyopia Pathogenesis and clinical findings
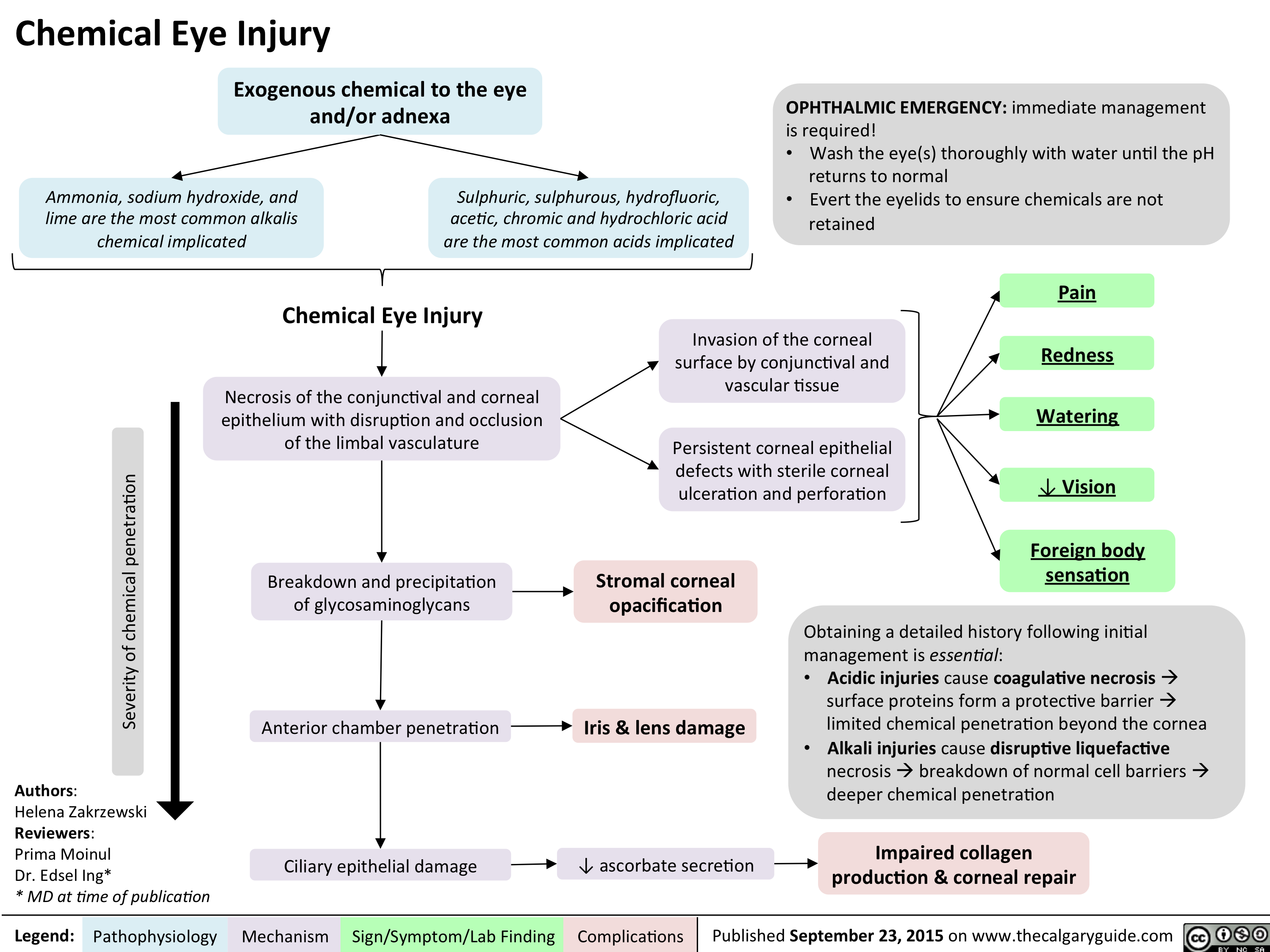
Chemical Eye Injury Pathogenesis and clinical findings
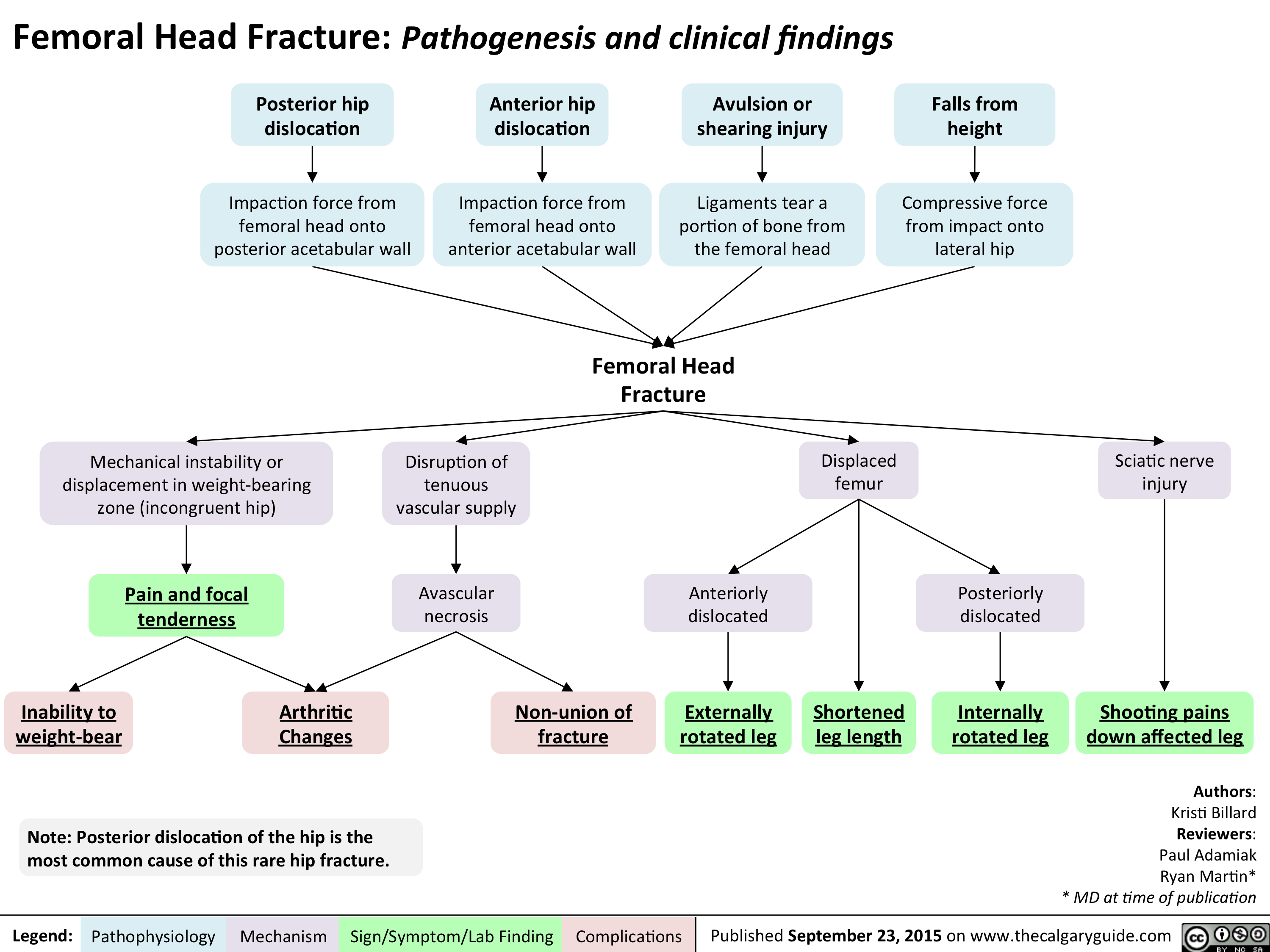
Femoral Head Fracture Pathogenesis and clinical findings
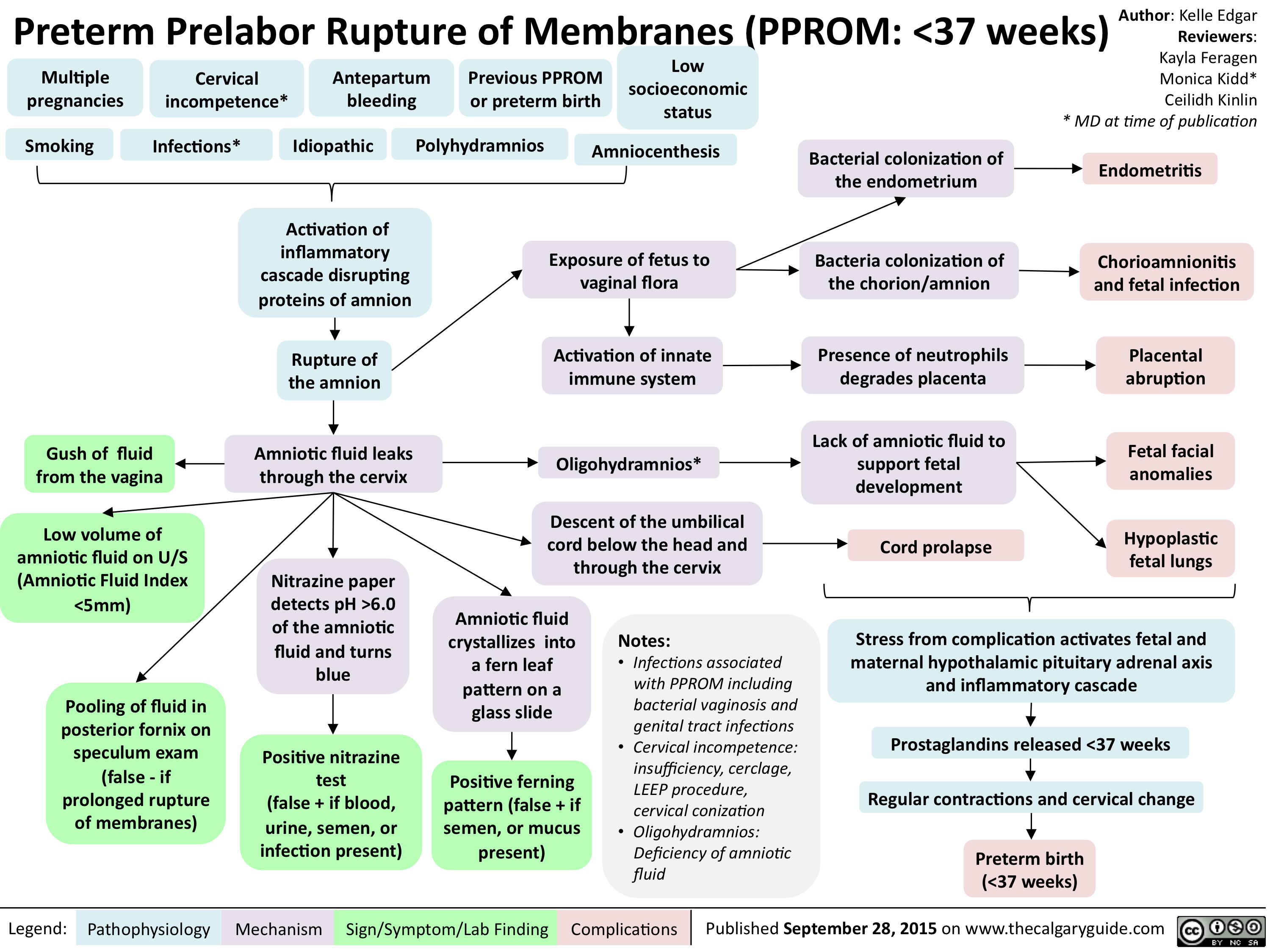
PPROM - Pathogenesis and clinical findings
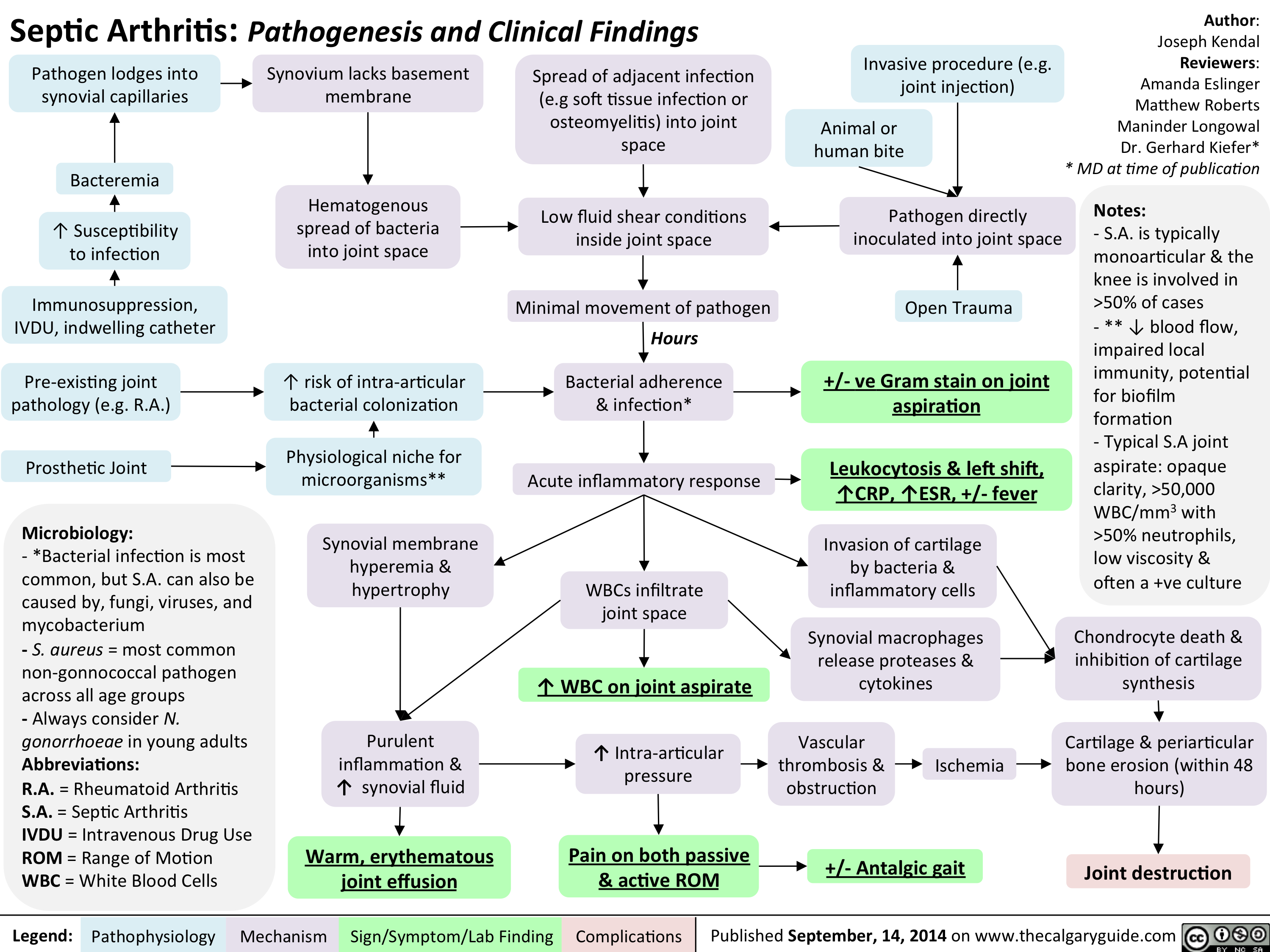
Septic arthitis pathogenesis and clinical findings
Family Med Slides Vitamin D Deficiency

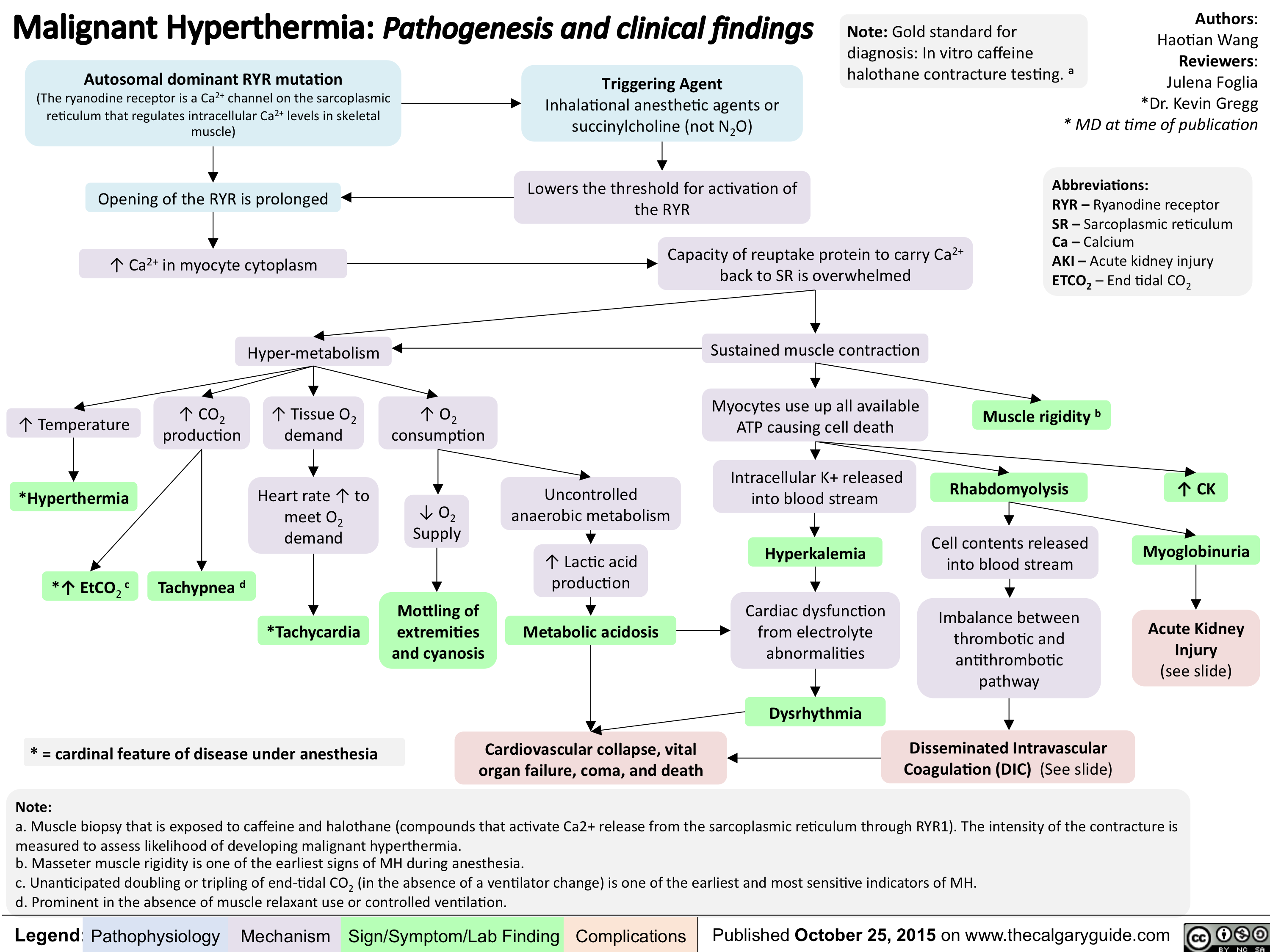
Malignant Hyperthermia-Pathogenesis and clinical findings
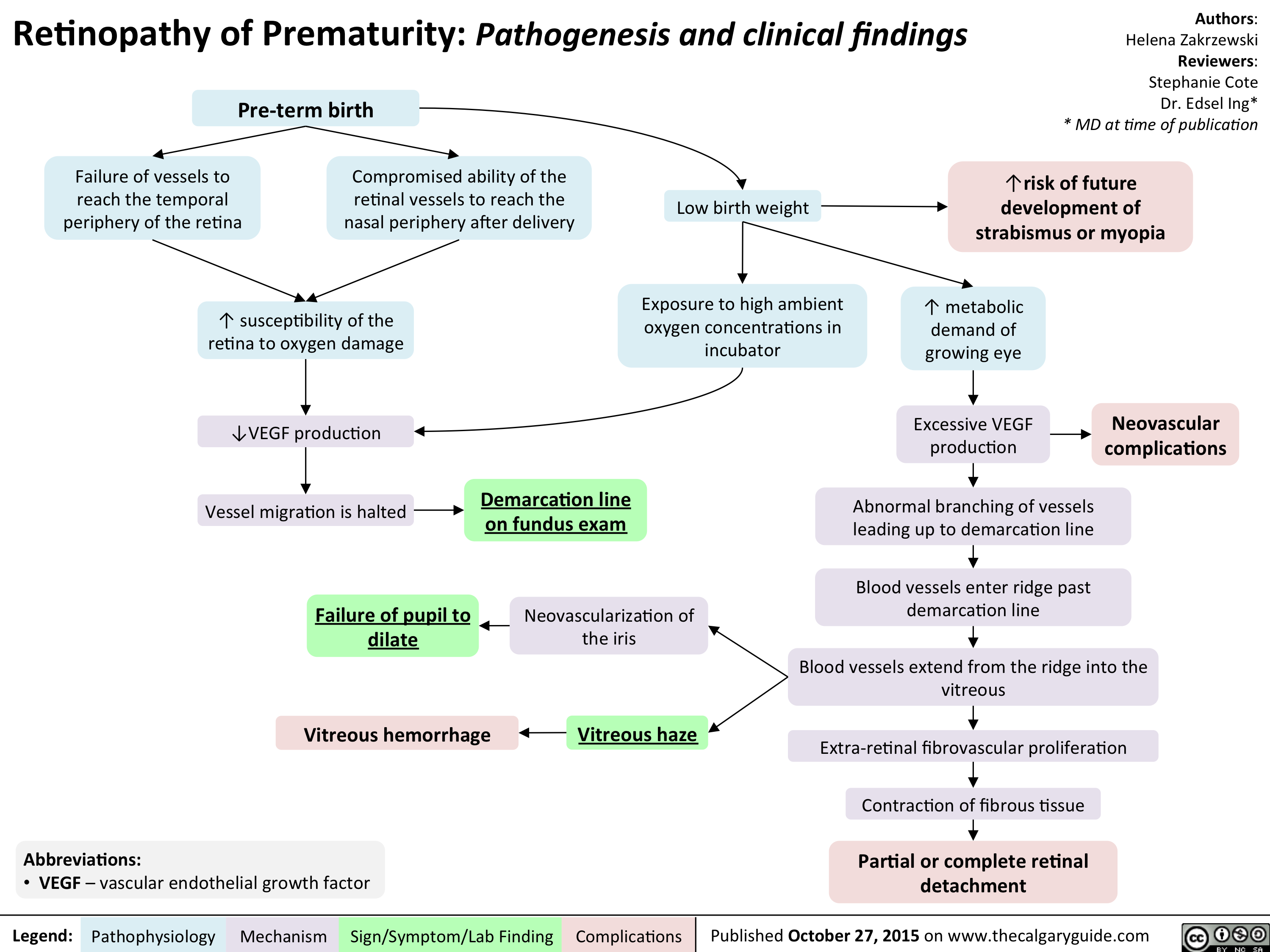
Retinopathy of Prematurity - Pathogenesis and clinical findings
Orthostatic Hypotension-Pathogenesis and clinical findings

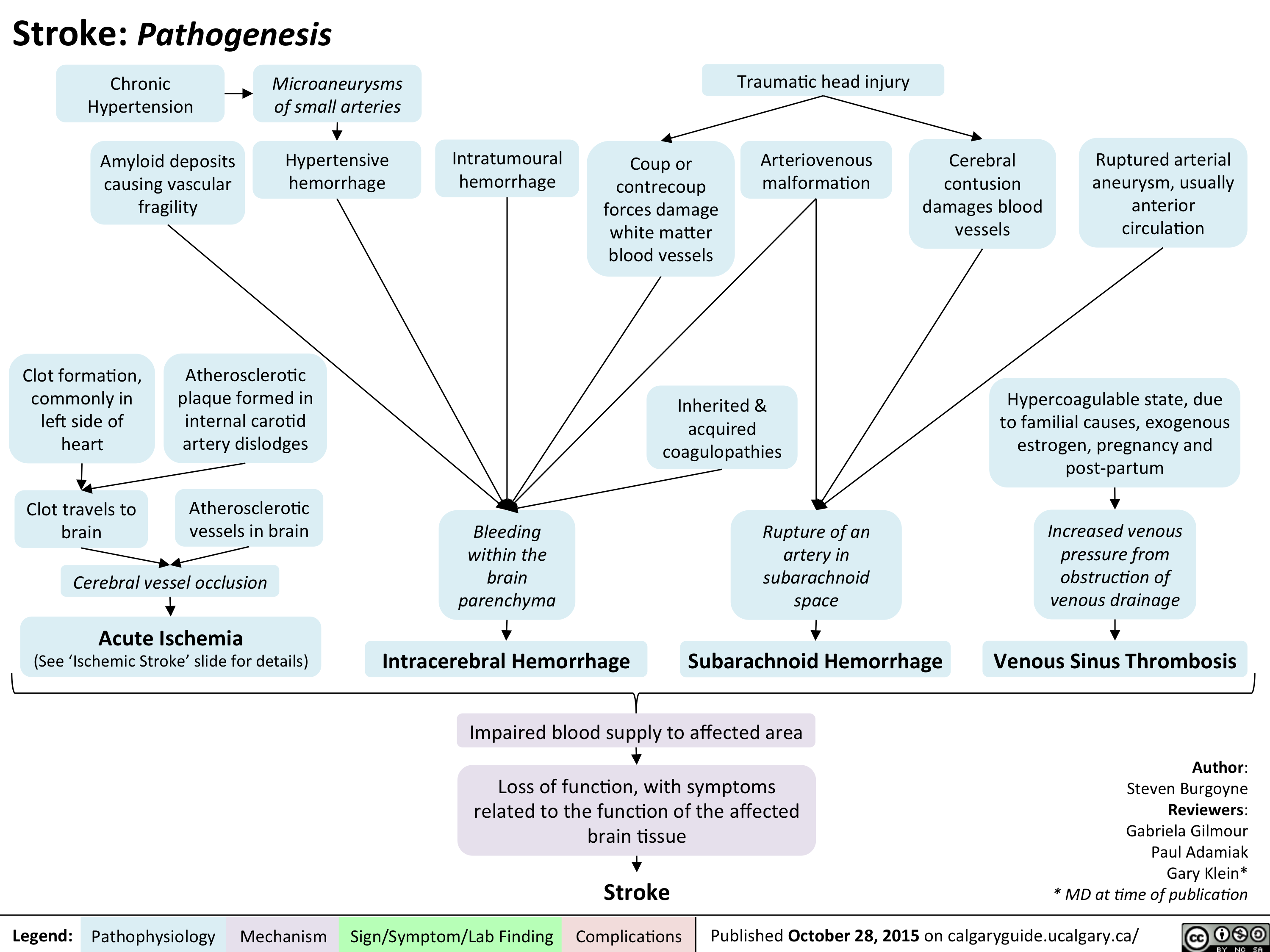
Stroke - Pathogenesis
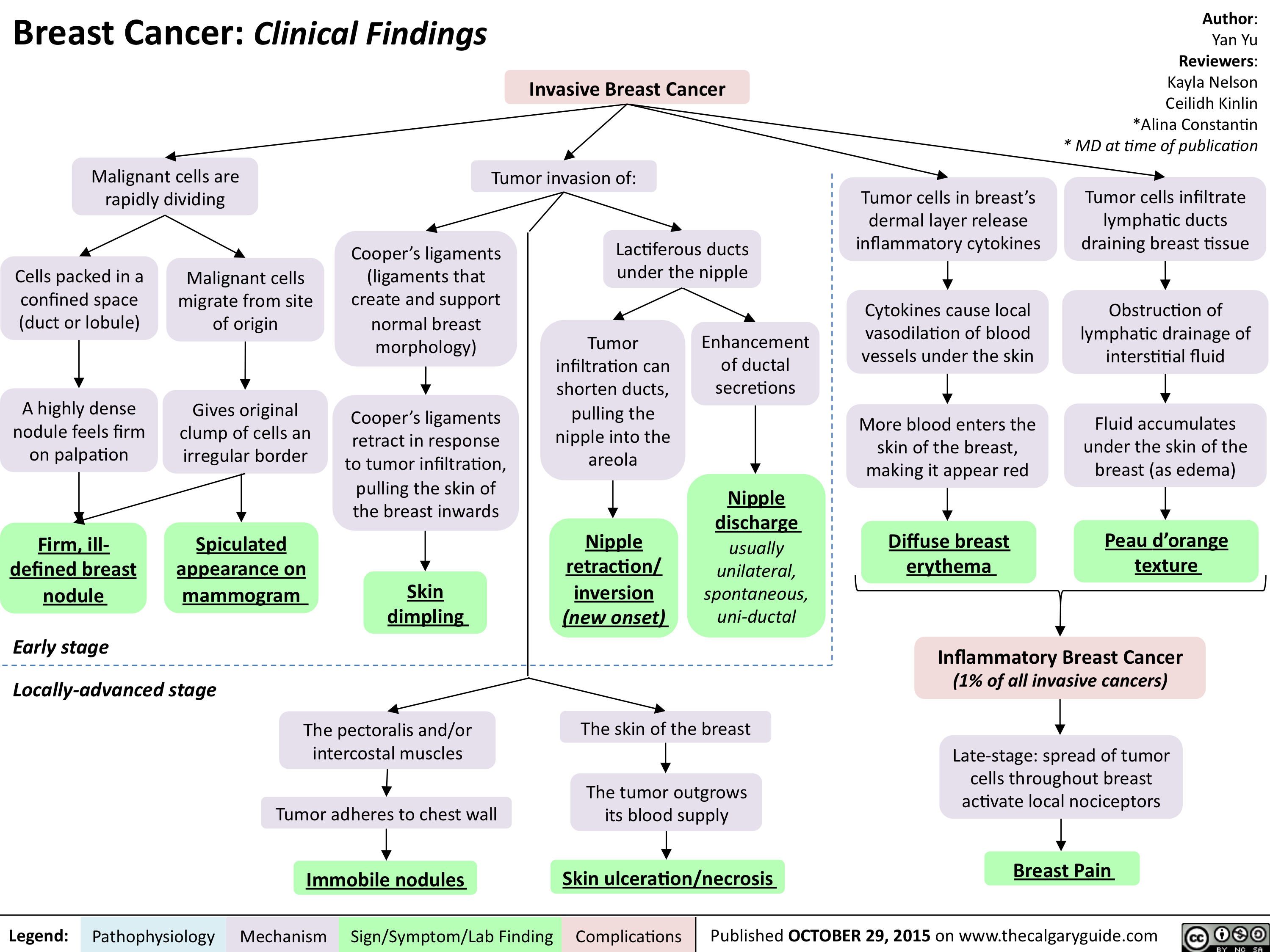
Breast Cancer - Clinical findings
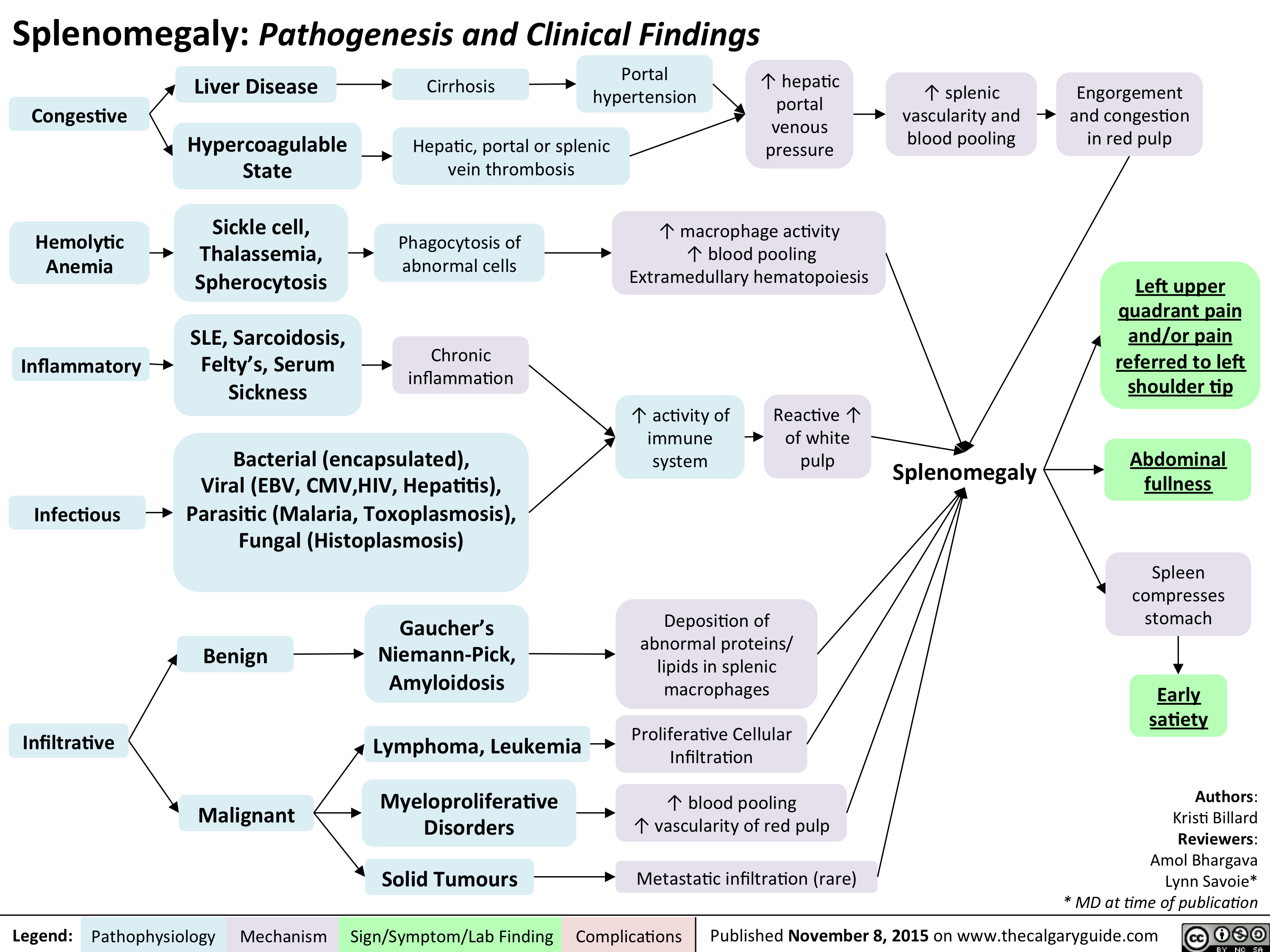
Splenomegaly - Pathogenesis and clinical findings
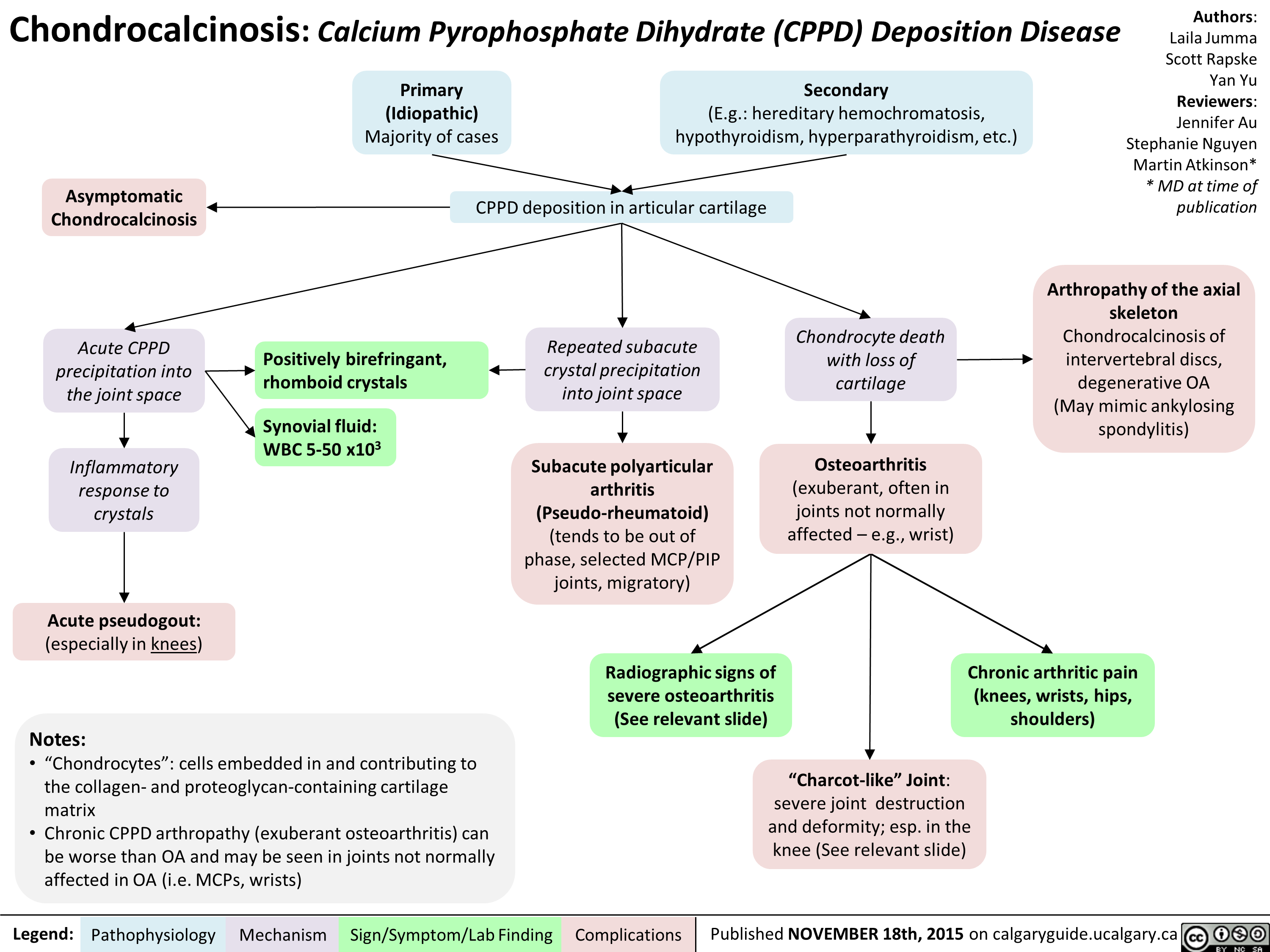
Chondrocalcinosis Calcium Pyrophosphate Dihydrate Deposition Disease
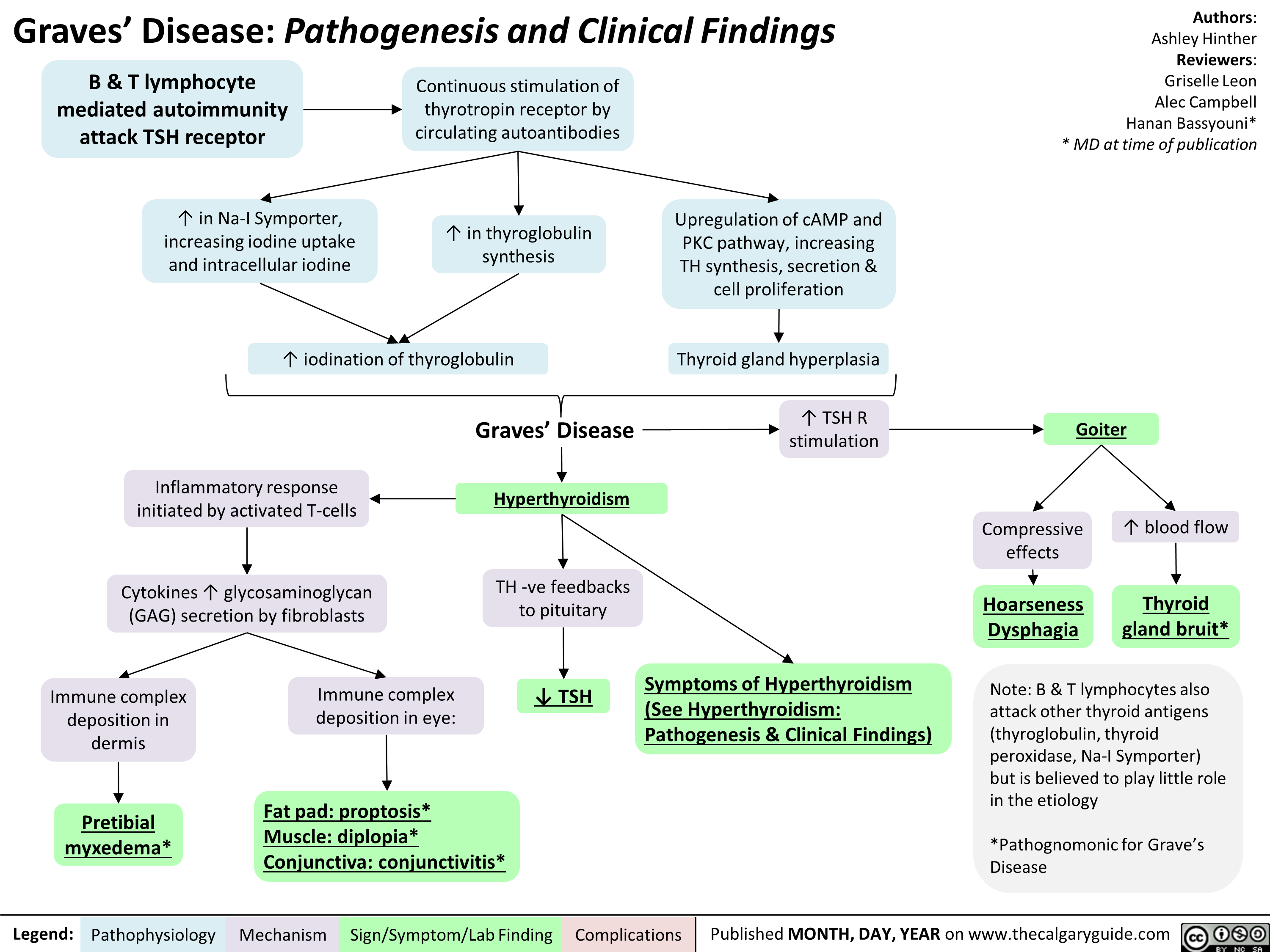
Graves' Disease Pathogenesis & Clinical Findings
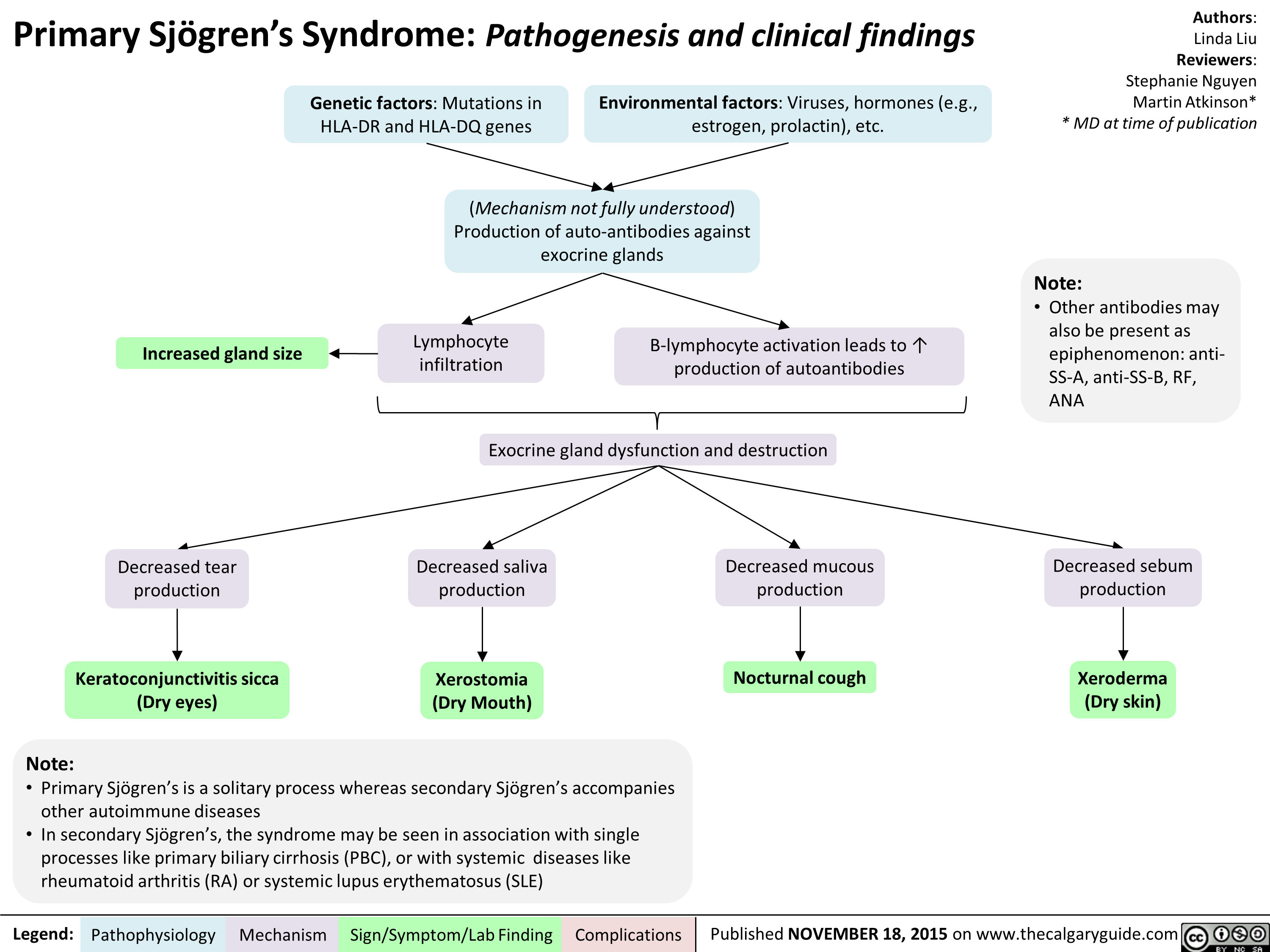
sjogrensyndrome
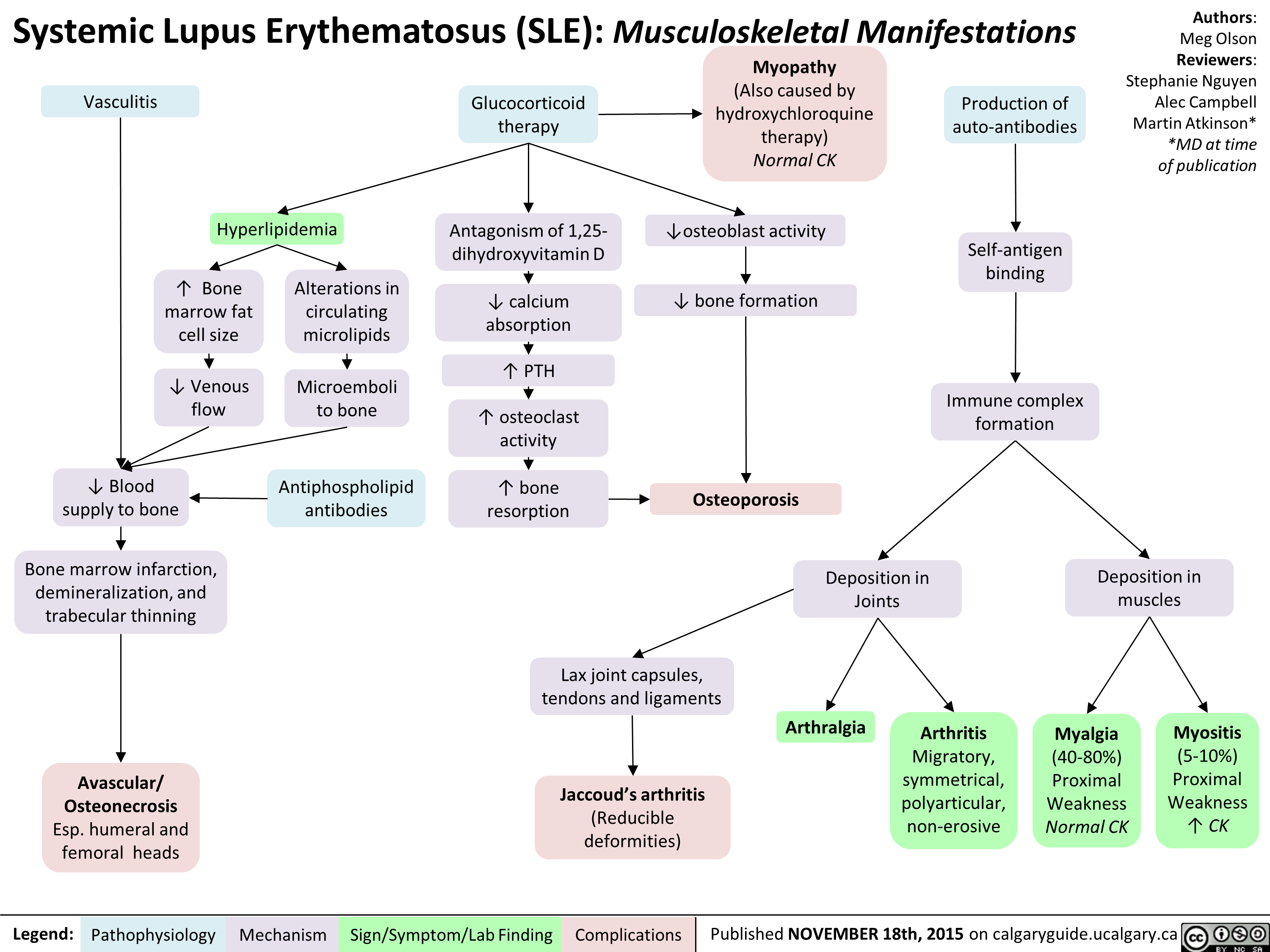
Systemic Lupus Erythematosis SLE Musculoskeletal Manifestations
Hashimoto's Thyroiditis Natural History and Clinical Findings
Hashimoto's Thyroiditis Pathogenesis and Clinical Findings
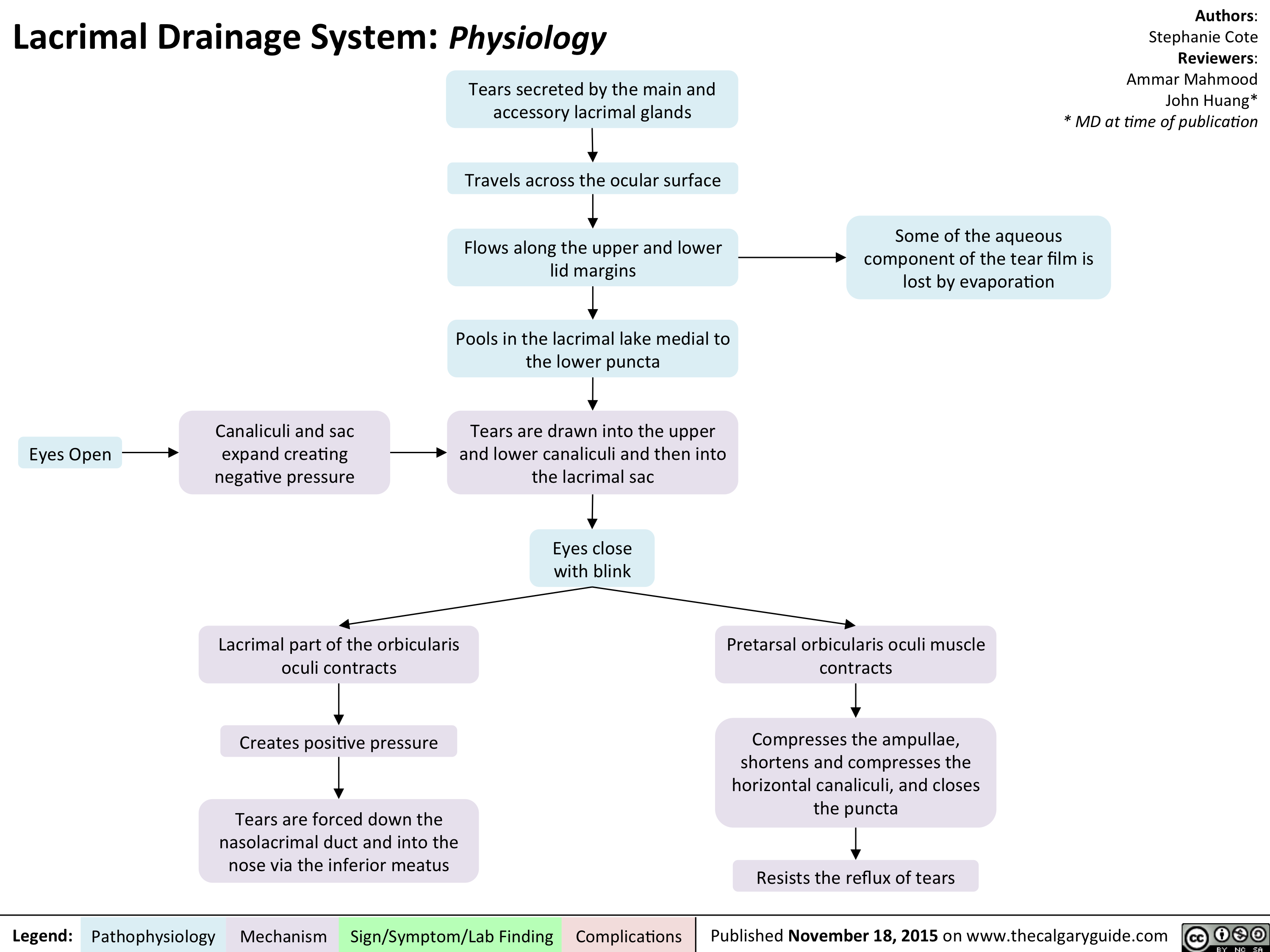
Lacrimal Drainage System - Physiology
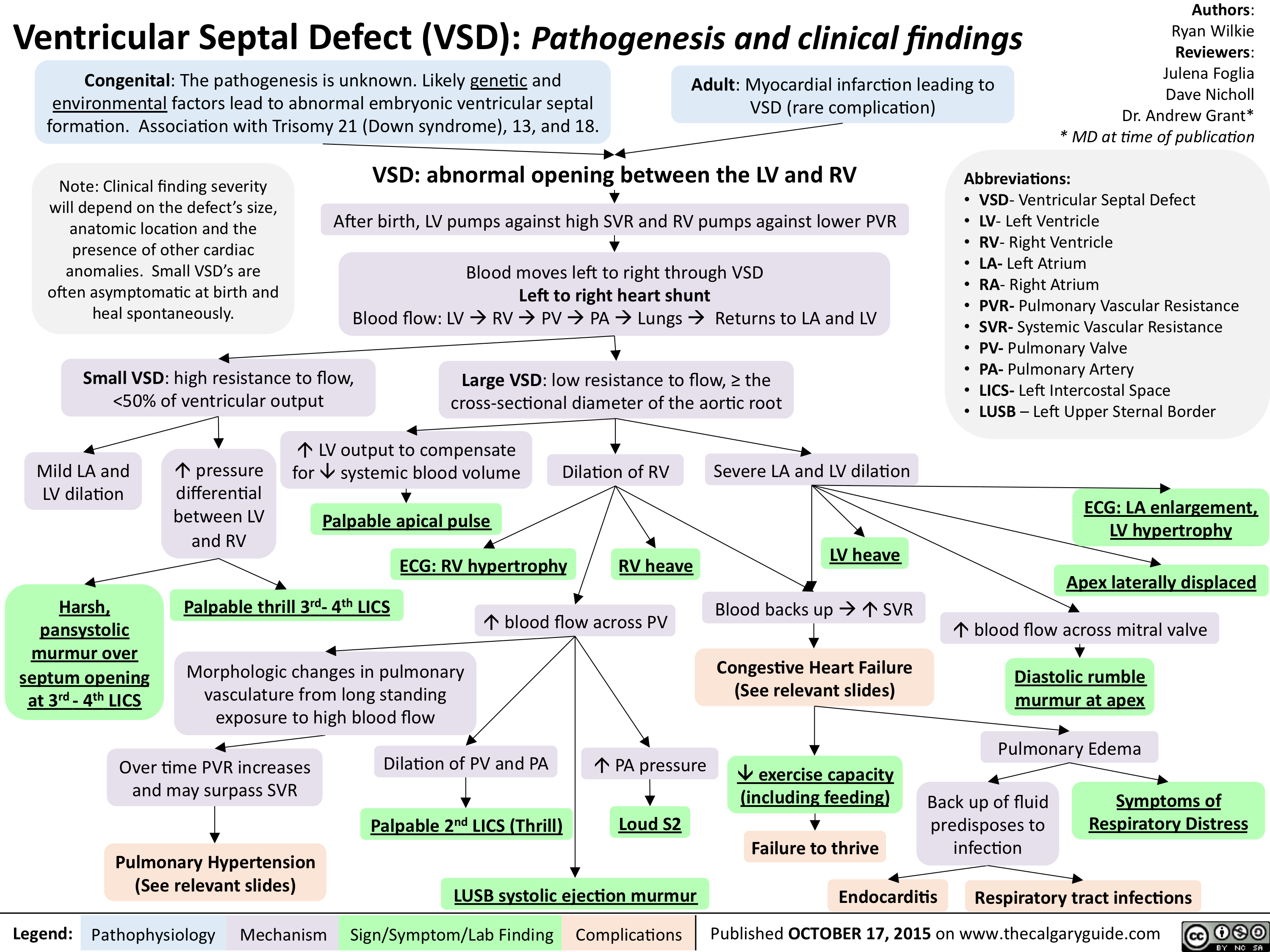
Ventricular Septal Defect (VSD)-Pathogenesis and clinical findings
Transfusion-associated Graft Versus Host Disease - Signs and Symptoms
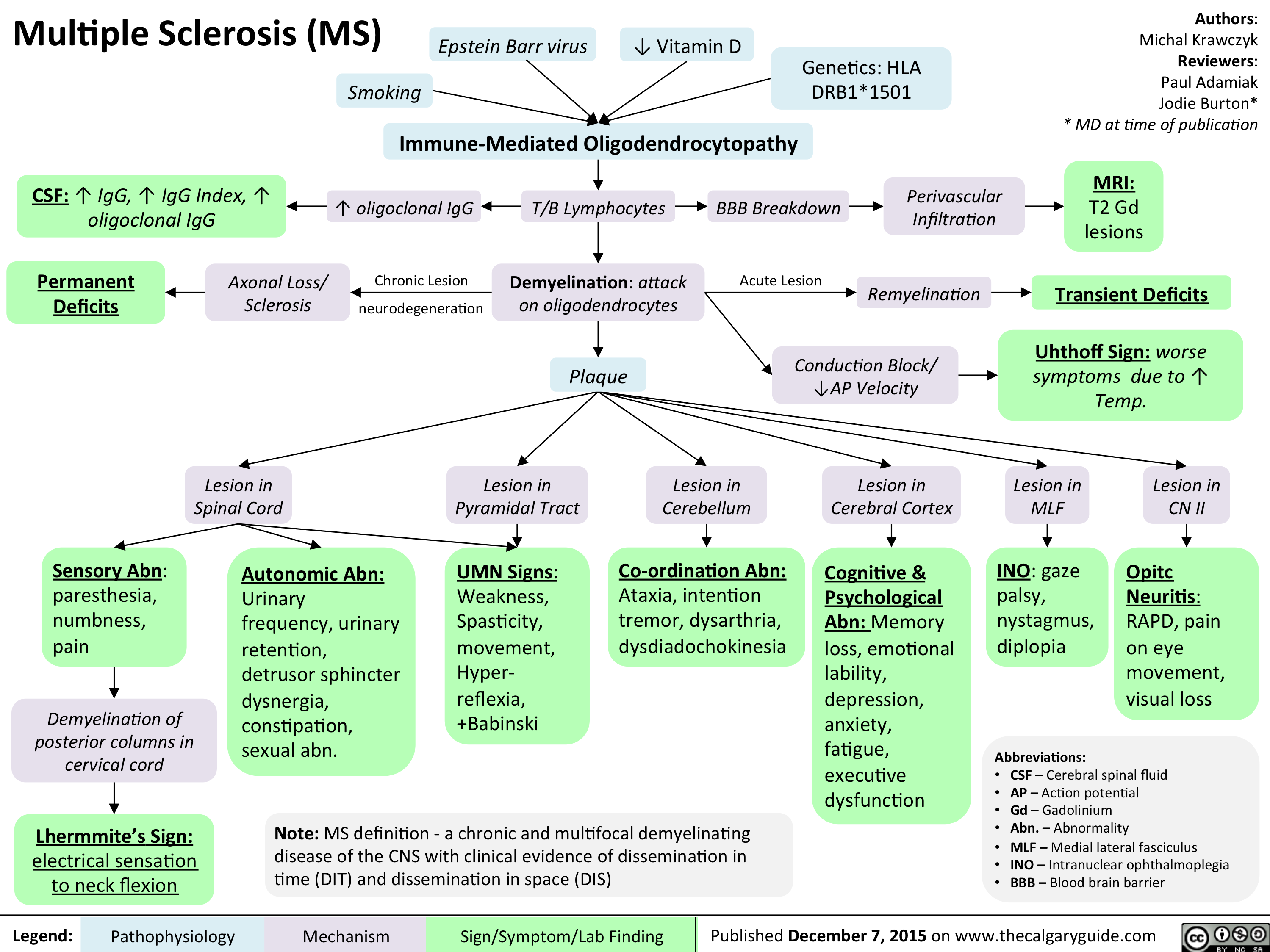
Multiple sclerosis (MS)
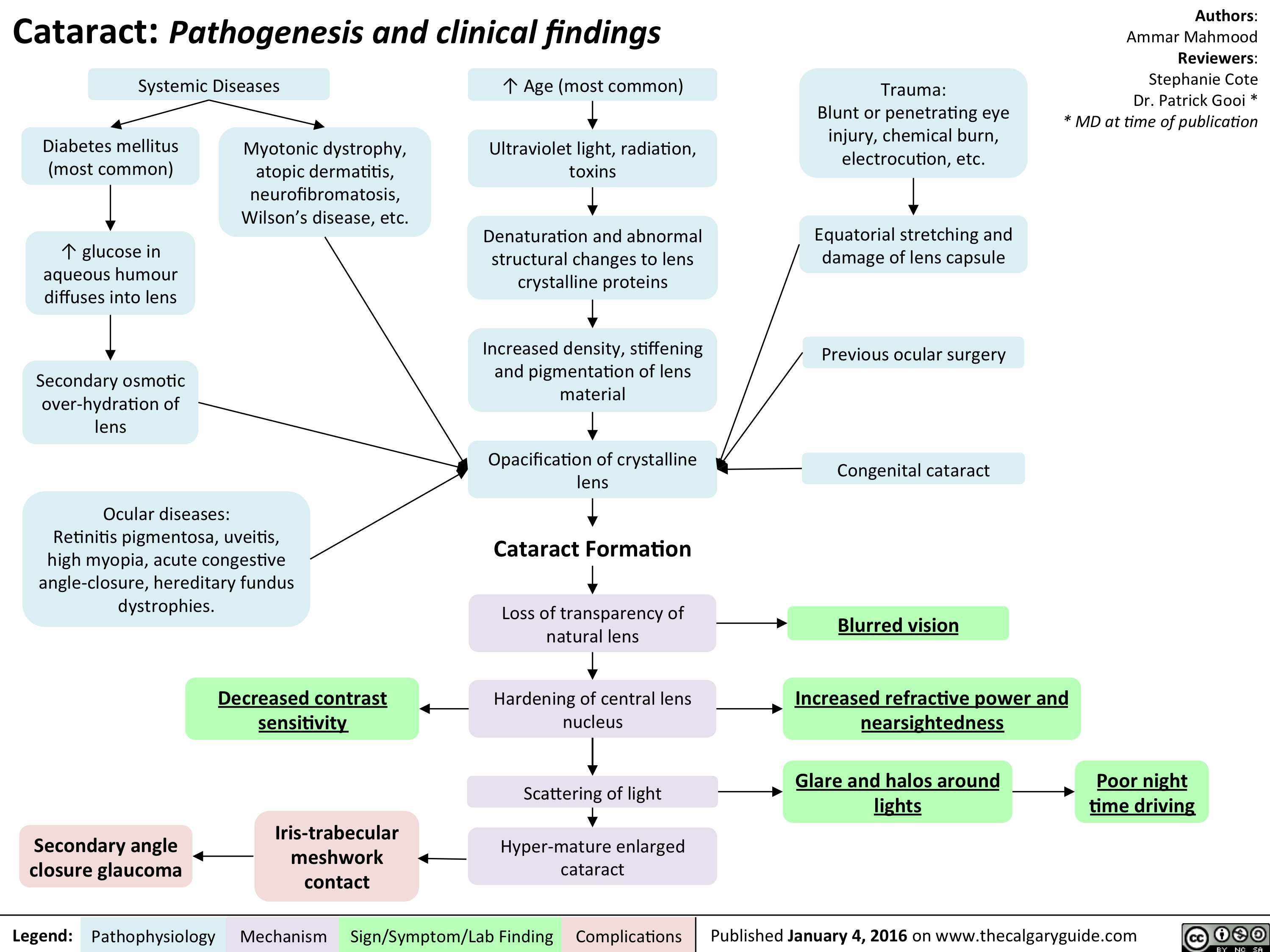
Cataracts - pathogenesis and clinical findings
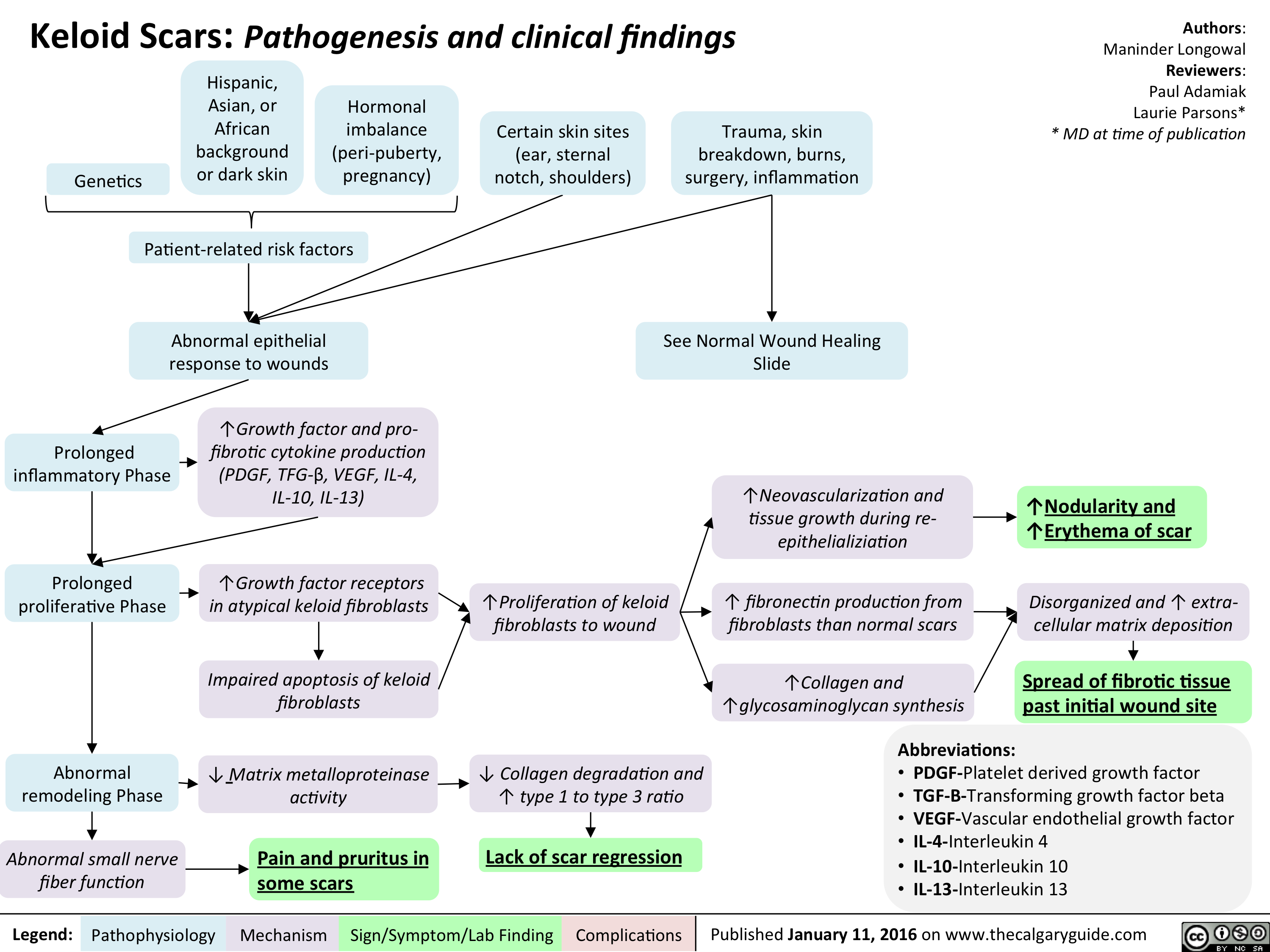
Keloid scar - pathogenesis and clinical findings
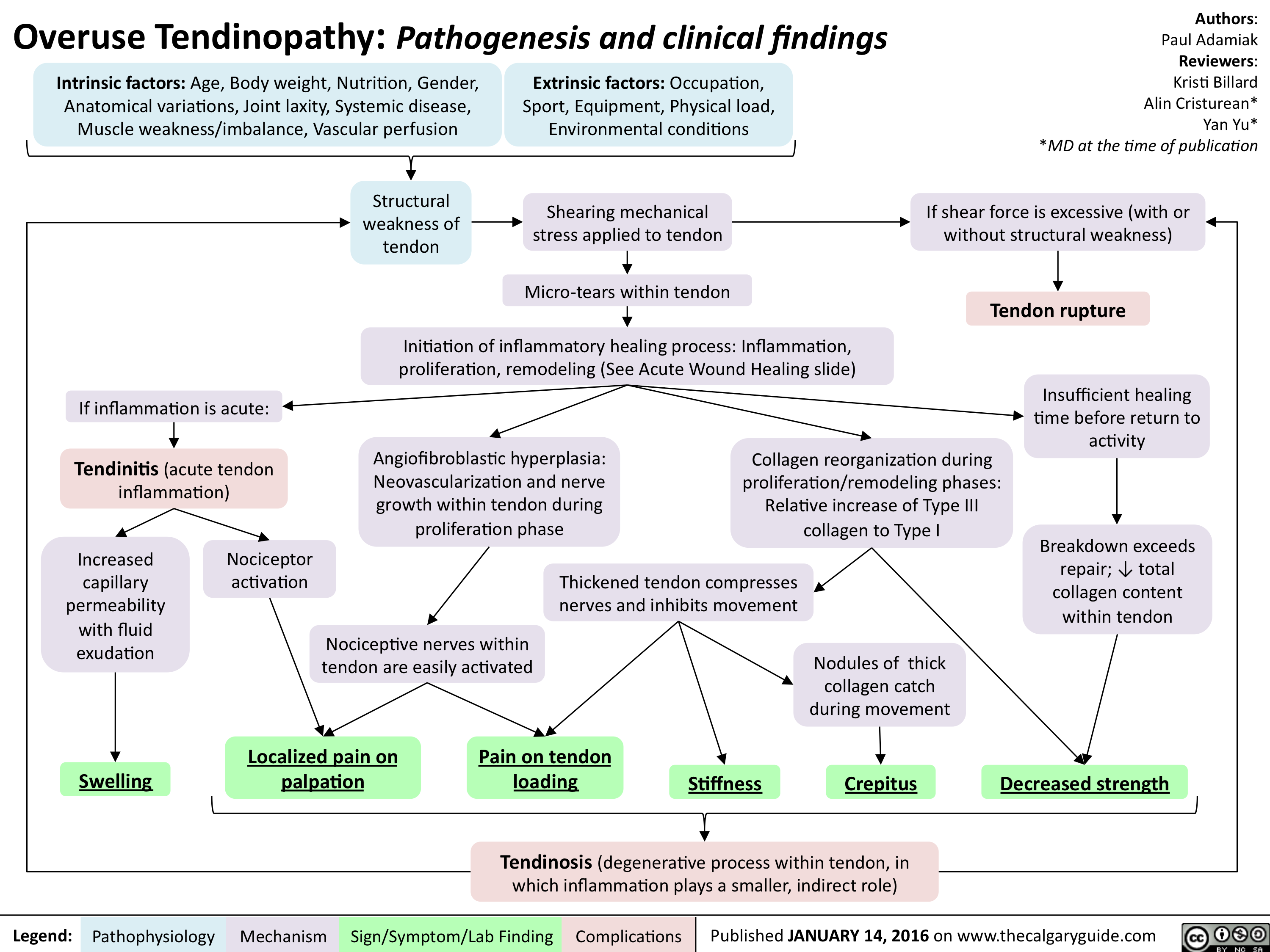
Overuse Tendinopathy -Pathogenesis and clinical findings
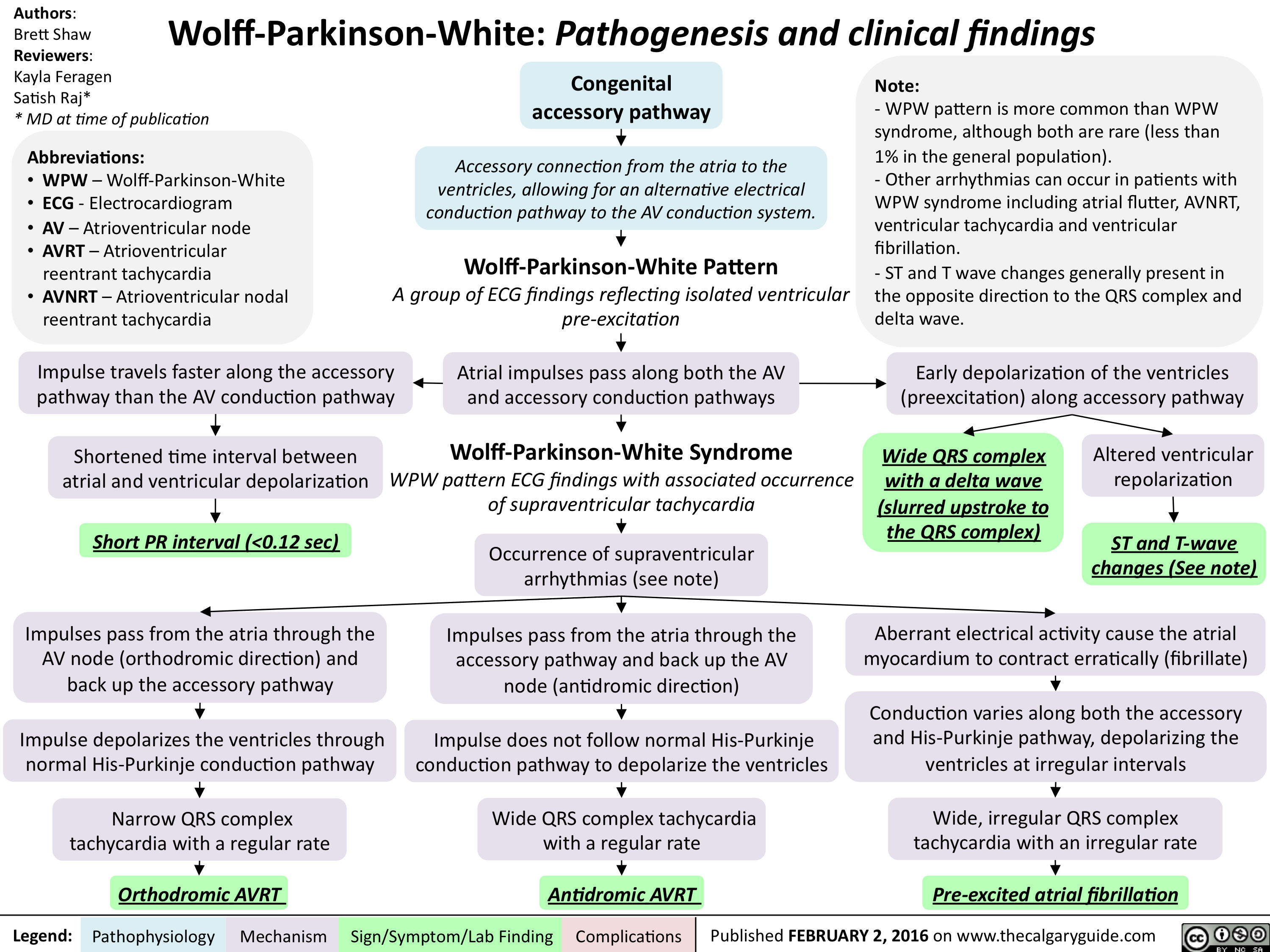
Wolff Parkinson White - Pathogenesis and clinical findings
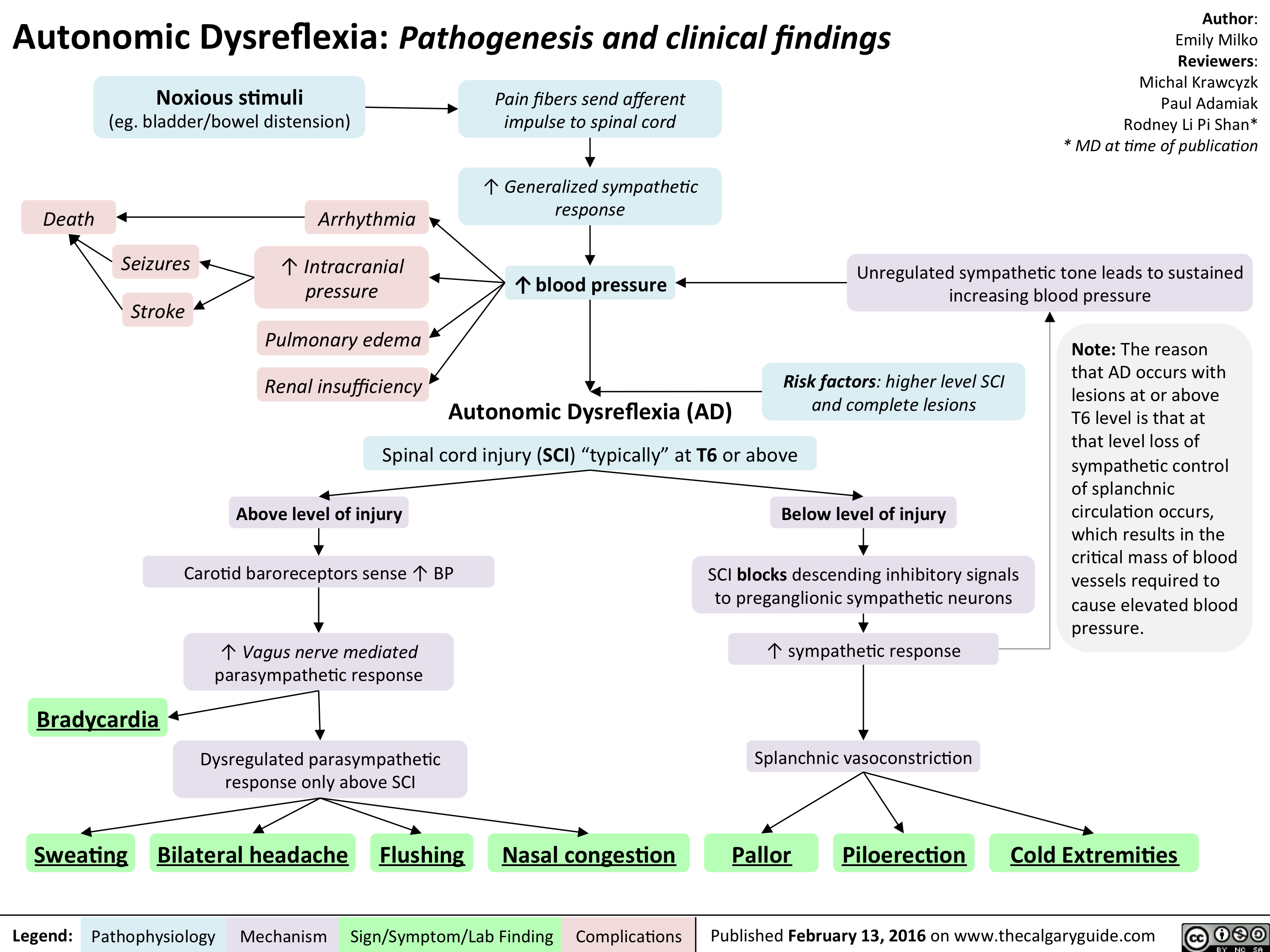
Autonomic Dysreflexia - Pathogenesis and clinical findings
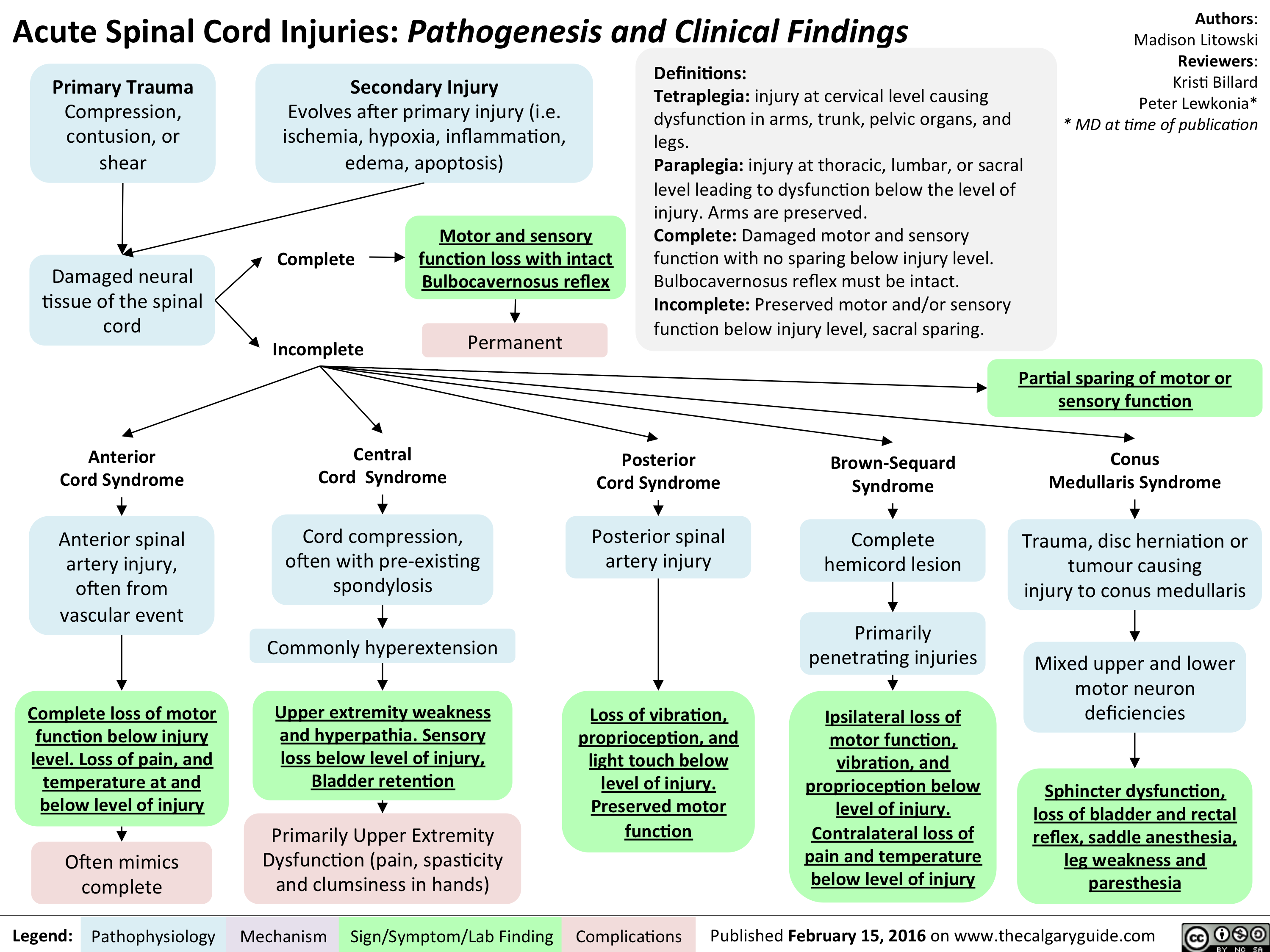
Acute Spinal Cord Injuries - Pathogenesis and clinical findings
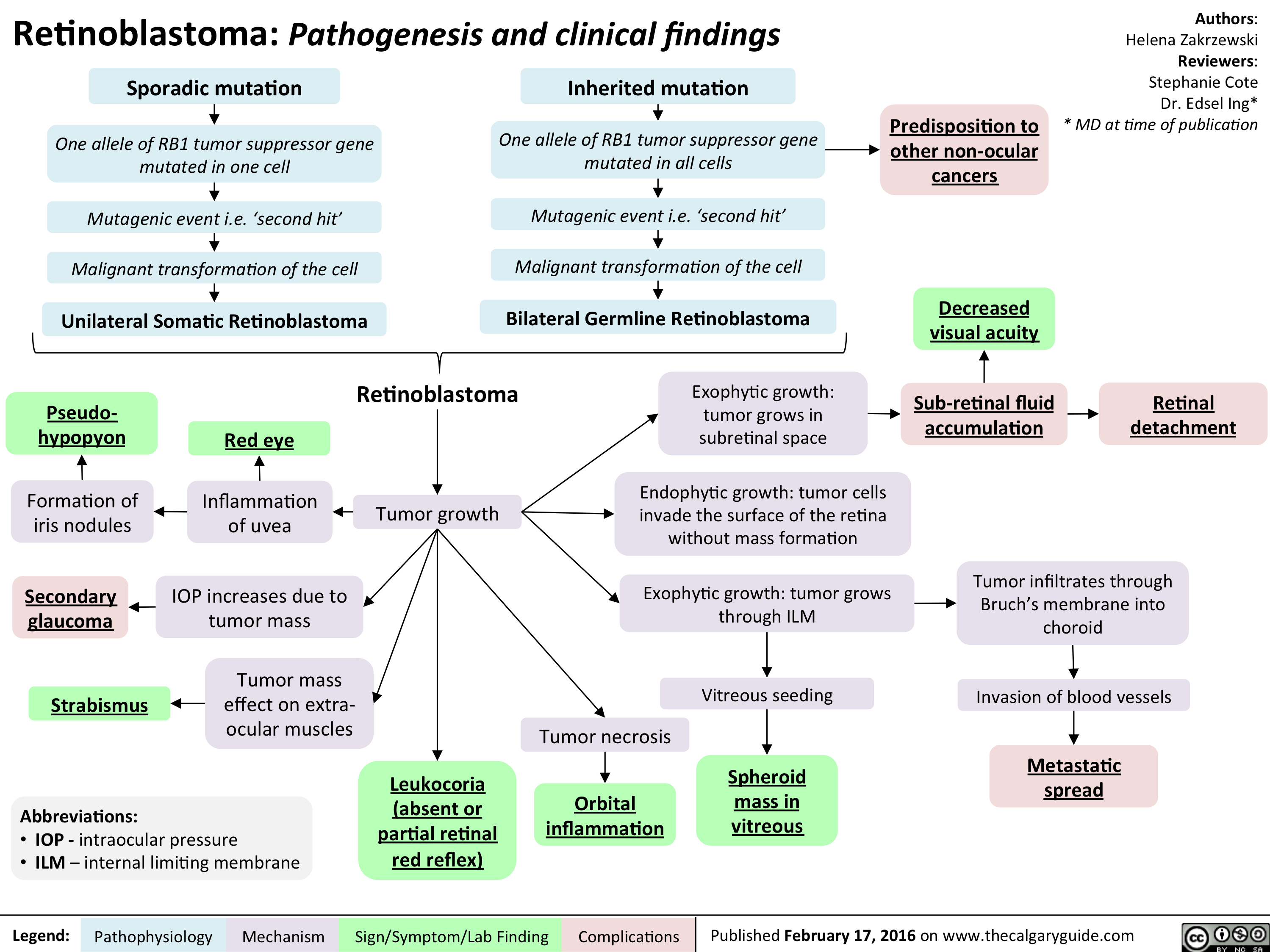
Retinoblastoma - Pathogenesis and clinical findings
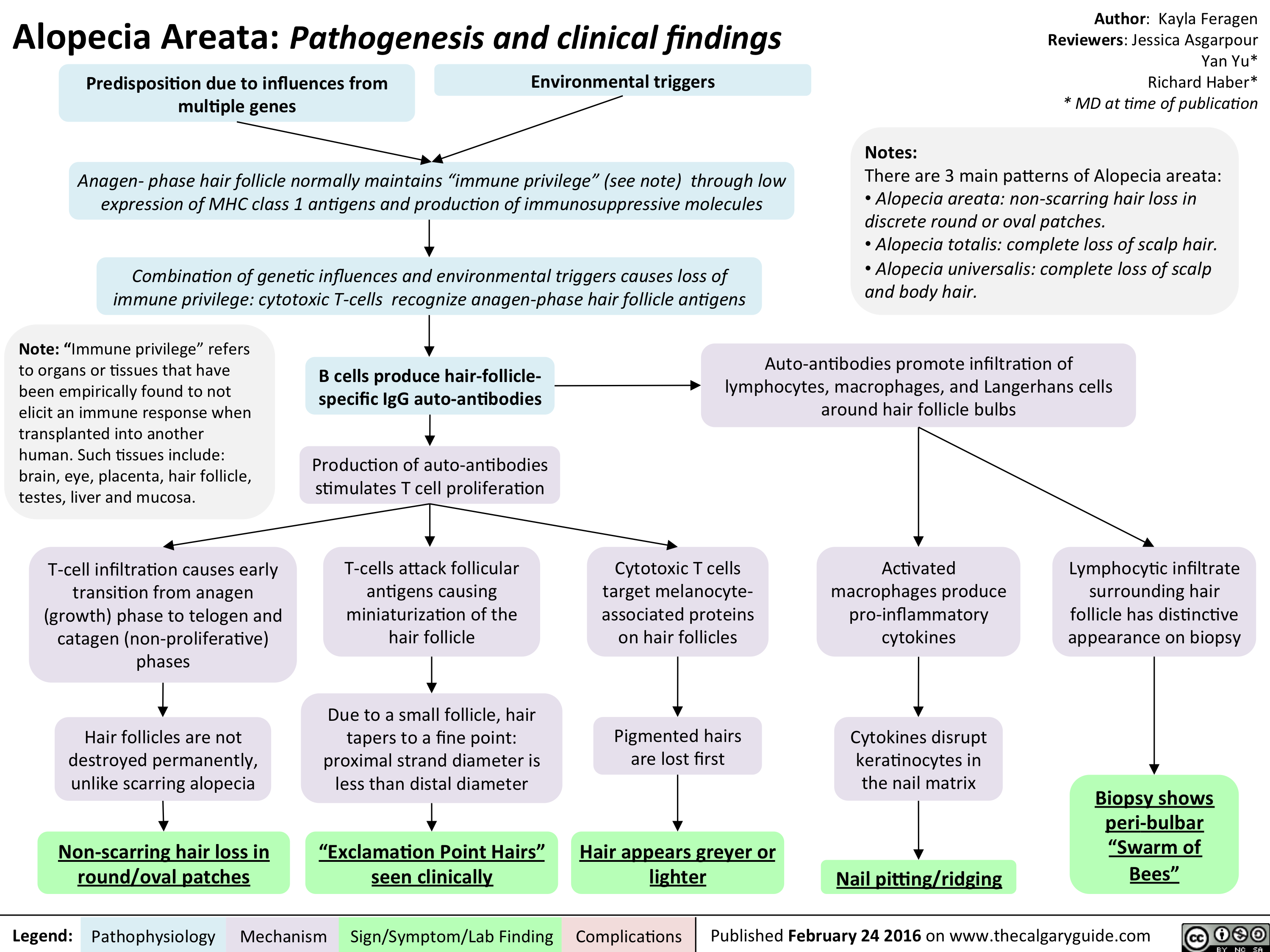
Alopecia Areata - Pathogenesis and clinical findings
Seasonal Affective Disorder - Pathogenesis and clinical findings v2

Yu, Y - Schizophrenia Pathogenesis and Clinical Findings - March 26 2016
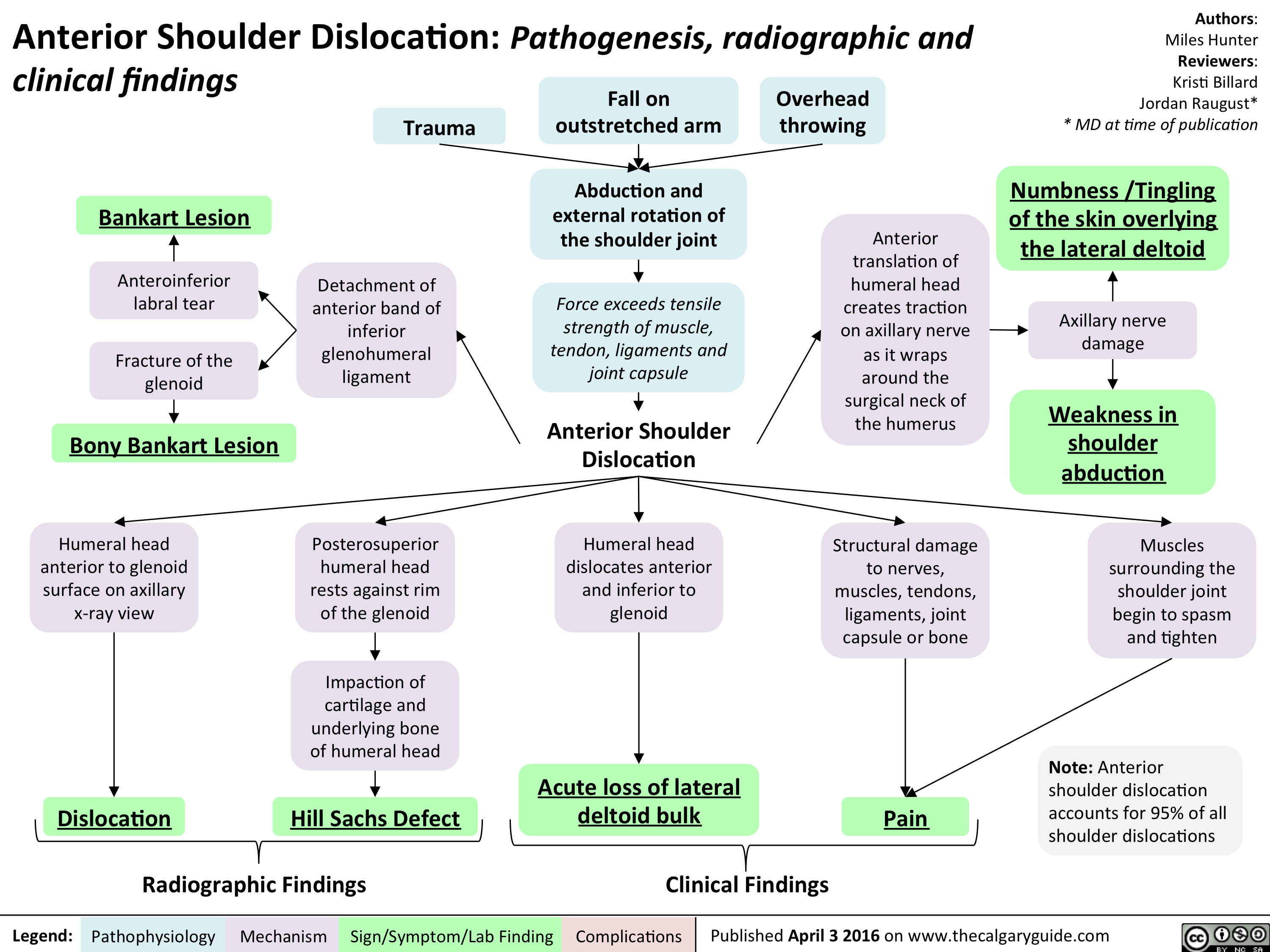
Anterior Shoulder Dislocation - Pathogensis clinical and radiographic findings
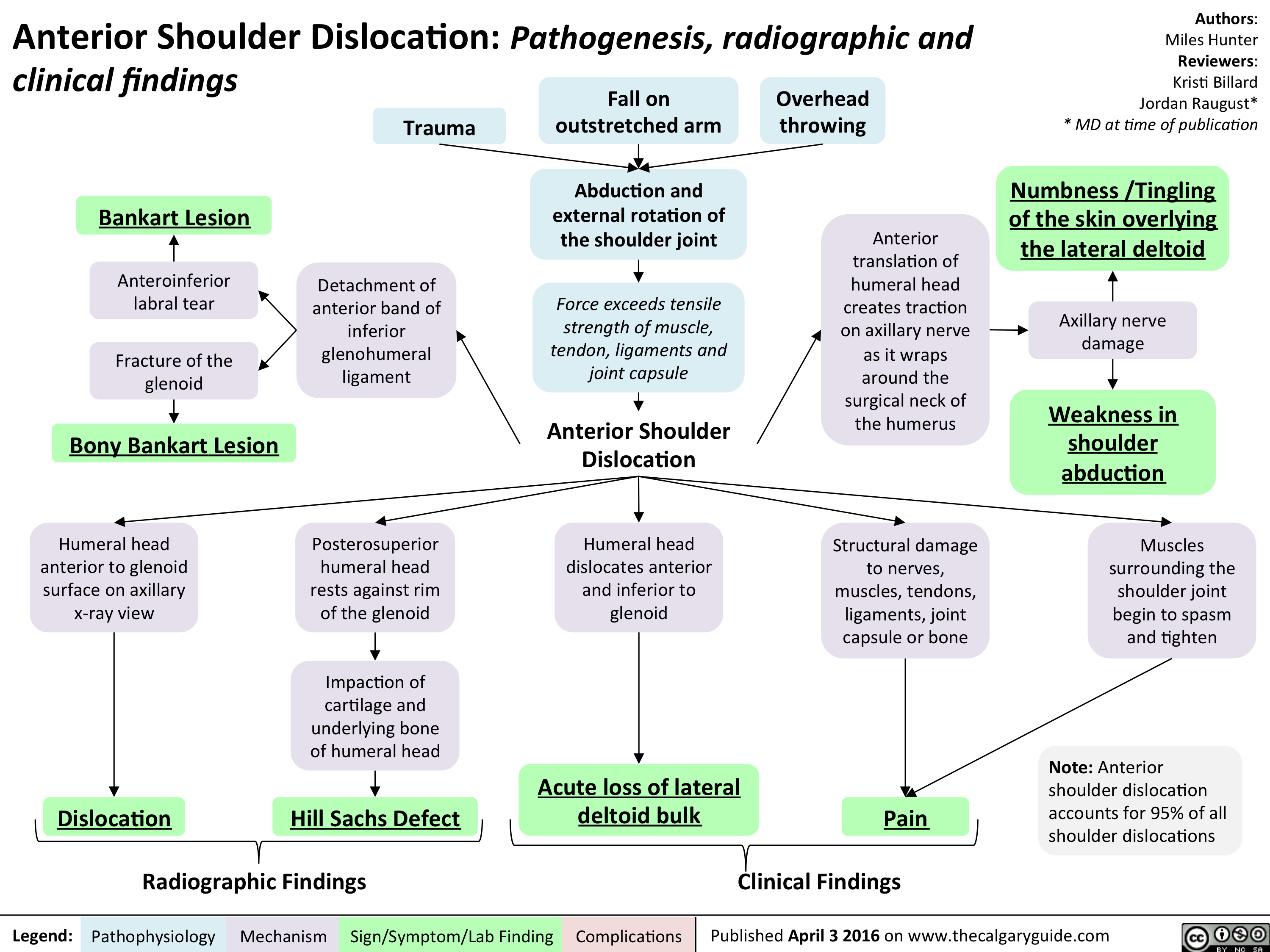
Anterior Shoulder Dislocation - Pathogensis clinical and radiographic findings
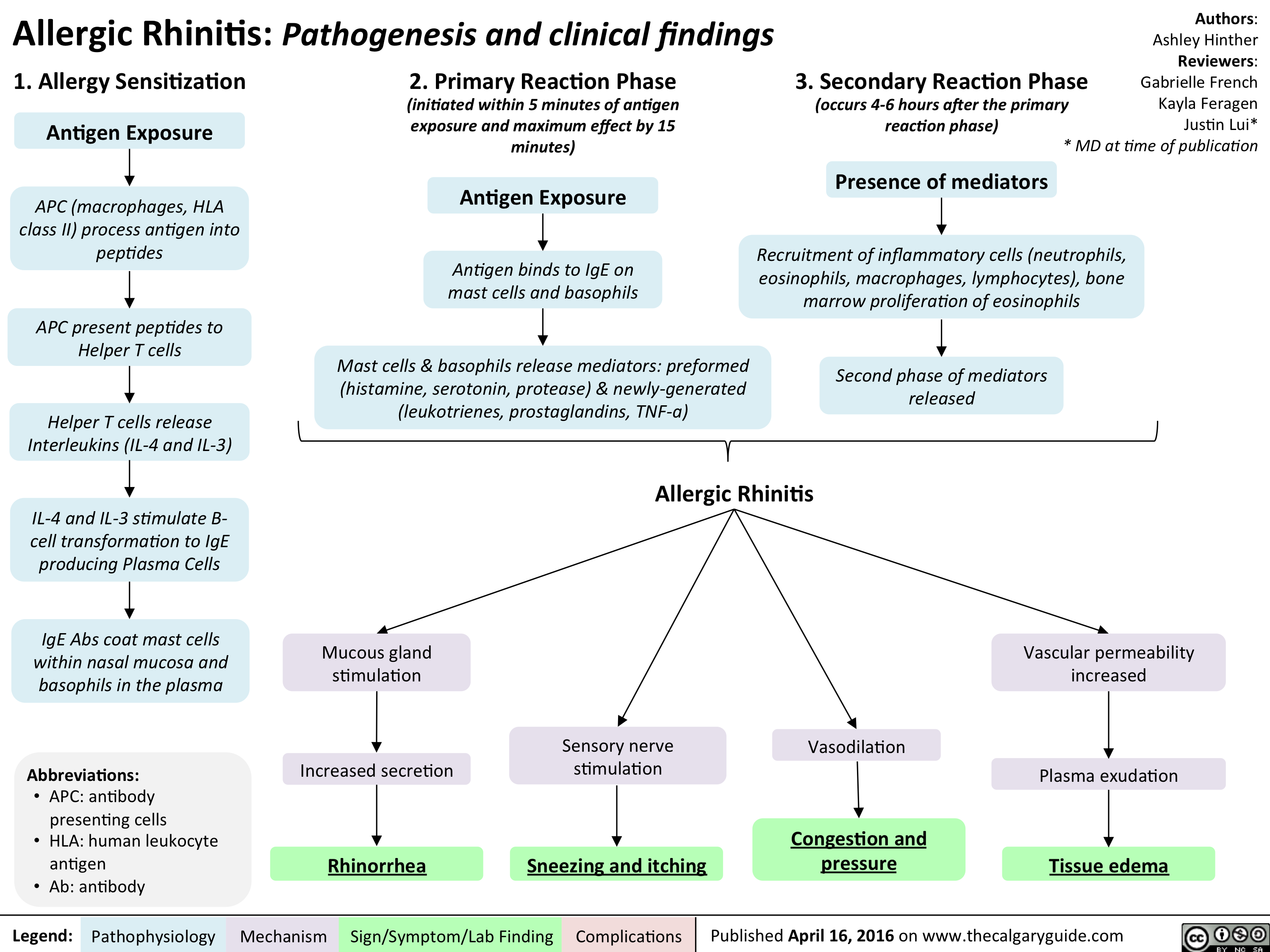
Allergic Rhinitis - Pathogenesis and clinical findings
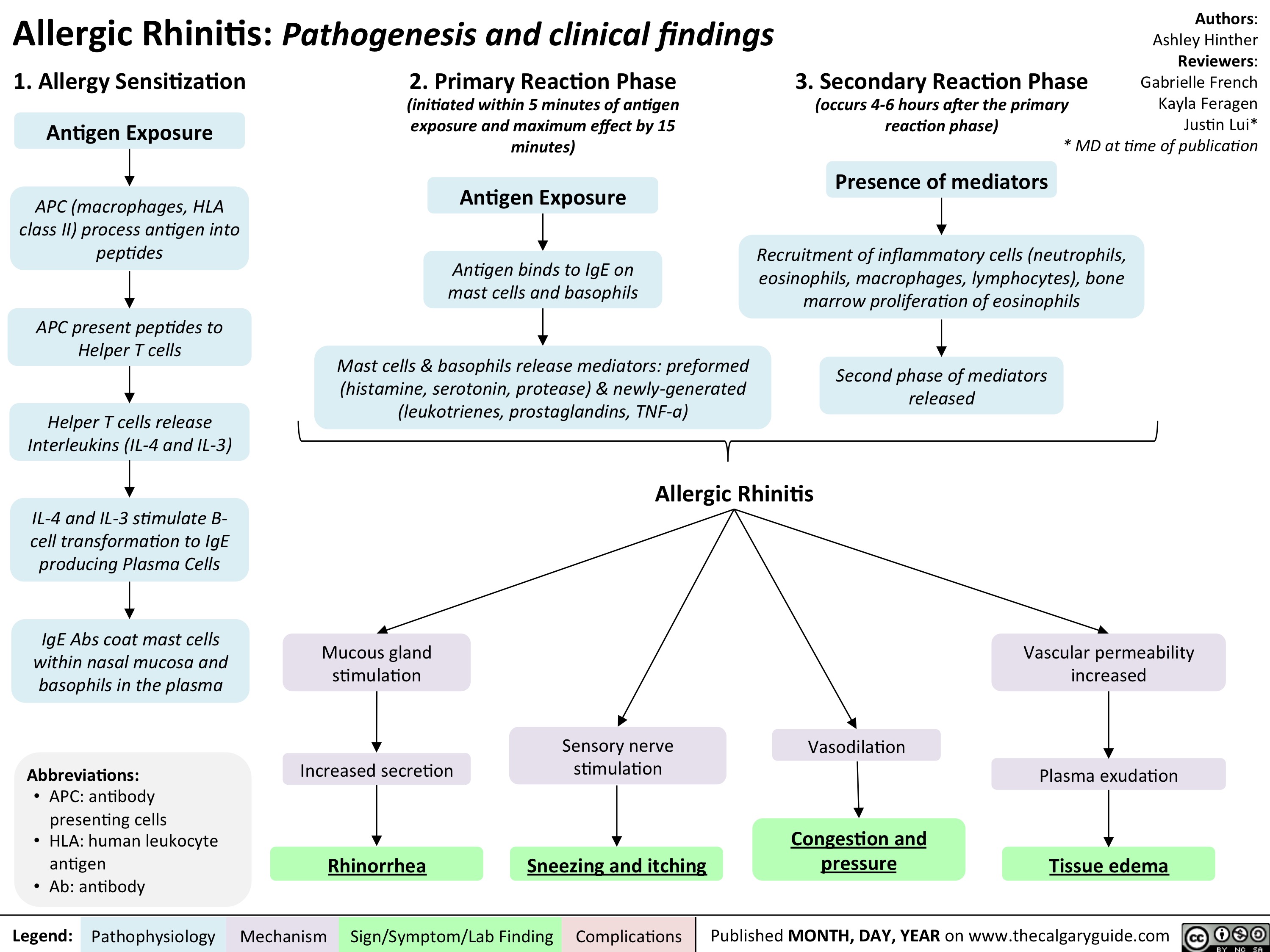
Allergic Rhinitis - Pathogenesis and clinical findings
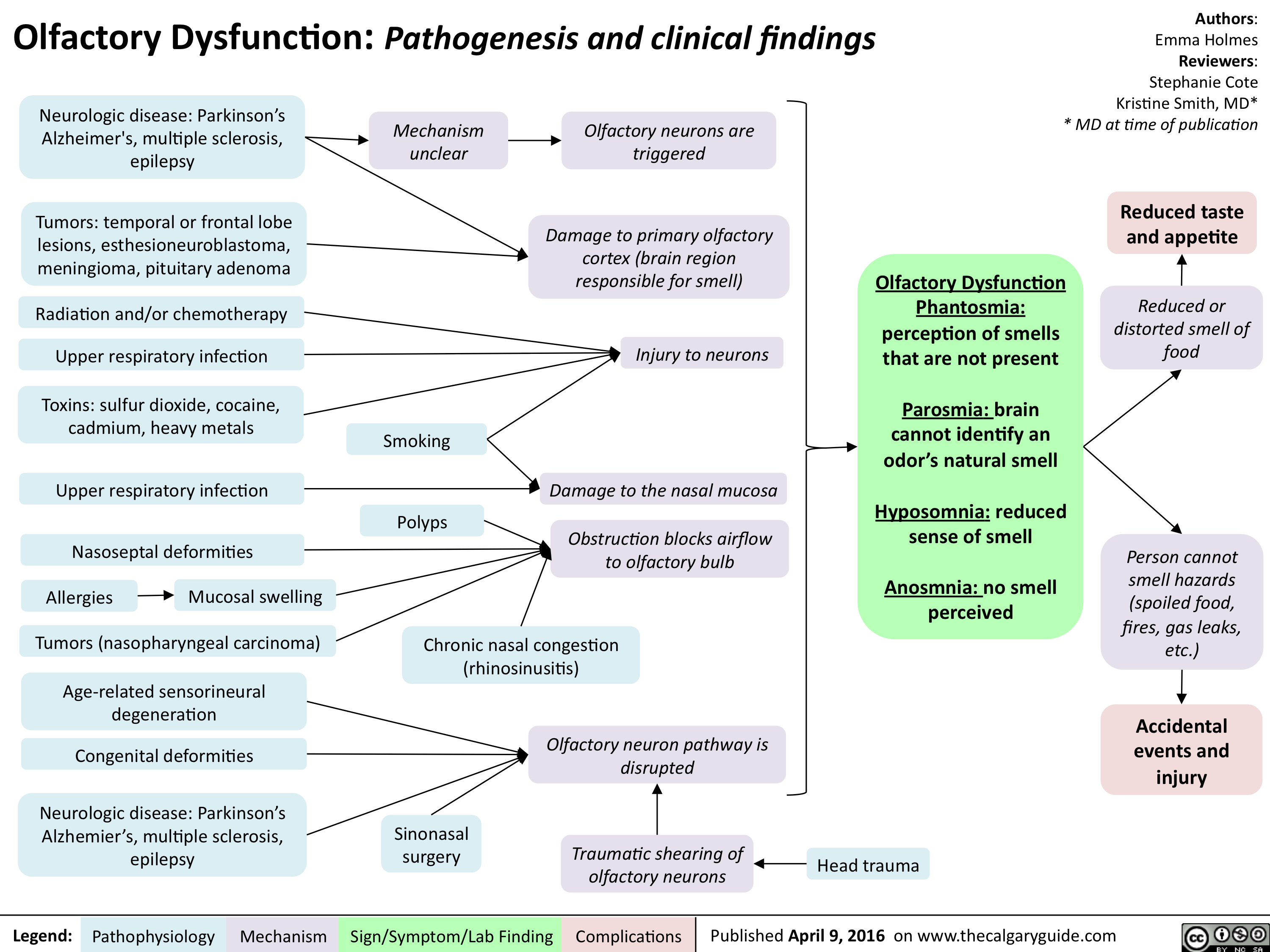
Olfactory Dysfunction - Pathogenesis and clinical findings
Tinnitus

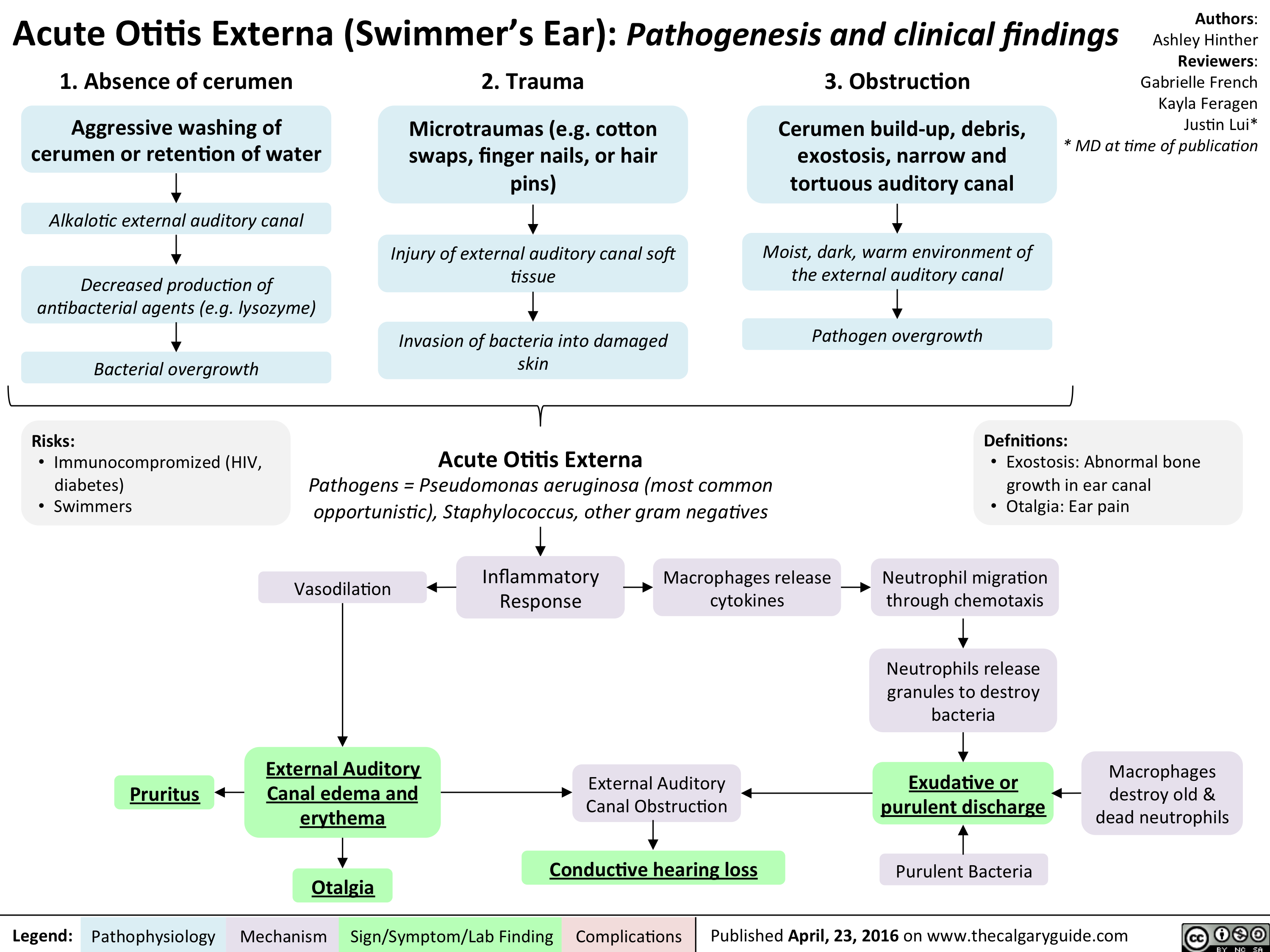
Acute Otitis Externa
Psoriasis: Pathogenesis and clinical findings

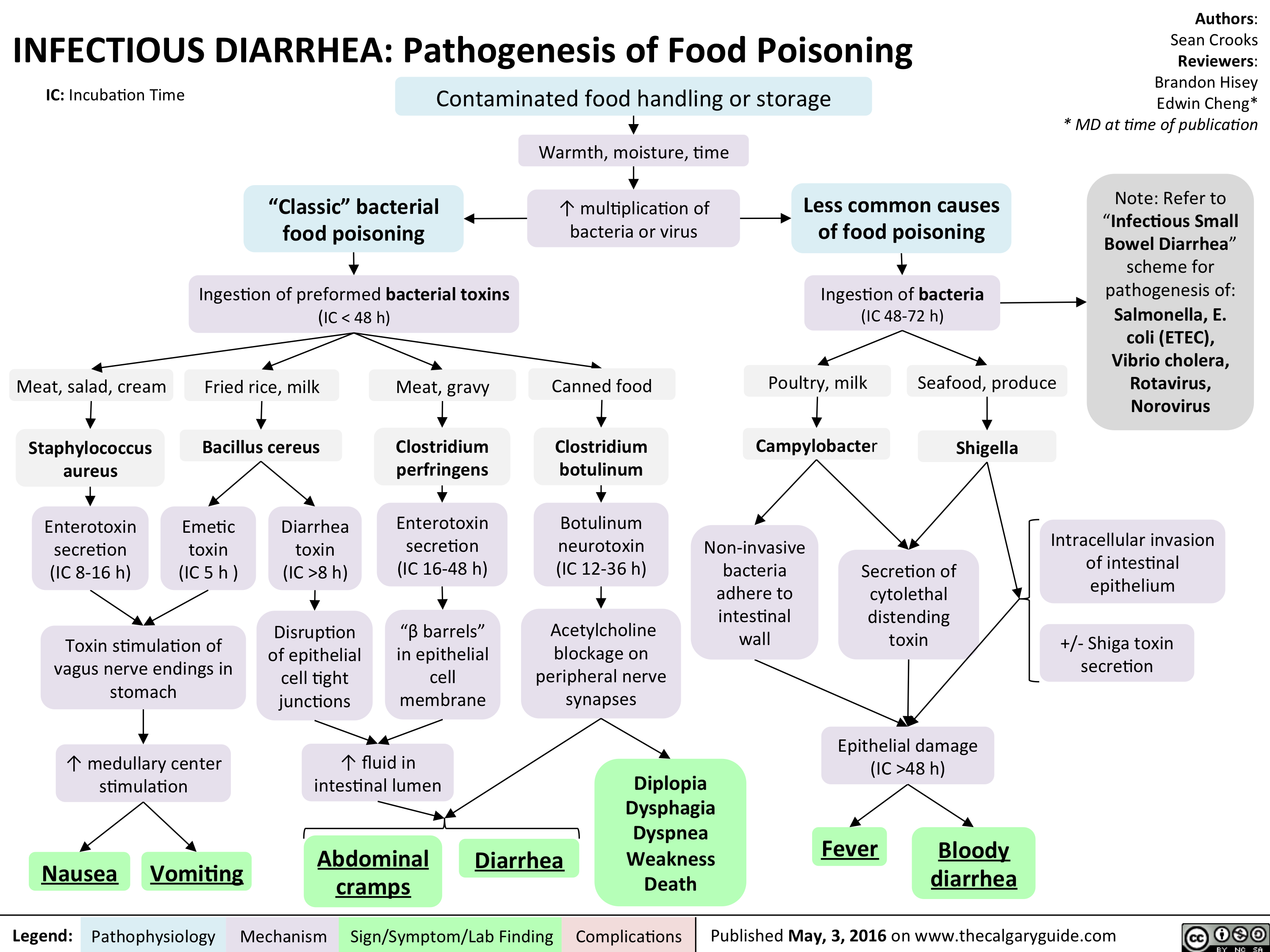
InfectiousFoodPoisoning
1st gen antipsychotics Translated

Anti-Psikotik Generasi Kedua: Mekanisme dan Efek Samping
2nd generation antipsychotics Translated
Anti-Psikotik Generasi Kedua (Atipikal): Mekanisme dan Efek Samping
Anti-Psikotik Generasi Ketiga: Mekanisme dan Efek Samping
1st gen antipsychotics Translated
2nd generation antipsychotics Translated
1st gen antipsychotics Translated
3rd gen anti-psychotics Translated
Schizophrenia Pathogenesis Translated
Pathogenesis of Anxiety Disorders Translated
SAD Gangguan Afektif Musiman Translated
PTSD Translated
Panic Disorder Translated
OCD Translated
Bipolar Disorder Translated
MDD Translated
SSRIs Translated
Bupropion Translated
SNRIs Translated
Thacker, J - Social Anxiety Translated
DSM - Axis to Formulation Translated
Alcohol Use Translated
Seasonal Affective Disorder: Pathogenesis and clinical findings
Seasonal Affective Disorder: Pathogenesis and clinical findings
Slide1
Slide1

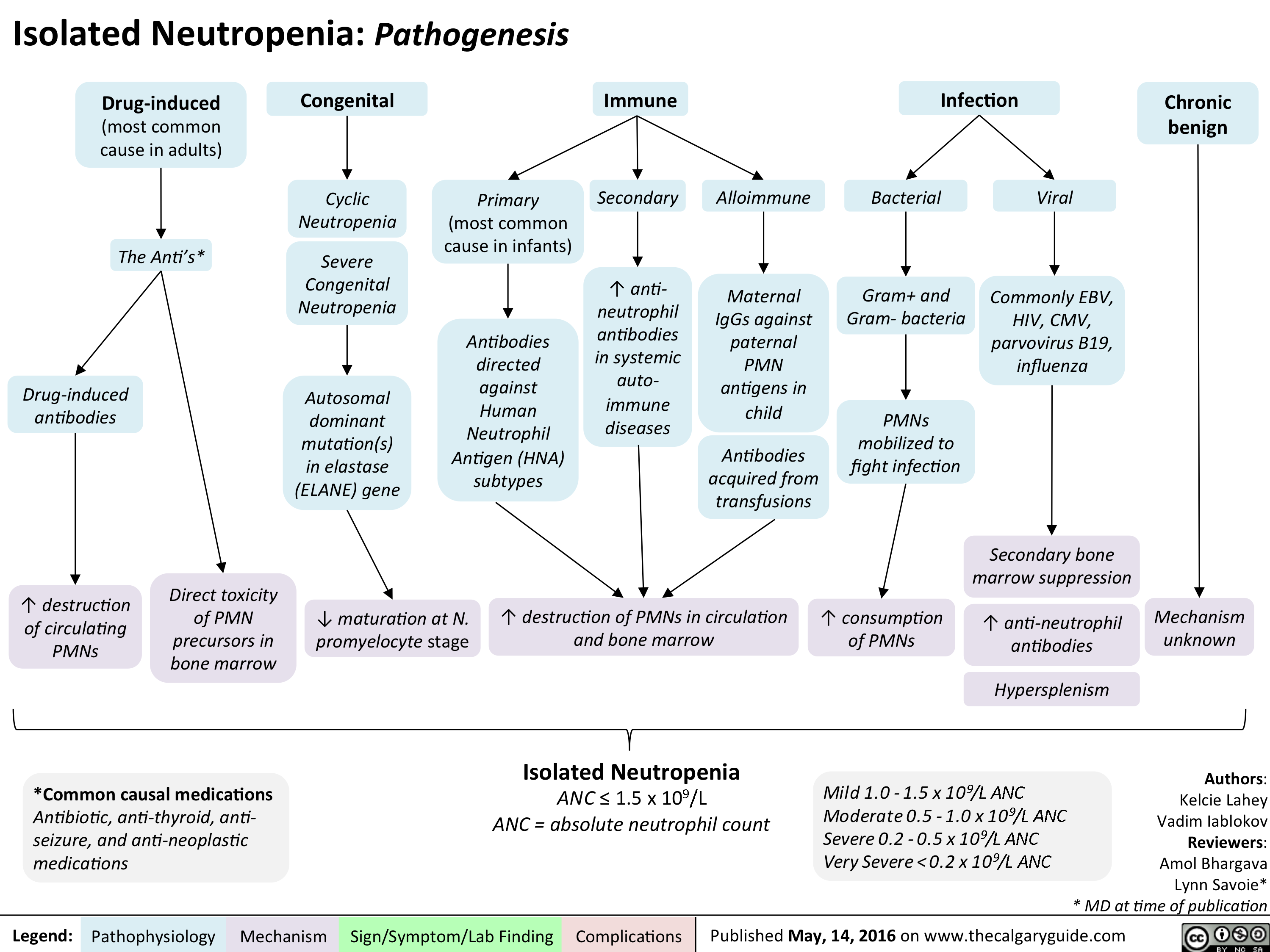
Isolated Neutropenia
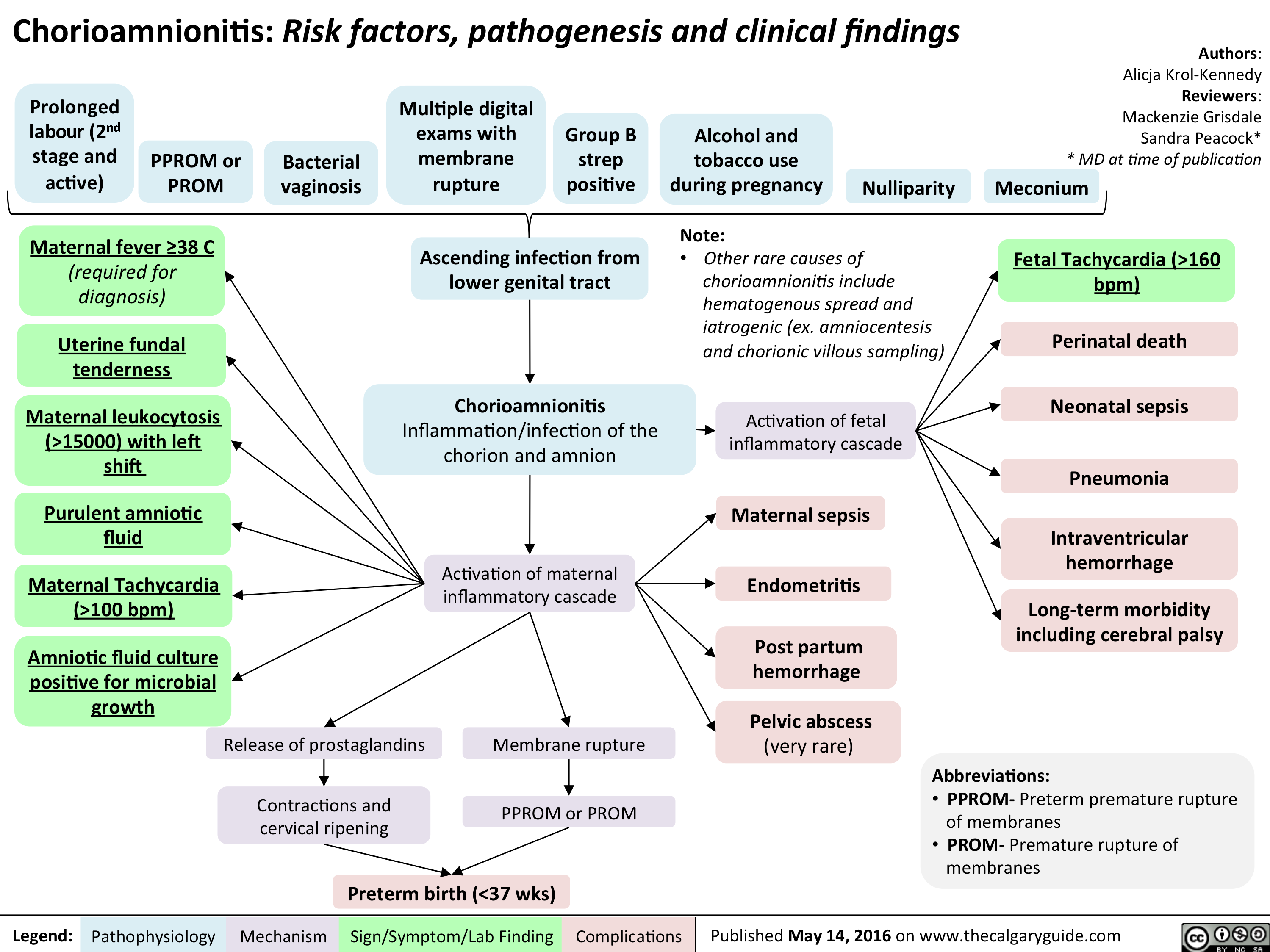
Chorioamnionitis: Risk factors, pathogenesis and clinical findings
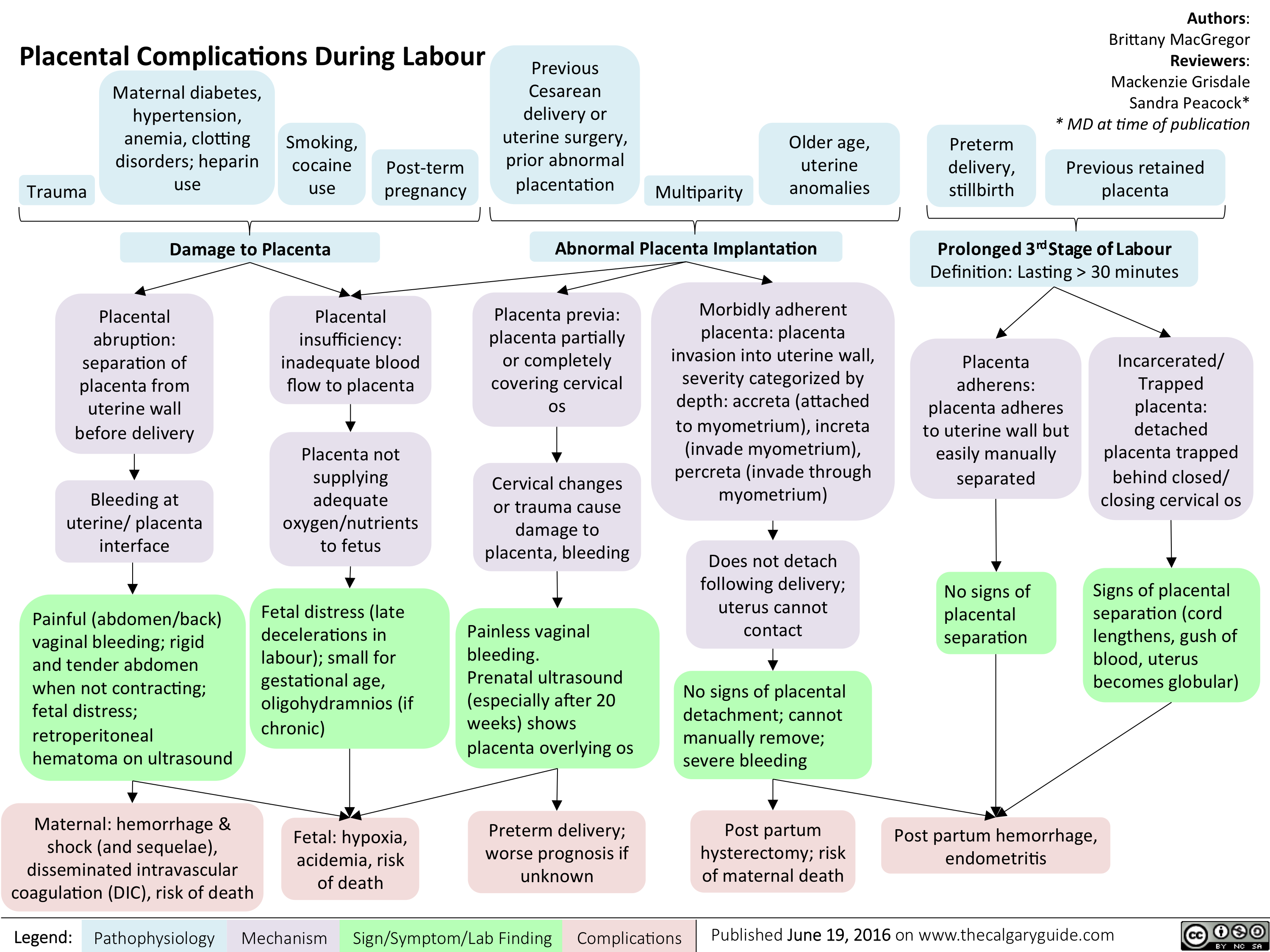
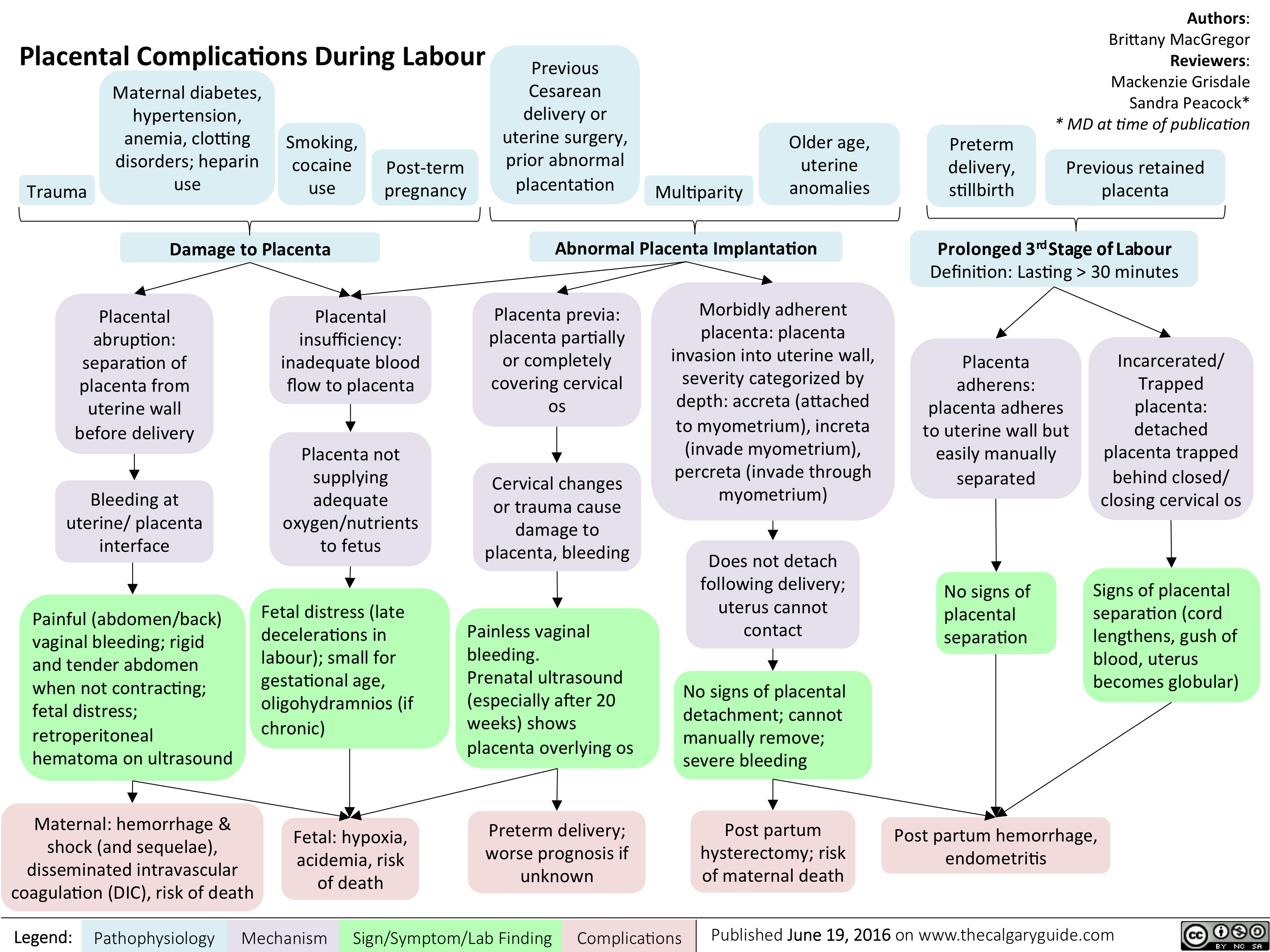
Placental Complications During Labour
Placental Complications During Labour
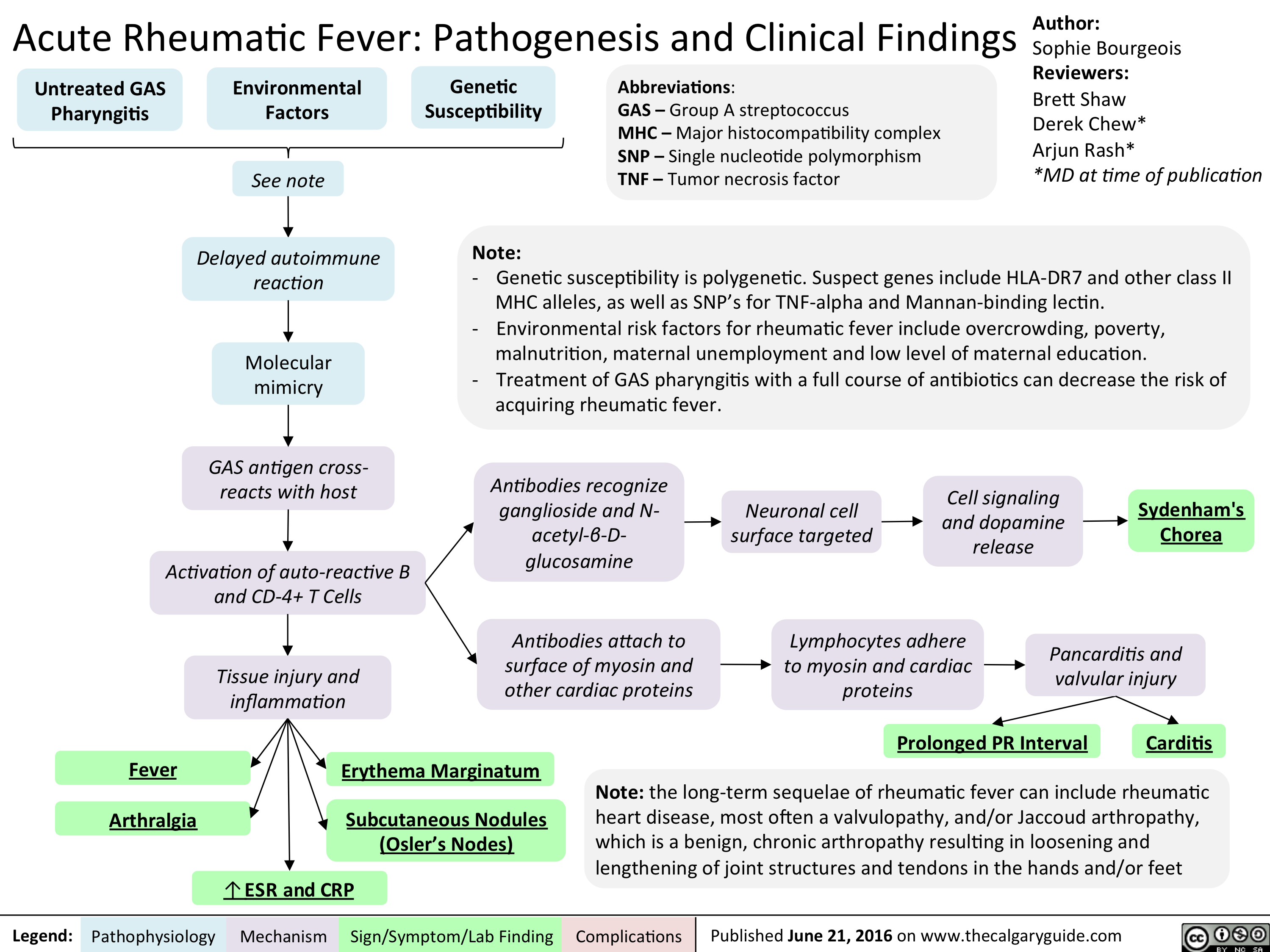
Acute Rheumatic Fever- Pathogenesis and Clinical Findings
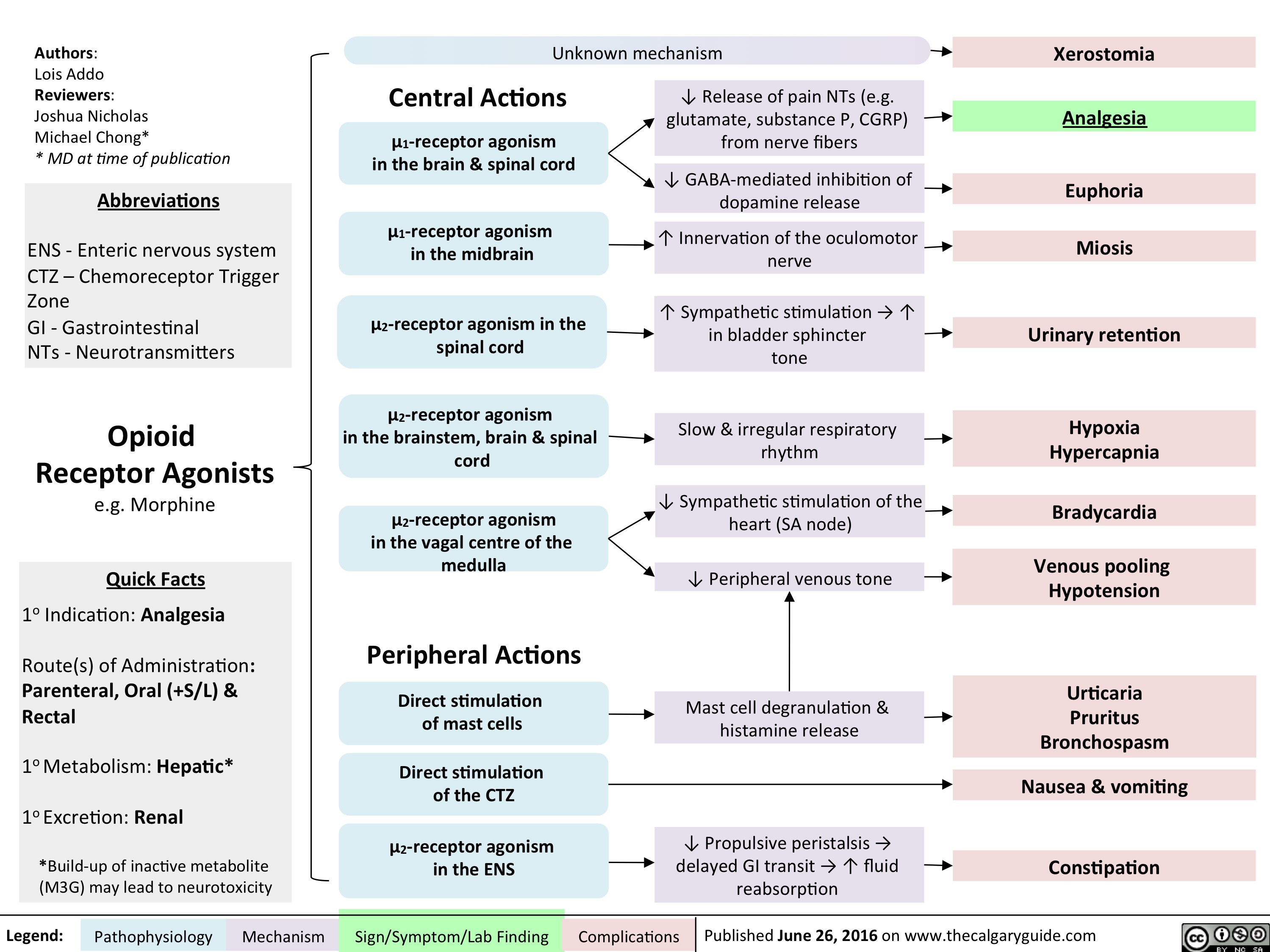
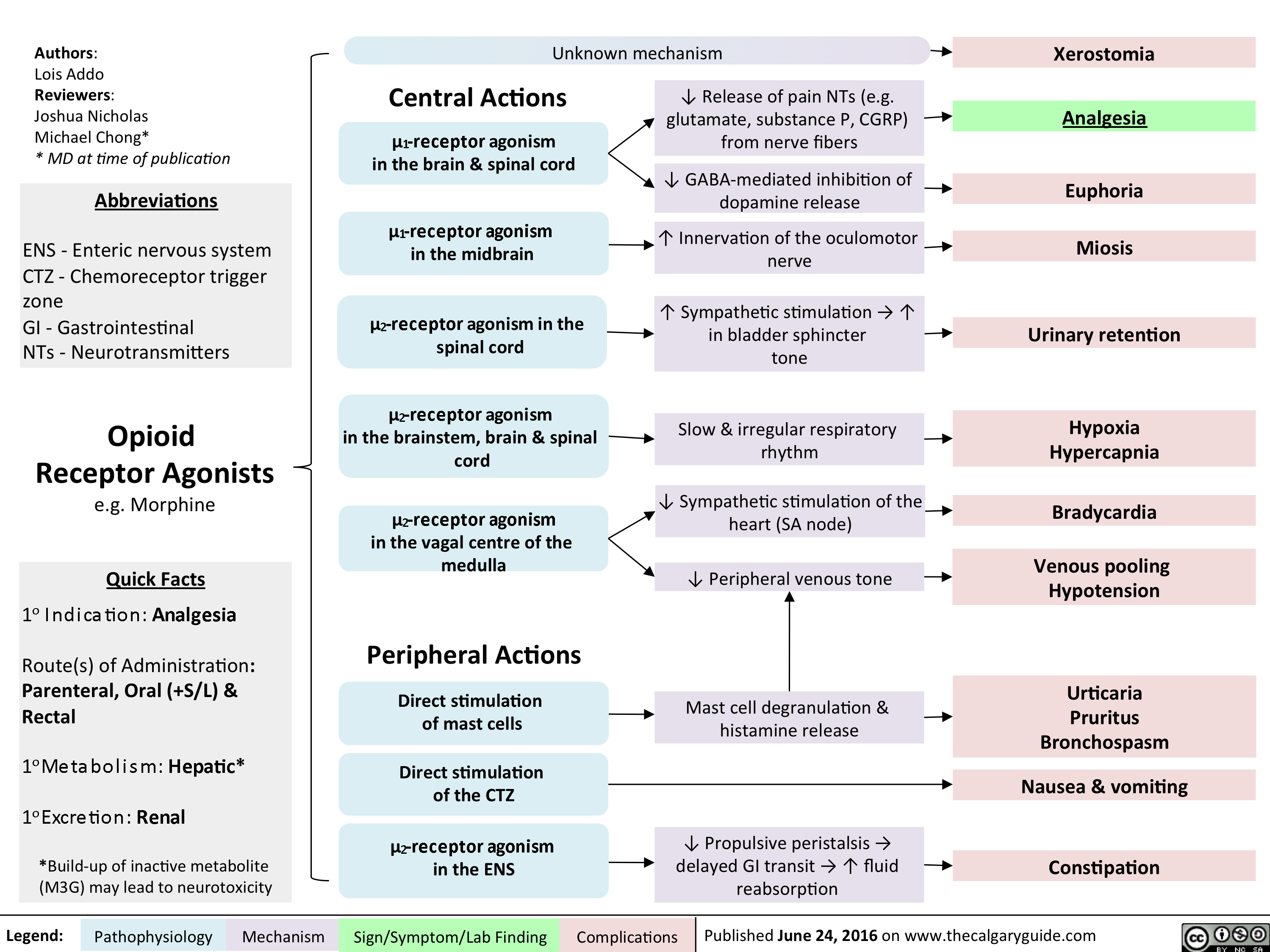
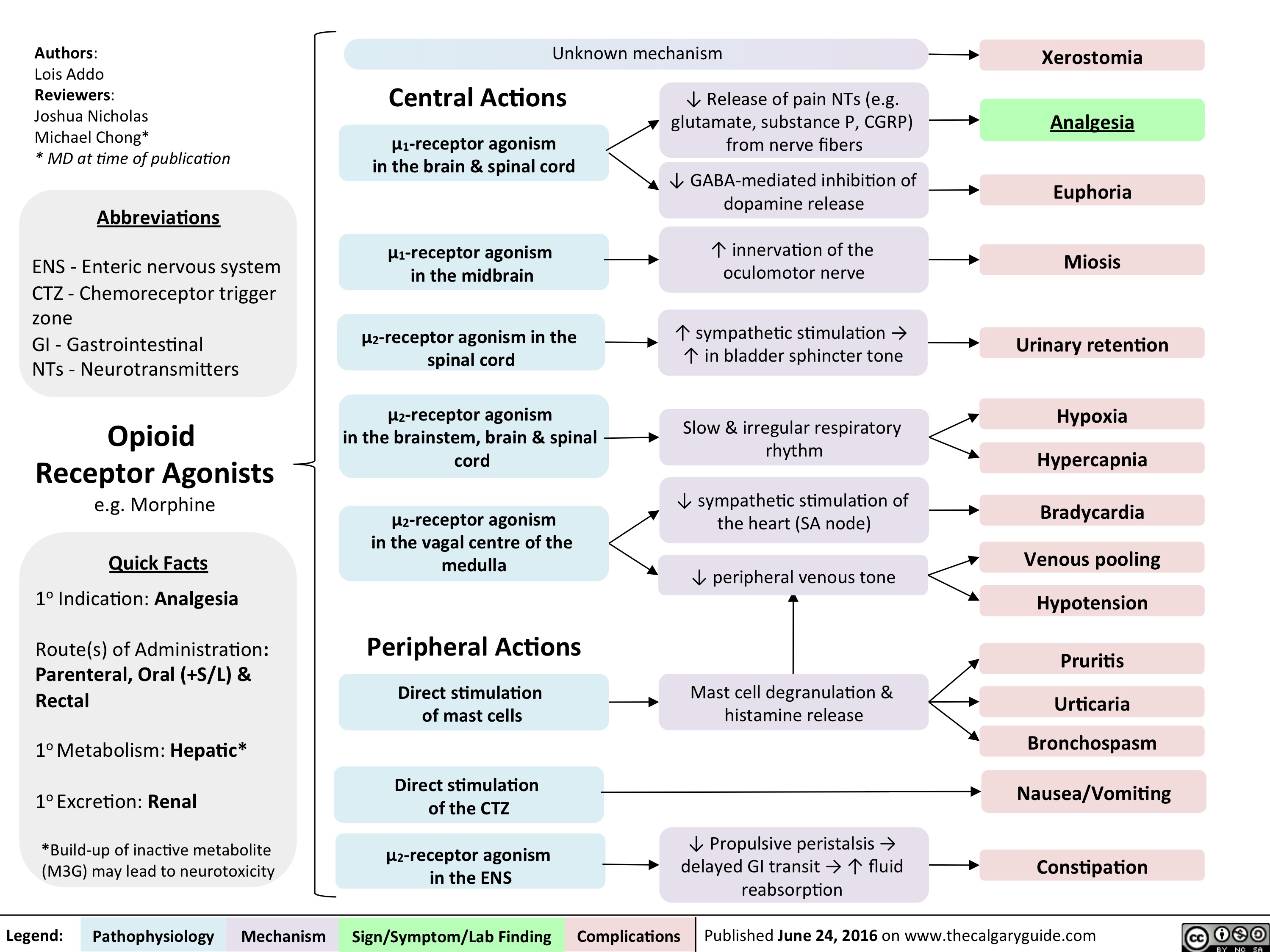
Opioid Receptor Agonists
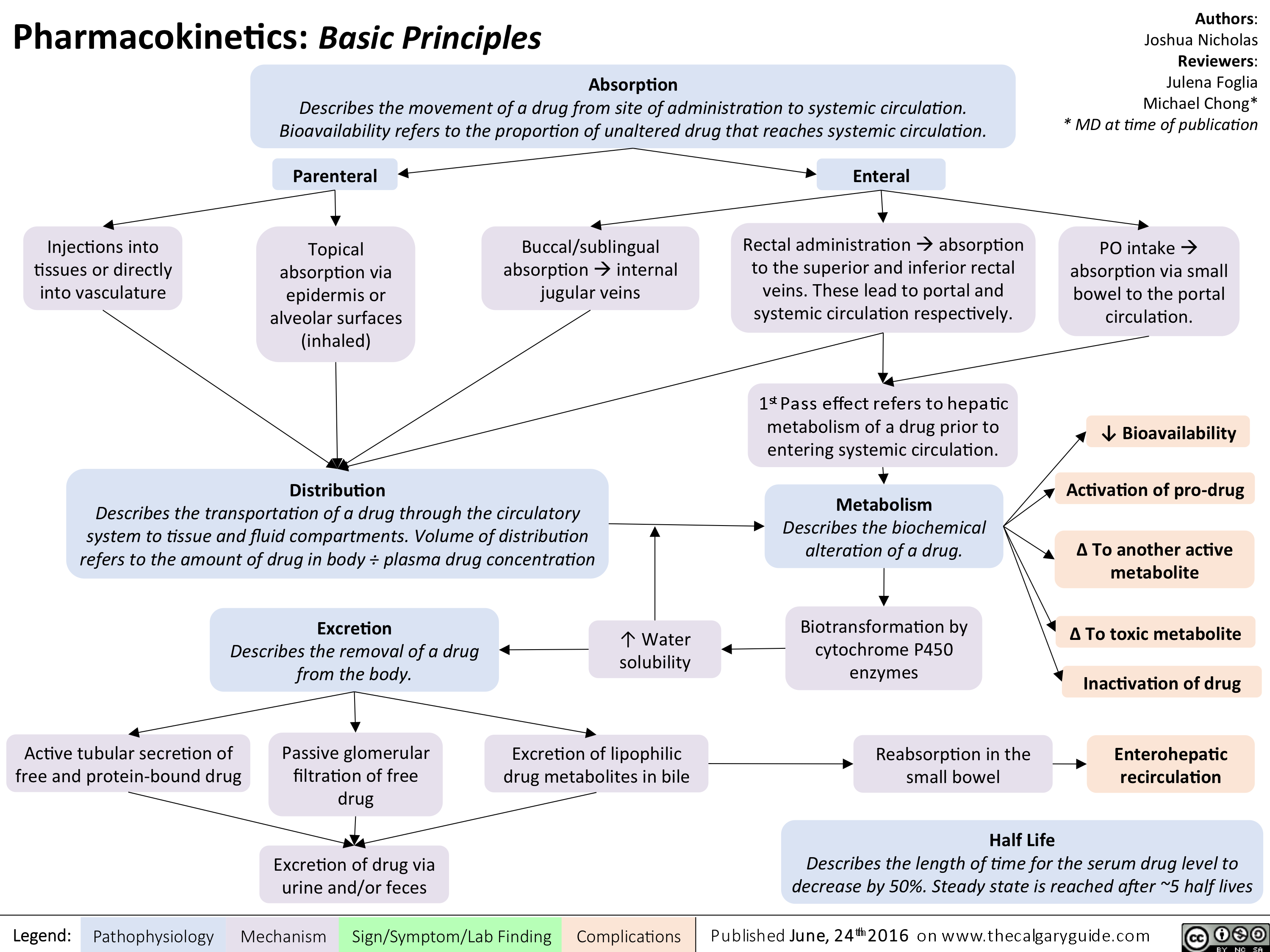
Pharmacokinetics Basic Principles
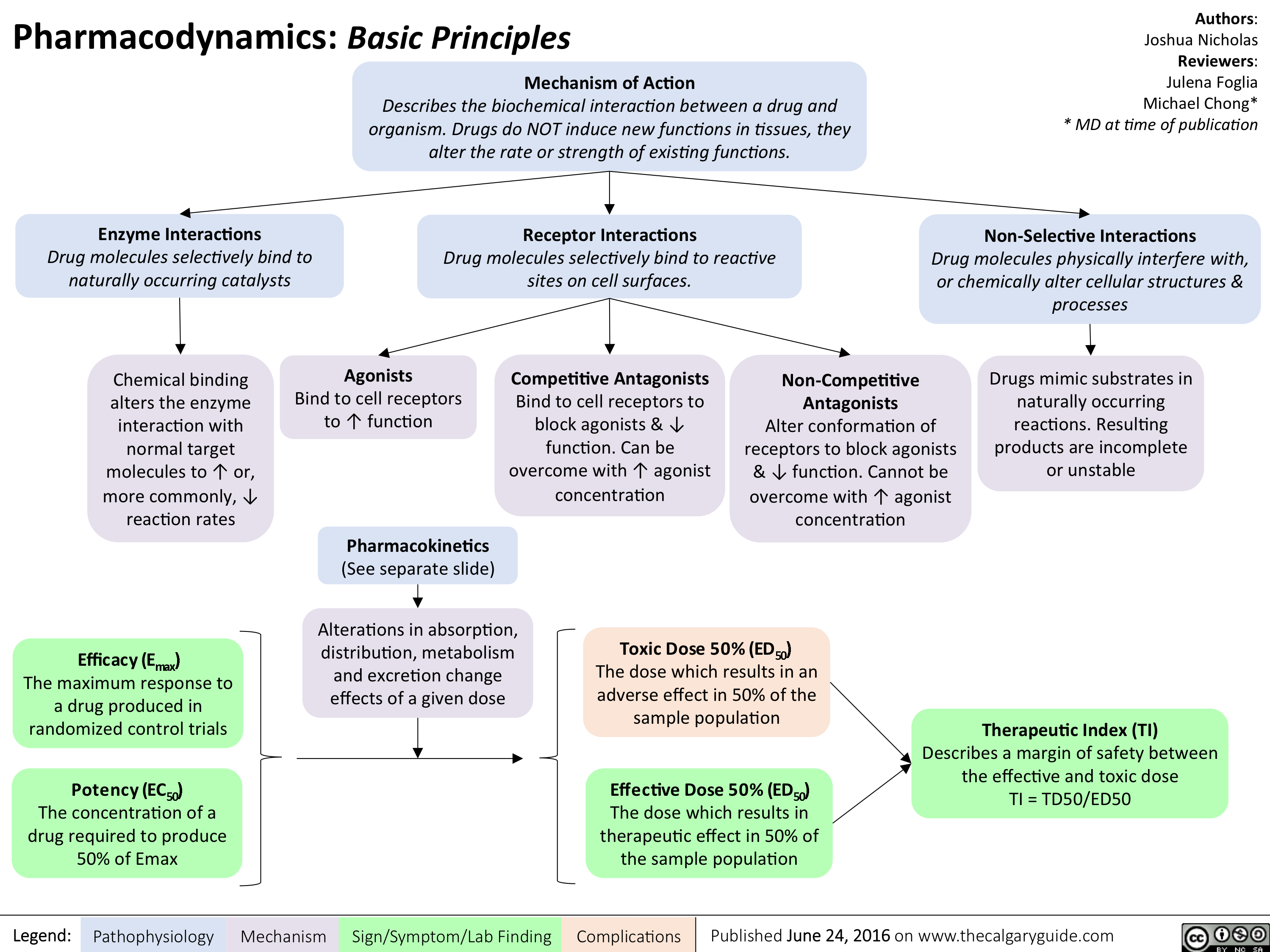
Pharmacodynamics Basic Principles
Opioid Receptor Agonists
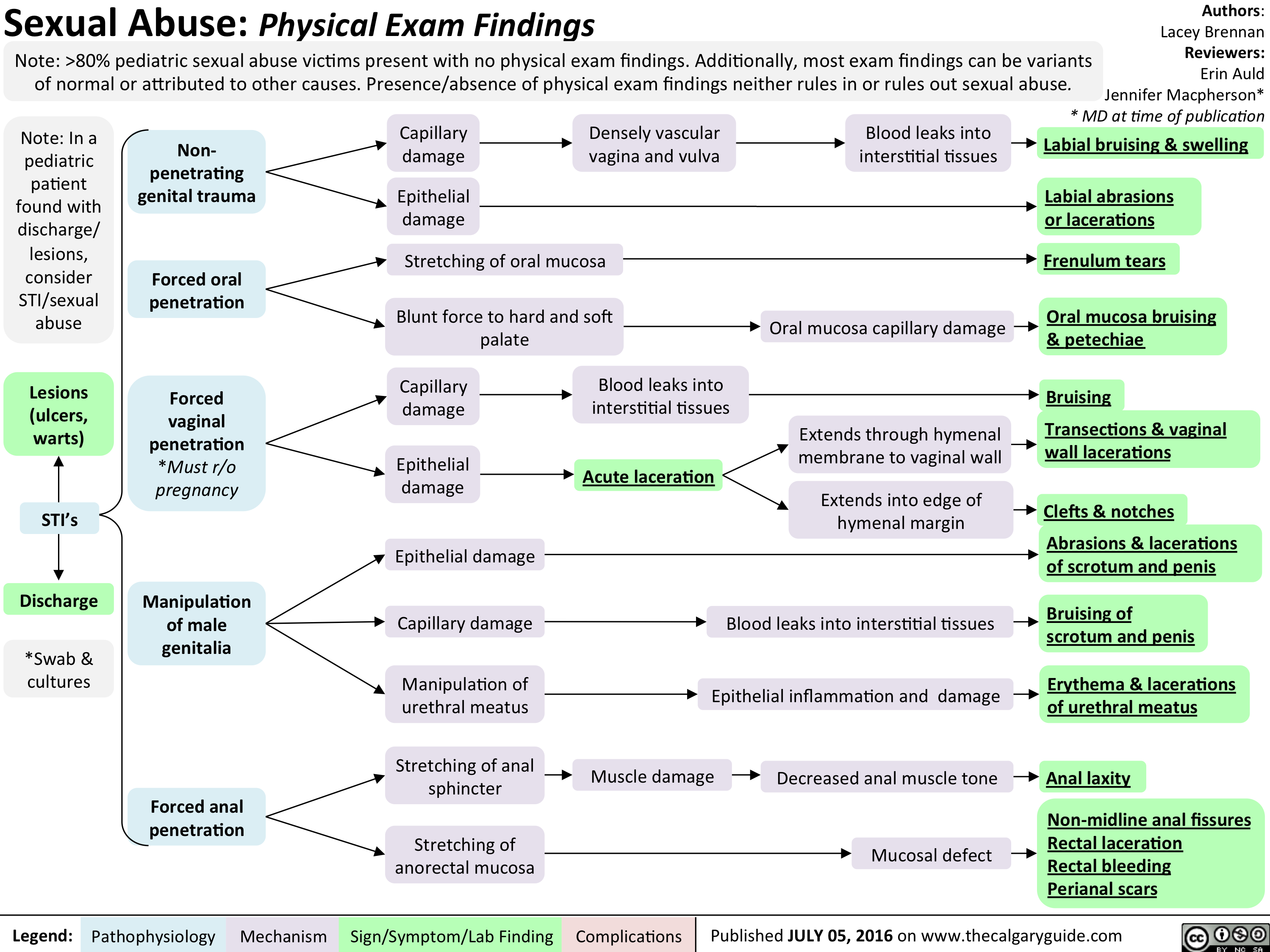
Peds Sexual Abuse
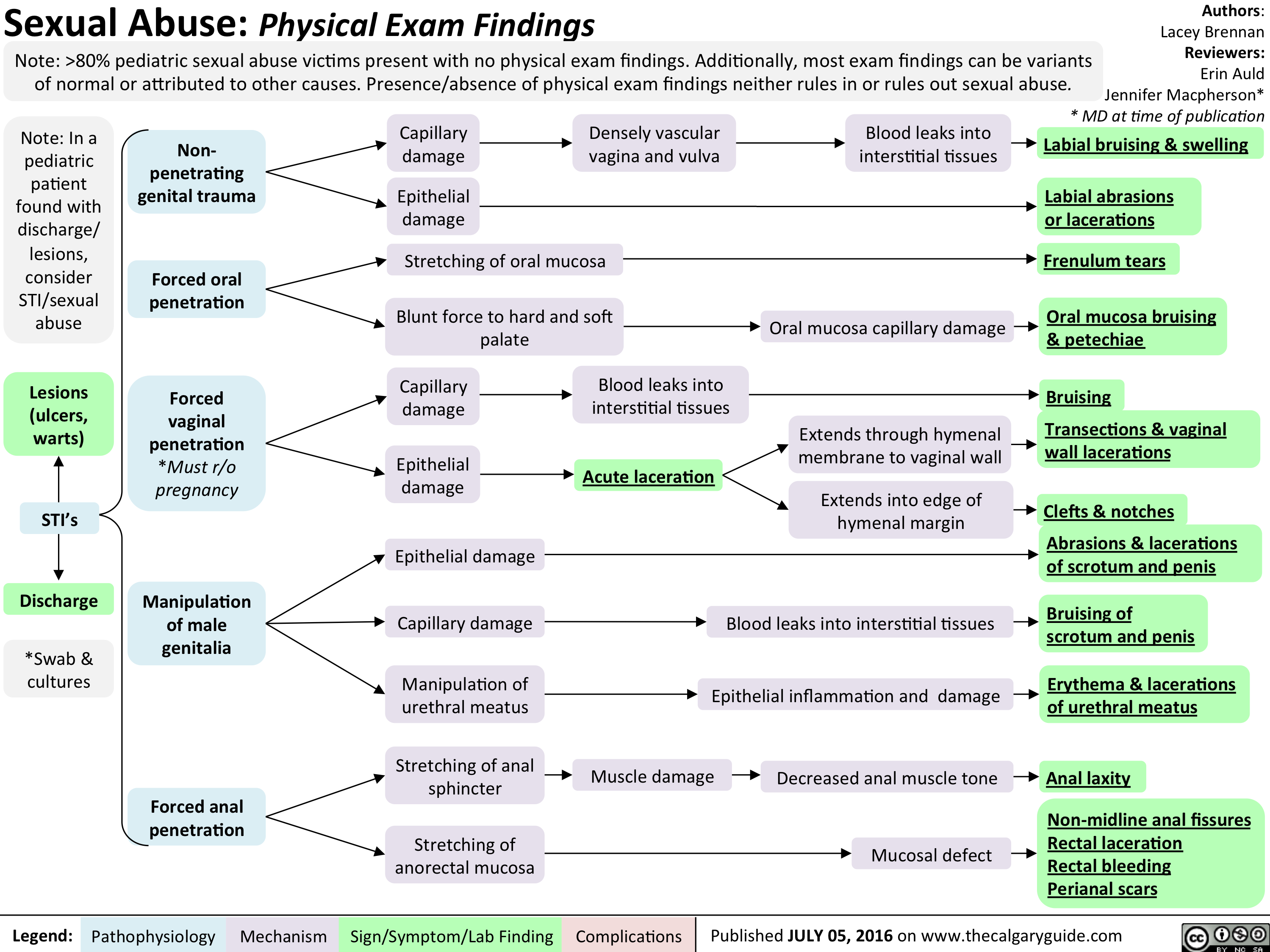
Peds Sexual Abuse
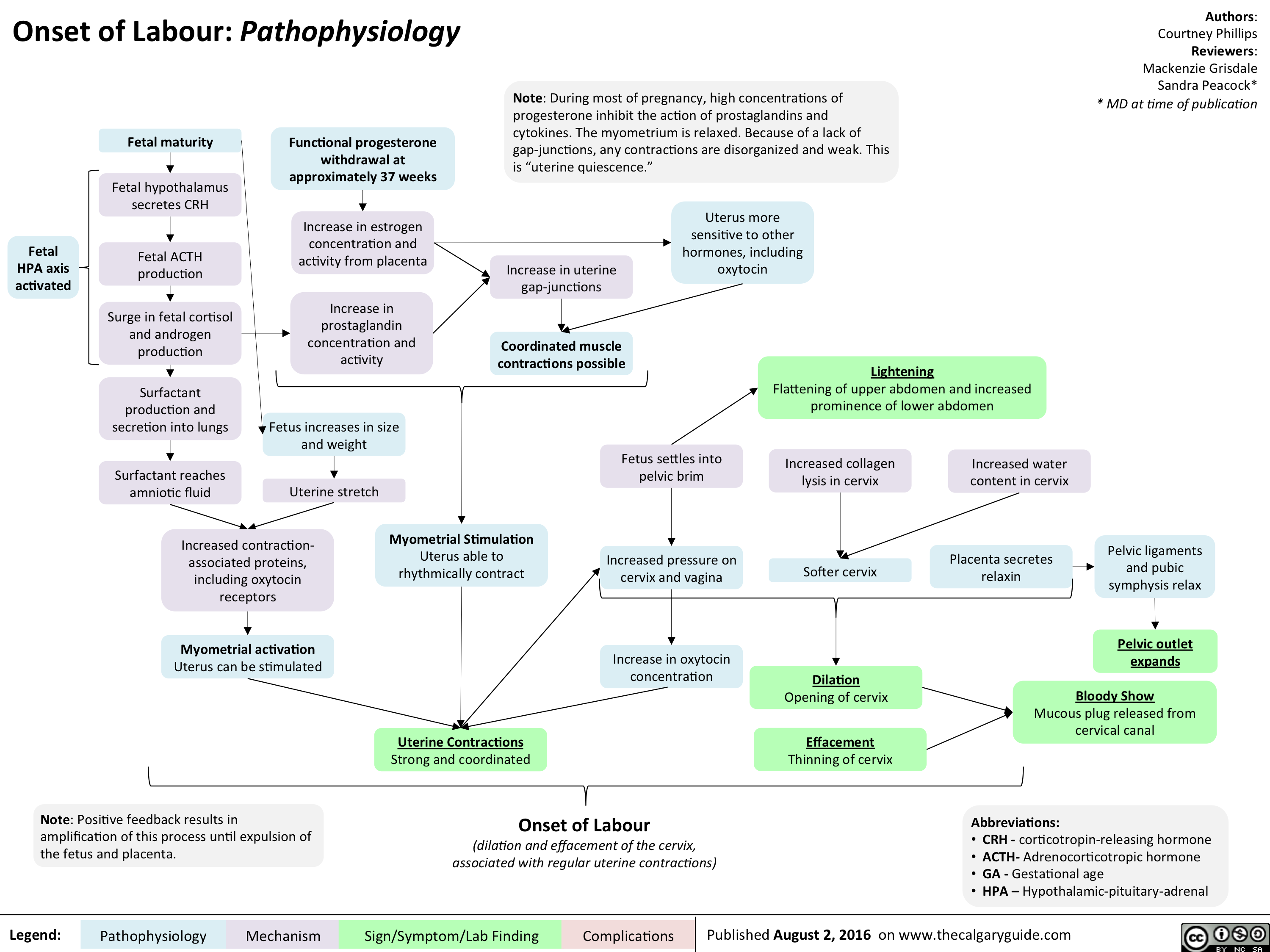
Onset of Labour- Pathophysiology
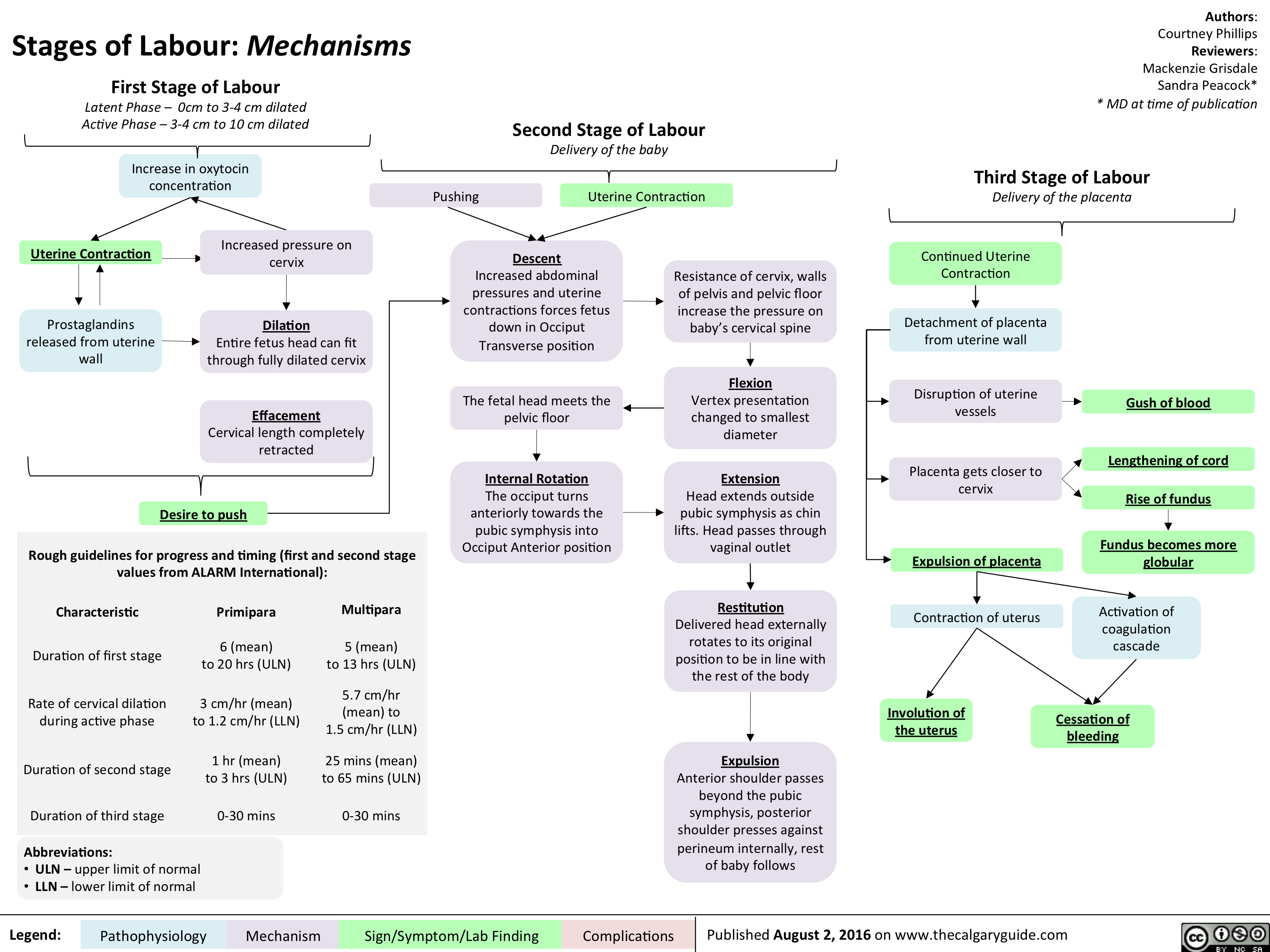
Stages of Labour- Mechanisms
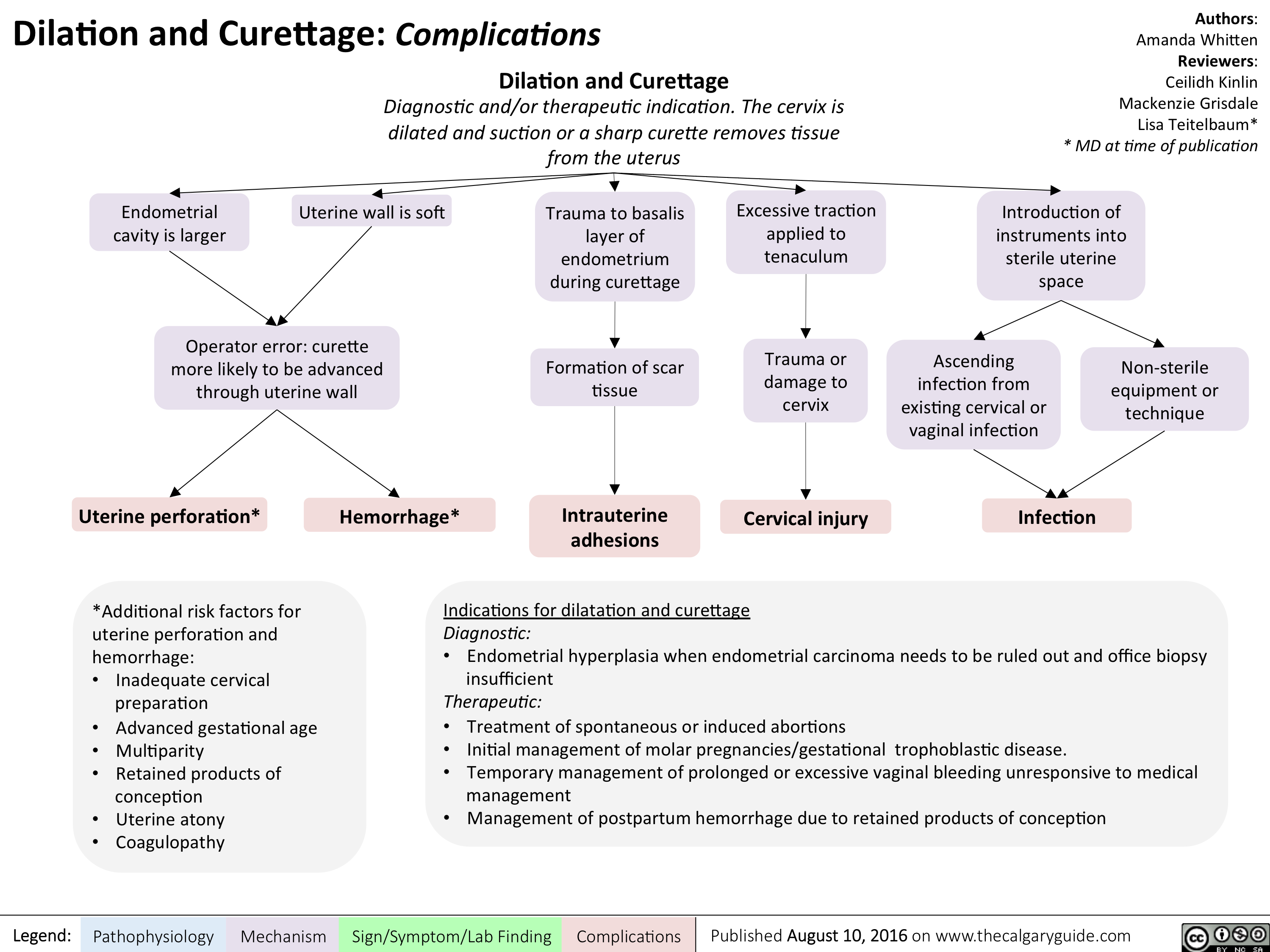
Dilatation and Curettage - Complications
myasthenia-gravis-final

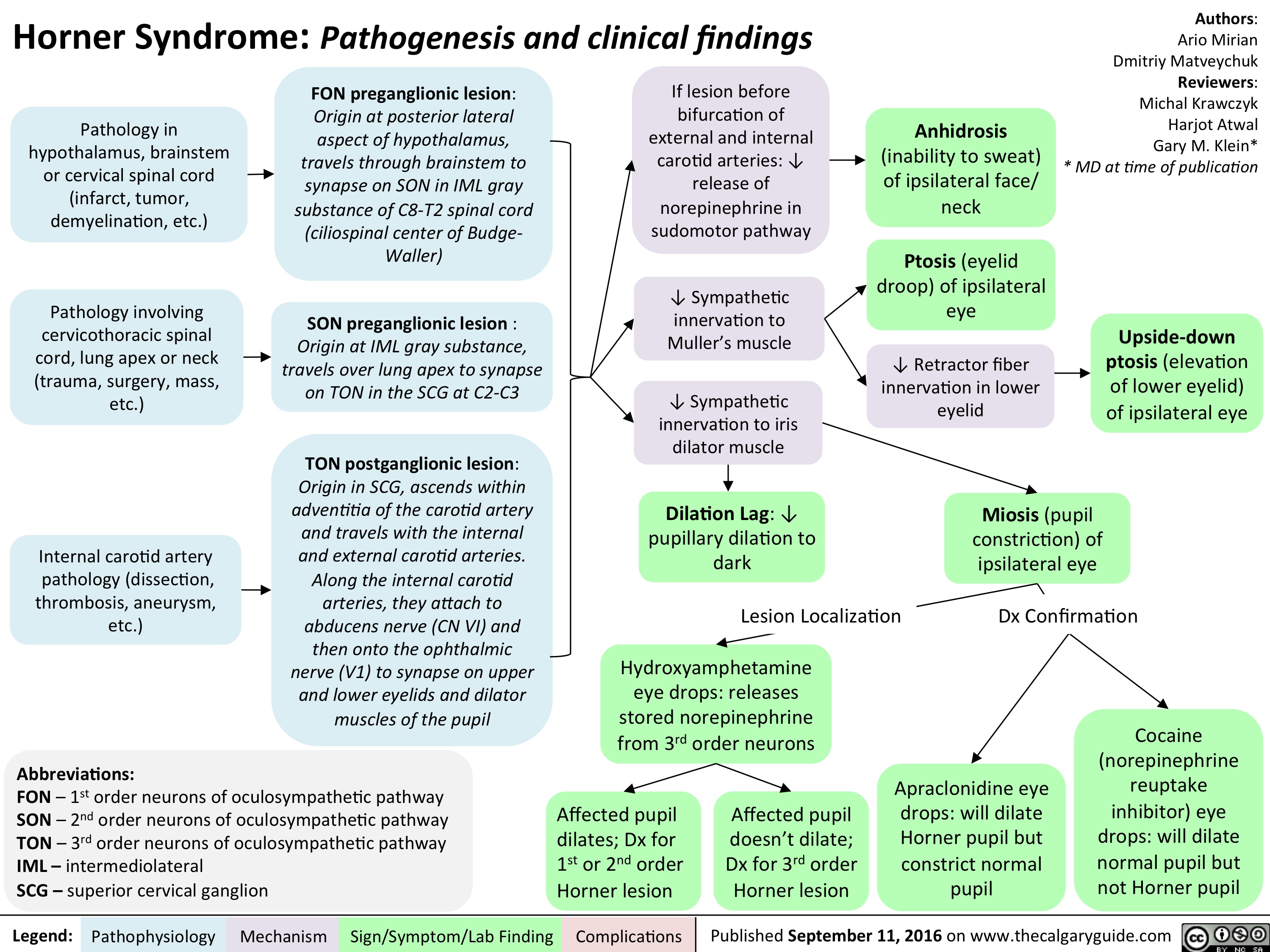
horner-syndrome
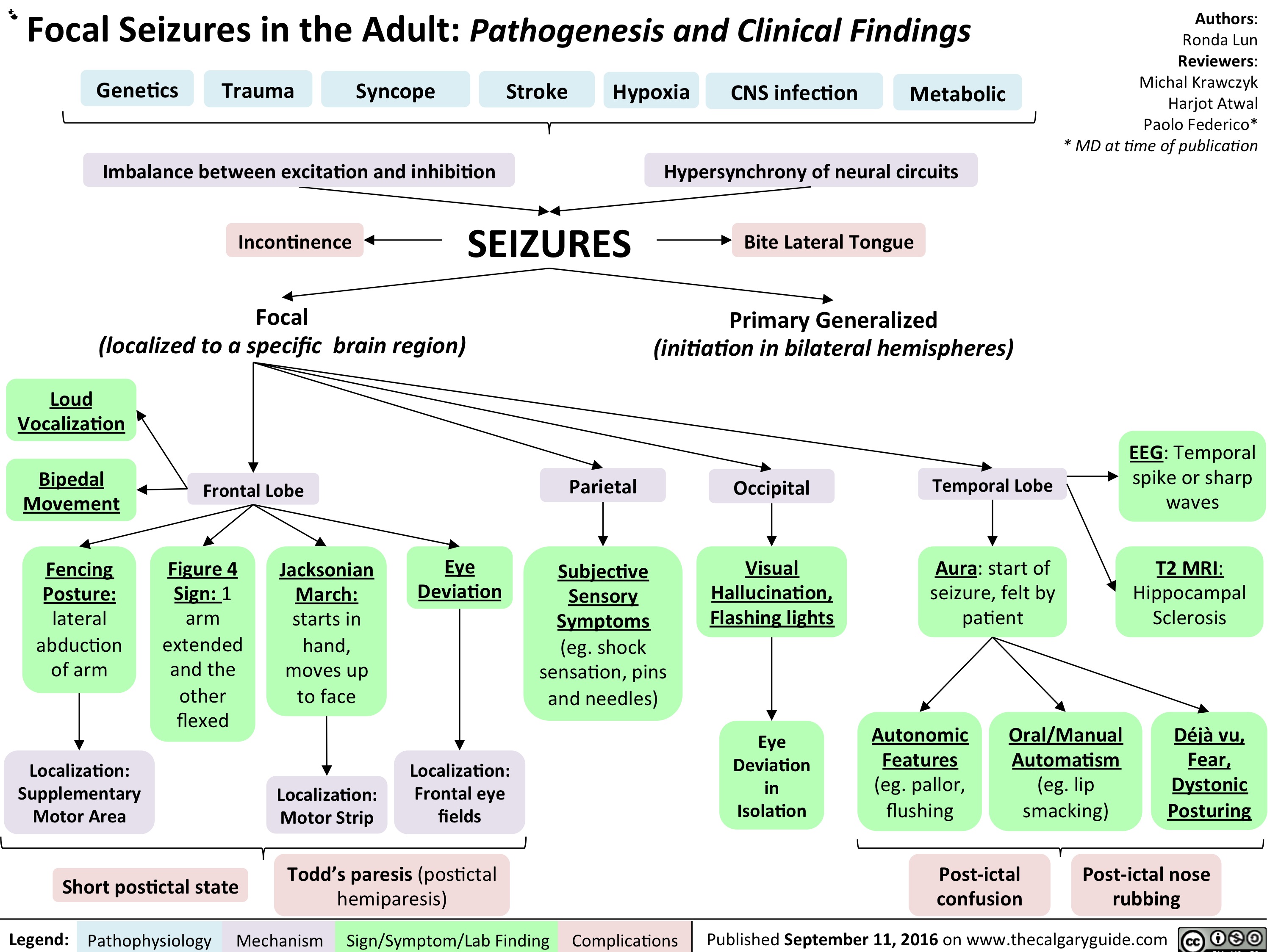
Focal Seizures in the adult: Pathogenesis and Clinical Findings
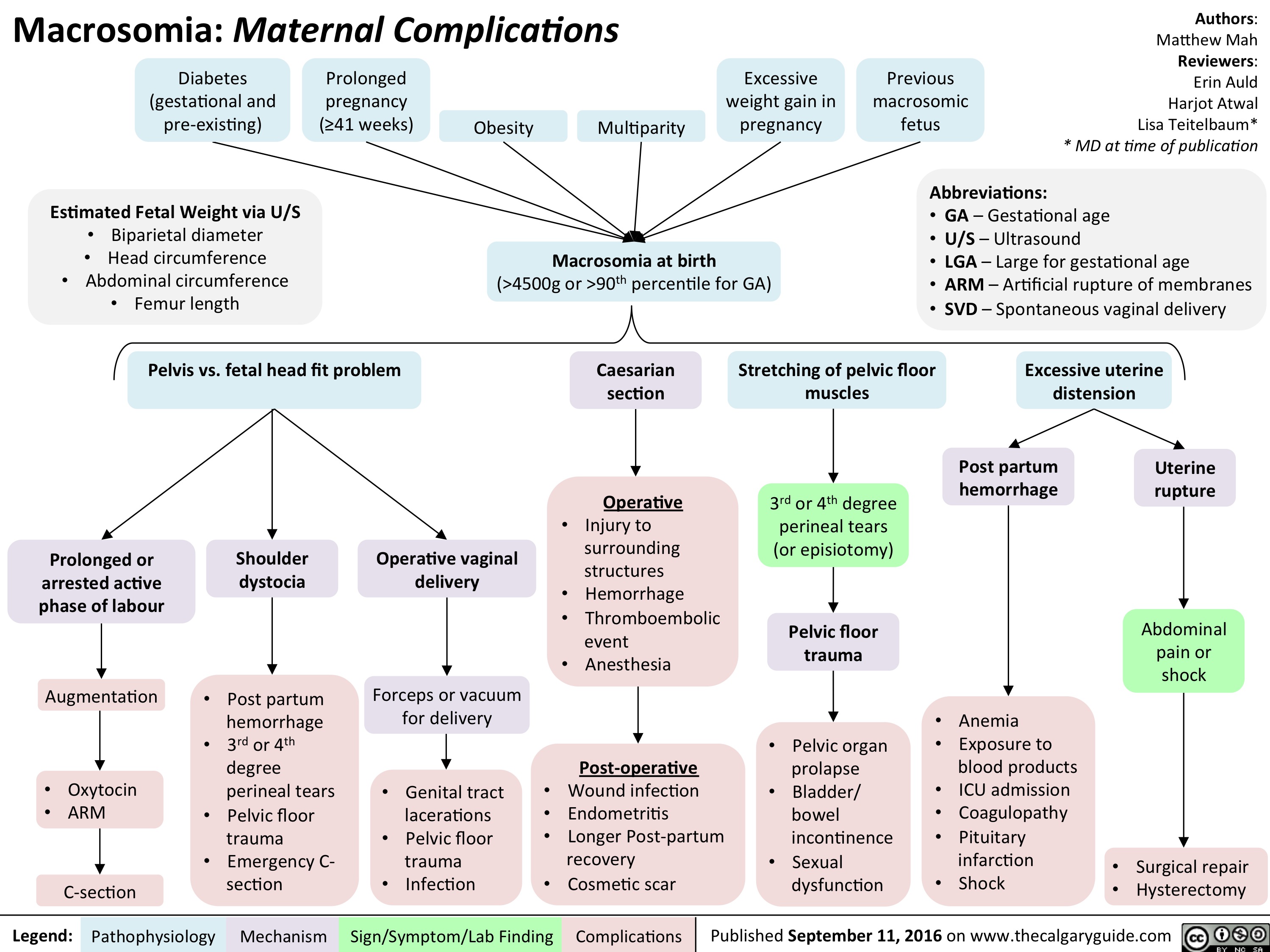
Macrosomia: Maternal Complications
Pediatric Uncompensated Shock: pathogenesis and clinical findings

Type 1 Respiratory Distress Syndrome

acute-closed-angle-glaucoma

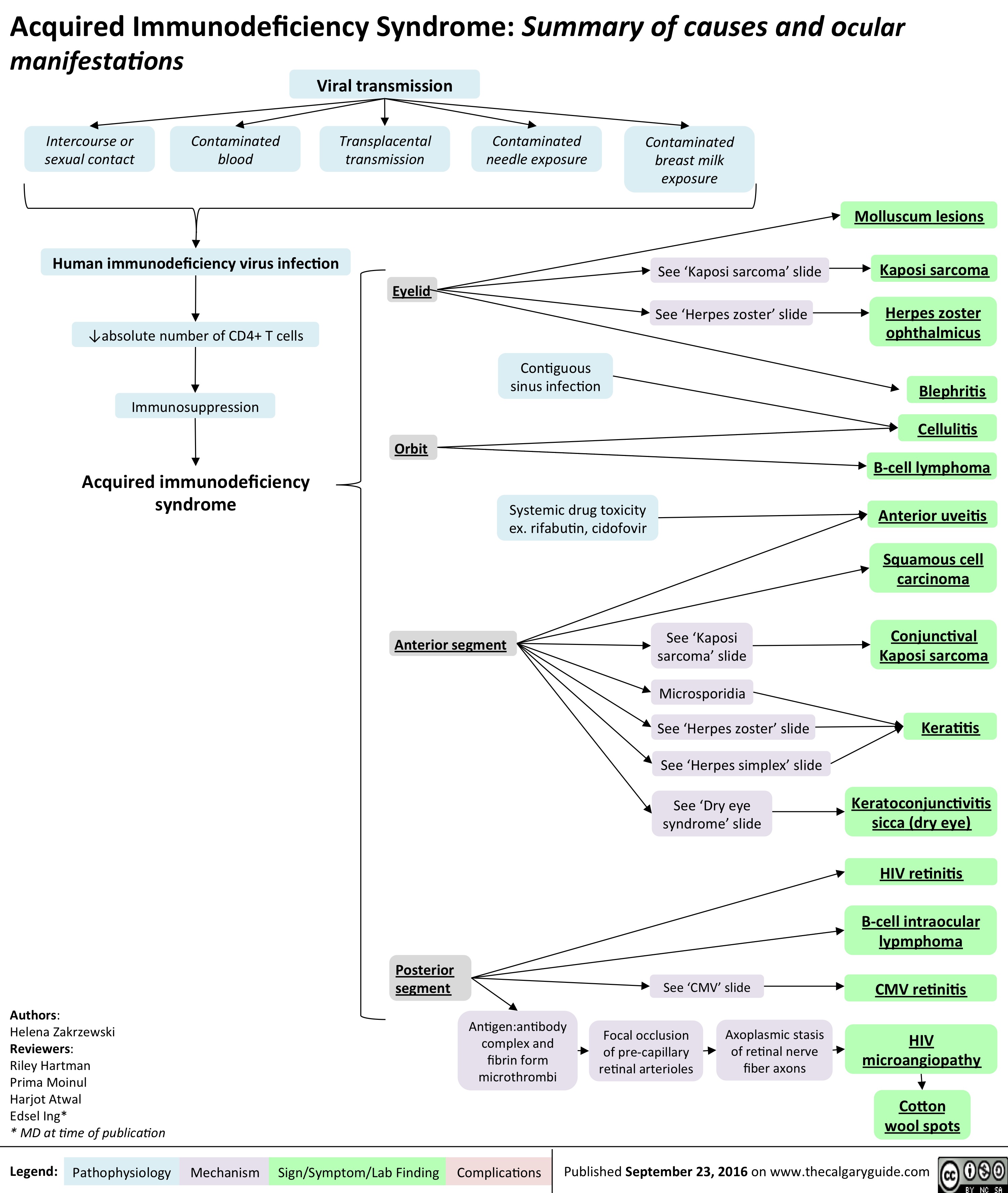
aids-and-cmv-retinitis
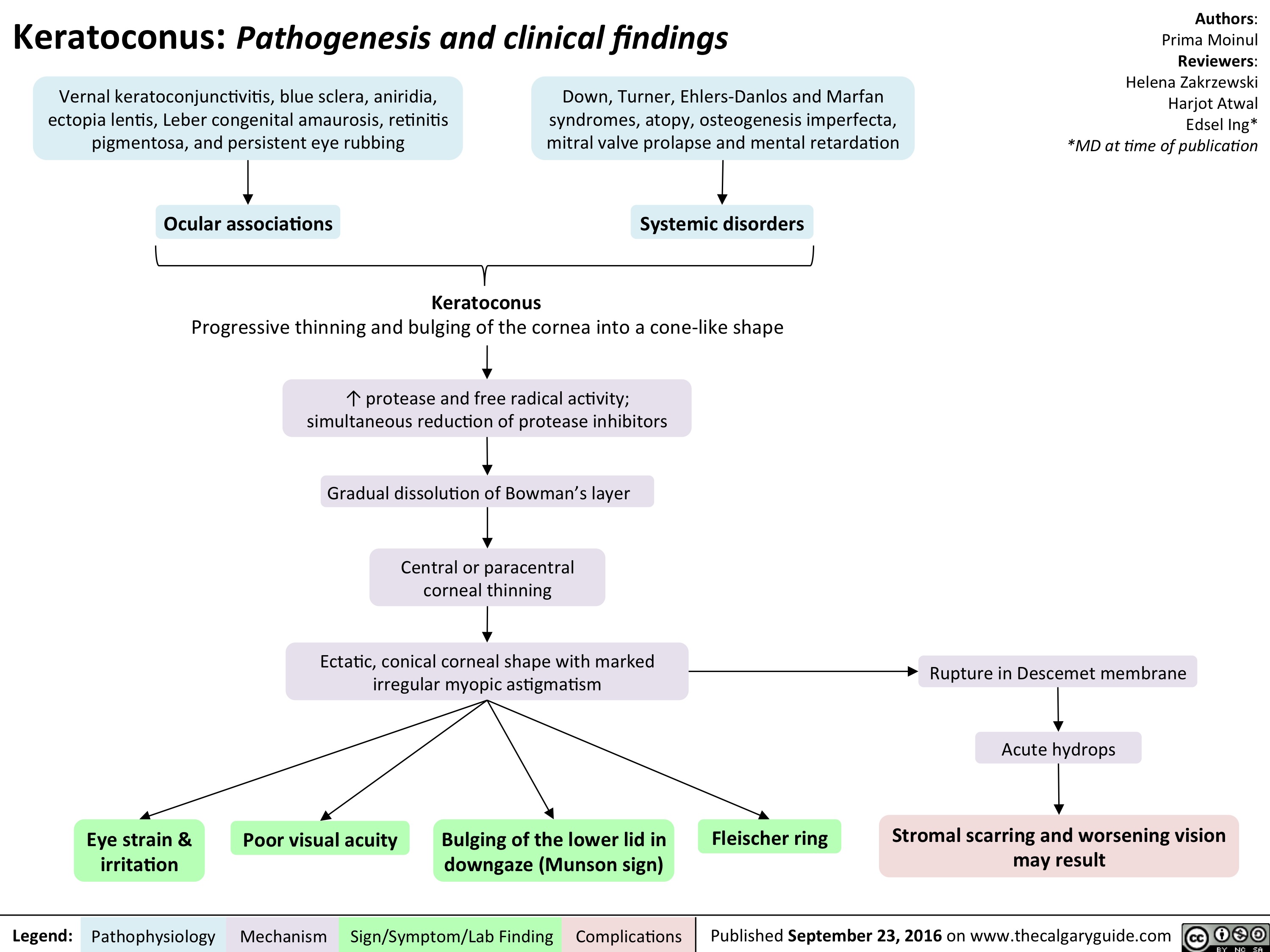
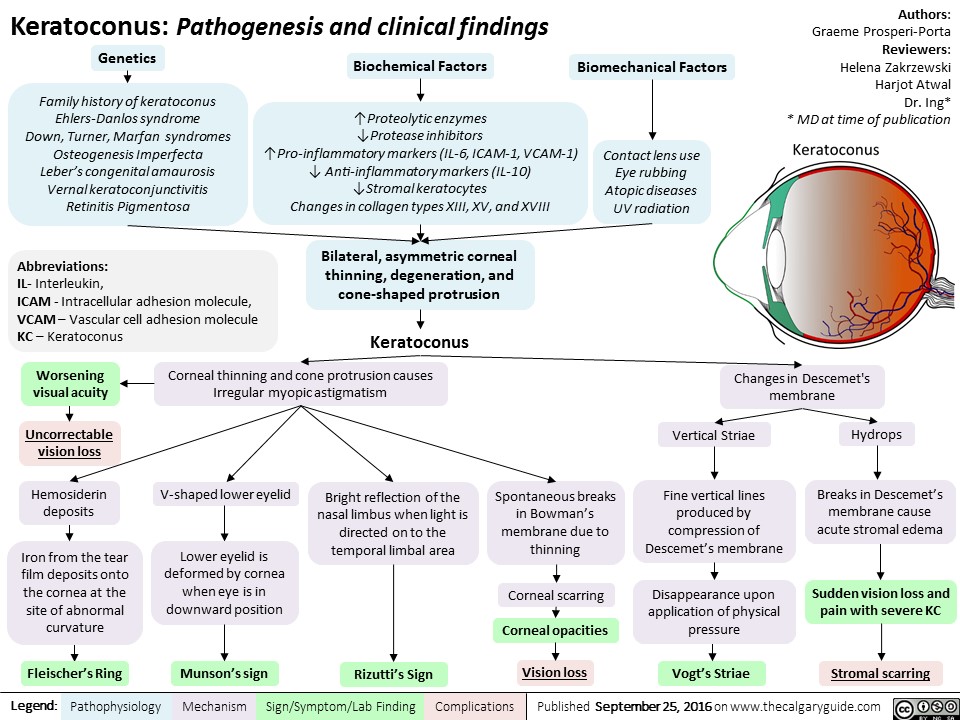
keratoconus
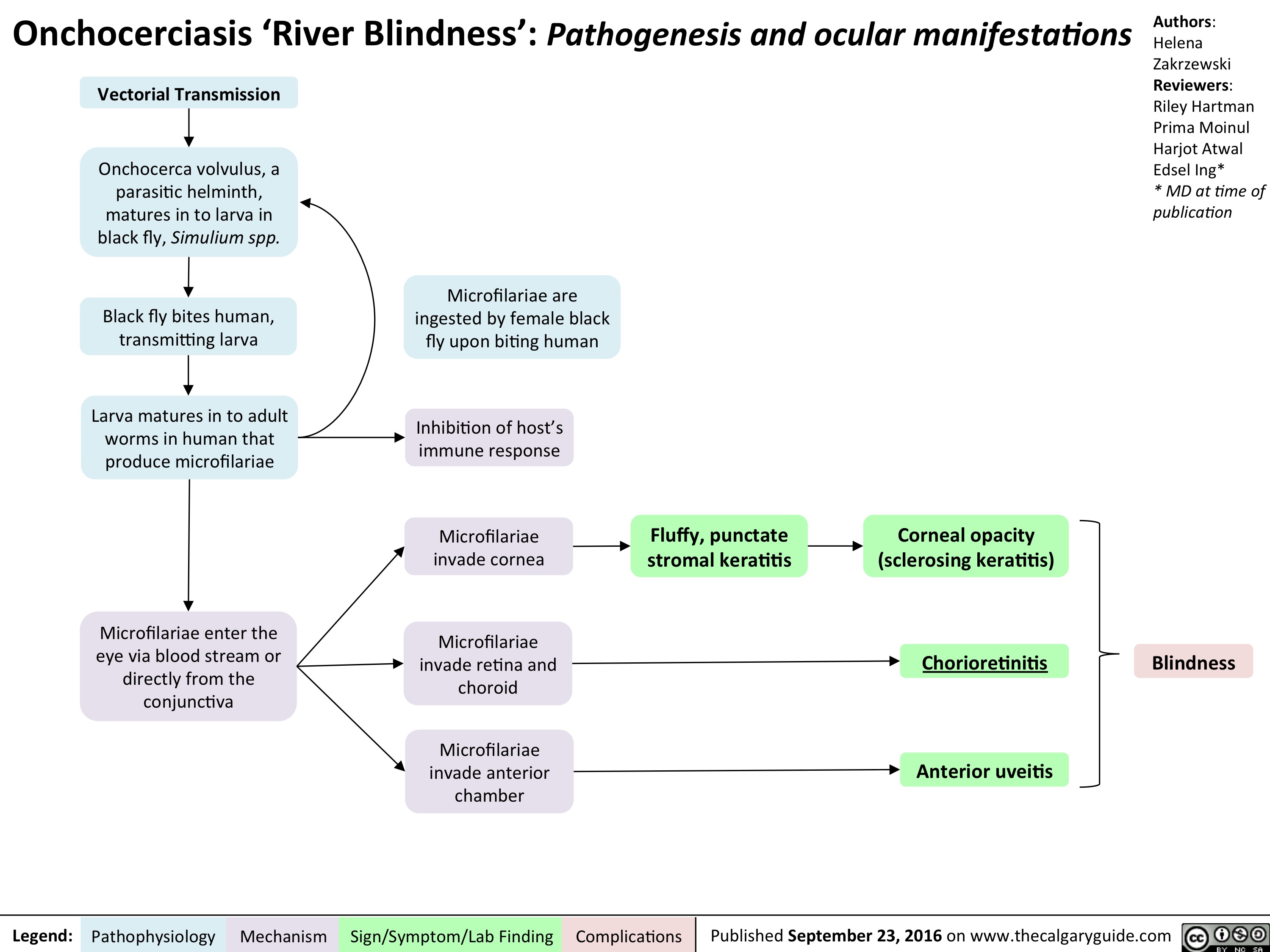
onchocerciasis
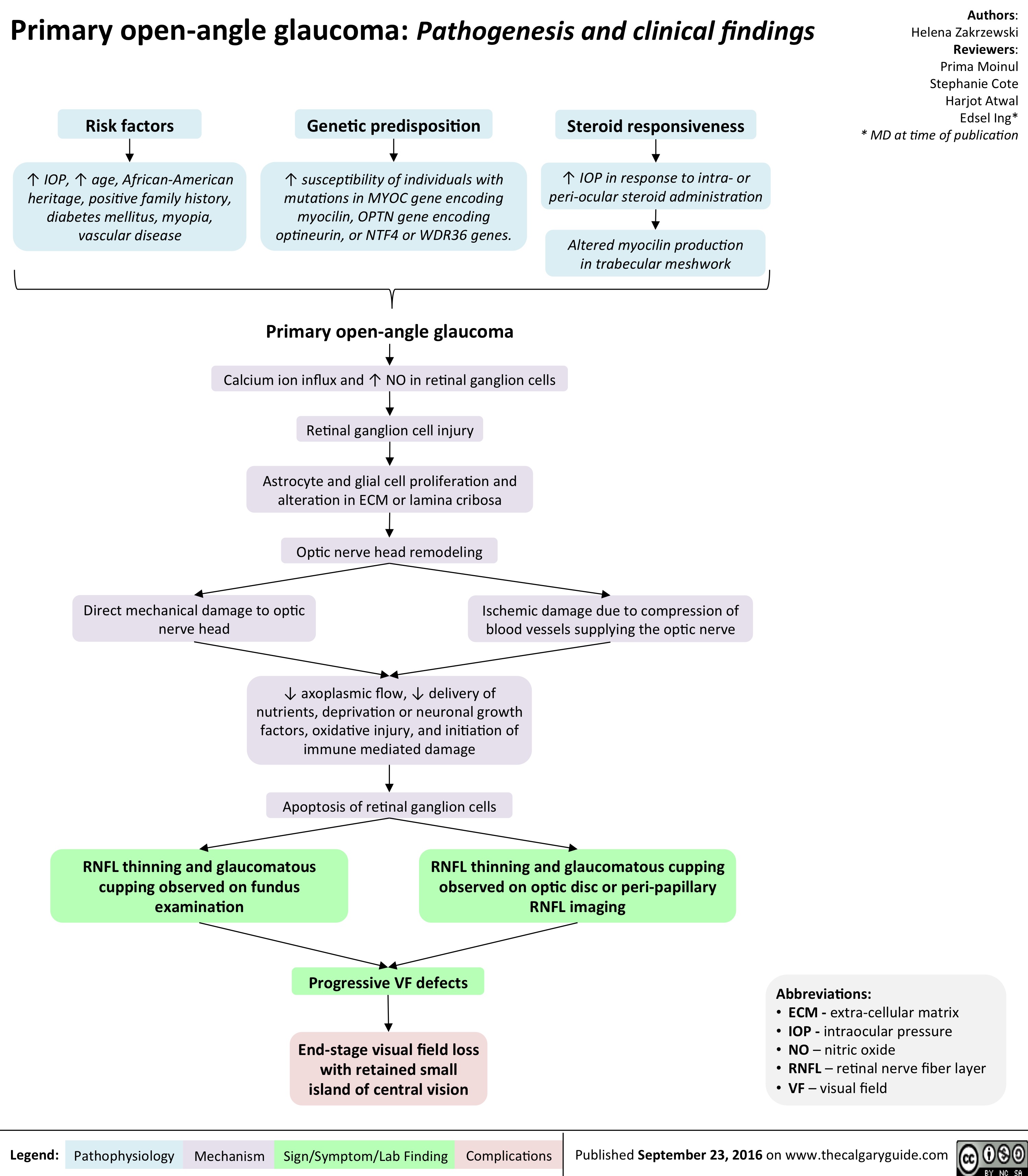
primary-open-angle-glaucoma
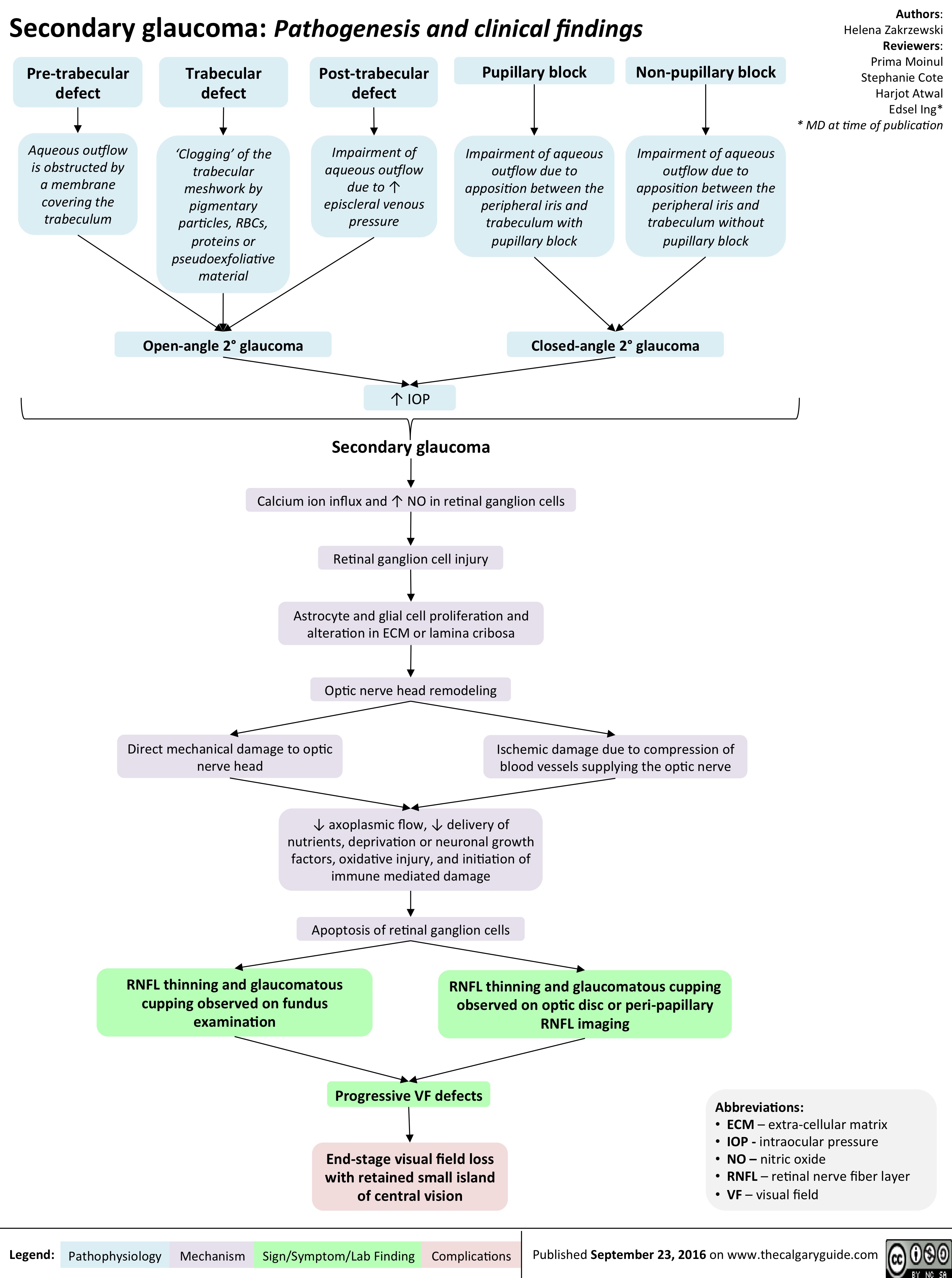
secondary-glaucoma
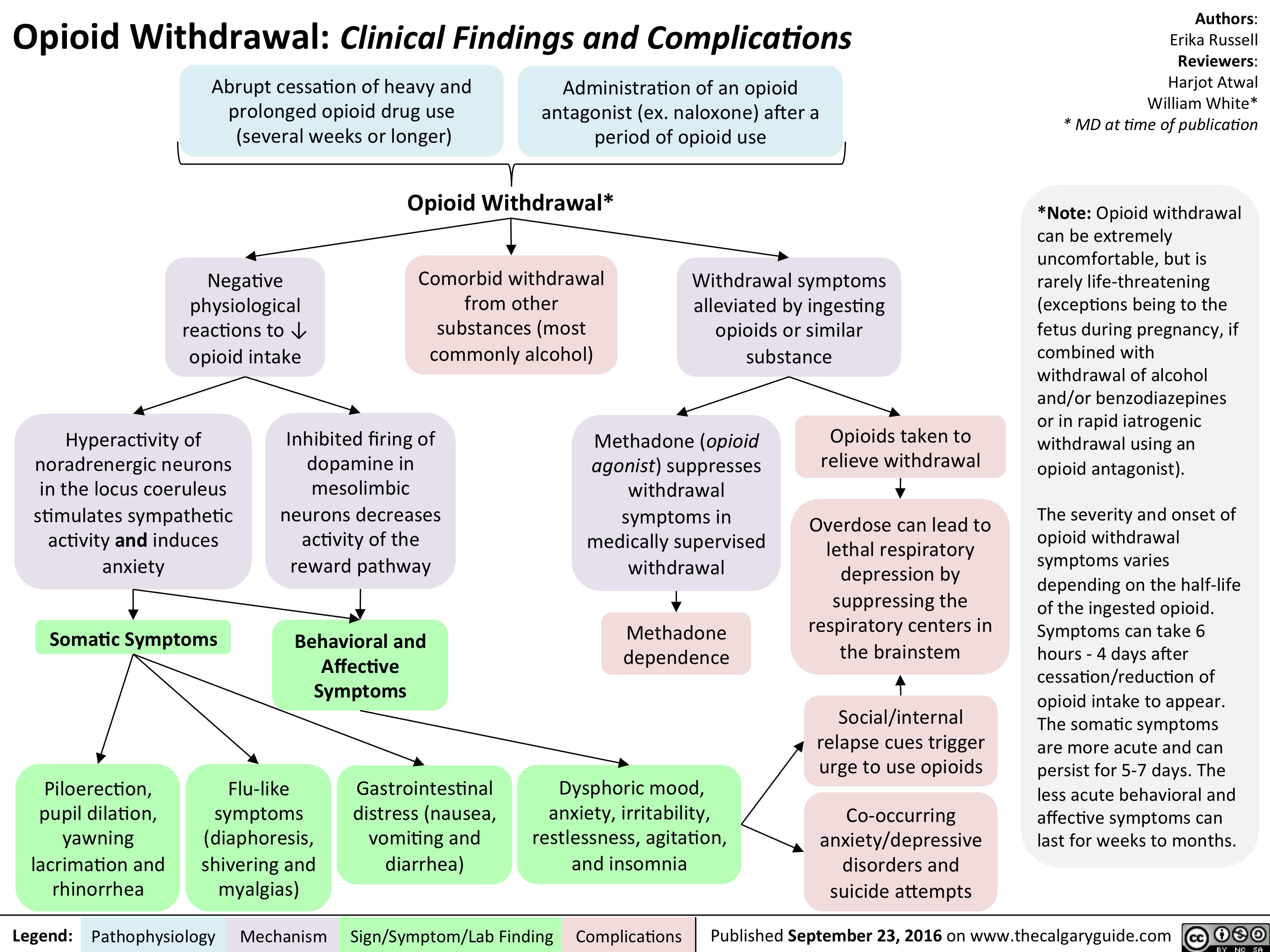
opioid-withdrawal
keratoconus
slide1
slide1
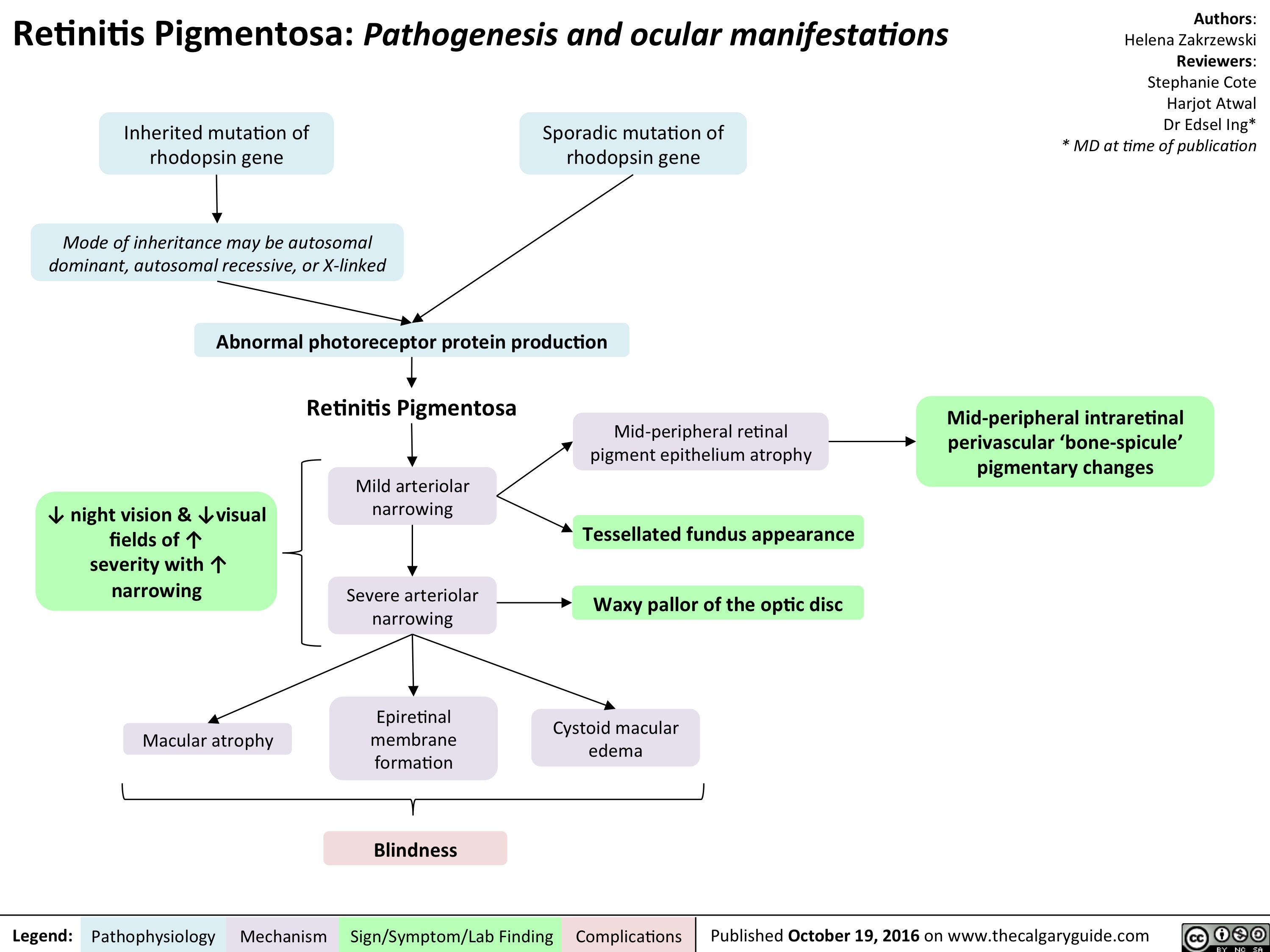
retinitis-pigmentosa-final
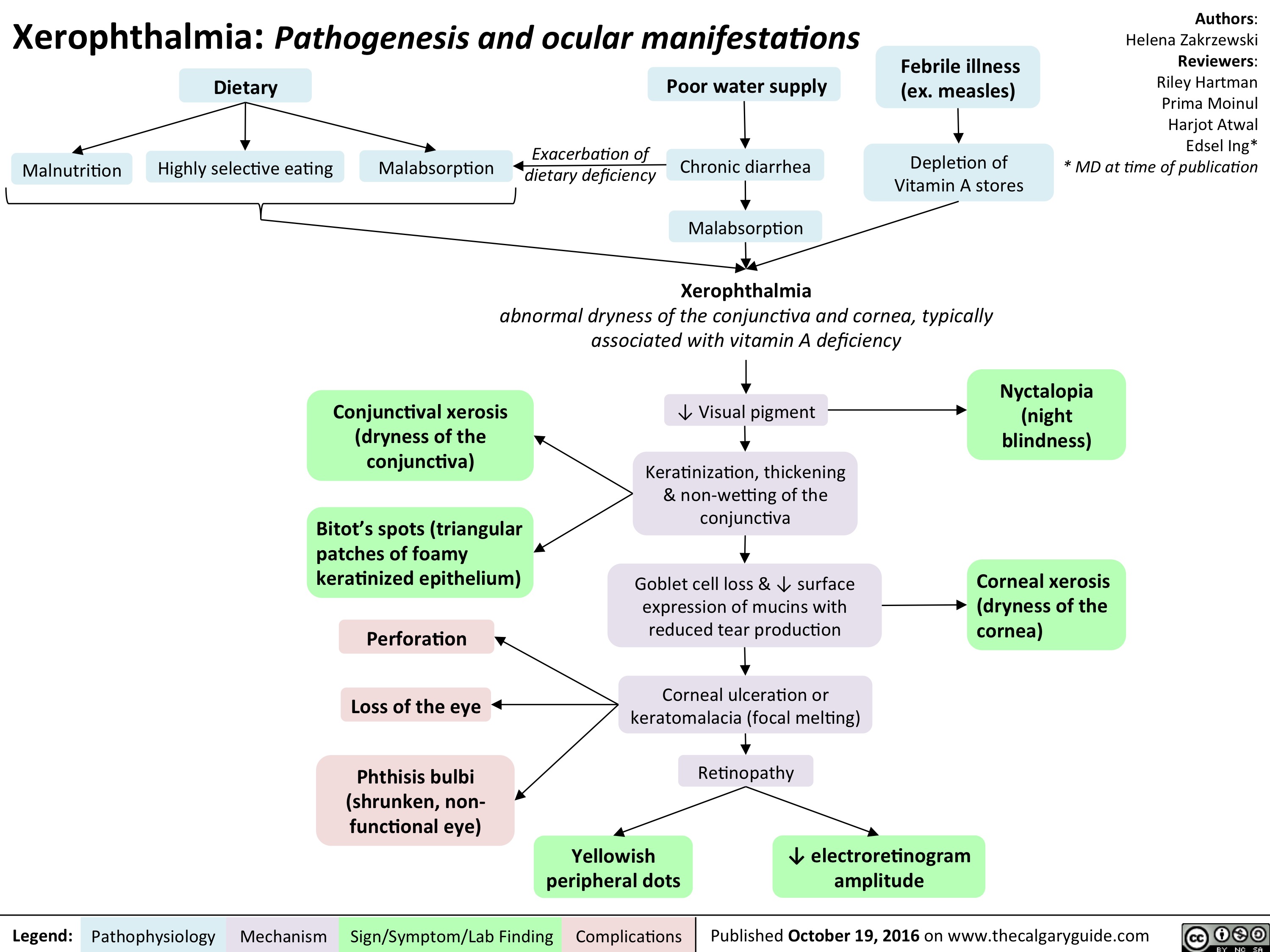
xerophthalmia-final
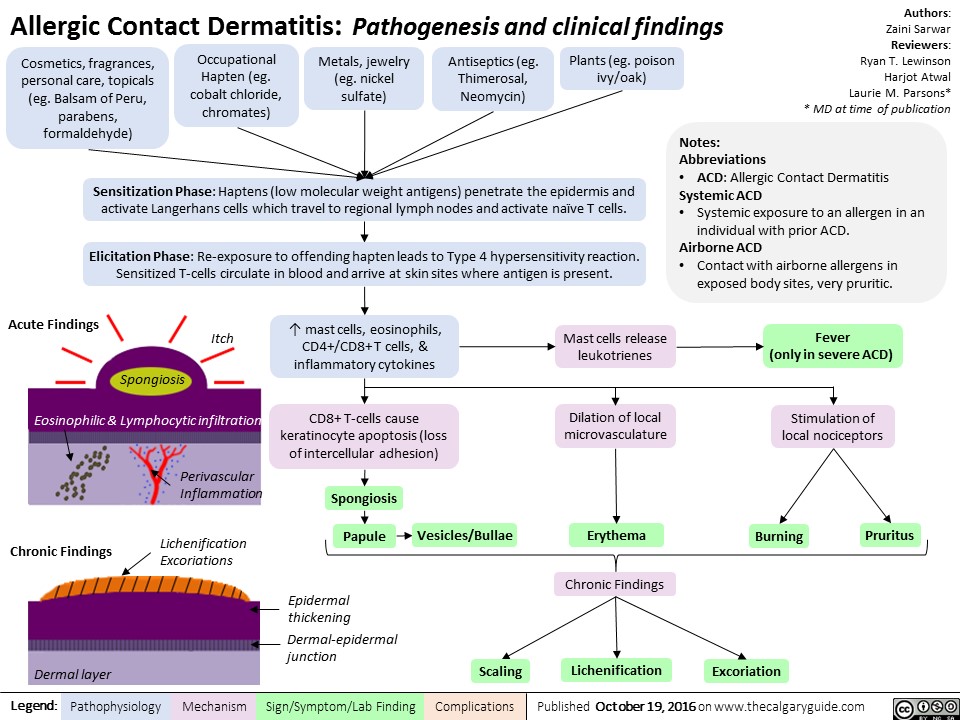
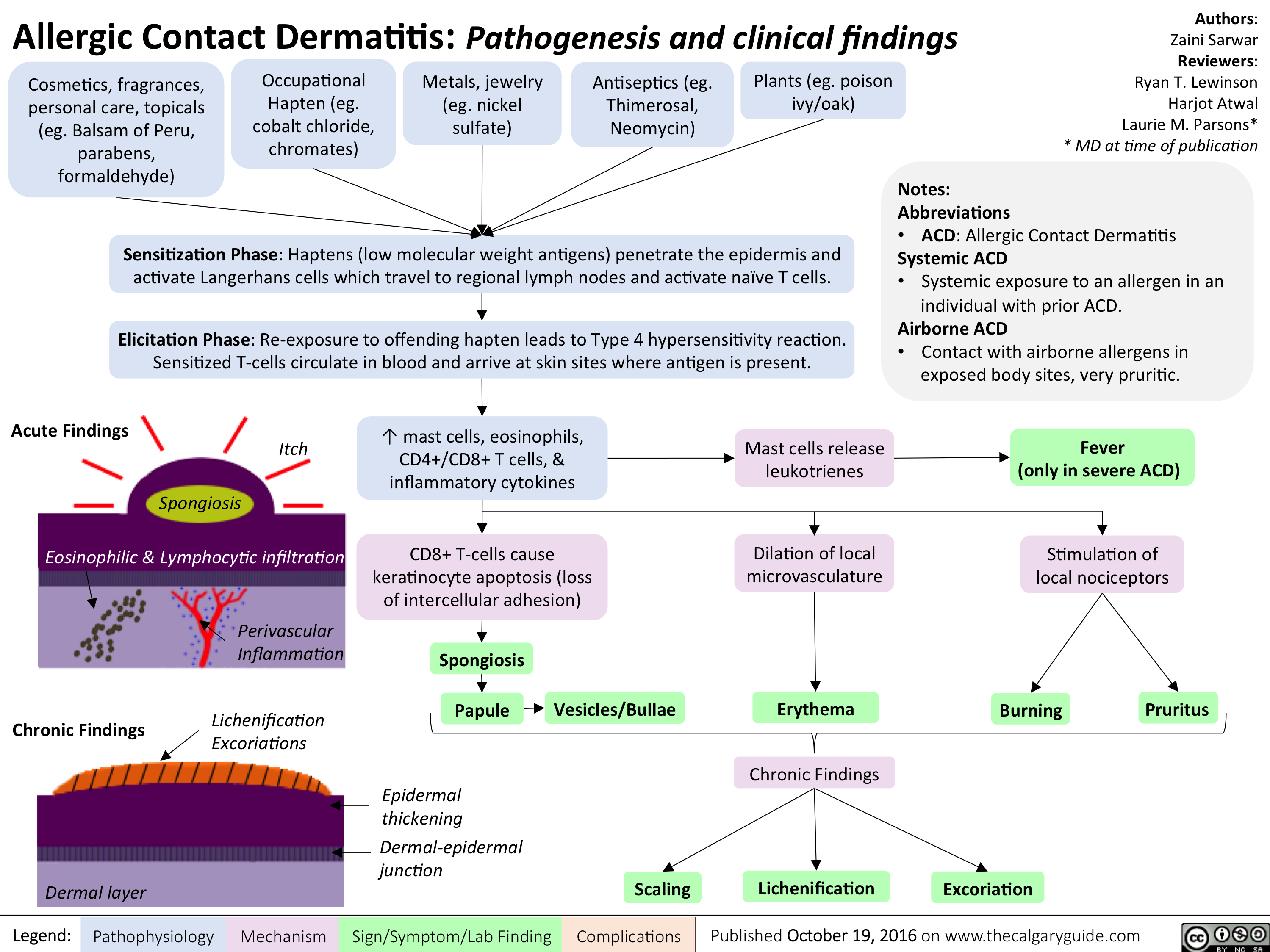
allergic-contact-dermatitis
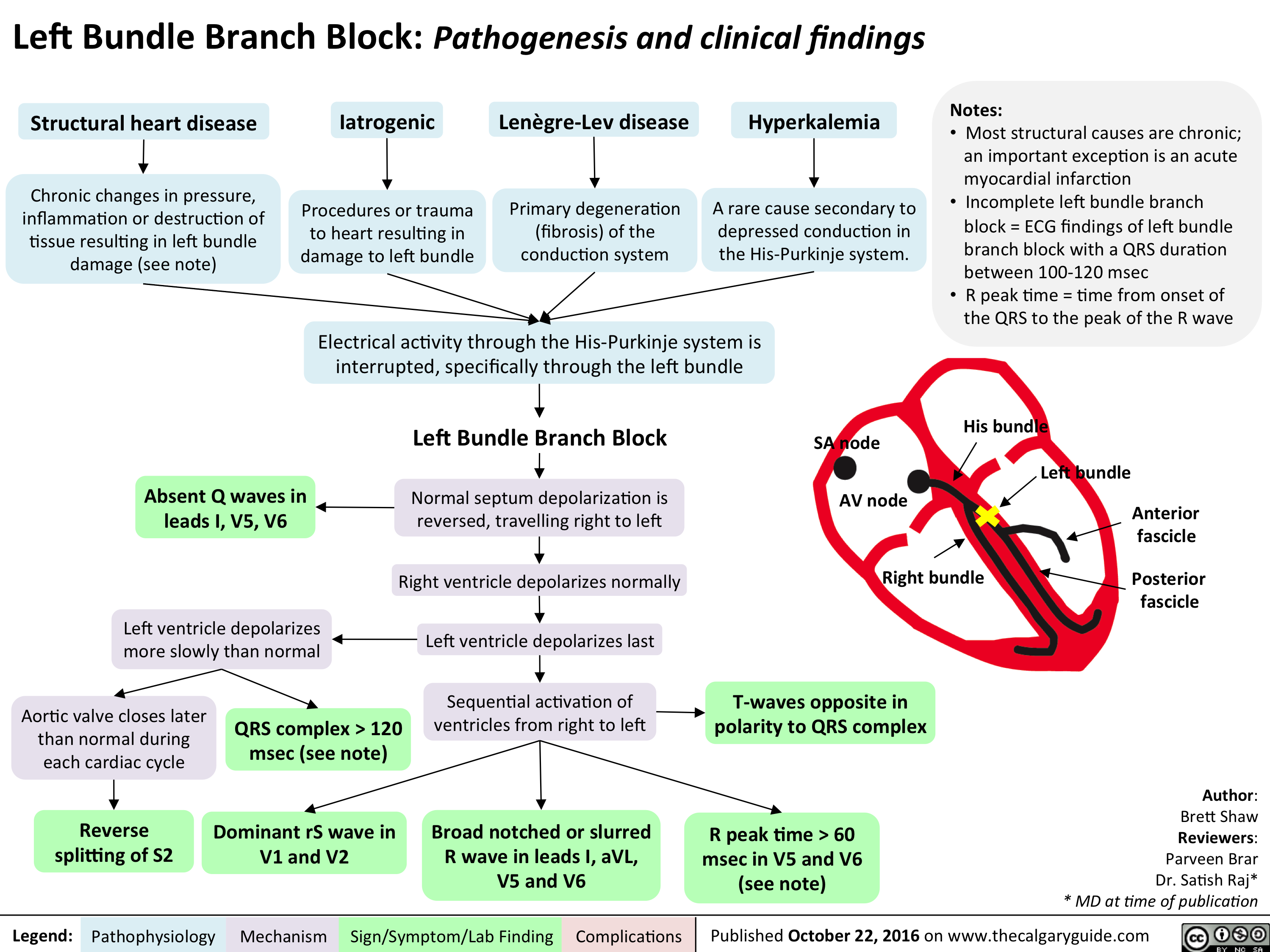
cardio_lbbb_oct-15
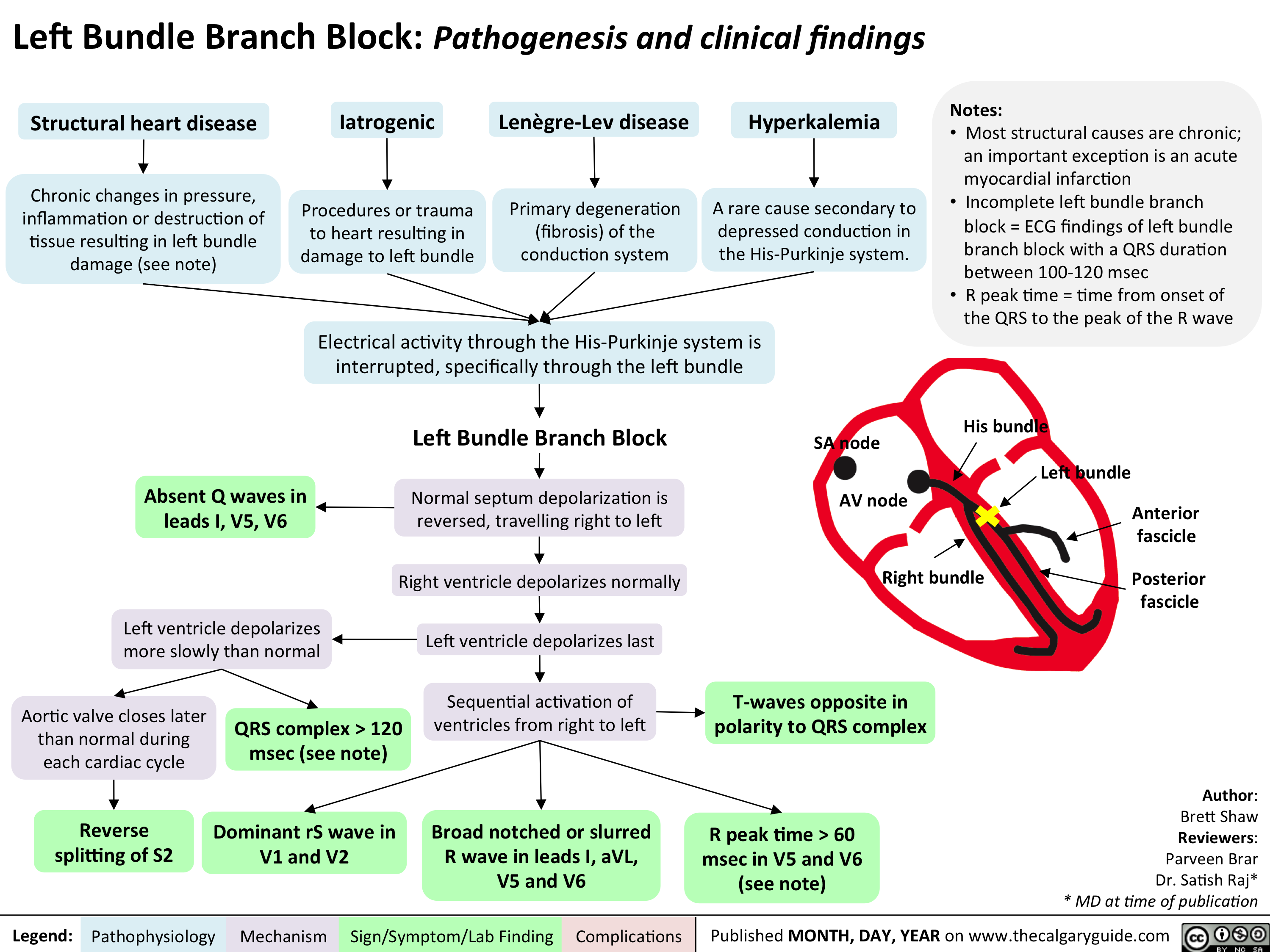
cardio_lbbb_oct-15
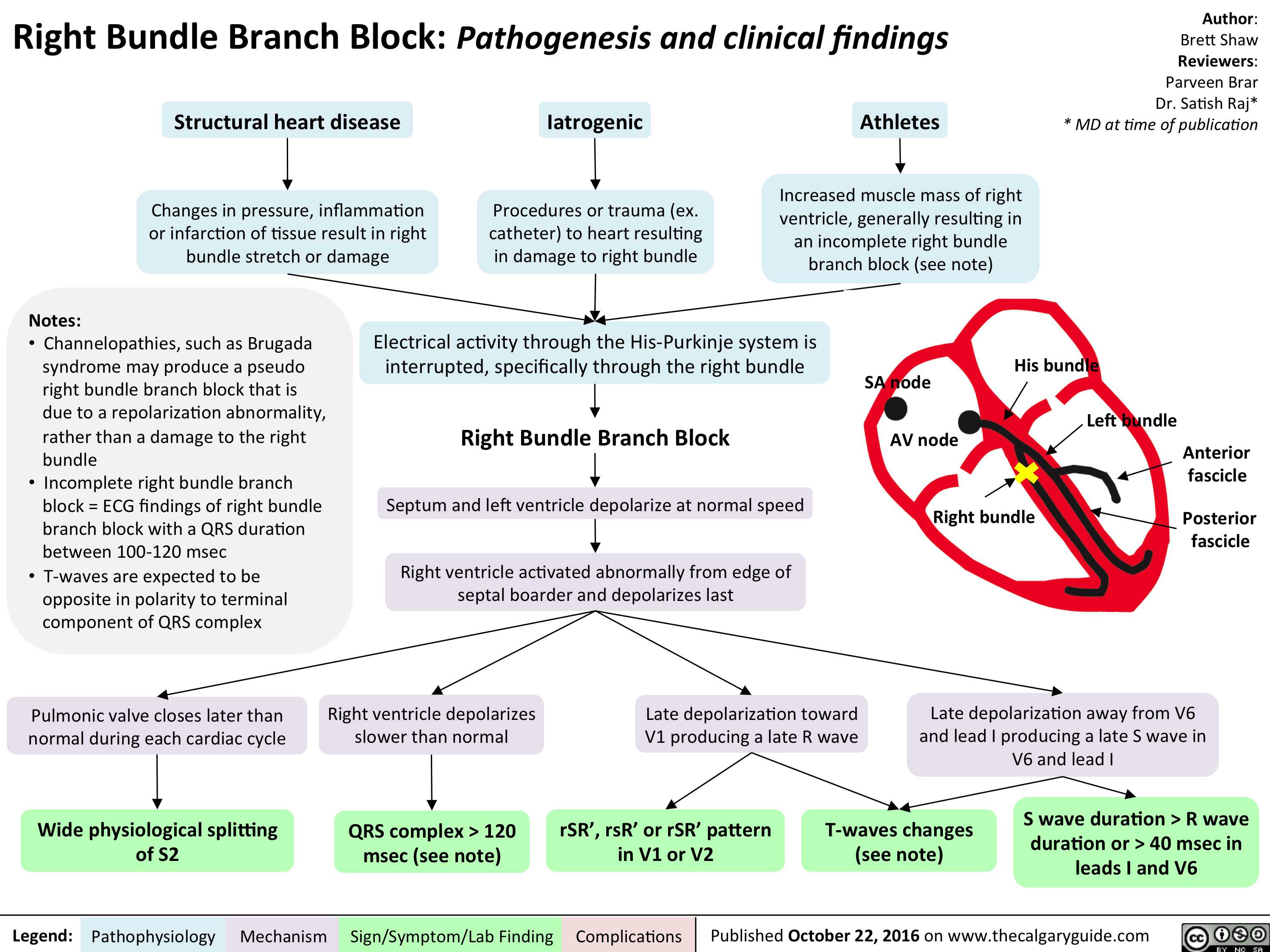
cardio_rbbb_oct-15
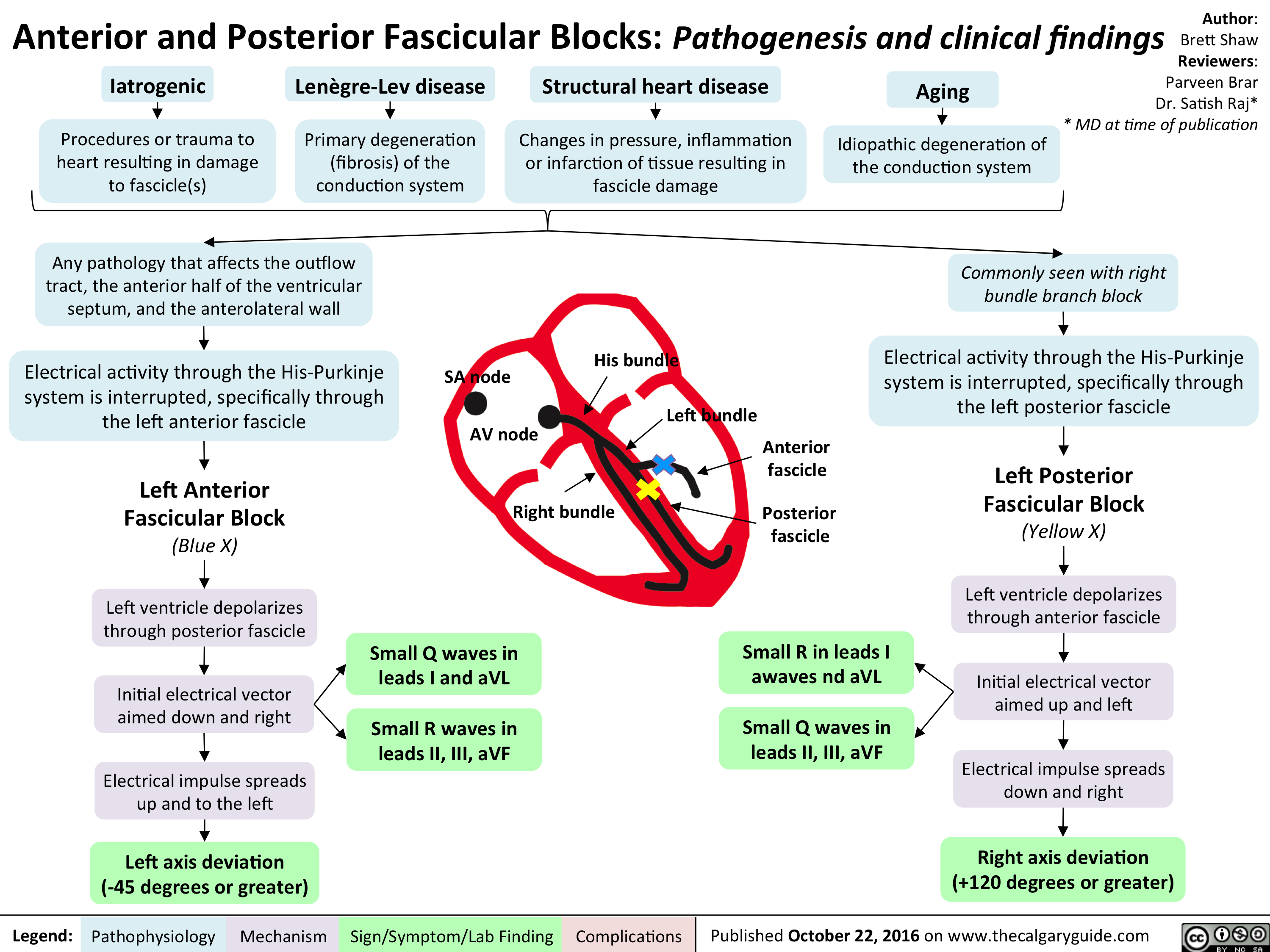
cardio_ant-and-post-fascicular-blocks_oct-15
allergic-contact-dermatitis
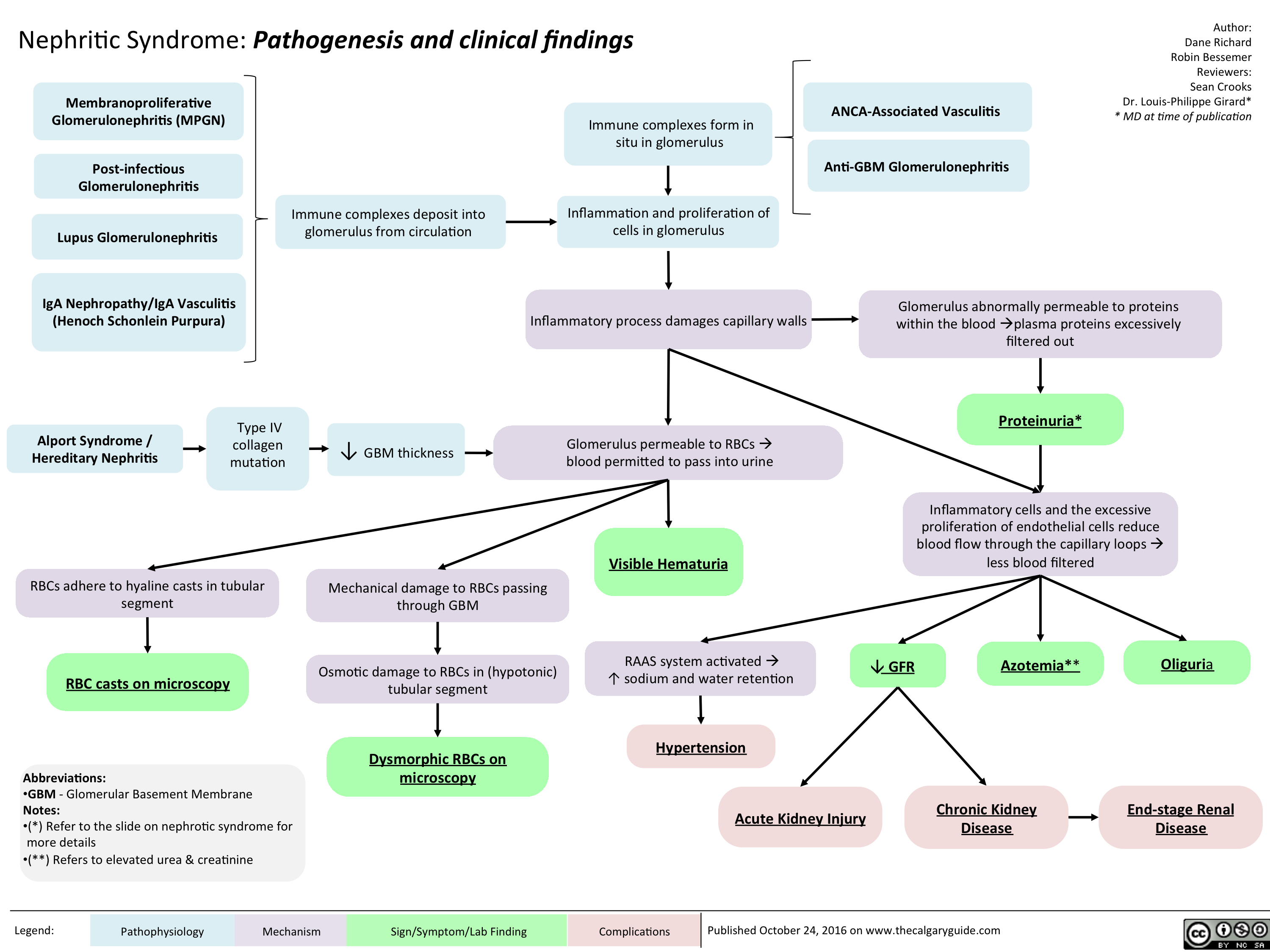
Nephritic Syndrome: Pathogenesis and clinical findings
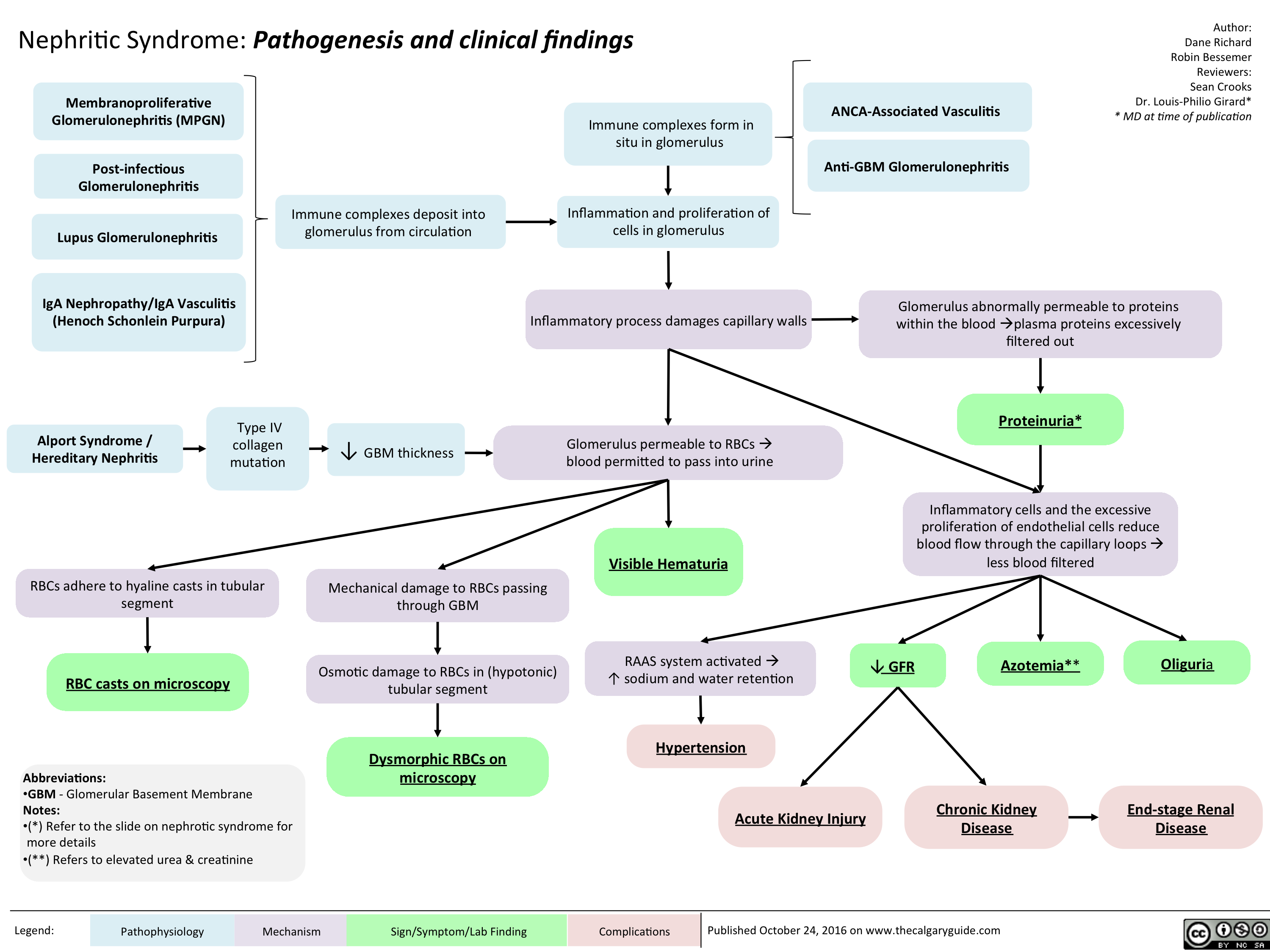
nephritic-syndrome
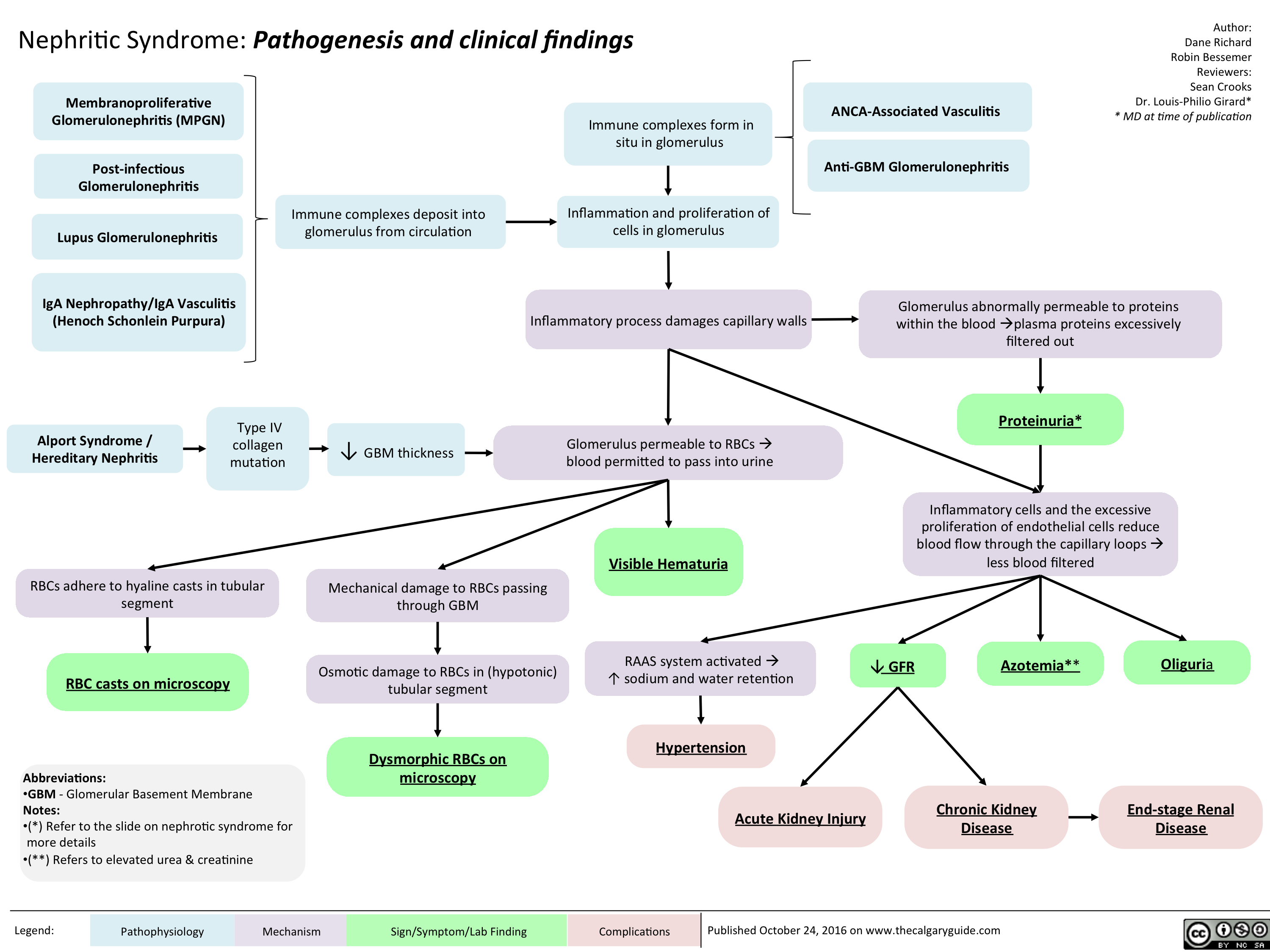
nephritic
Opioid Receptor Agonists
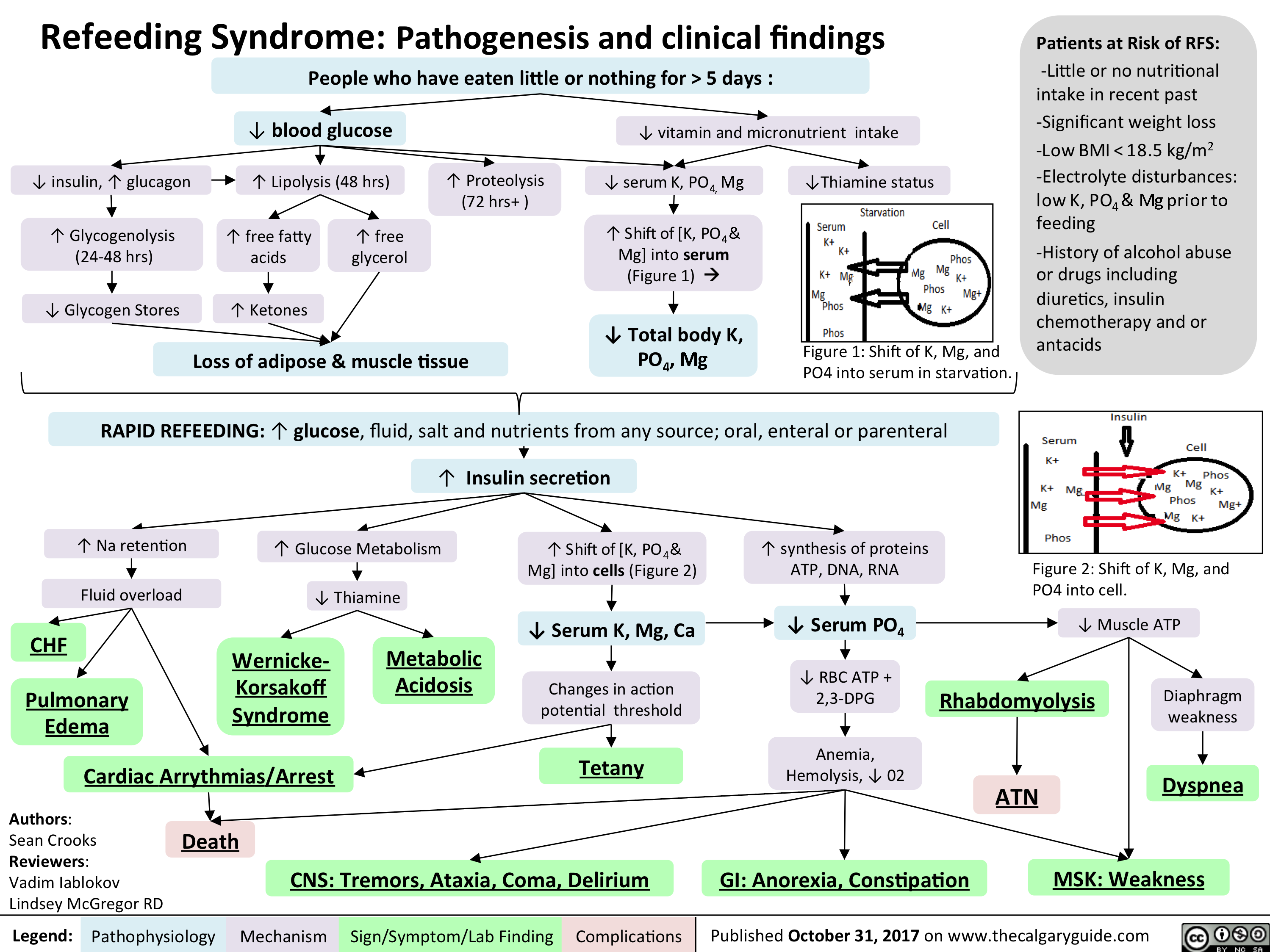
refeeding syndrome
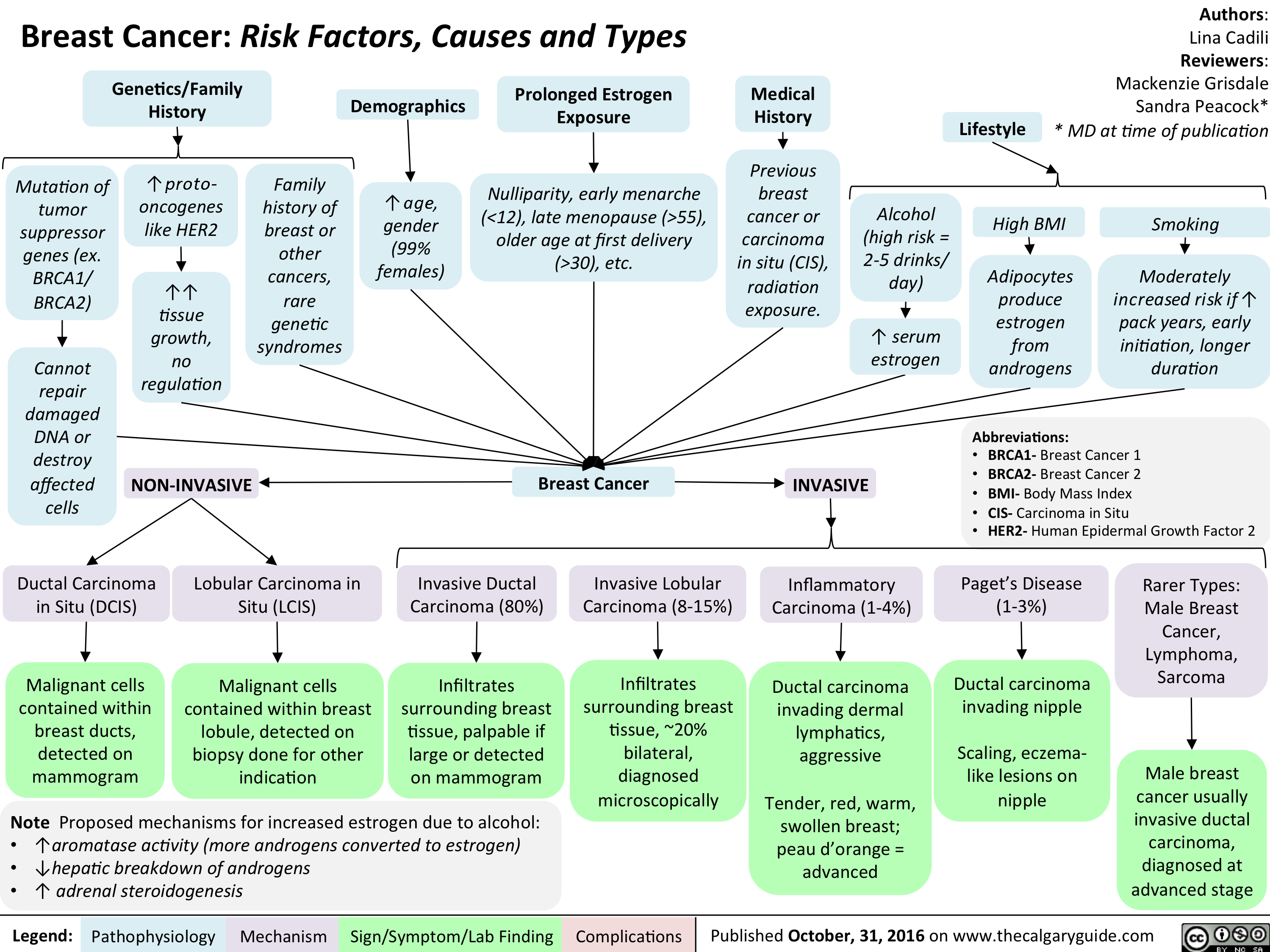
Breast Cancer Risk Factors Causes and Types
Hyperosmolar Hyperglycemic State
![Hyperosmolar Hyperglycemic State (HHS)
Note: HHS is only seen in Type II DM patients!
Note: In patients with either DKA or HHS, always look for an underlying cause (i.e. an infection)
Author: Yan Yu Reviewers:
Peter Vetere
Gill Goobie
Hanan Bassyouni* * MD at time of publication
Alters total body water & ion osmosis
Inadequate insulin production, insulin resistance, non- adherence to insulin Tx
Relative Insulin deficit
Stresses that ↑ Insulin demand: infections, pneumonia, MI, pancreatitis, etc)
Hyperglycemia
(Very high blood [glucose], higher than in DKA)
When blood [glucose] > 12mmol/L, glucose filtration > reabsorption, ↑ urine [glucose]
Glucosuria
Glucose in filtrate promotes osmotic diuresis: large- volume urine output
Polyuria
Dehydration
(↓ JVP, orthostasis: postural hypotension/ postural tachycardia, ↑ resting HR)
Some insulin still present, but not enoughsome glucose is utilized by muscle/fat cells, some remain in the blood
Cells not “starved”, but still need more energy
↑ release of Catabolic hormones: Glucagon, Epinephrine, Cortisol, GH
Body tries to ↑ blood [glucose], to hopefully ↑ cell glucose absorption
Hypothalamic cells sense low intra-cellular glucose, triggering feelings of hunger
Polyphagia
Note: the presence of some insulin directly inhibits lipolysis; thus, in HHS there is no ketone body production, and no subsequent metabolic acidosis and ketouria (unlike in DKA). If ketones are detected in an HHS patient it’s likely secondary to starvation or other mechanisms.
↓ ECF volume, ↑ ECF osmolarity (i.e. hypernatremia)
↑ Gluconeogenesis ↑ Glycogenolysis (in liver)
↓ Protein synthesis, ↑ proteolysis
(in muscle)
↑ Gluconeogenic substrates for liver If the patient doesn’t drink enough
water to replenish lost blood volume If pt is alert and
Electrolyte imbalance
water is accessible
Water osmotically leaves neurons, shrinking them
Neural damage: delirium, lethargy, seizure, stupor, coma
↓ renal perfusion, ↓ GFR
Renal Failure
(pre-renal cause; see relevant slides)
Polydipsia Note: in HHS, body K+ is lost via osmotic diuresis. But diffusion of K+ out of cells
may cause serum [K+] to be falsely normal/elevated. To prevent hypokalemia, give IV KCl along with IV insulin as soon as serum K+ <5.0mmol/L. But ensure patient has good renal function/urine output first, to avoid iatrogenic hyperkalemia!
Note: Electrolyte imbalances (i.e. hyperkalemia, hypernatremia) are worsened by the acute renal failure commonly coexisting with DKA/HHS
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 3, 2016 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/Hyperosmolar-Hyperglycemic-State-HHS.jpg "Hyperosmolar Hyperglycemic State (HHS)
Note: HHS is only seen in Type II DM patients!
Note: In patients with either DKA or HHS, always look for an underlying cause (i.e. an infection)
Author: Yan Yu Reviewers:
Peter Vetere
Gill Goobie
Hanan Bassyouni* * MD at time of publication
Alters total body water & ion osmosis
Inadequate insulin production, insulin resistance, non- adherence to insulin Tx
Relative Insulin deficit
Stresses that ↑ Insulin demand: infections, pneumonia, MI, pancreatitis, etc)
Hyperglycemia
(Very high blood [glucose], higher than in DKA)
When blood [glucose] > 12mmol/L, glucose filtration > reabsorption, ↑ urine [glucose]
Glucosuria
Glucose in filtrate promotes osmotic diuresis: large- volume urine output
Polyuria
Dehydration
(↓ JVP, orthostasis: postural hypotension/ postural tachycardia, ↑ resting HR)
Some insulin still present, but not enoughsome glucose is utilized by muscle/fat cells, some remain in the blood
Cells not “starved”, but still need more energy
↑ release of Catabolic hormones: Glucagon, Epinephrine, Cortisol, GH
Body tries to ↑ blood [glucose], to hopefully ↑ cell glucose absorption
Hypothalamic cells sense low intra-cellular glucose, triggering feelings of hunger
Polyphagia
Note: the presence of some insulin directly inhibits lipolysis; thus, in HHS there is no ketone body production, and no subsequent metabolic acidosis and ketouria (unlike in DKA). If ketones are detected in an HHS patient it’s likely secondary to starvation or other mechanisms.
↓ ECF volume, ↑ ECF osmolarity (i.e. hypernatremia)
↑ Gluconeogenesis ↑ Glycogenolysis (in liver)
↓ Protein synthesis, ↑ proteolysis
(in muscle)
↑ Gluconeogenic substrates for liver If the patient doesn’t drink enough
water to replenish lost blood volume If pt is alert and
Electrolyte imbalance
water is accessible
Water osmotically leaves neurons, shrinking them
Neural damage: delirium, lethargy, seizure, stupor, coma
↓ renal perfusion, ↓ GFR
Renal Failure
(pre-renal cause; see relevant slides)
Polydipsia Note: in HHS, body K+ is lost via osmotic diuresis. But diffusion of K+ out of cells
may cause serum [K+] to be falsely normal/elevated. To prevent hypokalemia, give IV KCl along with IV insulin as soon as serum K+ <5.0mmol/L. But ensure patient has good renal function/urine output first, to avoid iatrogenic hyperkalemia!
Note: Electrolyte imbalances (i.e. hyperkalemia, hypernatremia) are worsened by the acute renal failure commonly coexisting with DKA/HHS
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 3, 2016 on www.thecalgaryguide.com")
cholesteatoma-nov-4-2016_final-edits
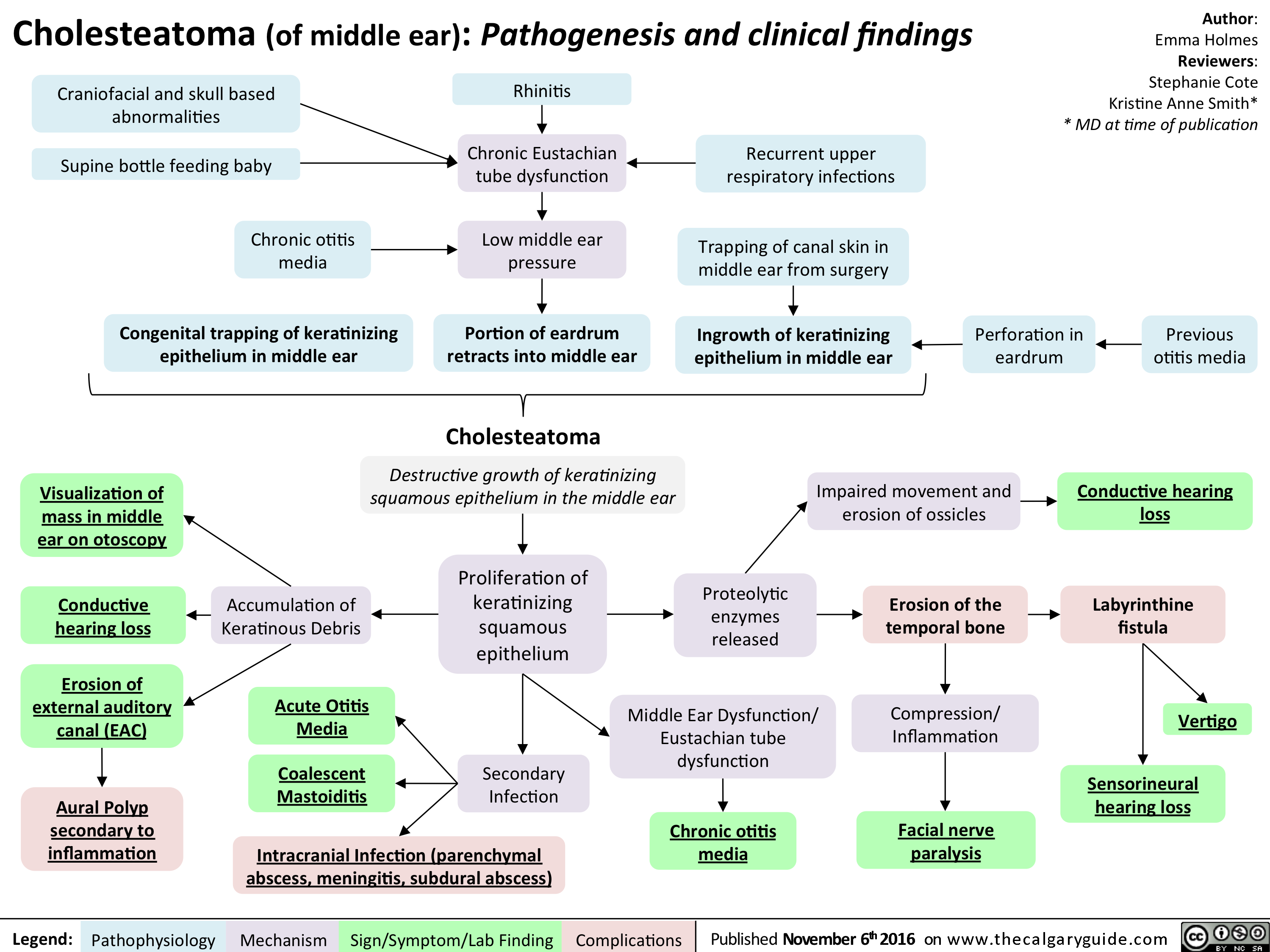
Ketamine
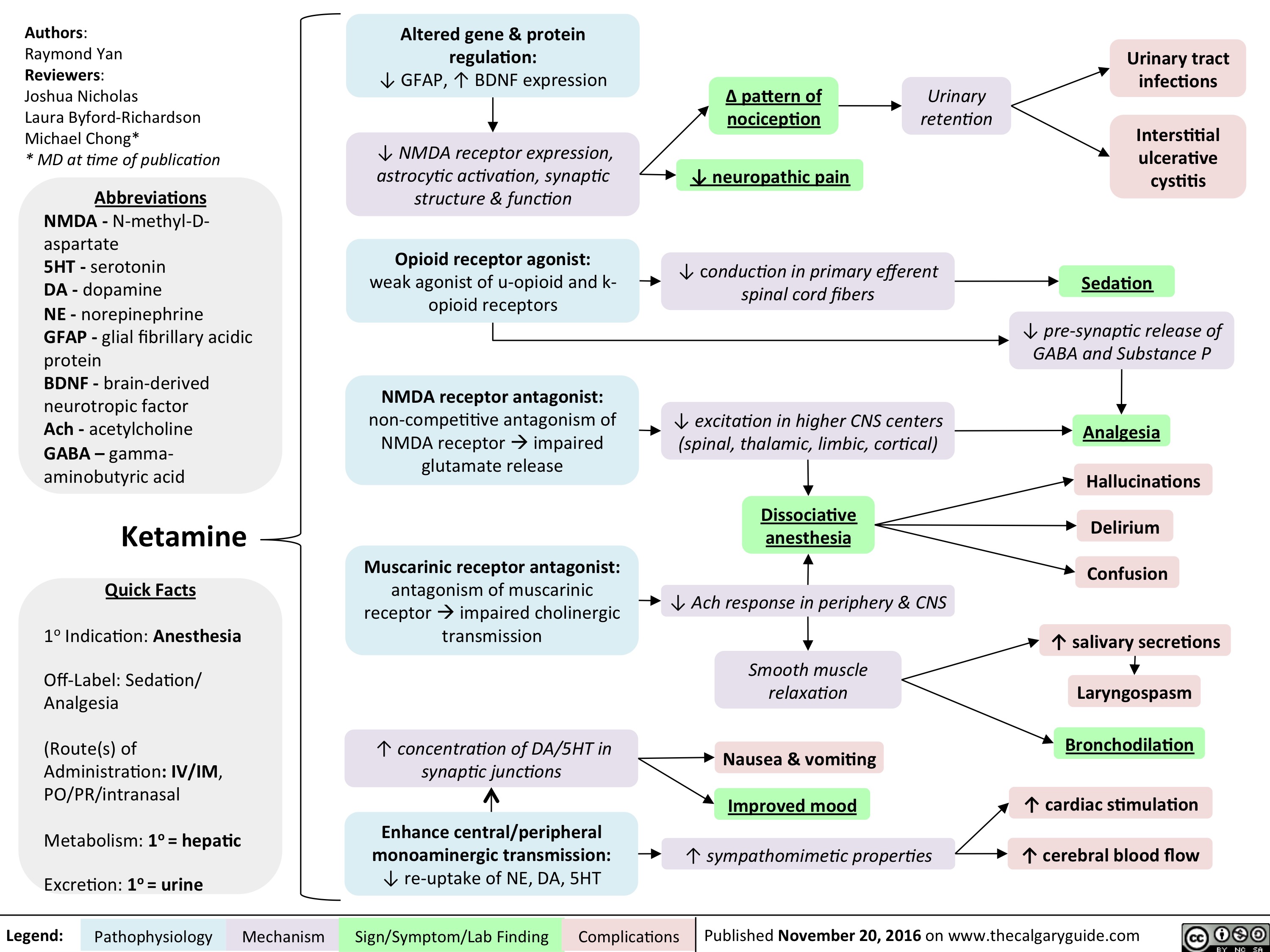
Neurotransmitters and Pharmacology behind Nausea and Vomiting
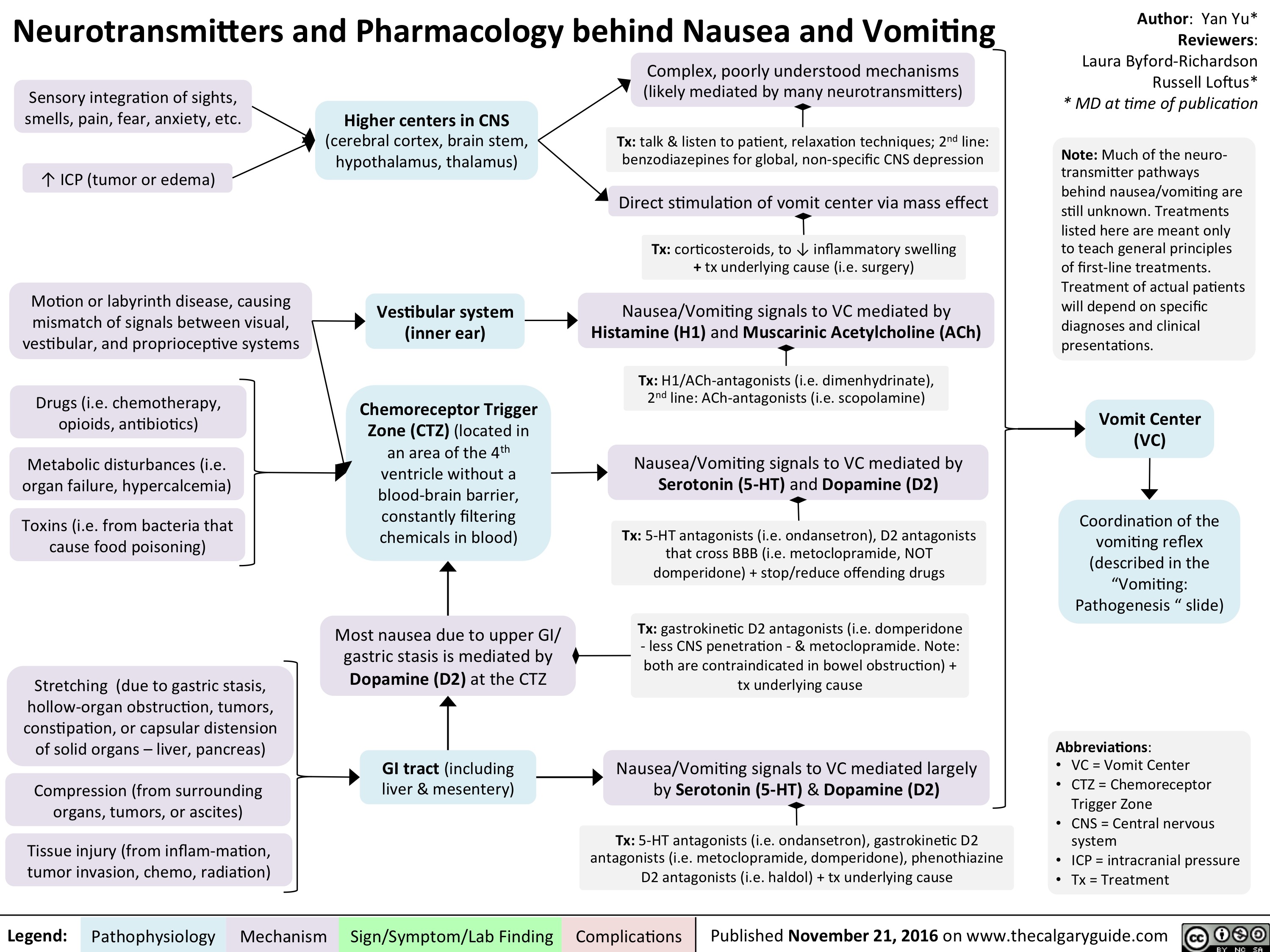
Neurotransmitters and Pharmacology behind Nausea and Vomiting
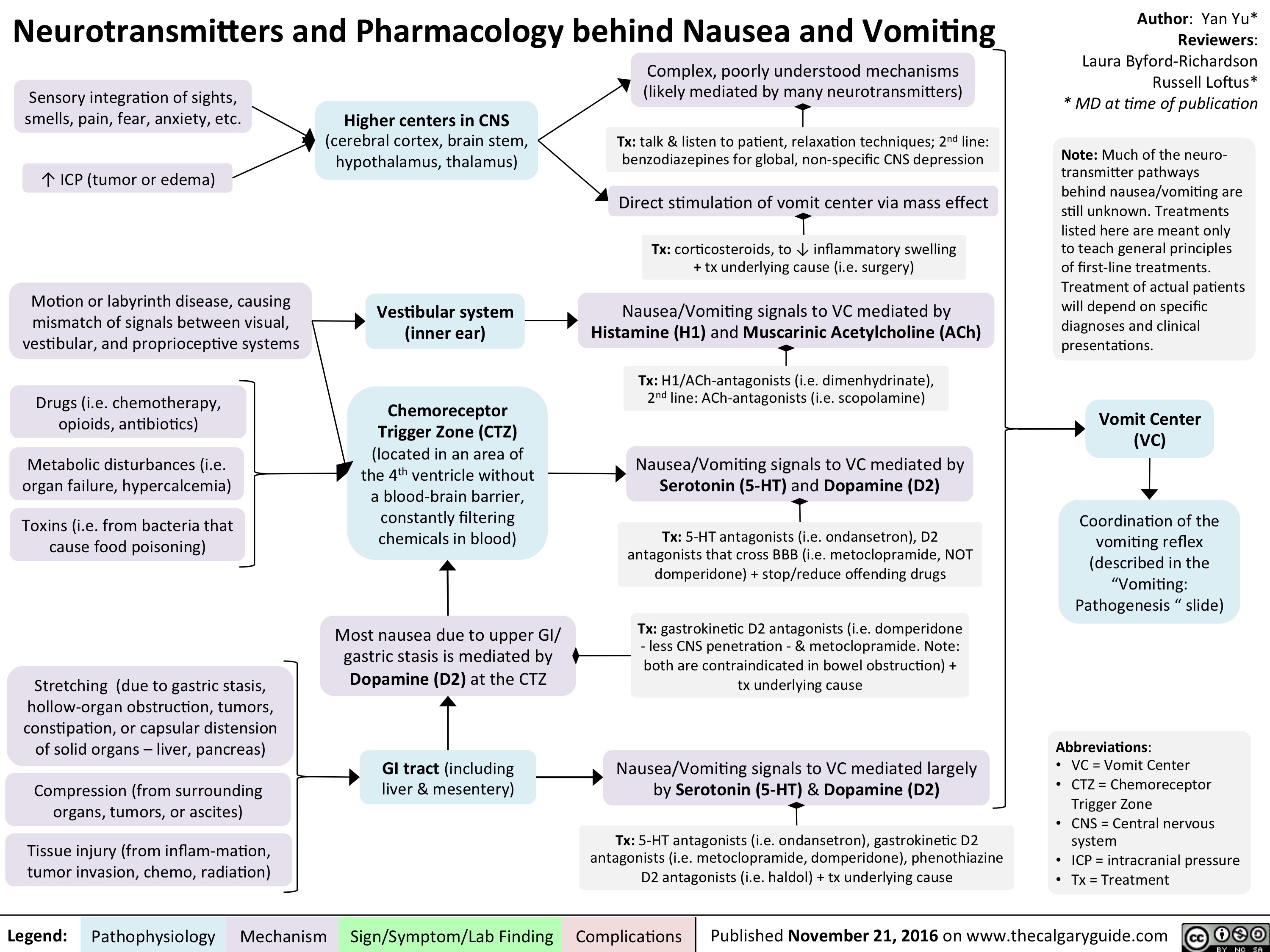
Neurotransmitters and Pharmacology behind Nausea and Vomiting
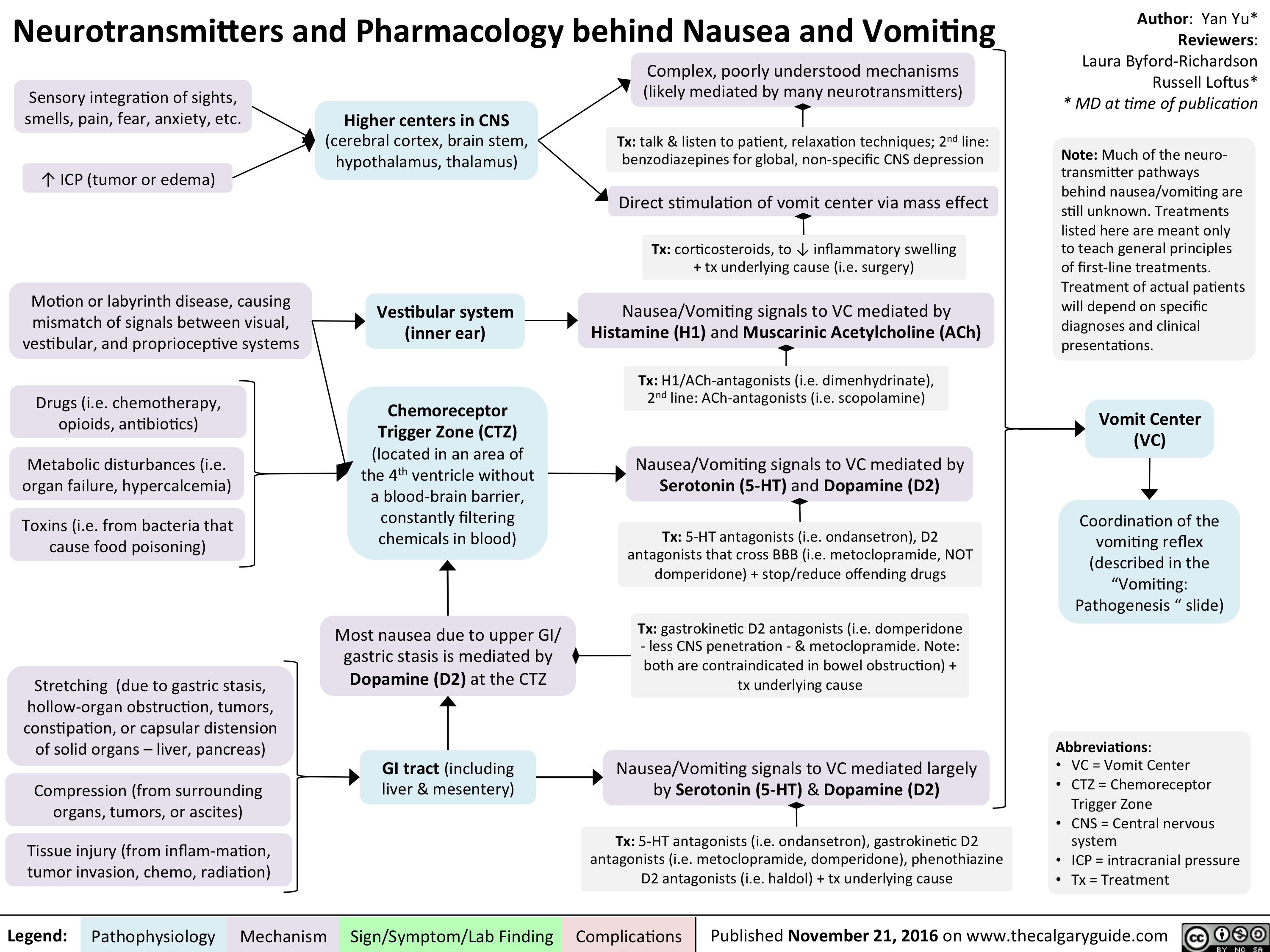
pathogenesis-of-neuropathic-pain
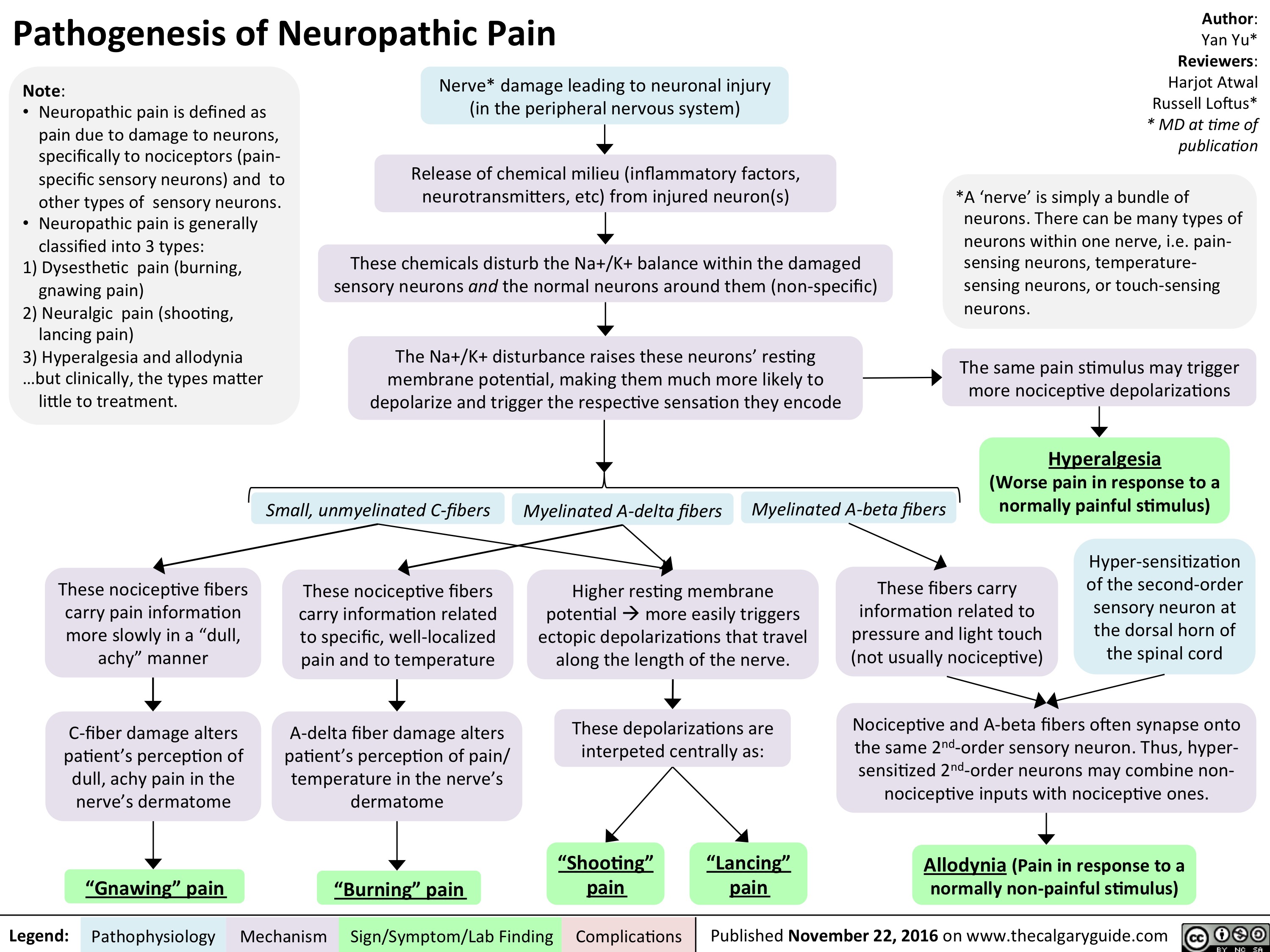
bn-pathogenesis
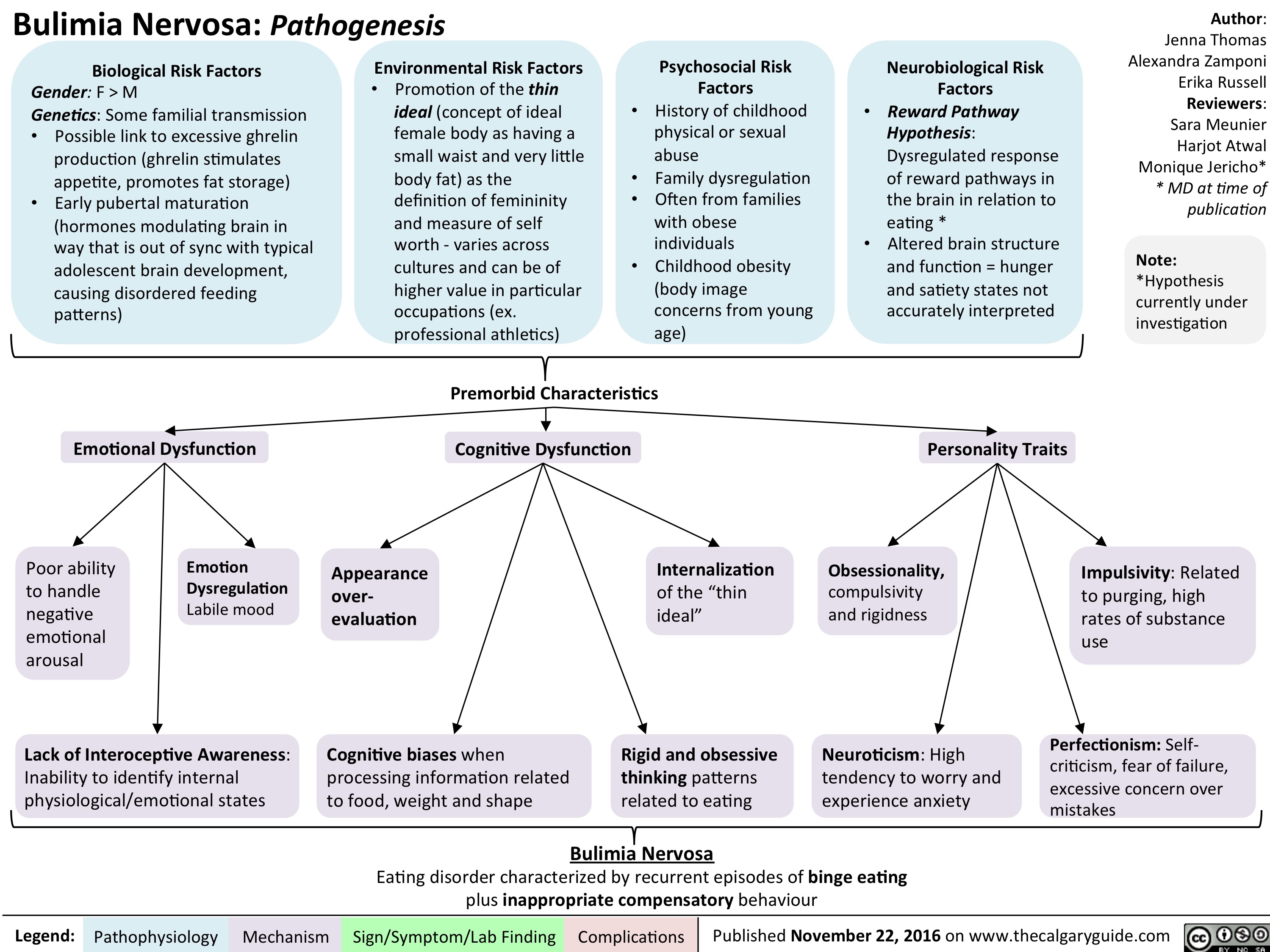
bn-signs-and-symptoms
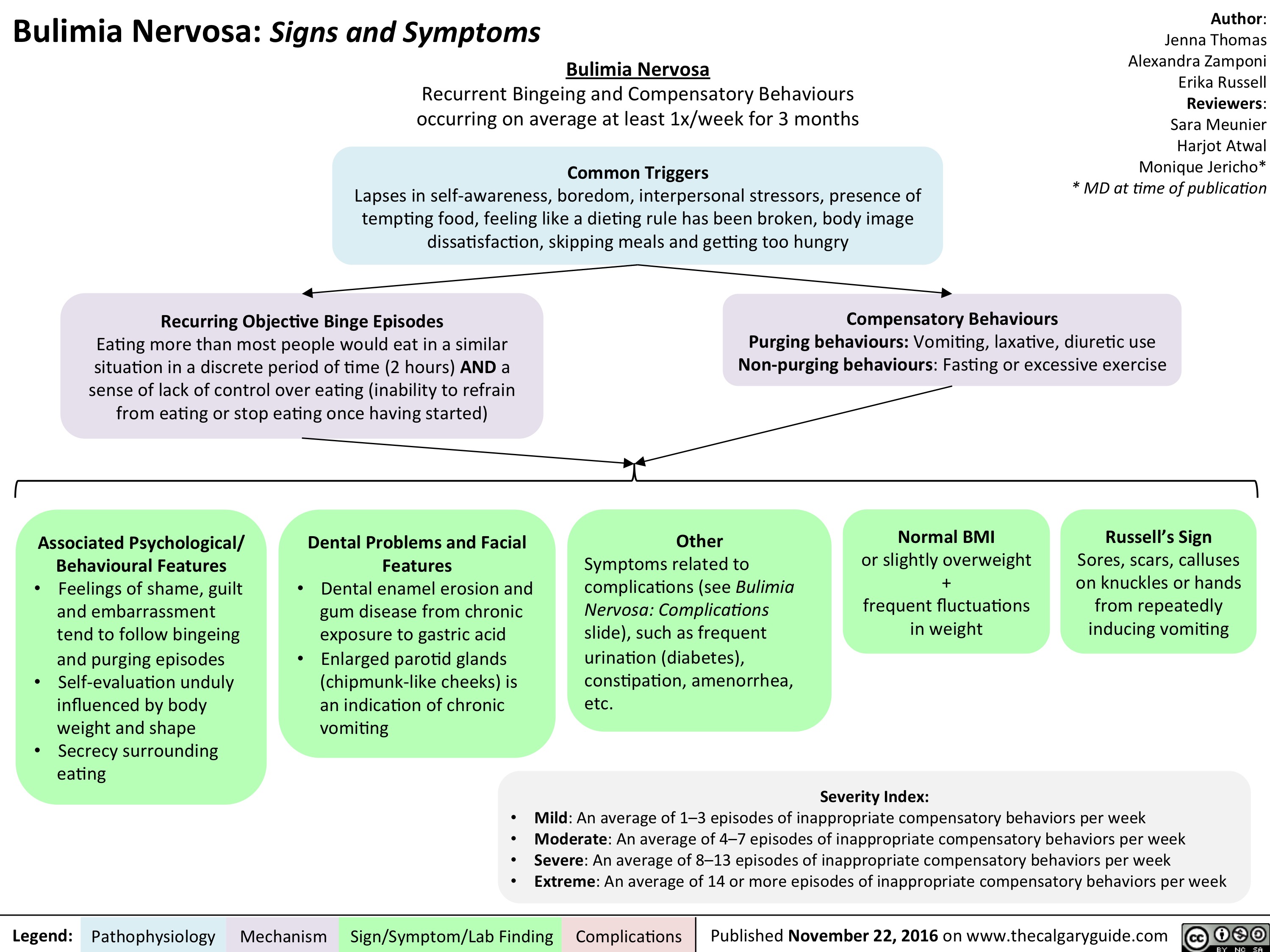
bn-complications
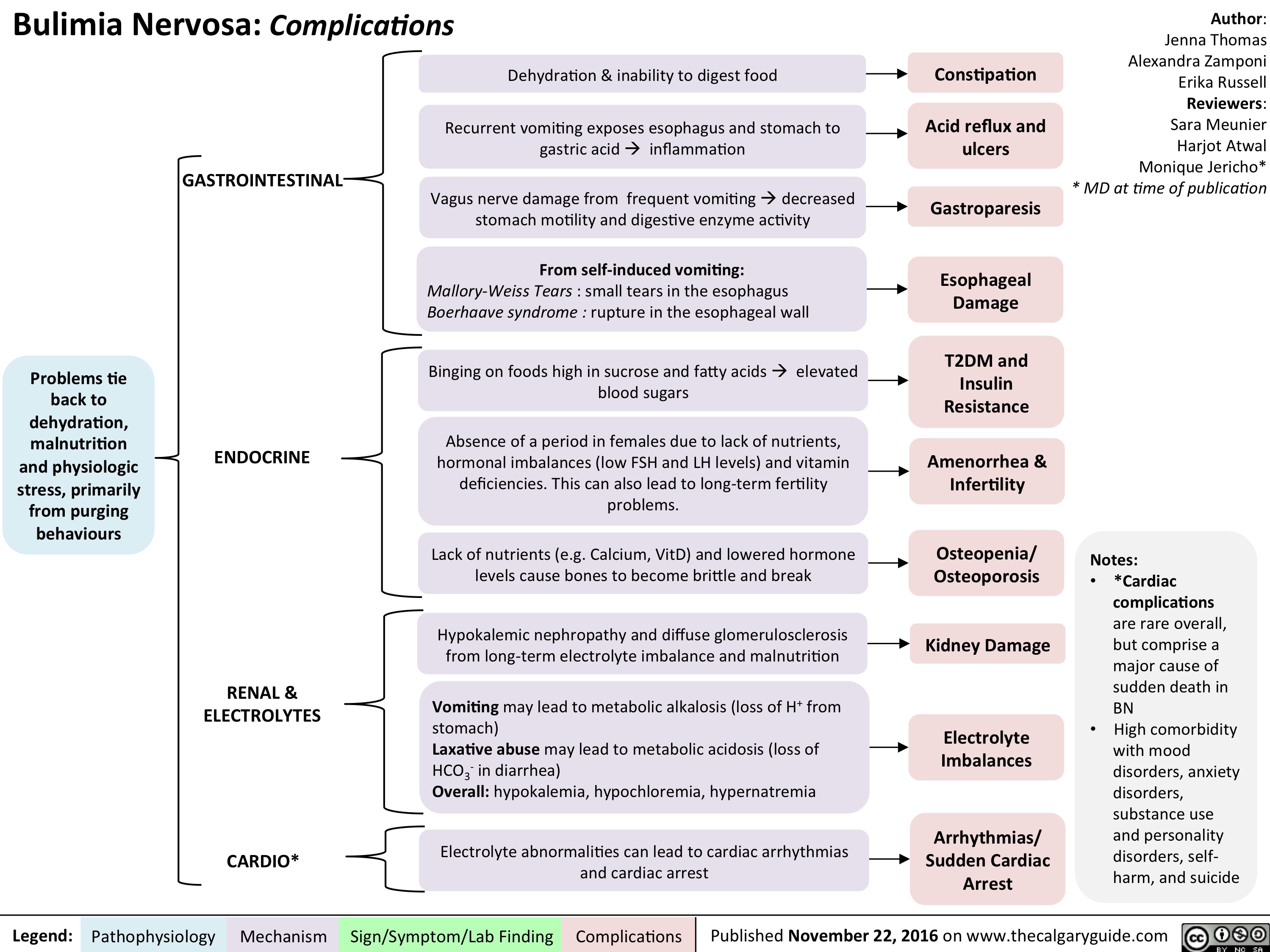
Small Bowel Bacterial Overgrowth: Pathogenesis and clinical findings
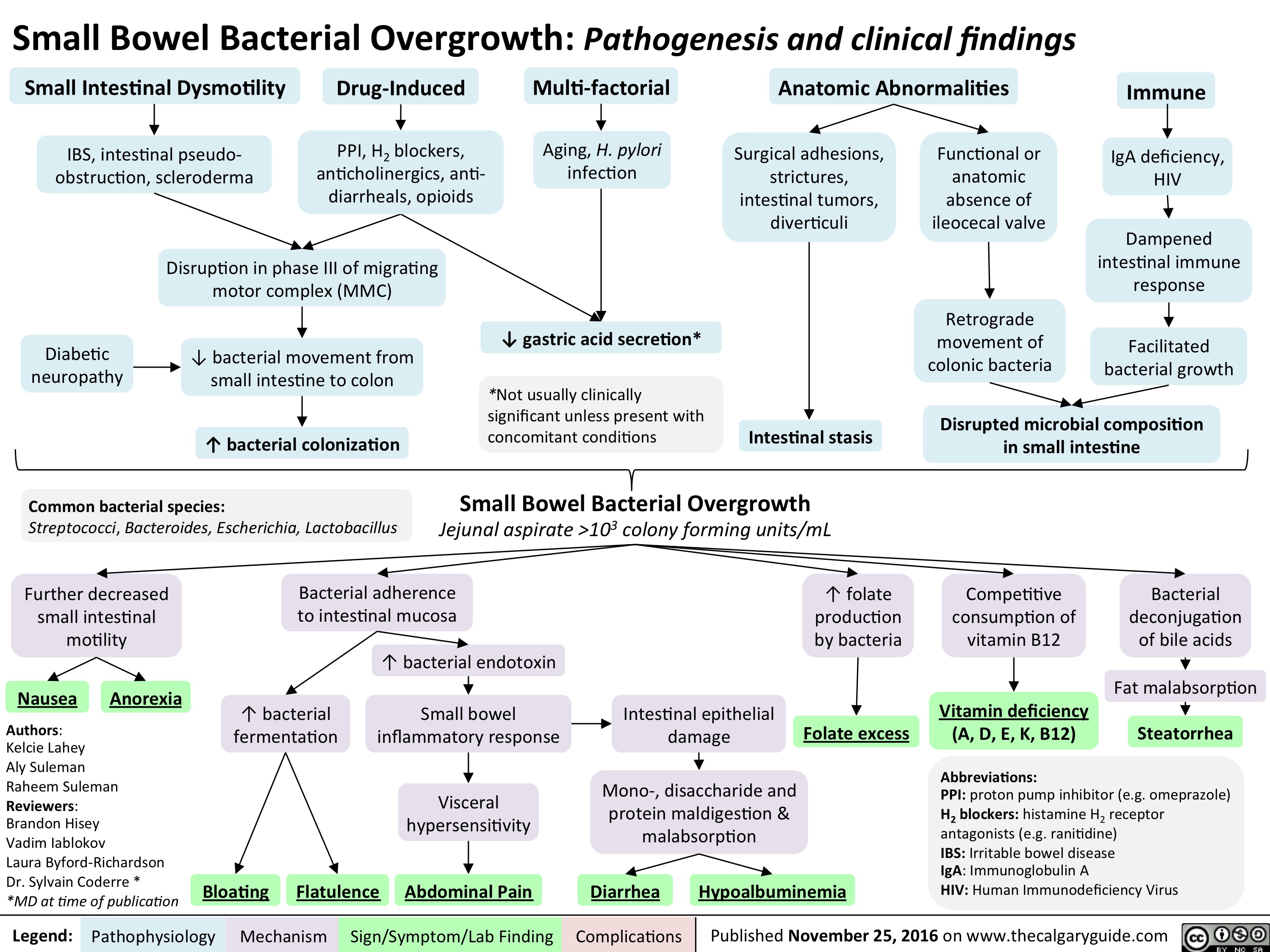
slide1
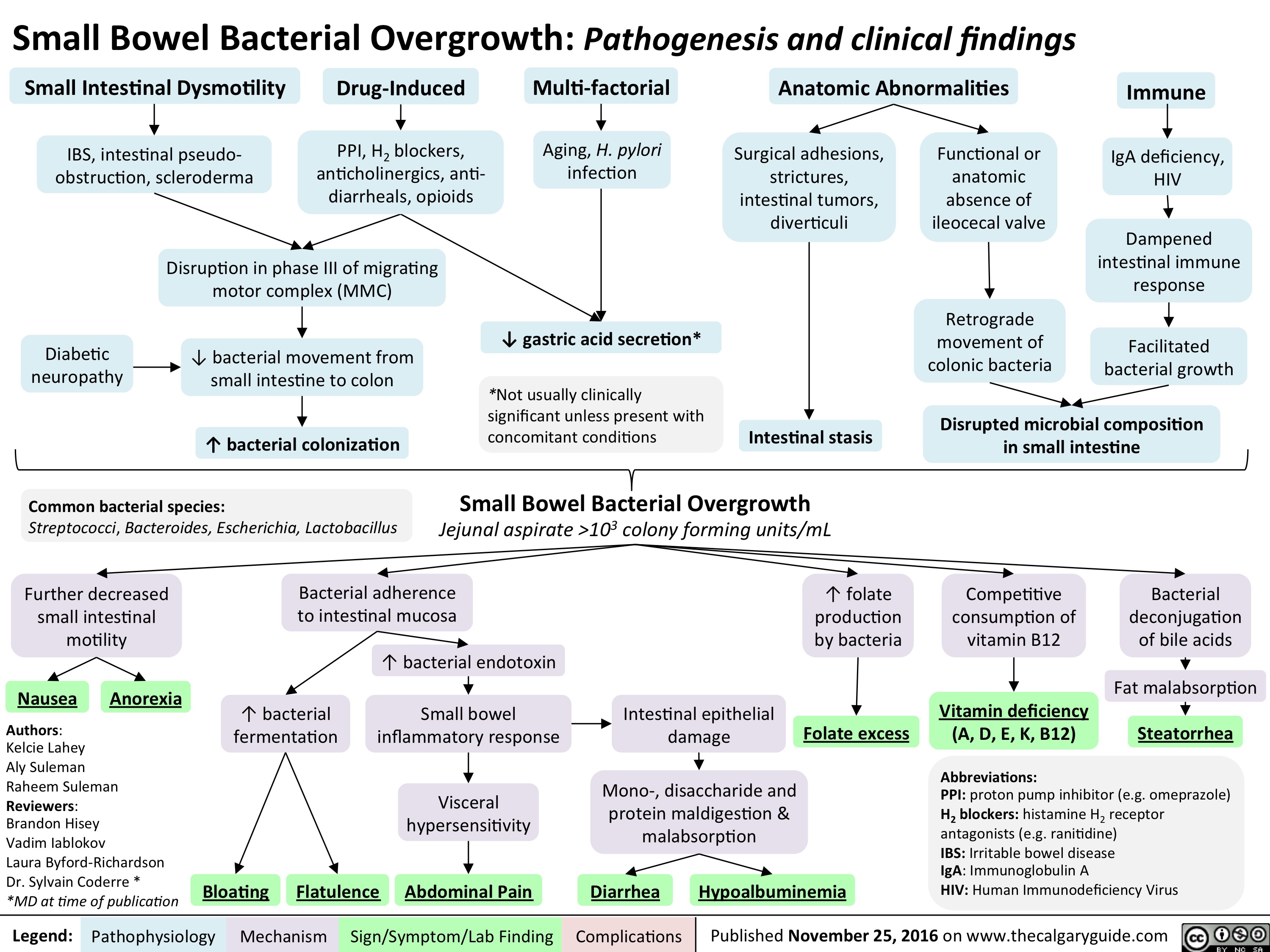
menstrual-cycle-physiology-the-hypothalamic-pituitary-ovarian-axis
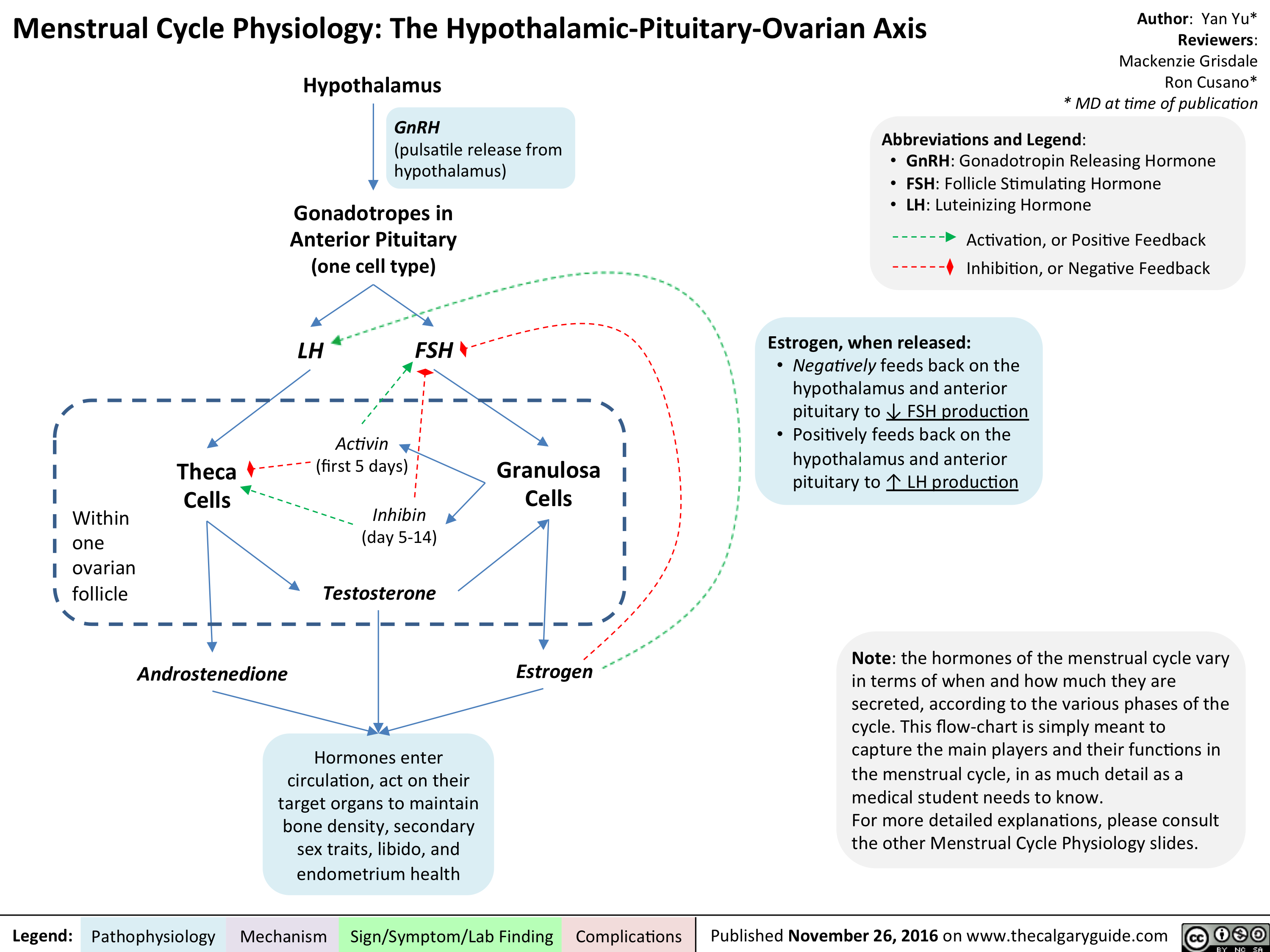
menstrual-cycle-physiology-correlating-the-ovarian-and-uterine-cycles
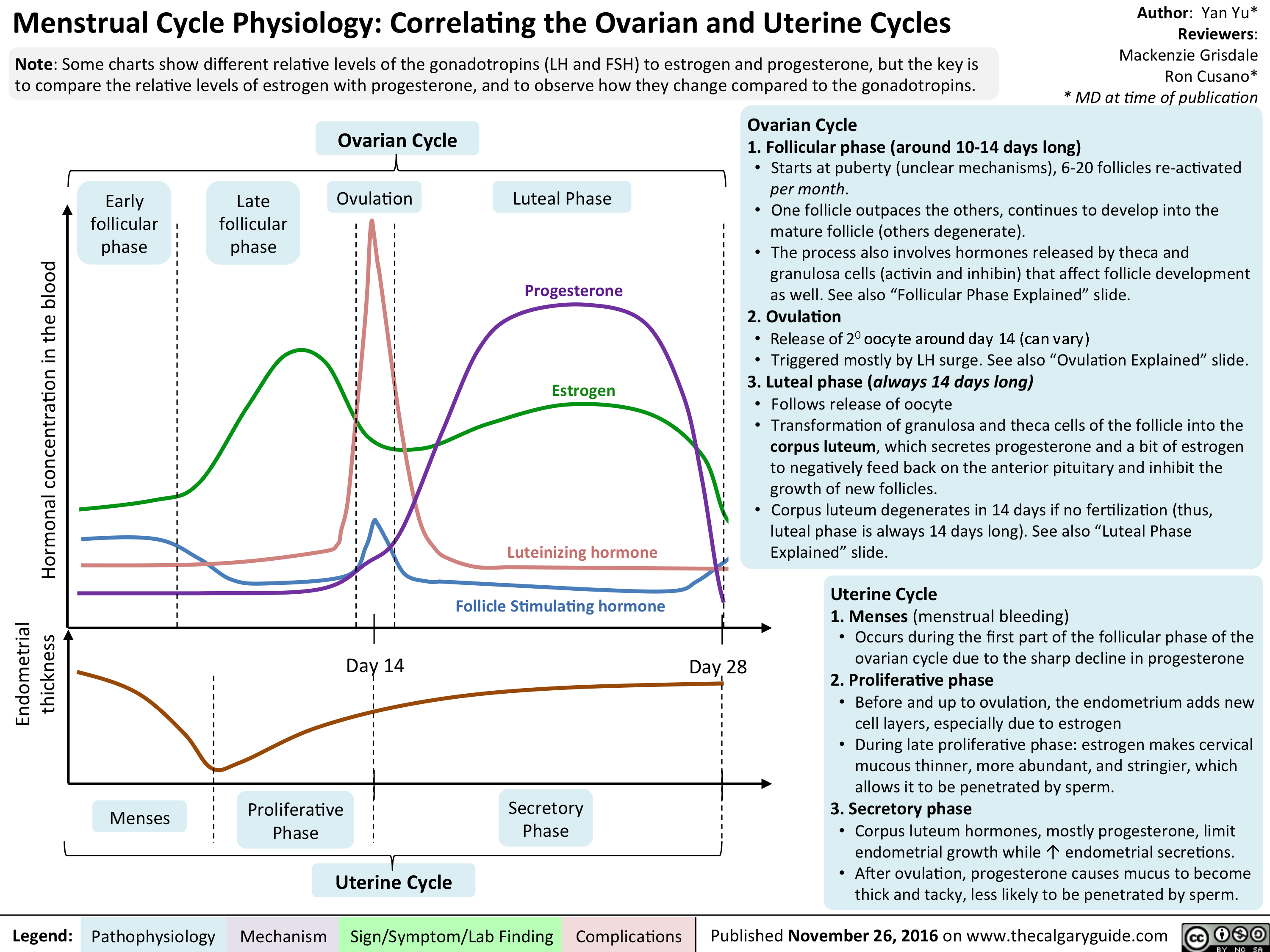
menstrual-cycle-physiology-ovarian-cycle-follicular-phase-explained
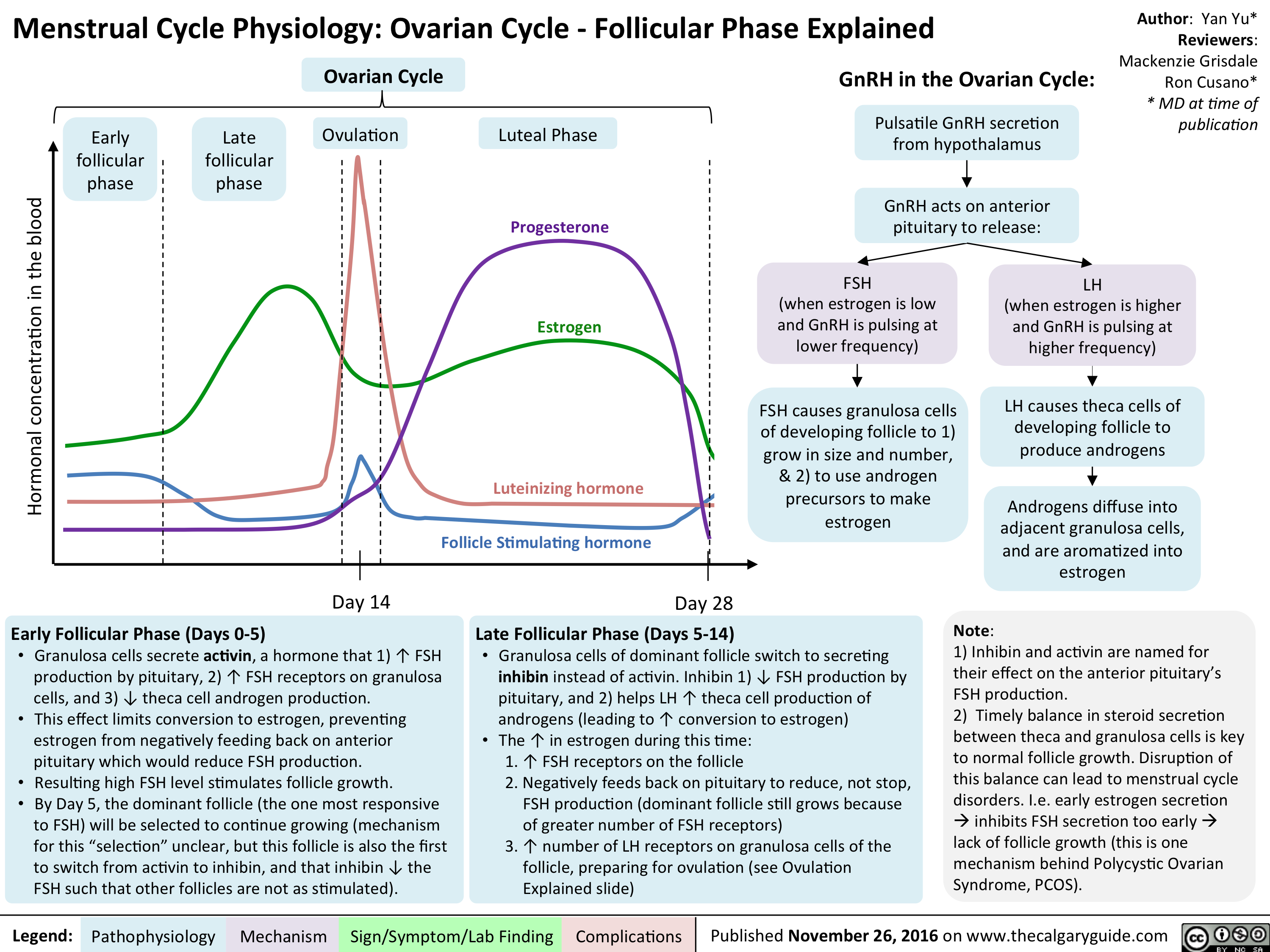
menstrual-cycle-physiology-ovarian-cycle-ovulation-explained

menstrual-cycle-physiology-ovarian-cycle-luteal-phase-explained
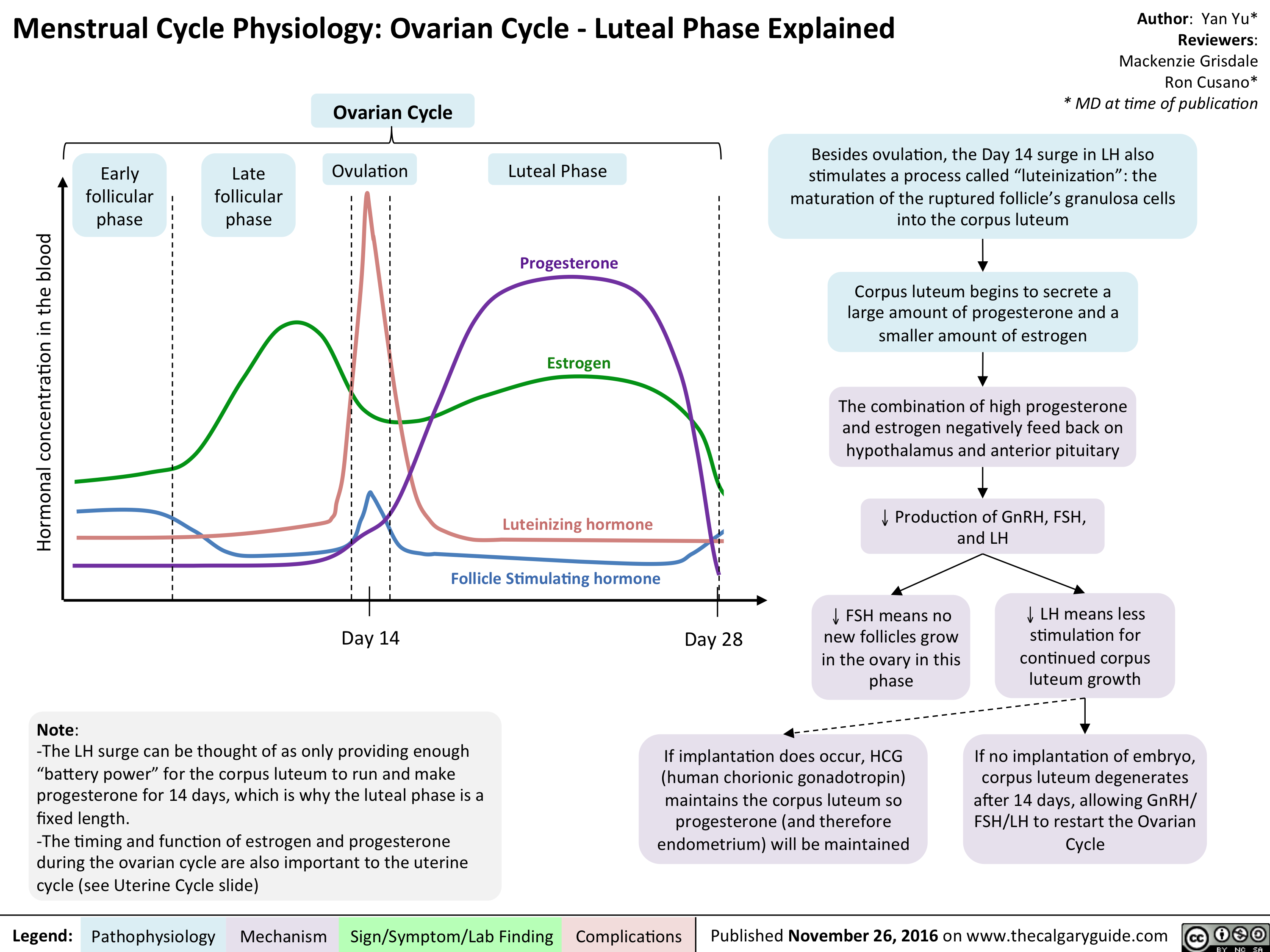
menstrual-cycle-physiology-the-uterine-cycle
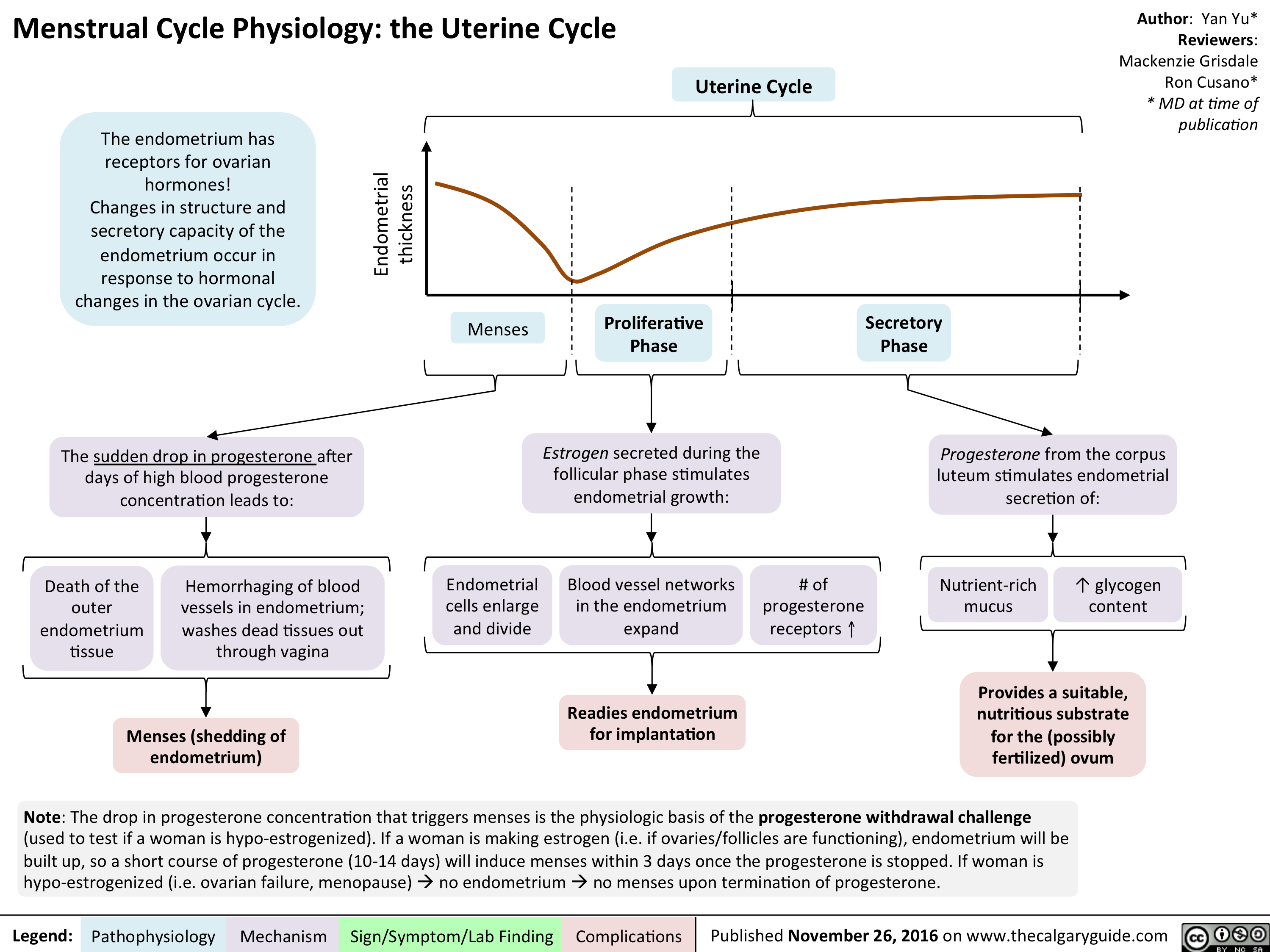
Shoulder Dystocia: Pathogenesis and Clinical Findings
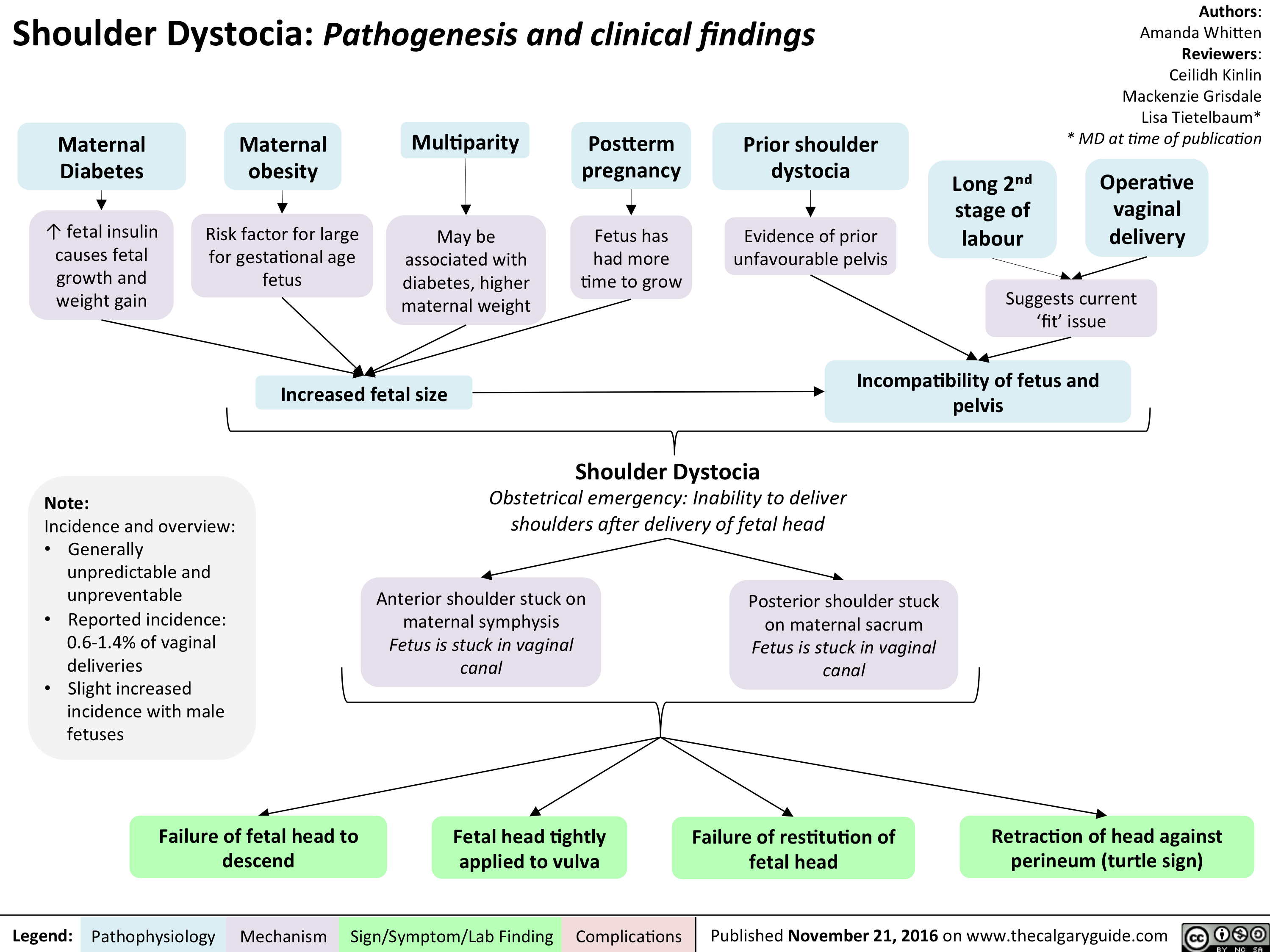
lvh-final
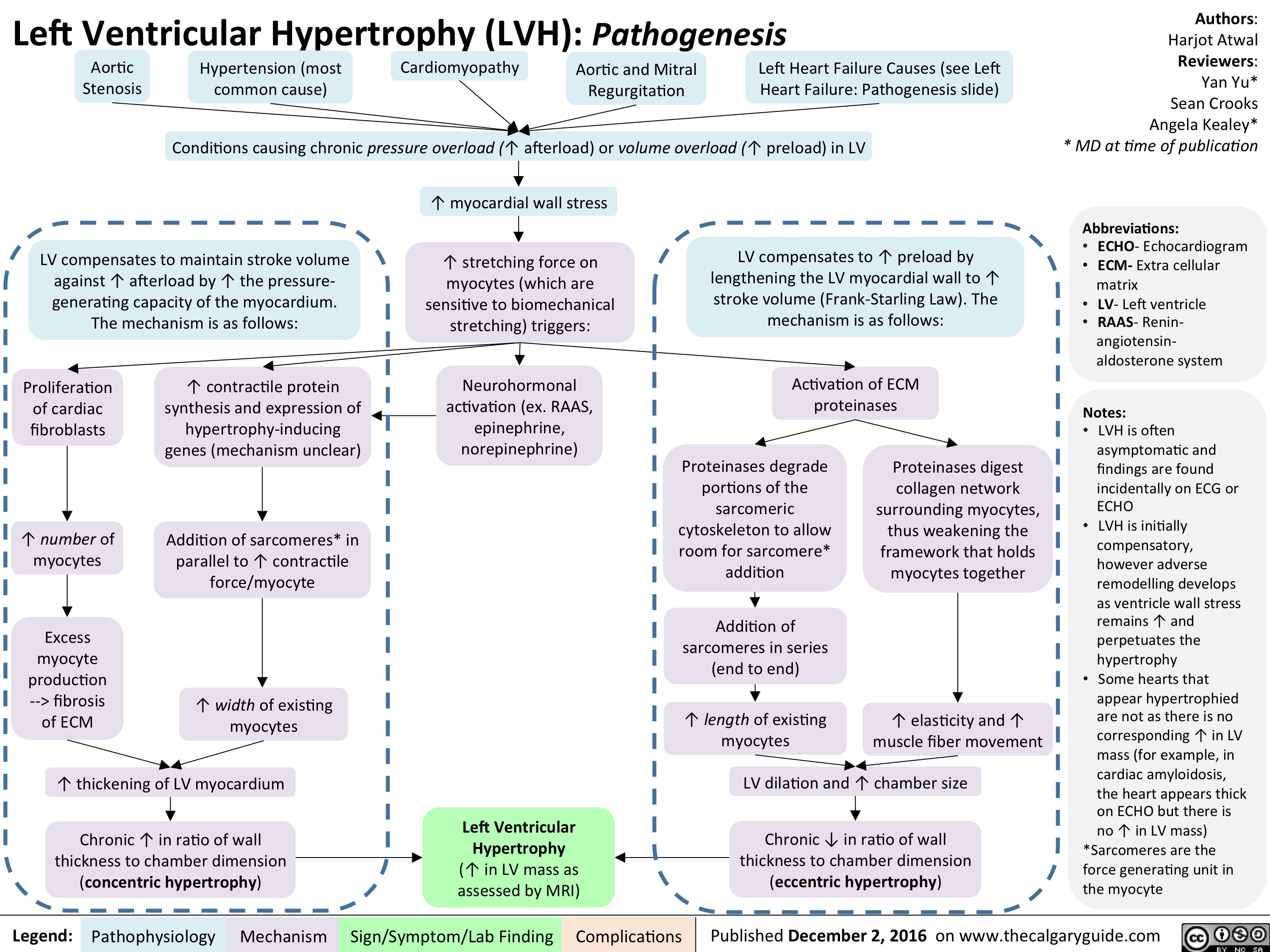
anorexia-nervosa
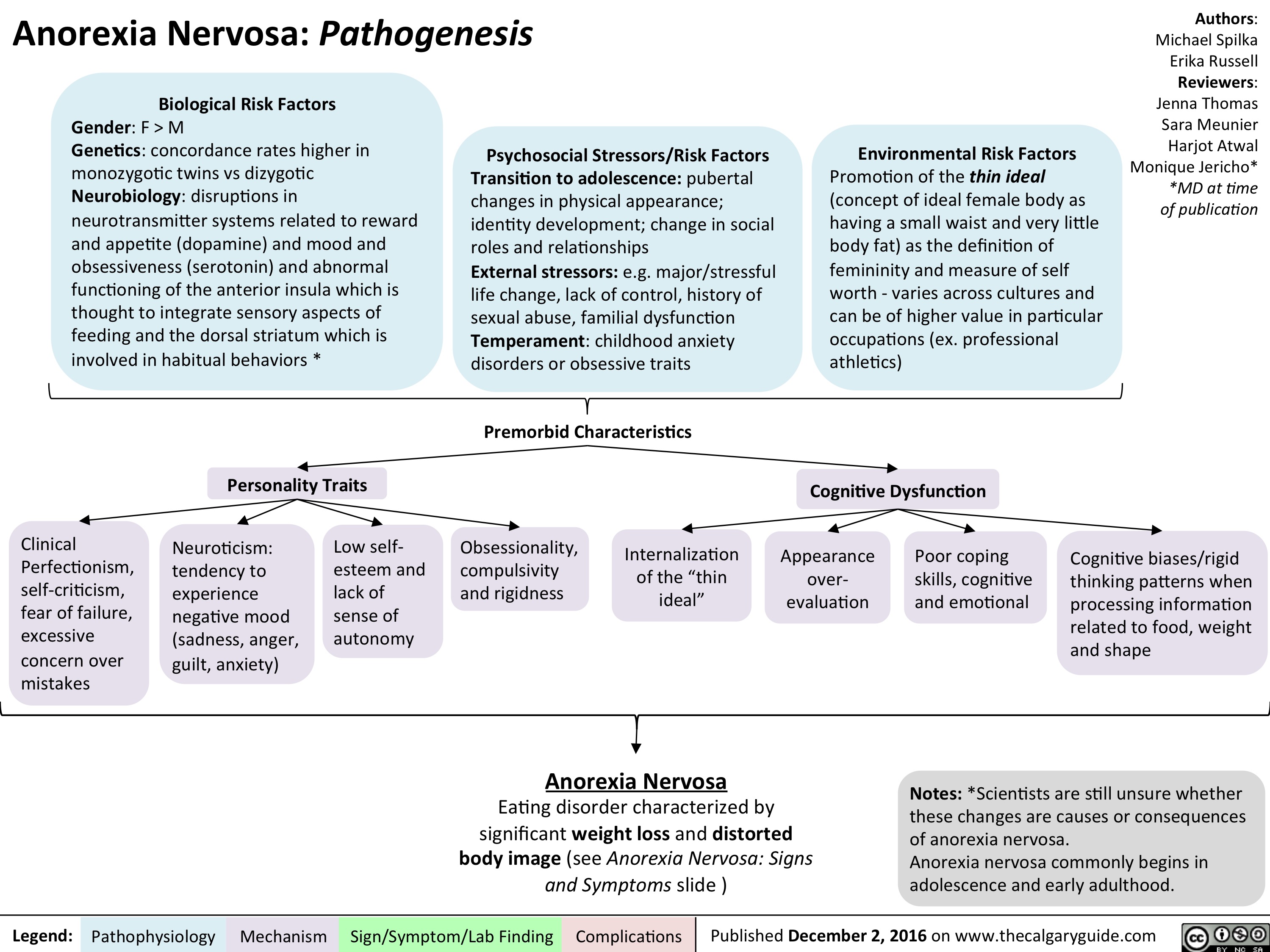
an-signs-and-symptoms
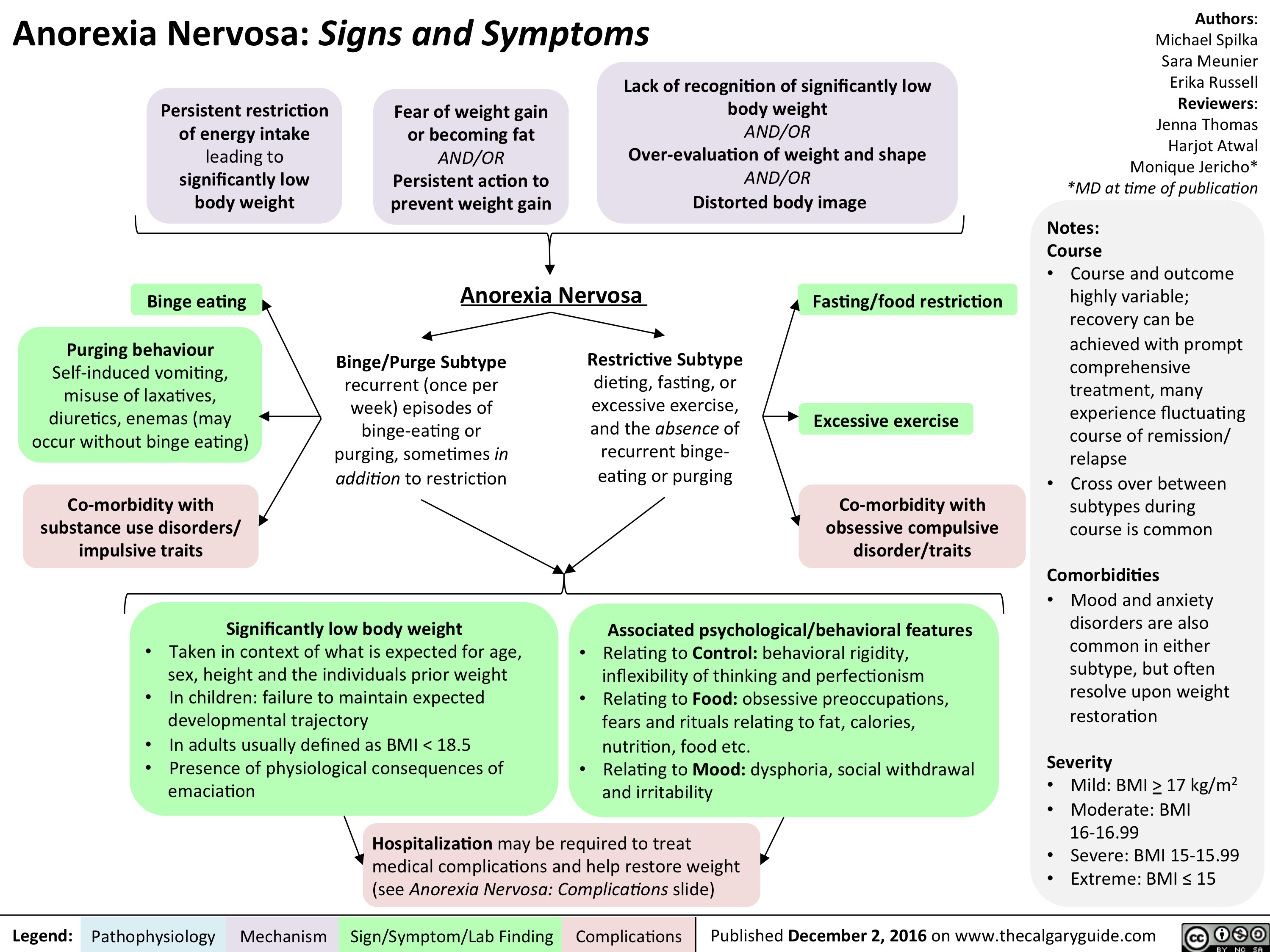
an-complications-final
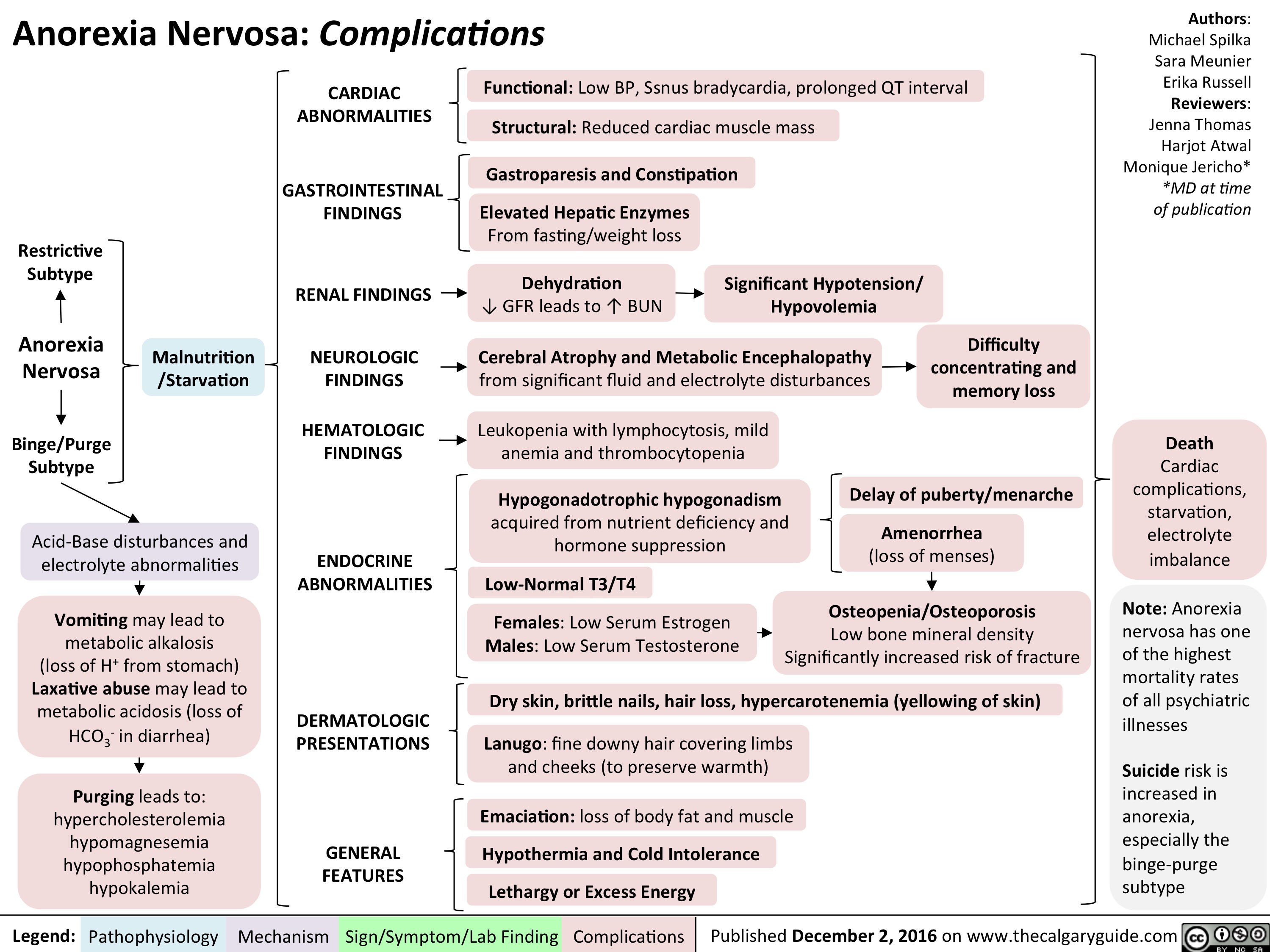
als-final
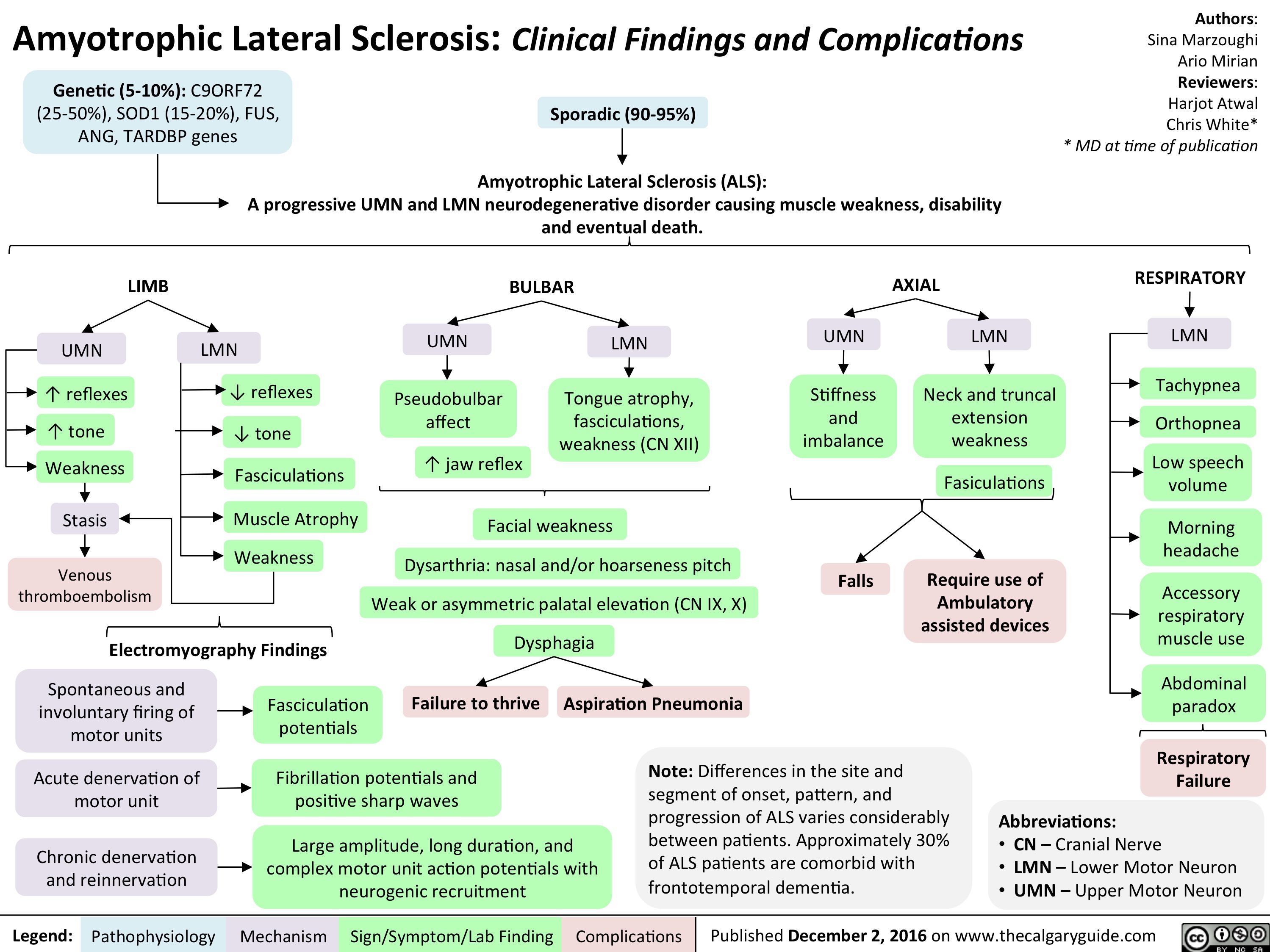
alzheimers-disease-final
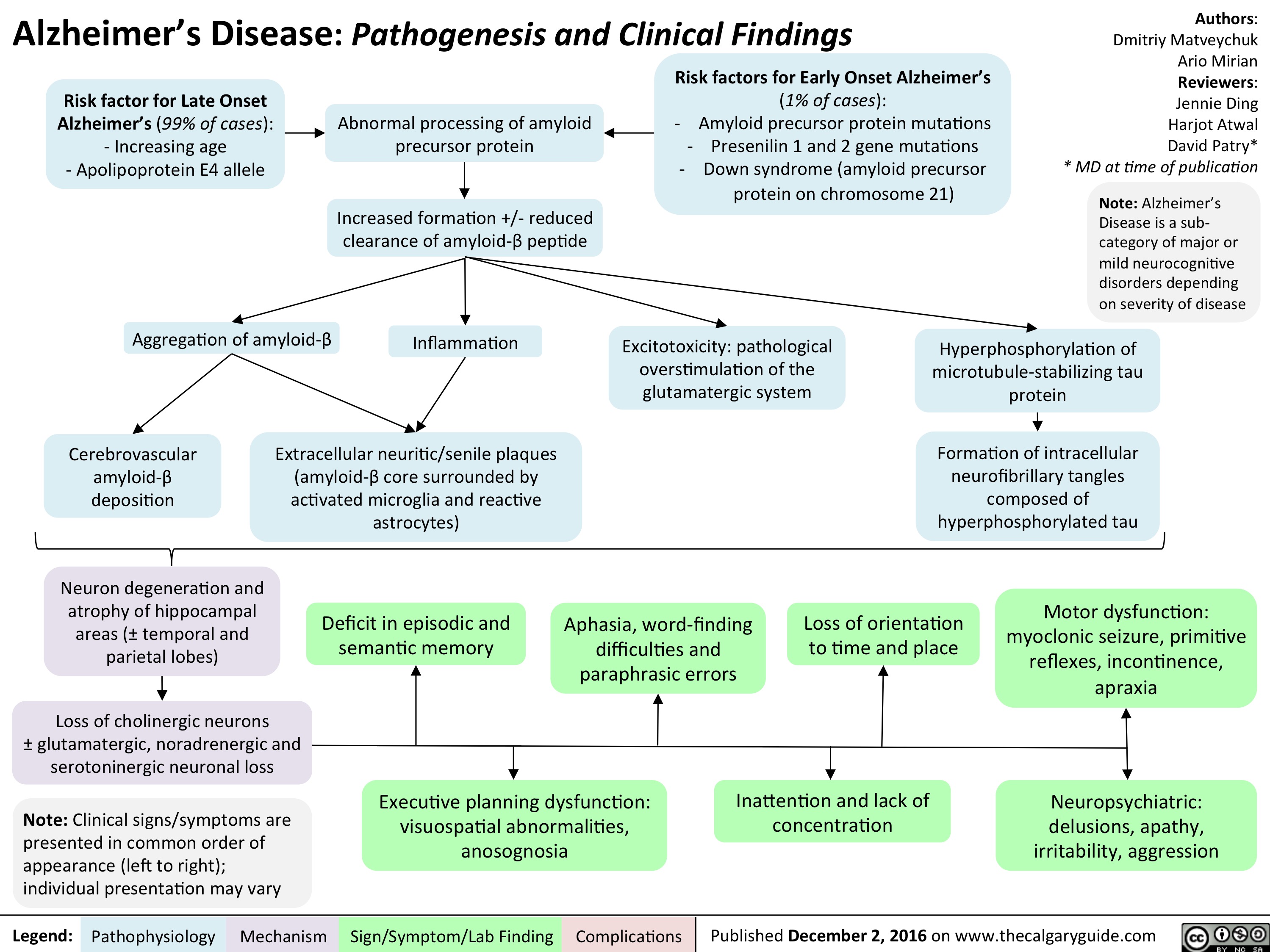
lewy-body-dementia-final
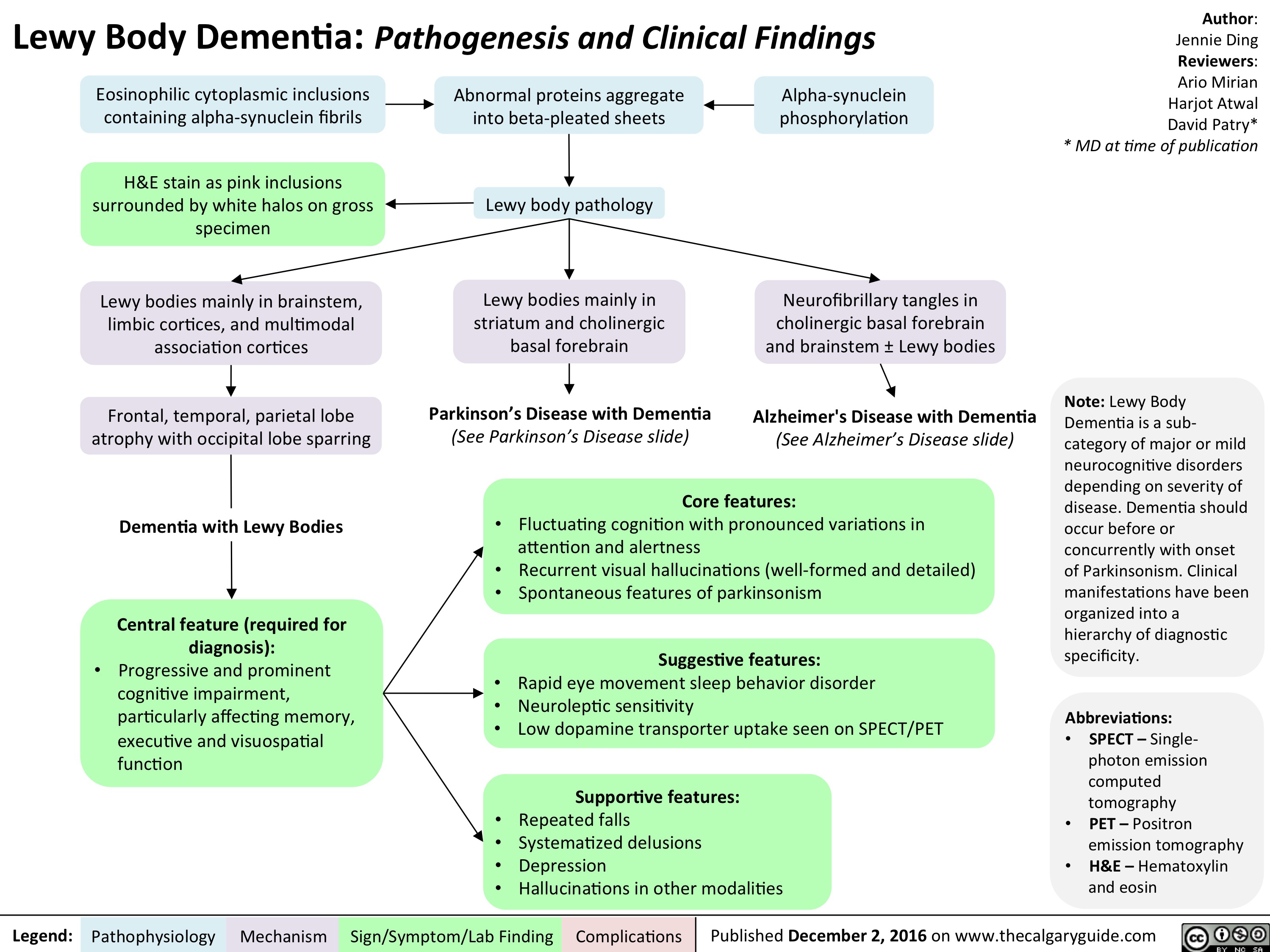
als-final
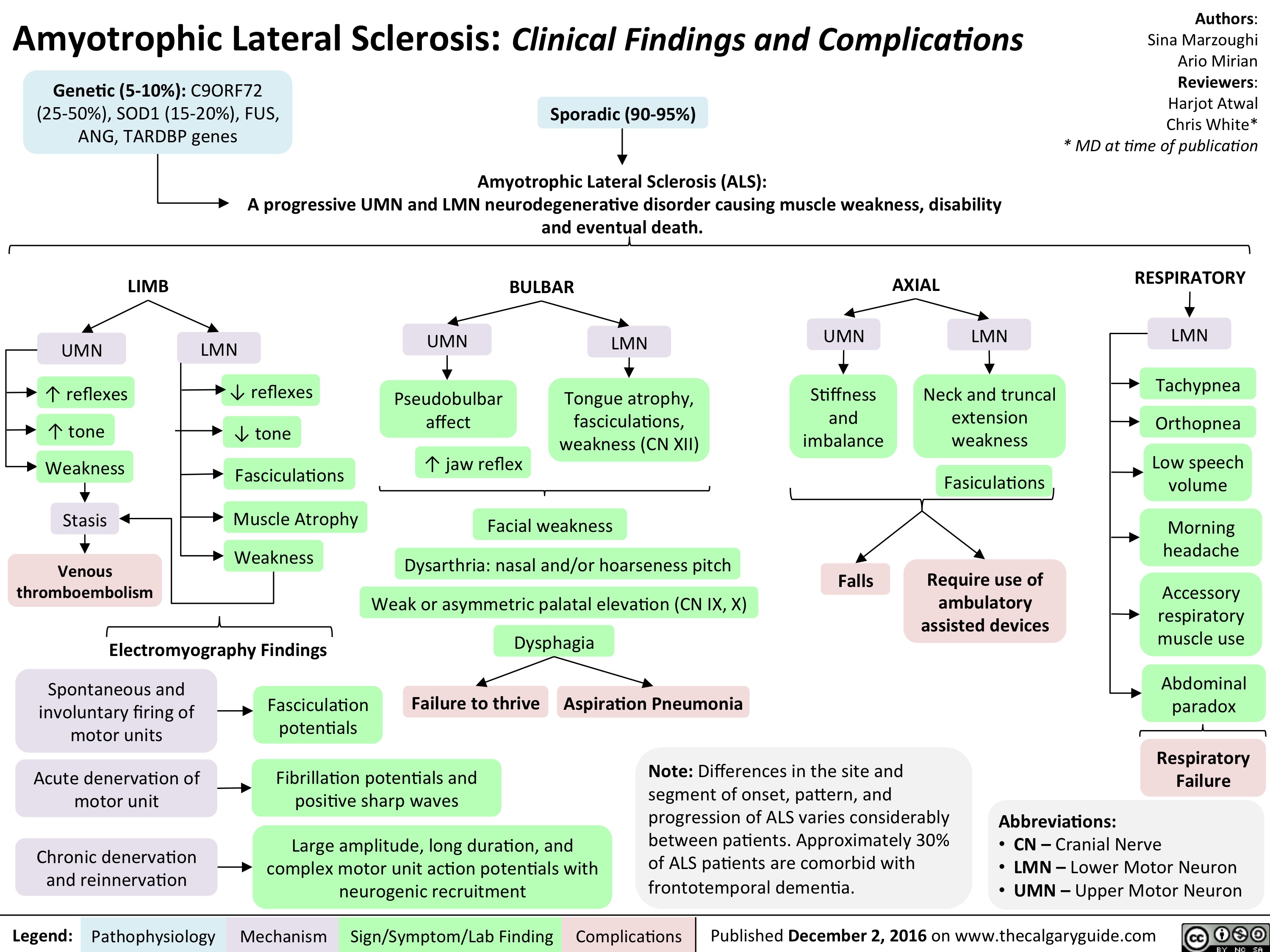
als-final
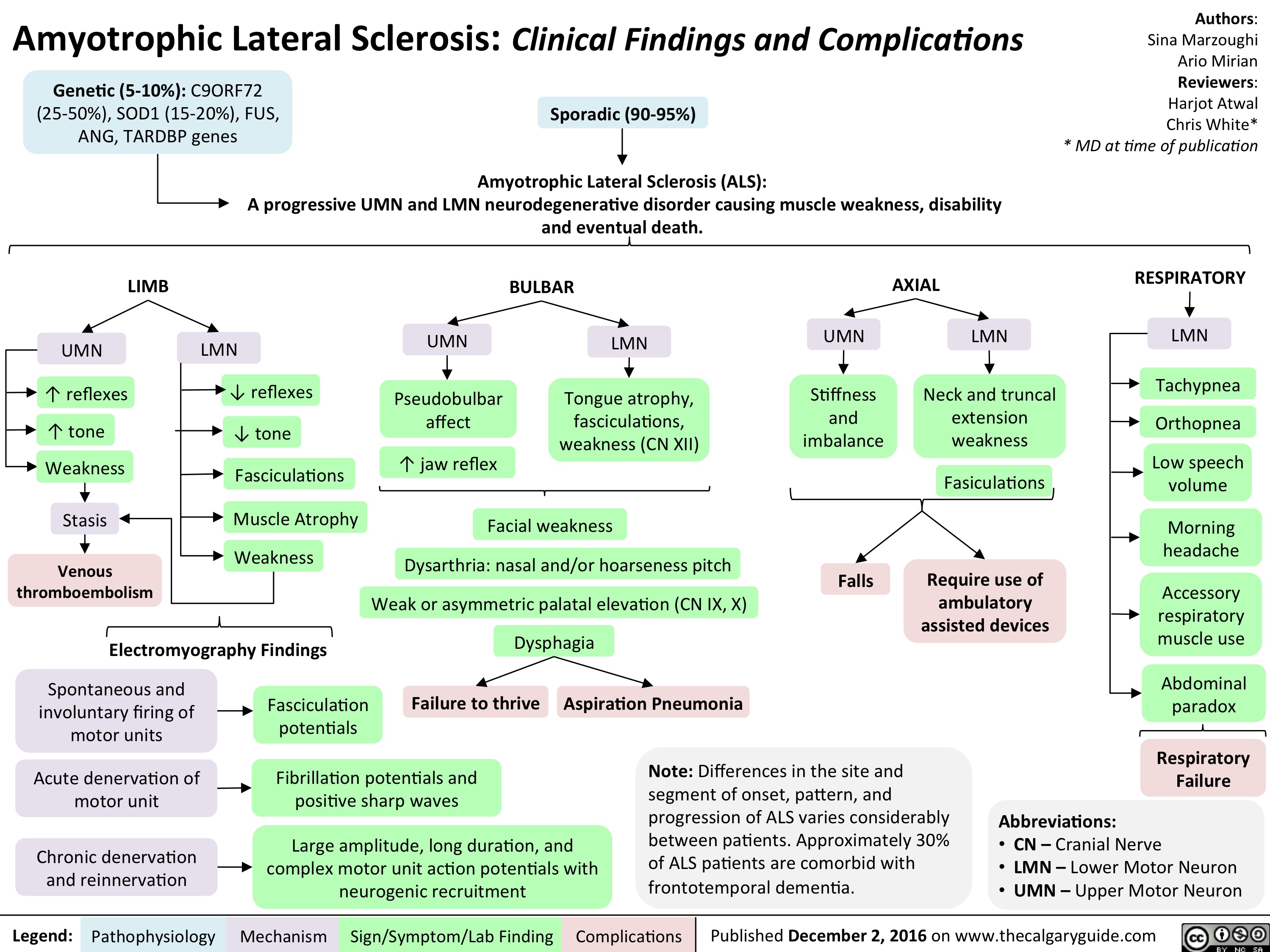
NSAIDs Final
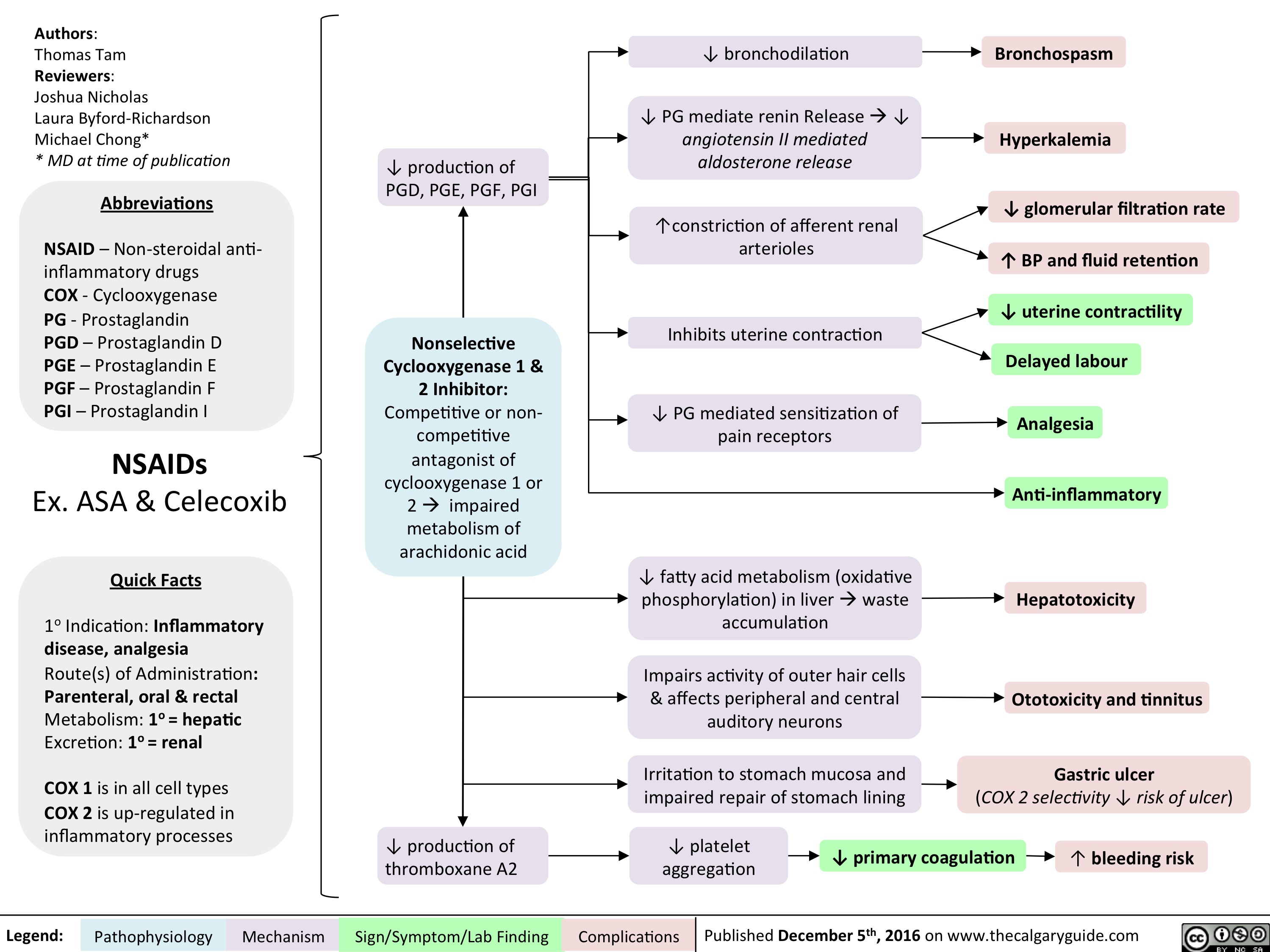
NSAIDs Final
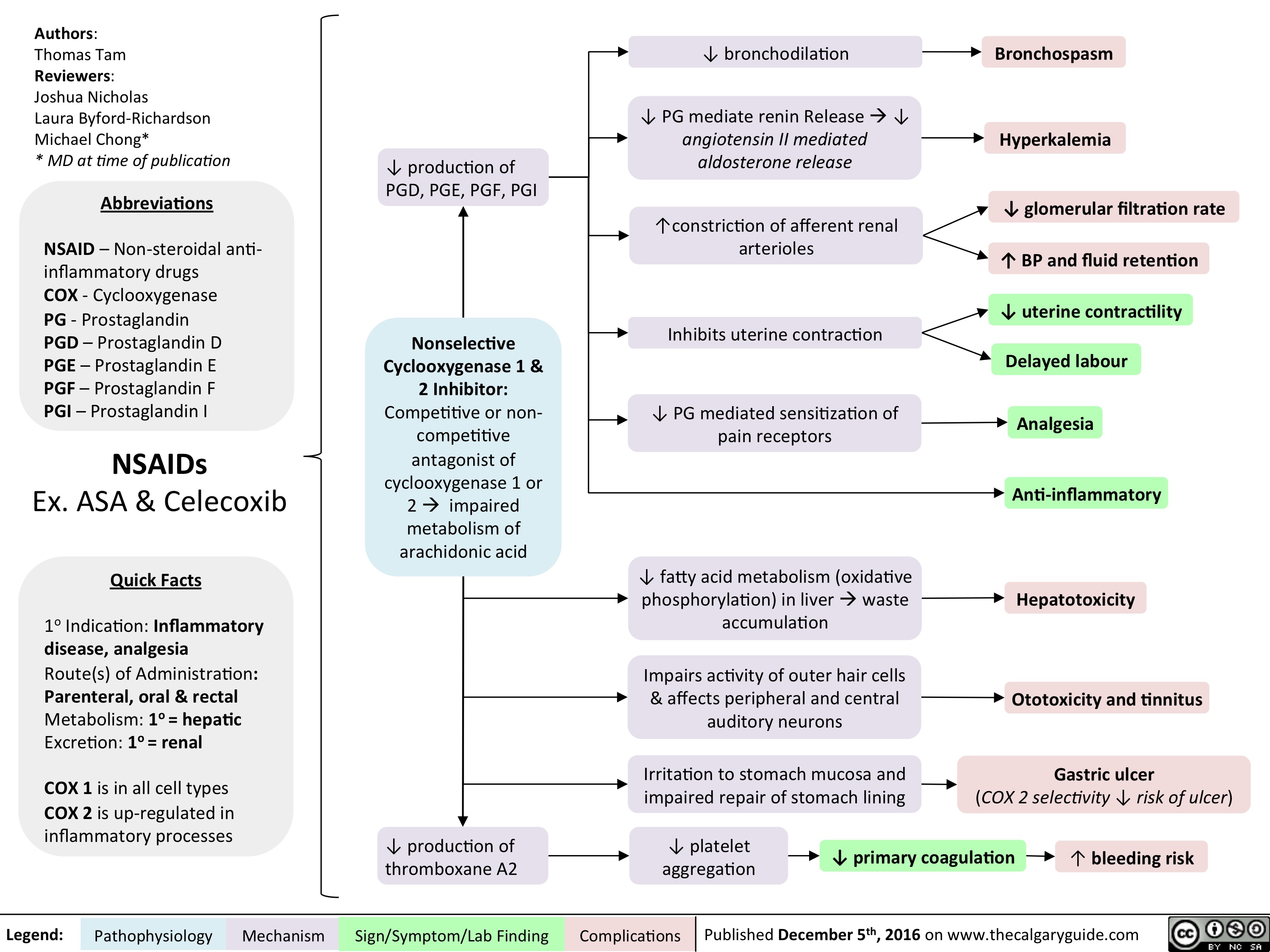
induction-of-labour-indications-and-contraindications
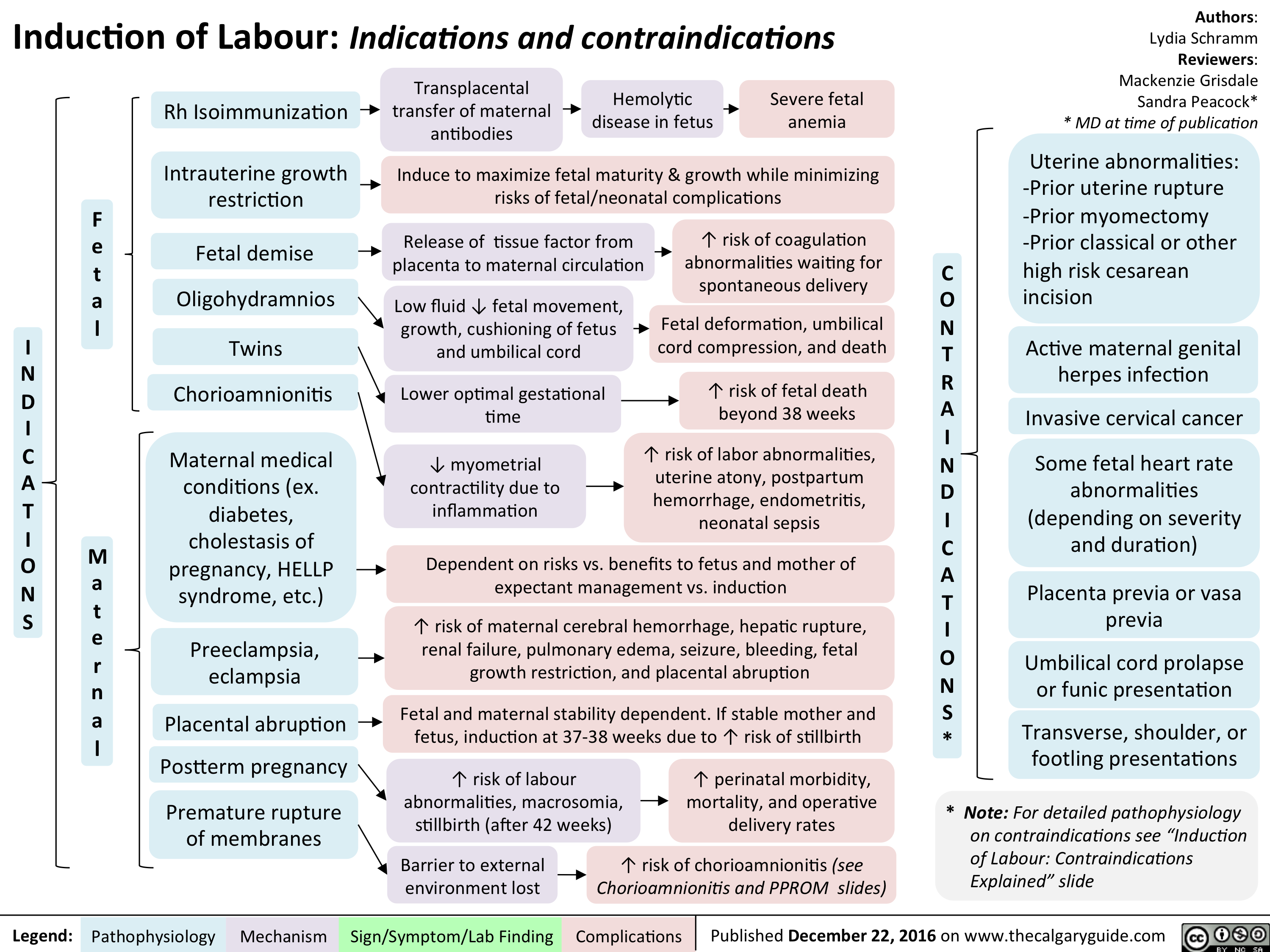
Stress Fracture v.5
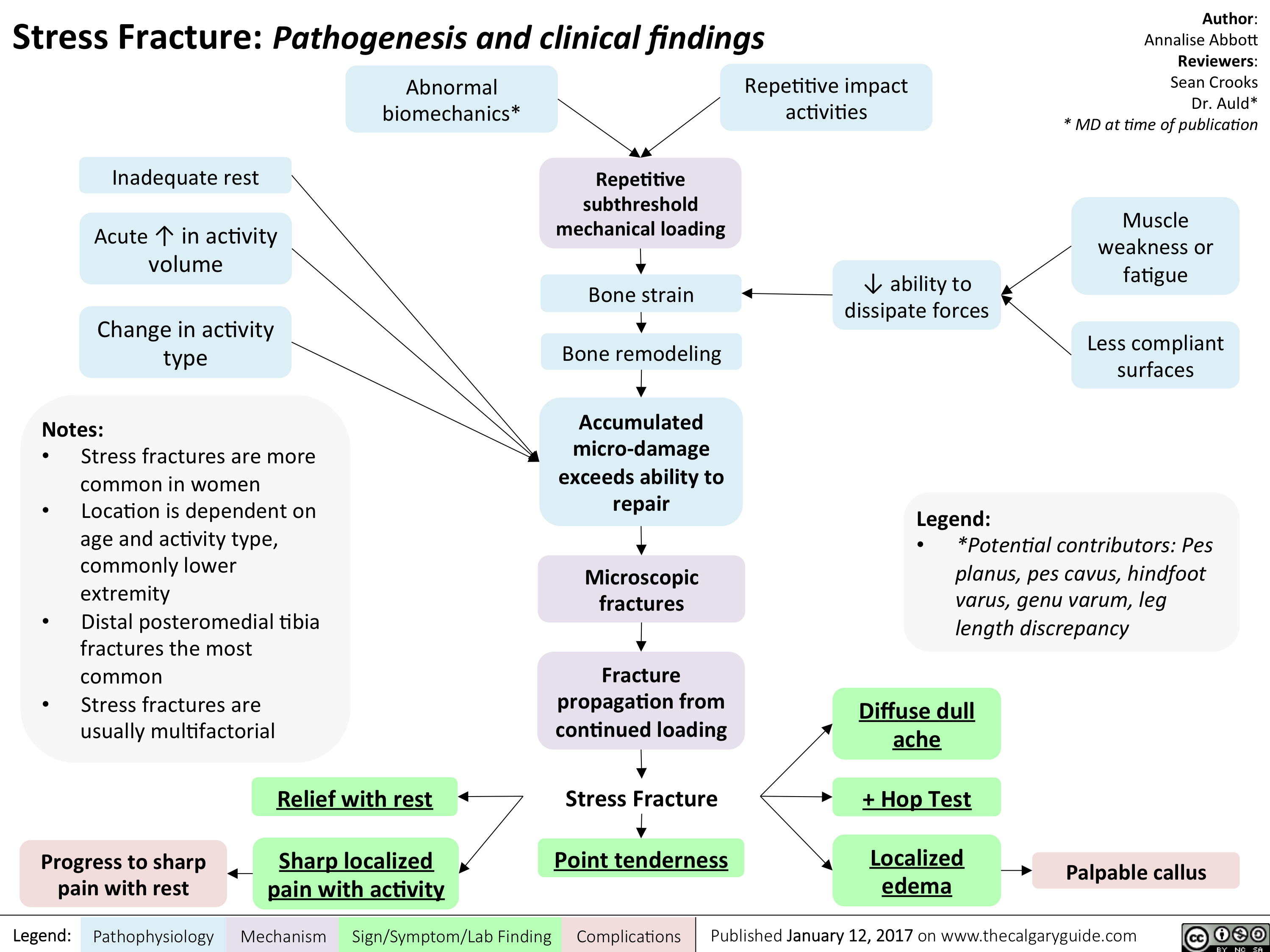
Placenta Accreta
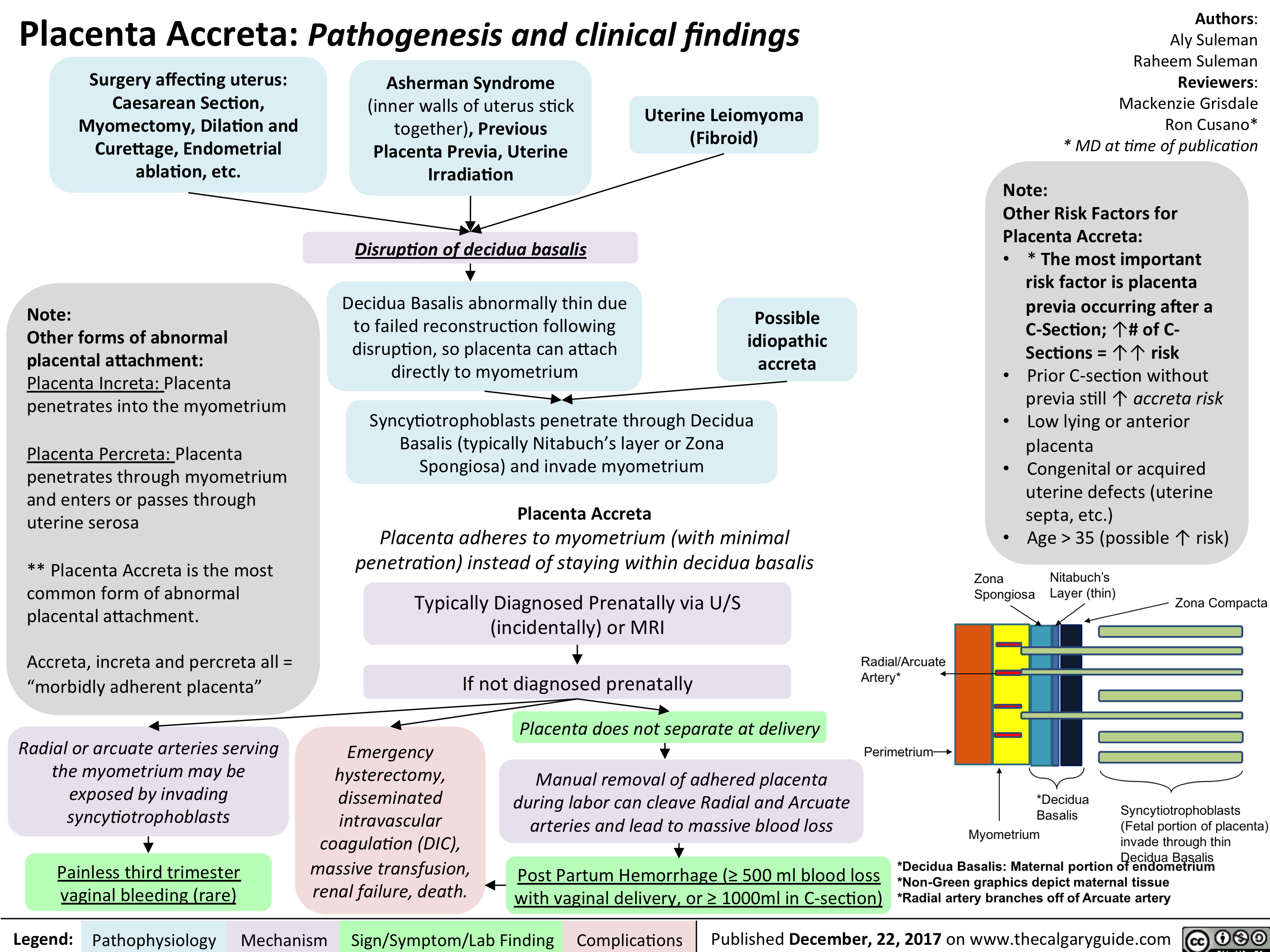
GDM: Risk factors and pathogenesis
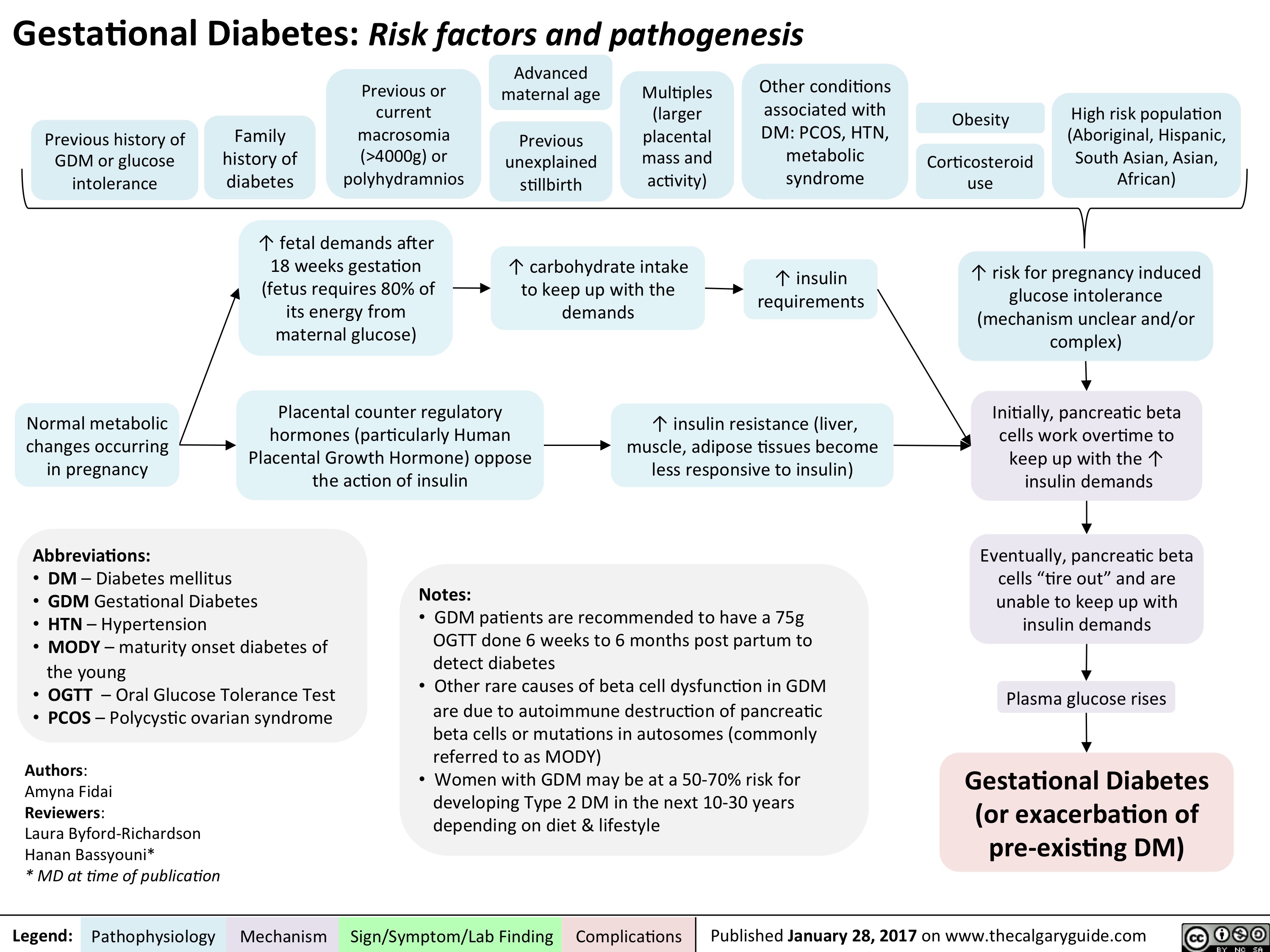
BPH Final
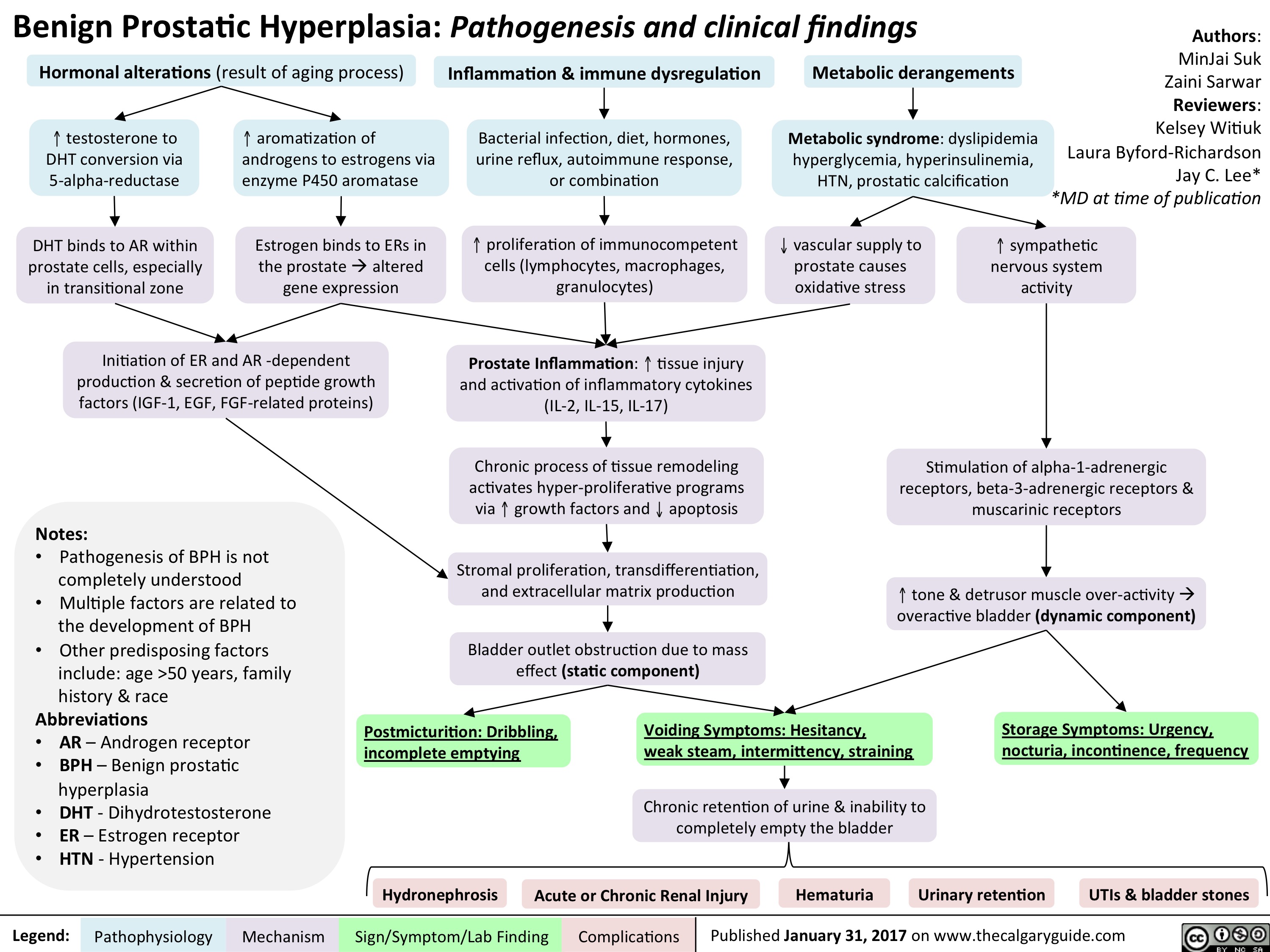
BPH Final
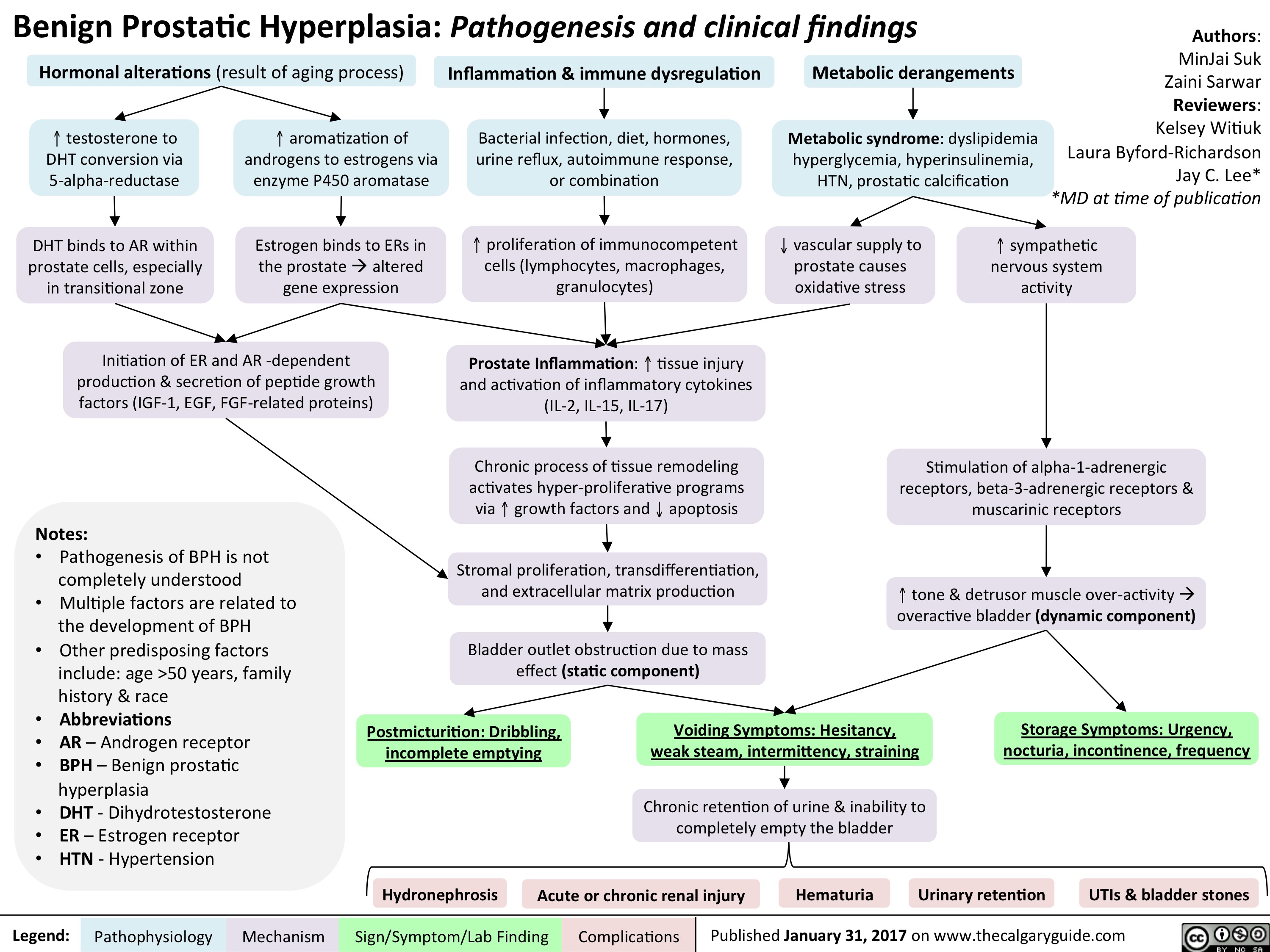
ASPD FINAL
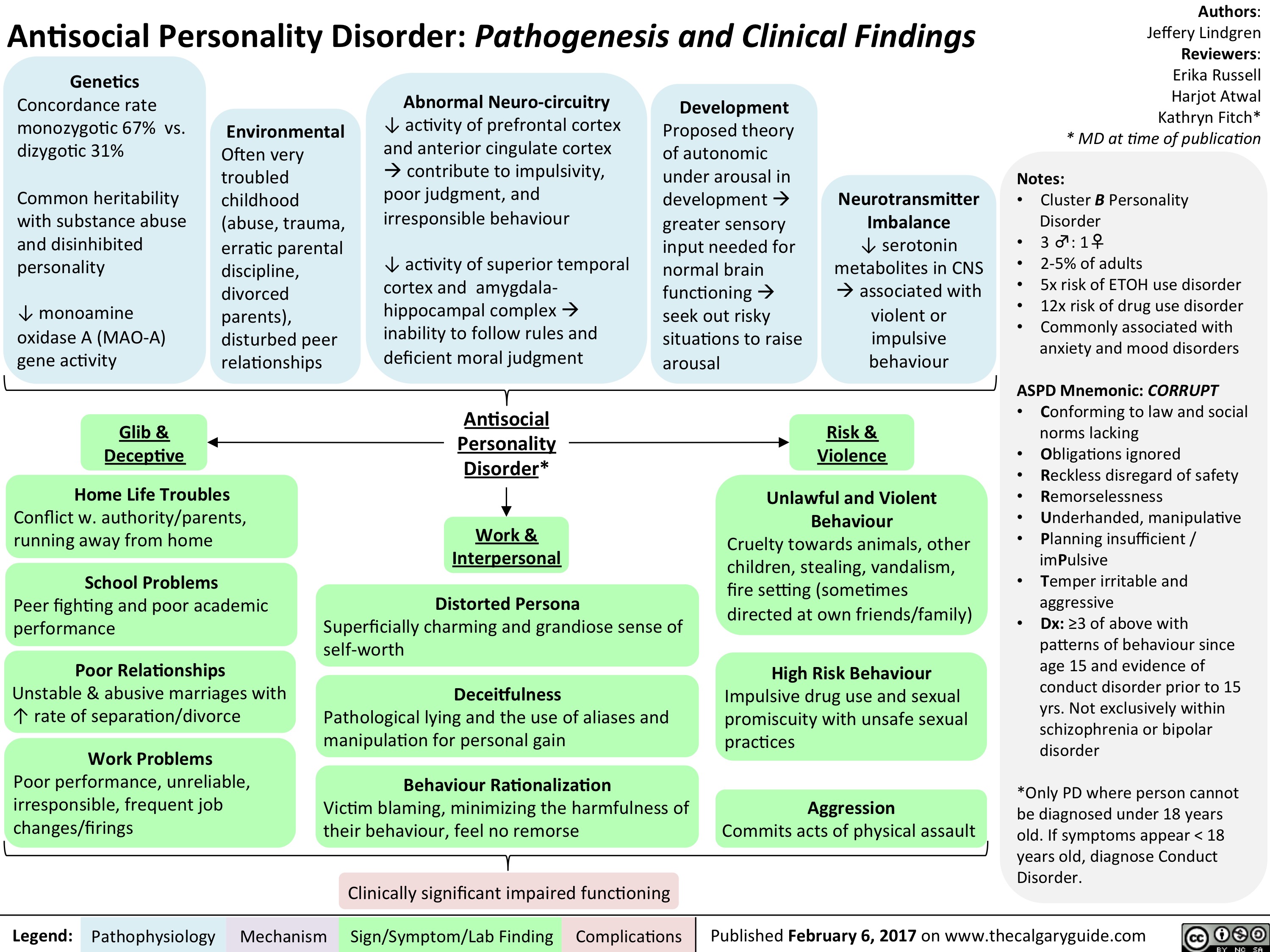
BPD FINAL
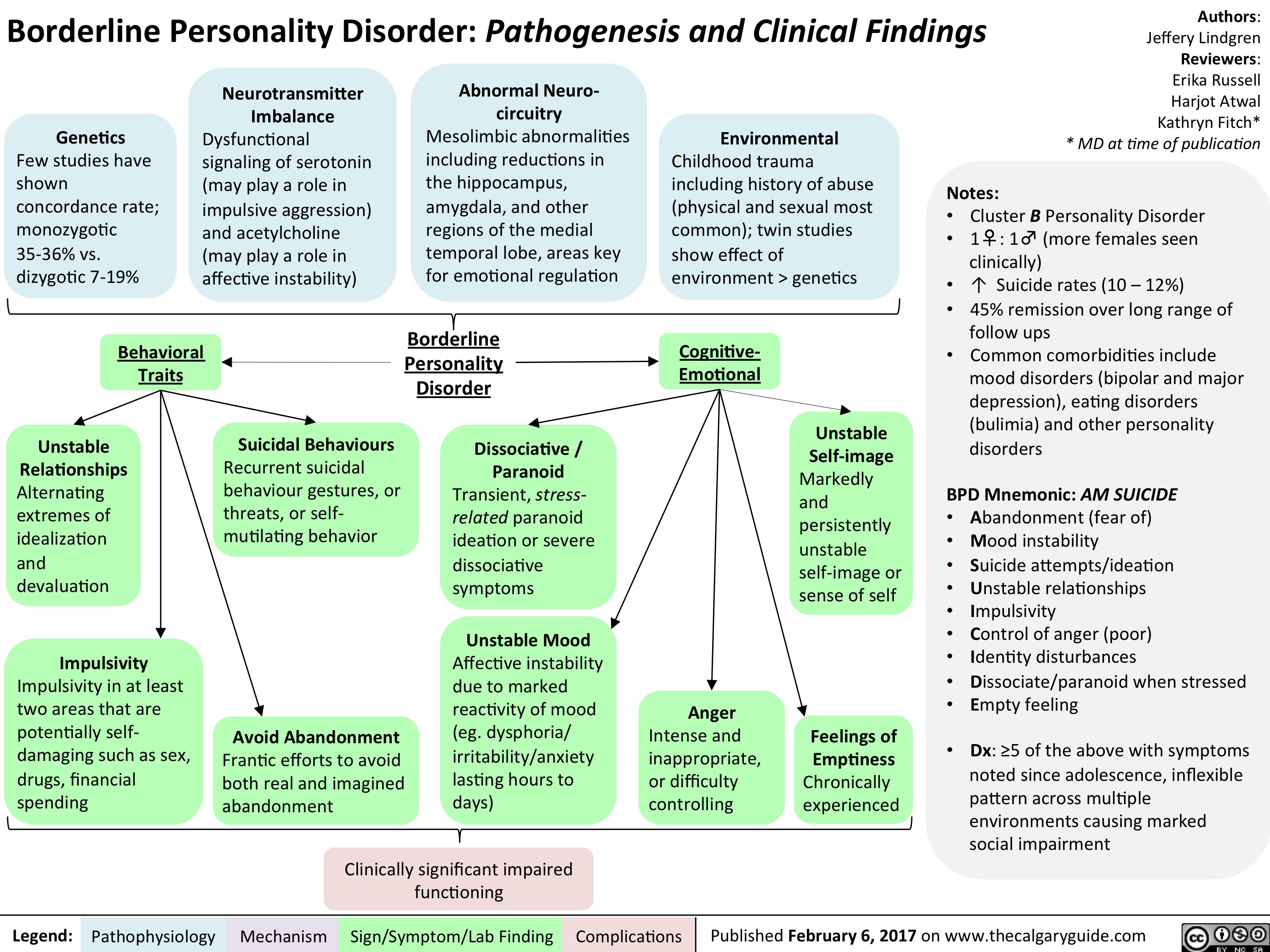
NPD FINAL
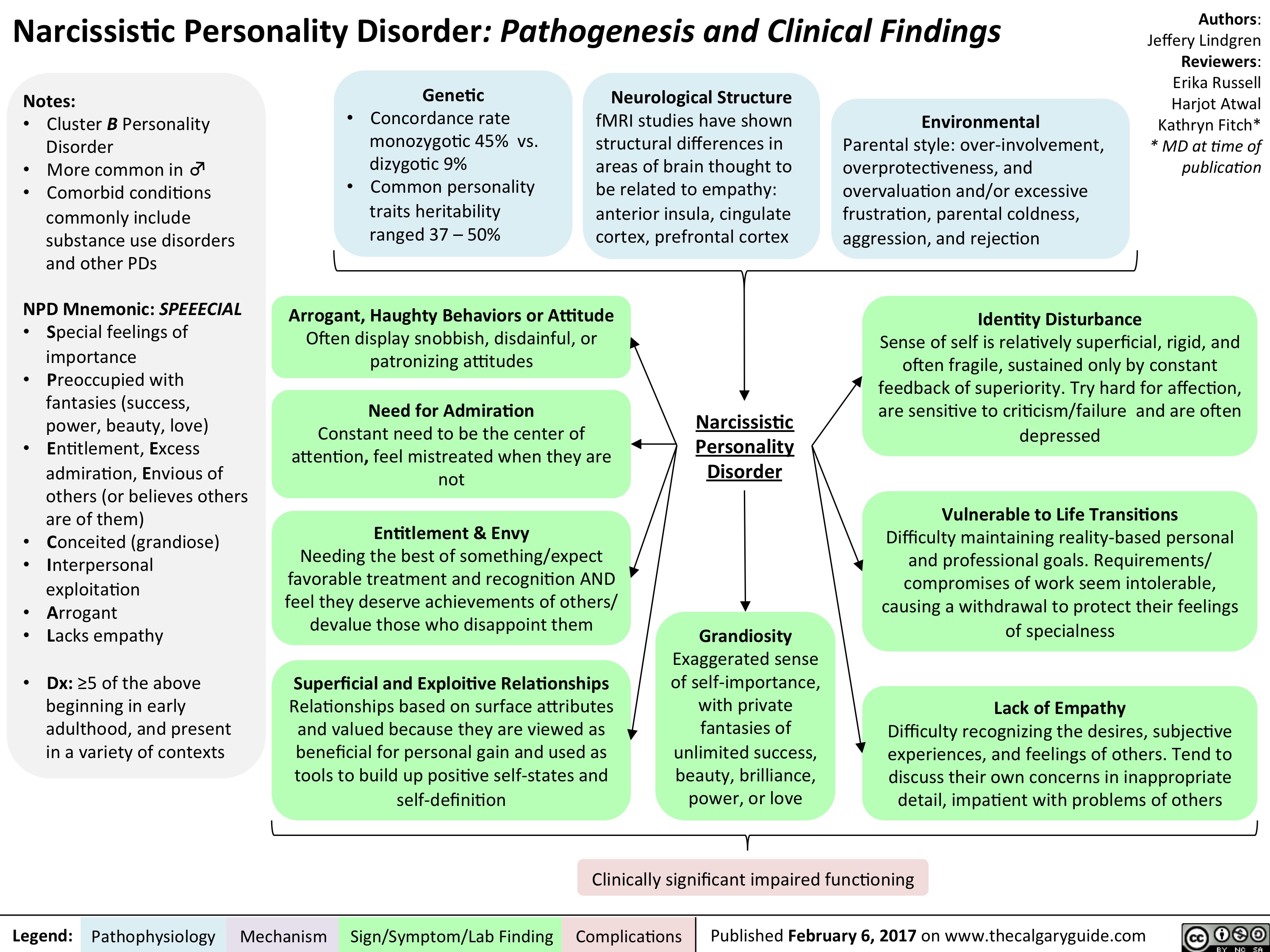
Lithium FINAL
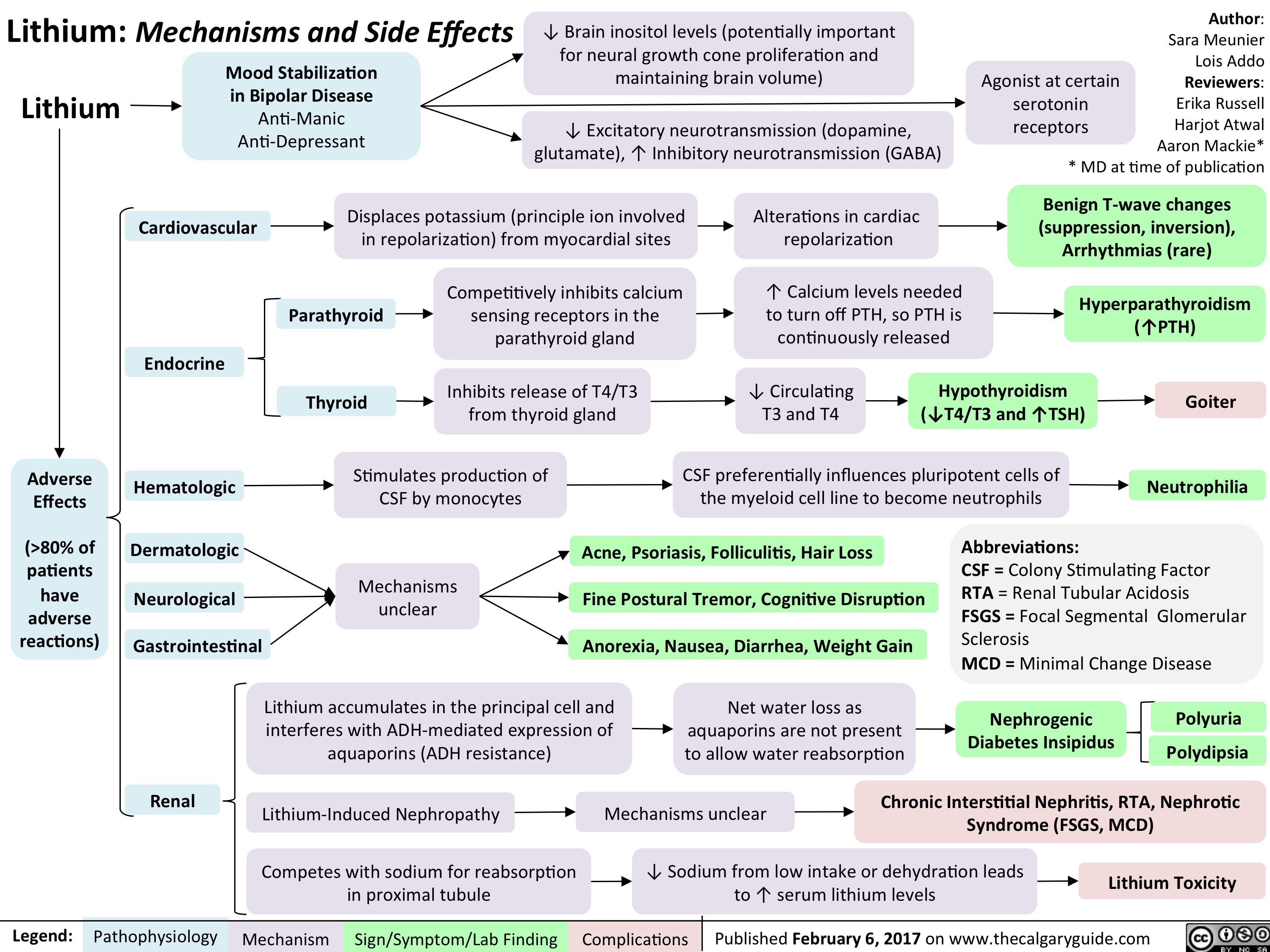
AF FINAL
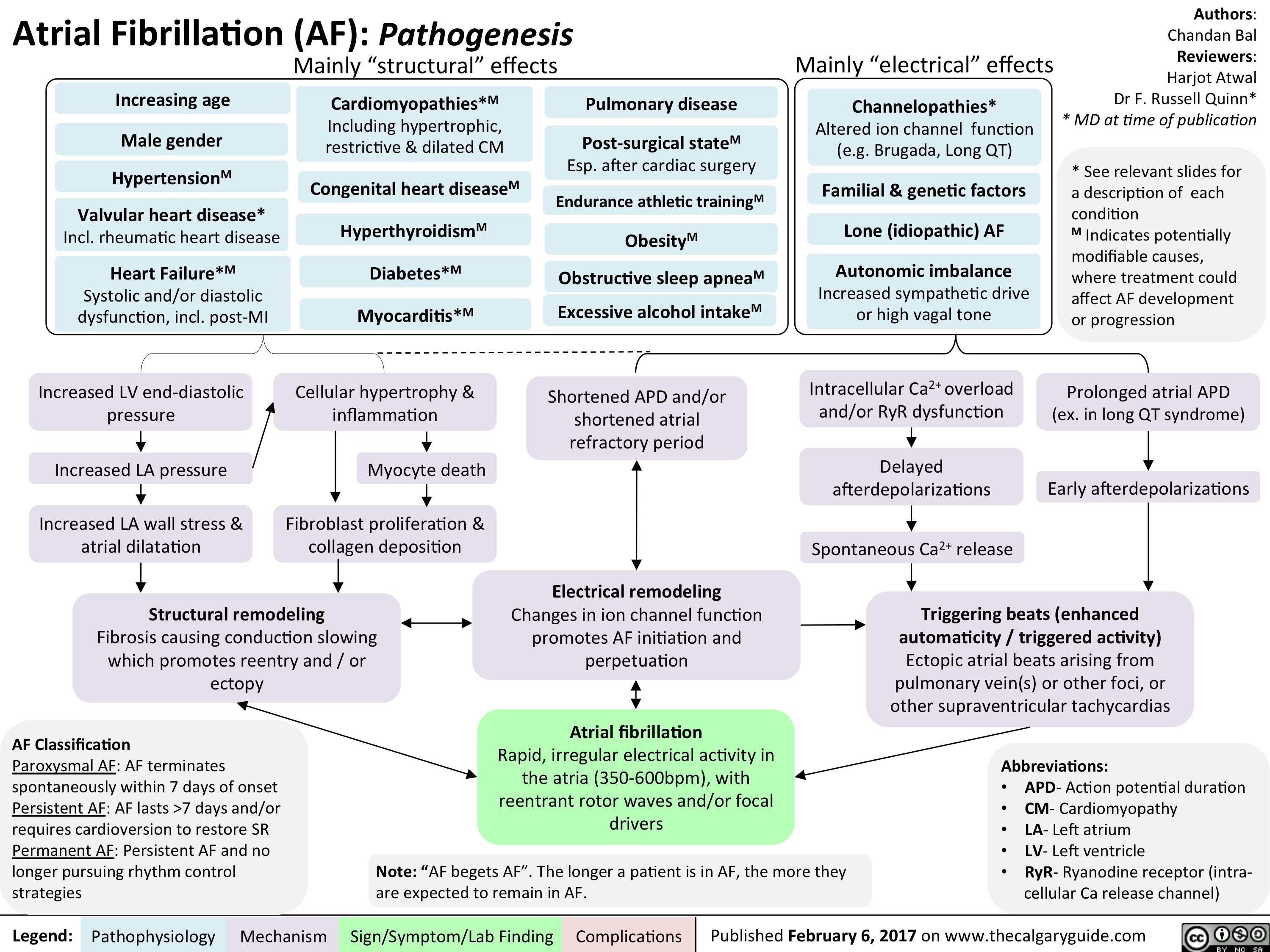
generalized-seizures-definitions

Lateral Medullary Syndrome FINAL
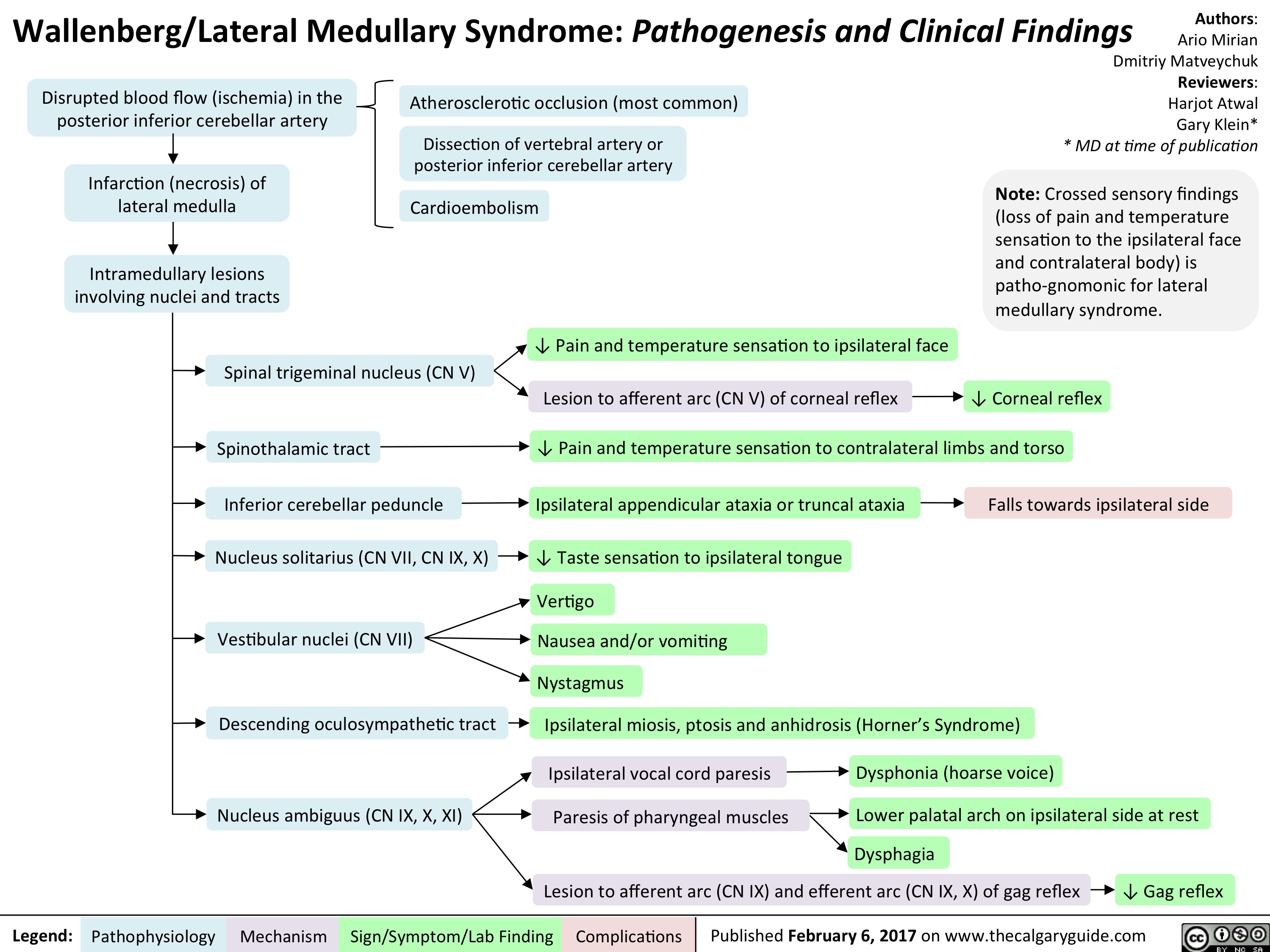
Subdural hematoma FINAL
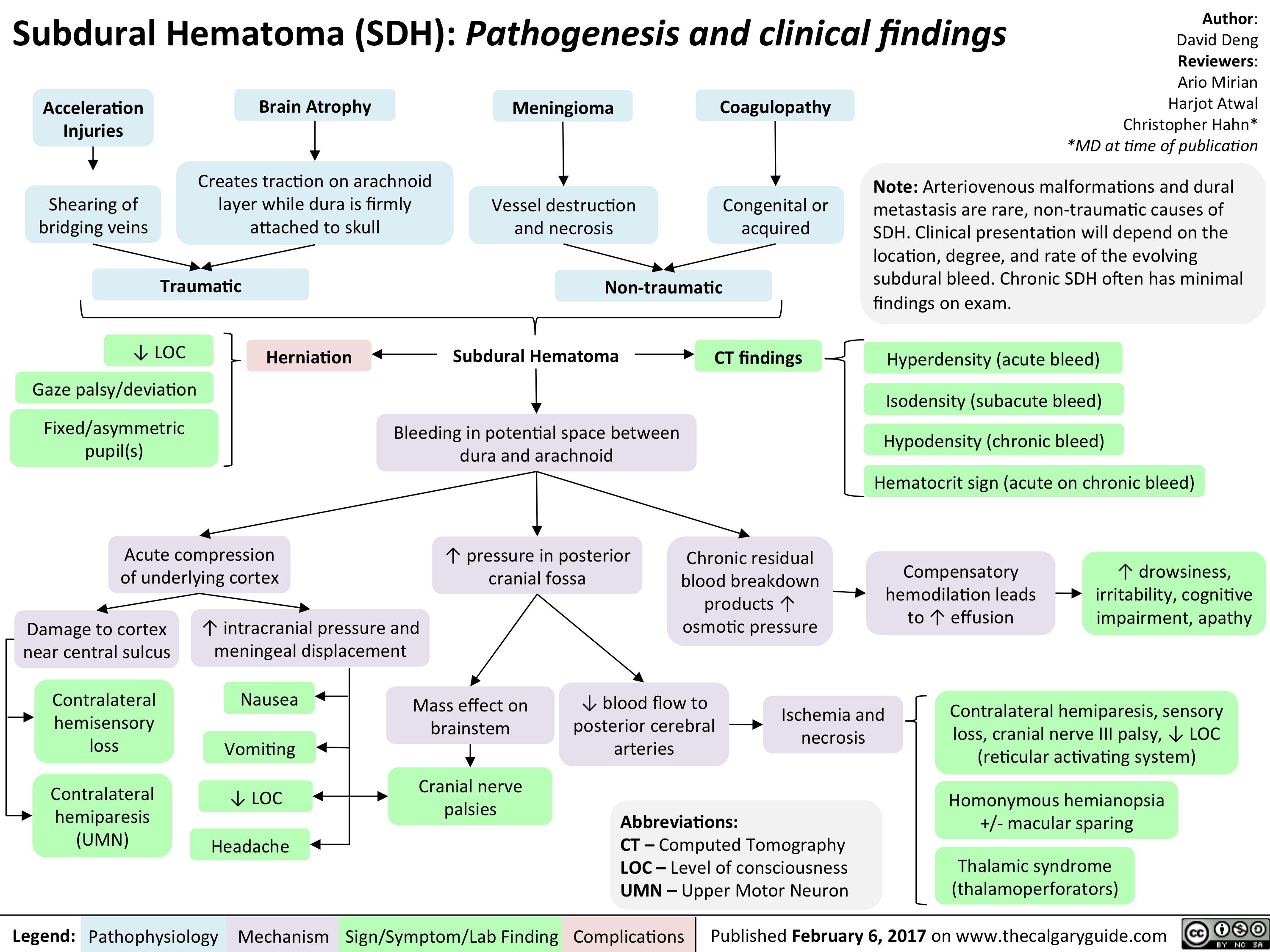
Staphylococcus Scalded Skin Syndrome FINAL
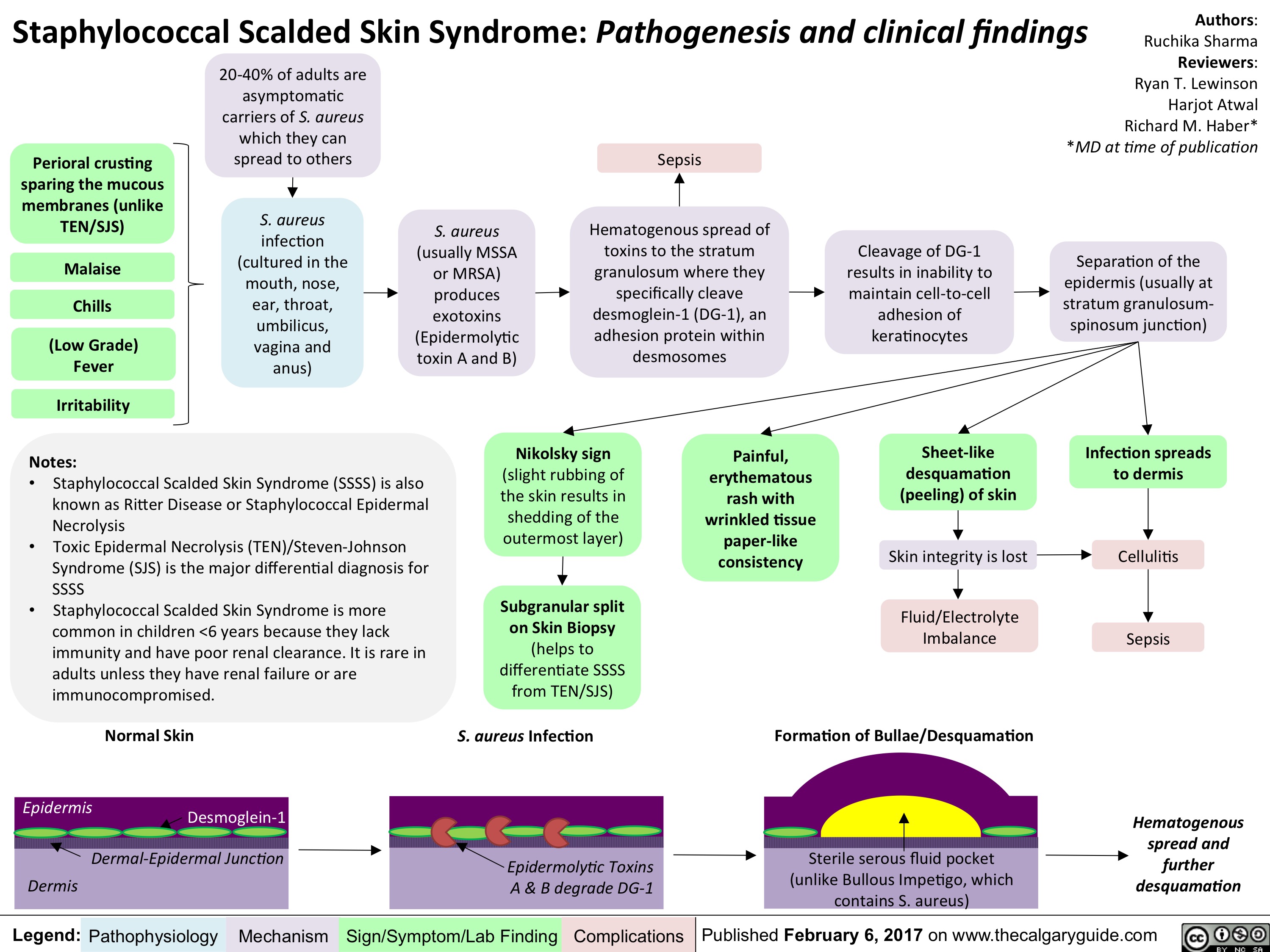
Manion contraception MOAs
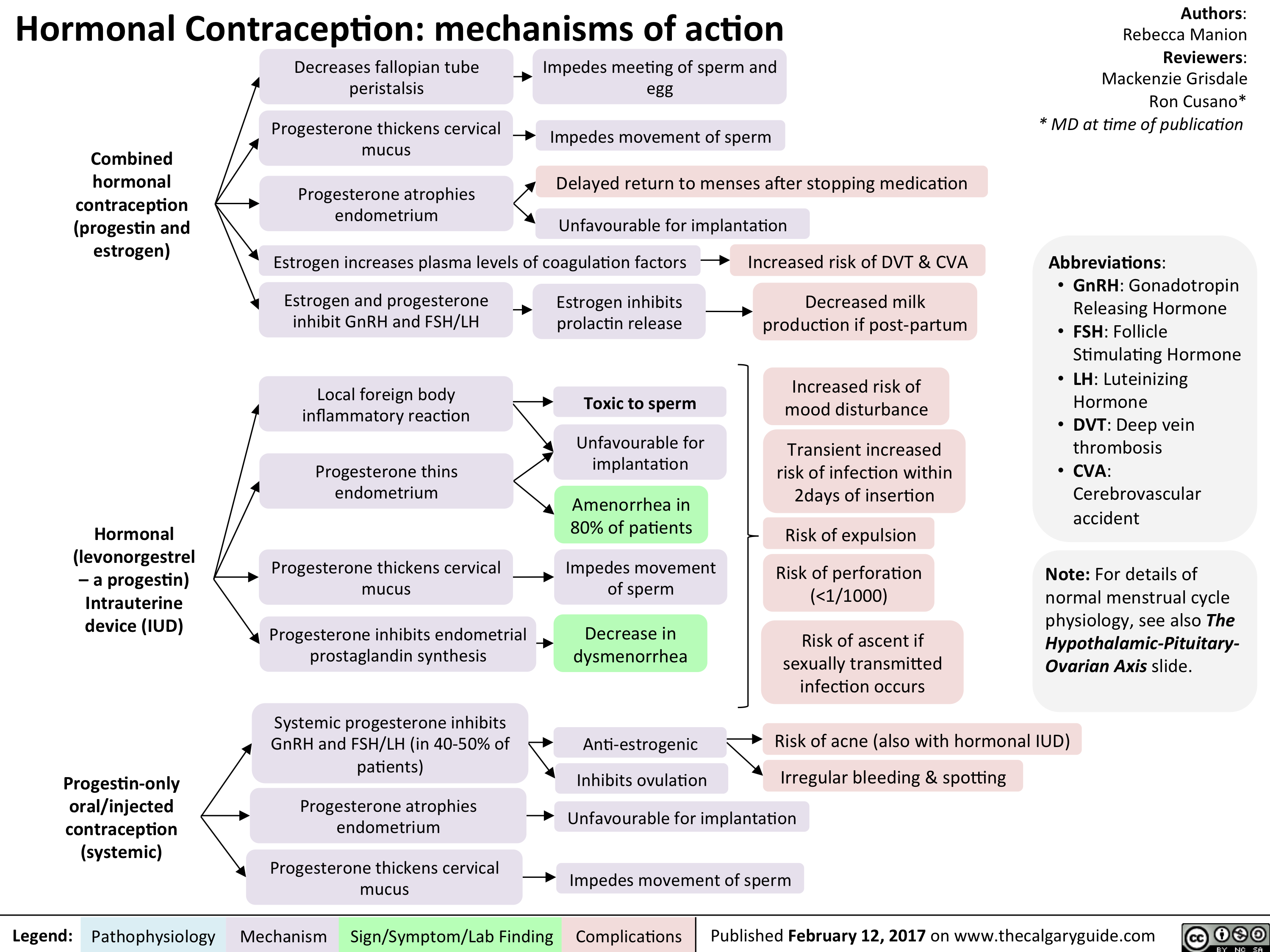
Manion contraception MOAs2
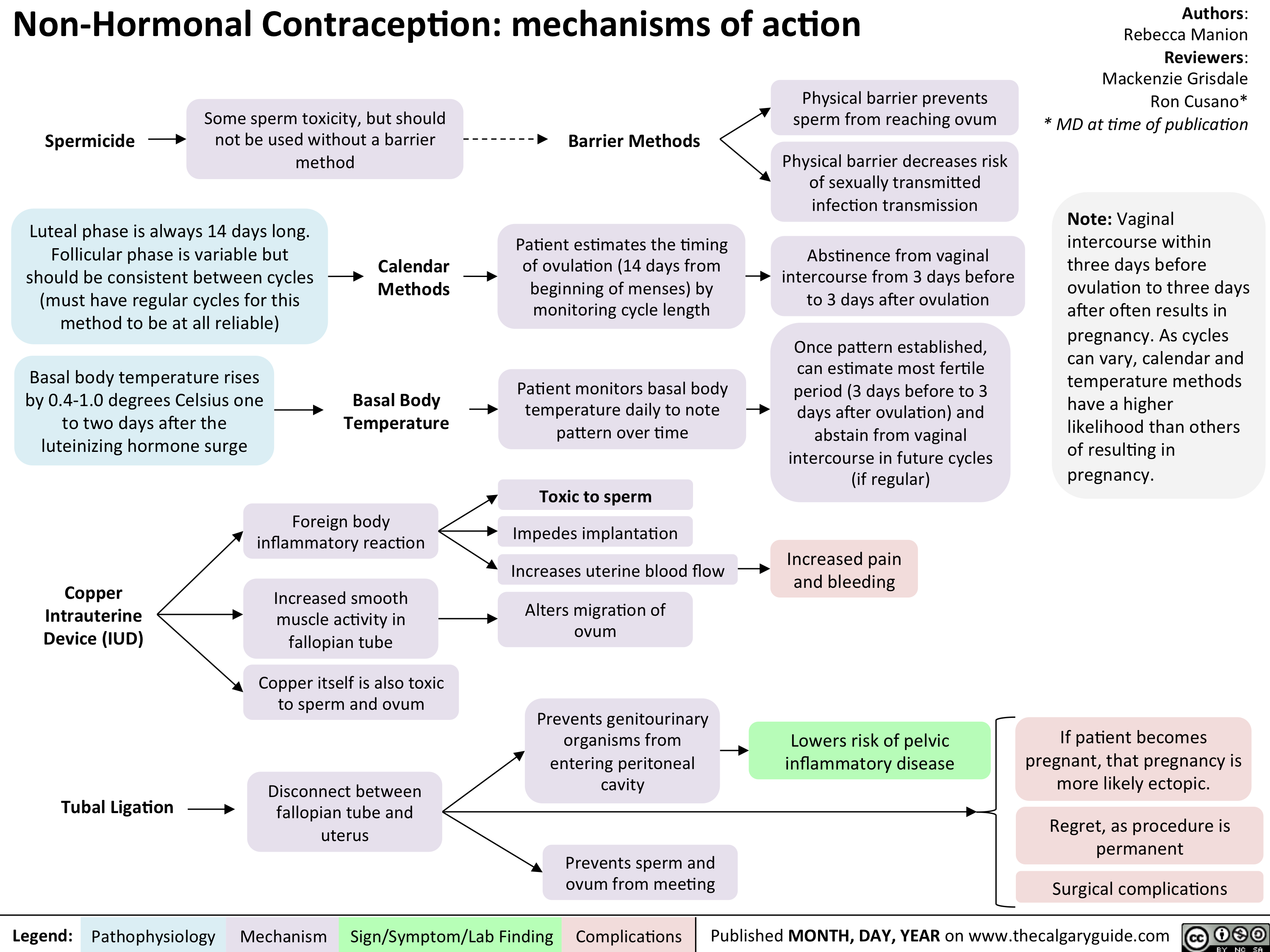
Common meds contra in Preg
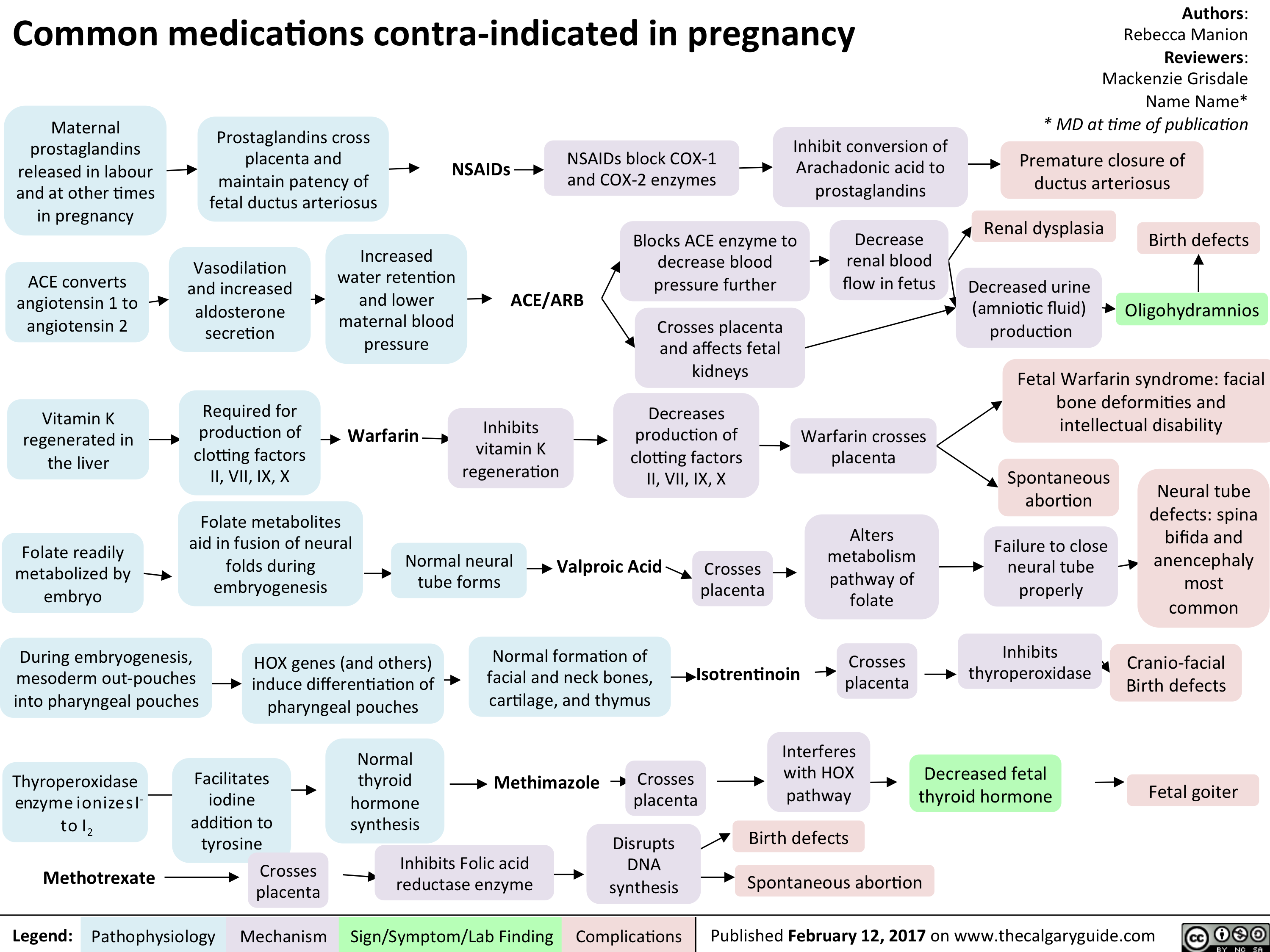
Non hormonal
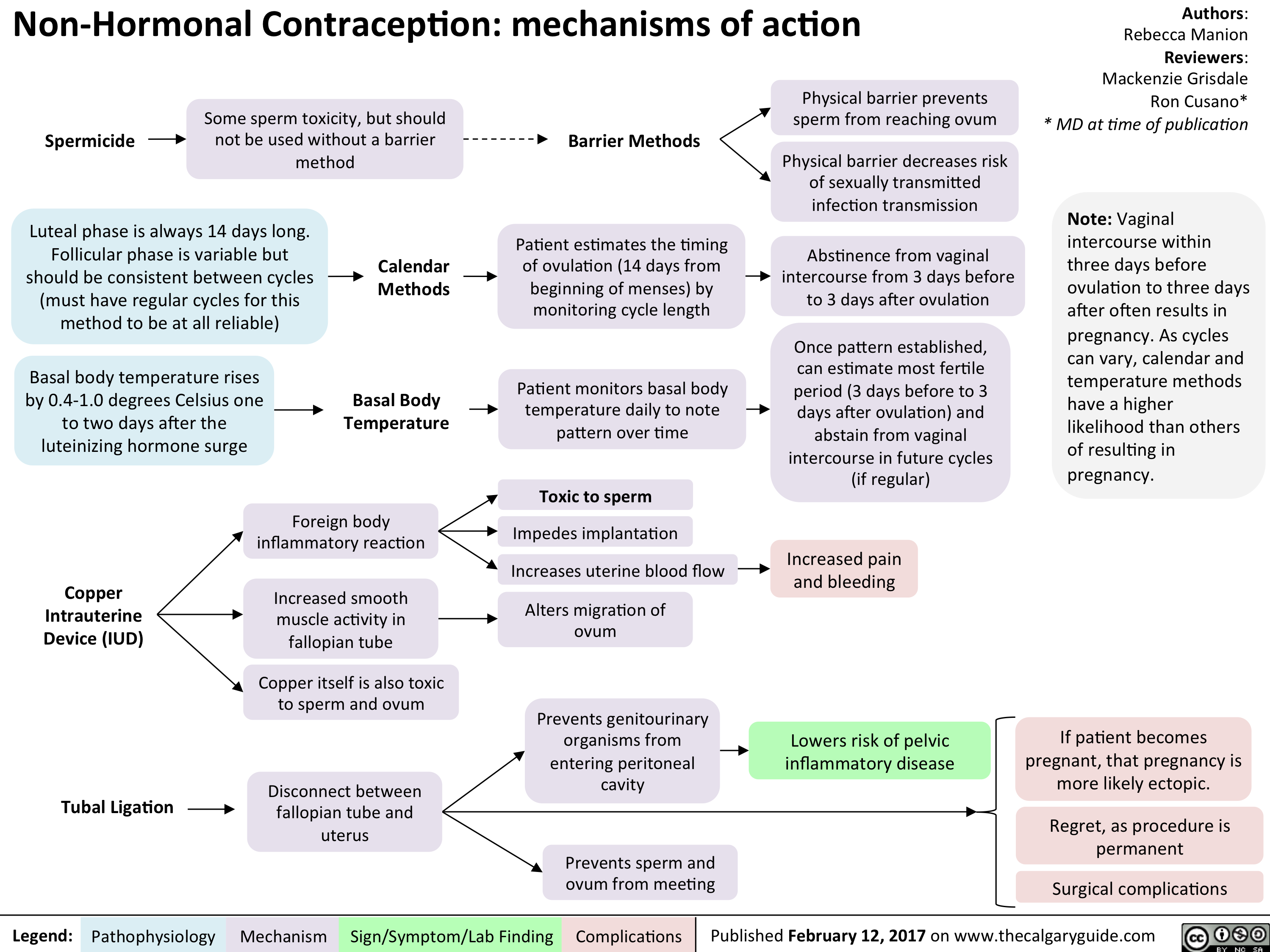
Vasa Previa
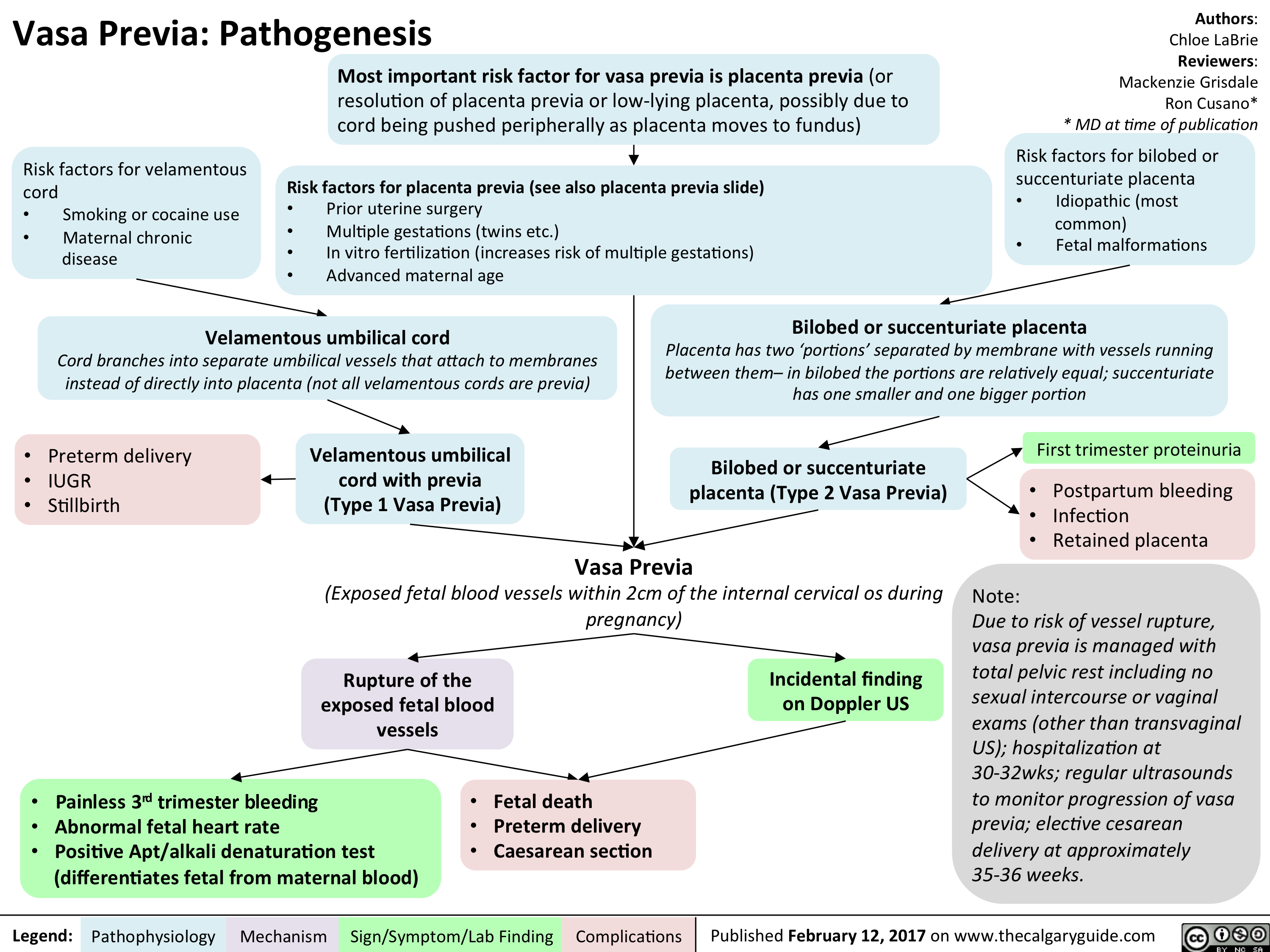
ASPD FINAL
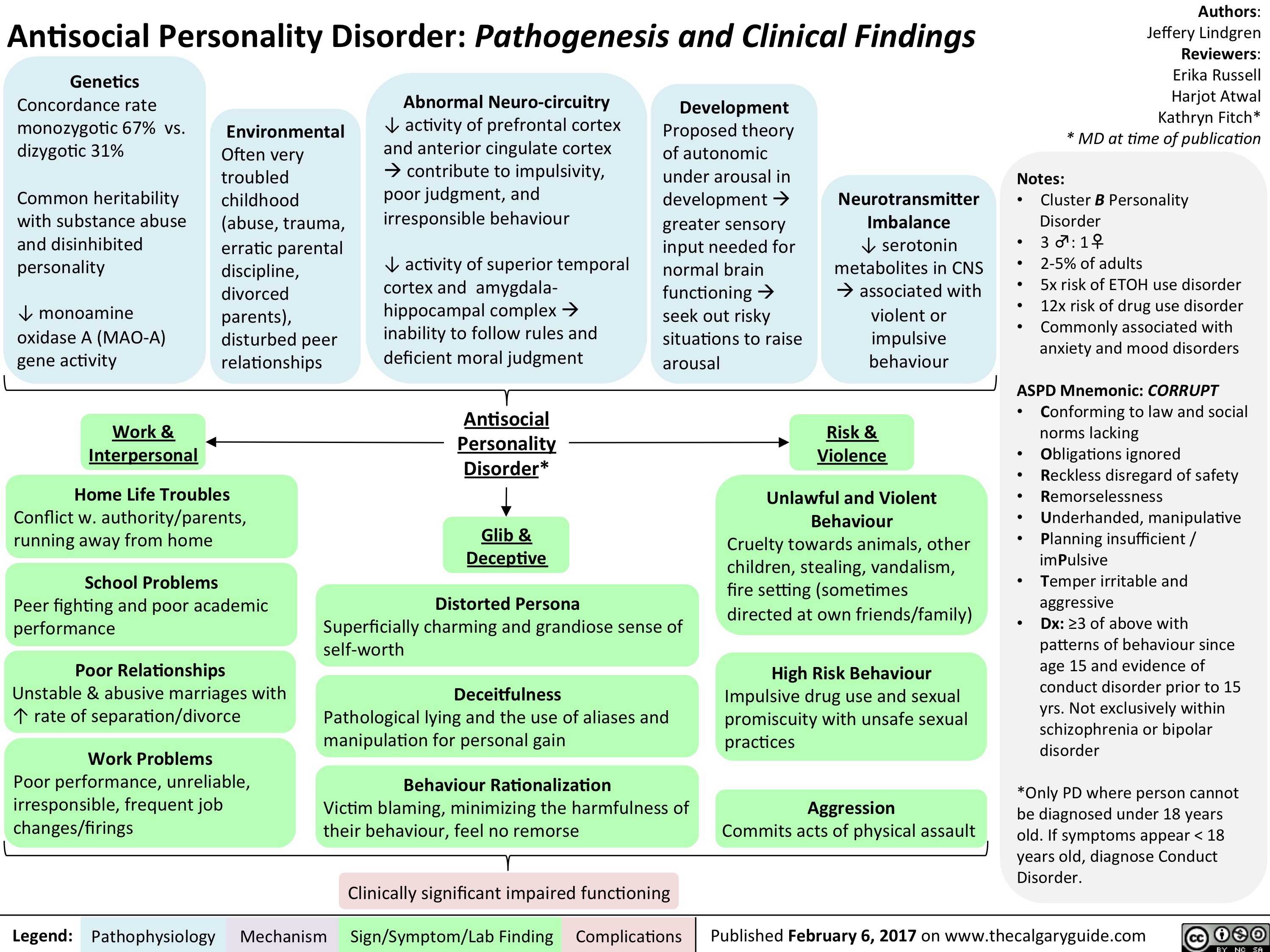
hypertension-in-pregnancy-overview-of-definitions
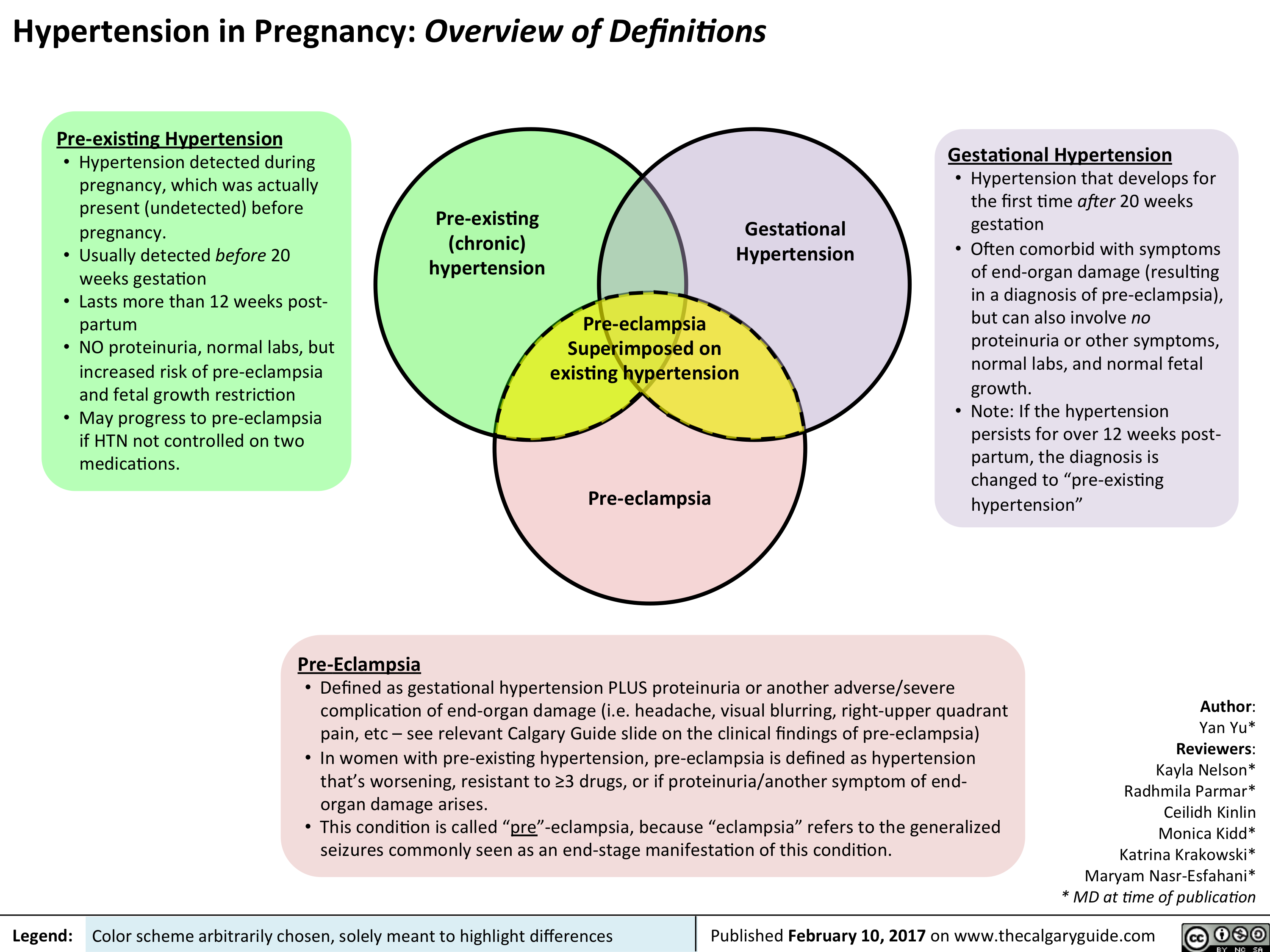
Yu Yan - Pre-eclampsia pathogenesis - publish
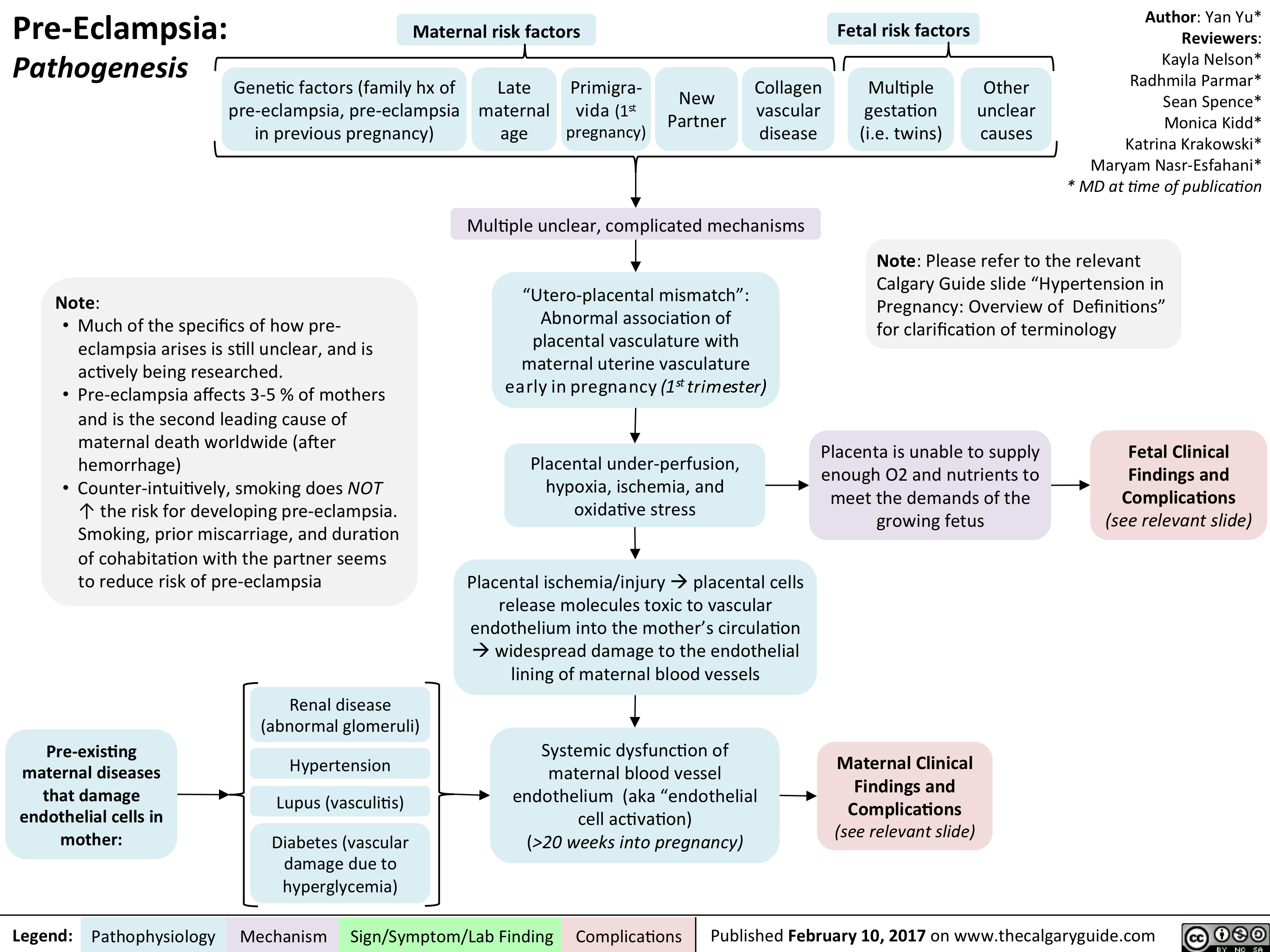
Yu Yan - Pre-eclampsia Maternal Complications - publish
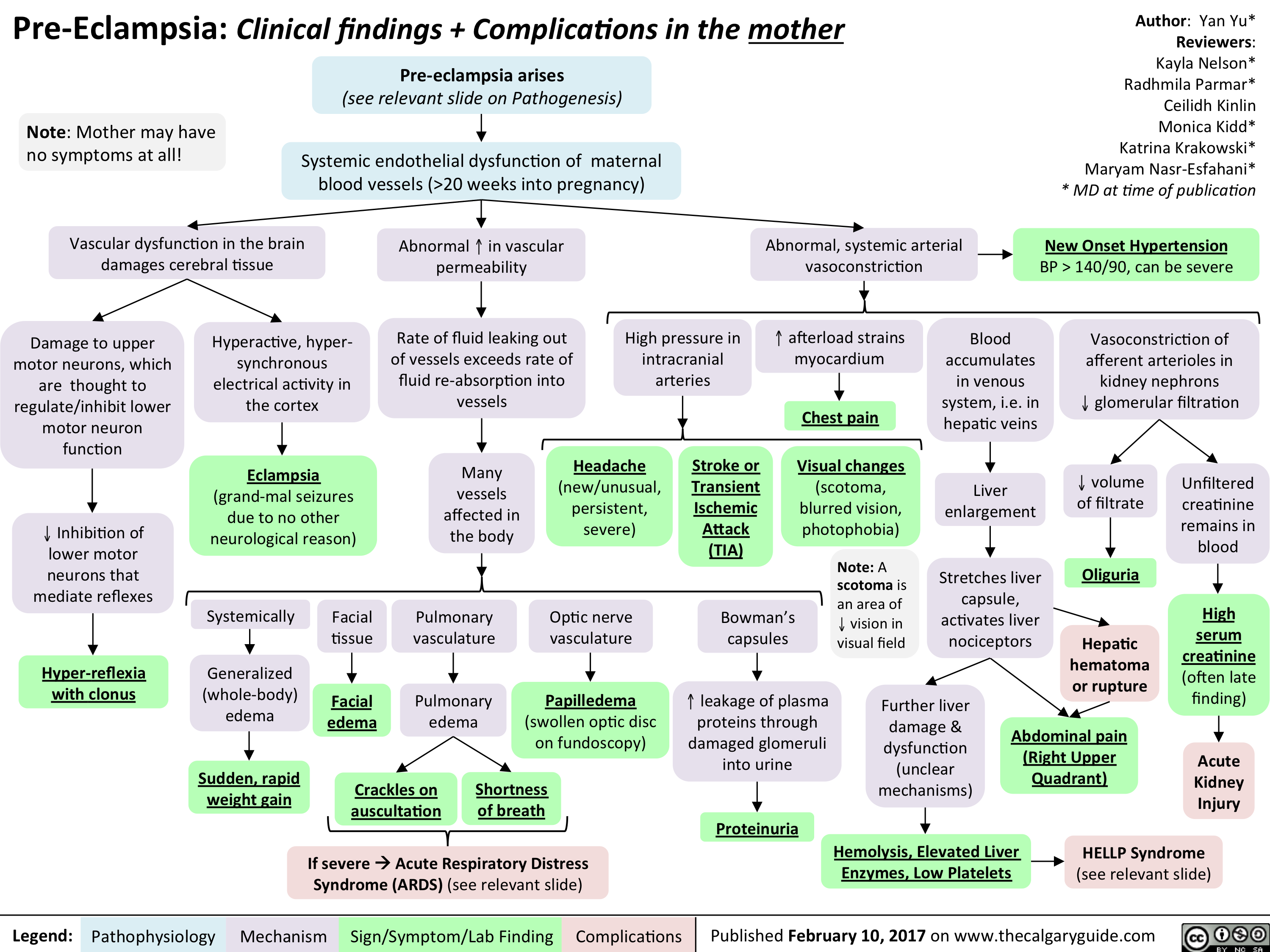
Yu Yan - Pre-eclampsia Fetal Complications - publish
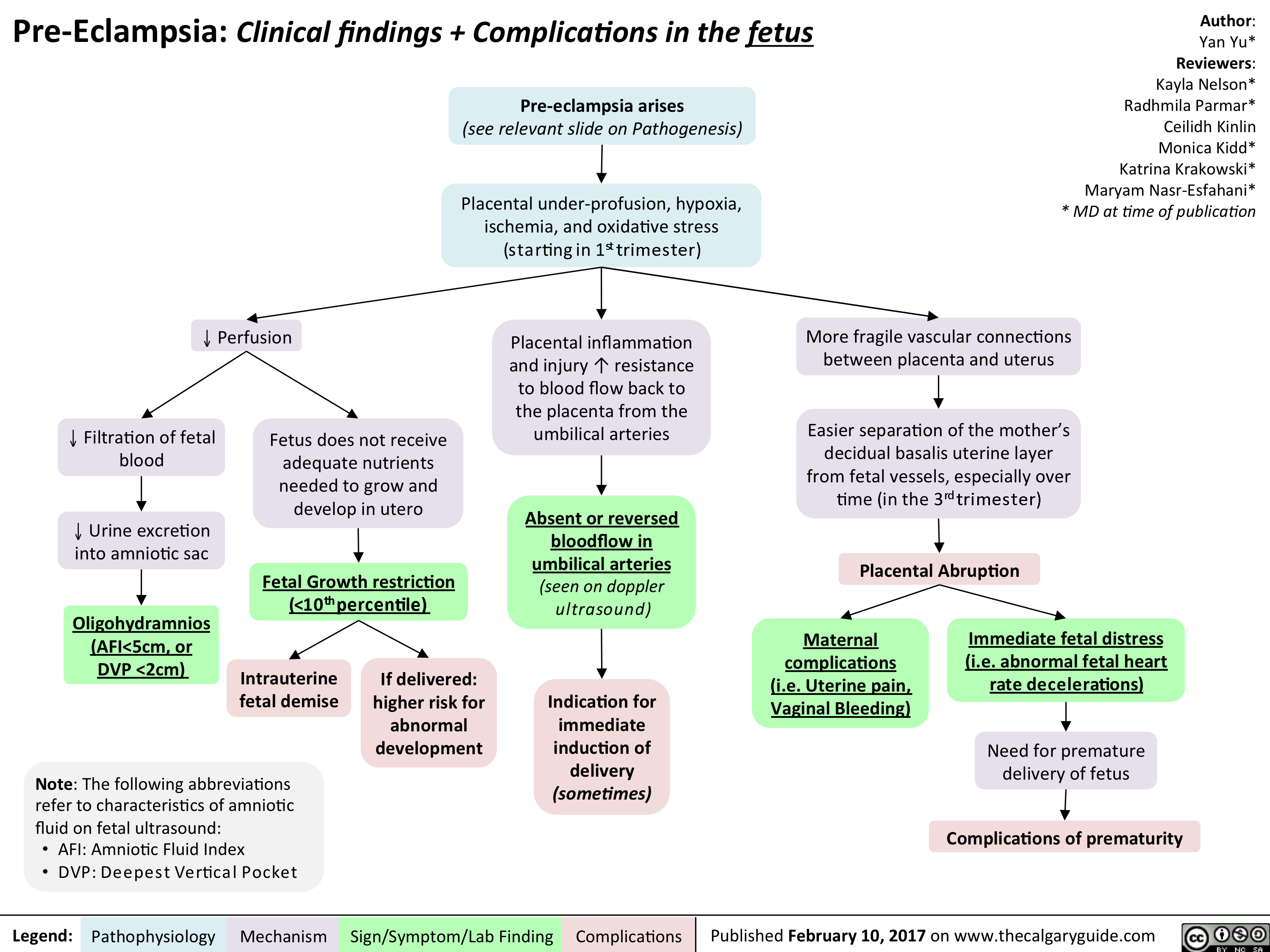
Altered Metabolism in the ICU
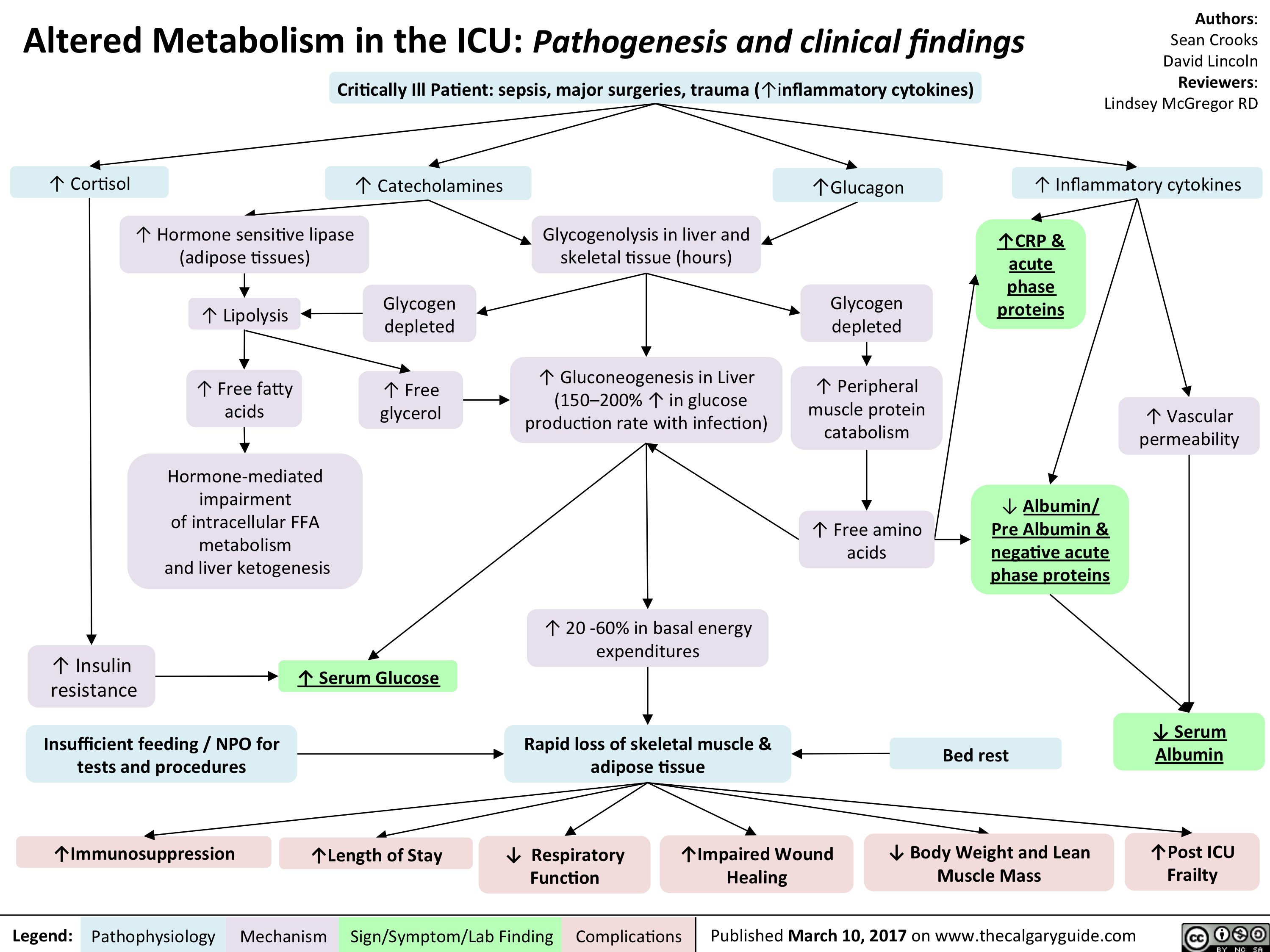
Altered Metabolism in the ICU- Pathogenesis and clinical findings
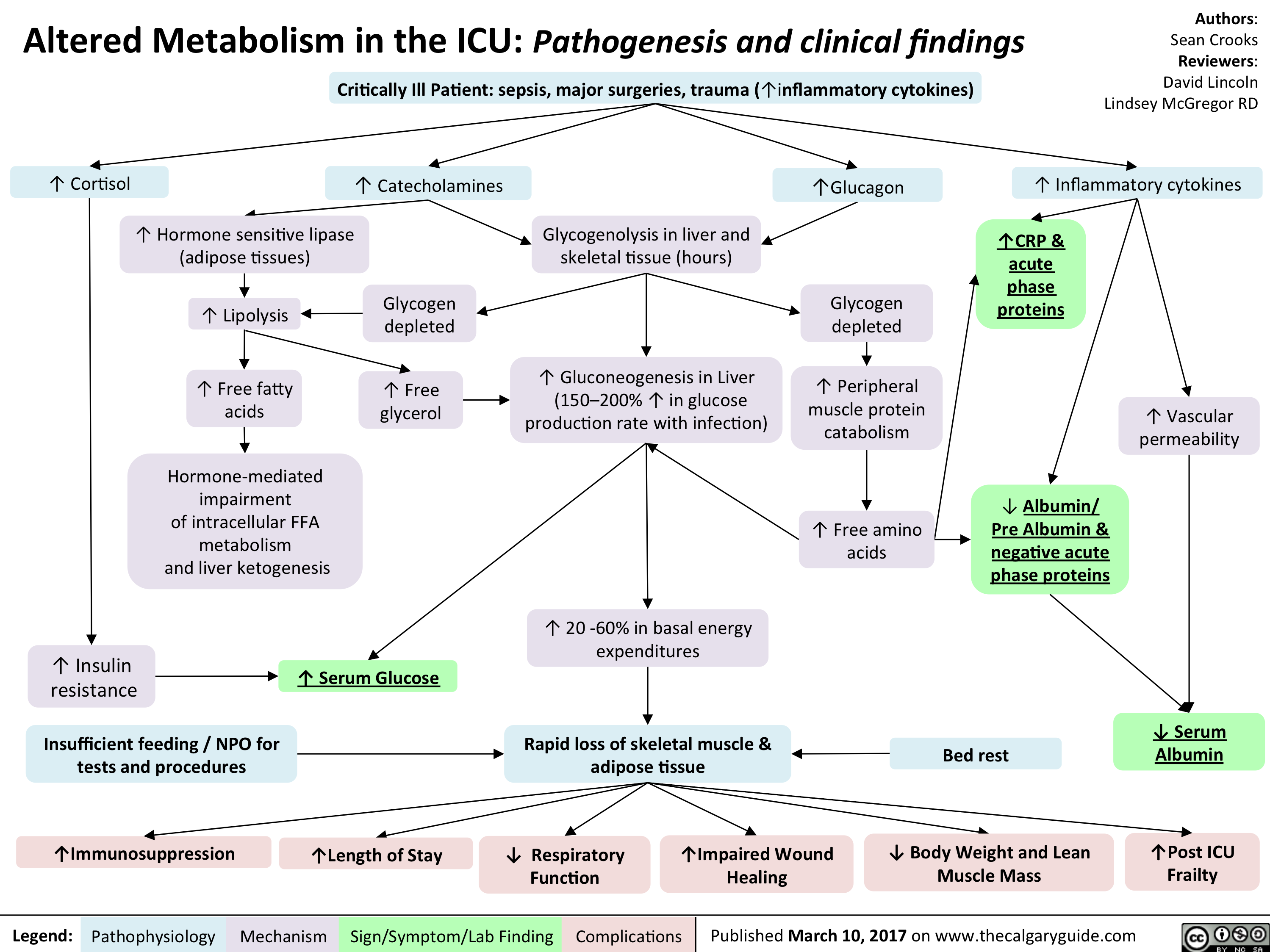
Mental Status Exam

Addiction Long-term Consequences

Addiction Pathogenesis
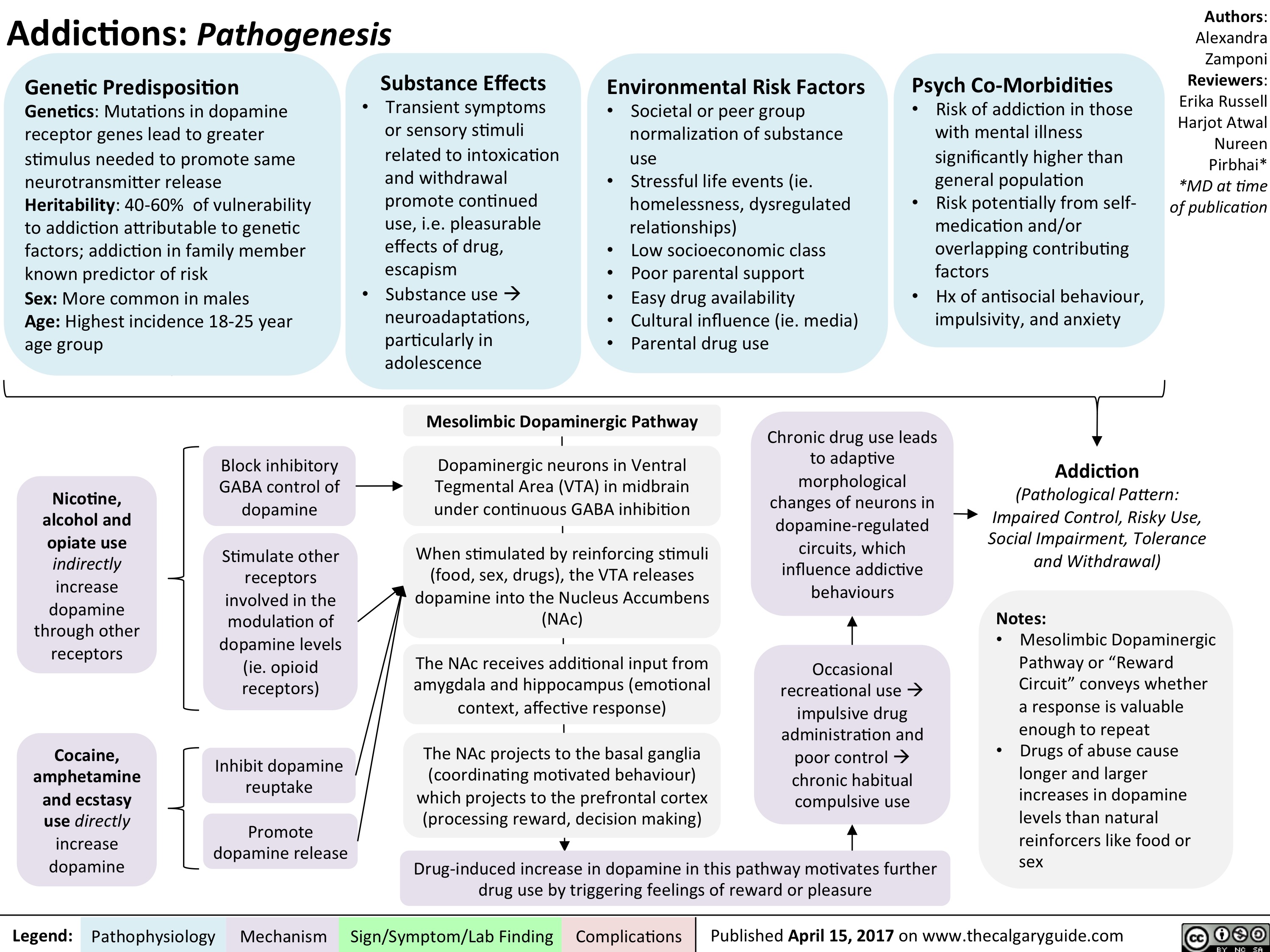
Non-accidental Burns
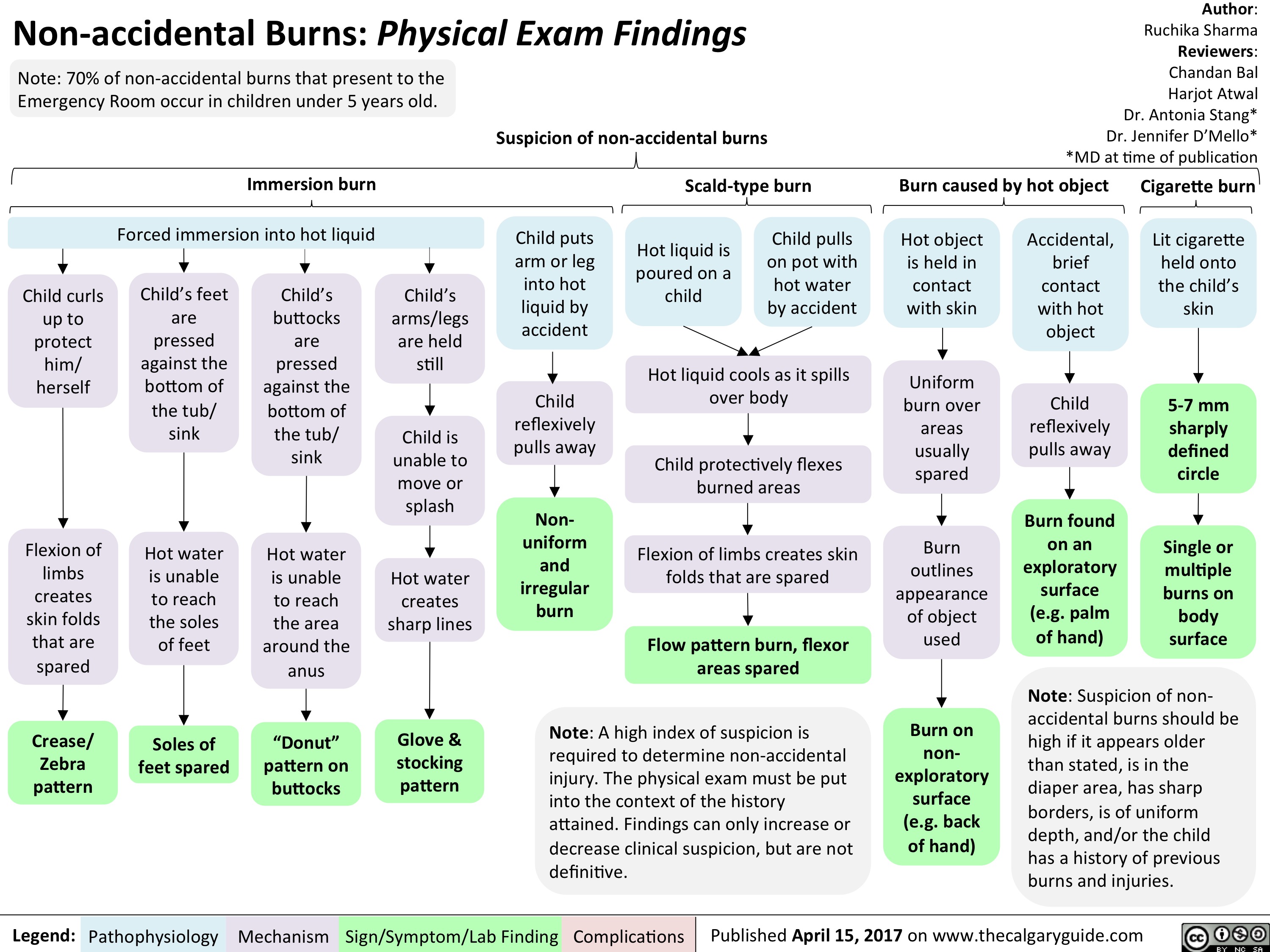
SLE-GI Manifestations
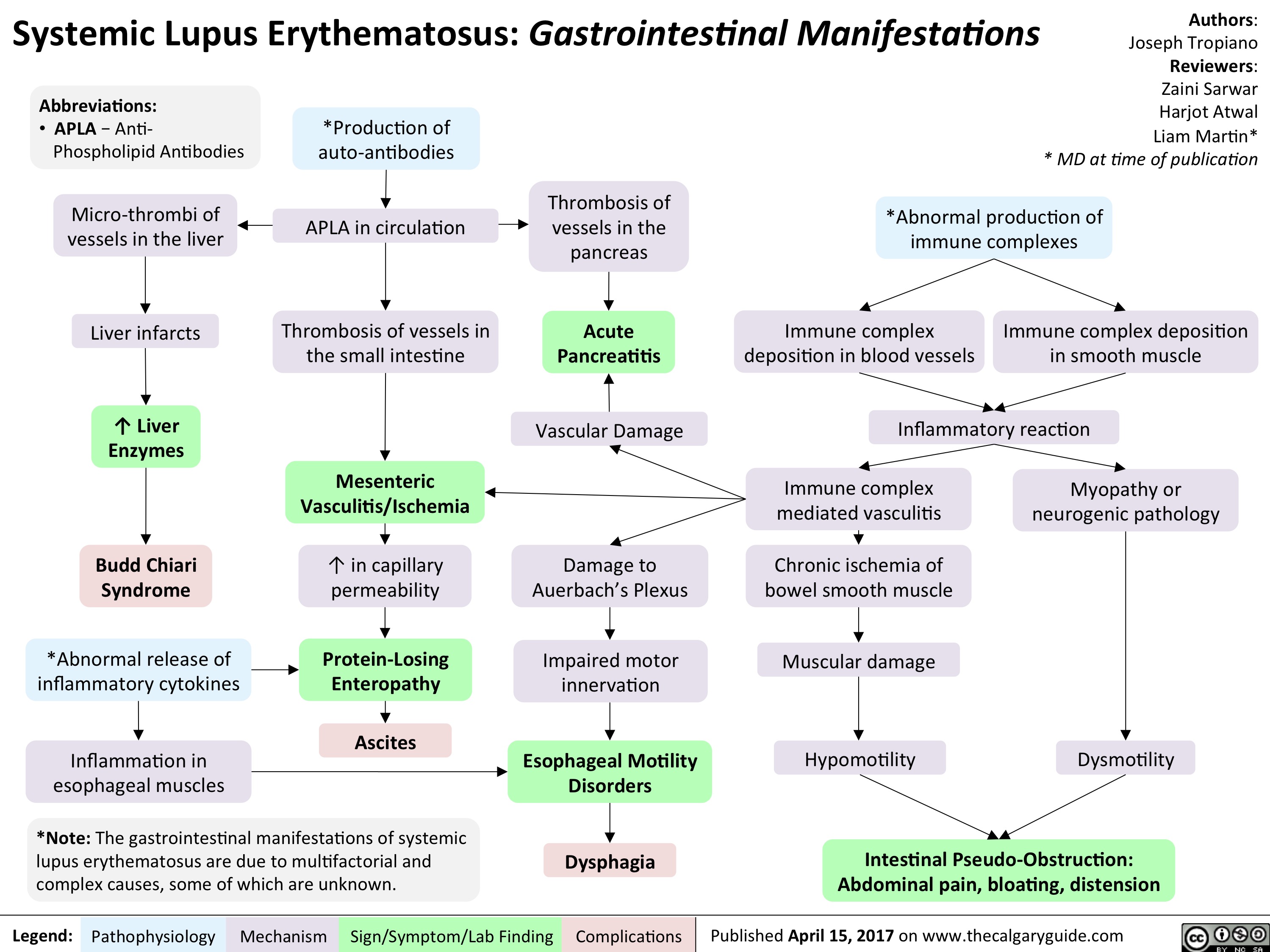
Testicular Torsion
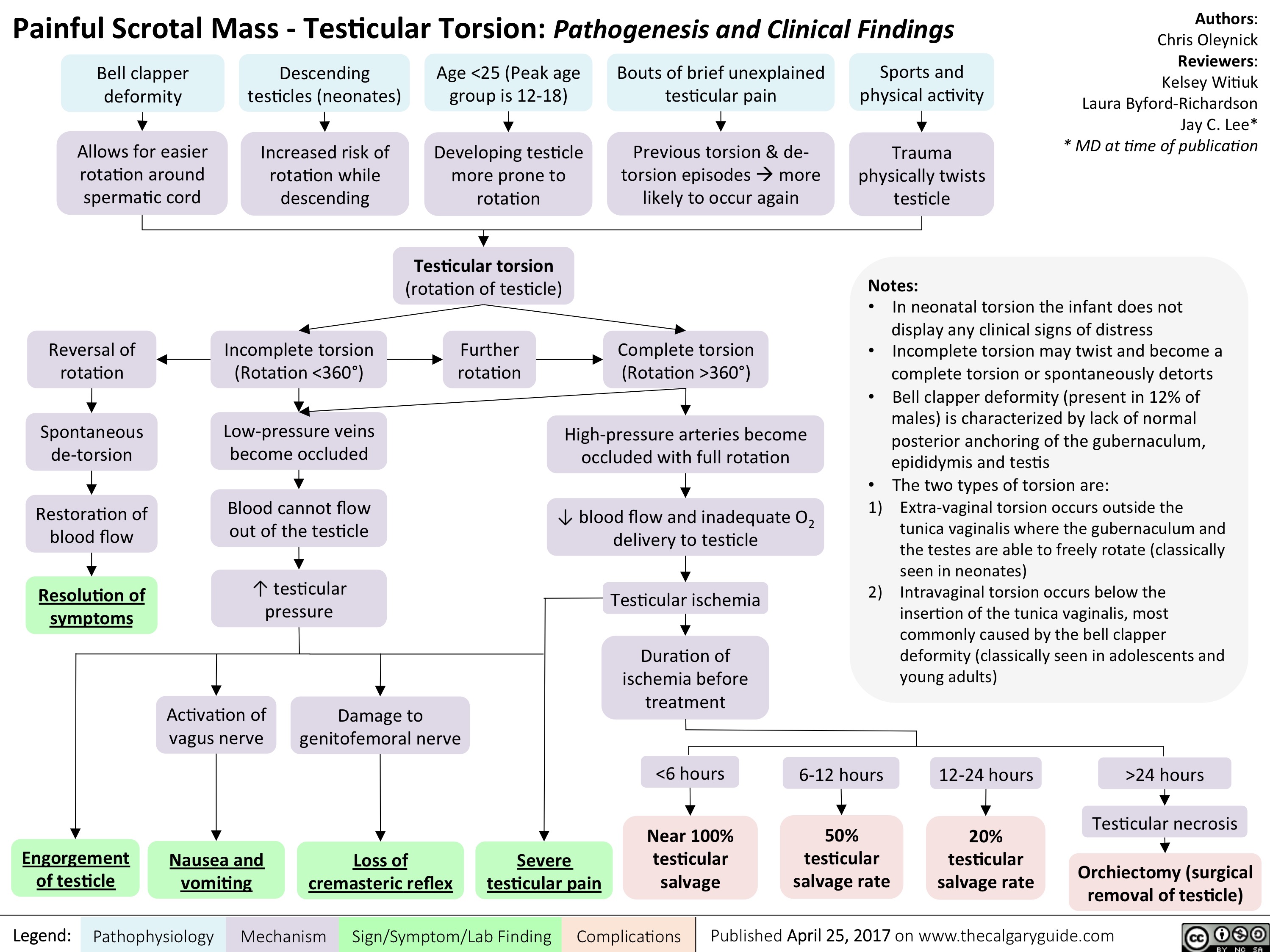
Acquired Hydrocephalus
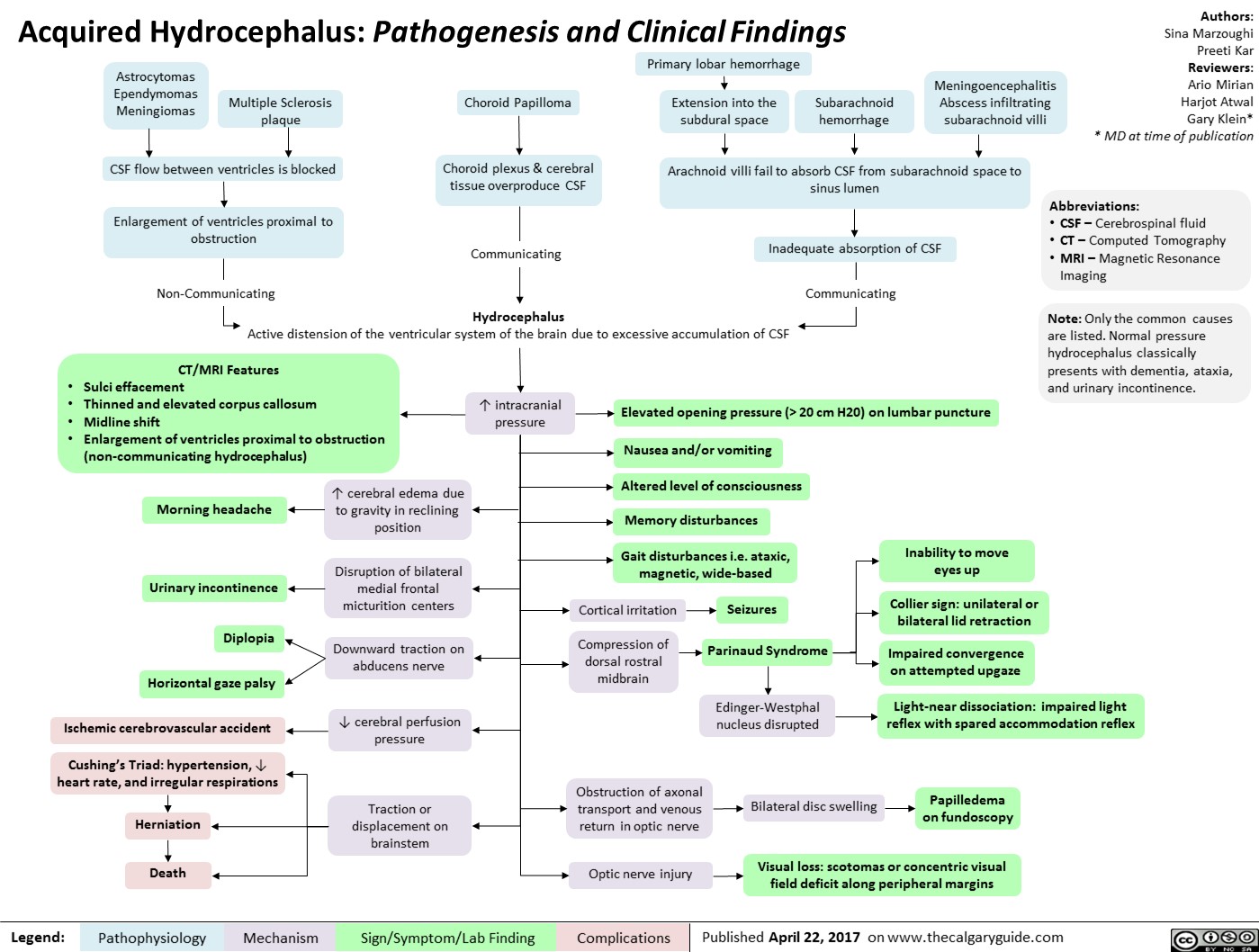
Kawasaki Disease
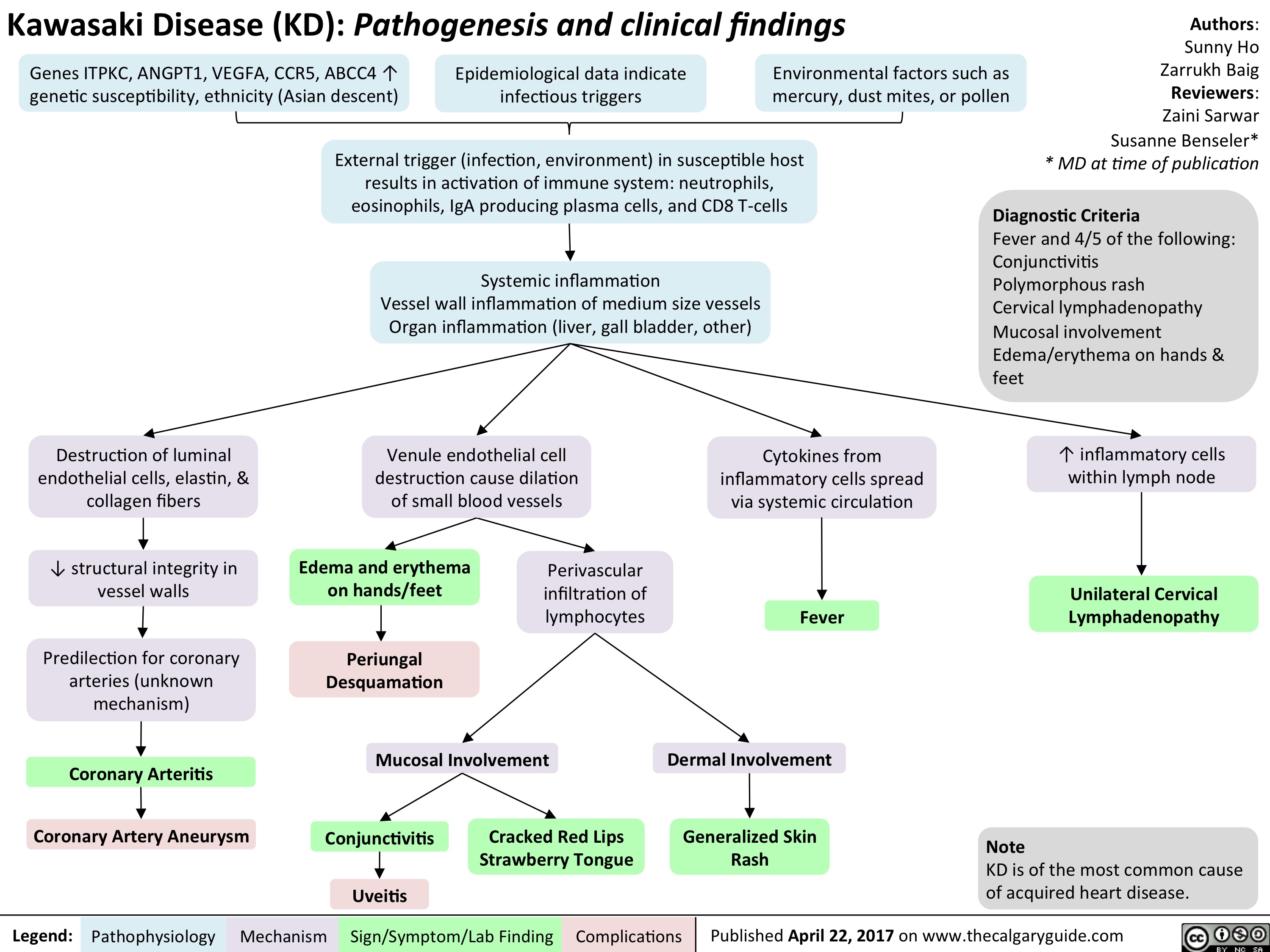
Secondary Hemostasis: Coagulation Cascade

systemic-lupus-erythematosus-gastrointestinal-manifestations

Critical Care Malnutrition
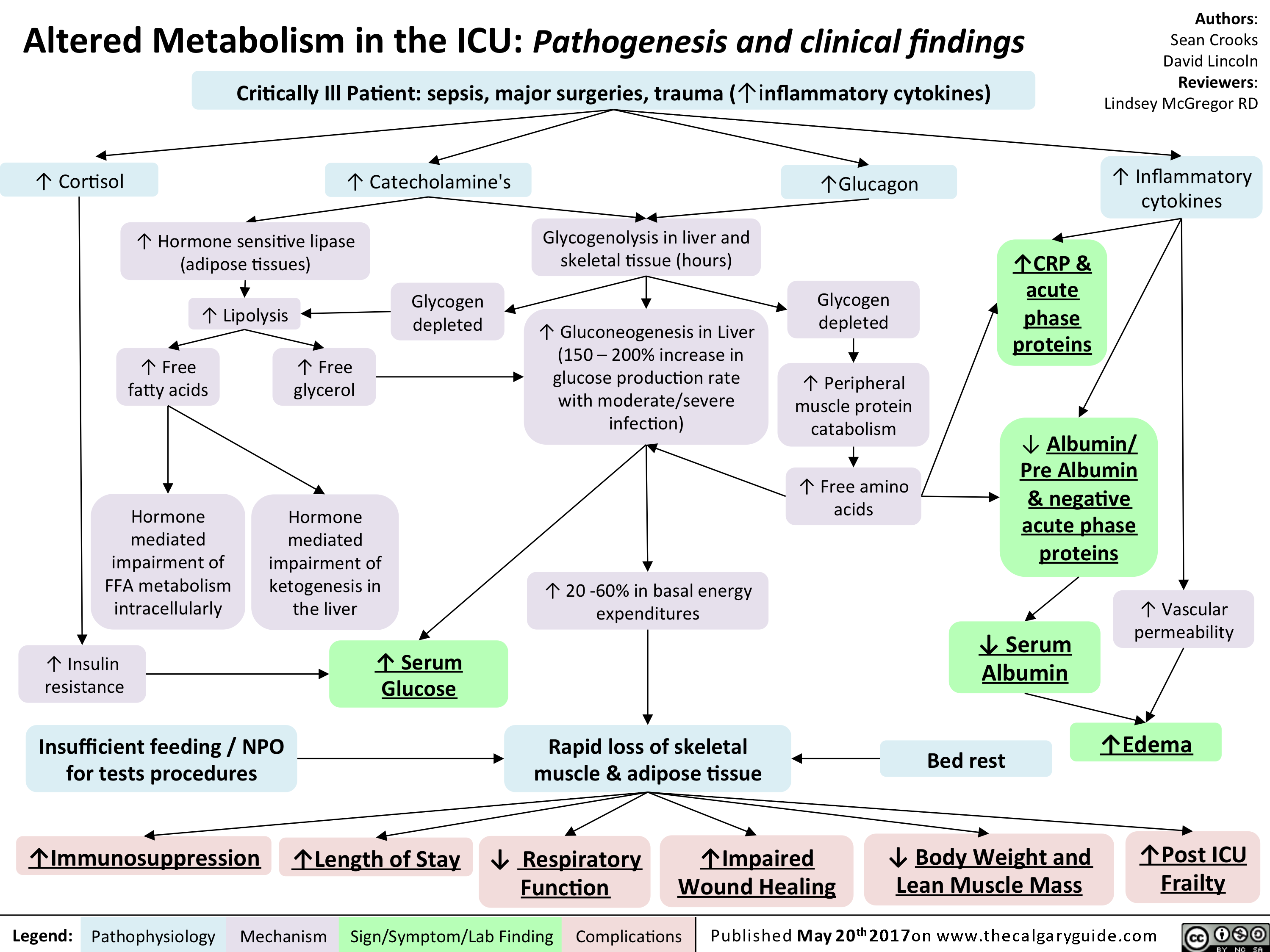
esophageal-gastric-varices

Legend:
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Complications
• Venous drainage of spleen backed up into gastric anastomoses
Tachycardia and hypotension
Anemia Death Melena Coffee ground emesis Hematemesis Bright red blood per rectum")
localized-pitting-edema

Authors: Sunny Fong Reviewers: Joseph Tropiano Adam Bass* * MD at time of publication
Central vein thrombosis
Deep vein thrombosis
T in venous pressure is transmitted to the capillaries
1` in capillary hydrostatic pressure
T in fluid extravasation from plasma into the interstitial space distal to site of obstruction or insufficiency
Localized Pitting Edema: Edema fixed at a specific anatomical site
Venous obstruction causes'` blood pooling distal to site of obstruction
Starling's Equation:
Net filtration gradient = LpS x ((Pap — Pint) Olcap
LpS = Porosity or permeability of the endothelial layer Pup = Capillary hydrostatic pressure Pint = Interstitial hydrostatic pressure ncap = Capillary oncotic pressure flint = Interstitial oncotic pressure
Note: An increase in net filtration gradient (eg. Increased capillary hydrostatic pressure or decreased capillary oncotic pressure) can lead to the formation of edema")
Neurotransmitters-and-Pharmacology-behind-Nausea-and-Vomiting - IN

2 Pusat lebih tinggi di SSP (korteks serebri, batang otak, hipotalamus, talamus)
Penyakit gerak atau labirin, menyebabkan ketidakcocokan sinyal antara sistem visual, vestibular, and proprioseptif
Obat-obatan (cth. kemoterapi, opiat, antibiotik)
Gangguan metabolik (cth. Gagal organ, hiperkalsemia)
toksin (cth. Dari bakteri penyebab keracunan makanan)
Peregangan (akibat stasis gaster, obstruksi organ berongga, tumor, konstipasi, atau distensi kapsuler organ padat — liver, pankreas)
Kompresi (dari organ sekitar, tumor, atau asites)
Jejas jaringan (dari peradanga, invasi tumor, kemoterapi, radiasi)
Legenda:
Sistem vestibular (telinga dalam)
Zona Pemicu Kemoreseptor (CTZ) (terletak di daerah ventrikel 4 tanpa sawar darah otak, secara konstan menyaring bahan kimia di darah)
Mekanisme kompleks dan belum dimengerti (mungkin dimediasi oleh banyak NT)
Tx: bicara dan dengarkan pasien, teknik relaksasi; lini-2: benzodiazepin untuk depresi SSP global, non-spesifik
Stimulasi langsung pusat muntah via efek massal
Tx: kortikosteroid, to 4, peradangan + tx penyebab (cth. pembedahan)
Sinyal mual/muntah ke pusat muntah dimediasi oleh Histamin (H1) dan Asetilkolin Muskarinik (ACh)
T
Tx: antagonis H1/ACh (cth. dimenhidrinat), Lini-2: antagonis ACh (cth. scopolamin)
Sinyal mual/muntah ke pusat muntah dimediasi Serotonin (5-HT) dan Dopamin (D2)
Tx: antagonis 5-HT (cth. ondansetron), antagonis D2 yang menembus sawar darah otak (cth. metoklopramid, bukan domperidon) + berhenti/kurangi obat penyebab
Kebanyakan m ua I a kibat stasis Tx: antagonis D2 gastrokinetik(cth. domperidon — saluran makan atas /lambung penetrasi SSP kurang - & metoklopramid. catatan: keduanya dikontraindikasikan pada obstruksi GI) + dimediasi Dopamin (D2) di CTZ tx penyebab
Patofisiologi Mekanisme
Saluran GI (termasuk liver & mesenterium)
Tanda/Gejala/Penunjang
Sinyal mual/muntah ke pusat muntah dimediasi terutama oleh Serotonin (5-HT) dan Dopamin (D2)
Tx: antagonis 5-HT (cth. ondansetron), antagonis D2 gastrokinetik (cth. metoklopramid, domperidon), fenotiazin antagonis D2 (i.e. haldol) + tx penyebab
Komplikasi
Penulis: Yan Yu* Penyunting: Laura Byford-Richardson Russell Loftus* Penerjemah: M Harmen Reza S* * MD (dokter) pada saat publikasi
Catatan: Kebanyakan jalur neurotransmiter pada mual/muntah masih belum diketahui. Tatalaksana yang tercantum di sini hanya bertujuan untuk menjelaskan prinsip umum terapi lini pertama. Terapi terapan pada pasien akan bergantung kepada diagnosis spesifik dan presentasi klinis.
Pusat Muntah
Koordinasi refleks muntah (dijelaskan di slide")
chronic-hypertensive-retinopathy-pathogenesis-and-clinical-findings
 • 1° HTN
Retinal Detachment
Vitreous Hemorrhage
Central/Branch Retinal Artery/Vein Occlusions
Risk Factors for 2° HTN (ex. Hyperaldosterone, Cushing's, Acromegaly, Chronic Kidney Disease, Obstructive Sleep Apnea, Diabetes Mellitus, Hypo/Hyper-thyroid, Adrenal Hyperplasia, Renal Artery Stenosis)
2° HTN
Ophthalmic Artery Hypertension ,17
Stage 1: Mild/vasoconstrictive
Stage 2: Moderate/sclerotic
Stage 3: Severe/exudative
Stage 4: Malignant
Abbreviations: • HTN — Hypertension • BRB — Blood-retinal barrier • RPE — Retinal pigment epithelium
Legend:
Pathophysiology
Mechanism
Acute and chronic vasospasm
Authors: Graeme Prosperi-Porta Reviewers: Stephanie Cote Usama Malik Johnathan Wong* * MD at time of publication
Diffuse and focal arterial narrowing and vascular tortuosity
Atherosclerosis and hyalinization causes arteriolar wall thickening resulting in a diffuse light reflex appearing red-brown coloured
Thickening of the arteriolar wall and/or sclerotic thickening at the arteriole/venule crossing compresses the underlying venule
BRB breakdown causes dot/blot hemorrhages in the inner retina and flame hemorrhages in the nerve fiber layer
Serum proteins and lipids leakage from damaged BRB appears as white or yellow areas with sharp margins
Occlusion of the terminal retinal arterioles causes fluffy white ischemic lesions in the inner retinal nerve fiber layer
Hyper-pigmented patches surrounded by a hypo-pigmented ring due to RPE clumping around atrophic areas in the choroid
Sign/Symptom/Lab Finding
lschemia of optic disc arterioles causes optic nerve swelling and blurred disc margins. Leakage of optic disc arterioles causes hemorrhage and disc edema.
Complications
Copper Wiring
AV nicking
Retinal Hemorrhages
Yellow Hard Exudates
Cotton-wool Spots
Elschnig's Spots
Papilledema")
central-retinal-artery-occlusion-pathogenesis-and-clinical-findings
 (i.e. Valvular, arrhythmias, congenital defects) (i.e. OCP, Protein C&S deficiency, ATIII deficiency) (i.e. leukemia/lymphoma, sickle cell, polycythemia) Endothelial cell damage Abnormal blood flow 1` coagulation and/or 1 blood viscosity and creates hypercoagulable state causing localized stasis 4, anti-coagulation inflammation
Abbreviations: • GCA — Giant Cell Arteritis • SLE — Systemic Lupus Erythematosus • GPA — granulomatosis with polyangitis • OCP — Oral contraceptive pill • ATIII — Anti-thrombin Ill
Thrombus formation
Blockage of central retinal artery
Central Retinal Artery Occlusion (CRAO)
Authors: Graeme Prosperi-Porta Reviewers: Stephanie Cote Usama Malik Johnathan Wong* * MD at time of publication Carotid Artery Atherosclerosis
Atherosclerotic plaque dislodges from carotid artery
The retina becomes pale 4, perfusion of retinal Slow retinal artery blood Acute retinal edema Ganglion cells and axons from NI, perfusion arterioles due to upstream flow allows for caused by ischemia results death due to ischemia CRAO segmentation of the blood column in a blurred appearance of the retina results in disc pallor seen months after CRAO The choroidal vessels supplying the macula via the posterior ciliary artery become more prominent within a background of retinal pallor")
Fragile X Syndrome
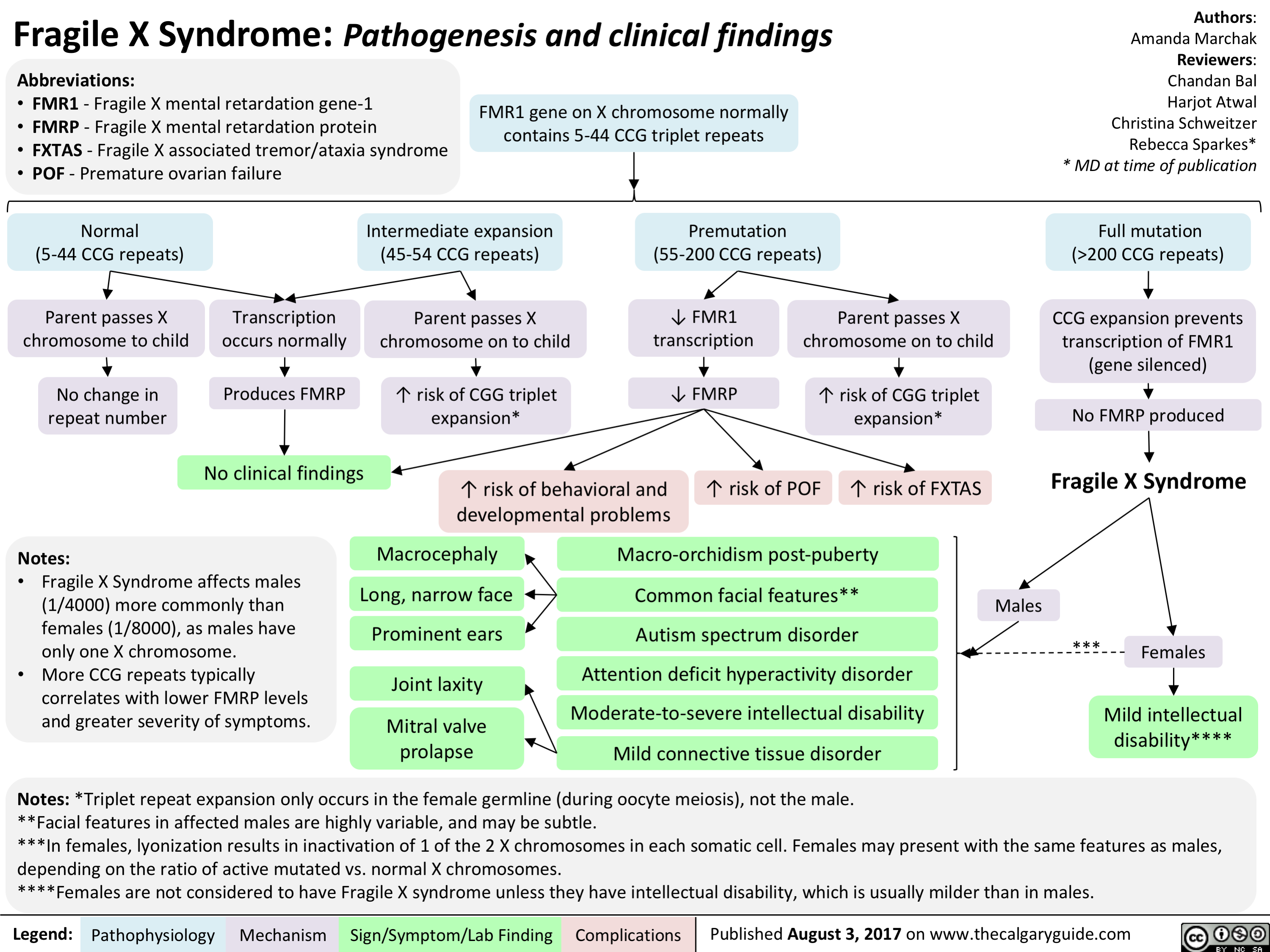
Attention Deficit Hyperactivity Disorder (ADHD)
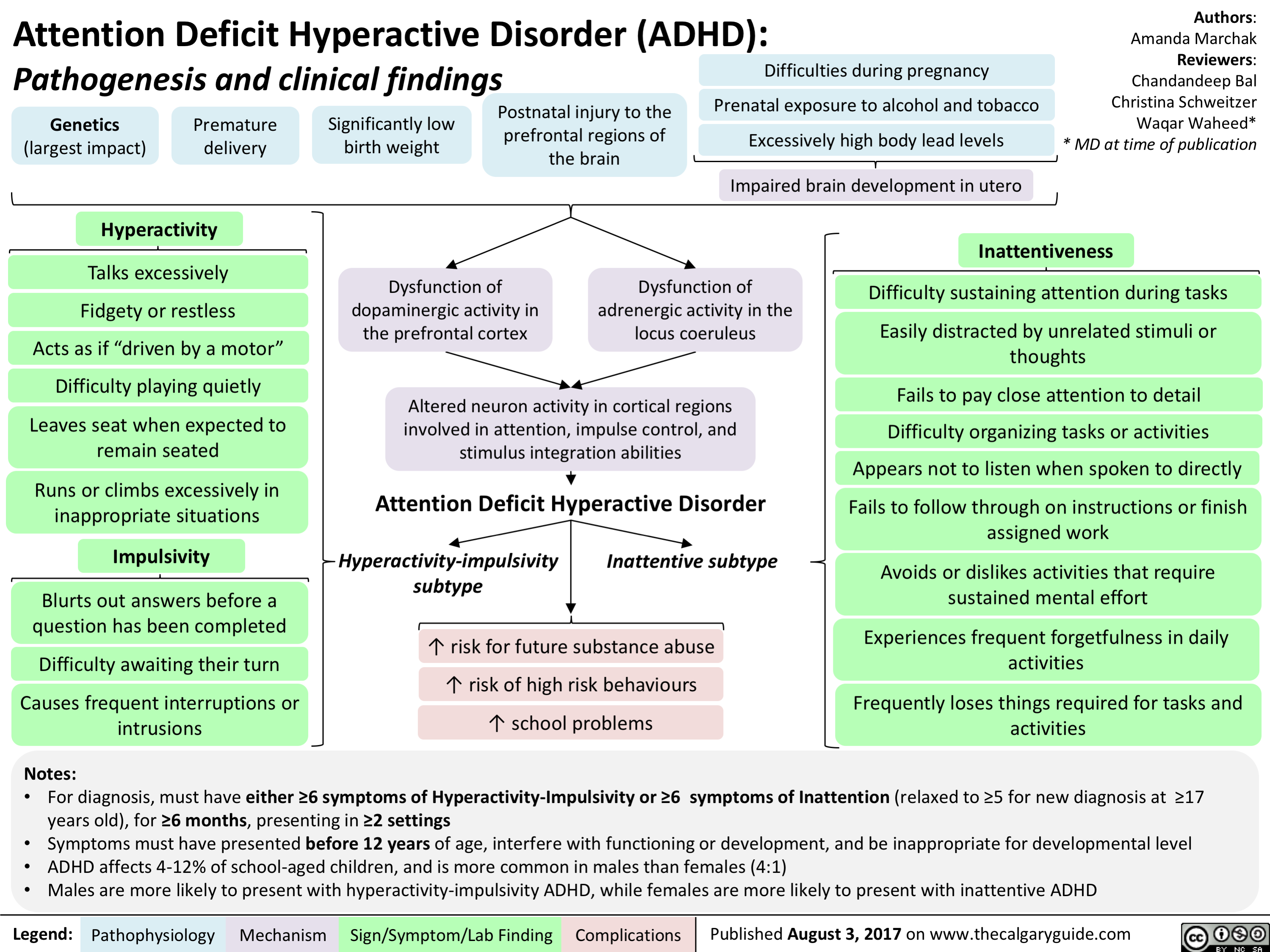
Oppositional Defiant Disorder (ODD)
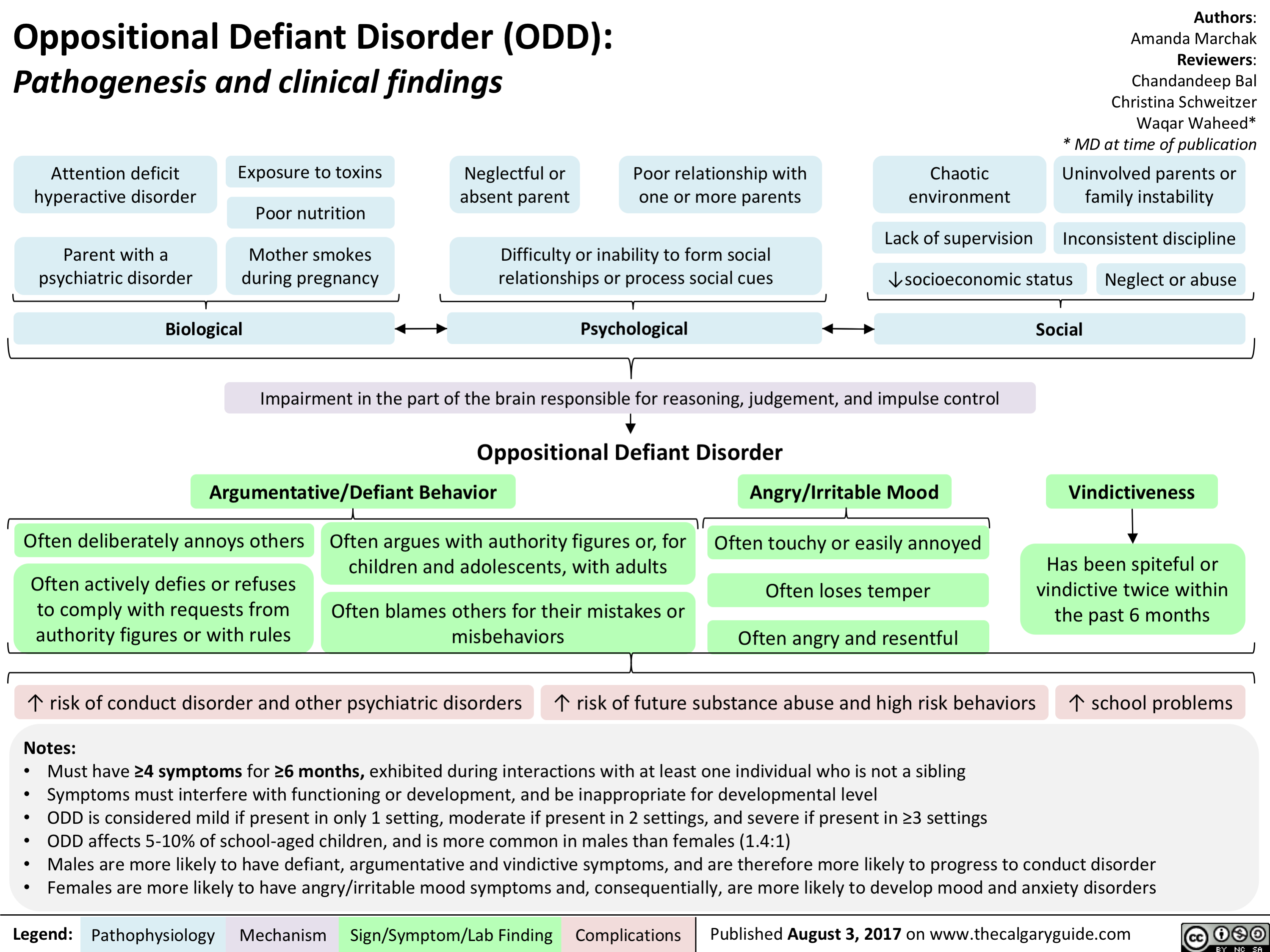
Conduct Disorder (CD)
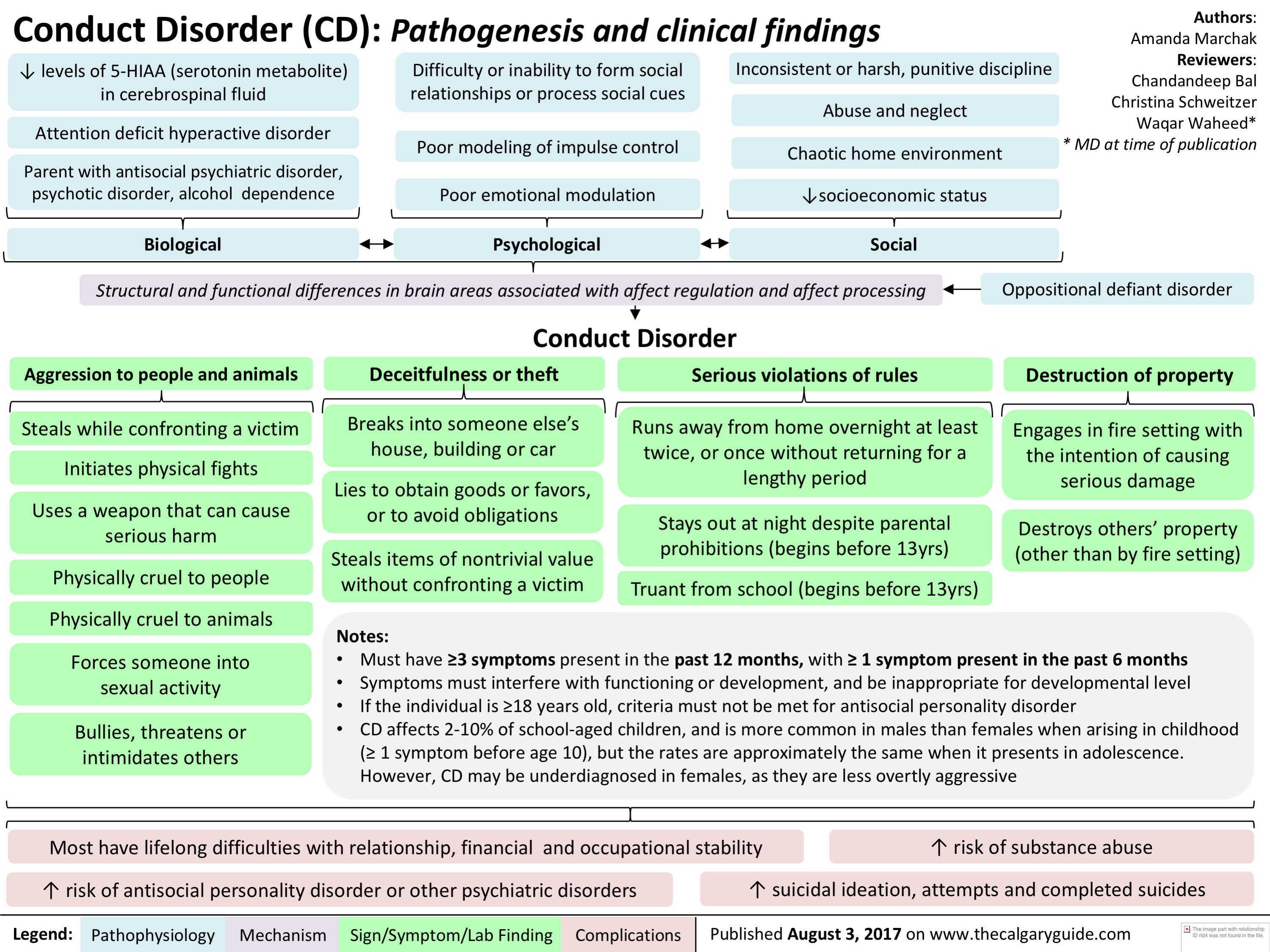
Down Syndrome

infectious-esophagitis-pathogenesis-and-clinical-findings

Herpes Simplex Infection of squamous cells and macrophages
Colonization facilitated by use of antacid therapy
Nuclear Large Superficial Squamous Macrophage inclusion bodies esophageal ulceration ulcers cell inclusion bodies aggregation Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications
Spores and pseudohyphae seen on biopsy
• Invas.on of underlying blood vessels
• White plaques over erythematous base
'1' neutrophils due to inflammatory response")
The Neuroanatomy and Physiology of Emotion
 Processes higher order emotions that 1— require recall, reason, and decision making (e.g., embarrassment) Integrates sensory information from the viscera in response to the inciting •
environmental object or event with information from the amygdala
Emotional feeling (i.e., conscious experience of emotion)
Thalamus
Emotionally salient environmental stimulus
Sensory input (e.g., vision, touch, smell, hearing, taste)
Hypothalamus ► (major output of the limbic system)
Olfaction*
Primary and Association Cortices •
Amygdala Processes lower order emotions that have fast, automatic, and conditioned responses (e.g., fear) Participates in formation and retrieval of emotionally relevant memories from neocortical areas, attaching emotional significance to sensory input
Hippocampus (key for memory consolidation and retrieval)
► Motor, Endocrine and Visceral systems
Notes: • The structures involved in emotions are defined as the limbic system • The thalamus, basal ganglia and PFC together form the corticostriatalthalmocortical loop which comprises the major emotional processing pathway in the brain • The Prefrontal Cortex (PFC) includes the orbitofrontal cortex (OFC), dorsolateral prefrontal cortex and anterior cingulate cortex • *Olfaction is the only sense that bypasses the thalamus and connects directly to the primary olfactory cortex
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Authors: Andrea Moir Reviewers: Erika Russell Usama Malik Brienne McLane* * MD at time of publication
Autonomic Nervous System (ANS)
The ANS automatically and unconsciously responds to the emotional stimulus (e.g., 11` HR, blushing)
Physical response to emotional stimulus Visceral sensation
Sensory receptors are stimulated by the ANS response and transmit this information to the somatosensory and insular cortices")
Serotonin Syndrome Pathogenesis and Clinical Findings
, opioids, antiemetic agents, triptans, weight loss agents, drugs of abuse (e.g. cocaine, amphetamines)
Therapeutic drug use
• Drug interactions (esp. combo of serotonergic agents) Serotonin Syndrome Variable combination of mental status changes, autonomic instability, and neuromuscular hyperactivity ranging from mild to life-threatening with an abrupt onset (within minutes to hours) after medication ingestion and most cases resolving within 24 hours of cessation of offending medication
Intentional self-poisoning
Excessive serotonergic activity at 5-HT receptors centrally (brainstem) and peripherally
serotonin synthesis and release
serotonin reuptake and metabolism
IN receptor agonism and sensitivity
4,
Drug-induced changes in the relative ratio of non-serotonergic neurotransmitters (e.g. increase in noradrenaline)
Altered Mental Status
Anxiety, confusion, agitation, hypervigilance, pressured speech, delirium, coma
Autonomic Instability
Shivering, diaphoresis, fever, diarrhea, tachycardia, mydriasis, hypertension
Authors: Preeti Kar Reviewers: Erika Russell Usama Malik Aaron Mackie* * MD at time of publication
Notes: The Hunter Serotonin Toxicity Criteria is used to make a clinical diagnosis • History of serotonergic agent taken within past 5 weeks + any of the following clinical features: • Spontaneous clonus • Inducible clonus and either agitation or diaphoresis • Ocular clonus and either agitation or diaphoresis • Tremor and hyperreflexia • Hypertonia, temperature > 38 °C, and either ocular clonus or inducible clonus
Neuromuscular Hyperactivity
Hyperreflexia, muscle rigidity (esp. lower extremities), myoclonus, tremor, incoordination, trismus*, opisthotonus*, ocular clonus*, seizures
*Notes: • Trismus or lockjaw, is the reduced opening of the jaw • Opisthotonus is an abnormal body position where the person is usually rigid and arches their back, with their head thrown backwards • Ocular Clonus is rhythmic or equal movements of both eyes; should be distinguished from nystagmus which has a fast and slow component
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Abbreviations: • 5-HT = serotonin • SSRI = selective serotonin reuptake inhibitors • SNRI = selective noradrenaline reuptake inhibitors • MOAI = monoamine oxidase inhibitors • TCA = tricyclic antidepressants")
Side Effects of ACEi/ARBs During Pregnancy

Side Effects of Methimazole During Pregnancy
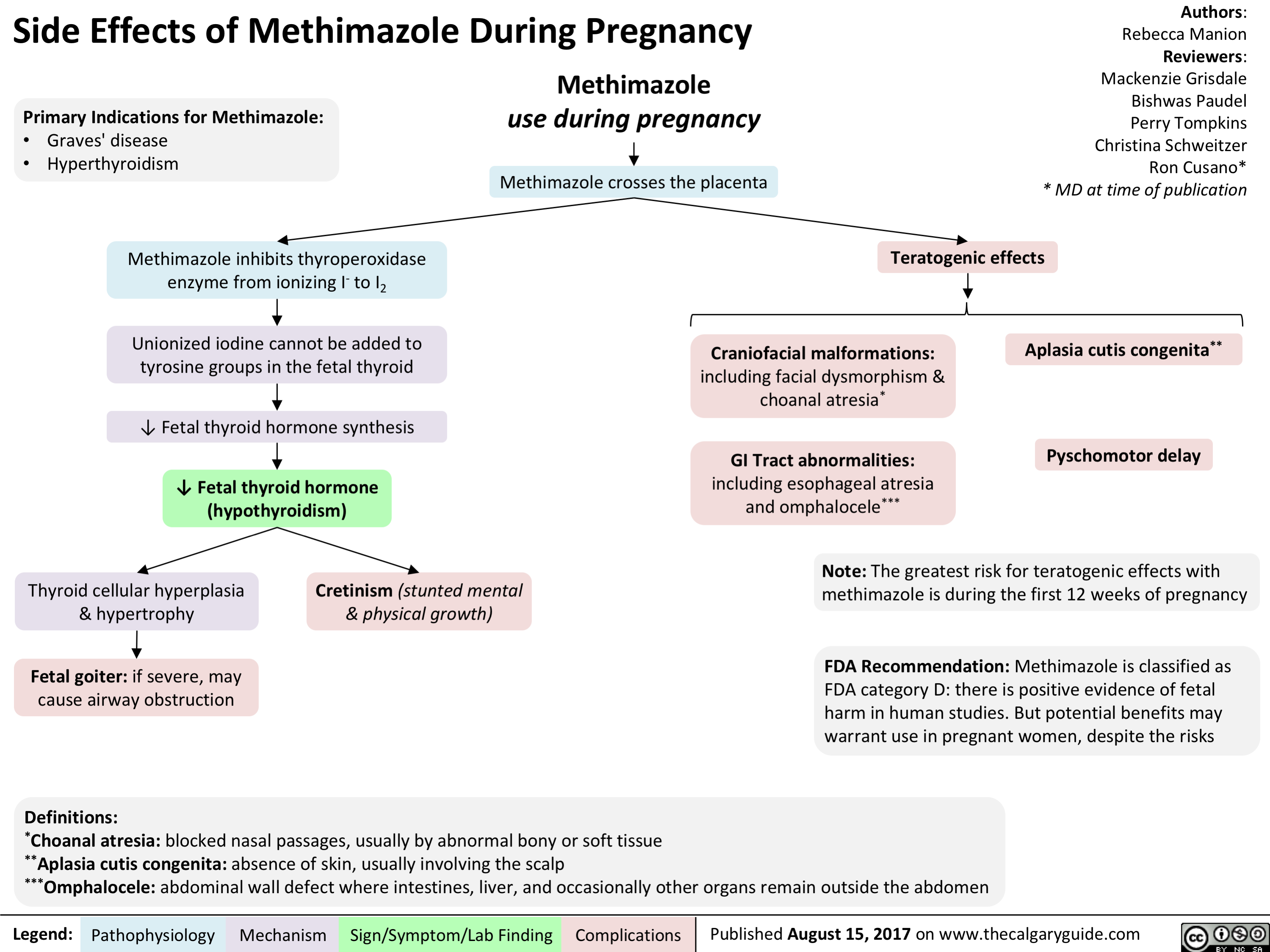
Side Effects of NSAIDs During Pregnancy

Side Effects of Valproic Acid During Pregnancy
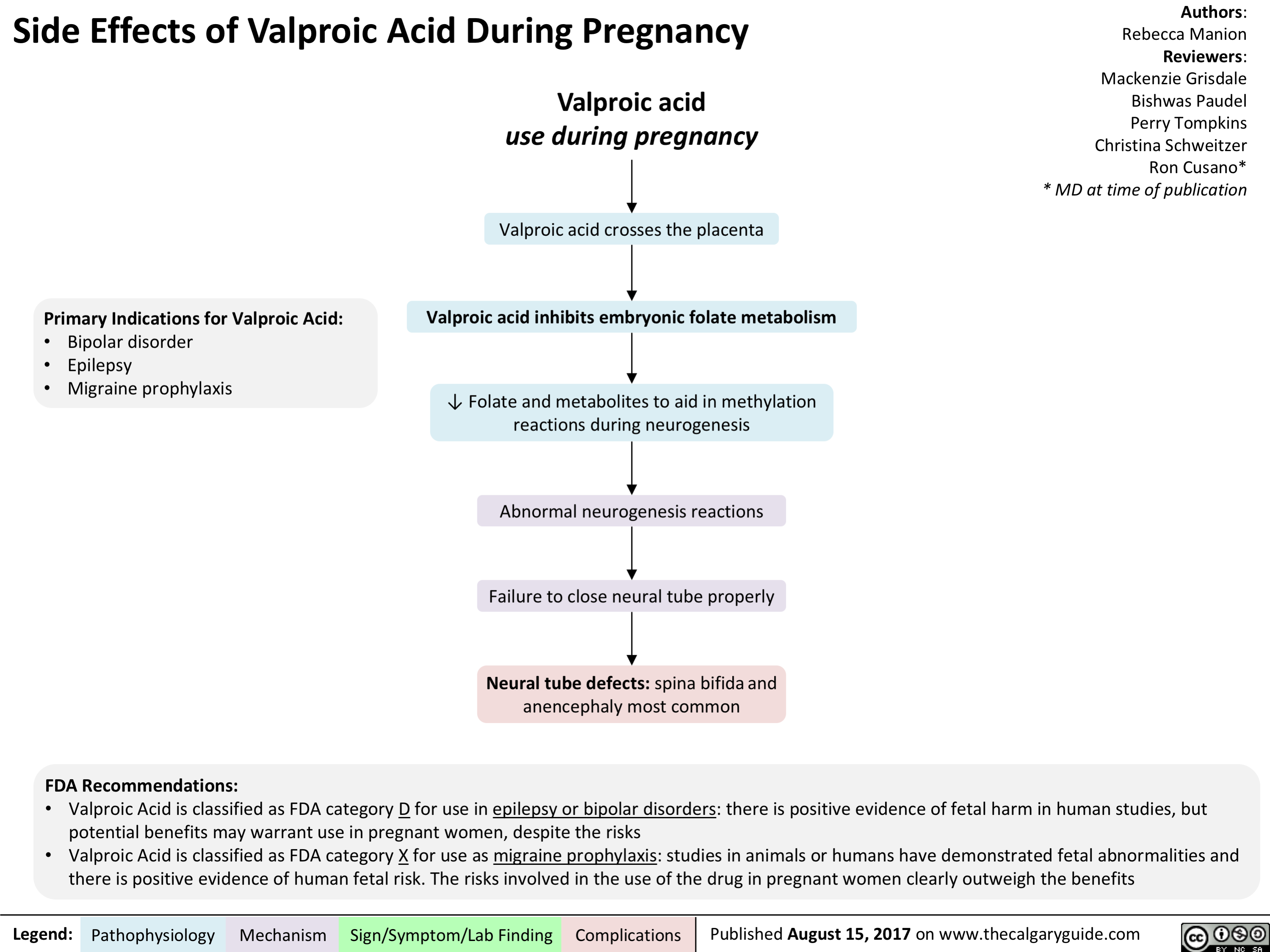
Side Effects of Warfarin During Pregnancy
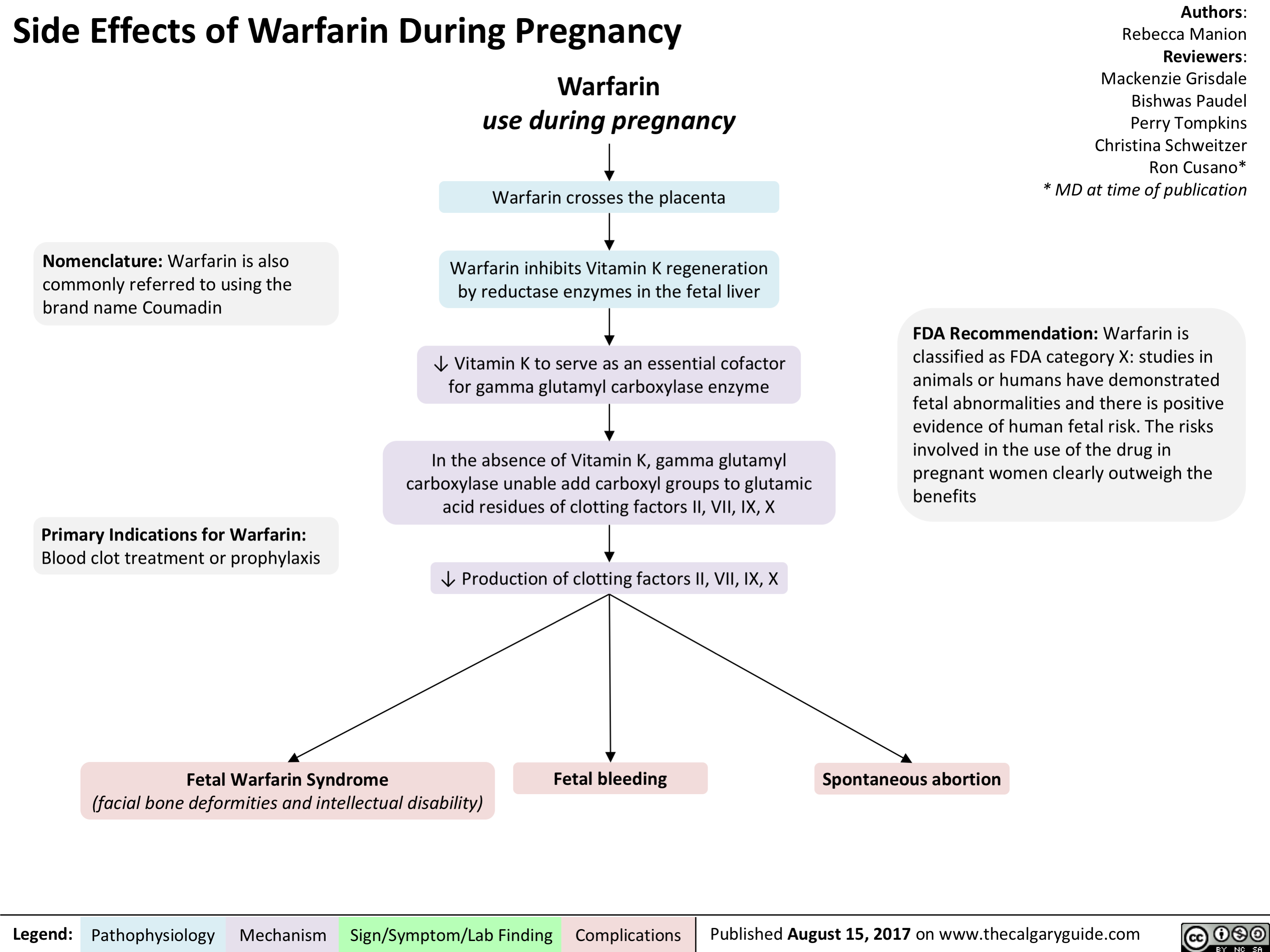
Pediatric Parasomnias and Nightmares: Pathogenesis and clinical findings

Hemolytic Disease of the Fetus and Newborn
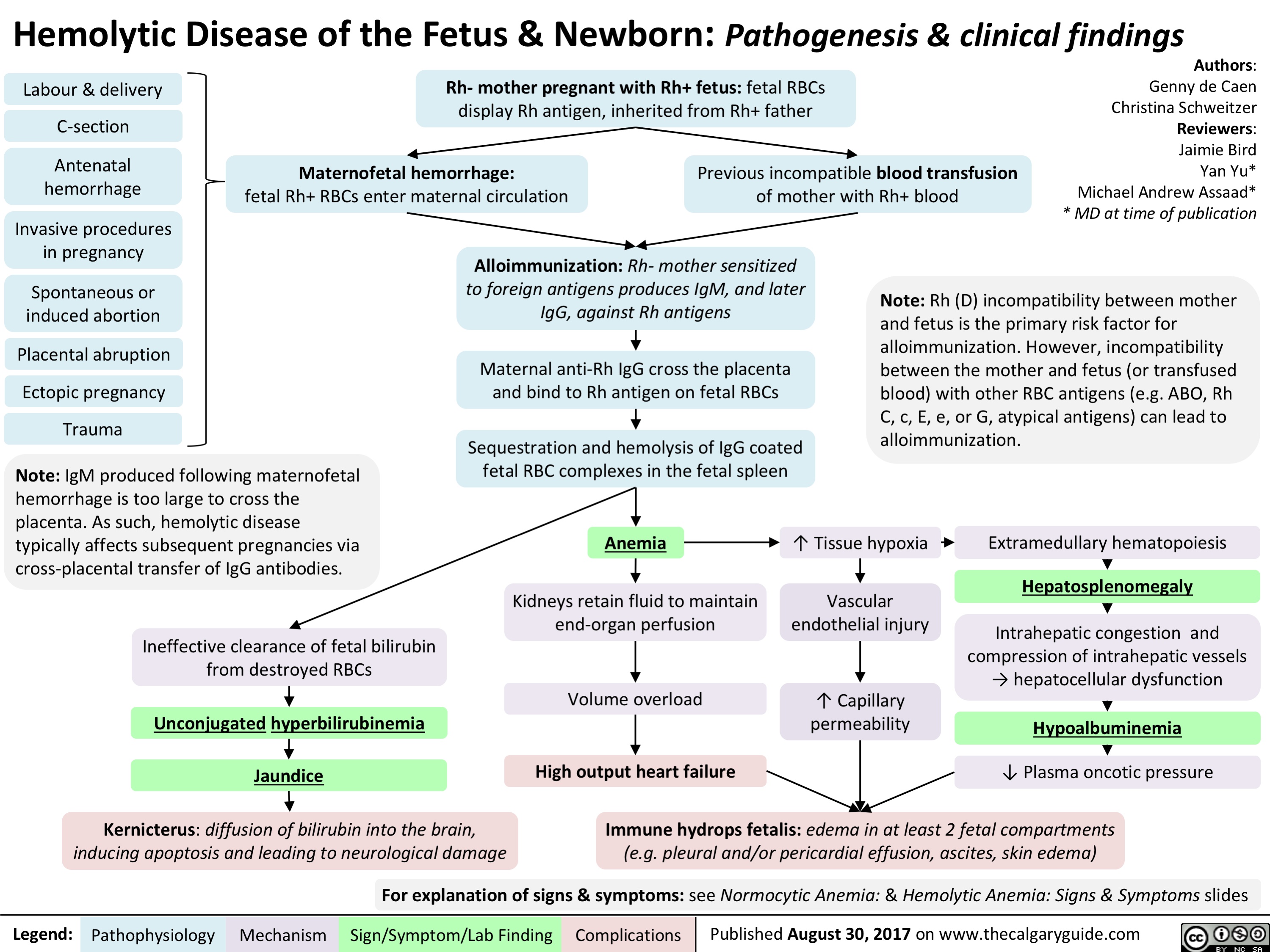
Trigeminal Neuralgia
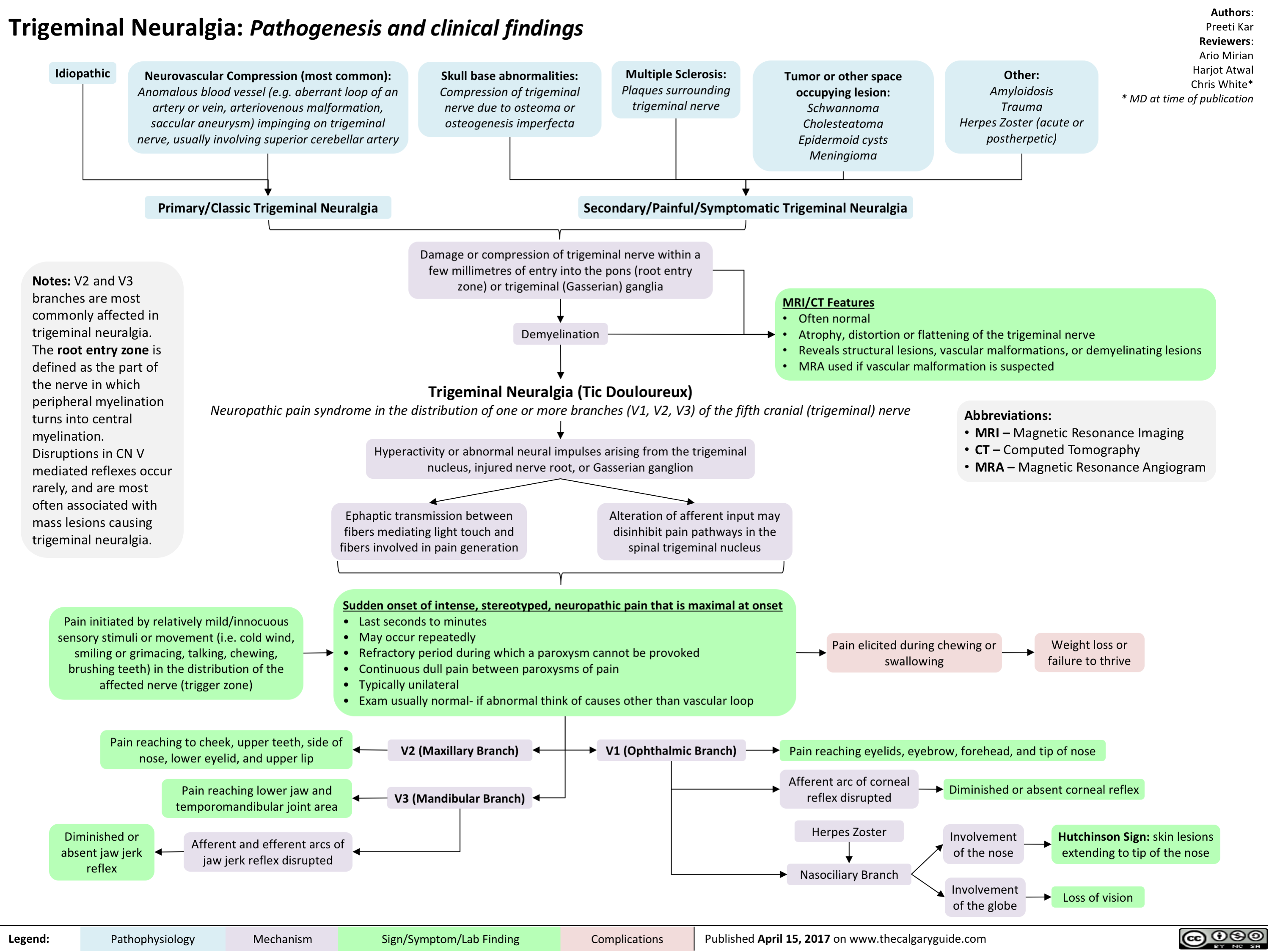
Mallory-Weiss Tear
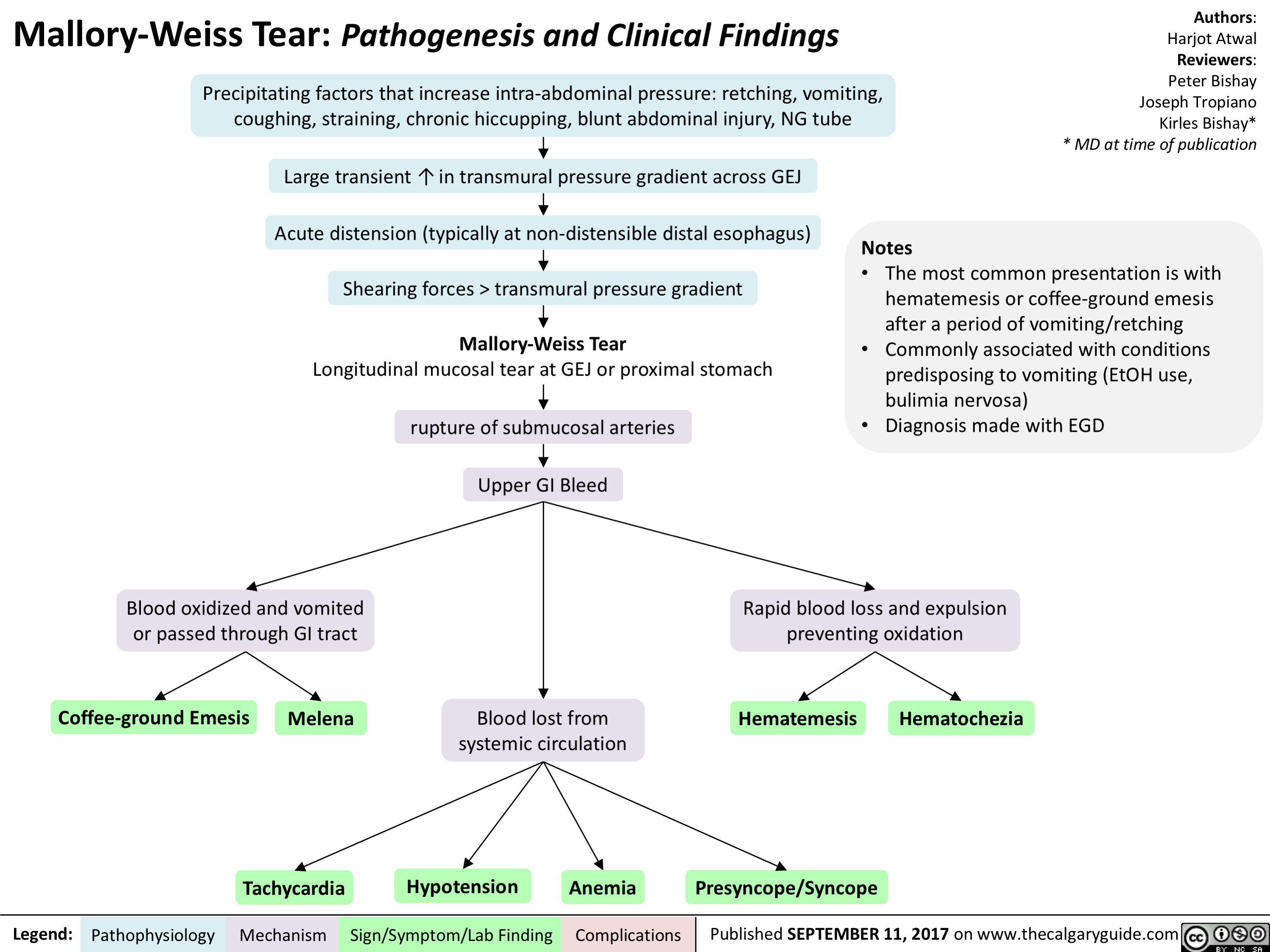
Unconjugated Neonatal Hyperbilirubinemia - Complications

pathogenesis-of-select-causes-of-constipation-in-adults-and-in-elderly
 Hypercalcemia) Hypothyroid-ism) Sclerosis) Scleroderma) Analgesics)
Mechanical I`Ca2+ = 4, Na+ Thyroid Demyelination Collagen Puborectalis Disturbance in obstruction in permeability in hormone of CNS neurons deposits into muscle and the gut-brain the bowel neurons deficiency colonic mucosa, leading to external anal sphincter fail interaction fibrosis of the gut wall to relax Interrupted 4, Excitability Possible Dysfunction of Narrowed Mechanism flow of bowel contents and tone of bowel smooth mechanisms: hormone autonomic nerves that anorectal angle and unknown, many Atrophy of the muscle receptor supply smooth muscle '`pressure of pathways changes, involuntary wall of the colon anal canal neuromuscular disorders, myopathy from bodily functions 1, Peristalsis of infiltration of 4, Ability of the Evacuation Visceral the bowel colon to contract of feces is hypersensitivity Abbreviations: the intestinal wall 4, Digestion less effective and 4, colonic and colonic motility motor • IBS-C: Irritable Bowel Syndrome with predominant constipation • CNS: Central Nervous System 4, Peristalsis of response after a meal the bowel
Opioids bind to Lt-opioid receptors on gut wall
Inhibition of excitatory neural pathways within the enteric nervous system
1, Peristaltic contractions
1
l• Colonic transit time")
1st gen antipsychotics (Slovenian translation) - FINAL VERSION
 primera: haloperidol, klorpromazin
antagonisti ACh M1 receptorjev zavirajo delovanje ACh po celem telesu (v ustih, prebavilih, o6eh, mo2ganih)
zaprtje
suha usta
zamegljen vid
kognitivna upolasnjenost
Legenda:
antagonisti histaminskih H1 receptorjev zavirajo delo-vanje histami-na v mo2ganih zaspanost
porast tel. teie
antagonisti adrenoceptorjev dilatacija gladkih miSic v stenah arteriol - te2ave pri vzdrievanju krvnega tlaka
ortostatska hipotenzija
mezolimbiZna pot VTA 4 limbicni sistem
mezokortikalna pot VTA prefrontalna skorja
tuberoinfundibularna pot hipotalamus 4 hipofiza
nigrostriatna pot substanca nigra 4 striatum
1
ekstrapiramidni simptomi (EPS)
avtorica: Sara Meunier pregledala: Yan Yu, Aaron Mackie*
* dr. med. ob objavi
4, pozitivnih simptomov terapevtski ueinek
4, odziv nagrajevalne poti
negativnih simptomov 11• kognitivnih simptomov teiave s pozornostjo in u6enjem
blokada DA vodi v izlaanje prolaktina iz adenohipofize
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
4, halucinacij
4, blodenj
otopelost
anhedonija
4. zanimanja za socialne stike
amenoreja
galaktoreja
okrajgave: VTA - ventral no tegmental no podraje DA - dopamin ACh - acetilholin
tardivna diskinezija Nenormalni asimetri6ni gibi obraznih mrgic, jezika in/ali udov, povzro6eni s kroni6no dopaminsko blokado. Letna incidenca pribliino 5 %, potencialno ireverzibilna!
patofiziologija mehanizem
iatrogeni parkinsonizem pojav zobatega kolesa, nestabilnost v drii, tremor v mirovanju, bradikinezija/akinezija
znak/simptom/laboratorijska najdba
akutna distonija kra migic vratu, okrog ob, jezikageljusti
akatizra obL'utek motorie'nega nemira
zaplet Objavljeno 15. junija 2017 na www.thecalgaryguide.com.")
2nd gen antipsychotics (Slovenian translation) - FINAL VERSION
: primeri: klozapin, olanzapin, kvetiapin, risperidon, paliperidon itd.
antagonisti dopaminskih D2 receptorjev zavirajo delovanje DA na D2 receptorjih po celotnih mo2ganih
antagonisti serotoninskih 2A receptorjev zavirajo delovanje 5-HT na 5-HT2A receptorjih po celotnih mo2ganih
antagonisti serotoninskih 2C receptorjev klozapin, olanzapin, kvetiapin
antagonisti ACh M1 receptorjev zavirajo delovanje ACh po telesu (v ustih, prebavilih, o6eh, mo2ganih)
antagonisti aradrenoceptorjev v oiilju dilatacija gladkih migic v stenah arteriol
antagonisti histaminskih H1 receptorjev zavirajo delovanje histamina po telesu
sano-presnovni kink' mehanizem neznan
Legenda:
patofiziologija mehanizem
Pomni: posledica velikih razlik v afiniteti za receptorska vezavna mesta so svojevrstni terapevtski in varnostni profili atipicnih a nti psi hoti kov. Kloza pi n med vsemi velja za najud nkovitejSega, a i ma tudi najve6 neZelenih uC'inkov, vkljUuja agranulocitozo (0,5-2 %). Tako predstavlja terapijo drugega izbora, potrebno je red no spremljanje bolnikove krvne slike.
mezolimbiEna pot DA blokada > 5-HT blokado
nigrostriatna pot 5-HT blokada > DA blokado
4, pozitivnih simptomov terapevtski ueinek
blokada 5-HT vodi v sprokanje DA v striatumu
tubero- blokada 5-HT zavre sprokanje infundibularna pot prolaktina v adenohipofizi
mezokortikalna pot
blokada 5-HT2c receptorjev stimulira sprokanje DA in NA v prefrontalni skorji
zamegljen vid
kognitivna upolasnjenost
sposobnost vzdrievanja krvnega tlaka
omotica
apetit
T tel. tee
ortostatska hipotenzija
tveganje za debelost
trigliceridi na tee
inzulinska odpornost —■ diabetes tipa 2
znak/simptom/laboratorijska najdba
4, halucinacii
blodeni
avtorica: Sara Meunier pregledala: Yan Yu, Aaron Mackie*
* dr. med. ob objavi
prevedel in priredil: Jan KejZar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
4, ekstrapiramidnih simptomov (EPS)*
4, hiperprolaktinemije*
prokognitivni in antidepresivni ainki
4, kognitivnih simptomov* 4, negativnih simptomov*
* Glede na anti-psihotike prve generacije, glej ustreznogradivo!
okrajgave: 5-HT - serotonin DA - dopamin NA - noradrenalin ACh - acetilholin
visoko presnovno tveganje: klozapin, olanzapin zmerno presnovno tveganje: risperidon, kvetiapin nizko presnovnotveganje:antipsihotikitretjegeneracije
1 tveganje za diabeti6no ketoacidozo pri bolnikih z visokim tveganjem tveganje za srbo-iilne dogodke tveganje za prezgodnjo smrt
zaplet Objavljeno 15. junija 2017 na www.thecalgaryguide.com.")
3rd gen antipsychotics (Slovenian translation) - FINAL VERSION
 primer: aripiprazol
delni agonist dopaminskih D2 receptorjev Veie se na D2 receptor, se hitro sprosti in znova veie. Ta ponavljajoc vzorec receptorske vezave molekulam DA v sinapsah ne pusti, da bi se vezale na D2 receptorje.
4,
prepre6uje vikk DA zaradi preve6 stimuliranih receptorjev in primanjkljaj DA zaradi premalo stimuliranih receptorjev")
Alcohol Use Disorder (Slovenian translation) - FINAL VERSION
 sprokanje endogenih opioidov skorji in mezolimbibem dopaminskem sistemu)
etanol dose2e dano koncentracijo v krvi hitreje (tj. v 6asa)
toleranca (zmanjgana ob'6utljivost na ainke etanola)
/1` vnos etanola za dosego enakih u6inkov
socialna okrnjenost
nezmoZnost izpolnjevanja obvez (na delu, v Soli, doma)
nadaljevanje (zlo)rabe kljub druZbenim problemom, povzro6enih z alkoholom
kljuthih druthenih, poklicnih in rekreativnih aktivnosti
•
tvegana uporaba substance
ponavljajo6e se raba alkohola v 'gkodIjivih situacijah
nadaljevanje rabe navkljub poznavanju posledic
Pomni: v DSM-5 sta prej lo6eni entiteti zloraba alkohola in odvisnost od alkohola zdruZeni v motnjo rabe alkohola (an. alcohol use disorder). Zloraba alkohola je bila prej definirana kot pitje navkljub ponavljajo6im se druZbenim in medosebnim teZavam ter teZavam z zakonom, odvisnost pa je predstavljala „podaljSek")
BMR (Slovenian translation) - FINAL VERSION
 )
Pomni: • Bipolar motnja tipa 1: maniba epizoda in/ali depresivna epizoda: priblrino 10 epizod manije in depresije v 2ivljenju bolnika v primeru nezdravljene bolezni • Bipolar motnja tipa 2: hipomaniba epizoda in depresivna epizoda • hipomaniba epizoda predstavlja bla2jo obliko manije, tj. brez funkcionalne okrnjenosti, brez psihotibih simptomov, brez hospitalizacije in v trajanju vsaj 4 zaporednih dni
znak/simptom/laboratorijska najdba
avtorici: Briana Cassetta, Sara Meunier pregledali: Yan Yu, Alexander Arnold, Philip Stokes*
* dr. med. ob objavi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
depresivna epizoda najmanj 2 tedna
depresivno razpoloienje
socialnega urriika
obEutkov krivde, tesnobe
brezupa
samomorilnih misli in vedenja
anhedonija
teiave s pozornostjo
A v spanju, utrujenost
A tel. teie, apetita
psihomotorna agitira nost ali upolasnjenost
zaplet Objavljeno 30. junija 2017 na www.thecalgaryguide.com.")
Bupropion (Slovenian translation) - FINAL VERSION
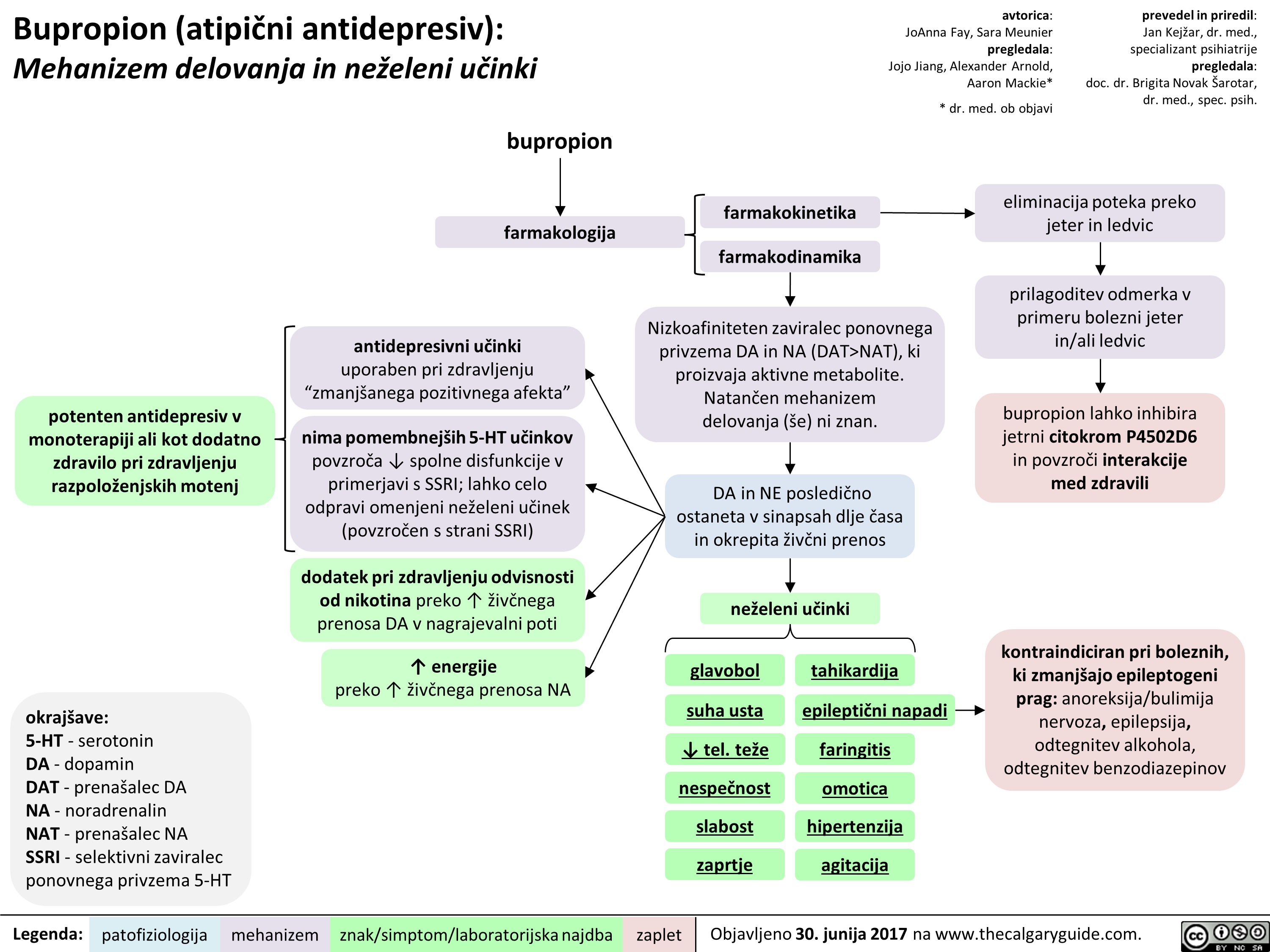 NAT), ki proizvaja aktivne metabolite. Natan'6en mehanizem delovanja (se) ni znan.
znak/simptom/laboratorijska najdba
DA in NE posledi6no ostaneta v sinapsah dlje Casa in okrepita 2iv6ni prenos
neieleni udnki
glavobol
suha usta
4, tel. tee nespeEnost slabost zaprtie
tahikardija
epileptiEni napadi
faringitis
omotica hipertenziia agitacija
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
eliminacija poteka preko jeter in ledvic
prilagoditev odmerka v primeru bolezni jeter in/ali ledvic
bupropion lahko inhibira jetrni citokrom P4502D6 in povzrod interakcije med zdravili
kontraindiciran pri boleznih, ki zmanIgajo epileptogeni prag: anoreksija/bulimija nervoza, epilepsija, odtegnitev alkohola, odtegnitev benzodiazepinov
zaplet Objavljeno 30. junija 2017 na www.thecalgaryguide.com.
" title="Bupropion (atipiEni antidepresiv): Mehanizem delovanja in neieleni utinki
potenten antidepresiv v monoterapiji all kot dodatno zdravilo pri zdravljenju razpoloienjskih motenj
okrajgave: 5-HT - serotonin DA - dopamin DAT - prenagalec DA NA - noradrenalin NAT - prenagalec NA SSRI - selektivni zaviralec ponovnega privzema 5-HT
Legenda:
bupropion
farmakologija
antidepresivni udnki uporaben pri zdravljenju "zmaniganega pozitivnega afekta"
nima pomembnelgih 5-HT udnkov povzraa spolne disfunkcije v primerjavi s SSRI; lahko celo odpravi omenjeni neieleni udnek (povzraen s strani SSRI)
dodatek pri zdravljenju odvisnosti od nikotina preko T iive'nega prenosa DA v nagrajevalni poti
energije preko T 2ivbega prenosa NA
patofiziologija mehanizem
farmakokinetika
farmakodinamika
avtorica: JoAnna Fay, Sara Meunier pregledala: Jojo Jiang, Alexander Arnold, Aaron Mackie*
* dr. med. ob objavi
Nizkoafiniteten zaviralec ponovnega privzema DA in NA (DAT>NAT), ki proizvaja aktivne metabolite. Natan'6en mehanizem delovanja (se) ni znan.
znak/simptom/laboratorijska najdba
DA in NE posledi6no ostaneta v sinapsah dlje Casa in okrepita 2iv6ni prenos
neieleni udnki
glavobol
suha usta
4, tel. tee nespeEnost slabost zaprtie
tahikardija
epileptiEni napadi
faringitis
omotica hipertenziia agitacija
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
eliminacija poteka preko jeter in ledvic
prilagoditev odmerka v primeru bolezni jeter in/ali ledvic
bupropion lahko inhibira jetrni citokrom P4502D6 in povzrod interakcije med zdravili
kontraindiciran pri boleznih, ki zmanIgajo epileptogeni prag: anoreksija/bulimija nervoza, epilepsija, odtegnitev alkohola, odtegnitev benzodiazepinov
zaplet Objavljeno 30. junija 2017 na www.thecalgaryguide.com.
" />
NAT), ki proizvaja aktivne metabolite. Natan'6en mehanizem delovanja (se) ni znan.
znak/simptom/laboratorijska najdba
DA in NE posledi6no ostaneta v sinapsah dlje Casa in okrepita 2iv6ni prenos
neieleni udnki
glavobol
suha usta
4, tel. tee nespeEnost slabost zaprtie
tahikardija
epileptiEni napadi
faringitis
omotica hipertenziia agitacija
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
eliminacija poteka preko jeter in ledvic
prilagoditev odmerka v primeru bolezni jeter in/ali ledvic
bupropion lahko inhibira jetrni citokrom P4502D6 in povzrod interakcije med zdravili
kontraindiciran pri boleznih, ki zmanIgajo epileptogeni prag: anoreksija/bulimija nervoza, epilepsija, odtegnitev alkohola, odtegnitev benzodiazepinov
zaplet Objavljeno 30. junija 2017 na www.thecalgaryguide.com.
" title="Bupropion (atipiEni antidepresiv): Mehanizem delovanja in neieleni utinki
potenten antidepresiv v monoterapiji all kot dodatno zdravilo pri zdravljenju razpoloienjskih motenj
okrajgave: 5-HT - serotonin DA - dopamin DAT - prenagalec DA NA - noradrenalin NAT - prenagalec NA SSRI - selektivni zaviralec ponovnega privzema 5-HT
Legenda:
bupropion
farmakologija
antidepresivni udnki uporaben pri zdravljenju "zmaniganega pozitivnega afekta"
nima pomembnelgih 5-HT udnkov povzraa spolne disfunkcije v primerjavi s SSRI; lahko celo odpravi omenjeni neieleni udnek (povzraen s strani SSRI)
dodatek pri zdravljenju odvisnosti od nikotina preko T iive'nega prenosa DA v nagrajevalni poti
energije preko T 2ivbega prenosa NA
patofiziologija mehanizem
farmakokinetika
farmakodinamika
avtorica: JoAnna Fay, Sara Meunier pregledala: Jojo Jiang, Alexander Arnold, Aaron Mackie*
* dr. med. ob objavi
Nizkoafiniteten zaviralec ponovnega privzema DA in NA (DAT>NAT), ki proizvaja aktivne metabolite. Natan'6en mehanizem delovanja (se) ni znan.
znak/simptom/laboratorijska najdba
DA in NE posledi6no ostaneta v sinapsah dlje Casa in okrepita 2iv6ni prenos
neieleni udnki
glavobol
suha usta
4, tel. tee nespeEnost slabost zaprtie
tahikardija
epileptiEni napadi
faringitis
omotica hipertenziia agitacija
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
eliminacija poteka preko jeter in ledvic
prilagoditev odmerka v primeru bolezni jeter in/ali ledvic
bupropion lahko inhibira jetrni citokrom P4502D6 in povzrod interakcije med zdravili
kontraindiciran pri boleznih, ki zmanIgajo epileptogeni prag: anoreksija/bulimija nervoza, epilepsija, odtegnitev alkohola, odtegnitev benzodiazepinov
zaplet Objavljeno 30. junija 2017 na www.thecalgaryguide.com.
" />
PTSD (Slovenian translation) - FINAL VERSION
: patogeneza in kliniene najdbe
predbolezenski dejavniki
genetika 30-% varianca*
skupen vpliv preteklih iivljenjskih stisk veda oUutijivost za dukvne travme
**Op. prey.: nepristranskost pozornosti (an. attentional bias) se nanak na podyrknost oz. nagnjenost Elovekovih zaz-nav k vplivu njegovih trenutnih misli. VeE v skupni bibliografiji psihologov A. Tverskyja in D. Kahnemana.
Legenda:
travmatski dogodek obaitki nemod in/ali izgube nadzora (npr. v okolikinah vojne, naravnih katastrof, spolnega napada, poroda)
intenziven Zustveni odziv ob du§evni travmi strah, nema ali groza
posttravmatska stresna motnja (PTSM)
nevrokemijske nepravilnosti spremembe v prenosu kortizola, GABA-e, dopamina
prekomerna Zustvena vzburjenost
anksioznost
posttravmatski dejavniki
pomanjkanje druibene podpore
stresni dejavniki v iivljenju
avtorica: Briana Cassetta pregledali: Sara Meunier, Yan Yu, Margaret Oakander*
* dr. med. ob objavi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
*Op. prey.: z narakanjem variance se ve6a fenotipska raznolikost v populaciji.
moteni spoznavni procesi
pove6ana odzivnost amigdale nepristranskostpozornosti** zoper sign ale ogroknosti
inhibicija hipokampusa vodi v drobljenje spomina
pove'Cana opreznost pretirana bojazijivost teiave s pozornostjo podoiivljanje duKevnih travm, npr. v obliki noZnih mor ali „iivega")
Lipid Physiology Slide
 Lipid Supply
Small Intestine: Absorption of dietary triglycerides and cholesterol
Lymph, then Plasma: Chylomicrons (ApoC2 , ApoB48 ) Transport of dietary Triglycerides and Cholesterol
Peripheral Tissues: Triglyceride uptake and Chylomicron metabolism via Lipoprotein Lipase receptors (in presence of ApoC2)
Plasma: Chylomicron Remnants (ApoE)
Liver: Chylomicron Remnant uptake via surface LDL receptors and LRP1 (in presence of ApoE)
Note: Key component carrier lipoproteins are indicated in bold parentheses. i.e. (ApoC2). _DL are Density Lipoproteins which can be High (HDL), Intermediate (IDL), Low (LDL), and Very Low (VLDL) Deficiencies in these lipoproteins often result in inability to shuttle lipids and ensuing hyperlipidemias.
Endogenous Triglyceride Supply
Liver: Synthesis of VLDL from FFAs, ApoB100, and Cholesterol
Plasma: VLDL (ApoB100, ApoC2, ApoE) Transport of endogenous triglycerides and Cholesterol
Peripheral Tissues: Triglyceride uptake and VLDL cleavage via Lipoprotein Lipase receptors (in presence of ApoC2)
Endogenous Cholesterol Supply
Plasma: IDL (ApoE ) Transport of Cholesterol and Triglycerides to Liver
Liver: IDL uptake via surface LDL receptors (in presence of ApoE)
IDL metabolism to LDL via Hepatic Lipase
Plasma: LDL (ApoB100, Apo E) Transport of Cholesterol
Peripheral Tissues: Cholesterol uptake via surface LDL receptors (in presence of ApoB100)
Author: David Lincoln Reviewers: Harjot Atwal Usama Malik Dr. Alexander A-C Leung* * MD at time of publication
Reverse Cholesterol Transport
Plasma: Immature HDL (ApoAl) Nascent in plasma
•
Peripheral Tissues: Cholesterol export via surface ABCA1/ABCG1 transporters
Abbreviations: • ABCA1 - ATP-Binding Cassette Transporter Al • ABCG1 - ATP-Binding Cassette Transporter G1 • FFAs - Free Fatty Acids • LCAT - Lecithin Cholesterol Acetyl Transferase • LRP1 - LDL Receptor-related protein • SRB1 - Scavenger Receptor B1
Plasma: Mature HDL (ApoAl) Free cholesterol is esterified via LCAT.
Some cholesterol remains in plasma via CTEP-mediated transfer of Cholesterol to lower density lipoproteins (i.e. VLDL, IDL)
Liver: Cholesterol ester uptake into liver via SRB1
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications Published September, 24,2017 on www.thecalgaryguide.com")
Subtrochanteric Femur Fracture
 damage Notes: weakens the ------------___________L_____---------- hone • Subtrochanteric region span, cm .tally from the lesser Subtrochanteric trochorder • Major haumas is most Femur Fracture common in young and low energy fall fractures in elderly
Mechanical instability
Pain with motion Point tenderness Inability to beercei ht
Gluseus maxlmus and minimus force vectors Abduction
Displaced
proximal femur
Psoas force vector Pirifo o
Non-union of fracture
External rotation
Legend: Pa.ophysiolo. Mechanism sign/Symptom/Lab Finding Complications
Published September, Mk 201, on envie thecelgeigguide CO. rum")
Ovarian Torsion
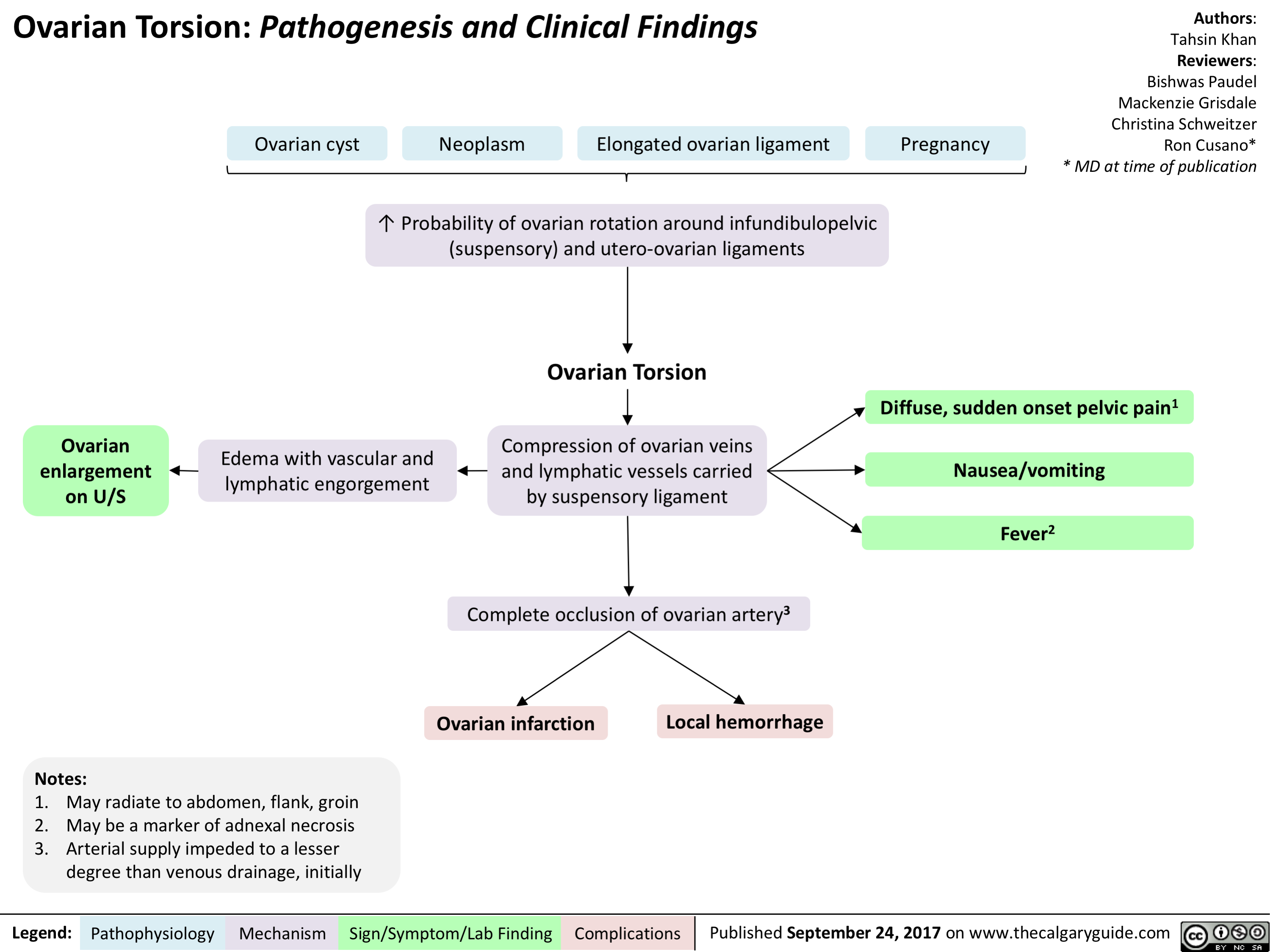
Non-Hodgkin Lymphoma
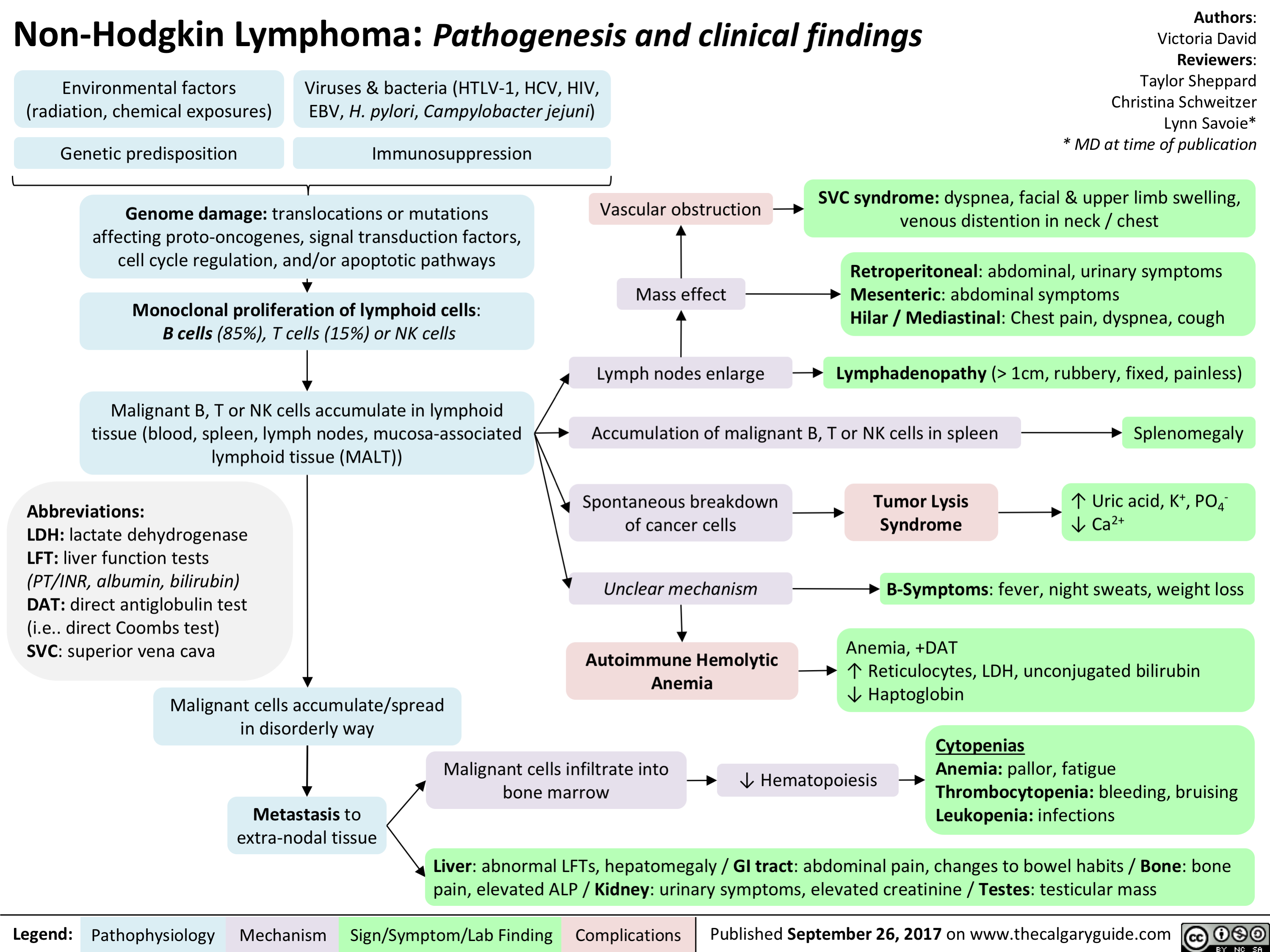
Pelvic Inflammatory Disease
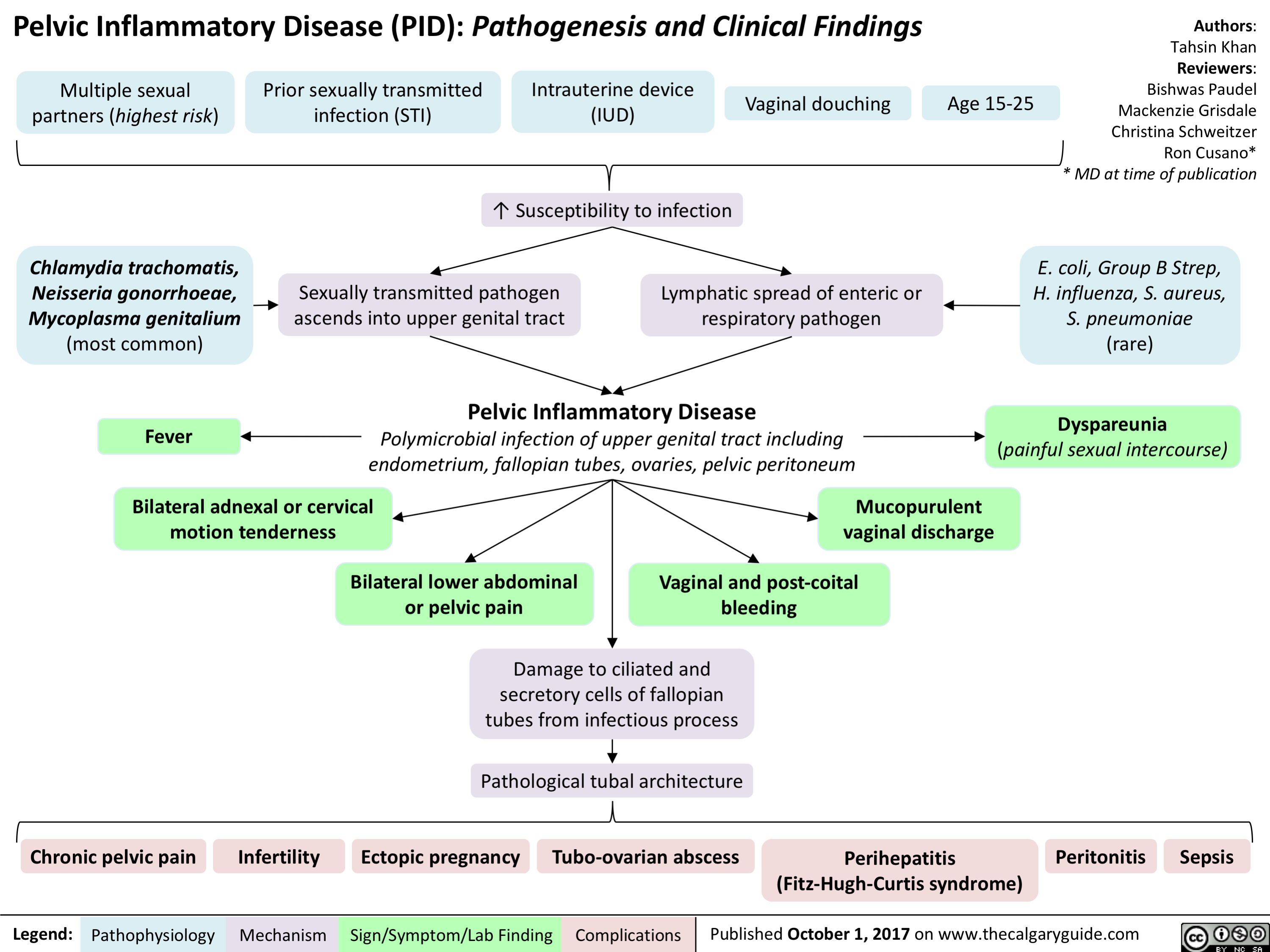
Pituitary Mass Effects
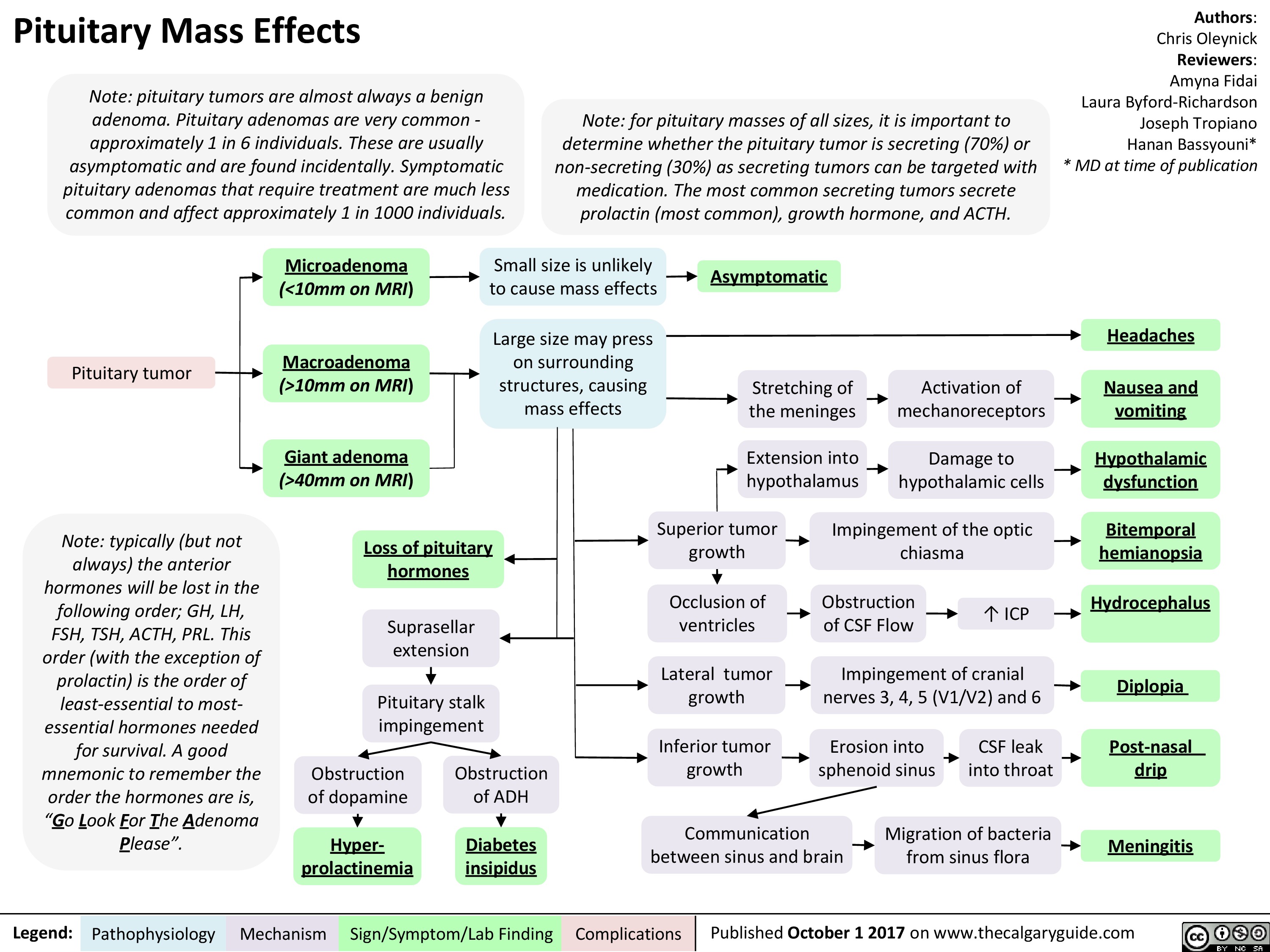 10mm on MRI) vomiting Giant adenoma Extension into hypothalamus —1■• Damage to hypothalamic cells Hypothalamic (>40mm on MRI) dysfunction Obstruction of dopamine Superior tumor growth Impingement of the optic chiasma Bitemporal Loss of pituitary hemianopsia hormones ICP Suprasellar extension Occlusion of ventricles Obstruction of CSF Flow Hydrocephalus Lateral tumor growth Impingement of cranial nerves 3, 4, 5 (V1/V2) and 6 4 Pituitary stalk impingement Diplopia Inferior tumor growth Erosion into sphenoid sinus CSF leak into throat Post-nasal Obstruction of ADH drip Communication between sinus and brain Migration of bacteria from sinus flora Hyper-Diabetes Meningitis prolactinemia insipidus
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 1 2017 on www.thecalgaryguide.com
" title="Pituitary Mass Effects
Note: pituitary tumors are almost always a benign adenoma. Pituitary adenomas are very common -approximately 1 in 6 individuals. These are usually asymptomatic and are found incidentally. Symptomatic pituitary adenomas that require treatment are much less common and affect approximately 1 in 1000 individuals.
Pituitary tumor
Note: typically (but not always) the anterior hormones will be lost in the following order; GH, LH, FSH, TSH, ACTH, PRL. This order (with the exception of prolactin) is the order of least-essential to most-essential hormones needed for survival. A good mnemonic to remember the order the hormones are is, "Go Look For The Adenoma Please".
Legend:
Note: for pituitary masses of all sizes, it is important to determine whether the pituitary tumor is secreting (70%) or non-secreting (30%) as secreting tumors can be targeted with medication. The most common secreting tumors secrete prolactin (most common), growth hormone, and ACTH.
Authors: Chris Oleynick Reviewers: Amyna Fidai Laura Byford-Richardson Joseph Tropiano Hanan Bassyouni* * MD at time of publication
Microadenoma Small size is unlikely to cause mass effects (<10mm on MRI) Asymptomatic Macroadenoma Large size may press on surrounding structures, causing mass effects Headaches Stretching of the meninges Activation of mechanoreceptors Nausea and (>10mm on MRI) vomiting Giant adenoma Extension into hypothalamus —1■• Damage to hypothalamic cells Hypothalamic (>40mm on MRI) dysfunction Obstruction of dopamine Superior tumor growth Impingement of the optic chiasma Bitemporal Loss of pituitary hemianopsia hormones ICP Suprasellar extension Occlusion of ventricles Obstruction of CSF Flow Hydrocephalus Lateral tumor growth Impingement of cranial nerves 3, 4, 5 (V1/V2) and 6 4 Pituitary stalk impingement Diplopia Inferior tumor growth Erosion into sphenoid sinus CSF leak into throat Post-nasal Obstruction of ADH drip Communication between sinus and brain Migration of bacteria from sinus flora Hyper-Diabetes Meningitis prolactinemia insipidus
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 1 2017 on www.thecalgaryguide.com
" />
10mm on MRI) vomiting Giant adenoma Extension into hypothalamus —1■• Damage to hypothalamic cells Hypothalamic (>40mm on MRI) dysfunction Obstruction of dopamine Superior tumor growth Impingement of the optic chiasma Bitemporal Loss of pituitary hemianopsia hormones ICP Suprasellar extension Occlusion of ventricles Obstruction of CSF Flow Hydrocephalus Lateral tumor growth Impingement of cranial nerves 3, 4, 5 (V1/V2) and 6 4 Pituitary stalk impingement Diplopia Inferior tumor growth Erosion into sphenoid sinus CSF leak into throat Post-nasal Obstruction of ADH drip Communication between sinus and brain Migration of bacteria from sinus flora Hyper-Diabetes Meningitis prolactinemia insipidus
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 1 2017 on www.thecalgaryguide.com
" title="Pituitary Mass Effects
Note: pituitary tumors are almost always a benign adenoma. Pituitary adenomas are very common -approximately 1 in 6 individuals. These are usually asymptomatic and are found incidentally. Symptomatic pituitary adenomas that require treatment are much less common and affect approximately 1 in 1000 individuals.
Pituitary tumor
Note: typically (but not always) the anterior hormones will be lost in the following order; GH, LH, FSH, TSH, ACTH, PRL. This order (with the exception of prolactin) is the order of least-essential to most-essential hormones needed for survival. A good mnemonic to remember the order the hormones are is, "Go Look For The Adenoma Please".
Legend:
Note: for pituitary masses of all sizes, it is important to determine whether the pituitary tumor is secreting (70%) or non-secreting (30%) as secreting tumors can be targeted with medication. The most common secreting tumors secrete prolactin (most common), growth hormone, and ACTH.
Authors: Chris Oleynick Reviewers: Amyna Fidai Laura Byford-Richardson Joseph Tropiano Hanan Bassyouni* * MD at time of publication
Microadenoma Small size is unlikely to cause mass effects (<10mm on MRI) Asymptomatic Macroadenoma Large size may press on surrounding structures, causing mass effects Headaches Stretching of the meninges Activation of mechanoreceptors Nausea and (>10mm on MRI) vomiting Giant adenoma Extension into hypothalamus —1■• Damage to hypothalamic cells Hypothalamic (>40mm on MRI) dysfunction Obstruction of dopamine Superior tumor growth Impingement of the optic chiasma Bitemporal Loss of pituitary hemianopsia hormones ICP Suprasellar extension Occlusion of ventricles Obstruction of CSF Flow Hydrocephalus Lateral tumor growth Impingement of cranial nerves 3, 4, 5 (V1/V2) and 6 4 Pituitary stalk impingement Diplopia Inferior tumor growth Erosion into sphenoid sinus CSF leak into throat Post-nasal Obstruction of ADH drip Communication between sinus and brain Migration of bacteria from sinus flora Hyper-Diabetes Meningitis prolactinemia insipidus
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 1 2017 on www.thecalgaryguide.com
" />
Acute Chest Syndrome (Sickle Cell Disease)
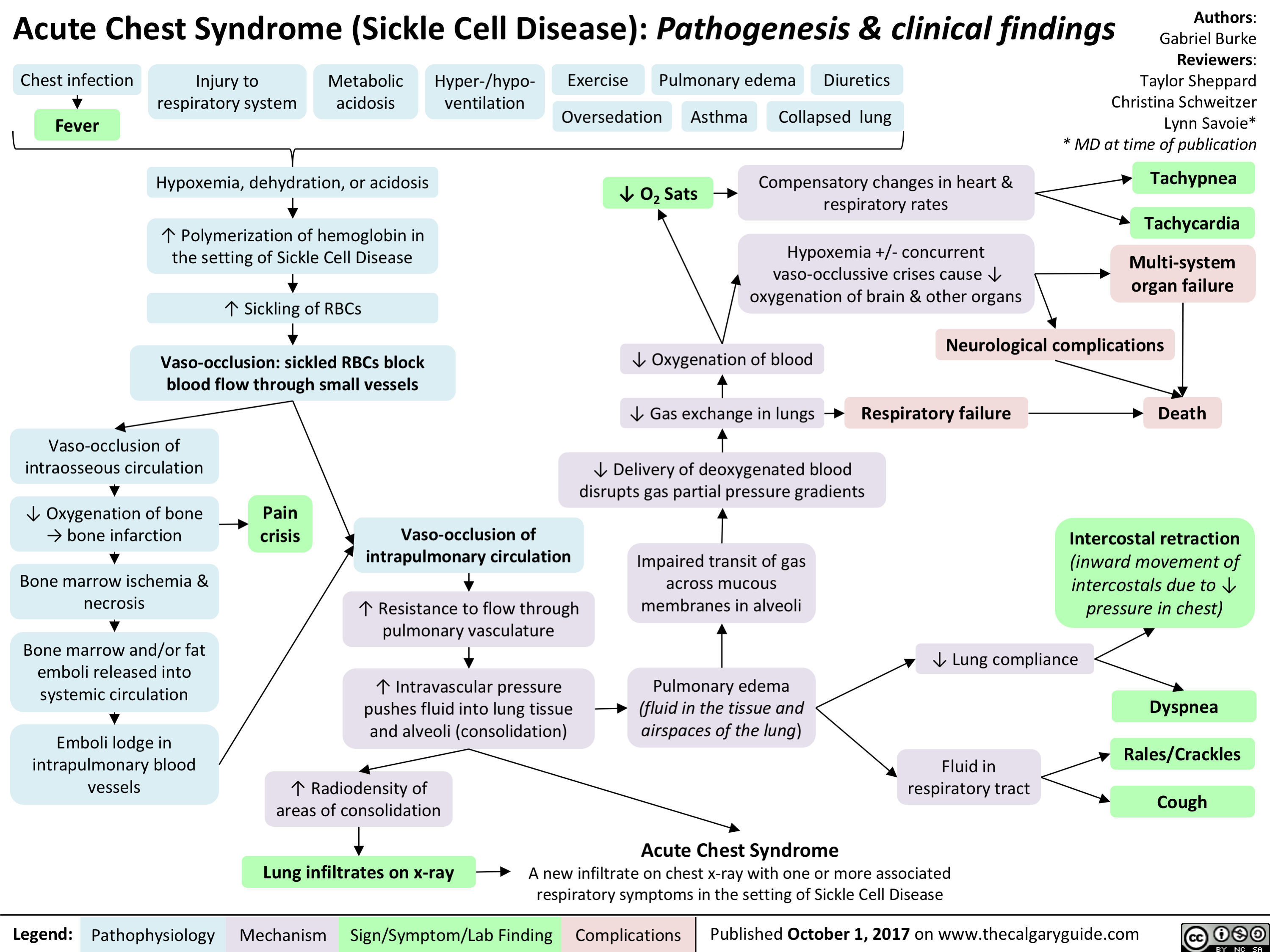
tetanus

Anaphylaxis - Pathogenesis
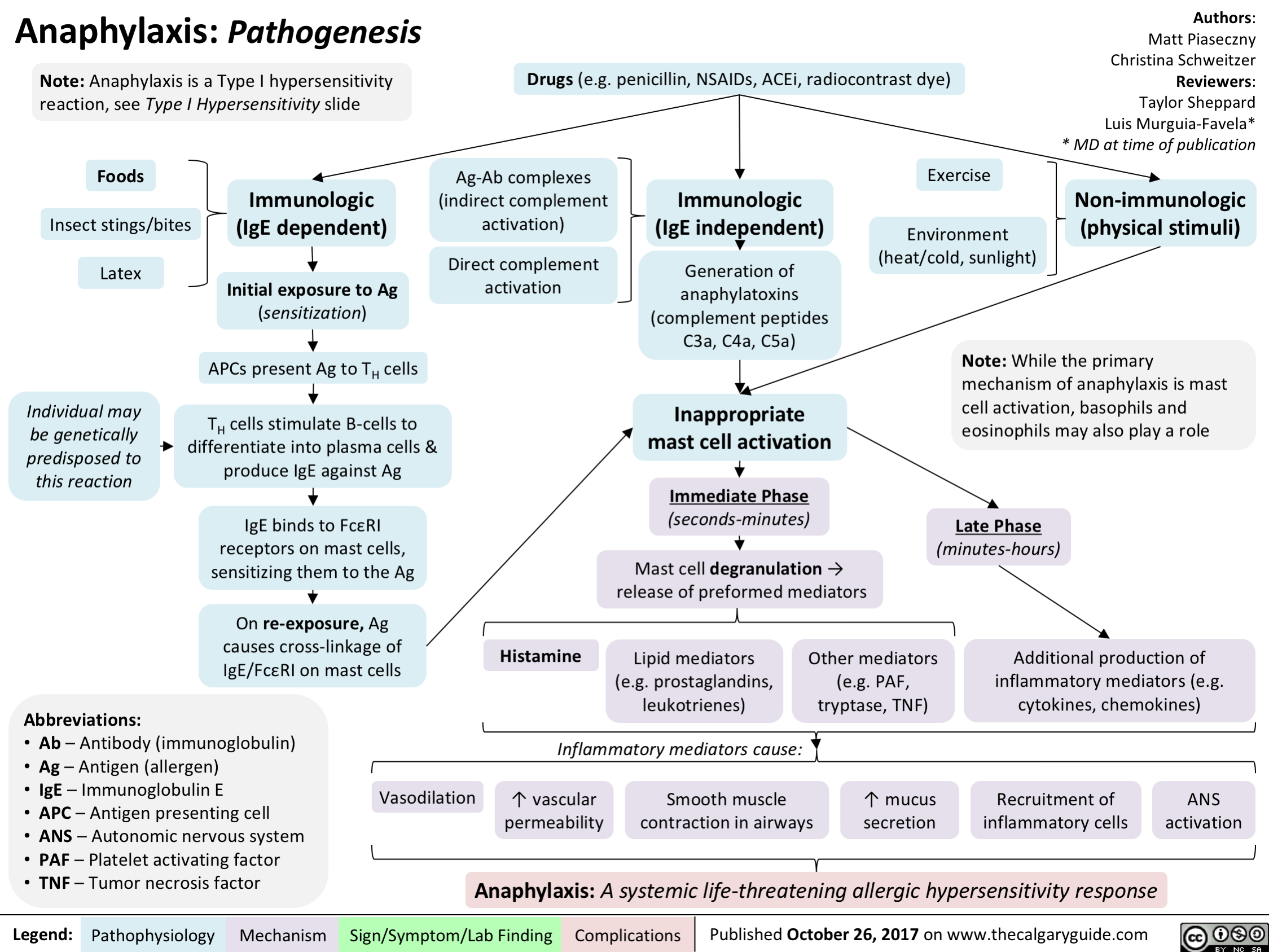
Ischemia: Pathogenesis of Cellular Injury and Death

Hepatitis C (HCV) Infections: Explaining Serology Patterns
 Infections: Explaining Serology Patterns
Seroconversion occurs on average 8-9 weeks after exposure to antigen
H CV RNA Negative
Anti-HCV Antibody Positive2
HCV RNA Positive4
1 HCV Screen
Anti-HCV Antibody Negative
Suspected acute HCV3
HCV RNA will be positive in blood within 1-3 weeks after exposure
No risk factors; likely no HCV exposure
HCV RNA Negative
No HCV exposure
HCV cleared spontaneously or with treatment or false positive antibody test6
Acute HCV (15%) 5Chronic HCV (85%)
HCV RNA negative 12 or 24 weeks after stopping therapy (SVR12 or SVR24)
Abbreviations: SVR12: sustained virologic response after 12 weeks SVR24: sustained virologic response after 24 weeks
Hepatocellular Carcinoma
Cirrhosis
Decompensation (ascites, variceal bleeding, encephalopathy)
7 Liver Transplant
Death
Authors: Emma Boyce Sarah Lacny Reviewers: Peter B i s h ay Joesph Tropiano Yin Chan* * MD at time of publication
Notes: 1Indications for HCV screen: born between 1945-1965, ↑ALT/AST, IVDU, received blood or organ transplant before 1992, received clotting factors before 1987, HIV infected or multiple sexual partners, tattoos and piercings (especially if done in prison), dialysis patients, Egyptian background 2There is no HCV vaccine; an anti-HCV positive test result indicates exposure to the virus 3Seve re l y immunocompromised, hemodialysis, possible exposure, clinical manifestations 4Assess genotype and viral load (HCVRNA), symptoms, and potential exposures to diagnose chronic versus acute HCV 5Acute HCV infection is defined as the first 6 months following exposure 6The anti-HCV antibody does not protect against future infections 7Liver transplant recipients have an 80% chance of developing a recurrent HCV infection
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published NOVEMBER 12, 2017 on www.thecalgaryguide.com")
Hepatitis C (HCV) Infection: Explaining Serology Patterns
 Infections: Explaining Serology Patterns
Seroconversion occurs on average 8-9 weeks after exposure to antigen
H CV RNA Negative
Anti-HCV Antibody Positive2
HCV RNA Positive4
1 HCV Screen
Anti-HCV Antibody Negative
Suspected acute HCV3
HCV RNA will be positive in blood within 1-3 weeks after exposure
No risk factors; likely no HCV exposure
HCV RNA Negative
No HCV exposure
HCV cleared spontaneously or with treatment or false positive antibody test6
Acute HCV (15%) 5Chronic HCV (85%)
HCV RNA negative 12 or 24 weeks after stopping therapy (SVR12 or SVR24)
Abbreviations: SVR12: sustained virologic response after 12 weeks SVR24: sustained virologic response after 24 weeks
Hepatocellular Carcinoma
Cirrhosis
Decompensation (ascites, variceal bleeding, encephalopathy)
7 Liver Transplant
Death
Authors: Emma Boyce Sarah Lacny Reviewers: Peter B i s h ay Joesph Tropiano Yin Chan* * MD at time of publication
Notes: 1Indications for HCV screen: born between 1945-1965, ↑ALT/AST, IVDU, received blood or organ transplant before 1992, received clotting factors before 1987, HIV infected or multiple sexual partners, tattoos and piercings (especially if done in prison), dialysis patients, Egyptian background 2There is no HCV vaccine; an anti-HCV positive test result indicates exposure to the virus 3Seve re l y immunocompromised, hemodialysis, possible exposure, clinical manifestations 4Assess genotype and viral load (HCVRNA), symptoms, and potential exposures to diagnose chronic versus acute HCV 5Acute HCV infection is defined as the first 6 months following exposure 6The anti-HCV antibody does not protect against future infections 7Liver transplant recipients have an 80% chance of developing a recurrent HCV infection
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published NOVEMBER 12, 2017 on www.thecalgaryguide.com")
Medical Conditions Causing Mania or Mania-Like Episodes: Pathogenesis
 pathway
4, myelin synthesis and neurotransmitter regulation
Altered Thyroid Activity Corticosteroid Use 7),
4, thyroid activity
4, central serotonin activity
4, postsynaptic beta-adrenergic receptor activity 4, in catecholamine (including dopamine) transmission
Adrenocortical hormones t Dopamine D2 receptor numbers (hypothesis)
Note: Mania is defined as at least 1 week of abnormally and persistently elevated, expansive, or irritable mood, and abnormally and persistently increased goal-directed activity or energy
By definition, a manic episode is not caused by drugs/medication or a medical illness, therefore those with a non-psychiatric underlying cause are mania-like episodes. Note as well that the conditions listed are not an exhaustive list
Legend:
Pathophysiology Mechanism
Manic episodes precipitated by Dopamine D2 receptor overactivity and 4, serotonergic regulation (hypothesis)
Additional environmental precipitating factors including lack of sleep, social stress, or change Mania or Mania-like Episode
Sign/Symptom/Lab Finding
Complications
Authors: Emily Ower Reviewers: Alexa Scarcello Usama Malik Dr. Lauren Zanussi* * MD at time of publication")
Left Heart Failure: Pathophysiology (Neurohormonal Activation)

Frank Starling Mechanism • The Frank Starling mechanism of the heart represents the relationship between preload (EDV) and SV • As preload (EDV) increases, SV increases, because higher volumes of blood in the ventricles stretch the cardiac fibers and increases cardiac contraction during systole. However, volume overload causes reduced SV.
Myocardial Dysfunction: • Left ventricular Compensatory 4, SV 4A, CO 4 Mechanisms
4, BP
Important equations: • BP = CO x SVR • CO = SV x HR Cardiac hemodynamics: • Stroke volume is affected by three factors 1) Preload (end-diastolic volume (EDV)) 2) Afterload (resistance to LV ejection) 3) Contractility (inherent strength of contraction of LV myocytes) Definition of heart failure: • Myocardial dysfunction (systolic or diastolic) results in decreased CO, such that the heart cannot meet the body's metabolic demands or can only do so at elevated filling pressures
Anti-diuretic hormone (ADH) activation: Arginine 4, BP 4 carotid sinus Vasopressin --• and aortic arch (V2) receptor baroceptors activation activation 4 I` ADH release
RAAS System: 4, BP 4 t release of renin from the juxtaglomerular kidney cells due to renal hypoperfusion
SNS System: In response to CO, 4 SNS t release of (catecholamines) norepinephrine and epinephrine
Adrenal Glands: Aldosterone release
Angiotensin II Type 1 receptor activation
al receptor activation
13, receptor activation
—•
Renal Collecting Ducts: t H2O retention
Renal Distal —• Tubules: t Na+ & H2O retention
Heart: Activation of fibroblasts 4 collagen synthesis and hypertrophy
Blood Vessels: Peripheral vasoconstriction 4 SVR
Heart: Chronic p, receptor activation 4 Ca2+ overload myocyte apoptosis
Heart: Increase HR to maintain normal CO
Maladaptive Response: t preload (EDV), —• volume overload
Abbreviations: • SV — Stroke volume • CO — Cardiac output • SVR — Systemic vascular resistance • BP — Blood pressure • RAAS — Renin-Angiotensin-Aldosterone System • SNS — Sympathetic nervous system
tin systemic and pulmonary congestion via the Frank-Starling Mechanism
Maladaptive 1` resistance Response: t BP, —• against LV afterload ejection 4 4, SV
Maladaptive Response: Adverse LV remodelling
Maladaptive Response: t myocardial oxygen demand and 4, diastolic time
4, contractility —• of the heart
4, coronary blood flow 4 myocardial ischemia
Physical signs and symptoms of congestive heart failure (see relevant slide)
Authors: Sunny Fong Reviewers: —• I Jack Fu Usama Malik Dr. Jason Waechter* *MD at time of publication")
Primary Spontaneous Pneumothorax: Pathogenesis and clinical findings

Malnutrition Smoking
Structurally compromised lung parenchyma
Notes: • PSPs usually occur at rest • Respiratory symptoms vary in severity • Suspect thoracic endometriosis in young women with recurrent PSPs that coincide with menstruation • *Pathophysiology of tension pneumothorax is described in a separate slide
Air leaks into the subcutaneous tissue
Subcutaneous emphysema
Authors: Lauren Hampton Reviewers: Kening (Midas) Kang Natalie Morgunov Sadie Kutz Usama Malik Leila Barss* * MD at time of publication
Thoracic Ischemia endometriosis
Mechanical forces of respiration create blebs Inflammation disrupts mesotheial and/or bullae ~ cell layer of the visceral pleura
47
Spontaneous rupture of blebs or bullae
47
Sudden onset pleuritic chest pain
71r
Primary spontaneous pneumothorax: Presence or introduction of air in the pleural space in a patient WITHOUT diagnosed or clinically apparent lung disease Tachycardia Abbreviations: Communication occurs between the alveoli and pleural space • FLCN- Folliculin gene • HCY- Homocystinuria • MFS- Marfan syndrome Alveolar pressure > pleural pressure • CTD- Connective tissue disease • PSP- Primary spontaneous Air from the lungs enters the pleural space pneumothorax • V/Q- ventilation/perfusion Air separates the chest from /1` intrapleural pressure • Sp02- oxygen saturation the lung parenchyma Small areas of lung collapse Blood flow to areas of On affected side: under un-opposed intrinsic atelectasis is maintained -• Si, chest wall expansion elastic recoil while ventilation 4, t resonance to percussion Si, or absent tactile fremitus Si, or absent breath sounds 4, lung compliance Shunting and V/Q mismatch Pleural line on chest x-ray 1` work of breathing Tension pneumothorax* Accessory muscle use, 4• Sp02, Sudden onset dyspnea, Tachycardia Hypotension, Juglar venous Tachypnea distension, Pulsus paradoxus")
Anksiozne motnje: patogeneza tesnobe

Depresivna epizoda/motnja: patogeneza in klinične najdbe

pomanjkanje tesnih, zaupnih odnosov
druibeni dejavniki
Prevalenca 10-15 % pri 2enskah in 5-12 % pri mogkih. Razmerje med 2enskami in mc&imi 2:1. Pogosteja pri razvezanih, laenih in samskih ter tistih z nizkim druThenoekonomskim stanjem.
depresivna epizoda/motnja simptomi (po DSM 5 merilih) prisotni tekom istega dvotedenskega obdobja in pomenijo odklon od premorbidne ravni funkcioniranja drugi simptomi pomanjkanje libida tesnoba razpolo2enje '6ez dan niha (ang. diurnal variation) huje pozimi (sezonska depresivna motnja) halucinacije (psihotiCna depresija) blodnje (psihotiena depresija) anhedonija (izguba zanimanj/u2itkov) depresivno razpolo2enje nejeknost ali povaan apetit s pridrdienimi spremembami telesne te2e (4, ali 1`) anergija (utrujenost) nespanost ali preva spanja okrajgave: 5-HT - serotonin NA - noradrenalin nastop v mesecu po porodu (poporodna depresija) obC'utki niC'vrednosti ali pretirane krivde psihomotorit'na upaasnjenost ali agitiranost upad spoznavnih sposobnosti (zlasti motnje pozornosti) ponavljajae se misli na smrt/samomor")
Obsesivno-kompulzivna motnja: patogeneza in klinične najdbe
 z bolnikovim vrednostnim sistemom (")
Panična motnja: patogeneza in klinične najdbe
.
izogibajoEe vedenje izogibanje okolikinam, ki poustvarjajo telesne ob6utke, podobne panithemu napadu (telesna vadba, u2ivanje kofeina ali alkohola, obisk savne)
Legenda:
patofiziologija mehanizem
kognitivno: bolnik si telesne obEutke razlaga kot katastrofibe 4 povet'anje vzburjenja
avtorica: Jenna Thomas pregledali: Saara Meunier, Yan Yu, Margaret Oakander*
* dr. med. ob objavi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
-1110
psiholoKki simptomi nenadzorovan strah pred simptomi/izgubo nadzora/smrtjo obt'utek izgubljanja stika z realnostjo
vzdrievalno vedenje
varovalno vedenje npr. posedovanje pomirjeval, iskanje najbli2je bolnignice (z namenom oUutka varnosti v primeru panibega napada)
znak/simptom/laboratorijska najdba
pogosto pridruiene druge dugevne bolezni: • anksiozne motnje (npr. generalizirana anksiozna motnja, posttravmatska stresna motnja, obsesivno-kompulzivna motnja) • ponavljajoea se depresivna motnja • bipolama motnja razpoloienja
prilakovanje vnoviZnega napada vsiljive misli in skrbi o tern, kdaj/kje se bo zgodil naslednji panibi napad in kakgne bodo posledice (srannota, nev'nosti)")
Sezonska depresivna motnja: patogeneza in klinične najdbe
, sindrom kasne zaspanosti, odvisnost od alkohola
nevrologki dejavniki nenormalen serotoninergibi prenos
serotoninska hipoteza: zni2ana konc. serotonina v zimskih mesecih
sezonska depresivna motnja
avtorica: Luxey Sirisegaram pregledala: Paul Adamiak, Phillip Stokes* * dr. med. ob objavi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
I
simptomi (po DSM 5 merilih) 2 depresivni epizodi v zadnjih 2 letih z nakazanim casovnim vzorcem pojavljanja
hipersomnija
hiperfagija
sla po u2ivanju ogljikovih hidratov
porast telesne te2e
patofiziologija mehanizem
sezonske posebnosti
sezonski vzorec pojavljanja pri depresivni epizodi/motnji
popolne remisije all obrati faze v dolaenem delu leta
ni povezave s specifithim sezonskim psihosocialnim stresorjem (npr. pove6anim obsegom dela v slu2bi)
znak/simptom/laboratorijska najdba
simptomi, po katerih se loEi od depresivne epizode/motnje
sezonski vzorec pojavljanja (torej v specifibem delu leta)
sezonske depresivne epizode morajo po 'gtevilu presegati ne-sezonske depresivne epizode")
Shizofrenija: patogeneza in klinične najdbe
 (prevladujaa teorija) predmet raziskav)
visoka stopnja izraianja Zustev • (ang. expressed emotion): iivljenje v okolju s pogostimi negativnimi komentarji na raC'un bolnika (I` tveganje za relaps)
shizofrenija
nepravilnosti v 2ivthem prenosu nevrotransmitorjev (predvsem dopamina) v razlithih predelih mo2ganov
dopaminergibega dopaminergiC'nega
prenosa v mezolimbibi poti
dopaminergibi nevroni te6ejo do Iimbicnih struktur in so odgovorni za nadzor nad razpolo2enjem in 6ustvi
moten prenos dopamina v tej poti naj bi bil kriv za pozitivne simptome shizofrenije
prenosa v mezolimbiC'ni poti
avtorica: Yan Yu pregledali: Sara Meunier, Briana Cassetta, JoAnna Fay, Philip Stokes*
* dr. med. ob objavi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
Pomni: • Ceravno smo vzroke za shizofrenijo sprva iskali v biologkih dejavnikih, zdaj vse bolj prepozna-vamo vlogo tako psihologkih (npr. kognitivnih stereotipov) kot druibenih dejavnikov (npr. stresa ali osame) v njeni etiologiji. • pri shizofreniji lahko odkrijemo tudi nevropsihologke primanjkljaje: motnje spomina, psihomotorike in pozornosti ter te2ave s psihi6no prilagodljivostjo. • Genetske modifikacije C4 gena naj bi ravno tako igrale va2no vlogo v etiologiji bolezni, saj v 6asu adolescence povzro6ajo pove6ano zmanjgevanje gtevila sinaps (nova hipoteza).
dopaminergibi nevroni te6ejo do razlibih predelov mo2g. skorje (npr. moten prenos dopamina v tej frontalnega re2nja) in so odgovorni poti naj bi bil kriv za negativne za migljenje, odlaanje, tvorbo simptome shizofrenije jezika in razpolo2enje
negativni simptomi (okrnjeno izraianje 6ustev, 6ustvena otopelost, osiroma§en govor, brezvoljnost, ‘iY miselna zavrtost, nedruiabno vedenje)
blodnje (nespremenljiva, zmotna prepriEanja, odstopajoEa od bolnikovega kulturnega ozadja)
Legenda: patofiziologija mehanizem
ha lucinacije (zaznave brez dra2ljajev; obiC'ajno pri shizofreniji a kustiC'n e)
dezorganiziran/nesmisein govor (tangencialni odgovori, ohlapne asociacije, besedna solata)
znak/simptom/laboratorijska najdba
hudo dezorganizirano vedenje, vkljauja katatonijo (neodzivnost na zunanje dra2ljaje)")
Serotoninski sindrom: patogeneza in klinične najdbe
, opioidi, antiemetiki, triptani, zdravila za izgubo tel. te2e, ilegalne psihoaktivne snovi (npr. kokain, amfetamini)
terapevtska raba
1
interakcije (se posebej pri kombinacijah serotoninergikov) namerna samozastrupitev
serotoninski sindrom raznolika kombinacija sprememb v psihiZnem stanju, vegetativne nestabilnosti in iivZnomigiZne hiperaktivnosti, ki sega od blage do iivljenje ogroiajoL'e z nenadnim nastopom (v nekaj minutah do urah) po administraciji zdravil(a), v vecini primerov pa se razregi v <24 urah po prekinitvi jemanja odgovorne snovi
prekomerna serotoninergitha aktivnost 5-HT receptorjev centralno (v moiganskem deblu) in periferno
sinteza in privzem in T receptorski agonizem sprogEanje 5-HT presnova 5-HT in ok'utljivost
z zdravili povzraene spremembe v relativnem razmerju ne-serotoninergithih nevrotransmitorjev (npr. pove6anje konc. noradrenalina)
spremenjeno psihreno stanje
tesnoba, zmedenost, agitacija, hipervigilnost, dolgoveznost, delirij, koma
vegetativna nestabilnost
mrzlica/drgetanje, 6ezmerno potenje, vraina, driska, tahikardija, ra8irjene zenice, hipertenzija
avtorica: Preeti Kar pregledali: Erika Russell, Usama Malik, Aaron Mackie*
* dr. med. ob objavi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
Pomni: za klinicno postavitev diagnoze uporabljamo Hunterjeva merila serotoninske toksiZnosti: - zgodovina jemanja serotoninergithih snovi v preteklih 5 tednih + kateri koli od naslednjih pogojev: • spontani klonus • inducirani klonus in bodisi agitacija bodisi L'ezmerno potenje • aesni klonus in bodisi agitacija bodisi L'ezmerno potenje • tremor in hiperrefleksija • hipertonija, tel. temperatura >38 °C in bodisi aesni klonus bodisi inducirani klonus
ihgnomigiZna hiperaktivnost
hiperrefleksija, mR")
Zaviralci privzema serotonina in noradrenalina (SNRI): mehanizem delovanja in neželeni učinki
: mehanizem delovanja in neieleni utinki
zaviralci privzema serotonina in noradrenalina predstavnika: venlafaksin, duloksetin
konc. 5-HT in NA v 02S/P2S
farmakologija
farmakokinetika farmakodinamika
nenadna prekinitev jemanja zdravila ali vnos
avtorici: JoAnna Fay, Sara Meunier pregledali: Jojo Jiang, Alexander Arnold, Jessica Asgarpour, Aaron Mackie*
iz krvnega obtoka jih odstranijo jetra
zavirajo prenagalec za privzem NA (NET) in prenaalec za privzem 5-HT (SERT)
5-HT in NA ostaneta v sinapsah dlje in podaVata oz. okrepita iiv6ni prenos
odtegnitev namerno predoziranje nenamerno povzrocene interakcije nepri6akovan odziv na terapevtski odmerek prekometna v aktivnost 02S/P2S sindrom 1` 5-HT omotica 5-HT serotoninski omotica driska nejegZnost nespeEnost nespanost slabost utrujenost glavobol vegetativna * iivEnomiKiEne kognitivne hiperaktivnost nepravilnosti spremembe vrtoglavica potencialno iivljenje ogroiajoE spolne hipertenzija olesni klonus agitacija motn'e porast tahikardija tremor akatizra tel. tee raigir-ene hiperrefleksija zenice migiEni klonus
Legenda: patofiziologija
mehanizem
znak/simptom/laboratorijska najdba
1` NA
slabost
Zezmerno potenie
* dr. med. ob objavi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
v primeru ietrnih bolezni in/ali saasne rabe zaviralcev/sproncev CYPD26 ie potrebna prilagoditev odmerka
izboljganje depresivne in anksiozne simptomatike 1 blokada ponovnega privzema 5-HT in NA v sinapsah pa u6inka SNRI ne pojasni v celoti
posredno SNRI povzro6ijo sproManja nevrozaMitnih proteinov, denimo BDNF, ki bi naj imel po podatkih §tudij protivnetno delovanje
za dosego kliniEnega uZinka ie potrebnih 3-8 tednov all veZ zdravlienia
okralgave in opombe: 5-HT— serotonin NA— noradrenalin BDNF — mo2ganski nevrotrofiEni faktor 025 — osrednji 2ivEni sistem P2S — periferni 2ivEni sistem *vegetativen — nanagajoE se na avtonomni 2ivEni sistem")
Socialna anksiozna motnja: patogeneza in klinične najdbe

Selektivni zaviralci privzema serotonina (SSRI): mehanizem delovanja in neželeni učinki
: mehanizem delovanja in neieleni utinki
selektivni zaviralci privzema serotonina predstavniki: citalopram, escitalopram, fluoksetin, paroksetin, sertralin
farmakologija
Pomni: dolo6eni SSRI z ve6jo verjetnostjo povzro6ajo nekatere od na'gtetih neielenih ainkov. Zmanigamo jih lahko z zamenjavo z drugim SSRI, postopnim titriranjem odmerka ali razdelitvijo dnevnega odmer-ka. Antidepresivi lahko zvgajo tveganje za samomor pri mlajsih od 24 let, pri starelgih od 31 let pa ga lahko znilajo.
farmakokinetika
farmakodinamika
iz krvnega obtoka jih odstranijo jetra
zavirajo privzem 5-HT in povzraijo sinaptibe konc. 5-HT
avtorici: JoAnna Fay, Sara Meunier pregledali: Jojo Jiang, Alexander Arnold, Aaron Mackie*
* dr. med. ob objavi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
v primeru jetrnih bolezni je potrebna prilagoditev odmerka
lahko zavrejo jetrne encime citokroma P4502D6 in povzraijo interakcije med zdravili
tel. teie omotica 4 5-HT ostane v sinapsah dlje in podaVa oz. okrepi 2iv6ni prenos izboVanje depresivne in anksiozne simptomatike spolne motnje vrtoglavica nejeknost namerno predoziranje nenadna prekinitev jemanja zdravila ali I, vnos blokada ponovnega privzema 5-HT v sinapsah pa u6inka SSRI ne pojasni v celoti prekometna aktivnost 5-HT v 02S/P2S nenamerno povzro'6ene interakcije konc. 5-HT v O2S/P2S posredno SSRI povzraijo sprokanja nevrozakitnih proteinov, denimo BDNF, ki bi naj imel po podatkih gtudij protivnetno delovanje nepriakovan odziv na terapevtski odmerek serotoninski sindrom odtegnitveni sindrom
potencialno iivljenje ogroiajoE 1 vegetativna * iivEnomiKiEne nepravilnosti kognitivne spremembe omotica tremor za dosego kliniEnega uEinka je potrebnih hiperaktivnost slabost none more 3-8 tednov ali veE zdravljenja okrajgave in opombe: 5-HT— serotonin BDNF — nnoiganski nevrotrofi6ni faktor 025 — osrednji 2ivcni sistem P2S — periferni iivcni sistem *vegetativen— nanagajo6 se na avtonomni iivcni sistem hipertenzija olesni klonus agitacija Eezmerno")
Nevroanatomija in fiziologija čustev
![Nevroanatomija in fiziologija tustev
bazalni gangliji
prefrontalna skorja obdeluje 6ustva vgje-ga reda, ki zahtevajo priklic, razum(sko) presojo in sposobnost odloCanja (npr. sramota) senzorne informacije iz notranjih organov kot odziv na spralne okoljske objekte ali dogodke integrira z informacijami iz amigdale
Zustveni obEutki (npr. zavestne izkugnje Zustev)
1—
talamus
Zustveno izstopaja okoljski drailjaj
zaznave (npr. vid, sluh, tip, oku'ganje, vonjanje)
avtorica: Andrea Moir pregledali: Erika Russell, Usama Malik, Brienne McLane*
* dr. med. ob objavi
hipotalamus (glavna izhodna [ang. output] struktura limbibega sistema)
voh*
prim. in asociacijski predeli mo2g. skorje •
amigdala obdeluje 6ustva niijega reda, torej tista s hitrimi, samodejnimi in pogojevanimi odzivi (npr. strah) sodeluje pri tvorbi in priklicu C'ustveno pomembnih spominov iz neokortikalnih podrodj, torej zaznavi pripi§e neko Custveno vrednost
hipokampus (kljaen za utrditev in priklic spominov)
motorl6ni, endokrini in visceralni sistemi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
avtonomni zivcni sistem (A2S) A2S se samodejno in podzavestno odziva na okoljske dra2ljaje (npr. s '(` frekvence sr6nega utripa ali zardevanjem)
telesni odziv na Zustveni drailja(
Pomni: • Strukture, ki sodelujejo pri C'ustvovanju, se imenujejo limbiEni sistem. • Talamus, bazalni gangliji in prefrontalna skoraj skupaj tvorijo kortiko-striato-talamo-kortikalno zanko, ki predstavlja glavno pot za obdelavo C'ustev v moiganih. • Prefrontalna skorja vkljue'uje orbitofrontalno skorjo, dorzolateralno prefrontalno skorjo in sprednjo cingulatno skorjo. • *Voh je edini cut, cigar vlakna zaobidejo talamus in se stekajo neposredno v primarno olfaktorno skorjo.](http://calgaryguide.ucalgary.ca/wp-content/uploads/2017/11/The-Neuroanatomy-and-Physiology-of-Emotion-Slovenian-translation-FINAL-VERSION.png "Nevroanatomija in fiziologija tustev
bazalni gangliji
prefrontalna skorja obdeluje 6ustva vgje-ga reda, ki zahtevajo priklic, razum(sko) presojo in sposobnost odloCanja (npr. sramota) senzorne informacije iz notranjih organov kot odziv na spralne okoljske objekte ali dogodke integrira z informacijami iz amigdale
Zustveni obEutki (npr. zavestne izkugnje Zustev)
1—
talamus
Zustveno izstopaja okoljski drailjaj
zaznave (npr. vid, sluh, tip, oku'ganje, vonjanje)
avtorica: Andrea Moir pregledali: Erika Russell, Usama Malik, Brienne McLane*
* dr. med. ob objavi
hipotalamus (glavna izhodna [ang. output] struktura limbibega sistema)
voh*
prim. in asociacijski predeli mo2g. skorje •
amigdala obdeluje 6ustva niijega reda, torej tista s hitrimi, samodejnimi in pogojevanimi odzivi (npr. strah) sodeluje pri tvorbi in priklicu C'ustveno pomembnih spominov iz neokortikalnih podrodj, torej zaznavi pripi§e neko Custveno vrednost
hipokampus (kljaen za utrditev in priklic spominov)
motorl6ni, endokrini in visceralni sistemi
prevedel in priredil: Jan Kejiar, dr. med., specializant psihiatrije pregledala: doc. dr. Brigita Novak Sarotar, dr. med., spec. psih.
avtonomni zivcni sistem (A2S) A2S se samodejno in podzavestno odziva na okoljske dra2ljaje (npr. s '(` frekvence sr6nega utripa ali zardevanjem)
telesni odziv na Zustveni drailja(
Pomni: • Strukture, ki sodelujejo pri C'ustvovanju, se imenujejo limbiEni sistem. • Talamus, bazalni gangliji in prefrontalna skoraj skupaj tvorijo kortiko-striato-talamo-kortikalno zanko, ki predstavlja glavno pot za obdelavo C'ustev v moiganih. • Prefrontalna skorja vkljue'uje orbitofrontalno skorjo, dorzolateralno prefrontalno skorjo in sprednjo cingulatno skorjo. • *Voh je edini cut, cigar vlakna zaobidejo talamus in se stekajo neposredno v primarno olfaktorno skorjo.")
Diabetic Foot: Pathogenesis and clinical findings
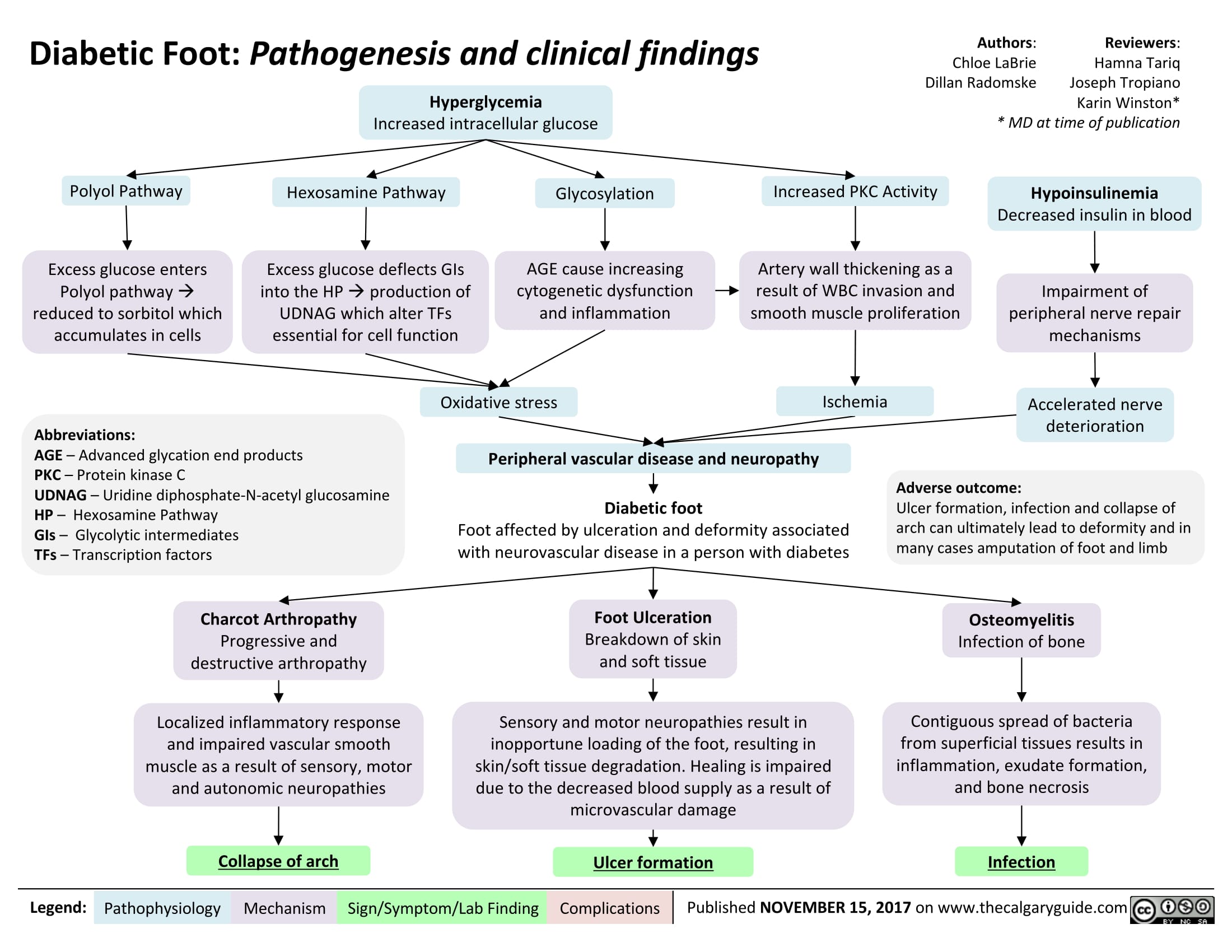
Classification of Pelvic Ring Fractures: Mechanisms, Clinical Features and Complications
 Ring • Instability with External rotation of rotational force on each leg(s) iliac crest' • vectors LC Scrotal, labial or 15 or S1 dermatomal perinea! hematoma parasthesia2 Flank hematoma Vertical Shear (VS) Axial shear force (i.e. fall)3 Loss of rectal tone or Perinea! lacerations Anterior Posterior Compression (APC) Lateral Compression (LC) perirectal sensation De-gloving injuries Direct/indirect AP force causing diastasis of pubic symphysis (i.e. MVC, cyclist)3 *Combination APC Grade Lateral compressive force, causing inward rotation of pelvis (i.e. MCV rollover, pedestrian vs auto)3 Grade 1 Rami ipsilateral LC Grade • Gross hematuria VS Vertical displacement, anterior & posterior through SI joint APC Grade 1 LC Grade 3 Type 1 or 2 injury on the side of trauma + APC on the opposite side of trauma Pubic symphysis diastasis < 2.5cm APC Grade 2 of two can 3 of above occur Sacral on the unilateral 2 Pubic symphysis diastasis Anterior SI diastasis, posterior ligaments intact. Disruption sacrospinous and sacrotuberous ligaments compression fracture side of trauma with or bilateral rami fractures fracture and posterior ilium fracture dislocation APC 2 + disruption of posterior SI ligaments and possible vascular injury
Abbreviations: SI = Sacroiliac Notes: *1- Low sensitivity *2- Most Common *3- Common Mechanisms Authors: Meaghan Mackenzie Reviewers: Annalise Abbott Usama Malik Dr. Prism Schneider* * MD at time of publication Complications Chronic Instability Urogenital Injuries (posterior urethral tear, bladder rupture) NW. Venous thromboembolism Neurologic Injury (L5 and S1)")
Open Fractures: Mechanisms, Clinical Features and Complications
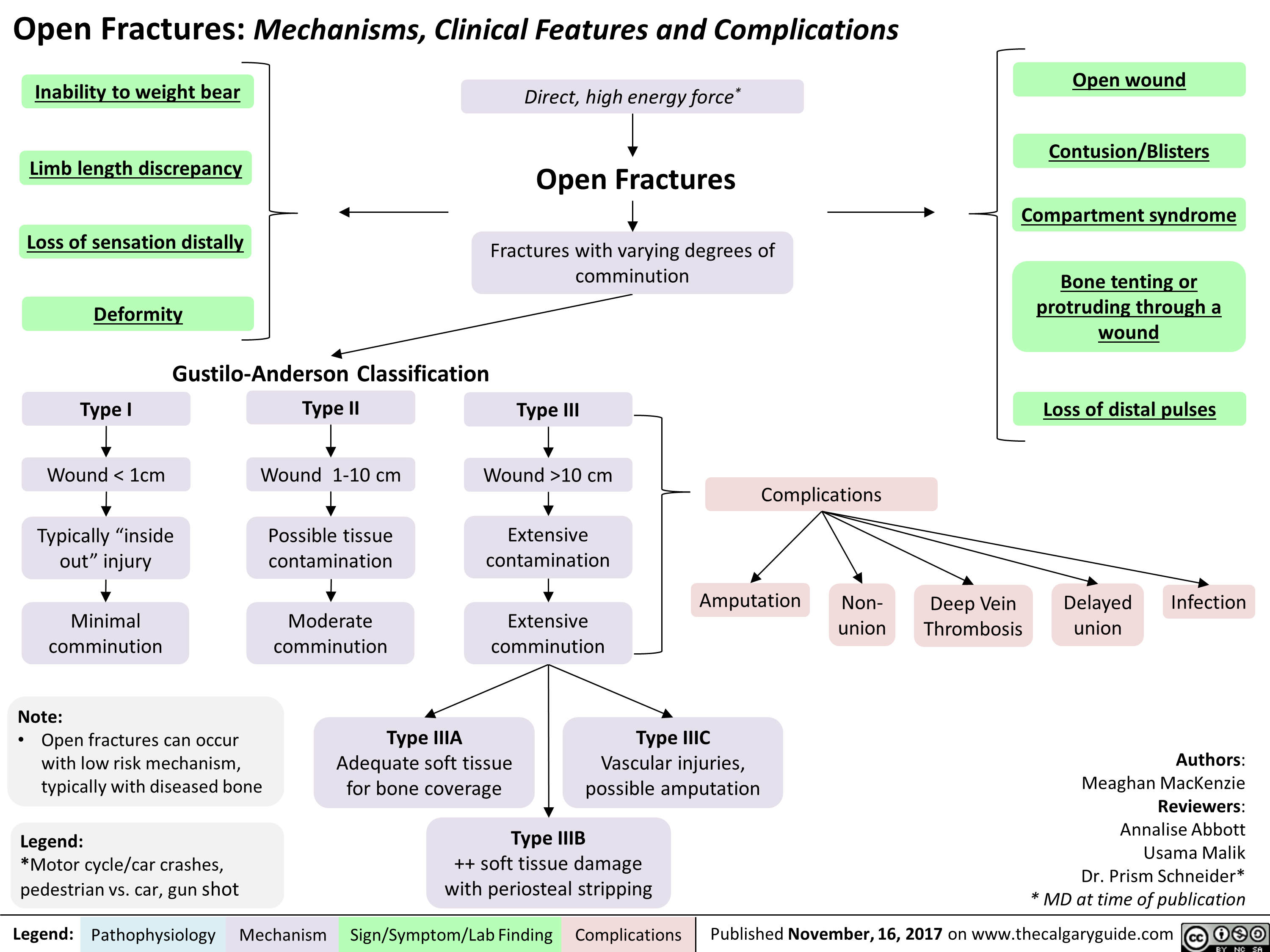 10 cm
4,
Extensive
contamination
Extensive
comminution
Type IIIA
Adequate soft tissue
for bone coverage
Legend: Pathophysiology Mechanism
Complications
Open wound
Contusion/Blisters
Compartment syndrome
Bone tenting or
protruding through a
wound
Loss of distal pulses
Amputation
Type IIIC
Vascular injuries,
possible amputation
•
Type IIIB
++ soft tissue damage
with periosteal stripping
Sign/Symptom/Lab Finding
Non-
union
Deep Vein
Thrombosis
Delayed
union
Infection
Authors:
Meaghan MacKenzie
Reviewers:
Annalise Abbott
Usama Malik
Dr. Prism Schneider*
* MD at time of publication " title="Open Fractures: Mechanisms, Clinical Features and Complications
Inability to weight bear
Limb length discrepancy
•
Loss of sensation distally
Deformity
Gustilo-Anderson Classification
Type I
Wound < 1cm
Typically "inside
out" injury
Yir
Minimal
comminution
Type II
Wound 1-10 cm
4,
Possible tissue
contamination
Moderate
comminution
Note:
• Open fractures can occur
with low risk mechanism,
typically with diseased bone
Legend:
*Motor cycle/car crashes,
pedestrian vs. car, gun shot
Direct, high energy force*
Open Fractures
Fractures with varying degrees of
comminution
Type Ill
Yir
Wound >10 cm
4,
Extensive
contamination
Extensive
comminution
Type IIIA
Adequate soft tissue
for bone coverage
Legend: Pathophysiology Mechanism
Complications
Open wound
Contusion/Blisters
Compartment syndrome
Bone tenting or
protruding through a
wound
Loss of distal pulses
Amputation
Type IIIC
Vascular injuries,
possible amputation
•
Type IIIB
++ soft tissue damage
with periosteal stripping
Sign/Symptom/Lab Finding
Non-
union
Deep Vein
Thrombosis
Delayed
union
Infection
Authors:
Meaghan MacKenzie
Reviewers:
Annalise Abbott
Usama Malik
Dr. Prism Schneider*
* MD at time of publication " />
10 cm
4,
Extensive
contamination
Extensive
comminution
Type IIIA
Adequate soft tissue
for bone coverage
Legend: Pathophysiology Mechanism
Complications
Open wound
Contusion/Blisters
Compartment syndrome
Bone tenting or
protruding through a
wound
Loss of distal pulses
Amputation
Type IIIC
Vascular injuries,
possible amputation
•
Type IIIB
++ soft tissue damage
with periosteal stripping
Sign/Symptom/Lab Finding
Non-
union
Deep Vein
Thrombosis
Delayed
union
Infection
Authors:
Meaghan MacKenzie
Reviewers:
Annalise Abbott
Usama Malik
Dr. Prism Schneider*
* MD at time of publication " title="Open Fractures: Mechanisms, Clinical Features and Complications
Inability to weight bear
Limb length discrepancy
•
Loss of sensation distally
Deformity
Gustilo-Anderson Classification
Type I
Wound < 1cm
Typically "inside
out" injury
Yir
Minimal
comminution
Type II
Wound 1-10 cm
4,
Possible tissue
contamination
Moderate
comminution
Note:
• Open fractures can occur
with low risk mechanism,
typically with diseased bone
Legend:
*Motor cycle/car crashes,
pedestrian vs. car, gun shot
Direct, high energy force*
Open Fractures
Fractures with varying degrees of
comminution
Type Ill
Yir
Wound >10 cm
4,
Extensive
contamination
Extensive
comminution
Type IIIA
Adequate soft tissue
for bone coverage
Legend: Pathophysiology Mechanism
Complications
Open wound
Contusion/Blisters
Compartment syndrome
Bone tenting or
protruding through a
wound
Loss of distal pulses
Amputation
Type IIIC
Vascular injuries,
possible amputation
•
Type IIIB
++ soft tissue damage
with periosteal stripping
Sign/Symptom/Lab Finding
Non-
union
Deep Vein
Thrombosis
Delayed
union
Infection
Authors:
Meaghan MacKenzie
Reviewers:
Annalise Abbott
Usama Malik
Dr. Prism Schneider*
* MD at time of publication " />
Bronchogenic Carcinoma - Pancoast Tumors Pathogenesis and clinical findings

Endothoracic fascia
1— Parietal pleura •
1—
Upper ribs
Large Cell
Carcinoma
Adenocarcinoma
Squamous Cell
Carcinoma
Primary Bronchogenic
Carcinoma
Pancoast tumor:
Local/metastatic growth in
ipsilateral lung apex
Disruption of structures
adjacent to superior
pulmonary sulcus
NSCLC (more common)
Invasion of airways
► causing obstruction
(later stages)
Author:
Bradley Stebner
Daniel Meyers
Midas (Kening) Kang
Reviewers:
Natalie Morgunov
Sadie Kutz
Usama Malik
Kerri Johannson*
*MD at time of publication
Notes:
• Pancoast Tumor: Malignant
lesion occupying the superior
pulmonary sulcus (lung apex)
Bronchogenic carcinoma:
primary malignant neoplasm
arising from epithelium of
bronchus or bronchiole
Pancoast tumors can be caused
by primary or metastatic
pulmonary neoplasms
(described here) as well as
infectious foci
Hemoptysis
Compression of C8
and T1 nerves
•
Disruption of paravertebral
sympathetic chain
Shoulder • Weakness in intrinsic Horner's • 4, sympathetic to to iris muscle Syndrome 4, sympathetic radial to eccrine sweat gland
Pain (ulnar hand muscles
nerve) 4, sympathetic innervation STM
Paresthesia in
4th /5th digits and
arm/forearm medial
Ptosis Mi o sis Anhidrosis Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Compression of SVC
SVC Syndrome
•
4, venous return to
RA
4, Cardiac output to
lungs
Dyspnea
Disruption of RLN
1
Hoarse voice
4, venous drainage
from upper thoracic
cavity
Retention of fluid in
upper limb
•)r
Facial and limb swelling")
Polycystic Ovarian Syndrome

Nitrous Oxide

Anxiolysis
Myeloneuropathy
Encephalopathy
Subacute Combined Degeneration of spinal cord
Peripheral Neuropathy
Hyperhomocysteinemia
Megaloblastic Anemia
Irreversible inhibition of methionine synthase
Modulation of nociception
Stimulation of neurons in PAG of midbrain causes release of E O Ps and/or DY N s
Activation of opioid receptors in GABA-ergicnuclei of pons causes inhibition of inhibitory GABA-ergicpathway
Activation of descending noradrenergic system in spinal cord posterior grey column
Inhibition of primary afferent and second-order neuron nociception
Analgesia
Authors: Parthiv Amin Reviewers: Billy Sun Joseph Tropiano Michael Chong* * MD at time of publication
Abbreviations •CaM-calmodulin •cGMP-cyclic guanosine monophosphate •DYN-dynorphin •EOP-endogenous opioid peptide •GABA-γ-aminobutyric acid •N2O-nitrous oxide •NDMA-N-methyl-D-aspartate •NOS-nitric oxide synthase •PAG-periaqueductal grey area •PKG-protein kinase
Nitrous Oxide
NDMA receptor antagonism: Inhibition of the N D M A glutamate receptor
Closure of NDMA receptor channel
Inhibition of ionic currents
↓ central nervous system excitability
Anesthesia
Quick Facts
1°Use: Anesthesia Adjuvant 2°Use: Analgesia, Dental Sedation, Anxiolytic
Route of Admin.: Inhalation Metabolism: None Excretion: 1°=Lung (exhalation)
Min. Alveolar Conc.: >100% @1atm = Incomplete Anesthetic
Vitamin B12 Inactivation: N2O irreversibly oxidizes Vitamin B12 (cobalamin)
Pyramidal Cell Vacuole Reaction: Swelling of endoplasmic reticulum and mitochondria
Reversible pyramidal cell neurotoxic vacuole reaction in posterior cingulate / retrosplenial cortex
Neurotoxicity
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January,07, 2018 on www.thecalgaryguide.com")
Hyperthyroidism

Hyperthyroidism
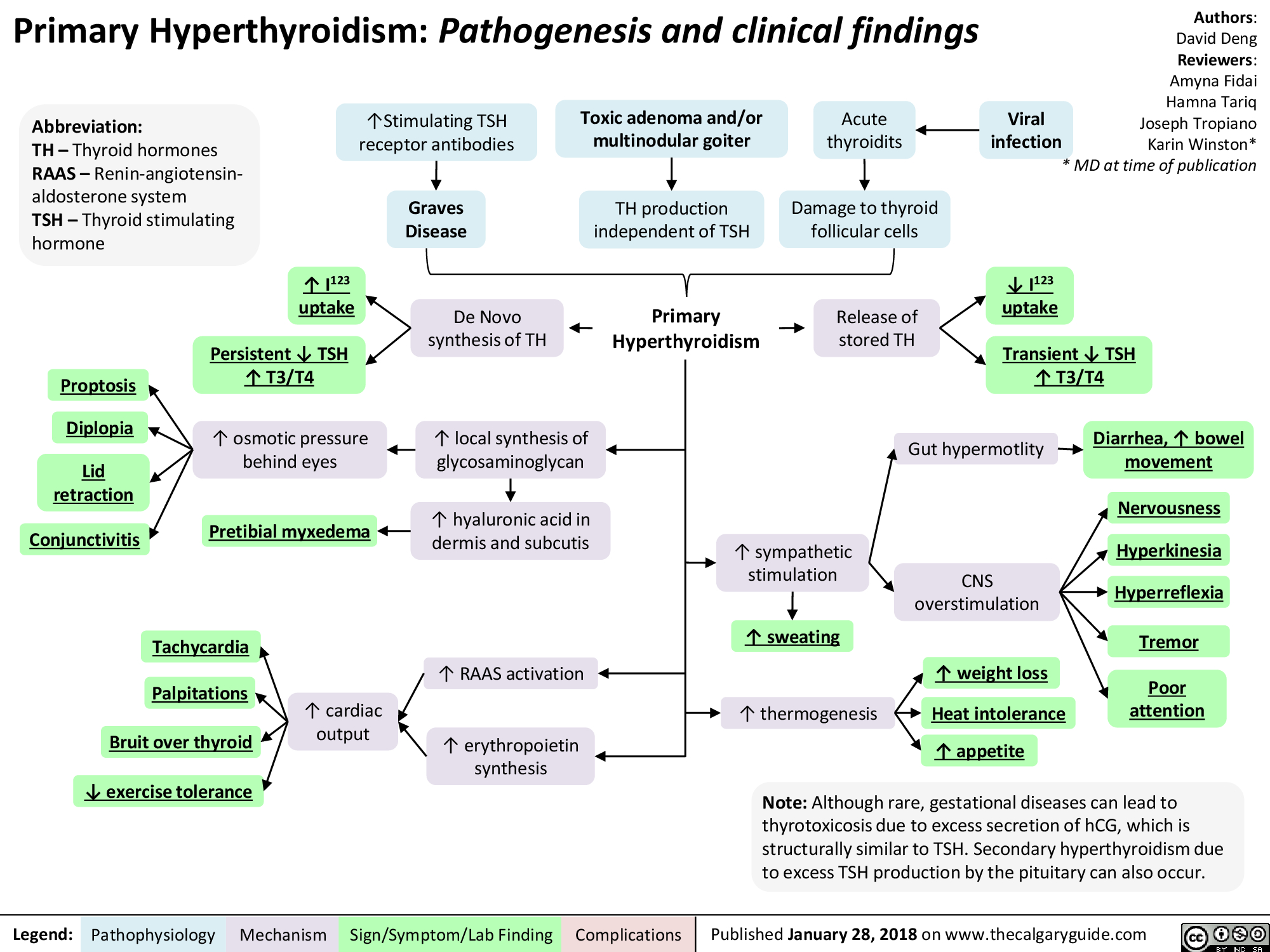
Growth Hormone Excess

Somatotroph adenoma in anterior pituitary
Microduplications in chromosome Xq26.3
4— Plain film
CT/M RI
GH secretion 1\ frequency and amplitude
► GH excess
Imaging 4— Acromegaly/Gigantism
Stimulation/ repression of other hormones
Authors: David Deng Reviewers: Amyna Fidai Hamna Tariq Joseph Tropiano Karin Winston * MD at time of publication
intracranial Pressure
Headache 4—
4, visual confrontation
4, visual acuity
Bitemporal hemianopsia
Abbreviations: • GH: Growth hormone • GHRH: Growth hormone releasing hormone • FSH: Follicle stimulating hormone • LH: Luteinizing hormone • TSH: Thyroid stimulating hormone
Legend:
4--
Local IGF-1 overproduction
Median nerve edema
Connective tissue Carpal tunnel overgrowth syndrome
Acne 4
Coarse features
Hyperhydriosis
Pathophysiology Mechanism
Hypertrichiosis
Macrognathia 1—
Enlarged hands and feet
Sign/Symptom/Lab Finding
Excess insulin secretion
\I, insulin receptor numbers and affinity
Acanthosis Nigricans
Impaired glucose tolerance
Cardiovascular disease
Weight gain
Cardiac arrhythmia
Valvular damage
ejection fraction
► HTN
Notes: • Acromegaly and gigantism share the same pathophysiology but differ mainly in terms of time of onset of GH excess. GH excess prior to growth plate fusion 4 gigantism. GH excess after growth plate fusion 4 acromegaly. • Other rare causes of acromegaly include GHRH hypothalamic tumors and ectopic secretion of GHRH by neuroendocrine tumors.
Complications
Published January 28, 2018 on www.thecalgaryguide.com")
Asthma Acute Exacerbation: Pathogenesis and Treatment
: An episode of increased symptoms due to decreases in airflow
Abbreviations • PCO2: Partial pressure of CO, in arterial blood • PEF: Peak expiratory flow • SABA: Short-acting beta-2 agonists • Sp02 : Blood oxygen saturation level
Mild to moderate exacerbation: PEF 50% of predicted
Titrate O2 toSpO2, 92%, give SABA & steroids ■
Good response: symptoms resolved, PEF > 80%
[Treat at home with SABA as needed and steroids
Dyspnea
Bronchoconstriction
1` Residual volume and 1` PCO2
Respiratory failure
1` Air trapping causes '1' intra-alveolar pressure
Severe exacerbation: PEF 50% of predicted Educate patient regarding medications, Loss of Pulsus inhaler technique & [consciousness paradoxus follow up with primary care provider I
Legend: Pathophysiology Mechanism
Titrate O2 to402 93%, give SABA, steroids & magnesium sulfate
Sign/Symptom/Lab Finding
{Worsening symptoms and/or respiratory failure: Do not delay intubation, send to ICU, give SABA, steroids & magnesium sulfate
Authors: Luke Gagnon Reviewers: Midas (Kening) Kang Usama Malik Lian Szabo* * MD at time of publication
4, Delivery of oxygen rich air to alveoli 4, Oxygenation of blood
Drowsy and confused
Central cyanosis
• Tachycardia
Pneumothorax
[Depending on 1 severity: Observation or place chest tube")
Bronchiectasis Pathogenesis and clinical findings
, MAC complex infection, COPD, allergic bronchopulmonary aspergillosis, chronic infections
Irreversibly dilated bronchi
Chronic bronchial infection and inflammation
1
Easily collapsible airways
I Bronchiectasis (persistent and progressive damage to lungs)
Chronic cough (mucopurulent)
Defect in immunity and/or mucus clearance
Persistent bacteria in airway (commonly Pseudomonas/Staph aureus)
Inflammatory response
Rhinosinusitis
Abbreviations: • A1AT — Alpha-1-antitrypsin • COPD — Chronic Obstructive Pulmonary Disease • HIV — Human Immunodeficiency Virus • MAC — Membrane Attack Complex • VQ— Ventilation/Perfusion ratio
Legend:
Pathophysiology Mechanism
Fever
Sign/Symptom/Lab Finding
Failure to thrive (children)
Authors: Rebecca (Becky) Phillips Reviewers: Midas (Kening) Kang Usama Malik Eric Leung* * MD at time of publication
Notes: • Can be focal (single lobe/segment) or diffuse (both lungs) • Mainly in elderly • 1% prevalence in children
Tissue damage
Epithelial destruction of airways
Further impairment of bacterial clearance
Persistent inspiratory adventitious sounds (crackles > wheezing)
Complications
Structural damage to bronchial walls
Obstructive pulmonary function tests
Hemoptysis
Chest pain
VQ mismatch and 4, gas exchange
4, oxygenation
Digital clubbing (rare)
Fatigue Dyspnea
Cyanosis (uncommon)")
Chronic Thromboembolic Pulmonary Hypertension (CTEPH) Pathogenesis
: Pathogenesis
Acute Pulmonary Thromboembolic Event
Mechanical breakdown, Fibrinolysis
—5%: Incomplete thrombus resolution after 2 years (Etiology unknown)
*
Clot resolution (>90%)
Hypothesis 1: Increased hypercoagulability Hypothesis 2: Impaired clot lysis Hypothesis 3: Impaired angiogenesis Hypothesis 4: Inflammatory thrombosis • Associated with 1` levels of • Fibrin more resistant to • Impaired VEG-F function (unknown if cause or effect) plasma Factor VIII plasmin-mediated lysis • Ventriculoatrial shunts • Infected pacemaker wires • Splenectomy • Inflammatory bowel disease
Unresolved thromboemboli incorporates into blood vessel wall by fibrosis leading to fibrothrombotic organization
Authors: Dinusha T. Senaratne Reviewers: Midas (Kening) Kang Usama Malik Natalie Morgunov* Lian Szabo* * MD at time of publication
Legend:
Webs, bands and slow blood flow In-situ thrombosis expanding the fibrotic thrombus and branch occlusion Abbreviations: BP: Blood pressure PE: Pulmonary embolism PH: Pulmonary hypertension RAD: Right atrial dilatation RHF: Right heart failure RVHD: Right Ventricular hypertrophy/dilatation RVP: Right ventricular pressure VEGF: Vascular endothelial growth factor Proliferation of vascular and inflammatory cells proximal to lesion sites Adaptive vascular remodeling BP in patent vessels of the pulmonary vasculature For signs and symptoms refer to PH slide ■ Progressive PH
CTEPH (Chronic Thromboembolic pulmonary hypertension): Chronic occlusion of the pulmonary arteries due to intraluminal fibrosis of thromboembolic material from unresolved PE clots
Pathophysiology Mechanism
Progressive'(` RVP causes RAD and RVH/D
Sign/Symptom/Lab Finding
Progressive RHF
Complications
For signs and symptoms refer to RHF slide")
Lung cancer clinical findings and paraneoplastic syndromes

Obstruction of proximal airway
Inability to clear inhaled pathogens Postobstructive pneumonia
Cough, fever, dyspnea
Local tumor growth
Spread of tumor to pleural surface
Chest Pleural discomfort effusion
• Obstruction or compression at local site
Uncontrolled abnormal cell growth in one or both lungs 4 Lung Cancer
Airway invasion
Hemoptysis
Lambert-Eaton syndrome (Production of auto-antibodies against Calcium channels)
Muscle weakness
I` effort to Compression at the Compression Superior vena ventilate the laryngeal nerve of brachial cava lungs nerve plexus compression Impaired innervation to the vocal cords Dyspnea Shortness of Arm/shoulder/ Face/arm breath Voice hoarseness neck pain edema
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Authors: Yoyo Chan Reviewers: Midas (Kening) Kang Usama Malik Leila Barss* * MD at time of publication
Tumor secretes biologically active substances
Paraneoplastic Syndromes 4 Associated symptoms with malignant diseases
TGF131 extracellular matrix protein
Fingers clubbing
PTHrP T calcium release from bones
Hypercalcemia Serum calcium >2.6 mmol/L
ADH 1 SIADH T water reabsorption 1
Hyponatremia Serum sodium <135mEq/L
Abbreviations: • ACTH: Adrenocorticotropic hormone • ADH: Anti-diuretic hormone • PTHrP: Parathyroid hormone-related protein • SIADH: Syndrome of inappropriate antidiuretic hormone production • TGFI31: Transforming growth factor beta 1
1` ACTH
cortisol release and production
Cushing's syndrome (symptoms and signs caused by prolonged cortisol exposure)
Muscle weakness, hyperglycemia, severe hypokalemia")
Impetigo Pathogenesis and clinical findings

Pressure Ulcers Pathogenesis and clinical findings

Must remove slough/eschar to determine stage
-110.
Kennedy terminal ulcer (often precedes death)
—1111.
Pressure Ulcers: Pathogenesis and clinical findings
Bed, wheelchair, stretcher, car seat
External physical compression
Involuntary muscle movement, passive repositioning of torso Shear forces (dermis/epidermis fixed through contact with a surface while deeper tissues are moved; vessels angulate and thrombose, creating undermining of ulcer)
Inability to move well, aging skin (loss of elasticity, blood flow, and subcutaneous fat) Friction (person dragged across surface, damaging stratum corneum)
Bowel/bladder incontinence, diaphoresis, wound drainage Moisture (skin maceration)
4, in movement (coma, neuro injury, post-surgery, etc.) Limited mobility
Unrelieved pressure greater than arterial capillary pressure (>32 mmHg, with more rapid ulcer formation at higher pressures; normal range 12-32 mmHg) Disrupts blood supply and deprives tissues of oxygen and nutrients Pressure Ulcer (local injury to skin and/or underlying tissues, often over bony prominence)
Authors: Rebecca (Becky) Phillips Reviewers: Gurleen Chahal Usama Malik Laurie M. Parsons* * MD at time of publication
Notes: • More common in ages 65+ • Risk factors: diabetes, peripheral arterial disease, immunodeficiency, steroid therapy, smoking, dementia, poor nutrition, sensory deficit, circulatory disturbance, prolonged immobility • Grading system from National Pressure Ulcer Advisory Panel
Pear- or butterfly-shaped sacral ulcer
Stage I (non-blanchable erythema of intact skin; heralds impending ulcer)
May be warmer, painful, edematous, indurated, or discolored compared to surrounding tissue
Legend:
Stage II (partial thickness skin loss)
Erosion, serum-filled blister, or shallow ulcer with red-pink wound bed
Pathophysiology Mechanism
Stage III (full thickness skin loss; damage to subcutaneous tissue but not underlying fascia)
*
Exposed subcutaneous fat. May have slough, undermining, or tunneling (nose bridge, ear, occiput, and malleolar ulcers will appear shallow due to absence of subcutaneous tissue)
Sign/Symptom/Lab Finding
Stage IV (full thickness tissue loss)
Bone, tendon, or muscle exposed. Slough or eschar may be present. Often have undermining or tunneling
Complications
Bacterial invasion via contiguous spread (commonly S. Aureus and coagulase-negative staphylococci)
Osteomyelitis")
Benign Prostatic Hyperplasia: Pathogenesis and medications

Note: MoA not fully established
PDE-5 inhibitors (e.g. tadalafil)
Bladder and prostate smooth-muscle a-1 receptor antagonism
—110.
Relaxation of bladder outlet and prostate smooth-muscle
Authors: Michael Korostensky Reviewers: Alex Tang Usama Malik Dr. Jay Lee* * MD at time of publication
Acronyms: 5-ARI = 5-a reductase inhibitors COX = cyclooxygenase DHT = dihydrotestosterone GnRH = gonadotropin-releasing hormone LUTS = lower urinary tract symptoms PDE-5-mediated cGMP degradation in prostate smooth-Improved urinary outflow muscle and associated vascular supply Relaxation of prostate smooth-muscle MoA = mechanism of action NSAID = nonsteroidal anti-inflammatory drugs PDE-5 = phosphodiesterase-5 -NO
5-ARIs (e.g. dutasteride)
LHRH receptor antagonists (e.g. cetrorel ix)
P3-adrenergic agonists (e.g. mirabegron)
anticholinergics (e.g. oxybutynin)
NSAIDs
1` Bladder pressures
Pathophysiology Mechanism
5-a-reductase activity
1, Conversion of testosterone into DHT
4, Progression of LUTS
1, Testosterone secretion from testicular Leydig cells 1, LH secretion from pituitary GnRH antagonism DHT production Relaxation of detrusor Bladder muscle 1` capacity Improved LUTS
Acetylcholine antagonism at muscarinic receptors Relaxation of bladder outlet smooth-muscle 1` volume to first detrusor contraction 4, Prostaglandin release Analgesia and 4, Prostatic ,f, COX activity ► inflammation —110. Bladder smooth-muscle hyperplasia (detrusor thickening) /1` Sensitivity (i.e. overactive detrusor) -1110. 1, Volume to first detrusor contraction LUTS")
Erectile Dysfunction: Pathogenesis

1. Assess CVD Disease risk* a. I% Blood pressure b. I% Fasting glucose or HbA1c c. TG's & cholesterol 1. Penile duplex sonography 2. Cavernosometry
Legend:
Endocrinologic Erectile Dysfunction
Hypogonadism, hyperprolactinemia, hyperthyroidism, alcoholism, iatrogenic
.J, circulating free testosterone
•
1. 4, 7 AM free testosterone* 2. l• Thyroid Stimulating Hormone 3. l• Prolactin 4. l• Follicle Stimulating Hormone 5. l• Luteinizing Hormone
4, release of NO and cGMP levels within corpora cavernosa and smooth muscle relaxation
Pathophysiology Mechanism
Neurogenic Erectile Dysfunction
Neurologic disease, trauma, iatrogenic, diabetes mellitus
Central (cerebral or spinal cord); peripheral (afferent/sensory neuropathy) or efferent (autonomic neuropathy)
4, parasympathetic nerve firing
4, NO release
Psychogenic Erectile Dysfunction
•
Sudden onset, sporadic (circumstantial), younger, nocturnal/AM erection present
•
Anxiety, depression, strained relationship, lack of sexual arousal, psychological disorder
Possible mechanisms include an imbalance of central neurotransmitters, over inhibition of spinal erection center by the brain, and sympathetic overactivity
1. Abnormal Nocturnal penile 1. Normal Nocturnal penile tumescence and rigidity* tumescence and rigidity*
Erectile Dysfunction -• (persistent or recurrent inability to achieve an erection sufficient to achieve desired sexual performance)
Sign/Symptoni/Lab Finding
Complications
Authors: Braden Milian Reviewers: Alex Tang Usama Malik Jay C. Lee* * MD at time of publication")
Mixed Urinary Incontinence Pathogenesis and clinical findings
 4, Urinary leakage preceded by a sudden, strong urge to void
Overflow Incontinence vir Overfilling of the bladder from obstruction; BOO (tumour, stone, BPH, urethral or bladder neck stricture)
Detrusor Overactivity Ilr OAB (idiopathic), CNS lesion (neurogenic), inflammation/ infection (cystitis, UTI), diabetes mellitus
4. Bladder Wall Compliance
Progressive t in intravesicle pressure during bladder filling pushing urine from the bladder
Authors: Braden Millan Reviewers: Alex Tang Usama Malik Jay C. Lee* * MD at time of publication
Stress Urinary Incontinence (SUI) + Episodic involuntary urinary leakage with sudden l• in intra-abdominal pressure
4.
Urethral hypermobility, intrinsic sphincter deficiency, or a poorly coapting urethra
4,
4, Pelvic floor muscle and ligament strength causing 4. tone of vesicoureteral sphincter unit; 4, urethral strength and associated striated and smooth muscle; iatrogenic
Legend:
Failure to Void Weak Stream (+ dribbling), Intermittent, Straining, '1` PVR if a complication of urinary retention; obstruction visible on cystoscopy
Failure to Store Frequency, Urgency, Nocturia, Dysuria if SUI or UUI not caused by obstruction
Pathophysiology Mechanism
Urodynamic Studies SUI — 4, urethral closure pressure with 11` IAP/Bladder Volume and urinary leakage UUI — involuntary detrusor contraction and/or detrusor sphincter dyssynergia
Incontinence, 4, Quality of Life, UTI's")
Penyembuhan Luka Akut: Patogenesis dan Temuan Klinis

•
0 — 7 hari
Proliferasi (kolagen, matriks ekstrasel & pembuluh darah)
4 - 14 hari
Remodeling ► (.j, pemb. darah & kolagen tersusun)
Lapisan Epidermis Batas Dermis-Epidermis Lapisan Dermis
Vasokonstriksi transien
Pembentukan sumbat platelet
Jejas endotel dan subendotel
mengaktivasijalur koagulasi
Sel mast melepaskan histamin merespon iritan
Penulis: Amanda Eslinger Penyunting: Heena Singh Yan Yu Laurie Parsons* Penedemah: M Harmen Reza S* * MD (dokter) pada saat publikasi
Inflamasi I Proliferasi I Remodeling
Perdarahan berkurang atau berhenti karena sumbat hemostatik (hemostasis)
Permeabilitas pemb. kecil terhadap neutrofil & makrofag
Aktivasi komplemen memicu sel endotel sekitar untuk melepaskan prostaglandins
TGF-8*, dibentukselama fase inflamasi, menarikfibroblas ke daerah luka
Klot Menyatukan Ujung luka Perdarahan
Leukosit proliferasi dan
menyapu kotoran dan bakteri
1 Suplai vaskuler dan vasodilatasi di daerah luka
Makrofag melepaskan transforming growth factor beta (TGF-8) *
-110.
1' Tekanan hidrostatik mendorong cairan dari pembuluh jaringan sekitar
Fibroblas& makrofag menstimulasi pertumbuhanjaringan dan angiogenesis yang menggantikan sumbat hemostatik. Akhirnya, reepiteliasisasi terjadi
8 — 365+ hari
Patofisiologi Mekanisme
Kolagen tipe 1 yang mengalami tautan silang secara luas menggantikan kolagen yang berserakan yang tersusun pada fase proliferasi
Tanda/Gejala/Hasil Lab
Komplikasi
Luka Sembuh
kadar —* protein dalam kolagen
Eritema
Edema
Keropeng
Penyembuhan
Luka Parut (Scar)")
Penyembuhan Fraktur: Tahapan dan Faktor Pengganggu
 (osifikasi intramembran)
Penyembuhan tulang tahap inflamasi, kalus halus, and kalus keras
Penulis: Spencer Montgomery Penyunting: Yan Yu Dr. Gerhard Kiefer* Penerjemah: M Harmen Reza S* * MD (dokter) pada saat publikasi
Legenda:
Fraktur
Catatan: Penyembuhan fraktur melibatkan campuran antara jalur penyembuhan primer dan sekunder
Tahap Inflamasi (0-7Hari)
Stabilitas relatif pada lokasi fraktur: (pergerakan pada ujung tulang) - e.g. bidai, paku intramedular, traksi
Penyembuhan tulang sekunder (indirek) (osifikasi endokondral)
Kerusakan pembuluh darah lokal 4 hematoma 4 4, perfusi/02 ke tulang 4 osteonekrosis pada garis fraktur 4 terbentuk inflamasi lokal
Pergerakan pada lokasi fraktur
++ nyeri
Tahap Kalus Halus (mgg 1— 3)
Tahap Kalus Keras (mgg 3 — bin 3)
Remodeling (bin — thn)
Patofisiologi Mekanisme
• 1Kondrosit menyusun tulang rawan di lokasi hematoma, menjembatani kedua ujung tulang 4 nyeri berkurang
1
Osteoblas mengendapkan Ca3(PO4)2 ke matriks tulang rawan, membentuk kalus,1` stabilitas lokasi fraktur
Faktor yang dapat mengganggu penyembuhan fraktur
Tembakau Memperlama waktu penyembuhan, mekanisme belum jelas. Tiga hipotesis: 1) Nikotin: 4, aliran darah, dapat bersifat toksik pada osteoblas 2) Karbon Monoksida: 4, 02 ke lokasi fraktur 3) Hidrogen Sianida: menginhibisi metabolisme oksidatif pada tingkat sel
Penyalahgunaan alkohol Memperlama waktu penyembuhan, mekanisme tidak diketahui
Kortikosteroid & AINS jangka panjang Menghalangi respon inflamasi yang membatu penyembuhan
Remodeling tulang oleh pasangan Osteoklas-osteoblas : mengikir kalus agar tulang dapat mencapai bentuk efisien, sepanjang jalur gaya mekanisnya
Tanda/Gejala/Penunjang
Komplikasi
Kuinolon Menyebabkan pembentukan kalus imatur
Defisiensi Vitamin C Mengurangi pembentukan kolagen (Vit C adalah kofaktor kunci sintesis kolagen)
Diabetes Produksi kalus lemah (studi hewan)
Rifampicin & gentamycin topikal Toksik terhadap osteoblas
Hipotiroidisme Menginhibisi osifikasi endokondral (studi hewan)
Defisiensi Vitamin D Kurangnya absorpsi Ca2+ & Fosfat dari saluran cerna, 4, mineralisasi tulang.")
RICE: Mekanisme Aksi

Ice (diaplikasikan pada lokasi cedera)
Compression (pembalutan lokasi cedera)
Elevation (tungkai dinaikkan lebih tinggi dari jantung)
Mengurangi aliran darah ke jaringan
Mekanisme belum dipahami
Tekanan mekanis pada lokasi cedera
_110,
pengiriman PMN dan makrofag ke lokasi luka
Mencegah jejas lanjutan terhadap jaringan yang terkena beban mekanis produksi sitokin (bahan-bahan proinflamasi) seperti TNF-a, PDGF, (3- FGF, EGF, dan TG F-(3 Inflamasi Penulis: Matthew Roberts Penyunting: Alexander Arnold Amanda Eslinger Bradley Jacobs* Penerjemah: M Harmen Reza S* * MD (dokter) pada saat publikasi • ►
Cairan berlebih terdorong kembali ke kapiler dan limfe
Gravitasi pengembalian darah vena menuju sirkulasi sistemik
Abbreviations: • PMN- Netrofil Polimorfonuklear • TNF-a- Tissue Necrosis Factor-Alpha • PDGF- Platelet Derived Growth Factor • 13-FGF- Basic Fibroblast Growth Factor • EGF- Epidermal Growth Factor • TGF-13- Transforming Growth Factor Beta
Legenda: Patofisiologi Mekanisme
4, Edema (akumulasi cairan di ruang interstisial)
*Note: Penyembuhan cedera merupakan keseimbangan antara mengontrol nyeri dan inflamasi yang cukup untuk memulai aktivitas. Tujuan utama RICE adalah untuk menurunkan inflamasi. Aktivitas itu sendiri menimbulkan nyeri dan inflamasi, namun merupakan faktor penting dalam proses rehabilitasi.
Tanda/Gejala/Penunjang
► 4, Nyeri
1% Rentang gerak (Range of motion), dan juga fungsi
1
Inisiasi olahraga rehabilitatif spesifik dini untuk memperbaiki rentang gerak, kekuatan dan propriosepsi
Tekanan pada lokasi cedera akan menyebabkan robekan mikro pada jaringan lalu menginduksi inflamasi dan perbaikan* Otot, tendon, tulang, atau ligamen yang cedera menjadi lebih kuat
Penyembuhan dini")
Hemostasis Sekunder: Kaskade Koagulasi
:
F8a
Ca 2+
F5a
Protrombin (F2*)
Uji Laboratorium Rutin: • PT — Lama terbentuknya sumbatan setelah aktivasi jalur ekstrinsik • INR — PT yang dinormalisasi • PTT — Lama terbentuknya sumbatan setelah aktivasi jalur intrinsik
Jalur ekstrinsik: Jejas pada jaringan
Kerusakan sel endotel vaskuler akan memaparkan sub-endothelial Tissue Factor (Faktor jaringan)
F10* F10a*
Ca2+
Ca2+
• Faktor jaringan (Tromboplastin)
F7a*
Kompleks faktor jaringan — F7a*
► Trombin (F2a*)
Fibrinogen (F1)
Defisiensi jalur intrinsik
Ca2+
► Fibrin (Fla) Koagulasi Pembentukan sumbatan (clot) Fibrin
Defisiensi jalur Defisiensi jalur ekstrinsik bersama
Penulis: Christina Schweitzer Penyunting: David Lincoln Yan Yu* Lynn Savoie* Penerjemah: M Harmen Reza S* * MD (dokter) pada saat publikasi
Abbreviations: • PT — Prothrombin Time • INR - International Normalized Ratio • PTT — Partial Thromboplastin Time • F — Coagulation Factor (Faktor koagulasi) • a —Activated coagulation factor (Faktor koagulasi teraktivasi) • N— Normal • HMWK — High molecular weight kininogen • * — bergantung Vitamin K (untuk info lebih lanjut, lihat slide Vitamin K Deficiency)
Jembatan keledai (tidak diterjemahkan): • PT = Ekstrinsik: Play Tennis outside • PTT = Intrinsik: Play Table Tennis Inside • Faktor intrinsik — TENET: Twelve, Eleven, Nine, Eight, Ten • Faktor jalur bersama — 10/5=2, 2/2=1 (F10, 5, 2, 1) • Faktor bergantung Vitamin K— 1972: F10, 9,
7, 2
Jalur intrinsik, ekstrinsik & bersama normal
N PT, l• PTT 1` PT, N PTT t PT, t PTT N PT, N PTT
Perdarahan Memanjang")
Fisiologi sistem Renin-Angiotensin-Aldosteron (RAAS)

Hipoperfusi Ginjal
Regangan baroreseptor pada dinding arteriol aferen
Hipotensi/ Hipovolemia
9 Pengiriman NaCI ke Makula Densa
9 Tekanan dirasakan oleh Baroreseptor Jantung & Arteri
Katekolamin di sirkulasi
Aktivitas saraf simpatis pada arteriol aferen
Stimulasi reseptorn-adrenergik pada arteriol aferen
Keseimbangan Glomerulotubuler (Mekanisme intrinsik ginjal diluar RAAS) *Hanya sebagian dari mekanisme tersebut
Angiotensin II 4 konstriksi arteriol eferen
01% Tekanan hidrostatik glomerulus
Jumlah cairan yang disaring
+ Konsentrasi sisa protein darah di glomerulus
Darah kental bergerak dari glomerulus menuju kapiler peritubuler
it pada kapiler peritubuler
9 Tekanan hidrostatik peritubular
Legenda:
Patofisiologi Mekanisme
Pelepasan Renin oleh sel-sel Jukstaglomerular pada arteriol aferen 4 berujung pada T Angiotensin II
Sekresi aldosterone dari korteks adrenal
1
Insersi KNaE pada Sel Prinsipal di DK
■
Aktivitas transporter NHE3 di dalam PCT
Reabsorpsi Na ke dalam darah, menarik H2O ke dalam darah melalui osmosis
Reabsorpsi H2O langsung ke dalam sirkulasi darah (via aliran gradien tekanan onkotik dan hidrostatik H2O)
Tanda/Gejala/Penunjang
Komplikasi
Author: David Waldner Reviewers: Yan Yu Sean Spence Sophia Chou* Penerjemah: M Harmen Reza S* * MD (dokter) pada saat publikasi
Hati secara normal mensintesis angiotensinogen dengan laju basal, melepaskannya ke dalam sirkulasi darah:
Vasokonstri ksi arteri sistemik
Tekanan darah
Daftar singkatan: • ACE: Angiotensin Converting Enzyme (disintesis oleh Ginjal dan Paru) • DK: Duktus Kolektivus • PCT: Tubulus Konturtus Proksimal • NHE3: Sodium Hydrogen Exchanger (Antiport) 3 • KNaE: Kanal Natrium (Sodium) Epitel • n:Tekanan onkotik")
Gradien pO2 Alveolus-arteri: Mengapa ada, dan mengapa penting
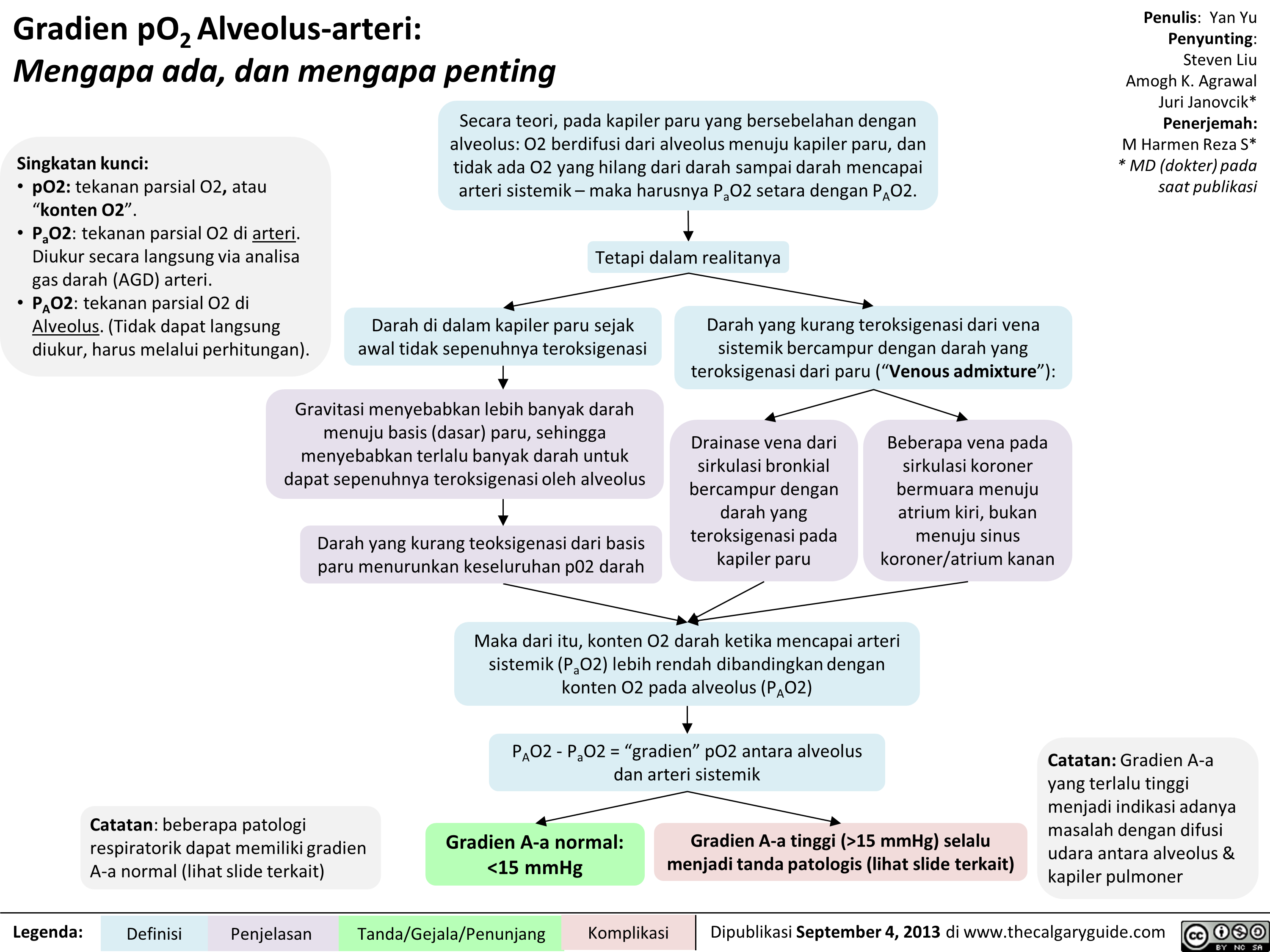 15 mmHg) selalu menjadi tanda patologis (lihat slide terkait)
Penulis: Yan Yu Penyunting: Steven Liu Amogh K. Agrawal Juri Janovcik* Penerjemah: M Harmen Reza S* * MD (dokter) pada saat publikasi
Catatan: Gradien A-a yang terlalu tinggi menjadi indikasi adanya masalah dengan difusi udara antara alveolus & kapiler pulmoner " title="Gradien pO2Alveolus-arteri: Mengapa ada, dan mengapa penting
Singkatan kunci: • p02: tekanan parsial 02, atau "konten 02". • Pa02: tekanan parsial 02 di arteri. Diukur secara langsung via analisa gas darah (AGD) arteri. • PA02: tekanan parsial 02 di Alveolus. (Tidak dapat langsung diukur, harus melalui perhitungan).
Secara teori, pada kapiler paru yang bersebelahan dengan alveolus: 02 berdifusi dari alveolus menuju kapiler paru, dan tidak ada 02 yang hilang dari darah sampai darah mencapai arteri sistemik— maka harusnya Pa02 setara dengan PA02.
1
Tetapi dalam realitanya
Darah di dalam kapiler paru sejak awal tidak sepenuhnya teroksigenasi
Gravitasi menyebabkan lebih banyak darah menuju basis (dasar) paru, sehingga menyebabkan terlalu banyak darah untuk dapat sepenuhnya teroksigenasi oleh alveolus
Darah yang kurang teoksigenasi dari basis paru menurunkan keseluruhan p02 darah
Catatan: beberapa patologi respiratorik dapat memiliki gradien A-a normal (lihat slide terkait)
Legenda: Definisi
Penjelasan
Darah yang kurang teroksigenasi dari vena sistemik bercampur dengan darah yang teroksigenasi dari paru ("Venous admixture"):
Drainase vena dari sirkulasi bronkial bercampur dengan darah yang teroksigenasi pada kapiler paru
Beberapa vena pada sirkulasi koroner bermuara menuju atrium kiri, bukan menuju sinus koroner/atrium kanan
.111••••■•
Maka dari itu, konten 02 darah ketika mencapai arteri sistemik (Pa02) lebih rendah dibandingkan dengan konten 02 pada alveolus (PA02)
PA02 - Pa02 = "gradien" p02 antara alveolus dan arteri sistemik
Gradien A-a normal: <15 mmHg
Tanda/Gejala/Penunjang
Gradien A-a tinggi (>15 mmHg) selalu menjadi tanda patologis (lihat slide terkait)
Penulis: Yan Yu Penyunting: Steven Liu Amogh K. Agrawal Juri Janovcik* Penerjemah: M Harmen Reza S* * MD (dokter) pada saat publikasi
Catatan: Gradien A-a yang terlalu tinggi menjadi indikasi adanya masalah dengan difusi udara antara alveolus & kapiler pulmoner " />
15 mmHg) selalu menjadi tanda patologis (lihat slide terkait)
Penulis: Yan Yu Penyunting: Steven Liu Amogh K. Agrawal Juri Janovcik* Penerjemah: M Harmen Reza S* * MD (dokter) pada saat publikasi
Catatan: Gradien A-a yang terlalu tinggi menjadi indikasi adanya masalah dengan difusi udara antara alveolus & kapiler pulmoner " title="Gradien pO2Alveolus-arteri: Mengapa ada, dan mengapa penting
Singkatan kunci: • p02: tekanan parsial 02, atau "konten 02". • Pa02: tekanan parsial 02 di arteri. Diukur secara langsung via analisa gas darah (AGD) arteri. • PA02: tekanan parsial 02 di Alveolus. (Tidak dapat langsung diukur, harus melalui perhitungan).
Secara teori, pada kapiler paru yang bersebelahan dengan alveolus: 02 berdifusi dari alveolus menuju kapiler paru, dan tidak ada 02 yang hilang dari darah sampai darah mencapai arteri sistemik— maka harusnya Pa02 setara dengan PA02.
1
Tetapi dalam realitanya
Darah di dalam kapiler paru sejak awal tidak sepenuhnya teroksigenasi
Gravitasi menyebabkan lebih banyak darah menuju basis (dasar) paru, sehingga menyebabkan terlalu banyak darah untuk dapat sepenuhnya teroksigenasi oleh alveolus
Darah yang kurang teoksigenasi dari basis paru menurunkan keseluruhan p02 darah
Catatan: beberapa patologi respiratorik dapat memiliki gradien A-a normal (lihat slide terkait)
Legenda: Definisi
Penjelasan
Darah yang kurang teroksigenasi dari vena sistemik bercampur dengan darah yang teroksigenasi dari paru ("Venous admixture"):
Drainase vena dari sirkulasi bronkial bercampur dengan darah yang teroksigenasi pada kapiler paru
Beberapa vena pada sirkulasi koroner bermuara menuju atrium kiri, bukan menuju sinus koroner/atrium kanan
.111••••■•
Maka dari itu, konten 02 darah ketika mencapai arteri sistemik (Pa02) lebih rendah dibandingkan dengan konten 02 pada alveolus (PA02)
PA02 - Pa02 = "gradien" p02 antara alveolus dan arteri sistemik
Gradien A-a normal: <15 mmHg
Tanda/Gejala/Penunjang
Gradien A-a tinggi (>15 mmHg) selalu menjadi tanda patologis (lihat slide terkait)
Penulis: Yan Yu Penyunting: Steven Liu Amogh K. Agrawal Juri Janovcik* Penerjemah: M Harmen Reza S* * MD (dokter) pada saat publikasi
Catatan: Gradien A-a yang terlalu tinggi menjadi indikasi adanya masalah dengan difusi udara antara alveolus & kapiler pulmoner " />
Gradien pO2 Alveolus-arteri: Penjelasan rumus (Penjelasan ringkas)

Untuk penjelasan fisiologis mengenai mengapa terdapat gradien A-a, silahkan lihat:")
Gradien pO2 Alveolus-arteri: Penjelasan rumus (Penjelasan secara ilmiah)

Untuk penjelasan fisiologis mengenai mengapa terdapat gradien A-a, silahkan lihat:")
Acetylcholinesterase Inhibitors
 effects
Salivation
Peristalsis
► Bradycardia
Bronchoconstriction
Bronchial Secretions
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications I Published March 3, 2018 on www.thecalgaryguide.com
0€3,0 BY NC SA")
Anticholinergics

Anticholinergics E.g. Atropine, Glycopyrrolate, Scopolamine
Abbreviations
ACh — Acetylcholine SA — Sino-atrial
Quick Facts
Primary indication in the OR = Combined with acetylcholinesterase inhibitors to prevent over-activation of the parasympathetic nervous system
Route of Administration = IV
Muscarinic (parasympathetic) effects
Competitive antagonism at muscarinic receptors in various organ systems
4, Binding sites for ACh at muscarinic receptors
Blockage of muscarinic ► receptors in SA node (esp. atropine)
► Smooth muscle relaxation in the bronchial airways
4, Respiratory tract mucosal ► secretions (esp. glycopyrrolate, scopola mine)
► Pupillary dilation
Tachycardia
Bronchorelaxation
Respiratory tract clearing
Mydriasis
► 4, Secretion of salivary glands —■ Dry mouth
► 4, Intestinal motility and peristalsis
► 4, Ureter and bladder tone
Constipation
Urinary retention
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications I Published March 3, 2018 on www.thecalgaryguide.com
0 0 4SI 0 I' it En")
non-depolarizing-neuromuscular-blocks-ndnmbs
 Eg. pancuronium, rocuronium, atracurium, vecuronium
Abbreviations NDNMBs — Non-Depolarizing Neuromuscular Blockers ACh — Acetylcholine
Quick Facts 1° Indication = Skeletal muscle paralysis to facilitate tracheal intubation, and used during indicated surgeries or mechanical ventilation
Route of Administration = IV
Metabolism & Excretion = Redistribution, hepatic clearance/renal excretion (extent varies greatly by drug). NOT degraded by acetylcholinesterase or pseudocholinesterase
See Acetylcholinesterase Inhibitors slide for reversal of NDN M Bs
Competitive antagonism at post-synaptic nicotinic receptors on muscles
Competitive antagonism at the pre-synaptic nicotinic receptors on neurons
Vagolytic effect (esp. pancuronium)
Anaphylactic/ anaphylactoid reactions
4, Binding sites for ACh at post-synaptic nicotinic receptors on muscles
4, Binding sites for ACh at pre-synaptic nicotinic receptors on neurons
Blockage of vagal muscarinic receptors in sinoatrial nodes
IgE antibodies attach to ammonium ion components of NDNMBs Non-immunologic mast cell degranulation (esp. atracurium)
4, Muscle cell depolarization
4, Positive feedback for continued ACh ► release in response to high frequency stimulation
Skeletal muscle paralysis
Tetanic fade, Train-of-Four fade
4, —• Parasympathetic Tachycardia effects on heart
Release of histamine from mast cells and basophils
Bronchospasm
Hypotension
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications I Published March 3, 2018 on www.thecalgaryguide.com
0€3,0 BY NC SA")
Propofol

4, Cerebral metabolic rate CNS —÷ 4, Cerebral oxygen consumption 4, Intra-cranial pressure
4, Systemic vascular resistance Hypotension ► Cardiovascular --■ —■ (with no change 4, Preload in heart rate) 4, Contractility
Respiratory /
♦ Hypercapnia 4, Hypoxic and --■ hypercapnic Hypoxia respiratory drive ♦ Apnea
4, Upper airway reflexes
Complications I Published MARCH 3, 2018 on www.thecalgaryguide.com
Lac.).T2")
Succinylcholine

Abbreviations ACh — Acetylcholine SA — Sino-atrial
Quick Facts 1° Indication = Skeletal muscle paralysis to allow tracheal intubation with the advantage of faster onset (30s-60s) and shorter duration (<10min) than non-depolarizing neuromuscular blocking agents
Route of Administration = IV
Metabolism & Excretion = redistribution and metabolism by pseudocholinesterase in blood plasma and liver
No reversal of succinylcholine available
Contraindicated in patients with traumatized, denervated, or immobilized muscles due to risk of cardiac arrest from hyperkalemia.
Agonist at nicotinic ACh receptors in muscles Generates action potential Not affected by synaptic acetylcholinesterase (unlike ACh)
Continuous end-plate depolarization
Inactivation of sodium channels
Prevention of repolarization and additional action potentials
Skeletal muscle paralysis
Succinylcholine mimics ACh in structure
♦ Fasciculation
♦ Myalgia
1` Serum lc (esp. in patients with muscle trauma/denervation/ immobilization)
1
Hyperkalemia
Malignant Hyperthermia (See Slide)
Agonist at nicotinic receptors in parasympathetic ganglia, sympathetic ganglia, and muscarinic receptors in SA node of heart
Parasympathetic effect (low dose succinylcholine) 4, Heart rate 4, Contractility
Cardiac arrest
1
Sympathetic effects (high dose succinylcholine)
t Heart rate t Contractility Catecholamine release
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications I Published March 3, 2018 on www.thecalgaryguide.com
0€3,0 BY NC SA")
Volatile Gases

Respiratory 4, Hypoxic and hypercapnic respiratory drive 4, Tidal volume 4, Alveolar ventilation Hypercapnia
1 t Respiratory rate
Musculoskeletal
Neuromuscular blockade and potentiation of NDNMBs
Muscle Relaxation
Malignant Hyperthermia (See Slide)
Complications I Published March 3, 2018 on www.thecalgaryguide.com
0 0 IS 0 riL - H")
non-depolarizing-neuromuscular-blocks-ndnmbs
 Eg. pancuronium, rocuronium, atracurium, vecuronium
Abbreviations NDNMBs — Non-Depolarizing Neuromuscular Blockers ACh — Acetylcholine
Quick Facts 1° Indication = Skeletal muscle paralysis to facilitate tracheal intubation, and used during indicated surgeries or mechanical ventilation
Route of Administration = IV
Metabolism & Excretion = Redistribution, hepatic clearance/renal excretion (extent varies greatly by drug). NOT degraded by acetylcholinesterase or pseudocholinesterase
See Acetylcholinesterase Inhibitors slide for reversal of NDN M Bs
Competitive antagonism at post-synaptic nicotinic receptors on muscles
Competitive antagonism at the pre-synaptic nicotinic receptors on neurons
Vagolytic effect (esp. pancuronium)
Anaphylactic/ anaphylactoid reactions
4, Binding sites for ACh at post-synaptic nicotinic receptors on muscles
4, Binding sites for ACh at pre-synaptic nicotinic receptors on neurons
Blockage of vagal muscarinic receptors in sinoatrial nodes
IgE antibodies attach to ammonium ion components of NDNMBs Non-immunologic mast cell degranulation (esp. atracurium)
4, Muscle cell depolarization
4, Positive feedback for continued ACh ► release in response to high frequency stimulation
Skeletal muscle paralysis
Tetanic fade, Train-of-Four fade
4, —• Parasympathetic Tachycardia effects on heart
Release of histamine from mast cells and basophils
Bronchospasm
Hypotension
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications I Published March 3, 2018 on www.thecalgaryguide.com
0€3,0 BY NC SA")
Succinylcholine
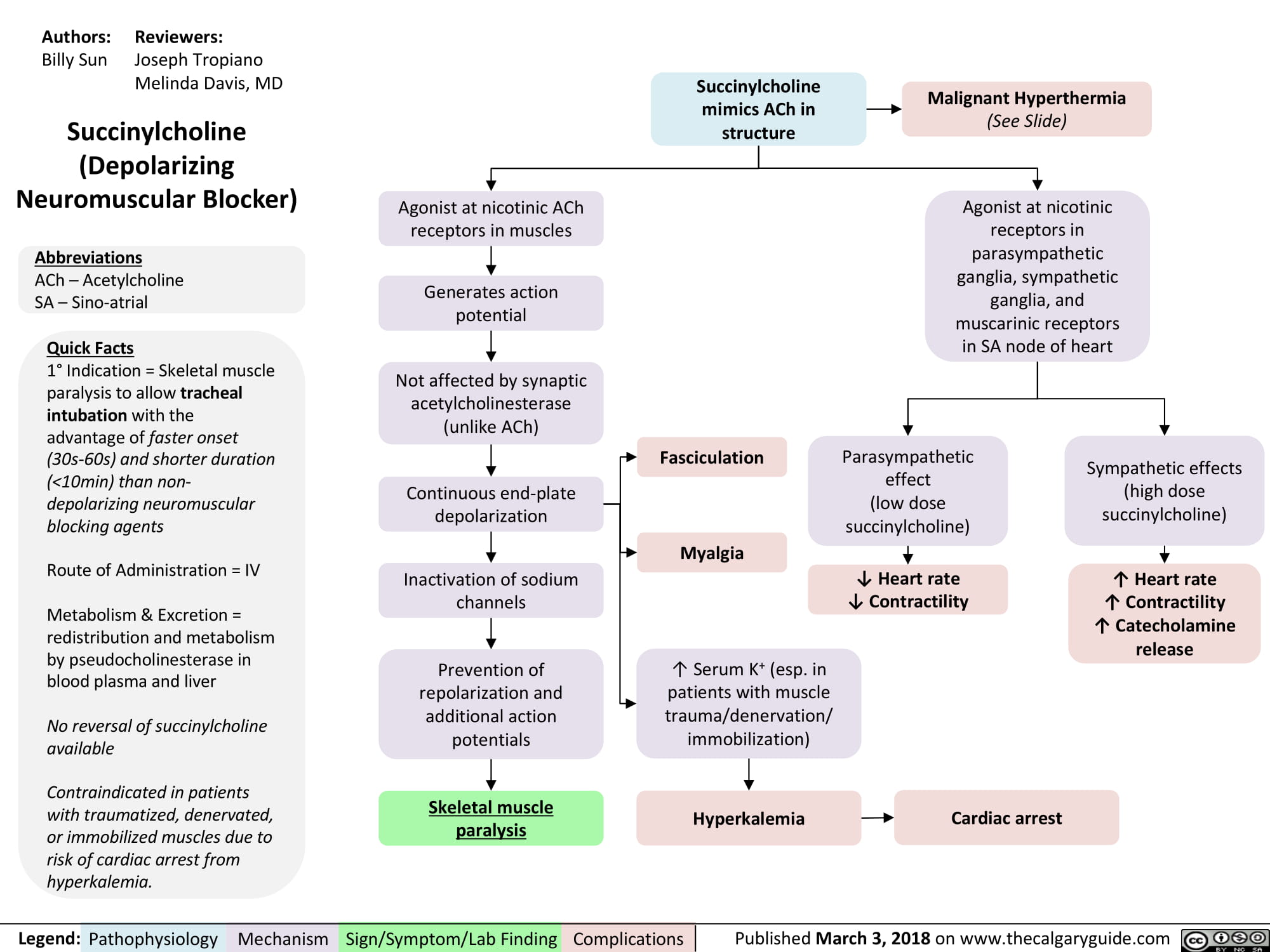
Clavicular Fracture: Pathogenesis and clinical findings
 (e.g. rowing) (87%) hand (6%) an object (7%) • • Acute fracture Stress fracture
Proximal third Group III (2.8%)
Undisplaced fracture
•
Shape of clavicle undergoes minimal change
Legend:
Middle third (mid-shaft) Group I (69%)
Clavicular Fracture
Displaced medial and lateral segments
Sternocleidomastoid muscle pulls the medial segment up
•••-•••11
Anterior Shoulder Pain
Pathophysiology Mechanism
Distal third Group II (29%)
Fracture is medial or lateral to the coracoclavicular ligaments
Pectoralis muscle and weight of arm pulls the lateral segment down and towards midline
Sign/Symptom/Lab Finding
Complications
Lateral Shoulder Pain
Authors: Jack Fu Reviewers: Reza Ojaghi Usama Malik Aaron J. Bois* * MD at time of publication
Notes: • There is no correlation between the mechanism of injury and the site of fracture (i.e., which")
Pediatric Pneumonia: Pathogenesis and clinical findings

Exposure to pathogen: inhalation, hematogenous, direct, aspiration
Susceptible host and/or virulent pathogen
Infection and proliferation of pathogen in lower respiratory tract/parenchyma
Pediatric pneumonia: Inflammatory response to proliferation of microbial pathogens at the alveolar level
Authors: Nicola Adderley Reviewers: Midas (Kening) Kang Usama Malik Eric Leung* * MD at time of publication
Notes: • Additional findings in pediatric pneumonia may include nausea, otitis, headache • Viral pathogens most common in children <2yrs; bacterial pathogens most common in children >2yrs • Interstitial pattern: suspect Mycoplasma pneumoniae, Influenza A + B, Parainfluenza • Lobar pattern: suspect S. pneumonia, H. influenzae, Moraxella, S. aureus
Local inflammatory response: neutrophils recruited to site of infection (LOBAR or INTERSTITIAL PATTERN, depending on pathogen) by epithelial cytokine release
At-- Irritation of contiguous structures and/or referred pain (mechanism unclear)
Acute abdominal pain
Accumulation of plasma exudate (from capillary leakage at sites of inflammation), cell-debris, serous fluid, bacteria, fibrin
Irritation of airways and failure of ciliary clearance to keep up with fluid buildup Cough
Legend:
Crack es, 4• breath sounds
Pathophysiology Mechanism
Fluid buildup in spaces between alveoli (INTERSTITIAL PATTERN)
Interstitial opacity on CXR
Fluid buildup in alveoli (LOBAR PATTERN)
J, efficiency of gas exchange (I` diffusion distance in INTERSTITIAL, J, surface area in LOBAR)
Lobar consolidation on CXR
Sign/Symptom/Lab Finding
Complications
Hypoxemia
Systemic inflammatory response:
Cytokine release (eg. TNF, IL-1)
1` respiratory drive
•
Tachypnea
Disruption of hypothalamic thermoregulation
Fever/chills
Respiratory accessory muscle use (chest indrawing, paradoxical breathing, muscle retractions)")
Radiological findings of child abuse
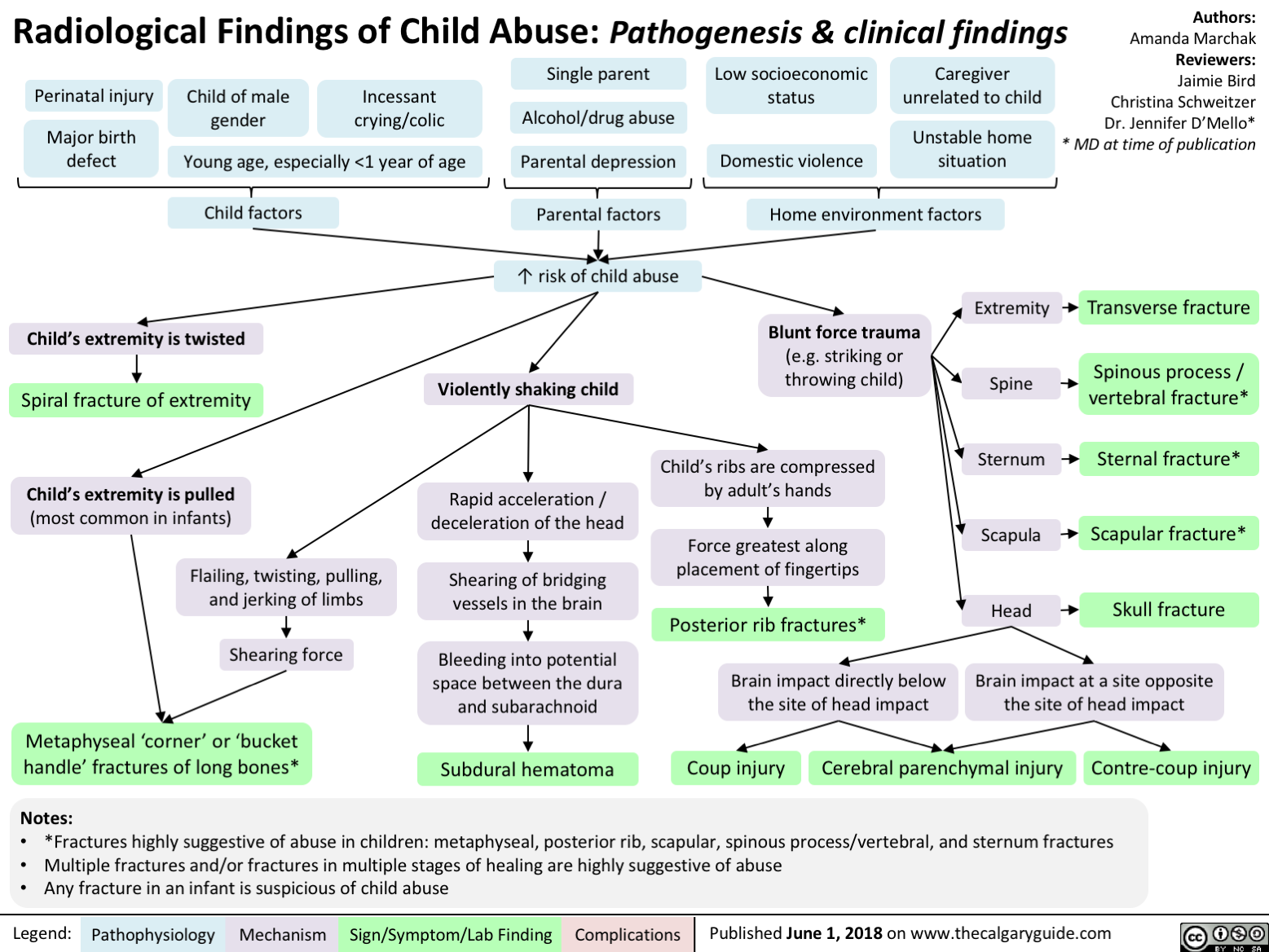
Non-Accidental Head Trauma
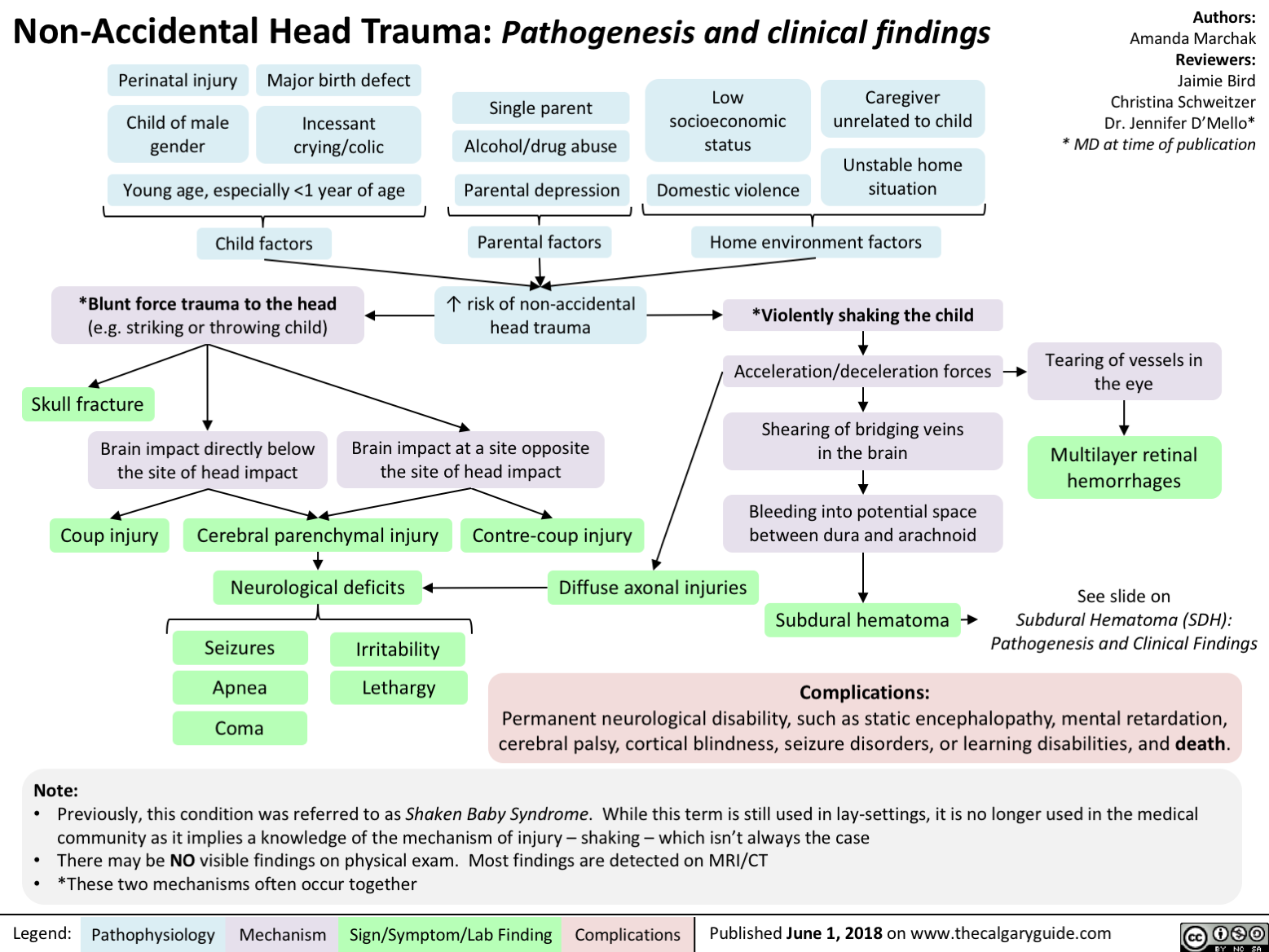
Duchenne Muscular Dystrophy
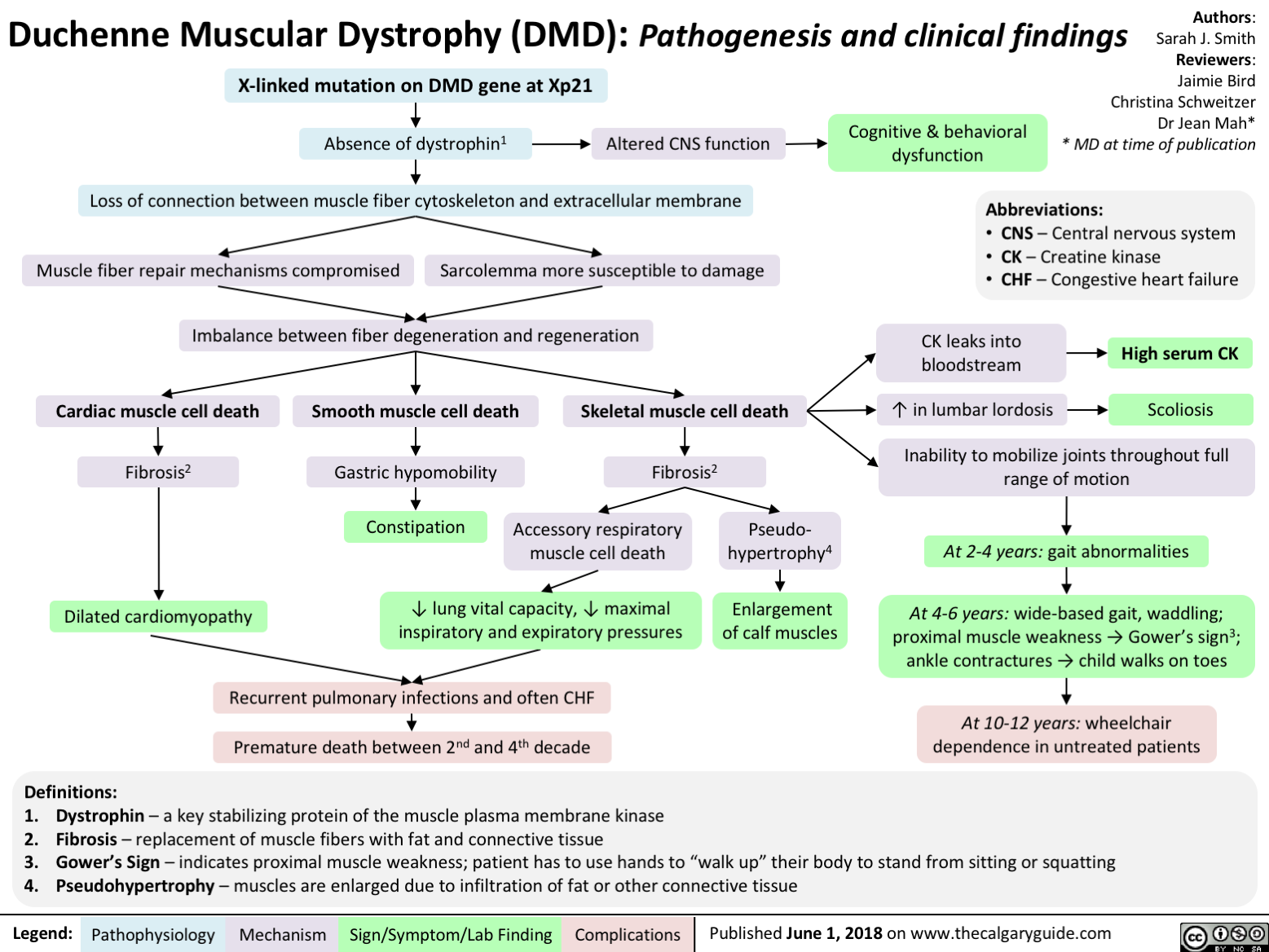
Acquired Inguinal Hernias: Indirect + Direct
, inferior epigastric vessels (suprlateral) and the inguinal ligament (inferior boarder)
Herniated contents become entrapped Groin erythema Pain on palpation Strangulation Vomiting • l• pain (SURGICAL ► Incarceration EMERGENCY) (SURGICAL Yir Fever EMERGENCY) Necrosis Compromise of vascular supply • Pain, Sepsis, fistula, abscess Bowel perforation formation")
Celiac Disease: Pathogenesis and clinical findings

Genetic predisposition -■ (Northern European, Down's syndrome, Associated with HLA DQ 2,8)
Note: *The anti-TTG antibody is an IgA anti-body, therefore if the patient is IgA-deficient, absence of anti-TTG does not rule out celiac
Anti-TTG in serum*
Anti-TTG reacts with TTG in skin
Deposition of anti-TTG in renal glomeruli
Dermatitis herpetiformis
Chronic Kidney Disease
Small Bowel Biopsy: Crypts of bowel become enlarged (hyperplasia) with architectural change, villous shortening
Legend: Pathophysiology
Mechanism
Exposure to prolamins (proteins found in wheat, rye, oats, barley)
TTG alters prolamin Altered protein fits more easily into HLA
HLA activates adaptive immunity
IgA generated against prolamin-TTG
Wheat prolamin (gliandin) interacts with and activates zonulin signalling
Gut epithelium becomes more porous
Large dietary proteins in epithelium disrupt tight junctions
Author: Matthew Harding Yan Yu Peter Bishay Reviewers: Dean Percy Jason Baserman Usama Malik Kerri Novak* * MD at time of publication
Inflammation of Intestinal epithelium Inflammation disrupts structure of bowel mucosa Mechanism Unknown Lymphocytes migrate to site of inflammation Extraintestinal Complications: Arthropathy Ataxia (gluten associated) Infertility Mild Hepatitis Villi of intestine atrophy Risk of Microscopic Colitis (50x) Malabsorption Extraintestinal manifestations: Chronic watery Fatigue Failure to thrive, weight loss Anemia (Fe, B12, folate) Peripheral neuropathy (B12, Ca) Ataxia (Ca) Dysrhythmia (Ca, K) Osteoporosis (Vit D, Ca) diarrhea + Intestinal manifestations steatorrhea: Pale, foul-smelling Abdominal bloating Steatorrhea (fat in stool) Diarrhea")
Celiac Disease: Complications
 Carbohydrate Protein Fat Secretory maldigestion maldigestion malabsorption diarrhea
Legend:
Fermentation by gut bacteria 1 Gas production
Bloating
Fat retained in stool
Steatorrhea
Abdominal pain
Pathophysiology Mechanism
Sign/Symptom/Lab Finding
Growth Retardation
Authors: Yoyo Chan Reviewers: Peter Bishay Usama Malik Sylvain Coderre* * MD at time of publication
IgA response
Autoimmune IgA deposits Lymphocyte response in sub-epidermal skin layer against enamel
Dermatitis Herpetiformis (Chronic pruritic blisters)
Nutritional deficiency
Dental enamel hypoplasia
Vitamin D and calcium deficiency
Zinc, selenium Folate Iron Osteoporosis deficiency deficiency deficiency Anemia t Risk of miscarriages")
Orofacial Clefts cleft lip cleft palate
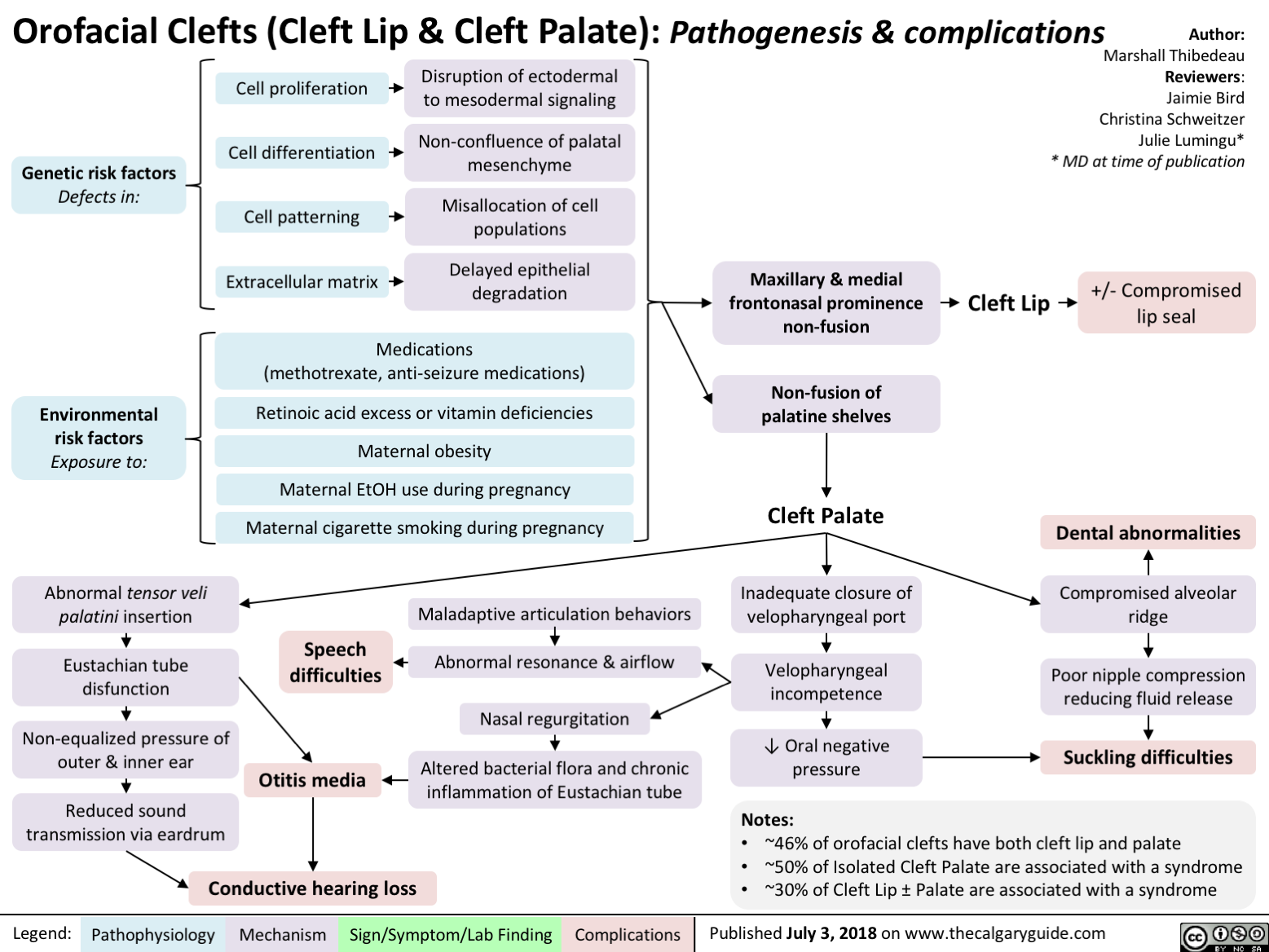
Cerebral Palsy clinical findings
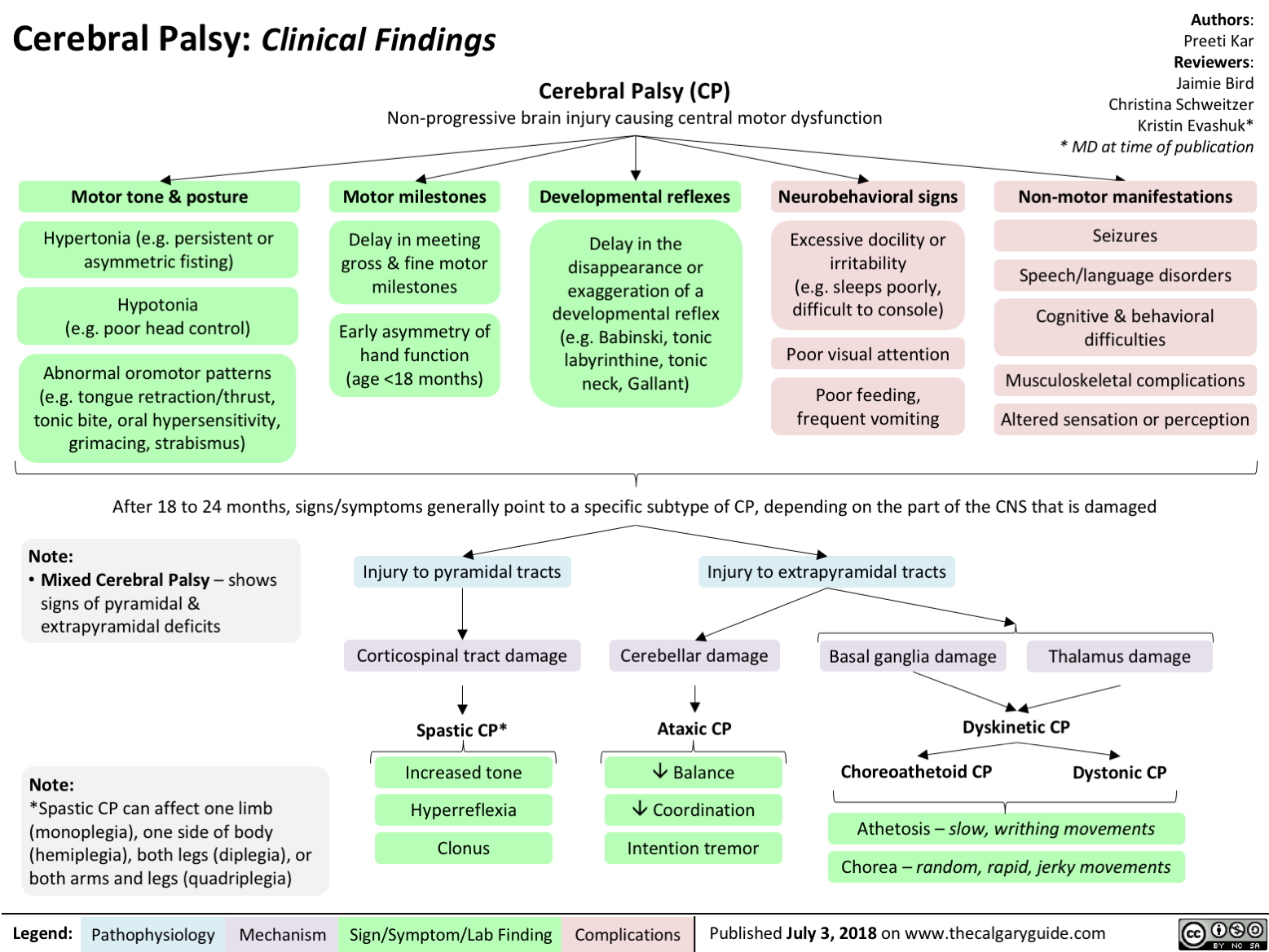
Developmental Coordination Disorder
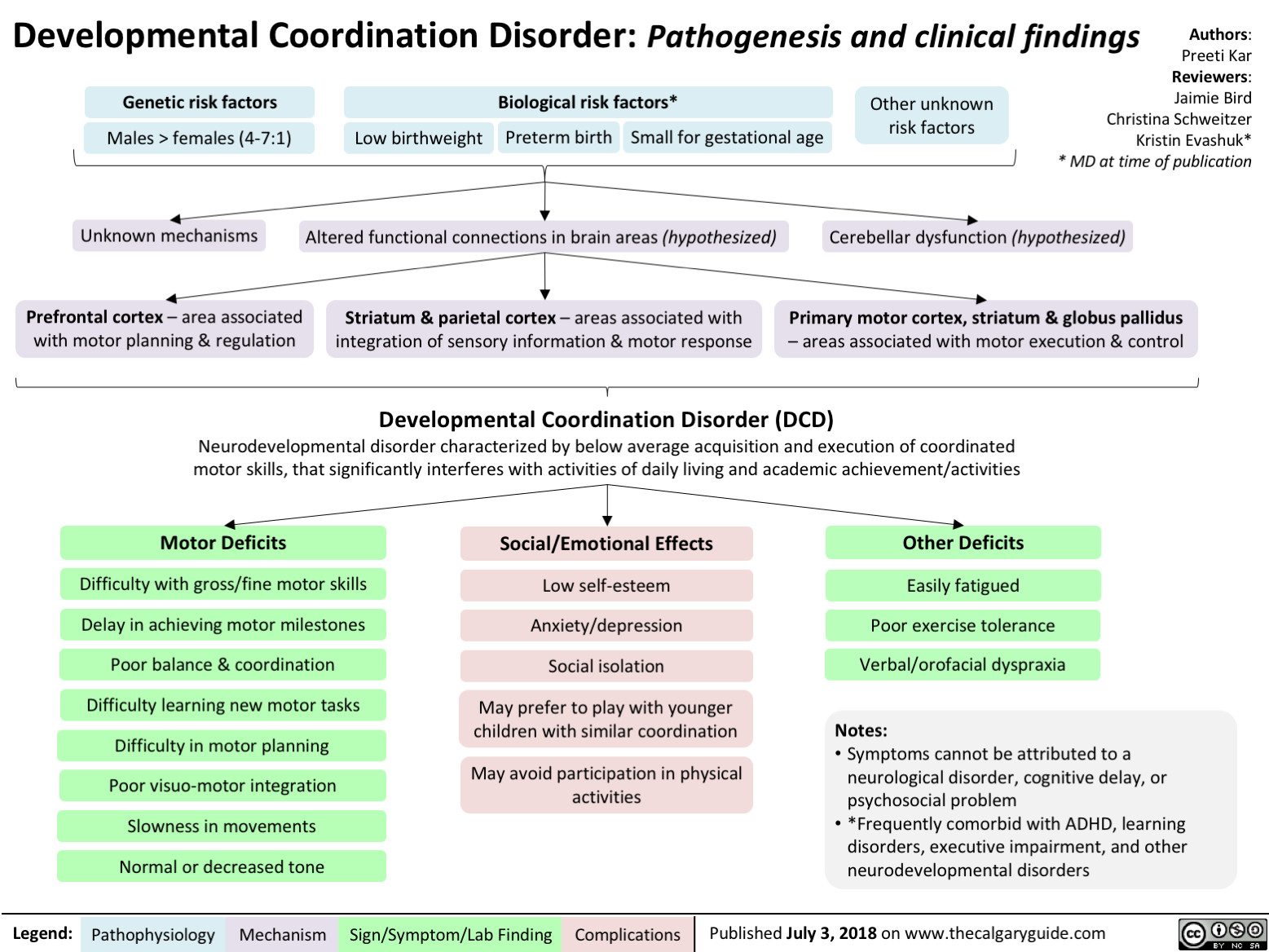
Sudden Infant Death Syndrome SIDS Triple Risk Model

Aplastic Anemia: Pathogenesis and Clinical Findings
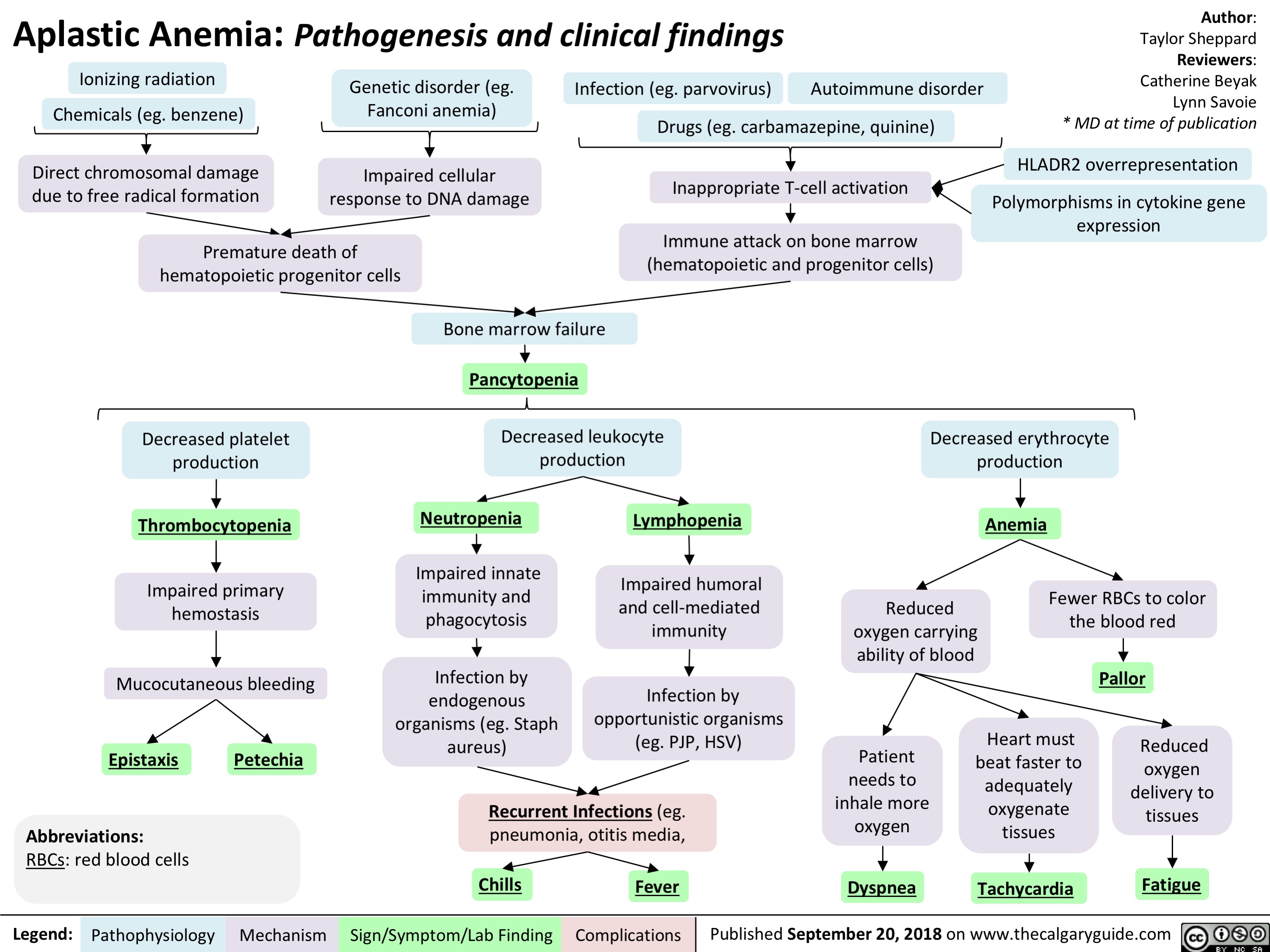
Feedback Loops Growth Hormone
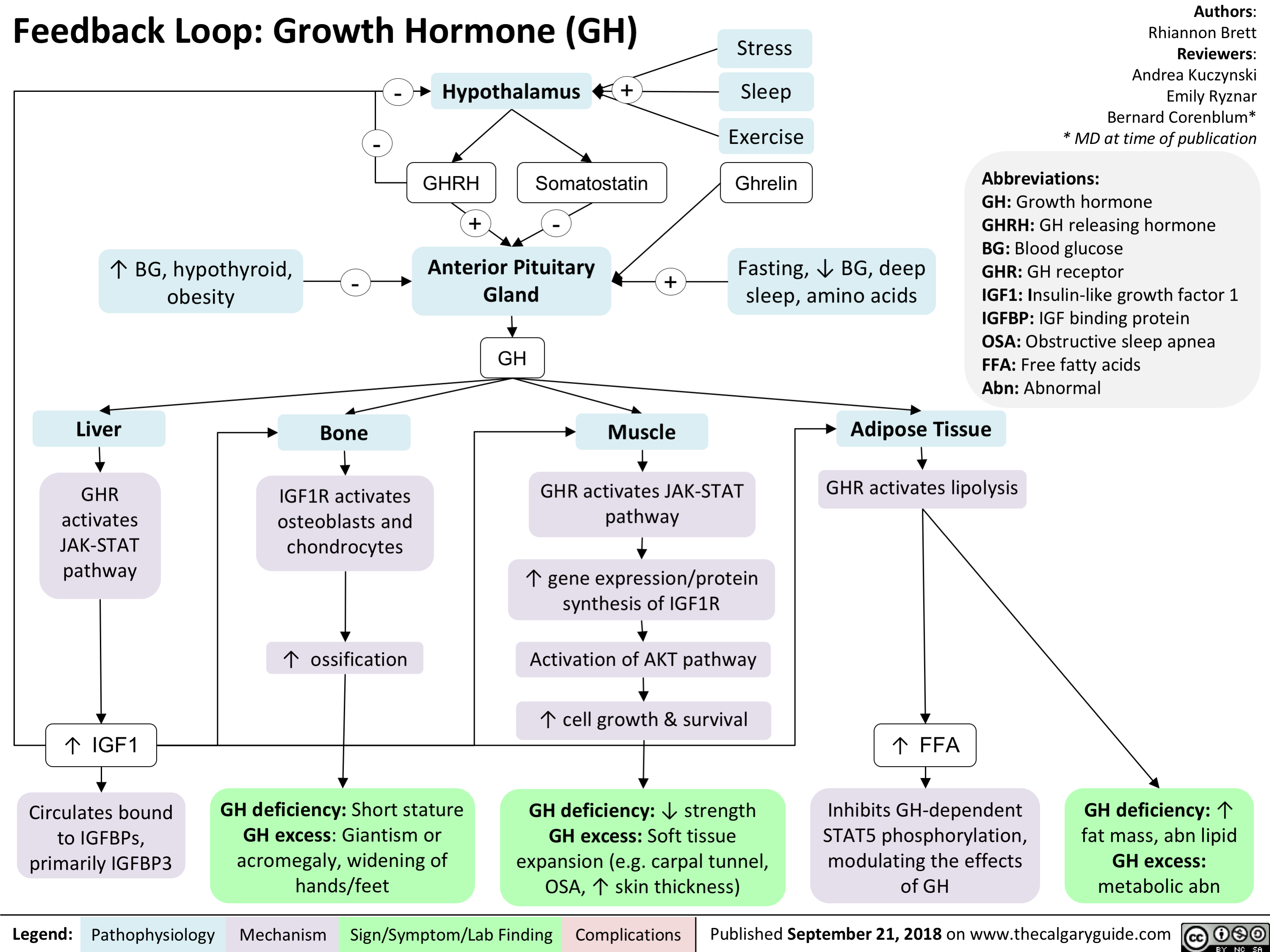
Kallmann Syndrome and Normosmotic Idiopathic Hypogonadotropism: Pathogenesis and Clinical Findings
 and Normosmic Idiopathic Hypogonadotropic Hypogonadism (nIHH): Pathogenesis and clinical findings
Authors: Danielle Lynch Reviewers: Nicola Adderley Josephine Ho* * MD at time of publication
Abbreviations:
GnRH – gonadotropin- releasing hormone
LH – luteinizing hormone FSH - follicle stimulating hormone
Notes:
• 4 male : 1 female
• KS, nIHH, and isolated
anosmia exist on a
spectrum
• KS has X-linked recessive,
autosomal dominant, autosomal recessive,
oligogenic, and idiopathic
forms
• KS and nIHH are also
associated with gene- specific features such as
cleft lip/palate, oculomotor synkinesis, hearing loss, and unilateral renal aplasia
• Diagnosis typically occurs around pubertal age, but may be earlier in males if micropenis and cryptorchidism are present at birth
Mutations in KAL1, NELF, and PROKR2
Abnormal olfactory bulb development
Mutations in FGFR1, FGF8, PROK2, PROKR2, HS6ST1, CHD7, WRD11, and SEMA3A or idiopathic
Mutations in
GNRH1, KISS1, KISS1R, TAC3, TACR3
Impaired migration of olfactory neurons from olfactory bulb to hypothalamus
Impaired migration of GnRH neurons from olfactory bulb to hypothalamus
Impaired GnRH neuron activity
Kallmann syndrome
(idiopathic hypogonadotropic hypogonadism with anosmia)
Normosmic idiopathic hypogonadotropic hypogonadism
Anosmia
Olfactory bulb aplasia
Abnormal /absent olfactory bulb on MRI
↓ GnRH ↓LH and ↓FSH
Delayed or absent puberty
Infertility
↓estrogen
In males: ↓testosterone
Cryptorchidism
Delayed epiphyseal plate closure
Micropenis (5-10%)
Uninhibited long bone growth
↑ length hands, arms, legs
Delayed bone age (hand/wrist x-ray)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 29, 2018 on www.thecalgaryguide.com")
Posterior Cruciate Ligament (PCL) Injury Pathogenesis and Clinical Findings
 Injury: Pathogenesis and Clinical Findings
Sport-related
Hyperextension Injury
Motor Vehicle Collision (MVC)
Fall on flexed knee Dashboard injury
PCL Injury
+ve Posterior draw test +ve Lachman or +/- Varus & Valgus Stress Test +/- McMurray
1
Multiligamentous injury
Notes: • The PCL is an important stabilizer in the knee and is the primary resistor of posterior translation of the tibia on the femur. • Isolated PCL injuries are uncommon and are often asymptomatic and acutely undiagnosed.
Legend: Pathophysiology Mechanism
Isolated PCL injury
+ve Posterior draw test -ye Lachman -ye Varus & Valgus Stress Test -ye McMurray
Chronic PCL deficiency and Knee Instability
1
1` Dynamic Stabilization with quadriceps tendon
1
Post-traumatic patellofemoral pain or arthritis
Sign/Symptom/Lab Finding
Authors: Luc Wittig Reviewers: Reza Ojaghi Usama Malik Dr. R. Buckley* * MD at time of publication
Classification of PCL Injuries Partial: Translation < 10 mm on posterior drawer test with the knee in neutral rotation. Some sort of end point is present. Complete isolated PCL: Posterior drawer test is positive with the knee in neutral rotation and is diminished with the knee in internal rotation. Combined PCL: The PCL is injured in conjunction with other structures, such as the ACL, posterolateral corner, and medial side.")
Feedback Loop: Adrenocorticotropic Hormone (ACTH)

Authors: Rhiannon Brett Reviewers: Andrea Kuczynski Bernard Corenblum* * MD at time of publication
Posterior Pituitary Gland
ADH
-
-
-
Hypothalamus
CRH
+
Anterior Pituitary Gland
ACTH, MSH, other hormones produced from POMC
ACTH
+
Adrenal Cortex
Activate ACTHR
Activate cAMP Activate PKA Activate Zona Fasciculata
Cortisol
Abbreviations:
CRH: Corticotropin Releasing Hormone
ADH: Anti-diuretic Hormone
ACTH: Adrenocorticotropic Hormone
MSH: Melanocyte Stimulating Hormone
POMC: Pro-Opiomelanocortin
ACTHR: ACTH Receptor
cAMP: Cyclic Adenosine Monophosphate
PKA: Protein Kinase A
DHEA(S): Dehydroepiandrosterone (sulfonated form) F: Female
M: Male
Excess: hirsutism, acne, oily skin, oligo- or amenorrhea, virilization in F
Deficiency: symptoms not typically seen due to gonadal production
Note:
Activate Zona Reticularis Activate Zona Glomerulosa
(minor effect)
Excess: central obesity, hirsutism, violaceous striae, weakness
Deficiency: weight loss, fatigue, weakness, nausea/vomiting, diarrhea
DHEA(S) Aldosterone
Specific to primary adrenal insufficiency: ↑ pigmentation, hyperkalemia
• Virilization is a red flag for an androgen- secreting tumor
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 2, 2018 on www.thecalgaryguide.com")
Feedback Loop- Thyroid Stimulating Hormone (TSH)

Authors: Josh Kariath Reviewers: Andrea Kuczynski Bernard Corenblum* * MD at time of publication
Stress
Excess: heat intolerance, tremor, proximal muscle weakness, palpitations, systolic HTN, brisk reflexes, weight loss, ↑ appetite, ↑ bowel movements
Deficiency: cold intolerance, firm gland of any size, fatigue, depression, weight gain, constipation, delayed relaxation of DTRs, diastolic HTN
Cortisol
-
+ +
Cold
Hypothalamus
TRH
TRH travels down
hypophyseal stalk through portal vessels
Anterior Pituitary Gland -
TSH
TSH travels through the blood
Thyroid Gland (Follicle) +
T3 T4
Converted into T3 in all target tissues
↑ BMR
-
Abbreviations:
TRH: Thyrotropin Releasing Hormone HTN: Hypertension
DTRs: Deep Tendon Reflexes
TSH: Thyroid Stimulating Hormone I2: iodine
CO: Cardiac Output
T3: Triiodothyronine
T4: Thyroxine
CNS: Central Nervous System
SNS: Sympathetic Nervous System BMR: Basal Metabolic Rate
-
Diet
I2
Excess: no real disorders
Deficiency: goiter
↑ CO, ↑ contractility, ↓ resistance
Hormone metabolism, bilirubin metabolism
Heart Liver
Bone growth Bone
↑ SNS activation, temperature homeostasis
CNS
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 2, 2018 on www.thecalgaryguide.com")
Anaphylaxis: Signs and Symptoms

Giant Cell Arteritis: Pathogenesis and Clinical Findings
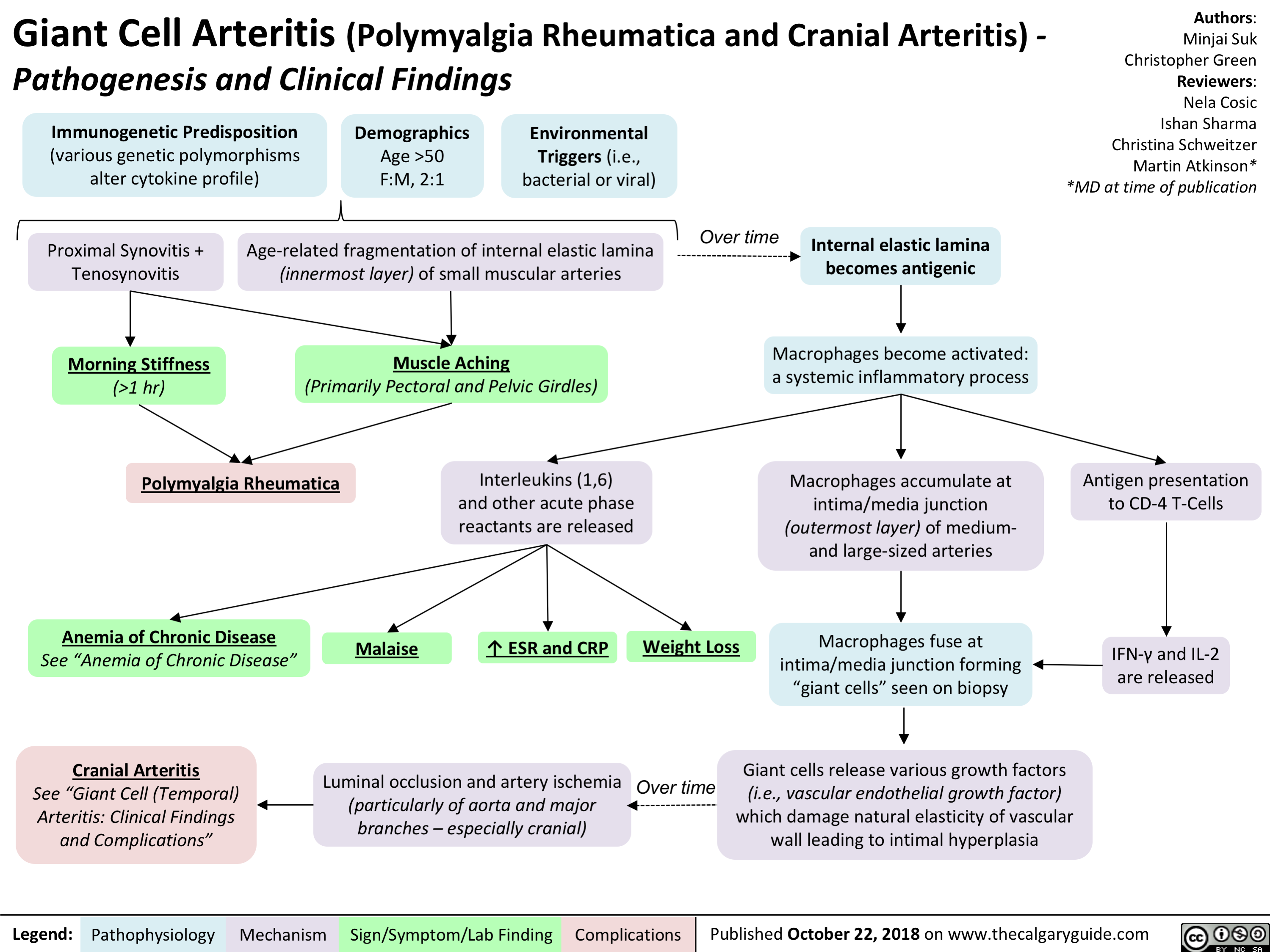
Acute Hemolytic Transfusion Reaction: Signs and Symptoms
Anaphylaxis: Treatments
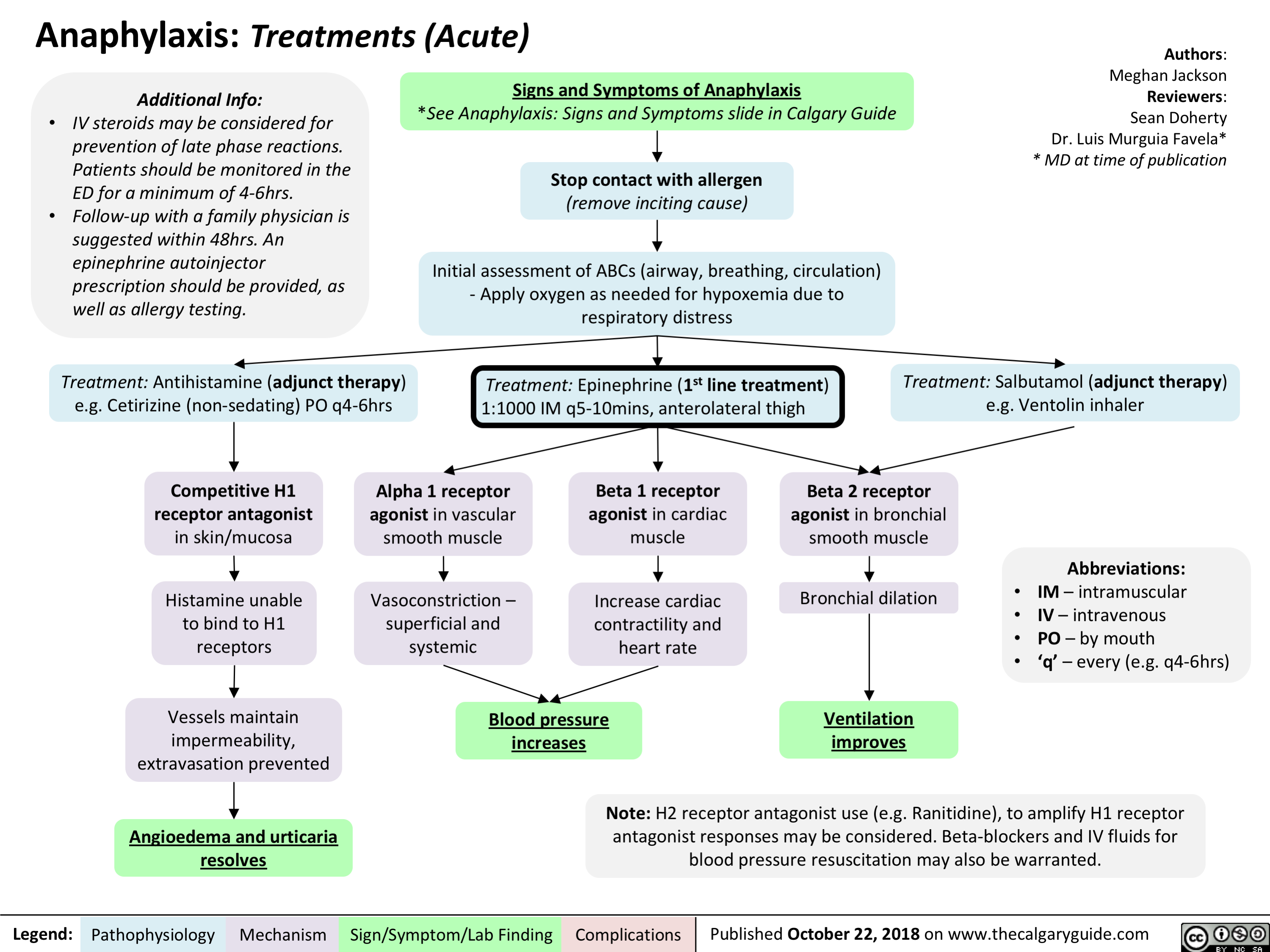
Glucocorticoid Induced Osteoporosis: Pathogenesis and Clinical Findings

intrauterine-growth-restriction-iugr-pathogenesis
: Pathogenesis
Authors: Ricki Hagen Reviewers: Jaimie Bird Sarah McQuillan* * MD at time of publication
Abbreviations:
• DM: diabetes mellitus
• HTN: hypertension • IUGR: intrauterine growth restriction
• SGA: small for gestational age
• SLE: systemic lupus erythematosus
• TORCH: Toxoplasmosis, Others, Rubella, CMV, HSV
Maternal Factors
Maternal-Fetal Factors Placental malformations
(Ex. previa, accreta, infarction, abnormal implantation, ischemia)
Gestational HTN/ Preeclampsia
Multiple gestation Gestational DM
Fetal Factors Structural anomalies
(often comorbid with cytogenetic disorders)
Congenital infections
(Ex. TORCH)
Inborn errors of metabolism
Chromosomal disorders/ genetic syndromes
Multiple unclear intrinsic fetal mechanisms
Note:
Teratogenic medications (Ex. Warafin, Valproic Acid, Folic Acid Antagonists)
High altitude living
Smoking, ETOH and/or drug use
Malnutrition/ Low pre-gestational weight
Multiple unclear extrinsic fetal mechanisms
Medical conditions
(Ex: chronic HTN, cyanotic heart disease, severe chronic anemia, kidney disease)
Autoimmune conditions (Ex. Type 1 DM, SLE)
Decreased uteroplacental blood flow
Nutrient supply to fetus compromised
Reduction of total body mass, bone
mineral content, and muscle mass
Blood flow redirected away from vital organs to brain, placenta, heart and adrenal glands
Reduction of overall fetal size to increase survival
IUGR
Failure to reach genetically determined growth potential
• IUGR is not synonymous with SGA • Constitutional SGA is due to
paternal and maternal factors such as height, weight, ethnicity, and parity; it is not associated with increased risk for infant mortality or morbidity
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October, 30, 2018 on www.thecalgaryguide.com")
fetal-alcohol-spectrum-disorder-pathogenesis-and-clinical-findings

Maternal alcohol consumption during pregnancy (greatest risk with binge drinking and daily/chronic intake)
Prenatal alcohol exposure to fetus via placenta-umbilical transport
Notes:
Fetal Alcohol Spectrum Disorder with Sentinel Facial Features (confirmed or unknown PAE)
Fetal Alcohol Spectrum Disorder without Sentinel Facial Features
• There is no known safe amount of prenatal alcohol exposure
(PAE). Although PAE below the threshold of >7 drinks/week or > 2 binge episodes (one binge episode is >4 drinks in one sitting) has not been associated with neurodevelopmental effects, there is insufficient objective evidence to deem this level of alcohol exposure safe.
Sentinel Facial Features
(confirmed PAE) Alcohol exposure between Alcohol acts directly as a teratogen
Vasoconstriction of placental-umbilical unit ̄ blood flow and ̄ oxygen delivery to fetus
Notes (continued):
• A multidisciplinary team is necessary for an accurate and comprehensive diagnosis and subsequent recommendations. Canadian Guidelines for diagnosis, 4-digit code, the APP Toolkit, University of Washington Lip- Philtrum Guide are different methods of assessing and diagnosing patients.
• While not specific to FASD, congenital abnormalities (e.g. heart defects, renal problems, auditory/visual impairments, skeletal defects) and growth deficits (prenatal and/or postnatal height or weight ≤ 10th percentile) are often associated with this disorder.
Smooth philtrum
Thin upper lip
day 15 and 22 of & indirectly via its metabolites pregnancy (most often)
Neuronal cell death & disruption of migration & proliferation Altered signaling, neurotransmitter imbalance, & neural connectivity Evidence of impairment in 3+ neurodevelopmental domains
Small palpebral fissures
(≥2 SDs below the mean for age & sex or < 3rd percentile)
Language Memory Attention Motor skills Cognition Affect regulation
Academic achievement
Executive function (including hyperactivity & impulsivity)
Neuroanatomy/ Neurophysiology (e.g. seizure disorder, abnormal brain structure as seen on brain imaging, microcephaly (head circumference ≤ 10th percentile))
Adaptive behavior, social skills, or social communication
Failure to reach age-appropriate milestones, challenges at school, aggression, delinquency, mental health challenges, substance use disorders
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 30, 2018 on www.thecalgaryguide.com")
Hydrocephalus: Clinical Findings

↓ or insufficient CSF absorption
(Communicating Hydrocephalus) Hydrocephalus
Enlargement of CSF pathways
Neuroimaging: ventriculomegaly
CSF accumulation
↑ ICP
Compression of blood vessels and altered cellular metabolism
Delayed neuronal migration (neonates)
Periventricular white matter tract damage
(variable) Seizures, developmental anomalies (e.g. learning disability, impaired speech)
Compression of brainstem cranial nerve nuclei and/or tracts
Distortion of meninges and blood vessels
Headache (worse in the morning), nausea/vomiting
Midbrain/brainstem dysfunction (as hydrocephalus worsens)
Lethargy/↓ LOC, neck stiffness
Irritable, feeding difficulty
Upward gaze palsy (Setting Sun sign)
Papilledema, CN 6 palsy
Infant
Older Child
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 30, 2018 on www.thecalgaryguide.com")
Orbital Cellulitis: Pathogenesis and clinical findings
 Periorbital cellulitis1,2
Hematogenous spread
Contiguous spread of infection
Pathogens reach orbital tissue (posterior to the orbital septum)
Spreads to periorbital tissue (anterior to the orbital septum)
Localized inflammation
Conjunctival chemosisa
Eyelid and periorbital edema
Pain on palpation
Induration
Warmth
Orbital Cellulitis Inflammation of orbital tissue Proptosis
Spreads to surrounding structures
Subperiosteal abscess Brain abscess Cavernous sinus thrombosis Meningitis Subdural empyema Orbital abscess
Notes:
Impinges on ocular muscles
Impaired extra- ocular movements
Pain with eye
movement or opthalmoplegia
Definitions:
Impinges on nerves
Afferent pupillary defect
Decreased visual acuity
Exposes cornea
Corneal drying and scarring
a. Chemosis: Edema of the bulbar conjunctiva
b. Panopthalmitis: inflammation of all coats of the eye including intraocular structures.
c. Endopthalmitis: inflammation of the interior of the eye.
1. See slide on Periorbital Cellulitis for how sinusitis can lead to the development of periorbital cellulitis
2. The micro-organism responsible for periorbital cellulitis varies depending on how the pathogen was introduced to the system.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 5, 2018 on www.thecalgaryguide.com")
Periorbital Cellulitis: Pathogenesis and Clinical Findings

Note: Also referred to as preseptal cellulitis
Dacryoadenitisa Conjunctivitisb
Acute chalazionc
Dacryocystitisd Hordeolume
Streptococcus pneumoniae, Moraxella catarrhalis, non-typable Haemophilus influenza (most common organisms)
Abrasion Insect bite
Burns Trauma
Local infection
Contiguous spread of infection
Sinusitis
Otitis media Hematogenous spread
Local break in skin Micro-organisms enter
Definitions:
Note:
Eye exam should reveal normal:
- extra-ocular
movements and globe
position
- pupillary reflex and
visual acuity
If any are abnormal, the presentation is no longer considered periorbital cellulitis, as the infection has likely spread beyond the preseptal compartment/orbital septum.
If the eye cannot be assessed, the patient NEEDS a CT scan.
Pathogens reach dermis and subcutaneous periorbital tissue
Periorbital Cellulitis
a. Dacryoadenitis: infection of the lacrimal glands
b. Conjunctivitis: inflammation of the conjunctiva
c. Chalazion: a benign, painless bump or nodule inside the upper or lower eyelid which results from healed internal hordeolums that are no longer infectious.
d. Dacryocystitis: an infection of the lacrimal sac, secondary to obstruction of the nasolacrimal duct at the junction of lacrimal sac.
e. Hordeolum: localized infection or inflammation of the eyelid margin involving hair follicles of the eyelashes or meibomian glands.
Spreads beyond preseptal compartment/orbital septum
Involves the orbit Orbital cellulitis
See slide on Orbital Cellulitis: Pathogenesis and clinical findings
Localized inflammation
Pain on palpation
Induration
Warmth
Eyelid and periorbital edema
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 5, 2018 on www.thecalgaryguide.com")
Child Abuse: Risk Factors and Possible Indicators
, especially <1 year old
↑ Risk
Note: Special Indicators for Sexual Abuse
Definition: Child Abuse
• Any act or omission
by a parent or caregiver that results in actual or potential harm to a child
• Includes physical, sexual, & emotional abuse, or neglect
Family Factors
Unrelated caregiver Low SES Single parent Domestic violence Social isolation
Indicators on History
Indicators on Physical Exam
Injury blamed on pet or sibling
Delays in seeking treatment
Frequent visits to different healthcare providers for injuries
Self-inflicted injury not compatible with child’s development
Child described as “difficult”
Hx of injury changes with time
History not compatible with injury
Extensive physical injury with hx of minor trauma
• • • • •
Regressive behaviour
Difficulty sleeping
Sexually inappropriate behaviour Sudden change in behaviour School difficulties
Burns (esp. immersion)
Frenulum tear in infants
Bruising: Pattern, Location (esp. face), Number, Shape (esp. ligature marks, instrumentation), Age of child (“those who don’t cruise don’t bruise”)
Abusive head trauma
See “Non-accidental Head Trauma” slide
Fractures (esp. posterior rib, shearing/twisting forces)
Evidence of injury with no hx of trauma
Suspicion of child abuse
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 5, 2018 on www.thecalgaryguide.com")
Circle of Willis: Anatomy and Physiology

*Anterior Communicating Artery (Acomm)
Note:
• Circle of Willis architecture serves as collateral circulation; i.e. there are alternative pathways for blood to travel in event of narrowing or occlusion of an artery
• * signifies common sites of aneurysm. These are junction sites that may become weak over time
• Anterior circulation: ICA, ACA, MCA; Posterior circulation: PCA, VA
• Findings from occlusion depend on the extent of occlusion and will
present with contralateral findings
• The cerebellar arteries are not included on this diagram
Supplies 2/3 of the lateral portions of frontal, temporal and parietal lobes, specifically UE and facial regions of the homunculus
Middle Cerebral Artery (MCA)
Supplies midbrain, thalamus, occipital lobe
Vertebral Arteries (VA)
Supplies brainstem, cerebellum, spinal cord, posterior portion of brain
Posterior Cerebral Artery (PCA)
Legend: Pathophysiology Mechanism
Sign/Symptom/Lab Finding Complications Published November 5, 2018 on www.thecalgaryguide.com
Basilar Artery (BA)
Supplies cerebellum, brainstem, occipital lobe
*Posterior Communicating Artery (Pcomm)
Internal Carotid Arteries (ICA)")
Mastoiditis: Pathogenesis and clinical findings

Distal middle ear is physically connected to mastoid air spaces
Pathogens spread from middle ear to the mastoid air spaces
Mucosa lining the mastoid becomes inflamed
Mastoiditis 1
Infection persists
Accumulation of pus in mastoid cavities
↑ pressure Formation of abscess cavities
Dissection of pus into adjacent areas
Infection spreads
Into intracranial compartment
See slide on Acute Otitis Media (AOM): Pathogenesis and Clinical Findings in Children
Post- operation
Trauma Infection
Notes:
1. Most common suppurative complication of AOM
Tenderness, erythema, swelling and fluctuance over the mastoid process
Inflammation spreads to external auditory canal
Cranial Nerve VII anatomically near mastoid
Cranial Nerve VIII anatomically near mastoid air space
Destroys bony septae b/t air cells (visible on CT)
Mastoid abscess
Swelling of external auditory canal
Mastoid inflammation disrupts nerve
Mastoid inflammation disrupts nerve
Petrositis
Facial nerve palsy
Sensorineural hearing loss Labyrinthitis
Osteomyelitis of the calvaria
Into adjacent bones
Underneath the periosteum Subperiosteal abscess Pinna is pushed out and
of the temporal bone
Into the neck beneath the attachment of the sternocleidomastoid and digastric muscles
forward
Dural venous thrombosis Temporal lobe abscess Meningitis
Epidural abscess Subdural abscess Cerebellar abscess
Bezold abscess
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 5, 2018 on www.thecalgaryguide.com")
Scarlet Fever: Pathogenesis and clinical findings

0-1 days post- pharyngitis
Pastia’s lines5
1-2 days post- pharyngitis
Appears on upper trunk and axillae
3-4 days post- pharyngitis
Spreads to remainder of body, sparring face6, palms and soles
7-10 days post- pharyngitis
Fades Desquamation7
Otitis media, sinusitis, pneumonia, bacteremia, osteomyelitis, meningitis, arthritis, erythema nodosum, hepatitis, acute poststreptococcal glomerulonephritis, and acute rheumatic fever
Fine maculopapular rash
Blanchable with Non-pruritic and pressure painless
Notes:
1. While the majority of infections are cases of GAS pharyngitis, rarely, it is possible to develop scarlet fever from a GAS skin infections. 2. Scarlet fever is most common in patients of this age group although, rarely, it can occur in adults.
3. White strawberry tongue is characterized by a white coating on the tongue through which edematous lingual papillae project.
4. Red strawberry tongue is characterized by a beefy red, edematous tongue covered in edematous lingual papillae.
5. Prominent erythema and petechiae in the body folds, especially the antecubital fossae and axillary folds. They tend to appear before the rash and persist through the desquamation phase.
6. Typically, the rash does not occur on the face, although facial flushing may be noted. When this occurs, there is perioral sparring.
7. Desquamation tends to occur ~1 week after the rash fades, most severely effecting the hands and feet, and lasts 2-6 weeks. While a classical presentation, not
everyone gets it.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 5, 2018 on www.thecalgaryguide.com")
Sinusitis: Pathogenesis and clinical findings

Tonsillitis: Pathogenesis and clinical findings
 infection1,2
Authors:
Amanda Marchak
Reviewers:
Nicola Adderley Jim Rogers Danielle Nelson* * MD at time of publication
Viral pathogen1
5-15 years3
Pathogen colonizes the nasopharynx
Pathogen colonizes oropharynx4 **
↑ vascular permeability Leakage of protein and fluid
into surrounding tissue
Inflammatory cytokine release
Inadvertent cellular injury and hemolysis
Tonsillar petechiae and erythema
Systemic inflammatory cytokines disrupt hypothalamic regulation
Fever
White blood cell (WBC) activation WBCs infiltrate site of infection
WBCs kill pathogen
Accumulation and deposition of cellular debris and products of inflammatory response
Tonsillar exudate
Note:
*When GAS is the pathogen, cytokine release and WBC activation is secondary to the release of exotoxins by GAS.
Swelling and irritation
↑ lymph drainage to regional nodes
Enlarged anterior cervical nodes
Cough
Note:
It is extremely important to distinguish between viral tonsillitis and bacterial tonsillitis. Viral tonsillitis is usually self-limited while GAS tonsillitis can be associated with a number of complications.
Notes:
Tonsillar tissue
Tonsillar edema
Nasal tissue6
Nasal congestion
Coryza
Nasal discharge irritates back of throat
Complications5:
Peritonsillar abscess, neck abscess, otitis media, sinusitis, pneumonia, scarlet fever, bacteremia, osteomyelitis, meningitis, arthritis, erythema nodosum, hepatitis, acute poststreptococcal glomerulonephritis, acute rheumatic fever, and toxic shock syndrome
1. In general, viral tonsillitis is more common than GAS infection. However, in the absence of cough and coryza (acute, isolated tonsillitis), GAS is more common.
2. While GAS is the most bacterial cause of tonsillitis, it can be caused by other pathogens.
3. GAS tonsillitis is most common in patients of this age group although, rarely, it can occur in adults.
4. When GAS colonizes the oropharynx, the primary location of infection determines how it’s identified.
• tonsils primarily effected = tonsillitis
• pharynx (throat) primarily effected = pharyngitis (See slide on Group A Streptococci
Pharyngitis: Pathogenesis and Clinical Findings) • both = pharyngotonsillitis
5. The listed complications are the result of exotoxins entering systemic circulation or the bacterial infection extending beyond the tonsils.
6. While viral tonsillitis tends to be associated with more upper respiratory tract symptoms, clinical signs and symptoms are NOT reliable for diagnosing GAS tonsillitis. Throat swab or rapid antigen detection test are the standards for diagnosis.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 5, 2018 on www.thecalgaryguide.com")
Stomach Acid Reducing Medications - Mechanisms of Action
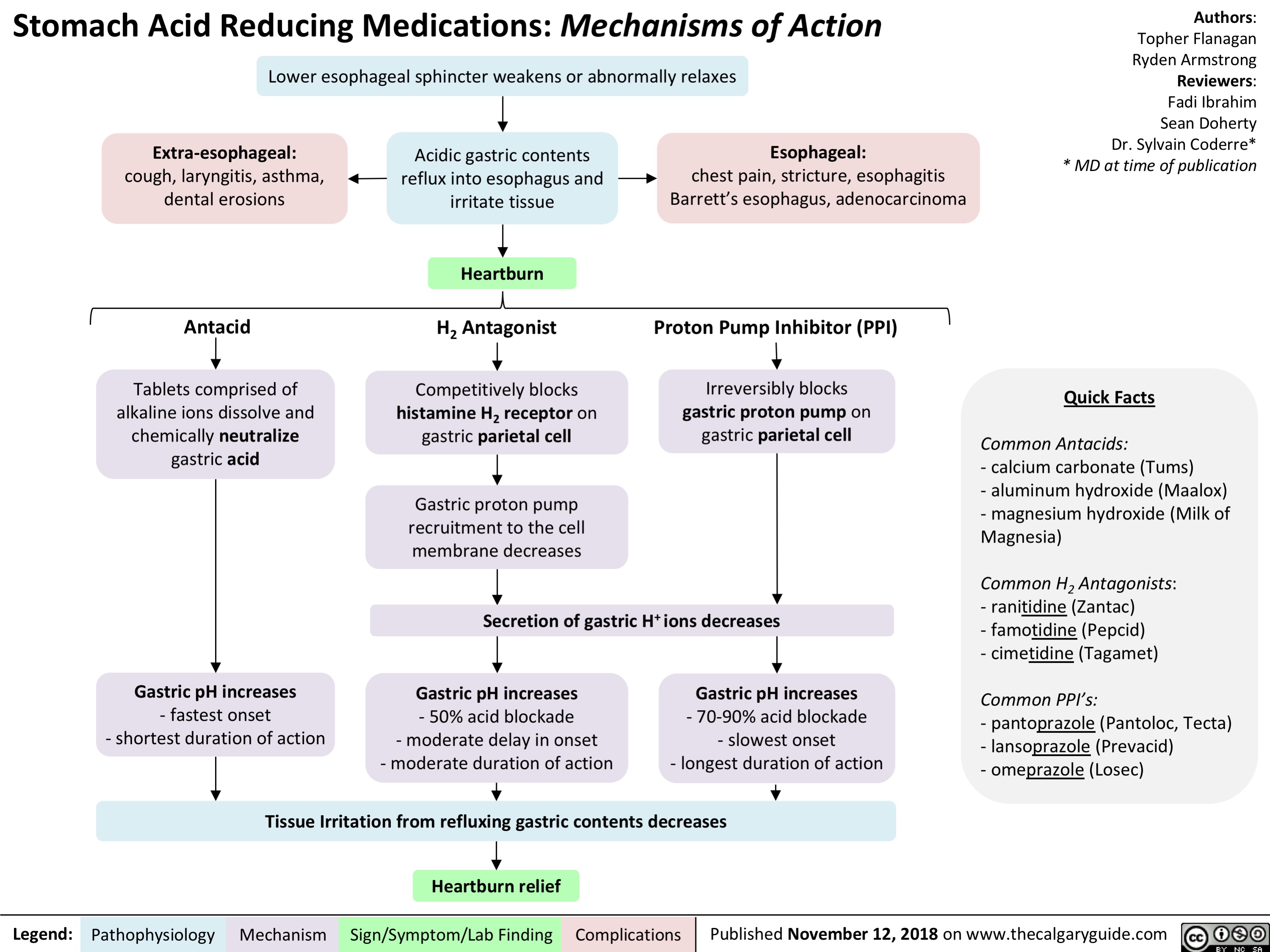
Dependent Personality Disorder Slide - Pathogenesis and clinical findings
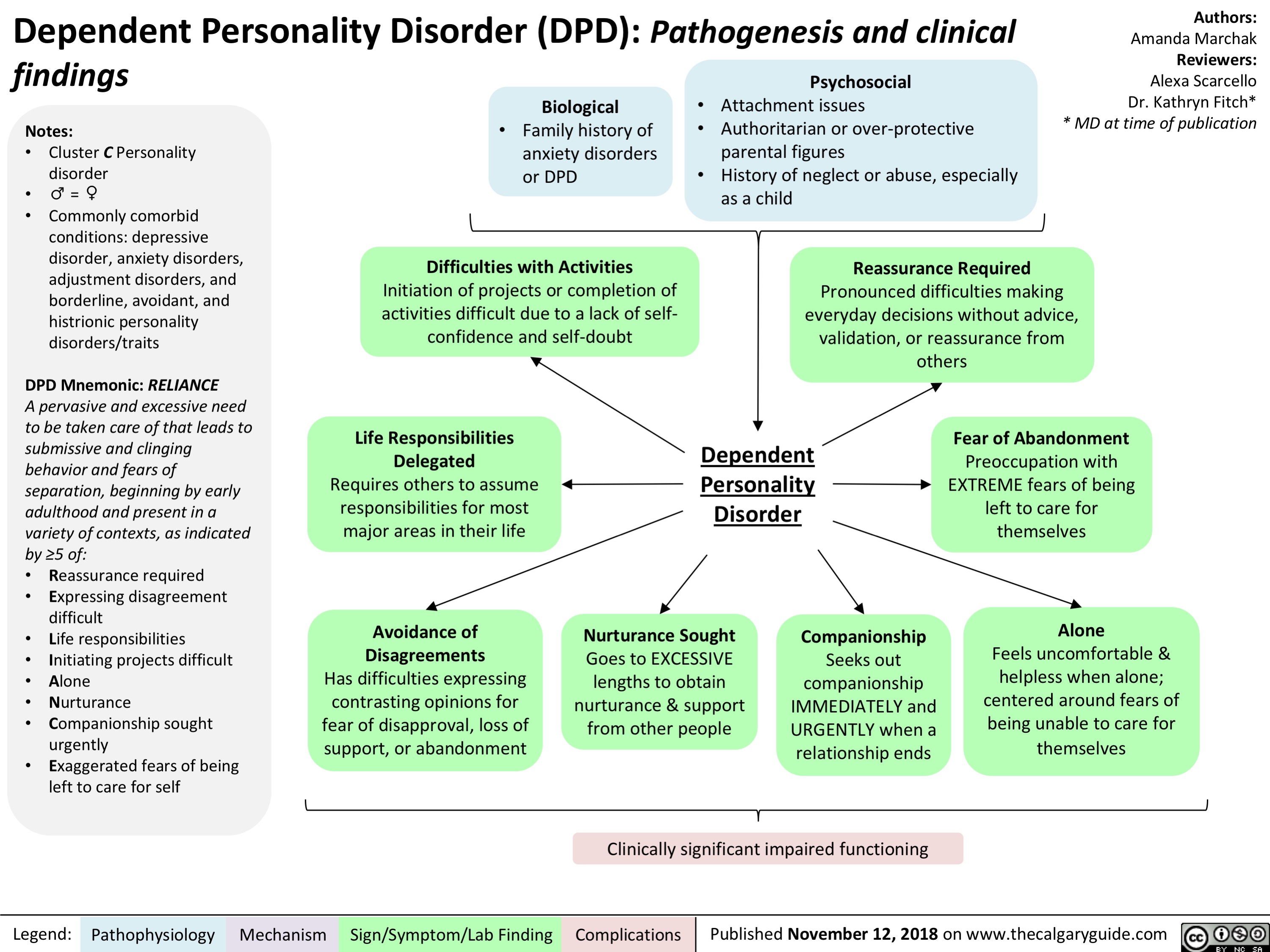
Obsessive-Compulsive Personality Disorder Slide - Pathogenesis and clinical findings

Brain Death: Pathogenesis assessment and clinical findings
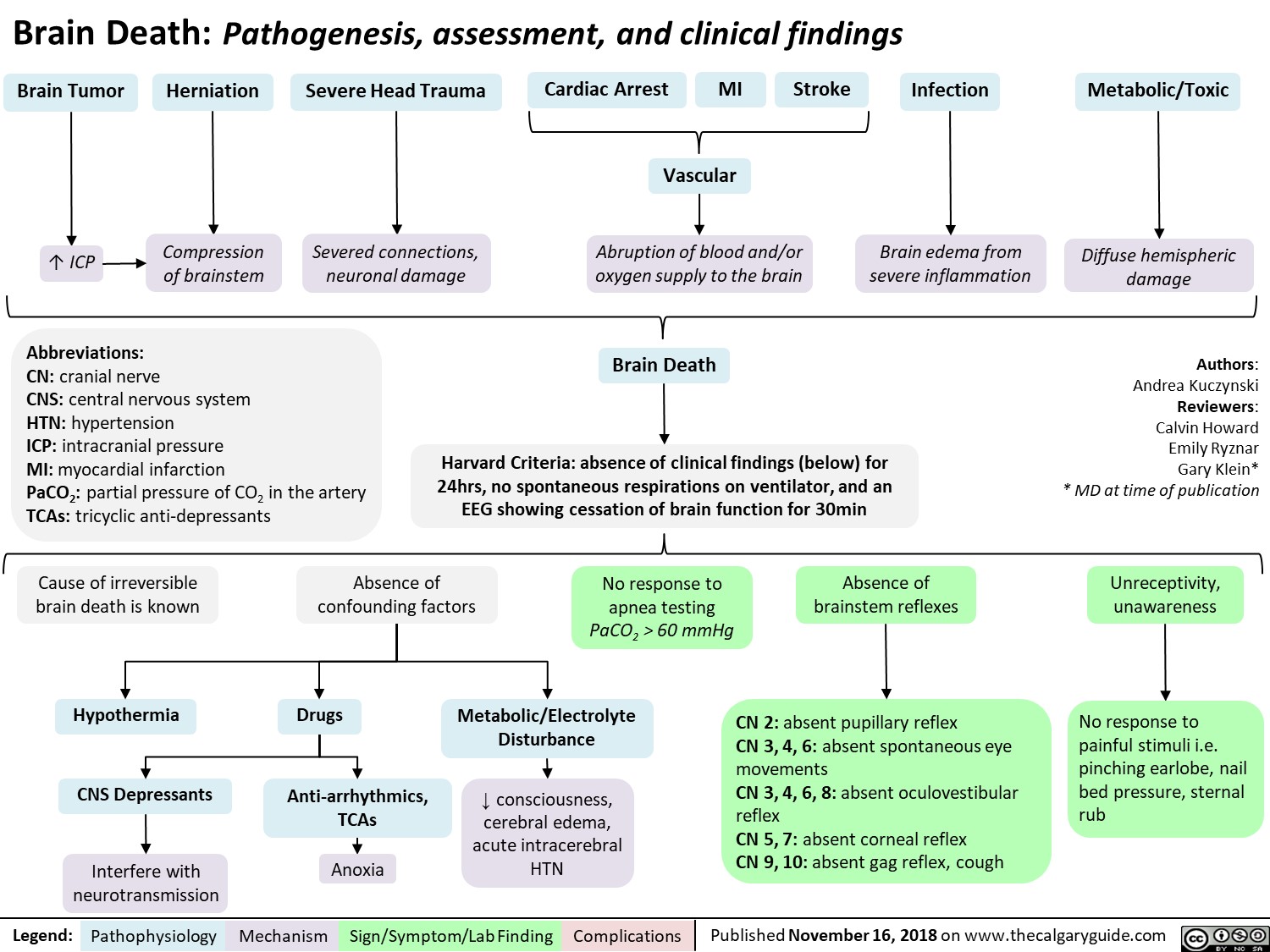
Benefits of Breast Milk: Mechanism of Action

Major Depressive Disorder: Complications

Avoidant Personality Disorder - Pathogenesis and clinical findings

Measures of Population Health
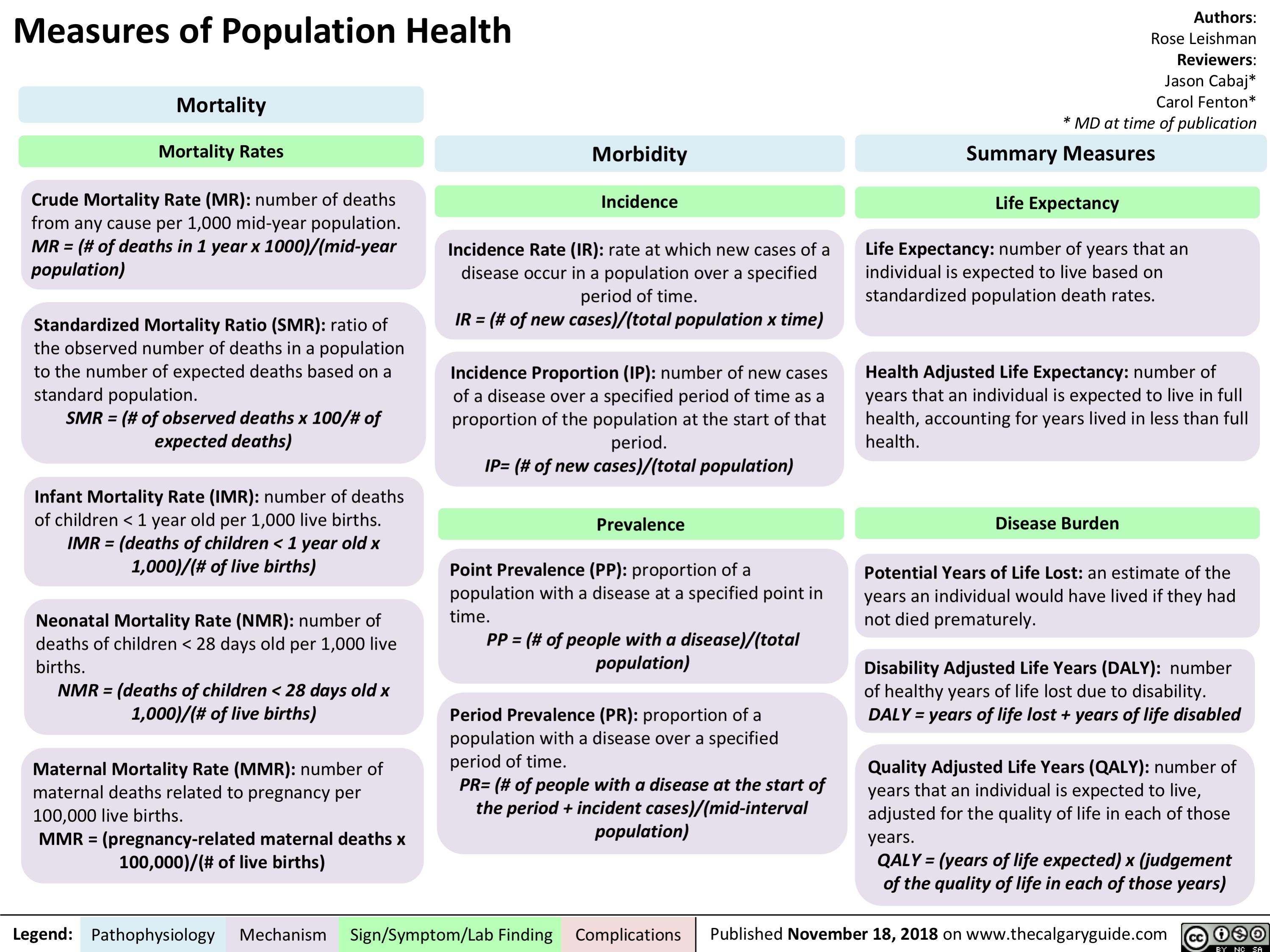
Employment as a Determinant of Health
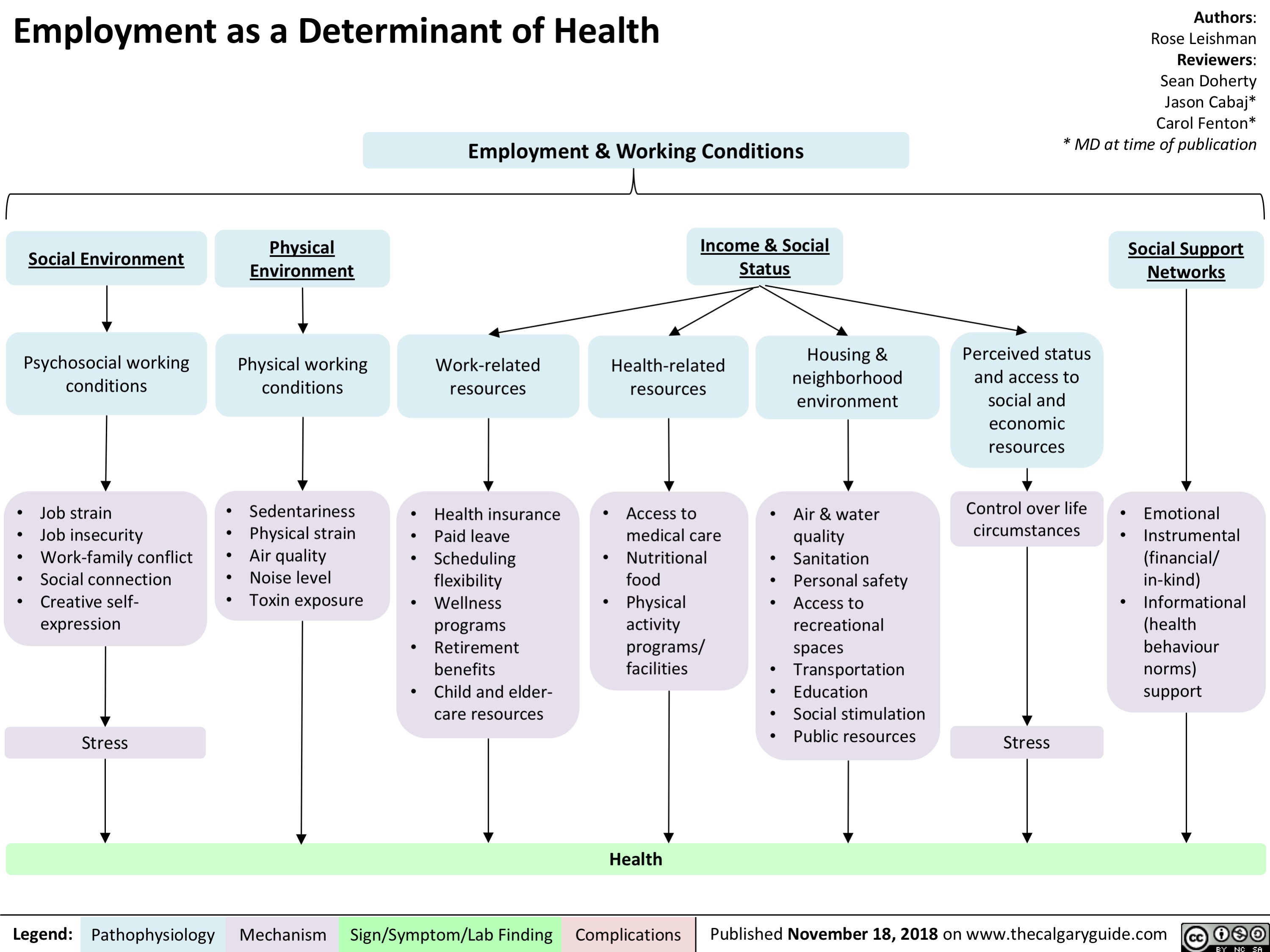
Menopause contraindications to hormone replacement therapy
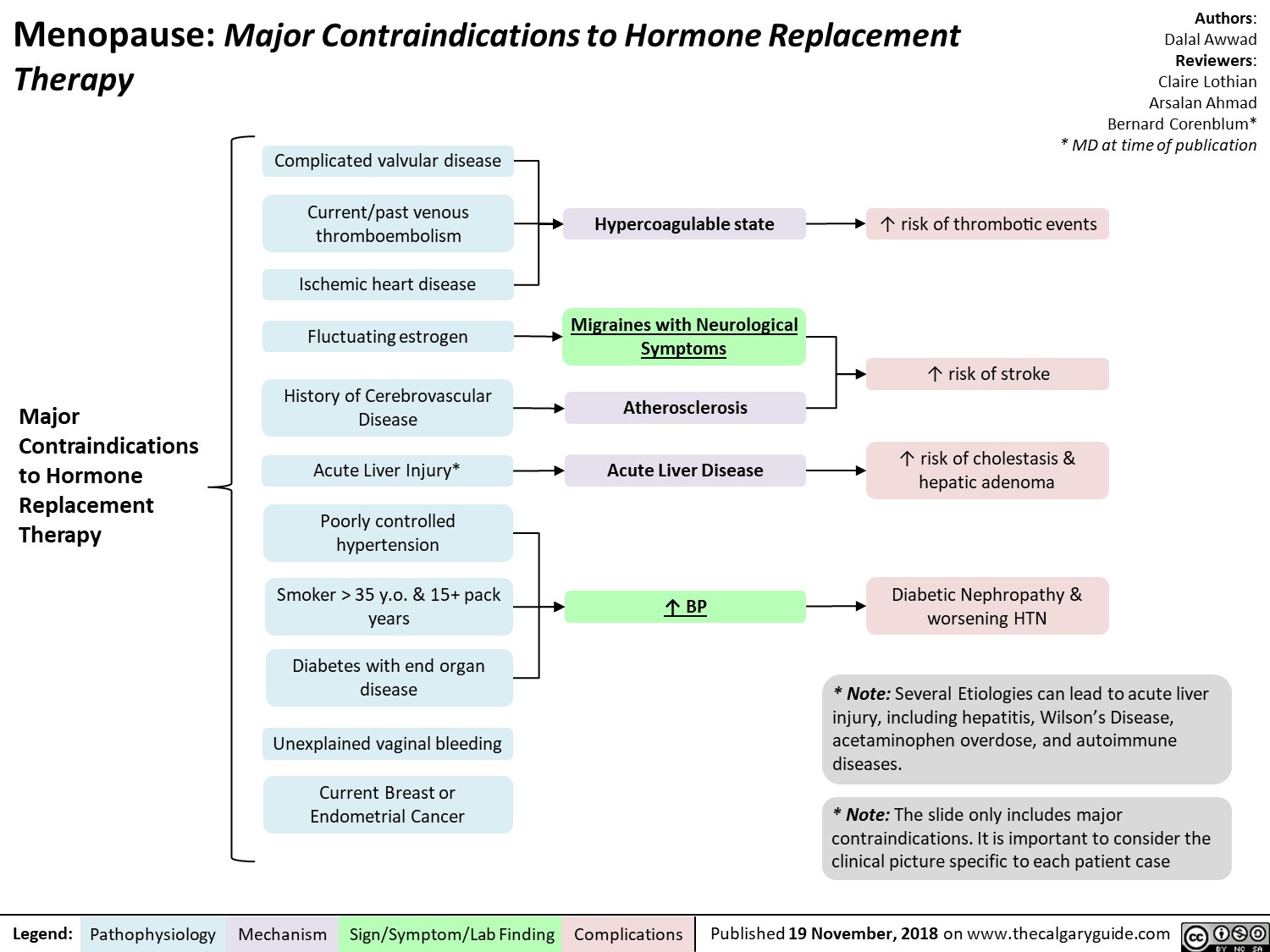
Phenylketonuria (PKU): Pathogenesis and clinical findings
![Phenylketonuria (PKU): Pathogenesis and clinical findings
Authors: Hamna Tariq Reviewers: Chandan Kaur Bal Nicola Adderley Rebecca Sparkes* * MD at time of publication
Abbreviations:
PAH – phenylalanine hydroxylase BH4 – tetrahydrobiopterin
Phe – phenylalanine
Tyr - tyrosine
LAT-1 - L-amino acid transporter 1 LNAA – large neutral amino acids NT – neurotransmitter
Biallelic mutations in PAH gene on chromosome 12q23.2
Loss of activity/deficiency of PAH
Inability to convert Phe to Tyr
Buildup of Phe and its metabolites
↑ transport of Phe via LAT-1 at the blood brain barrier
Phe outcompetes LNAA for binding sites on LAT-1
↓ LNAA transport
↓ cerebral protein synthesis and ↓ NT synthesis
White matter lesions, oxidative damage, hypomelination & demyelination
Sources of Phe
Dietary protein
Breakdown into amino acids
↓ Tyr and derivatives
↓ melanin
Fair skin and hair
Notes:
Endogenous recycling of amino acid stores
Phe oxidized to phenylacetate
Musty odor to urine, sweat and breath
• Autosomal recessive inborn error of metabolism; clinical severity depends on residual PKU activity
• This slide denotes clinical features of classical PKU in untreated patients. Symptoms develop within a few months of birth only if untreated.
• PAH, using a BH4 cofactor, converts Phe to tyrosine, which is necessary to produce epinephrine, norepinephrine, dopamine and melanin. (Rare inherited disorders of BH4 synthesis/recycling cause elevated Phe and neurologic symptoms.)
• PKU is screened for at birth in most developed nations.
• In early-diagnosed, continuously treated patients, ID,
microcephaly and neurologic features are not expected, but there is still an increased incidence of behavioral, emotional and social problems
↑ brain [Phe]
Behavioral, emotional & social problems (ADHD, mood disorders, aggression, ↓ self-esteem, ↓ social competency, ↓ autonomy)
Intellectual disability
(↓ language, memory & learning skills, executive function, IQ, school performance)
Neurological findings (tremor, shaking, seizures, poor coordination)
Microcephaly
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 19, 2018 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2018/11/Phenylketonuria_Final.jpg "Phenylketonuria (PKU): Pathogenesis and clinical findings
Authors: Hamna Tariq Reviewers: Chandan Kaur Bal Nicola Adderley Rebecca Sparkes* * MD at time of publication
Abbreviations:
PAH – phenylalanine hydroxylase BH4 – tetrahydrobiopterin
Phe – phenylalanine
Tyr - tyrosine
LAT-1 - L-amino acid transporter 1 LNAA – large neutral amino acids NT – neurotransmitter
Biallelic mutations in PAH gene on chromosome 12q23.2
Loss of activity/deficiency of PAH
Inability to convert Phe to Tyr
Buildup of Phe and its metabolites
↑ transport of Phe via LAT-1 at the blood brain barrier
Phe outcompetes LNAA for binding sites on LAT-1
↓ LNAA transport
↓ cerebral protein synthesis and ↓ NT synthesis
White matter lesions, oxidative damage, hypomelination & demyelination
Sources of Phe
Dietary protein
Breakdown into amino acids
↓ Tyr and derivatives
↓ melanin
Fair skin and hair
Notes:
Endogenous recycling of amino acid stores
Phe oxidized to phenylacetate
Musty odor to urine, sweat and breath
• Autosomal recessive inborn error of metabolism; clinical severity depends on residual PKU activity
• This slide denotes clinical features of classical PKU in untreated patients. Symptoms develop within a few months of birth only if untreated.
• PAH, using a BH4 cofactor, converts Phe to tyrosine, which is necessary to produce epinephrine, norepinephrine, dopamine and melanin. (Rare inherited disorders of BH4 synthesis/recycling cause elevated Phe and neurologic symptoms.)
• PKU is screened for at birth in most developed nations.
• In early-diagnosed, continuously treated patients, ID,
microcephaly and neurologic features are not expected, but there is still an increased incidence of behavioral, emotional and social problems
↑ brain [Phe]
Behavioral, emotional & social problems (ADHD, mood disorders, aggression, ↓ self-esteem, ↓ social competency, ↓ autonomy)
Intellectual disability
(↓ language, memory & learning skills, executive function, IQ, school performance)
Neurological findings (tremor, shaking, seizures, poor coordination)
Microcephaly
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 19, 2018 on www.thecalgaryguide.com")
Feedback Loop: Prolactin (PRL)

Authors: Nicola Adderley Reviewers: Andrea Kuczynski Bernard Corenblum* * MD at time of publication
Abbreviations:
TRH: Thyrotropin Releasing Hormone
DA: Dopamine
GnRH: Gonadotropin Releasing Hormone FSH: Follicle Stimulating Hormone
LH: Luteinizing Hormone
Note:
• PRL levels exhibit diurnal, menstrual, and age-related variation
• TRH has a stimulatory effect on PRL release; however, dopamine is the principal regulator of PRL secretion
Alveolar Cells of Breast Ducts
Milk production and release
Lactation
TRH
Suckling stimulus (via spinal afferents)
+
+
Hypothalamus + (arcuate nucleus)
DA
-
Anterior Pituitary Gland Lactotrophs
Uterus, immune cells, breast tissue, prostate
PRL
Hypothalamus
↓ GnRH secretion ↓ FSH/LH
↓ estradiol in females, ↓ testosterone in males
Limbic System
↓ libido
Immune System Organs
Promotes proliferation and maturation of immune cells
Oxytocin
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 19, 2018 on www.thecalgaryguide.com")
Vesicoureteric reflux (VUR): Pathogenesis and clinical findings
: Pathogenesis and clinical findings
Authors: Nicola Adderley Reviewers: Emily Ryznar *Lindsay Long * MD at time of publication
Abnormal function
Abnormal anatomy
Neurogenic bladder (e.g. cerebral palsy, constipation, spinal injury, iatrogenic)
Non-neurogenic bladder (neuropsychological)
Lower urinary tract abnormality (posterior urethral valves, meatal stenosis)
Bladder outlet obstruction
↑ pressure distorts UVJ
Upper urinary tract abnormality (ureters)
UVJ abnormality
Incomplete closure of UVJ during bladder contraction
Abbreviations
• UVJ - ureterovesicular junction • UTI – urinary tract infection
Failure of bladder sphincter to relax during bladder contraction
Vesicoureteric reflux (VUR):
Back flow of urine from the bladder into one or both ureters +/- kidneys
Migration of lower urinary tract bacteria to kidneys
Bacterial invasion of renal parenchyma
Upper UTI (pyelonephritis)
Incomplete emptying of bladder during Abnormal
↑ pressure in bladder
Bladder dilates
Dilated bladder on U/S
urination
Bacteria in bladder are not cleared during urination
voiding habits
↑ bladder capacity
Renal scarring
↓ functional renal tissue
*Chronic kidney disease (↓ GFR,
hypertension, proteinuria)
Flank tenderness
Fever, dysuria, urgency, frequency
Lower UTI (cystitis) Urinary stasis
Cloudy, foul- smelling urine
Urethral stricture
Notes
Urgency, dysuria, frequency
• First febrile UTI in an infant should trigger a work-up for VUR
• High likelihood of spontaneous resolution • *Late complication of severe VUR
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 19, 2018 on www.thecalgaryguide.com")
IVH Intraventricular Hemorrhage in Preterm Infants - Pathogenesis

↑ susceptibility to ischemia/reperfusion injury
GM capillary network is prone to hemorrhage
Hemorrhage in germinal matrix capillary bed, which drains into venous system
Intraventricular Hemorrhage
hemorrhage in periventricular subependymal germinal matrix
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 20, 2018 on www.thecalgaryguide.com")
Prader Willi syndrome: pathogenesis and clinical findings
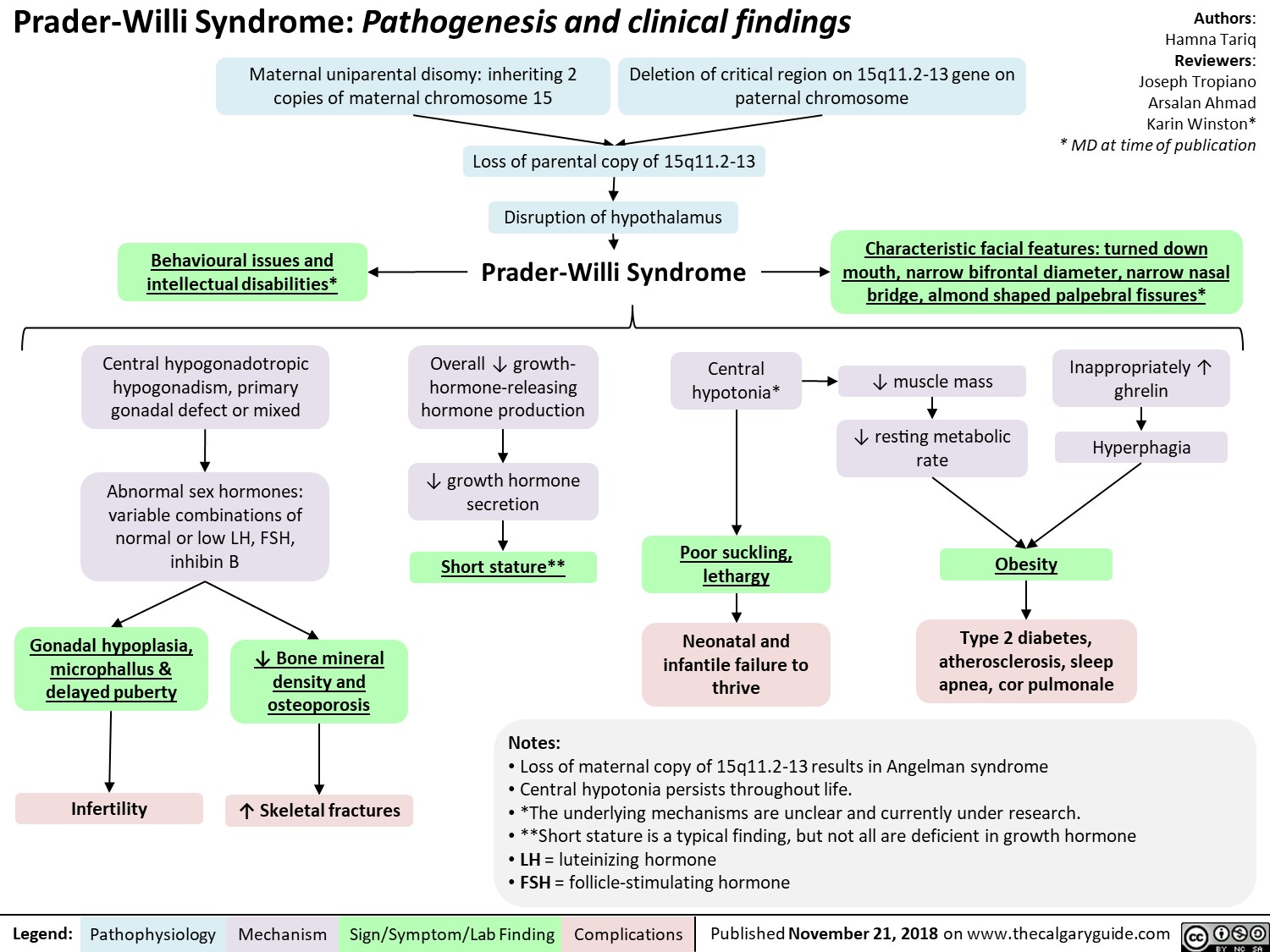
Anticonvulsants as Mood Stabilizers: Mechanism and Side-effect
, thrombocytopenia
Abbreviations: • VSSCs: Voltage-Sensitive Sodium Channels")
Benzodiazepine (BZD) withdrawal: clinical findings and complications
 withdrawal: clinical findings and complications
Abrupt cessation of chronic ingestion of BZDs
Administration of BZD antagonist (flumazenil) on patients who have developed -* tolerance/dependence to BZD
Withdrawal Seizure
Negative physiological reactions BZD intake inhibition a mygd to f, • of a la Withdrawal symptoms Benzodiazepine Withdrawal GABA receptor activity (less inhibition alleviated by ingesting BZD Tolerance GABA BZD intake Conformational changes in the GABA receptor 1, receptor's Withdrawal Insomnia Pro-excitatory 4— state of excitatory neurotransmitters) 4— to the agent activity affinity for the agent
A
Activation of ACC and OFC
Feelings of fear
Activation of PAG
Behavioural response of fight or flight
Legend: Pathophysiology Mechanism
Activation of hypothalamus '1` Cortisol CAD, T2DM, Stroke
Sign/Symptom/Lab Finding
Activation of PBN
V
t RR, SOB, Asthma, or a sense of being smothered
Activation of LC
t Sympathetic Activity
t BP, t HR variability, tremor, and diaphoresis
Authors: Usama Malik Reviewers: Sina Marzoughi Aaron Mackie* * MD at time of publication
Notes: • The onset of withdrawal can vary according to the half-life of the BZD involved. Symptoms may be delayed up to three weeks in BZDs with long half-lives, but may appear as early as 24 to 48 hours after cessation of BZDs with short half-lives.
Abbreviations: • ACC: Anterior Cingulate Cortex • BP: Blood Pressure • CAD: Coronary Artery Disease • HR: Heart Rate • LC: Locus Coeruleus • MI: Myocardial Infarction • OFC: Orbitofrontal Cortex • PAG: Periaqueductal Gray • PBN: Parabrachial Nucleus • RR: Respiratory Rate • SOB: Shortness of Breath • T2DM: Type 2 Diabetes
I` atherosclerosis, cardiac ischemia, MI, or sudden death")
Benzodiazepines: Mechanism of Action and Side Effects

Schizotypal Personality Disorder (SPD): Pathogenesis and clinical findings
: Pathogenesis and clinical findings
Genetics Environmental Neurobiological Changes Neurotransmitter /1` prevalence among first-More common among Significant atrophy of the Imbalance degree relatives of people with lower (predominantly left) lateral Dysfunction in synaptic probands with incomes and those never temporal lobe. Certain subregions dopamine degradation, Schizophrenia. Genes associated with married, divorced, separated, or widowed. of the prefrontal cortex have been shown to be enlarged. usually due to gene catechol-0- schizophrenia are also risk factors for Schizotypal PD. Volume 1, of specific temporal lobe subregions. methyltransferase (COMT).
Cognitive-perceptual •
Magical thinking Belief in paranormal or supernatural phenomena, such as superstitions, telepathy, weird fantasies
Unusual Perceptions Seeing a halo or aura, presence of unseen force, or bodily illusions
Ideas of Paranoia/ Reference Suspiciousness Believing Can range from coincidences persistent and have strong overt hostility, personal guardedness to significance pleasant and agreeable compliance
Schizotypal Personality Disorder Oddness/ disorganized
► Interpersonal
Lack Close Friends Deficit in finding social interactions gratifying, a form of social anhedonia
Constricted affect
Eccentric behavior Unusual thinking or or appearance speech Unconventional or Speech and thought idiosyncratic process can be hygiene, attire, or vague, unelaborate, social behaviors circumstantial, metaphorical, or stereotyped but not grossly incoherent or blocked
Social Anxiety Unrelenting, situationally generalized, unconditional, and does not tend to lessen with familiarity
Clinically significant impaired functioning
Authors: Usama Malik Reviewers: Sina Marzoughi Aaron Mackie* * MD at time of publication
Notes: • Cluster A Personality Disorder • 4.2CY : 3.7g - frequently diagnosed in fragile X syndrome • 3.9-4.6%of adults • More than half of these patients have at least one episode of major depression
SPD Mnemonic: ME PECULIAR • Magical thinking Experiences unusual perceptions • Paranoid / suspicious ideation • Eccentric behavior or appearance • Constricted or inappropriate affect • Unusual thinking or speech • Lacks close friends • Ideas of reference • Anxiety in social situations • Rule out psychotic or pervasive developmental disorders
• Dx: present in a variety of contexts causing marked social impairment")
Boutonniere Deformity: Pathogenesis and Complications

menstrual-cycle-physiology-ovarian-cycle-brief-overview

Complex Regional Pain Syndrome: Pathogenesis and clinical findings

Sensory: Hyperalgesia or allodynia
Sudomotor: Edema, sweating changes, asymmetric sweating Vasomotor: Temperature asymmetry, altered skin colour
Motor/trophic: Decreased range of motion, motor dysfunction, trophic changes
Definitions:
• Hyperalgesia: Heightened sensation of pain
• Allodynia: Pain caused by normally non-painful stimuli • Sudomotor: Relating to the sweat glands
• Vasomotor: Relating to the muscle within vasculature • Trophic: Relating to growth and atrophy of cells
• Cytokine: Molecules that recruit inflammatory cells
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 20, 2018 on www.thecalgaryguide.com")
Microangiopathic Hemolytic Anemia: Pathogenesis and clinical findings

↓ Inhibition of complement
Immune inflammatory
↑ Pressure in
↑ Extrinsic clotting pathway activation
TTP
(See TTP-HUS Slide)
Disruption of
endothelial cell
activation perfusion/ischemia response metabolism vasculature ↑Thrombin Deficient
Placental under-
renal afferent
↑ Complement pathway activation
MAC-mediated cell lysis
Cytokine release
Endothelial injury
Shear stress on endothelium
production
↑ Fibrin clot production and deposition in small vessels
ADAMTS13 protease enzyme
↓ Cleavage and ↑ accumulation of VWF multimers
Abbreviations:
• HELLP - Hemolysis, Elevated Liver Enzymes, Low Platelets • HUS - Hemolytic-Uremic Syndrome
• DIC - Disseminated Intravascular Coagulation
• TTP - Thrombotic Thrombocytopenic Purpura
• MAC - Membrane Attack Complex
• STEC - Shiga Toxin-Producing Escherichia coli
• VWF - Von Willebrand Factor
Pro-thrombotic Environment (see Virchow’s Triad Slide)
Platelet aggregation Mechanical obstruction of the vessel lumen
Hypercoagulable state
Thrombocytopenia
↑ RBC production in bone marrow
↑ Reticulocytes
Hemoglobin released from damaged RBCs Shearing of RBCs Anemia
Binds to haptoglobin Conversion to bilirubin in liver
↓ Free haptoglobin ↑Indirect bilirubin
Shistocytes Jaundice
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 13, 2018 on www.thecalgaryguide.com")
Neurogenic Claudication: Pathogenesis and Clinical Findings
 and myotomal distribution (weakness, cramping) of the impaired spinal nerve when walking or standing. Relieved with rest.
Symptoms distributed along the dermatome and myotome
Neurogenic
• Position dependent
• Dermatomal distribution
• Proximal to distal progression
Vascular
• Exercise dependent
• Sclerotomal distribution
• Distal to proximal progression
Hip extension
Buckling of ligamentum flavum and overlapping of adjacent vertebral laminae and facets
↓ canal size ↑ compression
Worsening of symptoms
Myotomal:
weakness, cramping
Dermatomal:
pain, paraesthesias
Modification of symptoms with movement and position
Exercise
↑ vasodilation of
spinal arteries ↑ compression
Hip flexion
Stretching of ligamentum flavum, reduction of overlap of adjectent vertebral laminae and facets, enlarged foramina
↑ canal size
↓ compression
Slow relief of symptoms (>30 min)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published December 7, 2018 on www.thecalgaryguide.com")
Atopic Dermatitis: Pathogenesis and Clinical Findings
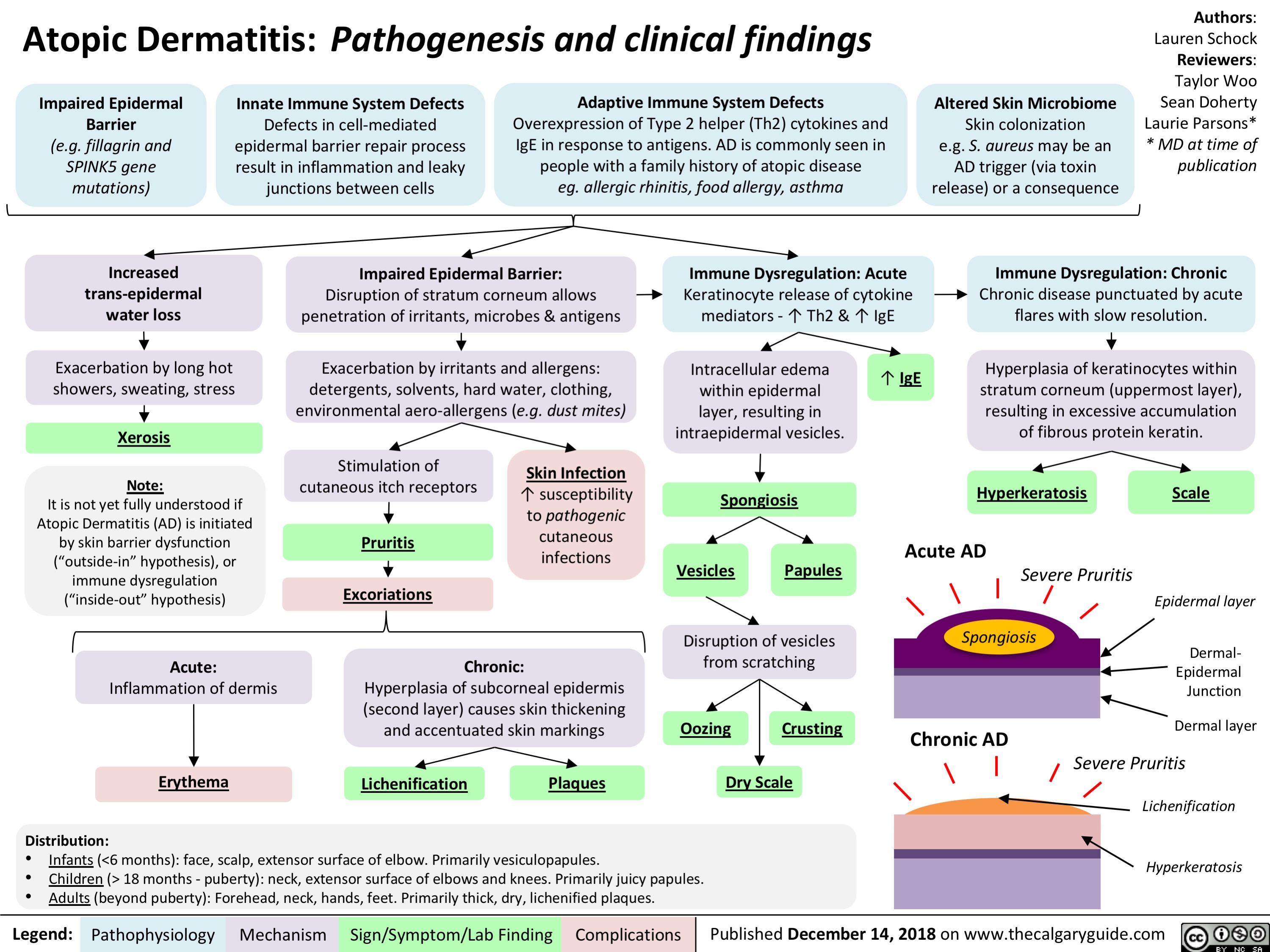
Rosacea: Pathogenesis and Clinical Findings
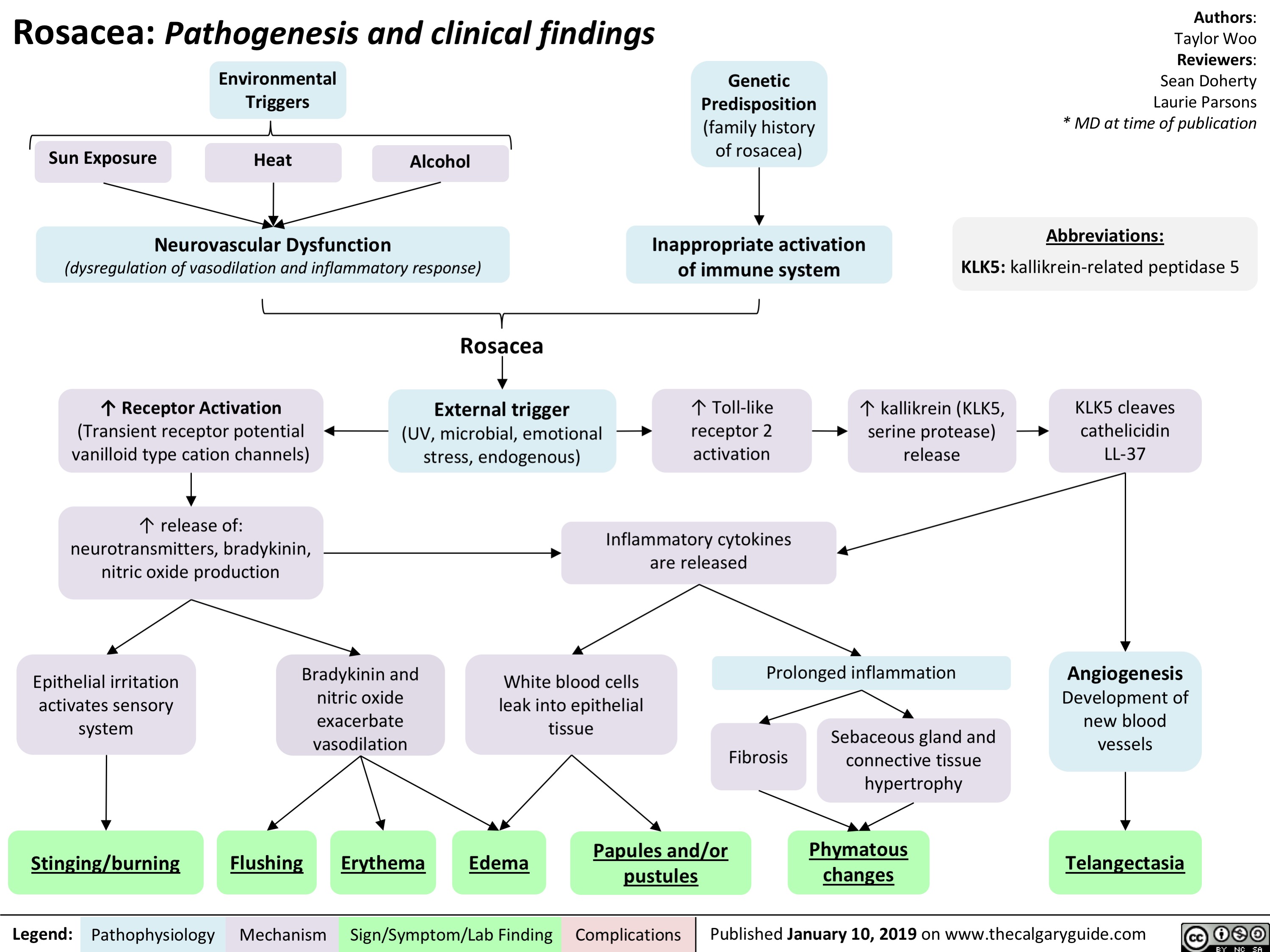
Hepatic Encephalopathy: Pathogenesis and Clinical Findings

Hypernatremia Physiology
![Hypernatremia: Physiology Unreplaced H2O loss
Hypodipsia
H2O shift into cells
Severe exercise, electroshock induced seizures
Transient ↑ cell osmolality
Na+ overload
Inappropriate IV hypertonic solution, salt poisoning
Abbreviations:
H2O: Water
GI: Gastrointestinal
DM: Diabetes Mellitus
DI: Diabetes Insipidus
Na+: Sodium ion
IV: Intravenous
ADH: Antidiuretic Hormone LOC: Level of Consciousness
Skin
Sweat, burns
GI
Vomiting, bleeding, osmotic diarrhea
Fluid [Na+] < serum [Na+]
↑ H2O loss compared to Na+ loss
Renal
DM, Mannitol, Diuretics
Absent thirst mechanism
Hypothalamic lesion impairs normal drive for H2O intake
Nephrogenic
↑ renal resistance to ADH
H2O Deprivation Test + no AVP response
↓ access to H2O
DI
Central
↓ ADH secretion
H2O Deprivation Test + AVP response
↑ [Na+] 10- 15 mEq/L within a few minutes
Weakness, irritability, seizures, coma
↑ thirst, ↓ urinary frequency and volume
Note:
Hypernatremia
Serum [Na+] > 145 mmol/L
Intracranial hemorrhage
Headache, vomiting, ↓ LOC
• Plasma [Na+] is regulated by water intake/excretion, not by changes in [Na+].
• Effects on plasma [Na+] of IV fluids or loss of bodily fluids is determined by the tonicity of the fluid, not the osmolality.
Authors: Mannat Dhillon Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 11, 2019 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2019/01/Hypernatremia-Physiology-.jpg "Hypernatremia: Physiology Unreplaced H2O loss
Hypodipsia
H2O shift into cells
Severe exercise, electroshock induced seizures
Transient ↑ cell osmolality
Na+ overload
Inappropriate IV hypertonic solution, salt poisoning
Abbreviations:
H2O: Water
GI: Gastrointestinal
DM: Diabetes Mellitus
DI: Diabetes Insipidus
Na+: Sodium ion
IV: Intravenous
ADH: Antidiuretic Hormone LOC: Level of Consciousness
Skin
Sweat, burns
GI
Vomiting, bleeding, osmotic diarrhea
Fluid [Na+] < serum [Na+]
↑ H2O loss compared to Na+ loss
Renal
DM, Mannitol, Diuretics
Absent thirst mechanism
Hypothalamic lesion impairs normal drive for H2O intake
Nephrogenic
↑ renal resistance to ADH
H2O Deprivation Test + no AVP response
↓ access to H2O
DI
Central
↓ ADH secretion
H2O Deprivation Test + AVP response
↑ [Na+] 10- 15 mEq/L within a few minutes
Weakness, irritability, seizures, coma
↑ thirst, ↓ urinary frequency and volume
Note:
Hypernatremia
Serum [Na+] > 145 mmol/L
Intracranial hemorrhage
Headache, vomiting, ↓ LOC
• Plasma [Na+] is regulated by water intake/excretion, not by changes in [Na+].
• Effects on plasma [Na+] of IV fluids or loss of bodily fluids is determined by the tonicity of the fluid, not the osmolality.
Authors: Mannat Dhillon Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 11, 2019 on www.thecalgaryguide.com")
Hyponatremia- Physiology
![Hyponatremia: Physiology
Authors: Mannat Dhillon Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Abnormal Renal H2O Handling (hypo-osmolar serum)
AKI/CKD Heart failure
↓ renal blood flow
↓ glomerular filtration
GFR < 25 mL/min, ↓ urine dilution ↑ H2O retention
Note:
• Plasma [Na+] is regulated by water intake/excretion, not by changes in [Na+].
• Artifactual hyponatremia can be differentiated by a normal or hyperosmolar serum.
Appropriate ADH secretion
↓ EABV
Hypovolemia: losses via GI, renal, skin, 3rd spacing, bleeding
Hypervolemia: heart failure, cirrhosis
↑ Na+/H2O absorption at PCT
↓ EABV, ↑ H2O retention
Urine [Na+] < 20 mmol/L
Hereditary: tubular disorders
(Bartter, Gitlemann syndromes).
Thiazide diuretics
Inappropriate: SIADH, hypothyroidism, AI
Normal EABV
Anti-diuresis
Primary polydipsia, eating disorder
↑ H2O or ↓ solute intake
↓ Osmoles
Impaired desalination
Block NCC
↑ H2O retention ↑ Na+/K+ excretion
Hyponatremia
Serum [Na+] < 135 mmol/L
Urine osmolality > 100 mmol/L
Urine osmolality < 100 mmol/L
Cerebral edema, ↑ intracranial pressure, vasoconstriction
If hypovolemic: ↓ JVP, ↓ blood pressure
Lethargy, altered mental status
Abbreviations:
AKI: Acute Kidney Injury
CKD: Chronic Kidney Disease
GFR: Glomerular Filtration Rate
H2O: Water
PCT: Proximal Convoluted Tubule
EABV: Effective Arterial Blood Volume
NCC: Na+/Cl- Co-Transporter
SIADH: Syndrome of Inappropriate ADH Secretion AI: Adrenal Insufficiency
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 11, 2019 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2019/01/Hyponatremia-Physiology-.jpg "Hyponatremia: Physiology
Authors: Mannat Dhillon Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Abnormal Renal H2O Handling (hypo-osmolar serum)
AKI/CKD Heart failure
↓ renal blood flow
↓ glomerular filtration
GFR < 25 mL/min, ↓ urine dilution ↑ H2O retention
Note:
• Plasma [Na+] is regulated by water intake/excretion, not by changes in [Na+].
• Artifactual hyponatremia can be differentiated by a normal or hyperosmolar serum.
Appropriate ADH secretion
↓ EABV
Hypovolemia: losses via GI, renal, skin, 3rd spacing, bleeding
Hypervolemia: heart failure, cirrhosis
↑ Na+/H2O absorption at PCT
↓ EABV, ↑ H2O retention
Urine [Na+] < 20 mmol/L
Hereditary: tubular disorders
(Bartter, Gitlemann syndromes).
Thiazide diuretics
Inappropriate: SIADH, hypothyroidism, AI
Normal EABV
Anti-diuresis
Primary polydipsia, eating disorder
↑ H2O or ↓ solute intake
↓ Osmoles
Impaired desalination
Block NCC
↑ H2O retention ↑ Na+/K+ excretion
Hyponatremia
Serum [Na+] < 135 mmol/L
Urine osmolality > 100 mmol/L
Urine osmolality < 100 mmol/L
Cerebral edema, ↑ intracranial pressure, vasoconstriction
If hypovolemic: ↓ JVP, ↓ blood pressure
Lethargy, altered mental status
Abbreviations:
AKI: Acute Kidney Injury
CKD: Chronic Kidney Disease
GFR: Glomerular Filtration Rate
H2O: Water
PCT: Proximal Convoluted Tubule
EABV: Effective Arterial Blood Volume
NCC: Na+/Cl- Co-Transporter
SIADH: Syndrome of Inappropriate ADH Secretion AI: Adrenal Insufficiency
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 11, 2019 on www.thecalgaryguide.com")
Coronary anatomy on ECG- Localizing Ischemia
 of the aortic valve left posterior left CA anterior aortic sinus right CA myocardium right coronary artery posterior descending right atrium ventricle SA AV nodes inferior MI leads II III aVF bradycardia heart blocks problems posterior MI V1 V4 leads anterolateral left main circumflex descending septum ventricle apex anteroseptal occlusion dominant T wave flattening inversion transmural reciprocal depression limb leads precordial leads")
Patent Ductus Arteriosus (PDA)- Pathogenesis and Clinical Findings
- Pathogenesis and Clinical Findings
Sun Bishay Gagnon Adderley Ryznar waechter circulating PGE2 low arterial oxygen content genetic factors char syndrome patent birth aortic pressure pulmonary artery pressure continuous flow from aorta to pulmonary artery via the PDA left to right shunt continuous flow murmur precordial activity S1 S2 accentuated pulse volume load dilation dysfunction left atrium ventricle displaced apex dynamic left ventricular impulse grade pulmonary blood flow systemic blood flow exercise intolerance wide systemic pulse pressure pulmonary artery pressure vascular changes resistance difficulty feeding infants failure to thrive heart failure respiratory distress pulmonary hypertension reversal of shunt adult complications eisenmenger syndrome clubbing cyanosis")
Arterial Insufficiency- Signs and symptoms

Venous insufficiency- Signs and symptoms

Takotsubo Cardiomyopathy- Pathogenesis and clinical findings

Meralgia paresthetica- Pathogenesis and Clinical Findings

Simple Febrile Seizure- Pathogenesis and clinical findings

Reactive Neutrophilia- Pathogenesis and Clinical Findings

Hypoxemia- Pathogenesis and clinical findings

Bronchopulmonary Dysplasia (BPD)- Pathogenesis and clinical findings
- Pathogenesis and clinical findings Adderley Mitchell antenatal post-natal prematurity intrauterine growth restriction genetic predisposition maternal smoking chorioamnionitis pregnancy induced hypertensive disorders post natal mechanical ventilation sepsis O2 toxicity patent ductus arteriosus insult to lungs pro inflammatory cytokines disruption pulmonary vascular alveolar development reduced pulmonary vascular resistance vascular growth and altered vasoreactivity
dysmorphic capillary beds remodelling of pulmonary arteries artery hypertension suboptimal repair abnormal remodelling interstitial fibrosis diffuse haziness interstitial thickening cxr impaired pulmonary gas exchange hypoxia signs of respiratory distress retractions wheezes crackles DLCO airway resistance obstructive lung disease FEV1 separation and alveolar hypoplasia functional alveoli surface area gas exchange")
Neuromuscular Junction (NMJ)- Physiology and pharmacology
- Physiology and pharmacology calcium ion ions voltage gated ca2+ channels acetylcholine ACh receptors nicotinic SNARE protein complex AChR receptor sodium muscle specific kinase action potential voltage gated Ca2+ channels activated release presynaptic terminal binds")
Biliary Atresia (BA)- Pathogenesis and clinical findings
- Pathogenesis and clinical findings Intrauterine environment genetic factors abnormal bile duct development toxic inflammatory response viral immunologic injury to bile duct epithelia pathophysiology poorly understood histology consistent with obstruction on liver biopsy biliary atresia progressive idiopathic fibre-obliterative disease extra-hepatic biliary tree biliary obstruction on intra-operative cholangiogram (diagnostic) partial complete bile duct obstruction delivery of bile acids to small intestine pressure in bile duct absorption of fat and soluble vitamins vitamin K+ deficiency coagulopathy INR PTT bruising petechiae acholic pale stool failure to thrive elimination of bilirubin conjugated direct bilirubin jaundice pruritus excreted urine dark urine diaper yellow pressure bile duct GGT backs up in liver cholestatic hepatitis firm enlarged liver fibrosis cirrhosis ALT AST Horwitz Adderley McKenzie")
Inflammatory-Cascade-Pathogenesis-and-Clinical-Findings
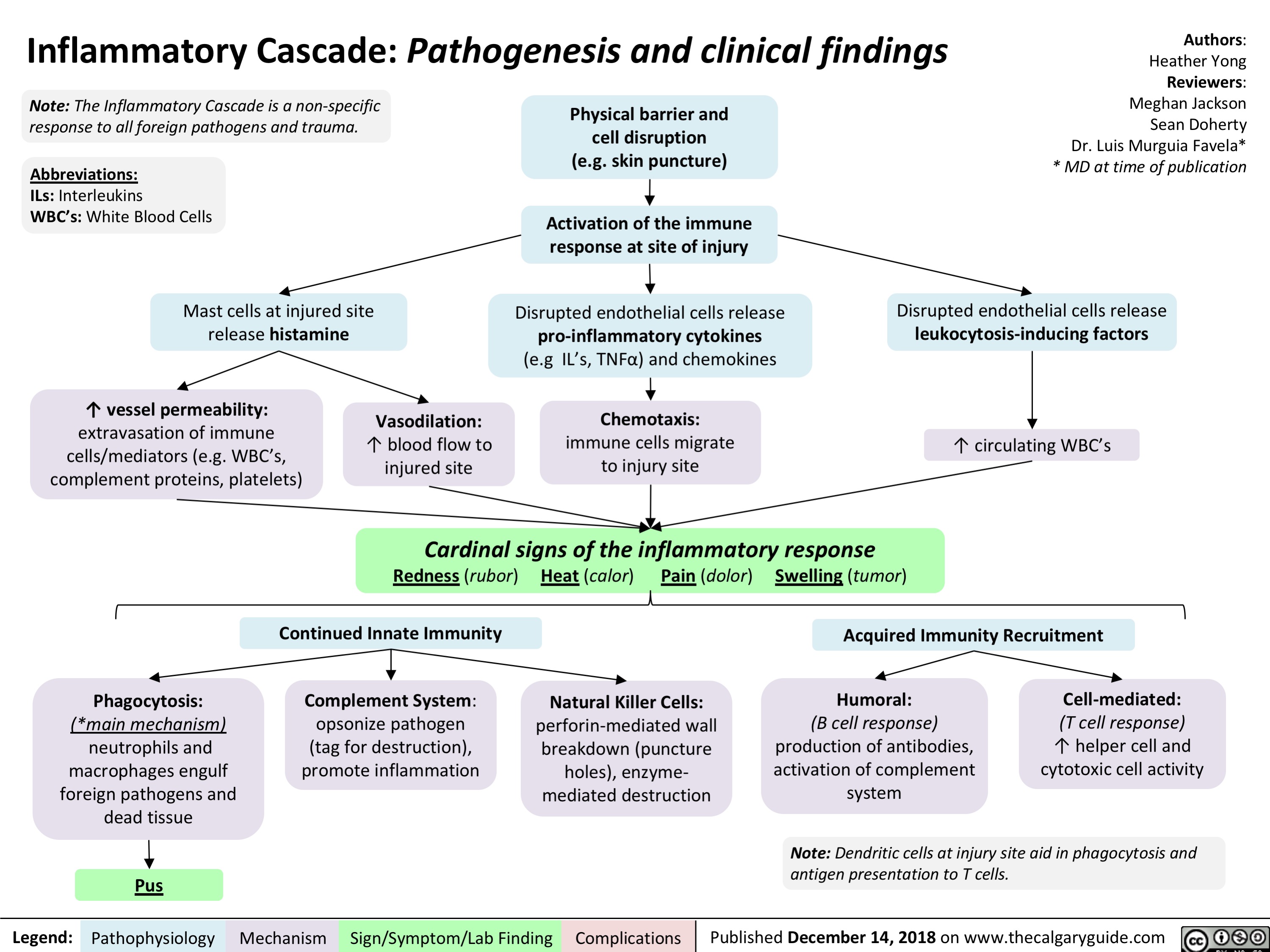
Sepsis, and Septic Shock- Pathogenesis and Clinical Findings

Comorbidities
Immunosuppression or ↑ susceptibility (e.g. splenectomy)
Pathogen virulence
Invasion and host immune avoidance
Vulnerable infection site
↑ likelihood of spread of infection & mortality
Genetics
↑ Sensitivity of innate immune response
Community acquired
Hospital acquired
Infection of host
Innate immune response
Fever, Leukocytosis/ Leukopenia, Left Shift/ Bandemia
Compensatory response
Tachypnea, Altered Level of Consciousness, Hypotension
↓ perfusion and oxygen delivery to organs
Dysregulated Host Response
Pro- and anti-inflammatory response
Life-threatening organ dysfunction caused by a dysregulated host response to infection
The Sequential Organ Failure Assessment (SOFA) or quick
SOFA (qSOFA) Scores may be used to assess mortality risk
Respiratory
↓ PaO2 / FiO2 (mmHg)
Nervous
↓ Level of consciousness
Septic Shock
Cardiovascular
↓ Mean Arterial Pressure
Organ Dysfunction
Liver
↑ Bilirubin
Kidney
↑ Creatinine, Acute oliguria
Coagulation
Thrombocytopenia, ↑ INR or aPTT
Require vasopressors to ↑ mean arterial pressure
Persistent hypotension despite adequate fluid resuscitation
↓ Mean Arterial Pressure (< 65 mmHg), ↑ Lactate (> 2 mmol/L)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 12, 2019 on www.thecalgaryguide.com")
adrenergic-agonists-for-treating-hypotensionlow-blood-pressure
 β1-receptor
activation on
cardiac
myocytes
↑ contractility
α1-receptor
activation on
the smooth
muscle of blood
vessel walls
↑ intra-cellular Ca2+
in these cells, ↑
their contraction
Ephedrine
Direct
effect
Indirect
effect
↑ release of endogenous norepinephrine
from the adrenal medulla (see above)
Mimics epinephrine
(see above)
Primary
Indications:
anaphylaxis,
cardiac arrest
Primary
Indications:
Hypovolemic states
(e.g. blood loss),
Low systemic
vascular resistance
states (e.g. sepsis,
Anesthesia-induced
hypotension)
Primary
Indications:
mainly used in
Anesthesiainduced
hypotension
↑ intracellular
Ca2+ ↑ rate of
myocyte
contraction
Phenylephrine
↑ Cardiac
Output
↑ heart rate
↑ strength
of myocyte
contraction
↑ arterial
wall tone
↑
stroke
volume
Pushes more
blood to flow
back to heart
(↑ preload)
↑ systemic vascular
resistance (SVR)
More blood in
ventricles stretch
myocytes more
optimally for ↑
contractility
(Frank Starling
Law)
↑ venous
wall tone
↑ Blood
Pressure
Nonspecific activation of α and β receptors on other areas of the body
(e.g. on the autonomic nervous system) as well as on cardiac myocytes
Hypertension
Cardiac Dysrythmias: e.g.
palpitations, ventricular fibrillation
Tremors Cardiac
arrest
All four
drugs")
Hyperkalemia- Physiology
![Hyperkalemia: Physiology ↓ Renal Excretion
↑ Intake
↓ Intracellular Shift
Acute and chronic kidney disease; CHF
Principal Cell Dysfunction (TTKG < 7)
ACEi/ARB; AI; heparin
Hypovolemia (TTKG > 7)
↓ EABV
↓ distal flow of Na+ and H2O
Urine [Na+] < 20 mmol/L
Cell lysis
↑ osmolarity H2O efflux
Solvent drag
β2 inhibition α1 stimulation
Digoxin ↓ A
NAGMA ↓ insulin
↓ NHE1 activity
Diabetic nephropathy; NSAIDs
↓ A: ↓ R
K+ sparing diuretics; voltage- dependent RTA
↓ Na+/K+ ATPase activity
↓ GFR
↓ A: ↑ R ↑ A: ↑ R
↓ CCD K+ secretion
↑ K+ availability
↑ K+ release
↓ intracellular K+ influx
Chronic: Desensitize voltage- gated Na+ channels and ↓ membrane excitability
ECG: Peaked T-waves, ↑ PR interval, flat/absent P-wave, ↑ QRS, QRST “sine wave”
Hyperkalemia
Serum [K+] > 5.1 mmol/L
Acute: ↑ extracellular [K+] makes the RMP less (-)
Abbreviations:
A: Aldosterone
AI: Adrenal Insufficiency
CCD: Cortical Collecting Duct
CHF: Congestive Heart Failure
EABV: Effective Arterial Blood Volume H+: Hydrogen ion
K+: Potassium ion
Na+: Sodium ion
NAGMA: Normal Anion Gap Metabolic Acidosis
NSAIDs: Non-steroidal anti-inflammatory drugs Note:
Muscle weakness or paralysis, ↓ urinary acid excretion
R: Renin
RTA: Renal Tubular Acidosis
RMP: Resting Membrane Potential TTKG: Transtubular Potassium Gradient
• Pseudohyperkalemia should always be excluded; can be caused by thrombocytosis, leukocytosis or improper blood withdrawal technique.
Authors: Mannat Dhillon Joshua Low Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 6, 2019 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2019/03/Hyperkalemia-Physiology-.jpg "Hyperkalemia: Physiology ↓ Renal Excretion
↑ Intake
↓ Intracellular Shift
Acute and chronic kidney disease; CHF
Principal Cell Dysfunction (TTKG < 7)
ACEi/ARB; AI; heparin
Hypovolemia (TTKG > 7)
↓ EABV
↓ distal flow of Na+ and H2O
Urine [Na+] < 20 mmol/L
Cell lysis
↑ osmolarity H2O efflux
Solvent drag
β2 inhibition α1 stimulation
Digoxin ↓ A
NAGMA ↓ insulin
↓ NHE1 activity
Diabetic nephropathy; NSAIDs
↓ A: ↓ R
K+ sparing diuretics; voltage- dependent RTA
↓ Na+/K+ ATPase activity
↓ GFR
↓ A: ↑ R ↑ A: ↑ R
↓ CCD K+ secretion
↑ K+ availability
↑ K+ release
↓ intracellular K+ influx
Chronic: Desensitize voltage- gated Na+ channels and ↓ membrane excitability
ECG: Peaked T-waves, ↑ PR interval, flat/absent P-wave, ↑ QRS, QRST “sine wave”
Hyperkalemia
Serum [K+] > 5.1 mmol/L
Acute: ↑ extracellular [K+] makes the RMP less (-)
Abbreviations:
A: Aldosterone
AI: Adrenal Insufficiency
CCD: Cortical Collecting Duct
CHF: Congestive Heart Failure
EABV: Effective Arterial Blood Volume H+: Hydrogen ion
K+: Potassium ion
Na+: Sodium ion
NAGMA: Normal Anion Gap Metabolic Acidosis
NSAIDs: Non-steroidal anti-inflammatory drugs Note:
Muscle weakness or paralysis, ↓ urinary acid excretion
R: Renin
RTA: Renal Tubular Acidosis
RMP: Resting Membrane Potential TTKG: Transtubular Potassium Gradient
• Pseudohyperkalemia should always be excluded; can be caused by thrombocytosis, leukocytosis or improper blood withdrawal technique.
Authors: Mannat Dhillon Joshua Low Reviewers: Andrea Kuczynski Kevin McLaughlin* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 6, 2019 on www.thecalgaryguide.com")
Torsades de Pointes (TdP)- Pathogenesis and Clinical Findings
![Torsades de Pointes (TdP): Pathogenesis and Clinical Findings
Drugs (e.g. Class 1A [quinidine], Class III [sotalol,
amiodarone], TCAs, erythromycin, quinolones, anti-histamines)
Sinus bradycardia, AV block
Metabolic abnormality (hypo K+/Ca2+/Mg2+)
Primary heart disease: ischemic, congestive heart failure, cardiomyopathy
Acquired long QT syndrome
Congenital long QT syndrome
↓ repolarizing current/ depolarizing current in cardiomyocytes
Mutated cardiac ion channels
Author: Nicola Adderley Reviewers: Luke Gagnon Emily Ryznar *Saman Rezazadeh *George Veenhuyzen MD at time of publication*
↓ repolarizing current in cardiomyocytes
QTc interval
Prolonged ventricular action potential duration
Early after depolarization (EAD) triggering PVC
Torsades de Pointes
Illustrated changes to action potential:
Normal cardiac action potential
EAD
Abbreviations: TCAs: tricyclic antidepressants AV: atrioventricular QTc: QT interval, corrected for heart rate
PVC: premature ventricular contraction
VF: ventricular fibrillation
SR: sinus rhythm
Polymorphic ventricular tachycardia initiated by PVC in the setting of QT interval prolongation and maintained by functional re-entry
Non-sustained TdP
Asymptomatic, palpitations, syncope (length-dependent)
Illustrated changes to ECG Strip:
OR
Sinus rhythm restored
Degeneration to VF
Sudden cardiac death
Prolonged repolarization
Triggered beat (PVC)
A
BCDE
A. Prolonged QT interval B. PVC
C. PVC triggers TdP
D. Non-sustained TdP
E. Return to SR
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 10, 2019 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2019/03/Torsades-de-Pointes-TdP-Pathogenesis-and-Clinical-Findings-.jpg "Torsades de Pointes (TdP): Pathogenesis and Clinical Findings
Drugs (e.g. Class 1A [quinidine], Class III [sotalol,
amiodarone], TCAs, erythromycin, quinolones, anti-histamines)
Sinus bradycardia, AV block
Metabolic abnormality (hypo K+/Ca2+/Mg2+)
Primary heart disease: ischemic, congestive heart failure, cardiomyopathy
Acquired long QT syndrome
Congenital long QT syndrome
↓ repolarizing current/ depolarizing current in cardiomyocytes
Mutated cardiac ion channels
Author: Nicola Adderley Reviewers: Luke Gagnon Emily Ryznar *Saman Rezazadeh *George Veenhuyzen MD at time of publication*
↓ repolarizing current in cardiomyocytes
QTc interval
Prolonged ventricular action potential duration
Early after depolarization (EAD) triggering PVC
Torsades de Pointes
Illustrated changes to action potential:
Normal cardiac action potential
EAD
Abbreviations: TCAs: tricyclic antidepressants AV: atrioventricular QTc: QT interval, corrected for heart rate
PVC: premature ventricular contraction
VF: ventricular fibrillation
SR: sinus rhythm
Polymorphic ventricular tachycardia initiated by PVC in the setting of QT interval prolongation and maintained by functional re-entry
Non-sustained TdP
Asymptomatic, palpitations, syncope (length-dependent)
Illustrated changes to ECG Strip:
OR
Sinus rhythm restored
Degeneration to VF
Sudden cardiac death
Prolonged repolarization
Triggered beat (PVC)
A
BCDE
A. Prolonged QT interval B. PVC
C. PVC triggers TdP
D. Non-sustained TdP
E. Return to SR
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 10, 2019 on www.thecalgaryguide.com")
Shoulder Dystocia: Complications

Previous
shoulder
dystocia
Size discrepancy between fetal
shoulders and maternal pelvis
Multiparity
Maternal
diabetes
Inadequate
uterine tone (over
distension of
uterus, prolonged
2nd stage) and
birth canal trauma
from complicated
delivery
**Attempts to
disimpact and/or
deliver a
macrosomic fetus
Traction to head
can lead to
stretching and
tearing of
brachial plexus
nerves
Intentional or
incidental
fracture of the
fetus’:
Dysfunctional
or prolonged
labour and/or
contractions
↓ oxygenation
to fetus
Authors:
Danielle Hubbert
Risk Factors: *Up to 50% have no risk factors = Obstetrical Emergency that is challenging to predict Mark Diaz
Fetal death
Legend: Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications Published March 12, 2019 on www.thecalgaryguide.com
Prolonged
2nd stage of
labour
Maternal
obesity
Operative
vaginal
delivery
Fetal anterior shoulder becomes impacted
against maternal pubis symphysis and
fails to deliver spontaneously with normal efforts
Clavicular fracture
Erbs palsy (C5-6)
Klumpke palsy (C8-T1)
(rarely permanent)
Episiotomy or
3rd-4th degree
perineal tears Postpartum
hemorrhage
Hypoxia/asphyxia (see PPH slide)
Turtle sign – fetal head
retracts tight against
perineum
Uterine
rupture
Antepartum Risks Intrapartum Risks
Cord
Compression
Weakened and
distended
musculature
Fetal Complications Maternal Complications
Clavicle, to
↓ diameter
of shoulders
Humerus, when
sweeping
posterior arm
across chest
Humeral
fracture
Reviewers:
Dalynne Peters
Angela Deane
Ingrid Kristensen*
*MD at time of publication")
Primary Myelofibrosis pathogenesis and clinical findings

within hematopoietic
stem cells
Non-driver mutations in
other myeloid genes
(e.g., LNK, CBL, TET2,
ASXL1, IDH)
Constitutive activation of
cellular proliferation
pathways
↑ cell signaling
↑ gene transcription and
expression
Cellular proliferation and
resistance to apoptosis
Proliferation of abnormal
megakaryocytes
↑ neutrophil engulfment
by megakaryocytes
↑ growth factor release
by megakaryocytes
Stimulation of
fibroblasts
Stimulation of
endothelial cells
New blood vessel formation
↑ osteoprotegerin Unbalanced osteoblast
proliferation Osteosclerosis
Fibrosis of the
bone marrow
Anemia
Bleeding and
bruising
Infections
Fatigue and pallor
Bone pain
Increased cell
turnover
Tumor lysis
syndrome
Cachexia, night sweats,
fever/chills, malaise
Expanding
marrow pushing
against bone
Extramedullary
hematopoiesis Hepatomegaly
Portal
hypertension
Splenomegaly
↑ LDH
Thrombocytosis
Leukocytosis
Secretion of
coagulation
inducing cytokines
Arterial and
venous
thromboembolism
↓ blood cell
production
&
leukoerythroblastosis
Thrombocytopenia
Leukopenia
↑ K+, PO4
2-, uric acid
↓ Ca2+
Bone pain
Periostitis
Immature granulocyte and
erythroid precursors with blasts
↑ cytokine
production
(+)
↑ sequestration of blood cells
Disseminated
intervascular
coagulation
(see MAHA slide)
Definitions:
Periostitis – Inflammation of the
membrane surrounding bone
Osteosclerosis – Abnormal hardening
and increased in density of bone")
Hemorrhoids - Pathogenesis and Clinical Findings

Increased Intra-Abdominal Pressure
I.e. pregnancy, constipation, chronic straining,
lifting, cirrhosis
Hemorrhoids: Pathogenesis and clinical findings
Dilations originate from inferior
hemorrhoidal venous plexus
Vascular cushions engorge
along anal canal
Legend: Published March 30, 2019 on www.Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications thecalgaryguide.com
Authors:
Aleeza Manucot
Reviewers:
Yoyo Chan
Sean Doherty
Dr. Sylvain Coderre*
* MD at time of publication
Supporting tissues of anal cushions weaken,
disintegrate, or deteriorate
Inflammatory reaction
occurs, involving vascular
wall and connective tissue
Thrombosis
Pain
↑ mucus secretions or fecal
soiling of prolapsing
hemorrhoids
Cushion epithelium erodes via
damage from compression
Painless
rectal
bleeding
Bleeding without prolapse
Prolapse with spontaneous
reduction
Prolapse requiring manual
reduction
Irreducible
1st degree
2nd degree
3rd degree
4th degree
Infarction and thrombosis
Acute severe pain
Anal cushions prolapse (downwardly slide)
into rectum or open space
Dentate line: divides
the upper two thirds
and lower third
of the anal canal
EXTERNAL Hemorrhoids
- Found distal to the dentate line
- Somatic innervation
Somatic nerve
receptors activated
Sebaceous glands
↑ secretions around
area of hemorrhoid
Itching Perianal
irritation
Swelling
Inflammation creates
prothrombotic state
Hemorrhoids")
gastroesophageal-reflux-disease-gerd-complications
: Complications
Esophageal stricture
disease
Esophagitis
Esophageal
adenocarcinoma
Barrett’s esophagus
GERD
Reflux of gastric content into distal esophagus
Damage to squamous
esophageal epithelium
Legend: Published March 30, 2019 on www.Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications thecalgaryguide.com
Authors:
Wendy Wang
Reviewers:
Yoyo Chan
Sean Doherty
Dr. Sylvain Coderre*
* MD at time of publication
Squamous esophageal
epithelium undergoes
metaplasia to become
columnar epithelium
This predisposes cells to
premalignant changes
(dysplasia)
Collagen is deposited
where ulcers heal
Asthma/Chronic Cough
Chronic Laryngitis
Laryngeal and
Tracheal Stenosis
Extra-esophageal Complications Esophageal Complications
Airway becomes
irritated
Fibroblasts proliferate
and deposit granulation
tissue in airway
Tissue deposition
leads to narrowing of
laryngeal and
tracheal space
Damage to pharyngeal
lining and airway
Esophageal tissue repeatedly
exposed to stomach acid
Pro-inflammatory cells and cytokines
are recruited to the area
Definitions:
• Metaplasia: abnormal change in the
nature of a tissue
• Pro-inflammatory cells and cytokines:
Mediators of inflammation. Examples
of cells include macrophages and T
cells, cytokines include IL-17, IL-2, IL-4
Over time, collagen fibers
contract
Bronchoconstriction
↑ vagal
tone
↑ bronchial
reactivity
Cough sensory
nerve endings are
stimulated
Vagal reflex
is activated
Activation of
cough center in
brainstem
↑ inflammation of
squamous epithelium
Ulcers form in esophagus")
autosomal-dominant-polycystic-kidney-disease-adpkd
:
Pathogenesis,
Clinical Findings,
and Complications
Author:
Yan Yu*
Reviewers:
David Waldner*
Sean Spence*
Andrew Wade*
* MD at time of
publication
Legend: Published April 14, 2019 on www.Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications thecalgaryguide.com
One theory (mechanism unclear): these mutations in the polycystin
gene result in dysfunctional Ca2+ channels on epithelial cells
PKD1 mutation
(~78%)
Abnormal Ca2+ entry disrupts intracellular Ca2+ signaling
In the Kidney: all segments of the nephron develop cysts: sacs of flattened epithelium
filled with proteinaceous fluid, replacing normal parenchyma with dysfunctional tissue
PKD2 mutation
(~15%)
Expansive cell
proliferation
Low urine
Osmolality
(< 500
mmol/kg)
Abnormally expandable
basement membranes
PKD3 mutation
(rare)
↑ fluid
secretion
95% inherited, autosomal dominant mutations
5% spontaneous mutations
In adults, the same pathophysiology occurs
in epithelial tissue throughout the body
When pH of urine <5.5, uric acid is in
its protonated form & is less soluble
àprecipitates uric acid stones
Nephrolithiasis
Urine accumulates within cysts Cyst growth
Pyelonephritis
Damaged
tubules
leak
proteins
into filtrate
Proteinuria
Flank pain
Inability to
concentrate
urine
Low urine
specific
gravity
(<1.010)
¯ NH3 production,
↑ acidity of renal
tubule (¯ pH)
Activates
nociceptors Cyst hemorrhage
Urine stasis à
precipitation of
CaOxalate stones
within cysts
Multiple Renal Cysts
(bilaterally, in cortex and
medulla, on Ultrasound)
In the Brain:
expansion &
weakening of
cerebral
arterial walls
“Berry
Aneurysms” 9-
12%
(ask about this
on Family Hx!)
In many organs:
epithelial tissue
expansion &
fluid secretion
In the Heart:
abnormal valve
collagen matrix
Valve prolapse
& regurgitation
Liver (90%),
spleen/pancreas
(5-10%), thyroid
(rare) cysts
In seminal vesicles:
Cyst formation disrupts
sperm motility
Infertility
In GI tract: Cyst
formation
Herniations,
diverticuli
Dysfunctional
collecting ducts
Abdominal mass
(enlarged kidneys)
(may be palpable)
Blood leaks into
renal tubules
Hematuria (isomorphic)
Bacteria
accumulate
in the static
urine
Dysfunctional
proximal tubules
Unknown
mechanisms à
¯ urine citrate
àmore urine
Ca2+ binds to
oxalate than to
citrate à↑ Ca-
Oxalate stones
Note: PKD1 mutations have
more severe prognosis than
PKD2 mutations (earlier
disease onset, larger cysts)
Vessels
tear
more
easily
Stretches
renal
capsule
Cysts compress renal vasculature
¯ Glomerular perfusion
To ↑ perfusion à
kidneys activate RAAS
Hypertension")
Rickets and Osteomalacia: Pathogenesis and Clinical Findings

Shear forces
bend the
osteopenic
bone
Short stature
Diffuse skeletal pain
(bone tenderness)
Osteopenia
reduces bone
density and
cause fractures
with minimal
force applied
If hypophosphatemic,
production of ATP and
other high energy
molecules declines
Unequally
distributed
forces and
muscle/tendon
tension
stimulate
nociceptors
Legend: Published November 26, 2012 on www.Pathophysiology Mechanism Sign/Symptom/Lab Finding Complications thecalgaryguide.com
Calcification inhibitors
(excess exposure to Al,
Fluoride, etidronate)
Lack, or reduced
function, of
mineralization
enzymes (like ALP)
Lack of bone mineral components:
1. Phosphate: renal tubule disorders, vit D
or Phosphate deficiency, ↑FGF23
2. Calcium: severe deficiency (infants)
Rickets: Occurs before
epiphyseal closure
Epiphyseal
plates do not
fuse, impairing
bone growth
Bowed legs
Cartilage in epiphyseal
plates cannot become
ossified
Disruption in
calcium ion
homeostasis
↓ GI
absorption of
Ca2+ into
blood
↓ Kidney
reabsorption
of Ca2+ into
blood
↓ energy available
to muscle
Author:
Payam Pournazari
Reviewers:
Yan Yu
Spencer Montgomery
David Hanley*
* MD at time of
publication")
Polyarteritis Nodosa (PAN): Pathogenesis and Clinical Findings
: Pathogenesis and clinical findings
Environmental triggers
Infectious/viral agents (commonly Hepatitis B)
Medical Comorbidities Malignancies (most commonly hairy-cell leukemia)
Immunogenetic Predisposition: patient is genetically predisposed to a dysregulated immune response
Fever
↑ ESR and CRP
Postulate 1
Viral antigen-antibody complexes deposit in vasculature, causing lesions and activating cellular inflammatory response
Authors: Nela Cosic, Yan Yu* Reviewers: Sean Doherty Martin Atkinson*
* MD at time of publication
Palpable or necrotic purpura
Malignant Hypertension
Renal Insufficiency
Myocardial ischemia
Heart failure Diffuse myalgias
Postulate 2
Viral replication causes direct injury to vascular endothelial cells
↑ Anti- endothelial cell autoantibodies (AECA)
Altered cytokine profile (↑TNF-α, IL-1β, IFN-α, IL- 2)à↑ T-cell mediated immune response
Weight metabolism Loss
Autoimmune attack on various areas of the body
Malaise and/or Arthralgias (knees, ankles, elbows, wrists)
Orchitis: Testicular pain, erythema and/or swelling
Small intestine perforation GI Manifestations
Non-specific abdo pain
GI hemorrhage
Peripheral sensory changes: Distal mononeuropathy
multiplex
Polyarteritis Nodosa (PAN)
Focal segmental necrotizing leukocytoclastic vasculitis of medium or small-sized arteries
Inflammation of arteries damages the vascular endothelium of those arteries
Inflammation predisposes formation of arterial thromboses
Blockage of arteriesà tissue ischemia and possible necrosis (tissue cell death)
↑ basal
Arterial aneurysms
Inflamed subcutaneous arteries
Inflamed renal artery
àluminal narrowing and reduced blood flow to kidneys
Inflamed coronary artery à luminal narrowing, occlusion, thromboses
Segmental inflammation of muscular arteries, stimulating surrounding nociceptors. Muscle ischemia develops long-term.
Ischemia/necrosis of the testicles
Ischemia/necrosis of the small intestine
Ischemic vasculitic nerve damage: Immune complex deposition within vessel walls of arteries traveling with nerves leads to persistent vascular inflammation and ischemia of associated nerve
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 18, 2019 on www.thecalgaryguide.com")
dermatomyositis-dm-and-polymyositis-pm-pathogenesis-and-clinical-findings
 and Polymyositis (PM):
Authors: Merna Adly, Yan Yu* Reviewers: Nela Cosic Sean Doherty Martin Atkinson* * MD at time of publication
Pathogenesis and clinical findings
Immunogenetic and Cellular Predisposition
Genetic polymorphisms cause dysregulated immune response, cytokine profile, and protein expression in muscle cells
Demographics
F:M, 2:1
Bimodal age distribution:
- Juvenile: 7 years of age (mean) - Adult: 52 years of age (mean)
Malignancy
Tumor cells increase systemic inflammatory response, leading to increase of autoantigens associated with DM
↑ in DM-associated autoantibodies
(Ex. Anti-Mi-2/ Anti-Jo-1) Autoantibodies bind to DNA or RNA in muscles,
provoking a systemic inflammatory response
↑ chemokine and cytokine release in endothelial vasculature of muscles
Perivascular Capillary necrosis inflammation
Lack of blood supply to the myofibers causes endofascicular hypoperfusion and muscle ischemia
Muscle tissue damage:
Inflammatory infiltrates destroy cellular components of muscle (endoplasmic reticular, myofiber, and keratinocytes)
Environmental triggers
Infectious agents (ex. Picornavirus) or drugs (ex. statins) provoke immune response
Elevated Antinuclear Antibodies
Anti-Jo-1 Anti-OJ Anti-Mi2 Anti-SRP Anti-EJ Anti-PL12 Anti-PL7
These processes occur in the skin on the dorsum of the hands, forming hyperkeratotic flat red papules
These processes occur in the upper & lower eyelids, causing red-purple discoloration +/- swelling
Perifascicular atrophy
(Observed on histology)
Weaker GI tract musculature Weaker pulmonary musculature Weaker cardiac musculature
Dermatomyositis only:
Gottron Papules Heliotrope Rash
Damaged muscle cells release their internal cellular enzymes into the bloodstream
Elevation of muscle enzyme levels in serum:
Creatinine kinase (CK), lactate dehydrogenase (LD), aldolase, aspartate aminotransferase (AST), and alanine aminotransferase (ALT)
Muscle Biopsy Findings Muscle necrosis, fiber regeneration, diffuse CD8+ T lymphocytes infiltrates
Bilateral Muscle Weakness Subacute development, primarily deltoids and hip flexors affected
Dysphagia
Aspiration, respiratory compromise
Atrioventricular defects, tachyarrhythmias, dilated cardiomyopathy
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 18, 2019 on www.thecalgaryguide.com")
DiGeorge Syndrome: Pathogenesis and Clinical Findings
, though their role is less well understood.
Abbreviations:
• PA-VSD – pulmonary atresia
with ventricular septal defect
• TBX1 – T-box Protein 1
• VSD – ventricular septal defect
Heterozygous deletion at chromosomal region 22q11.2
The region’s main gene product, TBX1*, exhibits haploinsufficiency: even a heterozygote for this gene product, producing half the normal quantities of TBX1, is insufficient to produce a normal phenotype
Abnormal pharyngeal arch development
Hypoplastic / aplastic thymus ↓ T cells
(lymphopenia)
Craniofacial malformations (e.g. tracheomalacia, horizontal Eustachian tubes, cleft palate)
Impaired ear and sinus drainage
Abnormal conotruncus development
Heart defects
(e.g. interrupted aortic arch, tetralogy of Fallot, PA-VSD/VSD, truncus arteriosus)
Hypoplastic parathyroid glands
Hypocalcemia Seizures
(usually neonatal onset)
Memory Aid:
CATCH-22
Cyanotic congenital heart disease
Abnormal facies
Thymic hypoplasia Cognitive impairment Hypoparathyroidism, hypocalcemia
22q11.2 deletion
Abnormal T cell regulation
and development
Compromised cytotoxic T cells
Susceptibility to intracellular pathogens
Compromised helper T cells
↓ communication with memory B cells
↓immunoglobulins
(progressive hypogammaglobulinemia)
Susceptibility to extracellular pathogens
Autoimmunity and Atopy
Note: There is phenotypic variability in DiGeorge Syndrome. Other features include: thin upper lip, upslanted palpebral fissures, prominent nose, low-set ears, small mouth, hearing impairment, long tapered fingers, scoliosis, vertebral malformations, learning disabilities, and failure to thrive.
Viral Infections
Bacterial Infections
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 21, 2019 on www.thecalgaryguide.com")
Molluscum Contagiosum: Pathogenesis and Clinical Findings
:
• MCV I *more prevalent than other
subtypes except in
immunocompromised individuals
• MCVII
• MCV III
• MCVIV
Abbreviations:
- MCV: Molluscum contagiosum virus - NF-KB: nuclear factor kappa-light- chain-enhancer of activated B cells
(a transcription factor regulating genes responsible for innate & adaptive immune responses)
Sexually active adults: abdomen, genitals, inner thighs Children: face, trunk, limbs
Immunosuppression
Active Atopic Dermatitis Hot, humid climates Crowded living conditions
Risk factors for infection
Direct skin-to-skin contact with infected host Contact with contaminated objects
Molluscipox virus infection
of epidermal keratinocytes
Virus replicates in cytoplasm of epithelial cells
Cytoplasmic inclusion bodies form, multiply & push nucleus to edge of cell
Rupture and discharge of virus-packed inclusion bodies
MCV-released proteins inhibit NF-KB activation
Suppress host immune response to infection
Single or multiple, 2-6 mm, pearly white, discrete papules with central umbilication containing white, waxy curd-like core appearing on any cutaneous surface
Papule contains caseous plug
Squeezing the papule produces white cheesy fluid
Transmission of MCV to conjunctiva of eye
Scratching or removing lesions by curettage and cautery
Staphylococcus aureus infects lesion
Neutrophils & macrophages phagocytose bacteria
Immunosuppression
Impaired T-cell immunity fails to defend against MCV infection
Conjunctivitis
Scarring
Abscess
Widespread lesions
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 21, 2019 on www.thecalgaryguide.com")
acute-somatic-pain
 Thermal (eg: hot stove) Chemical (eg: inflammation)
Nociceptors activated at site of injury (1st order sensory neurons)
Nociceptive fibres (A∂ and C) carry noxious sensory information to the ipsilateral dorsal horn of the spinal cord
Excitatory neurotransmitters are released and stimulate 2nd order sensory neurons
2nd order sensory neurons immediately cross the midline of the spinal cord, and ascend up the opposite side’s anterolateral (aka spinothalamic) tracts, terminating in various locations:
Authors: Lisa Murphy Yan Yu* Reviewers: Mackenzie Gault Melinda Davis* * MD at time of publication
Nociceptors: neurons that detect noxious or painful stimuli and carry this information to the spinal cord. There are two major types:
A∂ fibres: myelinated, initial “sharp, fast” feeling
C fibres: unmyelinated, delayed, “dull, burning” feeling
To hypothalamus
2nd order neuron synapses in the hypothalamus
Hypothalamic neurons coordinate the body’s visceral response to pain
2
nd
To thalamus
order neuron terminates in thalamus
To brainstem
2nd order neuron synapses in brainstem’s reticular formation
To midbrain
2nd order neuron synapses in periaqueductal gray area (PGA) in the midbrain
In the thalamus, 2nd order sensory neurons synapse with 3rd order sensory neurons, which carry the signal to the cerebral cortex
Stimulates descending pathways to modulate the incoming pain signal
Decreased or increased perception of pain
Pain localization and sensation
Emotional and behavioural response
↑ Heart Rate
Nausea
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 25, 2019 on www.thecalgaryguide.com")
Small Bowel Infarction
 versus the colon’s dual blood supply (SMA and IMA)
• With decreased perfusion colonic tissue tends to suffer from ischemia rather than more serious infarction
• Colonic ischemia presents with pain, diarrhea, and rectal bleeding
Abbreviations
• SMA - Superior mesenteric
artery
• IMA - Inferior mesenteric artery
Atrial fibrillation
Blood stasis in left atria of heart more
prone to coagulation
Embolism occluding SMA
Hypertension, dyslipidemia, smoking, diabetes, + family hx
Atherosclerosis (of SMA)
Thrombosis in the superior mesenteric artery
↓ Arterial perfusion of the small intestine (↓ O2 delivery to bowel tissue)
Ischemia of bowels Infarction of bowels
Venous trauma
↓ blood flow and endothelial injury
hypercoagulable state
Mesenteric venous thrombosis, backing up arterial blood
Food in the
intestine ↑ demand for blood in gut
Death of cells under visceral peritoneum stimulates autonomic nerves
Post-prandial abdominal pain
Severe central abdominal pain
Small bowel infarction from
SMA occlusion is commonly pain progressive, and out of proportion with the patient’s physical exam findings
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 15, 2019 on www.thecalgaryguide.com")
Crohn's Disease

Inflammation of the GI tract lining
- Inflammation is “transmural”, spanning the entire thickness of the intestinal wall from luminal mucosa to the serosa.
- The inflammation occurs anywhere in the GI tract from the oral mucosa to the anal mucosa (from ‘gums to bum’) in skip lesion pattern.
Atrophy, scarring of the intestinal villi
Inflammatory cytokines destroy the mucosa epithelial cells of the GI tract wall, causing cell apoptosis and ulceration
↑ permeability of the blood vessels supplying the GI tract wall
Chronic inflammation impairs healing responses
Dysregulated wound healingàexcess
extracellular matrix deposition
Fibrosis leads to scar tissue and thickening of all layers of the GI tract
Strictures
Inflammation is systemic, affecting:
Joints Arthropathy Erythema
Impaired absorption of nutrients
Weight loss
Prolonged GI bleeding
Anemia
Transporter proteins responsible for Na+ reabsorption gradually disappear from the epithelium
More sodium (and thus water) is
retained in the GI tract lumen
Microperforations can penetrate through the intestinal wall
Anal fistulae (“holes” connecting the anus to the skin, bladder, peritoneum, small bowel, etc.)
Continued inflammation and/or infection can lead to:
Leakage of fluid out of capillaries into the GI tract
Luminal edema and swelling
Narrowing of GI lumenàbowel obstruction
Skin
Mouth Eyes
Liver
nodosum, pyoderma gangreno- sum
>5 canker sores
Uveitis
Iritis, scleritis
Sclerosing cholangitis
↓ fat absorption
Fatty acids (negatively charged) bind Ca2+, freeing oxalate from Ca2+
↑ oxalate absorbed into blood & filtered by kidney
Calcium oxalate kidney stones
Diarrhea
Abdominal cramping and pain
(see Bowel Obstruction page for full mechanism
Anal abscesses Inflammatory masses
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 15, 2019 on www.thecalgaryguide.com")
Hemophilia
 accounts for approx. 15% of cases
• Factor levels below 1% of normal constitutes severe disease, 1-5% moderate disease, and 5-40% mild disease
• The more severe the disease, the greater the odds of “spontaneous” bleeds occurring
Genetic defect on the X chromosome affecting the factor VIII or factor IX gene
Deficiency of functional factor VIII (Hemophilia A) or factor IX (Hemophilia B) in blood
Insufficient clotting action when faced with a bleeding challenge
Factor VIII/IX deficiency slows intrinsic clotting pathway
Factor VIII/IX not part of extrinsic clotting pathway
↑PTT Normal PT
Uncontrolled bleeding Occurs across entire body
Hemarthrosis (bleeding in joints) Intramuscular hematoma
Dental bleeds
Intracranial hemorrhage
GI/GU bleeds, etc.
Chronic hemophilia arthropathies
(main contributor to disability and reduced QoL)
In severe patients, repeated joint bleeds common
Recurrent bleeding into joints damages cartilage
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 15, 2019 on www.thecalgaryguide.com")
Signs and Symptoms of Pulmonary Embolism

Deep Vein Thrombosis – popliteal, femoral, iliac veins Clot migrates to IVCàright atrium of heartàright
ventricleàpulmonary vasculature
Large clots (saddle emboli) are lodged in pulmonary arteries
Small clots are lodged in pulmonary arterioles
Saddle embolus (pulmonary artery obstruction)
Back-up of blood into right heart
Right heart strain
↓ CO2 delivery to the lungs for exhalation
Less CO2 exhaled, CO2 builds up in the blood, triggers medullary chemoreceptors to ↑ respiratory rate
Well-ventilated (V) areas of lung do not receive adequate blood supply (Q); vice versa
V/Q mismatch
On V/Q scan
Signals brain to ↑ heart rate
Ischemic tissue becomes inflamed and adheres to pleura
Pleural friction rub
Sandpaper-like sound heard on auscultation
Pleuritic chest pain
Focal, localized chest pain that occurs with each breath
Clot ↓ pulmonary arterial/arteriolar blood flow
↓ delivery of deoxygenated blood to alveoli for oxygenation
Low O2 in blood (↓ O2 saturation) is detected by aortic/carotid chemoreceptors
Signals brain to ↑ respiratory rate
If circulation to lung periphery is cut off, sub-pleural lung tissue can become ischemic and infarct
Irritation of somatic sensory nerve endings on the parietal pleural membrane
Pain stimulates adrenergic response
Tachycardia
Dyspnea/shortness of breath (SOB)
Most sensitive indicator of PE, but not very specific
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 15, 2019 on www.thecalgaryguide.com")
Hemolytic Anemia - Pathophysiology
 may result in slightly macrocytic anemia (because reticulocytes have larger volumes than RBCs)
Defects in the RBC’s environment
Defects in RBC membranes
Ex. Hereditary Spherocytosis:
mutation causing deficiency of RBC structural proteins like ankyrin or spectrin
RBC membranes become weakened and form blebs that break off
↓ RBC surface area while volume remains constantà RBC becomes spherical
Spherocytes in spleen trapped and phagocytosed by splenic macrophages (extravascular hemolysis)
Defects in RBC internal contents (thalassemia, hemoglobinopathies, and metabolic defects)
Ex. Sickle Cell Disease: point mutation in hemoglobin (Hgb) structure (GluàVal)
Inappropriate Hgb polymerization in low oxygen environments due to mutationàRBC becomes rigid, forms a sickle shape
Inflexible RBCs become trapped in the spleen’s sinusoid membranes àphagocytosed by splenic macrophages (extravascular hemolysis)
Infection triggers immune system activation
Autoimmune processes
TTP/HUS (abnormal platelet aggregation blocking blood vessels)
Production of abnormal
antibodies and immune complexes targeted against RBC surface antigens
Immunoglobulin-bound RBCs are marked for
destruction by the immune system (by either the cell- mediated or complement- mediated pathways)
DIC (fibrin deposition blocking blood vessels)
Artificial heart valve
RBCs are sheared when they flow past an abnormal surface
Rate of hemolytic RBC destruction > rate of bone marrow RBC synthesis (reticulocytosis)
↓ total number of RBCs in the body (despite normal RBC production/volume)
Normocytic anemia
Authors: Yan Yu Katie Lin Man-Chiu Poon* Reviewers: Andrew Brack Julia Heighton JoyAnne Krupa Lynn Savoie* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 15, 2019 on www.thecalgaryguide.com")
Wilson's Disease

Hepatic Cu accumulation, deposition in hepatocyte lysosomes
Hepatocyte injury (speculated mechanism: free radicals)
Cu leak from damaged hepatocytes
Epidemiology:
• Autosomal Recessive condition with prevalence of 1:30,000 • 60% of cases present initially with neurologic Symptoms
• Fulminant cases present with acute liver failure and massive
hemolysis, treated with liver transplant
↓ ceruloplasmin release ↓ serum ceruloplasmin
Early asymptomatic liver dysfunction
Cu movement into bloodstream
Cu deposition in vulnerable tissues
Abbreviations:
• Cu - Copper
• AST - Aspartate Aminotransferase • ALT - Alanine Aminotransferase
↑ AST, ALT, and Bilirubin
↑ Serum free Cu (total usually low due to low ceruloplasmin)
Eyes: Kayser-Fleischer rings
CNS: Neurologic disease, Psychiatric disease MSK: Arthropathies
Kidney: Fanconi syndrome, Kidney stones
Chronic hepatitis, Cirrhosis with hepatic insufficiency, Portal hypertension, Hemolysis, Acute Liver Failure
Continued hepatocyte injuryà progressive liver damage
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 17, 2019 on www.thecalgaryguide.com")
chronic-myeloid-leukemia
: Pathogenesis and Clinical Presentation
Translocation of a Chr 9 segment onto Chr 22, creating a Philadelphia chromosome (Chr 22) containing the BCR-ABL1 fusion gene
Mutations from ionizing radiation
Other genetic abnormalities
Authors: Yan Yu Katie Lin Reviewers: Jennifer Au Crystal Liu Danielle Chang Lynn Savoie* *Indicates faculty member at time of initial publication
These genetic abnormalities accumulate in the earliest cell of the blood cell differentiation sequence: the pluripotent hematopoietic stem cell
Hematopoietic stem cell division in the bone marrow becomes unregulated
1. Chronic Stage (85% of clinical presentation): Hematopoietic stem cell division/differentiation in the bone marrow results in ↑ production of multiple blood cell lines (detectable on CBC, but patients are usually asymptomatic at this stage)
Acquired ↑ genetic abnormalities
2. Accelerated Stage
More and more immature precursor cells (”blasts”) divide and accumulate in bone marrow (where 10-19% of blood cells are “blasts”.) Blasts start to spill over into the peripheral blood
Acquired ↑ genetic abnormalities
3. Blast crisis (transformation into AML/ALL)
Neoplastic blast cells have filled up the bone marrow (where >20% of blood cells are blasts). More blasts spill out into the peripheral blood.
Multifactorial causes, most Weight loss, malaise, fever/
with unclear mechanisms
Neoplastic division of platelet precursor cells
Neoplastic division of WBC precursor cells, especially neutrophil precursors
Dividing “blasts” limit the space and resources available for RBC synthesis
chills, night sweats Thrombocytosis
Leukocytosis:
· Neutrophilia, basophilia, & eosinophilia
· “Left shift”: ↑ neutrophil & band production
· Disorderly WBC differential: i.e. “myelocyte bulge”
Trapping of WBC’s in the spleen enlarges the spleen
Splenomegaly:
· Left upper quadrant pain · Early satiety (large spleen compresses the stomach)
· Associated hepatomegaly (if spleen is overfilled & WBCs spill over into liver)
Anemia
↓ oxygenation of blood means blood is less red & body tries to compensate
Pallor Dyspnea Tachycardia
High turnover of these cancerous cells → excess cell lysis
Release of intracellular contents (uric acid, K+, LDH) into plasma
· Hyperkalemia · High (LDH)
Hyperuricemia
Gout
Acute Kidney Injury
Expanding marrow pushing on bone
Bone marrow expands into sternum
Bone pain
Sternal tenderness
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 15, 2019 on www.thecalgaryguide.com")
Secondary Polycythemia

Poor lung function
Renal artery stenosis
↓ blood flow to kidney
Kidney senses ↓ O2
High affinity Hb or CO poisoning
Hb does not easily unload O2
Tissues become hypoxic
Tumors (e.g. renal, hepatic, lung)
Secretes EPO in an unregulated way, as a “paraneoplastic syndrome”
High altitude
Obstructive sleep apnea
Episodic airway obstruction during sleep
Intermittent hypoxia
Cyanotic heart disease
Shunting of blood
Venous and arterial blood mixes
Poorly oxygenated blood
↓ O2 partial pressure
↑ EPO production independent of O2 (inappropriate response)
↑ EPO production due to hypoxia (appropriate response)
Abbreviations:
• Hb- Hemoglobin
• EPO- Erythropoietin • ILD- Interstitial Lung
Disease
• COPD- Chronic
Obstructive Pulmonary Disease
“Endogenous causes” of high EPO
Secondary Polycythemia
“Exogenous causes” of high EPO
Testosterone therapy Iatrogenic EPO (results in ↑ EPO synthesis administration
within the body)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published May 5, 2019 on www.thecalgaryguide.com")
Acute Lymphoblastic Leukemia
![Acute Lymphoblastic Leukemia (ALL): Pathogenesis and Clinical Presentation
Authors: Yan Yu, Katie Lin Reviewers: Crystal Liu, Kara Hawker, Jennifer Au, Lynn Savoie* * MD at time of initial publication
Note: ALL is much rarer than AML and is usually seen in children
Accumulation of genetic abnormalities in immature lymphoid precursor cells (B/T cell precursors)
Neoplastic lymphoid precursor cells (“blasts”) divide and accumulate in bone marrow
Abundance of blasts displaces other blood precursors from marrow, inhibiting their development/differentiati on
After neoplastic blasts fill up bone marrow, they spill out into blood
High turnover of these cancerous cells
Multifactorial causes, most with unclear mechanisms
Expanding marrow pushing on bone
Pancytopenia on CBC
20% of marrow is blasts (on bone marrow aspirate and/or biopsy)
Neoplastic blasts continue to divide and accumulate in lymph
nodes and spleen (can occur, but not that common)
Blasts detected as white blood cells on CBC
High rate of cell lysis
Weight loss, malaise, fever/chills, night sweats
Bone pain (worse than that felt in AML, especially in children)
↓ in neutrophils
↓ in RBCs
↓ in platelets, reduced blood clotting ability
Lymphadenopathy Splenomegaly
May cause leukocytosis, despite pancytopenia
Release of intracellular contents (uric acid, K+, LDH) into plasma
Greater chances of infection
Anemia
Fatigue, shortness of breath, pallor
Easy bruising and petechiae on skin
Hyperuricemia Hyperkalemia High [LDH]
Tumor lysis syndrome
Acute kidney injury
Gout
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published May 5, 2019 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/Acute-Lymphoblastic-Leukemia.jpg "Acute Lymphoblastic Leukemia (ALL): Pathogenesis and Clinical Presentation
Authors: Yan Yu, Katie Lin Reviewers: Crystal Liu, Kara Hawker, Jennifer Au, Lynn Savoie* * MD at time of initial publication
Note: ALL is much rarer than AML and is usually seen in children
Accumulation of genetic abnormalities in immature lymphoid precursor cells (B/T cell precursors)
Neoplastic lymphoid precursor cells (“blasts”) divide and accumulate in bone marrow
Abundance of blasts displaces other blood precursors from marrow, inhibiting their development/differentiati on
After neoplastic blasts fill up bone marrow, they spill out into blood
High turnover of these cancerous cells
Multifactorial causes, most with unclear mechanisms
Expanding marrow pushing on bone
Pancytopenia on CBC
20% of marrow is blasts (on bone marrow aspirate and/or biopsy)
Neoplastic blasts continue to divide and accumulate in lymph
nodes and spleen (can occur, but not that common)
Blasts detected as white blood cells on CBC
High rate of cell lysis
Weight loss, malaise, fever/chills, night sweats
Bone pain (worse than that felt in AML, especially in children)
↓ in neutrophils
↓ in RBCs
↓ in platelets, reduced blood clotting ability
Lymphadenopathy Splenomegaly
May cause leukocytosis, despite pancytopenia
Release of intracellular contents (uric acid, K+, LDH) into plasma
Greater chances of infection
Anemia
Fatigue, shortness of breath, pallor
Easy bruising and petechiae on skin
Hyperuricemia Hyperkalemia High [LDH]
Tumor lysis syndrome
Acute kidney injury
Gout
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published May 5, 2019 on www.thecalgaryguide.com")
Ulcerative Colitis

Immune response against the GI tract. (Unclear mechanism, but thought to be mediated by cytokine release and neutrophil infiltration)
Inflammation of the GI tract epithelial lining
- Starting at the rectum and moves up the colon and is continuous (does not invade the small intestine)
- Inflammation affects the mucosal and submucosal only
Diarrhea, abdo pain and cramping causing avoidance of food
Weight loss
Apoptosis of GI tract mucosa
Transporter proteins responsible for Na+ reabsorption gradually disappear from the epithelium
Ulceration, into the anus, and more severe
Prolonged Bleeding - GI and anus
Anemia, often iron deficiency
Inflammation ↑ permeability of the blood vessels supplying the GI tract wall
Fluid leak out of capillaries into GI tract wall, causes edema and swelling
Swelling narrows the GI tract lumen, causing bowel obstruction
Inflammation, ulceration, or infection at the anus (all involve the RECTUM!)
Anal irritation stimulates autonomic and somatic nerves leading up to the brain, causing the pt to want to defecate
Tenesmus, urgency, frequency (feeling or urgency to defecate, but little stool is produced)
Joints Skin
Arthroplasty/ joint pain
Erythema nodosum, pyoderma gangrenosum
Mouth >5 canker sores
More sodium (and thus water) is retained in the GI tract lumen
Bloody Diarrhea, usually bloody due to anal bleeding and ulceration bleeding
Abdominal Cramping and pain (see Bowel Obstruction page for full mechanism)
Eyes (uvea, iris, sclera)
Liver Blood
Uveitis
Iritis, scleritis
Sclerosing Cholangitis
Autoimmune hemolytic anemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published May 5, 2019 on www.thecalgaryguide.com")
HBV Serology

Anti-HBcAg IgM acute/recent infection
Anti-HBcAg IgG chronic/remote infection
(Due to vaccination or past exposure)
Marker of active viral disease and patient infectiousness
Detected in chronically infected patients or patients who have cleared infection
Never infected, never immunized
-
-
-
-
-
-
Chronic infection/carrier
+
+/-
+
-
+/-
+/-
Acute infection
+
+
-
-
+
-
Natural immunity (past infection)
-
-
+
+
-
+/-
Immunized
-
-
-
+
-
-
Historical Notes:
• HBeAg was previously used as a marker of viral replication
• Presence of Anti-HBeAg antibodies indicates that the antigen has been
cleared, representing seroconversion and a halt to viral replication
• HBV DNA is the current clinical marker of viral replication, and can be
used to assess viral load in the body
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published May 5, 2019 on www.thecalgaryguide.com")
Chronic Lymphocytic Leukemia

Clonal division of neoplastic B lymphocytes within lymph nodes
With continued cell division, B- cells spill over into the peripheral blood
Neoplastic B cells fail to die and continue to divide within lymph nodes over time
Neoplastic B cell precursors infiltrate the spleen and the bone marrow
A small % of CLL patients undergo Richter’s transformation, in which their disease evolves into Diffuse Large B-cell Lymphoma
Notes:
• CLL is the most common adult leukemia in developed nations.
• Prevalence of CLL ↑ with age, occurring most often in older people
Slow process of neoplastic cell division
Patients are most commonly asymptomatic at initial presentation
Multifactorial causes, most Weight loss, malaise, fever/chills, night
with unclear mechanisms
B-cell are detected as lymphocytes on a CBC
Lack of functional B cells ↓ body’s ability to produce antibodies for immune response
Neoplastic cells accumulate in lymph nodes
sweats
Lymphocytosis (B cell count >5x109/L for at least 3 months)
Hypogammaglobulinemia
Lymphadenopathy
↑ risk for infection, especially by encapsulated bacteria normally killed by antibodies
Hypercellular bone marrow (on bone narrow biopsy)
Splenomegaly
↑ sequestration of platelets and RBCs
↓ in RBCs ↓ in
platelets
Anemia
Thrombocytopenia (reduced blood clotting ability)
Fatigue, shortness of breath
Easy bleeding, easy bruising, petechiae
Abundance of B-cell precursors in marrow inhibits the development/differentiation of other cell types
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 30, 2019 on www.thecalgaryguide.com")
perforated-viscous
:
Author:
Yan Yu
Reviewers:
Michael Blomfield, Tony Gu, Dean Percy, Danny Guo Maitreyi Ramran* * MD at initial time of publication
Chest X-Ray (CXR)
Pathogenesis and Clinical Findings
Diverticulitis
Crohn’s disease Peptic ulcer (H. pylori
infection, NSAID use, ICU stress, etc)
Appendicitis
Malignant neoplasm
Irritates visceral peritoneum, stimulates autonomic nerves
Severe inflammation causes destruction of GI tract mucosa
Over time, Perforation of the GI tract wall
Bowel contents (air, fluids) released into peritoneal cavity
Massive peritoneal inflammation
Diagnostic investigations if a GI perforation is suspected
Dull diffuse abdominal pain
Severe, Sharp abdominal pain with peritoneal signs
Abdominal X-ray
Irritation of parietal peritoneum, stimulates somatic nerves
• Abdominal X-ray
• Intra-peritoneal air will coat the GI tract surfaces, giving them a faint white outline
under X-ray
• Chest X-ray of upright patient (Diagnostic)
• Intra-peritoneal air will rise above the peritoneal fluid when pt is upright, accumulating under the right hemi-diaphragm.
• Note: air under left hemi-diaphragm = normal gastric bubble
• CT? Most patients with suspected GI perforation will get a CT scan, but this is not the diagnostic gold standard (and access to CT can be limited, especially in rural settings)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published June 30, 2019 on www.thecalgaryguide.com")
acanthosis-nigricans-pathogenesis-and-clinical-findings

HELLP syndrome pathogenesis and clinical findings

Abnormal maternal immune tolerance of placentation in early pregnancy
Polymorphisms of FasL and receptor gene
↑levels of placental FasL in maternal circulation
Lesions in membrane separating maternal and fetal circulation
Release of inflammatory products from placenta into maternal circulation
Systemic maternal inflammatory response (activation of coagulation and complement pathways)
Microvascular endothelial activation, dysfunction, and damage
Widespread platelet aggregation and agglutination ↓ amount of platelets measurable on complete blood count
Low platelets
HELLP Syndrome
RBCs are sheared as they flow through damaged vessels
Microangiopathic hemolytic anemia (MAHA)
Lab findings indicative of hemolysis: normocytic anemia, high LDH & bilirubin, low haptoglobin
Microthrombin in hepatic circulation
Damage to hepatocytes
Elevated liver enzymes
Hemolysis, Elevated Liver Enzymes, Low Platelets
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 14, 2019 on www.thecalgaryguide.com")
Lyme Disease Pathogenesis and Clinical Findings

Tick bite from Borrelia burgdorferi infected Ixodes ricinus (tick from European countries)
Tick bite from Borrelia burgdorferi infected Ixodes scapularis (Deer tick/black-legged tick in SE Canada and NE United States)
Binding of OspC (a surface protein expressed by B. Burgdorferi) to human plasminogen allowing the spirochete to spread from bite site to other host organs and tissues
B. burgdorferi spreads through skin and other tissues via bloodstream in human host.
If tick bite lasts 36-72 hours or more, this is sufficient time for ticks to transmit the infection. (<36 hours of tick attachment results in a lower rate of infection: 1.2% -1.4%)
Lyme Disease
A vector-borne, infectious multi-system disease with highest risk in late spring and summer by the spirochete Borrelia burgdorferi
Early Disease Stage (<30 days)
Macrophages and T-cells produce ↑ inflammatory (TNF- α, IFN-γ) and ↑ anti-inflammatory cytokines, causing eosinophils to concentrate adjacent to the tick bite site
Early Disseminated Disease Stage (<3 months)
B. burgdorferi attach to host cell integrins
Pro-inflammatory response with production of matrix glycosaminoglycans and extracellular matrix proteins which have an affinity to attack collagen fibrils on the heart, nerves, and joints
1. Multiple erythema migrans 2. Meningitis
3. Meningoradiculoneuritis
4. Cranial nerve palsies
5. Carditis
6. Borrelial lymphocytoma
Late Disease Stage (>3 months)
Ongoing and repeated innate and adaptive host immune response to B. burgdorferi
Chronic inflammatory state results in synovial hypertrophy, vascular
proliferation, and ↑ mononuclear cell infiltrate in large joints
Large joint arthritis (most commonly affecting the knees)
Erythema migrans (a slowly expanding red skin patch with partial central clearing resulting in a “target clearing lesion” appearance) at site of tick bite
Systemic inflammatory response
after dissemination of the spirochete to body tissues and organs
Flu-like symptoms (fever, chills, muscle aches, headache, fatigue, joint aches, swollen lymph nodes)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 24, 2019 on www.thecalgaryguide.com
References
• David A. Wetter and Colin A. Ruff. CMAJ August 09, 2011 183 (11) 1281; DOI: https://doi.org/10.1503/cmaj.101533
• https://www.canada.ca/en/public-health/services/diseases/lyme-disease/causes-lyme-disease.html
• Borrelia burgdorferi Infection-Associated Surface Proteins ErpP, ErpA, and ErpC Bind Human Plasminogen. Catherine A. Brissette, Katrin Haupt, Diana Barthel, Anne E. Cooley, Amy Bowman, Christina Skerka, Reinhard Wallich, Peter F. Zipfel, Peter Kraiczy, Brian Stevenson. Infection and Immunity Dec 2008, 77 (1) 300-306; DOI: 10.1128/IAI.01133-08
• https://www.uptodate.com/contents/what-to-do-after-a-tick-bite-to-prevent-lyme-disease-beyond- the-basics
• Murray, T. S., & Shapiro, E. D. (2010). Lyme disease. Clinics in laboratory medicine, 30(1), 311–328. doi:10.1016/j.cll.2010.01.003
• Weedon, David. Weedon's Skin Pathology E-Book: Expert Consult-Online and Print. Elsevier Health Sciences, 2009.")
intraventricular-hemorrhage-in-preterm-infants-clinical-findings-and-complications
 in preterm infants:
Clinical findings and complications
Authors: Alexa Scarcello Reviewers: Nicola Adderley, Emily Ryznar, Yan Yu*, Jennifer Unrau* * MD at time of publication
Volpe Grading Grade I: germinal matrix
hemorrhage with no or minimal IVH (<10% of ventricular area)
Grade II: IVH (10-50% of ventricle) Grade III: IVH (>50% of ventricle;
usually distends lateral ventricle)
Grade IV/Intra-parenchymal echodensity (IPE): periventricular hemorrhagic infarction
Inflammation/dysfunction of arachnoid villi
↓ absorption of CSF 2° to obstruction of arachnoid villi
Communicating hydrocephalus (IVH grades II-IV)
Venous congestion
Venous infarction
Periventricular hemorrhagic necrosis
Destruction of periventricular motor tracts
Cerebral palsy
Rapid significant blood loss
↓ intravascular blood volume
Hypotension
↓ bloodflow to the brain to support brain function
Intraventricular Hemorrhage (IVH)
hemorrhage in periventricular subependymal germinal matrix
Ultrasound: blood in germinal matrix, ventricles, or cerebral parenchyma
Sudden ↓ hematocrit
Blood irritates contiguous structures
Variable neurologic findings; including altered level of consciousness, hypotonia, apnea, etc
Neuro- developmental abnormalities (varying severity)
See slide - Hydrocephalus: Clinical Findings in Pediatrics
This mechanism leads to three different possible clinical manifestations:
1. Silent Presentation (most common)
2. Stuttering/Saltatory Course: non-specific findings - hypotonia, apnea, altered level of consciousness, bradycardia, and ↓ Spontaneous movements
3. Catastrophic Deterioration (least common) Stupor or coma, decerebrate posturing, seizures, bradycardia, metabolic acidosis, bulging fontanelles, abnormal pupillary reflexes, inappropriate ADH secretion
Notes
• Incidence & severity are inversely proportional to gestational age
• 50% occur within 1st day of life, 90% by 3rd day
• As explained in the flow chart, the postnatal clinical presentations of
IVH fall into three categories (1-3)
• Symptoms of catastrophic bleeds are uncommon and usually caused
by rapid significant blood loss with subsequent neurologic findings 2° to meningeal irritation, inflammation, and potential mass effect/acute hydrocephalus; severe bleeds may also occur in the absence of clinical findings attributable to IVH
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 27, 2019 on www.thecalgaryguide.com")
Vitamin K Deficiency

Pancreatic insufficiency
Cholestasis
Malabsorption
Exposure to vitamin K antagonists (e.g., warfarin)
Inhibition of vitamin K epoxide reductase
↑ bleeding tendency
Gastrointestinal tract bleeds Intracranial bleeds Hemarthoses (bleeding into joints)
Easy bruising
Petechiae, purpura Heavy menstrual bleeds
Prolonged PT/INR
Note: PT/INR is more sensitive and validated for warfarin monitoring
↓ Activity of intrinsic clotting pathway
Prolonged PTT
↓ Activity of extrinsic clotting pathway
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published July 27, 2019 on www.thecalgaryguide.com")
Normocytic Anemia
![Normocytic Anemia: Causes, Signs, and Symptoms
Authors: Katie Lin Yan Yu Reviewers: Andrew Brack Jessica Tjong Man-Chiu Poon* Lynn Savoie* * MD at time of publication
Aplastic anemia: hypo-proliferation of bone marrow RBC precursors
Anemia of Chronic Disease
Splenomegaly
↑ RBC sequestration within enlarged spleen
Acute bleeding
Hemolysis (infection, autoimmune, RBC structural defects)
↓ RBC production
↑ RBC destruction/elimination
Normocytic Anemia:
[Hgb] <120g/L in females, <140g/L in males, with the RBC mean corpuscular volume (MCV) still within the normal range: 80-100 fL
RBCs that ultimately end up in the blood are still qualitatively normal/functional; there is a quantitative shortage of these RBCs in the blood relative to body needs
Spurious/False normocytic anemia:
Any fluid overload state (pregnancy, heart failure, kidney disease, etc.) can ↑ plasma volume which can dilute RBCs and cause apparent anemia, but the mean volume of each RBC is still normal
Normocytic Anemia
Heart needs to work faster to pump
sufficient oxygenated blood to tissues
↑ Heart rate
Reduced oxygen- carrying ability of blood
Patient feels oxygen- deprived, needs to inhale more oxygen as compensation
Dyspnea (shortness of breath) ↑ Respiratory rate (RR)
Not enough oxygen being delivered to body tissues, including brain
Fatigue
Reduced absolute number of RBCs means less RBCs to color the blood red
Pallor (especially conjunctival and palmar)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published July 27, 2019 on www.thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2015/05/Normocytic-Anemia-1.jpg "Normocytic Anemia: Causes, Signs, and Symptoms
Authors: Katie Lin Yan Yu Reviewers: Andrew Brack Jessica Tjong Man-Chiu Poon* Lynn Savoie* * MD at time of publication
Aplastic anemia: hypo-proliferation of bone marrow RBC precursors
Anemia of Chronic Disease
Splenomegaly
↑ RBC sequestration within enlarged spleen
Acute bleeding
Hemolysis (infection, autoimmune, RBC structural defects)
↓ RBC production
↑ RBC destruction/elimination
Normocytic Anemia:
[Hgb] <120g/L in females, <140g/L in males, with the RBC mean corpuscular volume (MCV) still within the normal range: 80-100 fL
RBCs that ultimately end up in the blood are still qualitatively normal/functional; there is a quantitative shortage of these RBCs in the blood relative to body needs
Spurious/False normocytic anemia:
Any fluid overload state (pregnancy, heart failure, kidney disease, etc.) can ↑ plasma volume which can dilute RBCs and cause apparent anemia, but the mean volume of each RBC is still normal
Normocytic Anemia
Heart needs to work faster to pump
sufficient oxygenated blood to tissues
↑ Heart rate
Reduced oxygen- carrying ability of blood
Patient feels oxygen- deprived, needs to inhale more oxygen as compensation
Dyspnea (shortness of breath) ↑ Respiratory rate (RR)
Not enough oxygen being delivered to body tissues, including brain
Fatigue
Reduced absolute number of RBCs means less RBCs to color the blood red
Pallor (especially conjunctival and palmar)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published July 27, 2019 on www.thecalgaryguide.com")
Appendicitis

The appendix is anatomically located in the RLQ; appendicitis may be confused with disorders of surrounding structures: Gynecological Diseases
• RuleoutpregnancywithHCG pregnancy test
• Rupturedovariancyst
• Ectopicpregnancy
• Mittelschmerz(mid-cycle
pain)
Gastro-intestinal Diseases
• Meckel’sdiverticulum (presents identically to appendicitis; surgically located 2 feet from ileocecal valve; mostly seen in children)
• Diverticulitis(presentsasleft sided appendicitis)
Non-GI Abdominal Issues
• Mesentericadenitisinkids <15: swollen mesenteric lymph nodes
• Renalcolic
Obstruction of appendiceal lumen (by fecalith, fibrosis, neoplasia, foreign bodies or lymph nodes in kids)
Appendix distension and spasms
↑ lumen pressure, ↓ blood flow to appendix
Ischemia, tissue necrosis, loss of appendix structural integrity
Bacterial invasion of the appendix wall, causing transmural inflammationandnecrosis
Stretching of visceral peritoneum, stimulation of autonomic nerves T9-T10
Progression of inflammation over several days (variable length of time)
Irritation of parietal peritoneum, stimulation of somaticnerves
If appendix not surgically removed
Perforation of colon wall, causing peritonitis, abscesses or death
Note: Symptoms hugely variable. Only 30% present with classic history. Diagnosis is mostly clinical. Further investigations:
CBC: Leukocytosis (due to inflammatory response) CT: Gold standard test. Thickened visceral membrane with enhancing (white) rim due to ↑ blood flow
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published July 27, 2019 on www.thecalgaryguide.com")
Acute GI Related Abdominal Pain

Bowel stretching, pulling, contracting
Abdominal pain type:
Diffuse, non-localized Dull, crampy, periodic Not associated with movement
Patient may writhe around, trying to get rid of the pain
Mesentery Intestinal lumen
Parietal peritoneum
(innervated by somatic nerves)
Cross-section of the GI tract
Cuts, structural damage, and inflammation in the bowel
Important Notes
• Acute abdominal pain can also result from non-
gastrointestinal causes, such as kidney stones, female reproductive tract issues, and urinary tract issues. For simplicity’s sake, only the GI-related acute abdominal pain disorders are listed here.
• The DDx of visceral abdominal pain is broad. Please consult relevant sections of the Calgary Black Book for the DDx.
• Keep in mind that visceral abdominal pain can also be caused by the “acute abdomen” diseases (if the diseases are presenting in their initial phases).
• • •
• • •
Abdominal pain type:
Sharp, well-localized
Excruciatingly painful, persistent Associated with movement of bowels
Patient often lies still to avoid abdominal vibration
Peritoneal signs
Abdominal guarding, pain with abdominal vibration (coughing, shaking, percussion, palpation)
Transition from diffuse to localized pain can indicate disease progression (e.g. from visceral to parietal peritoneal inflammation)
Note: bowel obstruction may or may not present as acute abdominal pain
Bowel Infarction
Appendicitis Diverticulitis
Acute Cholecystitis
Acute Pancreatitis
Perforated Ulcer
DDx of an “acute abdomen”:
A sudden, non-traumatic disorder of the abdomen that needs urgent diagnosis and treatment. Each topic will be further explored in their respective slides.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published July 27, 2019 on www.thecalgaryguide.com")
Operative vaginal delivery Complications of Vacuum
 Vacuum
Authors: Alexa Scarcello Reviewers: Claire Lothian, Crystal Liu, Yan Yu*, Ron Cusano* * MD at time of publication
Maternal trauma to surrounding structures to fit operative device
Traction and torsion on flexion point of fetal head, between anterior and posterior fontanelles
Pressure of device directly on fetal scalp
Pop-offs of vacuum cup
Rapid decompression and compression forces
Separation of underlying structures
Bleeding between skull and periosteom of neonate
Cephalohematoma
↑ breakdown of RBCs
↑ release of hemoglobin
Hemoglobin breakdown à↑ release of bilirubin into the bloodstream
Potential interference with spontaneous rotation of trunk
↑ risk of shoulder dystocia
Delivery during shoulder dystocia may traumatize infant’s shoulder
Brachial plexus injury
Head injury leads to potential ocular trauma
Retinal hemorrhage
Hyperbilirubinemia
Fetal scalp lacerations
Tentorial tears
Intracranial bleeding
Perineal lacerations
1° Lacerations: skin, subcutaneous tissue, vaginal epithelium 2° Lacerations: into superficial perineal muscles
3° Lacerations: extending to rectal sphincter
4° Lacerations: extending to rectal mucosa
Urethral injury
Rupture of emissary veins (connections between dural sinus and scalp veins)
Blood accumulation between epicranial aponeurosis and periosteom
Subgaleal hemorrhage
Large space in between these tissue layers ↑ capacity for blood accumulation here
Hypovolemia Death
Factors independent of operative device
Notes:
• •
Vacuums are now used more often (compared to forceps) due to ↓ maternal trauma
Caution in use if fetus <34wks
Jaundice
Less operator experience Higher fetal station
Poor head Rotation Longer active 2nd stage
↑ complication rate
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published Aug 4, 2019 on www.thecalgaryguide.com")
Ataxia Telangiectasia Pathogenesis and Clinical Findings
; involuntary muscle contractions, hypotonia, IQ decline, and abnormal eye movement
Loss of ATM leads to mitotic defects and arrest in gamete genetic recombination process
Gonadal dysgenesis and delayed puberty
DNA damage to tumor suppressors such as p53 and BRCA1
Impaired signaling of downstream cell cycle regulators
Impaired genome stability and increased disposition to cancer
↑ Acute Lymphocytic Leukemia of T cell origin (in children) and Chronic Lymphoblastic Leukemia (in adults)
Impaired recombination of DNA in immune cells
Thymic hypoplasia; humoral & cellular immunodeficiency
↓ or absent functional immunoglobulins IgA, IgE, and IgG2 that function to prevent respiratory infections
Respiratory infections with bronchiectasis and pneumonia
Cells less able to undergo apoptosis in response to ionizing radiation
Accumulation of DNA defects in the cells of sun exposed areas such as skin, hair, and conjunctiva
Mucocutaneous telangiectasia on the bulbar conjunctiva and ears between 2-6 years of age
May progress to involve periorbital skin, trunk, extremities, body folds, and other mucosal surfaces
Sterility
DNA damage and genomic instability
Premature melanocyte stem cell differentiation
Premature graying of skin and hair
Abbreviations:
• ATM – Ataxia-telangiectasia
mutated protein
• p53 – Tumor protein 53
• BRCA 1 – Breast cancer
susceptibility protein.
• IgA, IgE, IgG2 – Immunoglobulins
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 4, 2019 on www.thecalgaryguide.com")
Diverticulosis and Angiodysplasia

Angiodysplasia
Autoimmune Diseases
Unclear Mechanisms
These patients tend to have “arterial-venous malformations” that rise up to the mucosa of the lower GI tract
Irritation of these malformations leads to bleeding into the GI tract lumen
Lower GI bleed
(occult, slow, asymptomatic, large- volume blood loss, usually associated with iron deficiency anemia)
Renal Failure
Older Age
Gradual expansion over
time thins the diverticular wall
Capillaries within diverticuli burst and leak blood into the colon lumen
Lower GI bleed
(usually stops by itself)
Colon wall forms little outpouchings (diverticuli)
Stretching of colonic serosa stimulates
somatic sensory nerves innervating the colon
Bloating, cramping
(But most often PAINLESS)
Trapping of feces in the colonic diverticuli
Bacteria have more time to metabolize the undigested materials, producing gas
Flautulence
Irregular defecation
Both conditions share similar features:
• Both are common, and their prevalence increases with age
• Are relatively benign and most are easy to treat (80% stop w/o intervention)
• Both present without pain in a previously-well patient
• Together, account for 50-80% of lower GI bleeds (diverticulosis > angiodysplasia)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published August 4, 2019 on www.thecalgaryguide.com")
Erythema Nodosum pathogenesis and clinical findings
 ~28-48% of cases
Medications (Ex. Birth Control Pills, Sulfa drugs) ~3-10% of cases
Malignancy (ex. Lymphoma)
Autoimmune conditions (ex. Sarcoidosis and
Inflammatory Bowel Disease) ~11-25% of cases
Pregnancy ~1-3% of cases
Antigenic Stimuli / Bacteria / Viruses / Chemical Agents all could trigger the following process: Phase 1. Neutrophils Infiltrate the fibrous septa between fat lobules in the subcutaneous fat
Phase 2. Neutrophils release reactive oxygen species, leading to oxidative tissue damage and inflammation
Phase 3. Opening of inter-endothelial junction and the migration of more inflammatory cells into the septal venules, including macrophages, histocytes, and eosinophils
Phase 4. Macrophages secrete inflammatory cytokines, which stimulates the proliferation of more helper T cells (Th1)
Phase 5. Th1 cells secrete more cytokines, leading to the further release of Th1 cytokines and mediating the immune complexes deposition in the septal venules of the subcutaneous fat (panniculitis). The Th1 immune reaction is called Type IV Delayed Hypersensitivity Reaction
Phase 6. Activated macrophages produce hydrolytic enzymes and transform into multi- nucleated giant cells, called Miescher’s Radial Granulomas. These consist of small, well defined aggregations of small histocytes arranged radially around a small cleft of variable shapes in the septal venules of the subcutaneous fat
Phase 1-4. Lesions are red tender nodules, poorly defined, vary in size from 2-6 cm, and usually on shins ( 1st week)
Fat Lobules T lymphocytes
Macrophages
Note: we’ve done extensive research and can’t figure out why erythema nodosum happens mostly on the shins. If you have an answer, please email us!
Phase 5. Lesions become tense, hard, and painful; and they change in color into bluish or livid. (2nd week)
Phase 6. Lesions become fluctuant as in abscess, but do not ulcerate. Lesions fade to a yellowish color
Epidermal layer Dermal-Epidermal Junction
Dermal layer Subcutaneous Fat Layer
Phase 6. Miescher’s Radial Granulomas
Fat Lobules
T lymphocytes
Macrophages
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 25, 2019 on www.thecalgaryguide.com")
Colorectal Carcinoma pathogenesis and clinical findings

↓ appetite
Local bleeding
Abdominal Abscess
Weight loss
Acute blood loss
Iron deficiency anemia
Classification of tumours/abnormal growths:
1. Adenoma–abenigntumorfromglandular structures
2. Carcinoma–cancerarisingfromtheepithelial tissue of the skin or the lining of internal organs
3. Sarcoma–cancerarisingfromconnectivetissue
Mechanical bowel Obstruction
Ribbon (thin) stool
In rectum
Mass effect
Tumor ↓ bowel lumencaliber
Backed up contents mayberegurgitated
Cancerinvadesrectal sphincters, muscles, vessels&nerves
Compressing ureters, urine backs up into kidney
Compressing stomach
Abdominal distension/pain Invades blood vessels
Inflammatory
Bowel Disease Smoking
Abdominal radiation
Tubular adenomas
(pre- cancerous polyps)
Obesity
Local growth of tumor
Cell line mutations
Idiopathic
Uncontrolled cell division in the colon and rectum
Hereditary syndromes
Colorectal Carcinoma
(Develops over time)
Outside bowel serosa
Bowel perforation
Bowel to bowel/local organ fistulisation
Host immune cells release cytokines to combat cancer
Bowel contents leak
Metabolic abnormalities, ↑energy use
Tumor Spread Mechanisms:
1. Hematogenous 2. Lymphatic
3. Contiguous
4. Transperitoneal
Tumor cells spread distally
Friable vessels supply tumor
Metastatic Disease
Vessels Rupture
Occult bleeding &
melena (black stools) depletes stores of iron
Authors:
Karly Nikkel
Reviewers:
Michael Blomfield
Tony Gu
Yan Yu*
Edwin Cheng*
* MD at time of publication
Tumors develop in liver, lungs, brain, peritoneum and lymph nodes
Hematochezia (passage of fresh blood in stool)
Slow, chronic blood loss
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published August 25, 2019 on www.thecalgaryguide.com")
iga-vasculitis-henoch-scholein-purpura-pathogenesis-and-clinical-findings
 : Pathogenesis and clinical findings
Authors: Mia Koegler Nela Cosic Reviewers: Crystal Liu Yan Yu* Martin Atkinson* * MD at time of publication
Infectious Agents
50% have preceding upper respiratory tract infections, i.e., influenza virus or Group A Strep
Drugs
I.e., antibiotics (penicillin, erythromycin), NSAIDs and biologics (tumor necrosis factor α inhibitors)
Immunogenetic and cellular predisposition
Various genetic polymorphisms alter cell- mediated immune response, IgA levels elevated in 50% of people
↑ Circulating galactose-deficient IgA1 (GD-IgA1). Deficiency in galactosylation of IgAà↓ IgA serum clearanceàadhesion of IgA complexes, which then deposit into the endothelial lining of blood vesselsàattraction of various inflammatory cells to the area:
Formation of Secretion of Interleukin 8 (IL8) - cytokine that induces Neutrophils infiltrate Activation of complement immune complexes neutrophilic chemotaxis and macrophage phagocytosis the tissue site factors (C3, C4)
Leukocytoclastic vasculitis (histopathologic term for small vessels inflamed by neutrophilic autoimmune response)
Inflamed cutaneous vessels become enlarged in clusters
Symmetrical palpable purpura (red/purple, non- blanchable papules) distributed on lower limbs and buttocks areas
Cutaneous small vessel vasculitis (100%)
Inflamed gastric vessels - hemorrhage and edema within bowel wall
Gastrointestinal (85%)
Colicky abdominal pain (commonly in the periumbilical region), nausea, vomiting
Gastrointestinal
GI bleeding (hematemesis, melena), Intussusception
Glomerular mesangial proliferation and inflammation
↑ mast cell deposition in joints
Joints (60-85%)
Arthralgia's (common), arthritis (especially knees and ankles)
Arthralgia often transient. No permanent sequelae
Sympathetic nervous system activation
Glomerulosclerosis, tubulointerstitial and podocyte damage
Renal tissue ischemia
↑ Na sensitivity in renal tubules (↑ Na and water retention)
Renal (10-50%)
Increased renin secretion
HTN, nephrotic/nephritic syndrome, renal insufficiency
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 1, 2019 on www.thecalgaryguide.com")
Negative-Pressure-Pulmonary-Edema

Thrombotic Thrombocytopenic Purpura-Hemolytic Uremic Syndrome (TTP-HUS): Pathogenesis and clinical findings
: Pathogenesis and clinical findings
Thrombotic Thrombocytopenic Purpura
Hemolytic Uremic Syndrome
Shiga toxin from E. coli 0157:H7 infection
Acquired
ADAMTS13 auto-antibodies
Pregnancy/Post-partum Unclear mechanism
Failure to cleave large vWF multimers
Accumulation of large vWF multimers (Usually broken down by ADAMTS13)
Platelet aggregation and formation of platelet thrombi
Widespread microthrombi occluding blood vessels causing tissue damage/necrosis
Congenital ADAMTS13 mutation
Triggering event
ADAMTS13 deficiency
Drug dependent antibodies target platelets
Direct tissue toxicity (unclear mechanism)
ADAMTS 13 Inhibition Widespread hemolysis
Shut down of complement regulatory genes
Uninhibited membrane attack complex formation
Drugs (Quinine, Chemotherapy)
Abbreviations:
• vWF – von Willebrand Factor
• ADAMTS13 (vWF cleaving protein) – A
Disintegrin And Metalloprotease with a ThromboSpondin type 1 motif, member 13.
Formation of fibrin strands
Microangiopathic Hemolytic Anemia (schistocytosis)
Cellular damage due to fibrin deposit (intravascular, non- autoimmune hemolysis)
↑ serum indirect bilirubin
↑ serum lactate dehydrogenase ↓ serum haptoglobin
Authors:
Sean Spence Nicole Burma Reviewers: Tristan Jones Yan Yu Man-Chiu Poon* Lynn Savoie*
* MD at time of publication
Uncontrolled platelet activation and consumption
Thrombocytopenia
Reduced clotting ability
Purpura
Central Nervous System (CNS)
Confusion, severe headache, focal neurological findings
Heart
Patchy necrosis of myocardium
Arrhythmia, Sudden Cardiac Death
Kidney
Glomerular damage à↓ GFR + protein leakage into urine
Proteinuria, Acute Kidney Injury (AKI)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 1, 2019 on www.thecalgaryguide.com")
Acute-diverticulitis
 of the abdomen.
• PersistentLLQpain,abdominal guarding and peritoneal signs
• Constipation/obstipation
No bleeding (unlike diverticulosis)
Dehydration (low JVP, ↑ resting HR, orthostatic hypotension)
Inherent weakness in the muscle layers of the colonic wall
Low Fiber diet
↑ Stool transit time (↓colonic motility)
Stool build-up, ↑ pressure in colonic lumen
Epidemiology
• Diagnosis of developed nations,
total prevalence = 15%
• More prevalent with ↑ age:
• 30-50% by age 60 • 70% by age 80
Diverticula most commonly form in the descending and sigmoid colon
Triggers cytokine release
Irritationofparietal peritoneum → stimulation ofsomaticnerves
Inflamed vessels are more permeable & leak fluid from the blood into the colon
Mucosal and submucosal layers of the colon wall herniates through the circular muscle layer, creating colonic diverticula
Continued stress on diverticula causes micro-perforations → bacterial infection
Inflammation of diverticula reaches parietal peritoneum
Clotting of blood in the blood vessels feeding diverticula
Continued inflammation of diverticula causes complications over time
Fever
Complete bowel perforation (medical emergency)
Fistulae (through bladder, vagina, skin or gut)
Colonic fibrosis → GI strictures, colonic obstruction
Abscesses
Further Investigations:
• CBC: leukocytosis (due to inflammatory response) • CT = Gold Standard Diagnostic test: shows
inflamed diverticuli as well as complications (i.e. free air in peritoneum due to microperforations)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published September 1, 2019 on thecalgaryguide.com")
virchows-triad-and-deep-vein-thrombosis-dvt
:
Authors: Dean Percy Yan Yu Reviewers: Tristan Jones Ryan Brenneis Man-Chiu Poon* Maitreyi Raman* * MD at time of publication
Pregnancy, Oral Contraceptives (OCP)
Pathogenesis and Complications
Platelet Activation
Increased clot formation
Hypercoagulable State
↑ ability for the blood to coagulate upon stimulation
Inherited Disorders
Congenital defect in coagulation (ie. Factor V Leiden, Factor II
mutation, Protein S/C deficiency) ↑ blood clotting ability
Estrogen promotes
hypercoagulability, especially in presence of other risk factors
Notes:
• Venous thrombus causes pulmonary embolism, arterial thrombus causes stroke
• Previous DVT is risk factor for current DVT
Trauma/Surgery
Malignancy
Abnormal release of coagulation-promoting cytokines
Systemic injuryà activation of coagulation cascade
Hypertension
Bacteria Artificial Valve
Physically damages blood vessel walls
Adhere/invade vessel wall
Abnormal surface
Vessel Injury
Exposes tissue factor on damaged cells and subendothelium for vWF binding
Virchow’s Triad
Venous Stasis
Low blood flow rate over site of vessel injury, concentrating blood clotting factors at that site
Fat contains more aromatase, converts more androgens to estrogen
Sedentary lifestyle, poor venous return
Obesity
Clot formation typically occurs in leg veins
Deep, large veins allow for blood pooling (stasis, hypercoagulability) Venous return from legs often against gravity (stasis)
Valves in leg veins prone to backflow (stasis)
↓ muscle motion = ↓ venous blood flow
Fracture, immobilization, bedrest, long vehicle/airplane ride
Destruction of vein valve by clot
Venous Insufficiency
Clot prevents blood from returning to heart. Blood accumulating in the leg results in unilateral leg edema and venous inflammation (redness, warmth, tenderness)
1. 2. 3.
Clot embolizes to the lungs
Thromboembolus
-*Pulmonary embolism (acute life threatening complication)
-Chronic thromboembolic pulmonary hypertension
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published September 1, 2019 on thecalgaryguide.com")
Acute-Pancreatitis
![Acute Pancreatitis: Pathogenesis and Clinical Findings
Authors: Yan Yu Reviewers: Laura Craig Noriyah AlAwadhi Ryan Brenneis Maitreyi Raman* * MD at time of publication
Associated signs due to intra- abdominal hemorrhage from an unknown mechanism (classically associated with pancreatitis, but happens in <1% of cases):
Note:
It is not enough to just diagnose “acute pancreatitis”. Full management requires determining underlying etiology with further work-up.
Alcohol
↑ Toxic metabolites within pancreas and Spincter of Oddi Spasms
Gallstones
Migration to common bile duct blocks Sphincter of Oddi
Hypertriglyceridemia
Unknown
mechanism (rare)
Idiopathic
Further investigations:
CBC: Cell counts elevated, due to sever hypovolemia
Serum [Lipase]: Gold Standard Diagnostic Test; rupture of pancreatic cells releases lipase into circulation
Pancreatic secretions back up, ↑ pressure within pancreas
Hypercalcemia (Rare; Ca2+ depositions in bile ducts block outflow of pancreatic secretions)
Since pancreas is retroperitoneal, somatic
nerves in the parietal peritoneum are directly stimulated
Inflammation triggers cytokine release
Inflamed pancreas irritates adjacent intestines, causing ileus
Inflamed, more permeable blood vessels leak fluid into pancreas
• •
Cullen’s sign (bruising in peri-umbilical region) Grey-Turner’s sign (bruises along both flanks)
Sudden, severe epigastric pain (with peritoneal signs), radiates to the center of the back
Fever, nausea/vomiting
(general signs of inflammation)
Diminished bowel sounds Profound dehydration
(flat JVP, hypotension, tachycardia, oliguria) – may happen, not always
1. Pressure compresses pancreatic blood vessels, causing tissue ischemia.
2. Activation of inactive proteases (zymogens) digesting pancreatic tissue
Necrosis (death) of pancreatic cells
Inflammation self- perpetuates
Massive systemic inflammatory response
2 main complications, usually detected on CT;
may happen, but not always
1. Pancreatic pseudocyst (enlargement of the
pancreas due to fluid accumulation)
2. Pancreatic necrosis/abscesses (death of a part of the pancreas)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-published September 1, 2019 on thecalgaryguide.com](http://calgaryguide.ucalgary.ca/wp-content/uploads/2019/09/Acute-Pancreatitis.jpg "Acute Pancreatitis: Pathogenesis and Clinical Findings
Authors: Yan Yu Reviewers: Laura Craig Noriyah AlAwadhi Ryan Brenneis Maitreyi Raman* * MD at time of publication
Associated signs due to intra- abdominal hemorrhage from an unknown mechanism (classically associated with pancreatitis, but happens in <1% of cases):
Note:
It is not enough to just diagnose “acute pancreatitis”. Full management requires determining underlying etiology with further work-up.
Alcohol
↑ Toxic metabolites within pancreas and Spincter of Oddi Spasms
Gallstones
Migration to common bile duct blocks Sphincter of Oddi
Hypertriglyceridemia
Unknown
mechanism (rare)
Idiopathic
Further investigations:
CBC: Cell counts elevated, due to sever hypovolemia
Serum [Lipase]: Gold Standard Diagnostic Test; rupture of pancreatic cells releases lipase into circulation
Pancreatic secretions back up, ↑ pressure within pancreas
Hypercalcemia (Rare; Ca2+ depositions in bile ducts block outflow of pancreatic secretions)
Since pancreas is retroperitoneal, somatic
nerves in the parietal peritoneum are directly stimulated
Inflammation triggers cytokine release
Inflamed pancreas irritates adjacent intestines, causing ileus
Inflamed, more permeable blood vessels leak fluid into pancreas
• •
Cullen’s sign (bruising in peri-umbilical region) Grey-Turner’s sign (bruises along both flanks)
Sudden, severe epigastric pain (with peritoneal signs), radiates to the center of the back
Fever, nausea/vomiting
(general signs of inflammation)
Diminished bowel sounds Profound dehydration
(flat JVP, hypotension, tachycardia, oliguria) – may happen, not always
1. Pressure compresses pancreatic blood vessels, causing tissue ischemia.
2. Activation of inactive proteases (zymogens) digesting pancreatic tissue
Necrosis (death) of pancreatic cells
Inflammation self- perpetuates
Massive systemic inflammatory response
2 main complications, usually detected on CT;
may happen, but not always
1. Pancreatic pseudocyst (enlargement of the
pancreas due to fluid accumulation)
2. Pancreatic necrosis/abscesses (death of a part of the pancreas)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-published September 1, 2019 on thecalgaryguide.com")
Peptic Ulcer Disease

Toxin release
Inflammatory response
Inhibition of H+ detection in gastric antrum
H+ over-secretion
NSAID use
(including ASA
+/- other anti- platelet agents)
Ischemia
Zollinger–Ellison Syndrome (↑ acid secretion due to gastrin secreting tumor)
Stress
(in ICU setting)
Crohn’s disease
Cancer
(adenocarcinoma, SCC, lymphoma)
↑ Mucosal Injurious Substances: Acid: Gastrin, Histamine, AChàpromote
acid secretion in parietal cell
Toxins: drugs (for instance, NSAIDs) directly toxic to gastric epithelial cells, drugs that reduce platelet adhesion/plug
Authors: Dean Percy Yan Yu Reviewers: Sean Spence, Jason Baserman Paige Shelemey, Tony Gu, Kerri Novak* * MD at time of publication
COX-1 inhibition
Decreased prostaglandins
↑ H+ production, ↓
gastric mucous production
Toxicity to Gastric epithelial cells
↓ Gastroprotective Factors:
• Mucous: barrier between cells and HCl
• Blood flow: removes H+, supports mucosal cells
• Epithelial cells: physical barrier, HCO3- buffer
• Prostaglandins: ↓ H+ secretion, ↑ mucous
• •
production
Erosion of Mucosa
Erosion proceeds into blood vessels
Irritation of somatic innervation (T5-T8)
Bleeding into stomach
Bleeding into esophagus
Hematemesis
(Vomitting Blood)
Blood passes through GI tract, becomes oxidized by HCl & digestion
Melena
(black, tarry, foul- smelling stool)
Blood gets oxidized by HCl but moves back into esophagus
‘Coffee-ground’ Emesis
Notes:
Dyspepsia, Epigastric Pain
Nausea
• COX-2 inhibitors not always effective for gastroprotection
• In elderly patients and patients on NSAIDs, mucosal erosion can be silent (asymptomatic)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published September 22, 2019 on thecalgaryguide.com
Mechanism not well understood")
Rapid Sequence Induction and Intubation (RSII): Clinical Approach
: Clinical Approach
Authors:
Sandy Ly Reviewers: Wendy Yao
Melinda Davis*
* MD at time of publication
Reversible with Sugammadex (selective relaxant binding agent)
Responds to acetylcholinesterase
Reversible with acetylcholinesterase inhibitors
Not immediately reversible due to high dose
Classical RSII
Modified RSII
Induction Agent e.g. Ketamine or Propofol
(2 mg/kg)
Inhibitory effect on central nervous system
Cricoid pressure
(10 lbs pressure posteriorly)
Esophagus at the level of the cricoid obstructed
Reduced gastric regurgitation
Succinylcholine (2 mg/kg) acts similar to Ach
Depolarize end plate nicotinic receptors in skeletal muscle
Non-competitive with no antagonist
Rapid skeletal muscle paralysis
(<30 seconds) with short duration (<10 minutes)
Irreversible
Preoxygenation
with 100% O2 displaces nitrogen.
Functional residual capacity (2.5L) is filled with O2
Oxygen consumption (250 mL/min)
Extend time to desaturation (Ideal condition: 10 minutes)
Gastric distension with use of bag valve mask ventilation (positive pressure)
High dose Rocuronium (1 mg/kg) competitively antagonizes Ach
Decreased Ach binding on
nicotinic receptors in skeletal muscle
Rapid skeletal muscle paralysis (<60 seconds) with long duration (>45 minutes)
Quick Facts
Induction of anesthesia
Abbreviations
Ach – acetylcholine
See other pathways for more detailed pathophysiology
• •
•
RSII is used in patients with increased risk of gastric aspiration. Cricoid pressure is NOT THE SAME as BURP (backward, upward, rightward pressure).
Other induction agents possible (e.g. etomidate).
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 22, 2019 on www.thecalgaryguide.com")
Priapism
 pathways
Post-cavernosal venous drainage is mechanically obstructed e.g. sickle cell disease, dialysis etc.
Ischemic (Low-flow):
Inadequate venous function
Blood pools in corpora cavernosa
Cavernosal cell metabolism uses O2 and releases CO2 into pooled blood
Trabecular smooth muscle relaxes
Cavernosal artery smooth muscle relaxes
Lack of norepinephrine action on penile SM
Post-cavernosal venules are compressed against tunica albuginea
Trabecular smooth muscle and cavernosal artery smooth muscle do not contract
↑ pressure in corpora
↑PCO2 ↓pH
Acidosis
↓PO2
Tissue hypoxia
Tissue damage
Irreversible fibrosis leading to erectile dysfunction
Priapism
Prolonged erection lasting more than 4 hours; in absence of sexual stimulation; not relieved by ejaculation
Trauma to penis or adjacent areas
Authors:
Arsalan Ahmad
Reviewers:
Alec Mitchell
Darren Desantis*
Yan Yu*
* MD at time of publication
Cavernosal artery is damaged
Excessive, unregulated arterial blood flow into corpora cavernosa
Pain
Non-ischemic (High-flow):
Uncontrolled arterial flow
↑ volume of blood in corpora
↑ pressure in corpora
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 22, 2019 on www.thecalgaryguide.com")
Infantile Colic
 factors
↑ bile acid wasting ↓ bile acid production in immature in immature gut enterohepatic circulation
↓ bile acid availability
Psychosocial factors
Infant temperament Over/understimulation
Parental variables (e.g. parental stress)
Collectively, these factors influence the infant’s reactivity to adverse stimuli and the caregiver’s perception of whether crying is problematic.
Other biologic factors
Poor feeding techniques: under/ overfeeding, swallowing air, infrequent burping
Altered gut motility
GI discomfort
Infantile Colic
Dietary intolerances: cow’s milk protein, lactose
↑ gas production and gut distension
↓ mucosal barrier function
Loss of bacteriostatic effects of bile acids
Immature enteric nervous system
Intestinal microbial imbalance
↑ intestinal permeability
↑ systemic inflammation
Altered central and enteric neuronal function via microbiota-gut-brain axis
Altered perception of pain and other GI stimuli
Crying for no apparent reason that lasts > 3 hours/day and occurs ≥ 3 times/week for > 3 weeks in an otherwise healthy infant < 3 months old. There must be normal growth, development, and physical exam. Colic itself is a benign, self-limiting condition that resolves with time.
Facial flushing or grimacing Tense or distended abdomen
Drawing up of legs Clenching of fingers Stiffening of arms Arching of back
Distress expressed via behaviour
Loud, high- pitched, urgent cry
↑ risk of non- accidental trauma
GI factors directly affect infant’s behaviour
Hypothesized role of immature CNS regulation of circadian rhythm
↑ parental stress
Immature regulation of behaviour
Episodes cluster in evening and/or late afternoon
↑ risk of post- partum depression
Paroxysmal crying Inconsolable
Authors: Simonne Horwitz Nicola Adderley Reviewers: Crystal Liu Yan Yu* Danielle Nelson* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 28, 2019 on www.thecalgaryguide.com")
Macrosomia-Fetal-Complications

Size discrepancy between fetal shoulders and maternal pelvic inlet
Anterior shoulder becomes impacted behind the symphysis pubis during delivery
Shoulder Dystocia
(↑risk in infants of diabetic mothers – see slide on Gestational Diabetes)
Injuries acquired as a result of the birthing process in an infant with shoulder dystocia
↑ incidence of preterm birth
Surfactant deficiency
Respiratory Distress Syndrome
Umbilical cord compression
↓ delivery of oxygenated blood to fetus
Hypoxia/Asphyxia
Infant gasping
Perinatal aspiration of stained amniotic fluid
Meconium Aspiration Syndrome
↑ incidence of cesarean deliveries
↓ duration/absence of labour
↓ release of maternal epinephrine and glucocorticoids
↓ activation of epithelial sodium channels on type II pneumocytes
Delayed resorption of fetal lung fluid
Transient Tachypnea of the Newborn
Notes
↑ oxygen demands
Fetal hypoxia
↑ production of erythropoetin
Polycythemia Neonatal Jaundice
Maternal diabetes
↑ intrauterine exposure to
excessive nutrients and glucose
2Fetal Hyperinsulinism
↑ glucose utilization and suppression of hepatic glucose production
Termination of the maternal glucose supply at delivery
Hypoglycemia
Brachial Plexus Injury
Clavicular Fracture
Humeral Fracture
1. Complications of macrosomia ↑ with birth weight. Risk of stillbirth ↑ above 5 kg 2. Most common in the setting of poorly controlled maternal diabetes; however,
hyperinsulinism may be absent if macrosomia is secondary to a different etiology (e.g. post-term fetus, genetic conditions).
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published September 22, 2019 on www.thecalgaryguide.com")
intrauterine-devices-iuds-mechanism-of-action
: Mechanisms of Action
Authors: Danielle Chang Reviewers: Mirna Matta Crystal Liu Aysah Amath* * MD at time of publication
Intrauterine Device (IUD)
Contraceptive device that sits in the fundus of the uterus
Two Types
Copper
T-shaped polyethylene with fine copper wrapped around the vertical stem and arms
Releases copper in the uterus
Progesterone Releasing
IUD made of plastic containing levorgestrel (synthetic progesterin, progesterone receptor agonist)
Releases levorgestrel in the uterus Stimulate progesterone receptors
May inhibit ovulation through negative feedback on hypothalamus (not consistent evidence)
Foreign body reaction in endometrium
IUD creates local lysosomal activation and uterine inflammatory response Mechanism not fully understood
Spermicidal
High copper concentrations toxic to sperm
Alters sperm mobility
Decreases chance of fertilization
Suppresses endometrium
Thickening of the cervical mucus
Barrier to sperm penetration
Disturbs function of endometrium
Changes uterine environment
Thins the endometrium
Decreases number of blood vessels to the endometrium
Suppresses proliferation
Atrophies endometrial glands
Sloughing of the endometrium
Inflammatory reaction against blastocyst if fertilization occurred
Hostile environment for implantation
Decreased menstrual blood loss and eventual amenorrhea
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published October 12, 2019 on www.thecalgaryguide.com")
X-linked Severe Combined Immunodeficiency (SCID)
: Pathogenesis & clinical findings
Abbreviations:
• Ig: Immunoglobulin
• IL: Interleukin
• NK: Natural Killer
• Th2: T helper 2 cell
• Treg: T regulatory cell
↓ IL-15 signaling ↓NK cell differentiation
and proliferation
↓ or absent NK cells in the blood, bone marrow and peripheral lymphoid tissues
Impaired innate immune system
Chronic Stress Response
Mutation of the IL2-RG gene encoding the interleukin receptor common gamma chain located on the X-chromosome
↓ IL-2 signaling ↓T cell
proliferation
Sequence analysis shows mutated, duplicated or deleted IL2-RG gene
↓ IL-7 signaling Global ↓ in
lymphocyte survival
Absent thymic shadow on X-ray
↑ susceptibility to fungal infections
Complete defect in cell mediated and humoral immunity
↓ antibody responses to vaccinations
↑ susceptibility to extracellular pathogens, most notably bacteria
Authors: Kyo Farrington Reviewers: Paul Adamiak Jessica Tjong Louis Girard* *MD at time of publication
↓ IL-4 signaling ↓Th2
differentiation
↓T cell help for B cell activation and class switching
Dysfunctional B cells
Genetic Predisposition
↓ Treg development
↑ risk of developing an autoimmune disease
↓ T cell response to mitogens or
anti-CD3 stimulation
↓ or absent T lymphocytes in the blood, bone marrow and peripheral lymphoid tissues
↑ susceptibility to viral infections (often gastrointestinal ones like rotavirus and/or enterovirus)
Chronic diarrhea
Hypoplastic lymphoid tissues (I.e. tonsils, adenoids, lymph nodes)
Hypermetabolic State
Failure to thrive
↓ antibody production in response to antigen exposure
↓ IgA, IgM and IgG serum concentrations
Note: IL2-RG gene encodes the interleukin receptor common gamma chain, which is a sub-unit common to the receptor complexes for IL-2, IL-4, IL-7, IL-9,
IL-15 and IL-21. The bolded/italicized cytokines contribute most to the pathophysiology of X-linked Severe Combine Immunodeficiency (SCID).
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published October 12, 2019 on www.thecalgaryguide.com")
Ischemic Colitis
 supply blood to colon
Surgical repair of aorta
Borders of SMA and IMA collaterals at the splenic flexure and rectosigmoid junction are vulnerable to ischemia (“watershed” areas)
Atherosclerosis and narrowing of mesenteric arteries
Low flow state
(e.g., CHF, hypotension, arrhythmia)
Underlying CAD/PVD
Atrial fibrillation, endocarditis
Embolic arterial occlusion of SMA and/or IMA
Trauma, infection, clotting abnormalities
Mesenteric vein thrombosis
Vascular risk factors (e.g., smoking, hypertension)
Thrombotic arterial occlusion of SMA and/or IMA
Endograft coverage of IMA
Nonocclusive hypoperfusion
Inadequate blood flow to meet the cellular metabolic needs in the colon
Ischemic Colitis
Tachypnea Tachycardia Hyperthermia Hypotension
Ischemic period
Loss of oxygen and nutrients to bowel
Reperfusion period
Influx of O2àreacts to produce more oxygen free radicals
Lipid peroxidation
Systemic inflammatory response syndrome*
Nausea and vomiting
Abdominal pain (generally left sided)
Peritonitis
Leukocytosis
Systemic shock
(inadequate perfusion to tissue)
Author: Audrey Caron Michael Blomfield Reviewers: Tony Gu Yan Yu* Edwin Cheng* * MD at time of publication
Systemic shock
(inadequate perfusion to body tissue)
Hematochezia (Bloody stool)
Gangrene (tissue death)
Hemorrhage
Tissue damage/cell death (starting from mucosa and submucosa going outwards to serosa)
Mucosal ulceration
Colonic inflammation
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 10, 2019 on www.thecalgaryguide.com")
Incisional-Hernia
 that ↑ risk of infection
Post-op wound Infection
Obesity
Chronic constipation
Chronic cough Pregnancy
↓ clotting factors
Vigorous cough
Severe Hypertension
Seroma
Post-op hematoma Bulging fluid separates High risk
Sutures unsuitable Poor surgical for tension technique
↑ intraabdominal pressure
Fascial Incision separates
Notes:
fascial incision
surgeries* High Risk Surgeries*
Connective tissue disorder
Suboptimal fascial closure
• • •
Emergency surgeries Midline incisions
Acute abdominal surgeries
↓ wound healing/collagen synthesis
Fascial defect at previous incision site
Incisional Hernia:
Protrusion of tissues through prior fascial incision
• Deep wound infection = most common cause of incisional hernias
• Diagnosis on physical exam +/- CT scan if patient is obese
• Treatment = surgery
Bulge at prior incision site
Palpable fascial defect
Bowel and other abdominal contents protrude through defect
Mechanical bowel obstruction (see relevant slide)
Constipation /obstipation
Contents unable to be pushed back through defect (incarceration)
Vascular supply is compromised to herniated contents
Contents become ischemic (strangulated)
Prolonged pressure on skin & bowel over time
Ulceration & ischemia
↓ blood flow to skin layers
Discoloration of skin
Bulge ↑ with coughing/straining
Ulcers extend through bowel wall
Authors: Karly Nikkel Meaghan Ryan Reviewers Michael Blomfield Tony Gu Yan Yu* Edwin Cheng* *MD at time of publication
Colo-enteric fistula
Bowel Perforation
Abdominal Pain
Abdominal Distension
Nausea/ Vomiting
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 13, 2019 on www.thecalgaryguide.com")
Endometritis

Uterine tenderness
Pelvic and/or abdominal pain
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 26, 2019 on www.thecalgaryguide.com")
Hydrocele

Transillumination
Testicular Atrophy
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 26, 2019 on www.thecalgaryguide.com")
Varicocele
.
• Small varicoceles can be identified by preforming the Valsalva maneuver (decreases venous return).
• Unilateral right varicoceles are uncommon and should be investigated for underlying pathology causing obstruction.
Primary
Anatomically: the left spermatic vein drains into the left renal vein
Nutcracker Effect: The left renal vein can get pinched by the abdominal aorta and superior mesenteric artery
Backup of blood in left renal vein ↑ pressure in left spermatic vein
Secondary
Renal cell carcinoma or retroperitoneal masses
Inferior vena cava thrombus
External compression of spermatic vein
Obstruction of blood flow
↑ spermatic vein pressure
Vein valve leaflet failure & retrograde bloodflow back towards testicle
Dilation of pampiniform plexus and scrotal vein plexus
Varicocele
↑ scrotal blood volume ↑ volume in a closed
space
↑ pressure and distension of scrotal layers
↑ scrotal vein plexus pressure
Compliant veins distend, becoming visible through scrotum
Blood heats up the structures it flows through
Scrotal hyperthermia
Unsuitable environment for spermatogenesis
Loss of germ cell mass
Bag of Worms Sign
Dull ache/heaviness
Decreased fertility Testicular atrophy
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published November 26, 2019 on www.thecalgaryguide.com")
Aphasia
: Pathogenesis and clinical findings
Authors: Davis Maclean Reviewers: Heather Yong Tony Gu Yan Yu* Scott Jarvis* *MD at time of publication
Ischemic stroke (common)
Local Invasion (e.g. by a tumour, Head infection, or hemorrhage) Trauma
Intracerebral Hemorrhage
Dementia (e.g. Fronto- temporal Dementia)
Episodic occurrences (e.g., migraine, epilepsy)
Damage to language-dominant cerebral hemisphere (the left hemisphere, for the majority of humans):
Damage affecting Broca’s Area in the Inferior frontal gyrus (area 44 & 45)
Damage affecting Wernicke’s Area in the posterior part of the superior temporal gyrus (area 22)
Localization: Inferior frontal gyrus, superior sylvian fissure
Blood supply: superior division M2 branch middle cerebral artery
Localization: Posterior perisylvian region, temporal lobe
Blood supply: inferior division M2 middle cerebral artery
Sensory speech
areas still intact (posterior superior temporal lobe)
Intact comprehension (intact hearing & reading)
Impaired function of Broca’s Area
↓ output or generation of speech/ text
If function of nearby motor areas is also impaired
Contralateral hemiparesis (face, arm > leg)
If function of other nearby areas is also impaired
Impaired naming and repetition
Motor speech areas still intact (inferior frontal lobe)
Fluent (but non-sensical) speech output
Impaired function of Wernicke’s Area
Impaired compre- hension (i.e. cannot understand speech or text)
Loss of sensory speech input to motor areas
Errors in word usage, tense, structure
If function of nearby sensory areas is impaired
Contralateral sensory deficits
Broca’s Aphasia
Wernicke's Aphasia
(Expressive language impairment: non-Fluent)
Notes/Definitions:
(Receptive language impairment/Fluent: the person can talk but their speech is nonsensical)
• Dysarthria ≠ Aphasia (Dysarthria: disruption to neurons controlling the muscles that produce sounds, resulting in slurred/disjointed speech. Aphasia: acquired deficit in language comprehension or generation/output usually due to disruption of neurons in the cerebral cortex.)
• “Global” aphasia affects both receptive and expressive language.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 1, 2020 on www.thecalgaryguide.com")
Slide-authoring-process-FINAL-2
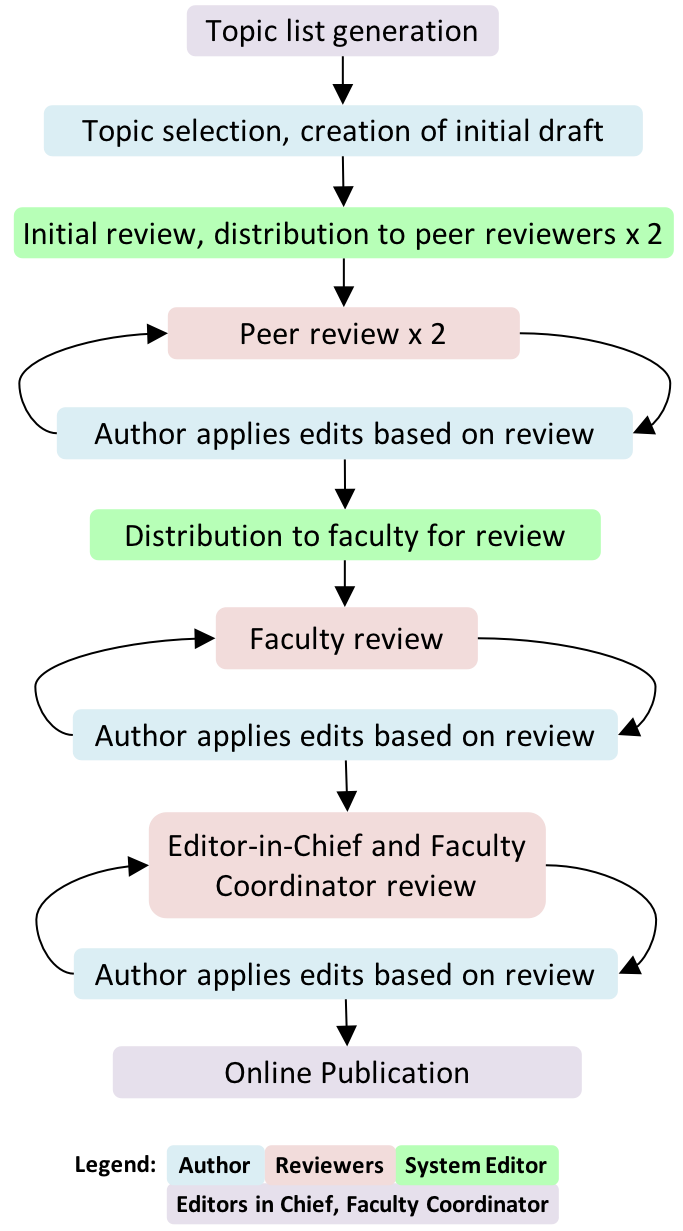
A1AT-Deficiency
 allele(s)
Accumulation of mutant α1AT protein as ordered polymers in endoplasmic reticulum of hepatocytes
↓ α1AT inhibition of Hepatocyte Injury tissue proteases (Mechanism unclear)
↓ release from hepatocytes
Cirrhosis, chronic hepatitis, hepatocellular carcinoma
↓ lung elasticity, ↓ ability for lung to expel air on expirationà gas trapping, hyperinflation, airway collapse over time
Role of Genetics:
Low serum α1AT
In the skin: Subcutaneous proteases > Anti- proteases
Unopposed proteolysis in subcutaneous tissues
Panniculitis (Rare, most cases associates with ZZ Genotype)
Lung Proteases > Anti-proteases àproteolytic destruction of lung parenchymaàpanacinar emphysema (accelerated by smoking)
Stigmata of chronic liver disease (ascites, jaundice, spider nevi, petechiae, etc.)
Symptoms of chronic obstructive pulmonary disease (COPD): barrel chest/High residual volume (RV), low vital capacity (VC), wheezes on auscultation, etc) – see relevant slide
Degree of α1AT deficiency dependent on genotype:
• MM gives normal α1AT levels
• MZ genotype produces levels ~ 35% of normal
• ZZ genotype produces severe deficiency ( <10% of normal)
• Null phenotype is completely deficient of α1AT
N.B. Heterozygotes almost never develop phenotypic α1AT deficiency syndromes. Even some homozygotes don’t manifest the disease.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published January 12, 2020 on www.thecalgaryguide.com")
Viral-Hepatitis
 of hepatocytes
Infection with chronic viruses (HBV and HCV) persist over time and additional symptoms may develop
RUQ pain/tenderness
If infection is prolonged or severe, inflammation becomes systemic
Release of hepatocyte’s cellular contents into the bloodstream
Infection with acute viruses (HAV and HEV) resolve over time, and the symptoms above normalize
Notes:
• HDV can only infect people with concomitant HBV infection
• HAV and HBV vaccines are the only ones that currently exist
• Not all patients with viral hepatitis will develop each of these symptoms. The presentations vary.
Fever, nausea, vomiting ↑ serum ALT, AST
↓ Hepatic metabolic activity (e.g. reduction of gluconeogenesis) ↓Serum Glucose
↓ Synthesis of plasma proteins (albumin, clotting factors, etc) ↓ Albumin, ↑ INR
Abbreviations:
• HAV - Hepatitis A Virus
• HBV - Hepatitis B Virus
• HCV - Hepatitis C Virus
• HEV - Hepatitis E Virus
• RUQ - Right Upper Quadrant
• ALT - Alanine Aminotransferase
• AST - Aspartate Aminotransferase
• INR - International Normalized Ratio
↓ Bilirubin clearance from blood, bilirubin ends up under the skin Jaundice Portal Hypertension
Encephalopathy, Splenomegaly, Esophageal Varices, Ascites, Caput Medusae, Edema
Encephalopathy, Muscle Wasting, Metabolic Bone Disease, Terry’s Nails, Ascites, Bruising, Clubbing, Edema
Spider Nevi, Altered Hair Patterns, Testicular Atrophy, Gynecomastia, Palmar Erythema
Progressive deterioration in liver function, possibly ending up in cirrhosis. (See slide on “Cirrhosis: pathogenesis and complications” for more details on mechanisms and full explanations.)
Hepatic Insufficiency Hyperestrogenism
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published January 12, 2020 on www.thecalgaryguide.com")
Multiple-Myeloma
 immunoglobulins
Normal SPEP: no spike in the gamma (γ) region
Notes:
• MGUSismuchmorecommon than MM!
• “Plasmacell”:Blymphocytes that produce antibodies/ immunoglobulins
Stimulation by specific antigens
Genetic changes/mutations accumulate over time in one type of plasma cell
Abbreviations/Definitions: • SPEP - Serum Protein
Electrophoresis
• Ig – Immunoglobulin • Monoclonal – “of one
specific genetic strain or subtype”
One type of plasma cell starts to proliferate abnormally
Monoclonal Gammopathy of Undetermined Significance (MGUS) (Premalignant, mild monoclonal plasma cell proliferation; asymptomatic)
In 1-2% of cases, further cytogenetic changes over time stimulate further proliferation of this plasma cell line
Multiple Myeloma (MM)
(extensive monoclonal B lymphocyte proliferation, causing end organ damage)
Slightly more monoclonal plasma cells will produce slightly more monoclonal Immunoglobulins
Small spike in the gamma (γ) region of the SPEP (less prominent compared to the spike in MM)
More monoclonal plasma cells result in far greater amounts of monoclonal immunoglobulins being secreted
Large spike in gamma (γ) region of the SPEP
Ig light chains accumulate in the tubules of kidney nephrons
Light chain casts obstruct tubules
Renal Insufficiency (↓GFR)
Osteoblasts ↑ expression of RANK-ligand (RANKL, an apoptosis regulator), and ↓ expression of Osteoprotegerin (OPG, a decoy receptor for RANKL)
↑ osteoclast activity vs osteoblast activityàbone loss
Clonal plasma cells overrun normal bone marrow, crowding out production of red blood cells, ↓ red blood cell counts
Anemia
Authors: Tristan Jones, Tyler Anker, Yan Yu Reviewers: Jennifer Au, Crystal Liu, Man- Chiu Poon*, Lynn Savoie* * MD at time of publication
Damaged bones hurt, & become more brittle
Bony pain, pathologic fractures
Osteolytic bone lesions
Osteoclasts release calcium from bone and into blood
Hypercalcemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 12, 2020 on www.thecalgaryguide.com")
Pathophysiology-Behind-the-Leukemias

Chromosomal Abnormality (duplication, loss, recombination error)
Combinations of these genetic defects causes reduced tumor suppressor gene expression and/or increased oncogene expression
Initiating Mutational Event
ALL
Any combination of mutations, chromosomal
alterations, or other genetic abnormalities that creates a neoplastic cell (incapable of regulating cell growth/division).
AML
CLL
CML
Translocation between Chr 9 and Chr 22à Philadelphia chromosome ( abnormal Chr 22)
àBCR-ABL1 oncogene (along with other genetic abnormalities)
•
In White Blood Cells and their precursors: Lack of cell growth inhibition and / or apoptosis.
• Over stimulation of cell division/growth Neoplastic blood cell incapable of regulated cell
division
Neoplastic cells uncontrollably divide in a monoclonal way: one neoplastic cell originates all successive cells
Genes regulating differentiation/maturation disrupted, affected neoplastic cells are incapable of further differentiation/maturation
Genes regulating maturation remain intact (affected neoplastic cell is capable of further differentiation/maturation)
Some neoplastic cells take time to mature furtheràless rapid disease progression (more indolent disease); cells don’t die
CLL: Chronic Lymphoid Leukemia
Note:
Although it is tempting to group the leukemias together for study purposes, it is best to learn the 4 main types of leukemias independently of one another, as they have a uniquely different pathophysiology and clinical presentation
Specific mutations cause slower disease progression
CML: Chronic Myeloid Leukemia
Degeneration during CML’s ”blast crisis”
Specific mutations cause rapid division and buildup of existing neoplastic cells àAcute/rapid disease progression.
ALL: Acute Lymphoblastic Leukemia AML: Acute Myeloid Leukemia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-Published January 19, 2020 on www.thecalgaryguide.com")
Aqueous-Humor-Production-and-Drainage
 through combined hydrostatic pressure + active transport
AH enters the posterior chamber
AH flows around the lens through the pupil into the anterior chamber
Temperature gradient cause aqueous humor to flow convectively: downwards at the cornea (colder, fluid denser); upwards at lens (warmer)
Abbreviations:
• AH – Aqueous Humor
• TM – Trabecular Meshwork
Provides nutrition, removes wastes, and transports neurotransmitters to the avascular lens and cornea.
Circulates inflammatory cells to avascular structures
Maintains structural integrity of ocular structures via intraocular pressure (10-21 mmHg)
AH leaves the anterior chamber via two pathways located near the limbus
Limbus
Trabecular Meshwork Pathway (~60-80 % of flow)
AH passes through the TM layers: Uveal, corneoscleral, and juxtacanalicular
Flows into Schlemm’s Canal
Flows through internal outflow channels into the external outflow channels, aqueous veins, intrascleral venous plexus, and the deep scleral venous plexus
Drains into the episcleral and conjunctival veins
Uveoscleral Pathway (~20-40 % of flow)
AH enters uveal meshwork and anterior ciliary body
Flows in suprachoroidal space
Passes outward through the sclera
Enters the scleral, and conjunctival veins
Drains back into systemic venous circulation
Inflow
Trabecular Outflow
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 19, 2020 on www.thecalgaryguide.com")
Innate-Immune-Response

Pathogens overcome physical barriers (e.g., epithelium, cilia)
Trauma
Damage-associated molecular patterns
Pathogen-associated molecular patterns
Examples of tissue-resident macrophages: • Alveolar macrophages – Lung
• Histiocytes – Connective tissue
• Kupffer cells – Liver
Recognition by pattern recognition receptors (e.g., toll-like receptors)
• Mesangial cells – Kidney • Microglial cells – Brain
• Osteoclasts – Bone
Microbe engulfed and exposed to oxidative burst
Microbes destroyed
Pus
Pro-inflammatory chemokines
Recruitment of circulating
granulocytes and monocytes
Pro-inflammatory cytokines (e.g., IL-1β, TNFα, IL-6)
Tissue-resident macrophage activation
Antimicrobial proteins
Unresolved infection/ inflammation
Antigen presented to T cells
Recruitment of adaptive immune response
Enhanced immune responses
Acute phase protein production by liver (i.e., C- reactive protein)
Prostaglandin production in the hypothalamus
Fever
Endothelial tight junctions on vasculature disrupted
Intravascular fluid leak into extravascular space
Edema
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published January 19, 2020 on www.thecalgaryguide.com")
vomiting-pathogenesis
 Center
Toxins circulating in bloodstream: Chemotherapy, Opioids
Offending substance travels through circulation and binds to receptors in the CTZ, outside the blood brain barrier
Abbreviations:
GERD: Gastroesophageal Reflux Disease PUD: Peptic Ulcer Disease
IBD: Inflammatory Bowel Disease
CTZ: Chemoreceptor Trigger Zone
CNX: Cranial Nerve Ten
H1: Histamine Receptor
M1: Muscarinic Receptor
Disrupted inner ear balance: Motion Sickness
Activation of H1 & M1 receptors in vestibular center traveling via Cerebellum
Stimulates Solitary Tract Nucleus (Medulla)
(Medulla)
Vagus Nerve (CNX) and enteric nervous system activation, resulting in:
Gastric relaxation, ↓ pylorus tone, retrograde duodenal peristalsis
Downward diaphragm contraction, abdominal & chest wall muscles contract: ↑ intra-gastric pressure
Vomiting
(Forceful expulsion of material from stomach and intestines)
Upper and lower esophageal sphincter relaxation and glottis closure
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Re-published February 16, 2020 on www.thecalgaryguide.com")
Pseudogout
 crystals from joints is inhibited by iron
Hypomagnesia
The relative absence of magnesium impairs pyrophosphatase activity, reduces pyrophosphate breakdown
Hypophosphatasia
Defective mineralization of calcium and phosphorous in bones
Idiopathic (vast majority of cases)
Mechanism unknown
↑ serum concentrations of Ca2+ or Pyrophosphate
Enhanced mineralization in chondrocytes (cells that make cartilage)
Abbreviations
• NTPPPH nucleoside triphosphate
pyrophosphohydrolase
• CPPD – Calcium Pyrophosphate
Dihydrate
Notes:
• There are different types of calcium pyrophosphate crystal deposition (CPPD) disease. This slide only covers “pseudogout”.
• Pyrophosphate (PPi) = 2 phosphate molecules = P2O74−
• Pyrophosphate is made from the breakdown of Adenosine triphosphate (ATP): ATP -> AMP + PPi
Once in cartilage, high levels of either calcium ions or pyrophosphate can result in them binding together, forming CPPD crystals
Aggregated CPPD crystals shed into synovial fluid
Neutrophils enter joint to phagocytose the crystals and release pyrophosphatase enzyme
Repeated crystal precipitation into joint space over time (subacute process)
CPPD crystals collect on collagen fibers in articular cartilage
Chondrocalcinosis, seen on high-resolution ultrasound and/or x-ray
CPPD crystals exhibit unique properties on polarizing microscopy
Inflammatory cascade
Positively birefringent (crystals appear blue parallel to axis of polarizer)
PAINFUL, warm, swollen joint (sudden onset)
↑ C-reactive protein (CRP); erythrocyte sedimentation rate (ESR)
Knees and wrist subjected to more trauma over a person’s lifetime
Knee > Wrist >>> any other joint affected
Wearing down of joint cartilage over time
Rapidly progressive osteoarthritis (see osteoarthritis slide)
Subchondral sclerosis & cysts, joint space narrowing, and osteophytes seen on x-ray
bone loss, hemarthrosis
Nerve damage over time
“Charcot-like” joint: severe weightbearing to areas that joint destruction/deformity,
Painless joint
Lack of sensation can cause tolerate it poorly
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 16, 2020 on www.thecalgaryguide.com")
C5-C9-deficiency
 causes Secondary (acquired) causes
All are autosomal recessive Biologic therapy ex. eculizumab Absence or suboptimal functioning of
Abbreviations:
• MAC: Membrane Attack
Complex
• CH50: Classic Hemolytic
Complement Test
• AH50: Alternative Hemolytic
Complement Test
• CNS: Central Nervous System • CSF: Cerebrospinal Fluid
≥1 terminal complement proteins
C5-C9 deficiency
Inability to form MAC
↑ susceptibility to systemic Neisseria infection
Commonly N. meningitidis Rarely N. monorrhoeae
Nasopharyngeal colonization of N. meningitidis, ↑ susceptibility to bacteremia
CH50 ± AH50 assay No lysis
Note:
Total complement activity assay <10% activity C5, C6, C7, C9 <50% activity C8
Varied bactericidal action via other complement proteins
• Risk of invasive meningococcal disease is 1000-10000X higher in C5-C9 deficiency than in the general population
• Reason is unknown
• C5-C9 deficient patients are not at greater
risk for contracting other gram (-) infections • Clinical meningitis in C5-C9 deficiency is less
severe and fatality is rare
Bacterial lysis
Especially gram (-)ve bacteria like Neisseria
Bacteria cross the blood-brain barrier, causing swelling and damaging brain tissue
Fatigue, fever, headache, altered mental status, etc.
Inflammation of CSF and meninges
Activation of dura and pia mater fibres
Headache, neck stiffness
Bacteria release toxins
Damage to surface blood vessels
Maculopapular rash
Exact mechanism unknown
Recurrent meningitis
CNS damage due Sepsis to recurrent
meningitis
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 16, 2019 on www.thecalgaryguide.com")
tinea-capitis-tinea-corpora-and-tinea-pedis
:
1. Trichophyton
2. Epidermophyton 3. Microsporum
Direct contact with infected humans, animals, or inanimate objects
Dermatophyte invades uppermost, non-living, keratinized layer of skin, the stratum corneum
Dermatophyte produces enzyme keratinase Keratinase catalyzes degradation of keratin
proteins in the skin Dermatophyte burrows deeper into skin
Keratinocytes release inflammatory cytokines in reaction to dermatophyte antigens
Dermatophyte moves outwards, away from site of infection, to new areas around the initial site
Classic pink-to-red ringed lesion, with central healing
Tinea corporis
Scaling of skin (such as between the toes: “maceration”)
Invasion of hair follicle
Hair shaft breaks
Alopecia (loss of hair) Pruritis(itchiness) Erythema (redness) Induration (swelling) Heat
Local inflammatory response in skin
Tinea capitis
Tinea pedis
Infection of the foot (aka. Athlete’s foot)
Infection of the scalp Infection of the trunk and extremities of the body
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 17, 2020 on www.thecalgaryguide.com")
Brain-Neoplasms

Mutagen exposure (e.g., radiation, carcinogens)
Errors of DNA replication
Acquired cell mutations leading to uncontrolled cell division in the brain
Inherited diseases (e.g., neurofibromatosis, tuberous sclerosis)
Primary Brain Tumours
(e.g., gliomas, meningiomas, pituitary adenomas)
Brain Neoplasms
Tumors in the brain arising from brain tissue itself (primary) or from non-brain tissue (metastatic)
Tumor produces vascular endothelial growth factor (VEGF) which generates new vessels (angiogenesis)
Tumor occupies intracranial space
↑Intracranial pressure
Tumor irritates grey matter
Seizures
Headaches Papilledema
Tumor outgrows and disrupts its blood supply
Cerebral ischemia and/or necrosis
Critically located tumors may damage specific neural pathways
Tumor invades, infiltrates, or replaces normal brain parenchyma
Friable blood vessels within tumor àeasy bleeding
Brain hemorrhage
Disrupted blood- brain barrier
↓ blood vessel integrity à ↑ serum leaks out
Edema
Injury to localized brain regions; symptoms vary depending on location of brain affected:
↑ penetration of substances
(e.g., drugs, toxins)
Mass pressing on surrounding structures (mass effect on brain)
Frontal lobe damage
Personality change
Cerebellar damage
Ataxia
Occipital lobe damage
Visual deficits
If adjacent to 3rd/4th ventricles,
tumor will impede flow of cerebrospinal fluid
Obstructive Hydrocephalus
Stretching of meninges; activation of mechanoreceptors affecting the chemoreceptor trigger zone
Vomiting Nausea
Brain tissue pushed down beyond the
tentorium cerebelli, squeezing on brain stem
Brain Herniation
Note: Clinical findings tend to be similar for primary brain tumors and intracranial metastases.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 17, 2020 on www.thecalgaryguide.com")
Umbilical-Cord-Prolapse
 position for delivery e.g. transverse presentation
Abnormal placentation
Poly- hydramnios
If membranes are ruptured, there is a large volume of fluid that may push the umbilical cord through the cervix
Multiple gestation
(second twin)
Multiparity
Multiple fetuses distend uterus
↑ laxity of the uterus ↑ space for cord to come down
Smaller fetal size
Fetus has not shifted into optimal delivery position
↑ space for fetus to move around in once first twin delivered
Placenta implanted near or over cervical opening
Large intrauterine space ↑ risk of mal- presentation
Abbreviations:
• PROM: Premature
The fetus does not adequately block the cervical opening Umbilical cord comes out through the cervix before the fetus does
Umbilical Cord Prolapse
Obstetrical emergency: Umbilical cord descends through the cervix before or alongside the fetus
Authors: Gabrielle Wagner Reviewers: Danielle Chang, Crystal Liu, Yan Yu*, Aysah Amath* * MD at time of publication
membranes
• PPROM: Preterm premature
rupture of membranes
Visible or palpable umbilical cord
Cord compression
Presenting part of the fetus compresses the cord as the fetus descends through the birth canal
Umbilical vasospasm
Exposure of the cord to cold or touch causes arterial vasospasms within the cordà↓ blood flow to fetus
Ante/intrapartum
Fetal hypoxia Post-Partum
Neonatal hypoxic-ischemic Cerebral Neonatal encephalopathy palsy death
Complicated variable fetal Prolonged fetal heart rate decelerations bradycardia
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published February 17, 2020 on www.thecalgaryguide.com")
mechanisms-of-opioid-analgesia-in-the-peripheral-nervous-system

Exogenous
Opioids derived from external source
Semi-synthetics
Synthesized from natural sources (ex. heroin)
Synthetics
Entirely created via synthesis (ex. fentanyl)
Endogenous
Opioids produced naturally in the body
Released in response or in anticipation of to painful stimuli
Endorphins
Enkephalins
Dynorphins
Inhibition of adenyl cyclase
↓ conductance of presynaptic Ca2+ channels
↑ conductance of postsynaptic K+ channels
↓Activity and production of cAMP
Activation of G- protein coupled receptors
↓ neuro- transmitter release
Inhibition of postsynaptic neuron
Blockage of nerve transmission
Binding to opioid receptor subtypes in nervous tissues mu (μ), kappa (k) delta (δ) - Majority of clinically relevant analgesic effects relate to mu (μ) receptor
↓ Release of Substance P and Glutamate in the dorsal horn of spinal cord
↓ Peripheral nociceptive signaling to thalamus and other brain areas
Inhibition of pain transmission to brain
Inhibition of GABA- releasing neurons in Periaqueductal grey (PAG) area
Activation of descending inhibitory pathways from PAG
Other/Systemic Side Effects
(For complete list and mechanism see Calgary Guide – Side effects of Opioids
Abbreviations:
cAMP (cyclic Adenosine mono-phosphate) – Cellular signaling molecule
GABA (gamma-Aminobutyric acid) – Inhibitory neurotransmitter
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 4, 2020 on www.thecalgaryguide.com")
pharmaceuticals-under-investigation-by-who-for-treating-covid-19-proposed-mechanisms
:
Yan Yu*, Stephen Vaughan*
* MD at time of publication
Note: This slide is based on literature available up to 03/30/2020. Medicines shown here are those included in the WHO SOLIDARITY trial, which were selected based on in vitro work and clinical data from MERS and SARS. Mechanisms are preliminary and there is insufficient data to support or refute the use of these agents for COVID- 19. Research is ongoing.
Viral replication is terminated
Fewer new cells infected
↓ activation of inflammatory and immune responses
Improvement or halt in progression of clinical signs of infection*
*See slide on pathophysiology and clinical findings of COVID19
Proposed Mechanisms
COVID-19 Viral Replication Pathway
Virus adheres to Angiotensin Converting Enzyme 2 (ACE-2) receptor on body cells
Endocytosis of virus in clathrin coated vesicles
Vesicles mature through endolysosomal pathway
Virus membrane fuses with mature endolysosome releasing viral RNA into cytosol
Viral RNA uses host cell ribosomes to make new viral proteins like RNA-polymerase
Viral RNA-polymerase incorporates nucleotides from the host cell
New viral RNA is produced
Viral RNA and proteins packaged into new viral particles
Viral particles released from cell
Chloroquine or Hydroxychloroquine (CQ, HCQ)
Weak basicity leads to ↑ pH of endosomes and lysosomes
N-terminal glycosylation of ACE-2 in Golgi is inhibited
Abnormal ACE-2 receptor expressed on cell surface
Viral membrane cannot fuse with immature endosome
Altered virus- ACE-2 interaction impairs entry into host cell
Viral contents are not released
Interferon-β (IFNβ) (Given with LPV/RTV)
Ritonavir (RTV)
(given with LPV)
Inhibition of CYP450, a drug metabolizing enzyme
↓ degradation of Lopinavir (LPV)
↑ plasma half life and duration of action of LPV
Binding to interferon receptor
Impaired maturation of endosomes
Activation of JAK/STAT pathway
Transcription of IFN- regulated genes
↑ expression of antiviral and immunomodulatory proteins
Antiviral effects may ↑ response to LPV/RTV (mechanism uncertain)
Remdesivir (RDV)
RDV is phosphorylated to RDV-triphosphate (RDV-TP)
Lopinavir (LPV)
Inhibition of viral 3- chymotripsin-like protease
Inhibition of viral replication (multiple mechanisms)
RDV-TP competes with ATP for binding to viral RNA polymerase
Viral protein precursors are not cleaved into mature viral proteins
Incorporation of RDV-TP terminates growing RNA
Newly formed viral particles can’t infect new cells
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published March 30, 2020 on www.thecalgaryguide.com")
GI-changes-during-pregnancy
 Tract
Pregnancyàhormonal and physical changes in the body
Mechanisms poorly understood
↑ human chorionic ↑ estrogen ↑ progesterone gonadotropin (hCG)
↑ uterus size
Uterus rises into
abdominal cavity
↑ intra-gastric pressure
↑ backup of stomach contents
Nausea & vomiting
In the extreme case:
Hyperemesis gravidarum (extreme vomiting causing weight loss, dehydration, ketosis)
Liver displaced upwards
Liver edge generally not palpable on exam
↑ blood pressure in veins within the abdomen
Veins around rectum & anus stretch under pressure
↑ blood flow to the gum tissue
↑ tendency for gingival bleeding & ulceration
Gingivitis
↑ neo- vascularization in lesions on skin
Pyogenic granuloma of pregnancy (shiny red papule with a raspberry-like surface)
Mechanism poorly understood
Ptyalism (excessive salivation)
Difficulty swallowing excess saliva
↑ gallbladder stasis
Biliary
sludge given time to solidify within gallbladder
Gallstones
↓ mobilization of intracellular calcium within smooth muscle cells
Smooth muscle relaxation in tissues such as the gallbladder & GI tract
Changes in taste perception
Dysgeusia
Cultural influences and psychological factors
Change in diet and dietary cravings
↓ lower esophageal sphincter tone
Retrograde transport of gastric contents into esophagus
Gastroesophageal reflux
↓ GI motility
Delayed gastric and intestinal emptying
Stool builds up in colon, and hardens as water is resorbed
Constipation
Pooling of blood within rectal veins àvenous thrombosis
Hemorrhoids
Fragile veins, more easily torn
Rectal bleeding
Change in gut microbiome
Authors: Simonne Horwitz, Yan Yu*
Reviewers: Claire Lothian, Crystal Liu, Ronald Cusano* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published April 29, 2020 on www.thecalgaryguide.com")
Fecal-Incontinence

↓ anal resting tone
Aging:
Degene- ration of muscle fibers
Movement disorders (e.g. arthritis, Parkinson’s); aging is a risk factorà ↓ mobility
↓ timely access to bathrooms
Inflammation
of colon (e.g., Ulcerative colitis, Radiation proctitis)
↓ capacity of
rectal smooth muscle to stretch
↓ capacity to store stool
↑ urgency of defecation
↑ reflex relaxation of internal anal sphincter
Chronic diarrhea, diarrhea- predominant irritable bowel syndrome, laxatives
Yan Yu* Erika Dempsey* * MD at time of publication
Stretch injury of Pelvic surgery
Chronic constipation
Build up of solid, immobile mass of stool in the rectum
Loose stool is able to flow around impacted stool, exiting anal canal (overflow diarrhea)
Sensory neuro- pathy (e.g. Diabetes)
Altered
mental conditions (e.g. stroke, dementia)
pudendal nerve (innervating the pelvic muscles and external anal sphincter)
Local neuronal damage
Impaired pelvic muscle and external anal sphincter motor control
Pelvic trauma
Rectal prolapse
Direct external anal sphincter impairment
↑ Stool volume
↑ Loose stools
Rectal hyposensitivity (↓ perception of rectal distension)
Patient fails to sense rectal fullness and voluntarily releases their external anal sphincter
Voluntary external anal sphincter contraction is no longer sufficient in closing the anus
Loose stool is more prone to escape through anal canal compared to solid stool
Continence mechanisms are impaired
Fecal Incontinence: The unintentional loss of solid or liquid stool
Skin Skin
Continence mechanisms are intact, but overwhelmed or ignored
infection Skin erythema
erosion
Inability to control what is widely considered a basic, fundamental bodily process
↑ caretaker burden Social stigma
↑ skin contact with acidic irritant (stool)
↑ rate of institutionalization, (e.g., admission into long-term care)
↓ confidence, sense of agency
↑ stress, anxiety
Skin inflammation
↓ social activity, work ↓ help-seeking ↓ treatment
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 2, 2020 on www.thecalgaryguide.com")
Placenta-Previa

• If patient presents with bleeding, a pelvic exam = risk of damaging placentaàmore bleeding
• Use transvaginal ultrasound to confirm location of placenta
Previous C/S Multiple gestation Maternal smoking
Placenta Previa
Presence of placental tissue that extends over the internal cervical os. (Pathogenesis unknown; preceding textboxes are risk factors only)
Previous placenta previa Increased maternal age Increased parity
Total placenta previa
Placenta completely covers the cervix
Partial placenta previa
Placenta covers cervix partially
Marginal placenta previa
Placenta near the edge of the cervix
Diagnosed early in pregnancy on routine abdominal ultrasound at 18-20 weeks Stretching of lower segment of uterus during 3rd trimester
OR
Alternate scenario:
One scenario:
This stretching elongates the space between the cervix and the placenta, relocating the stationary lower edge of the placenta away from the cervical os
Placenta previa resolves on its own
Reassuring: Placenta >2cm from cervical os on ultrasound
This stretching fails to move the placental away from the cervical os
Previa persists as uterus changes in preparation for labour:
Thinning of the lower segment of the uterus
Uterine contractions
Shearing forces to the placental attachment site
Painless bright red vaginal bleeding (90%)
↑ risk of clinically significant hemorrhage
Cervix becomes thinner (effaced) and opens (dilates)
Bleeding limits oxygen delivery to placenta, injuring placental tissue
Tissue injuryàActivates intracellular G-protein signalling pathways
Release of stored intracellular calcium àmyometrial contraction
Uterine contraction and bleeding (10%)
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 2, 2020 on www.thecalgaryguide.com")
Humoral-Immunity
 or circulate in the blood
Memory B cells proliferate and differentiate into plasma cells in response to re- exposure to antigen
↑ Rate and amplitude of secondary immune response on repeat exposure
Antigens (Ag) are produced from pathogens (bacteria, viruses, fungi, parasites) or the patient (via trauma, tumor, metabolism), & circulate in plasma, lymph, or other tissue
Clonal expansion
(proliferation of the activated B cells)
↑ WBCs (lymphocytosis) Autoimmune disease if B
cells recognize self-antigen
T cell-dependent Ag:
Ag-presenting cells (such as dendritic cells or macrophages) present Ag to CD4+ helper T cells and activate them. Activated helper-T cells then stimulate B cells
T cell-independent Ag:
Ags such as peptides, carbohydrates and lipids
may be directly recognized by B cells, triggering their activation
Complement:
Circulating serum complement proteins detect and bind Ag. Ags tagged with C3 complement fragment bind B cell co-receptor complex and enhance B cell activation.
Abbreviations:
Ab – Antibody
Ag – Antigen
Ig – Immunoglobulin WBC – White Blood Cell
Naïve B cells
Activated B cells
(in secondary lymphoid organs, such as the spleen or lymph nodes)
Plasma cells first produce IgM
Cytokines and T cells stimulate Ig class switching of B cells (changing the heavy chain constant regions of the Ig molecule)
Ig production switches from IgM to IgG, IgA, IgE, or IgD
IgG is the most common Ig in immune reactions. IgA concentrates at mucosa, IgE degranulates mast cells, IgD helps mature B cells.
Differentiation (into memory B cells or plasma cells)
Plasma cells produce antibodies, which contribute to immunity in 3 ways:
Opsonization: Abs coat pathogens, helping recognition by phagocytes
Neutralization: Abs bind to pathogen surface molecules that are needed to invade host cells, thereby neutralizing them
Activate Complement: Abs activate complement proteins via the classical pathway (see Complement Activation slide)
Clearance of pathogen by adaptive immune response
↑ Serum Ig
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 2, 2020 on www.thecalgaryguide.com")
Diabetic-Nephropathy

↑ Intrarenal angiotensin II
↑ Advanced glycation end products (AGE)
Shunting of glucose through non- glycolytic pathways (e.g. polyol)
Activation of Protein Kinase C (PKC) pathway
Excessive production and accumulation of glycolytic intermediates (e.g. sorbitol, hexosamine, succinate)
hyperglycemia
Succinate via GPR91
↑ Free radical production (oxidative stress)
Activation of cellular signalling, transcription factors and cytokines (e.g. TGF-β-Smad-MAPK, IGF-1, NF-κB)
↑NADPH oxidase activity
↑Blood volume ↑ Blood pressure ↑ Renal perfusion
Relative afferent arteriole dilatation, efferent arteriole constriction
Initial ↑ in glomerular filtration rate (GFR)
Podocyte loss/injury
Authors: Steven Chen Shannon Gui Yan Yu* Reviewers: Julia Heighton Ryan Brenneis Sophia Chou* * MD at time of publication
Initial glomerular hyperfiltration at time of diagnosis
↓ Production of matrix metallo- proteinases
Aberrant extracellular matrix (ECM) protein expression and accumulation
Sheer stress to glomeruli à pressure-induced damage
↑ Glomerular basement membrane permeability to proteins like albumin
↓ Extracellular matrix regulation
“Metabolic Pathway”
Mesangial matrix expansion
Kimmelstiel-
Wilson lesions (pink
hyaline nodules due to accumulation of damaged proteins)
Tubular fibrosis
Scarred glomeruli are less able to effectively filter blood
↓ in glomerular filtration rate (GFR)
Albuminuria
Usually occurs after ~5 years from time of diagnosis in T1DM; can occur at time of diagnosis in T2DM
Abbreviations
IGF: Insulin-like growth factor
MAPK: Mitogen-activated protein kinases NADPH: Nicotinamide adenine dinucleotide phosphate
NF-κB: Nuclear factor kappa-light-chain- enhancer of activated B cells
TGF-β: Transforming growth factor-β
Protein endocytosis into tubular cells causing inflammation
“Hemodynamic Pathway”
Diabetic Nephropathy
Overt diabetic nephropathy may take upwards of 15-25 years to develop
Note: The mechanisms presented here have been simplified. The cross- talk and signaling between the metabolic and hemodynamic factors do not manifest in a step-wise fashion, but rather occur in parallel.
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published May 3, 2020 on www.thecalgaryguide.com")
Infarctus du myocarde: Antécédents médicaux

Auteur: Yan Yu Traductrice: Olivia Genereux Réviseurs: Sean Spence Tristan Jones Nanette Alvarez* Marie Giroux* *MD au moment de publication
Sang du ventricule gauche reflue à l’oreille[e gauche et finalement s'accumule dans le système vasculaire pulmonaire
Haute pression du système vasculaire pulmonaire force fluide hors des capillaires et dans l'interstitium pulmonaire et les alvéoles
Inflammation myocardique locale
Médiateurs inflammatoires irritent les nerfs cardiaques (plexus cardiaque)
̄ Fonc8on systolique (myocarde nécro6que ne peut pas se contracter suffisamment)
Invasion généralisée des cytokines inflammatoires
Cytokines agissent les régulateurs de température hypothalamique
Fièvre légère
Irritation des nerfs sympathiques afférents (T1-T4)
Signal entre moelle épinière, a/n dermatomes T1-T4
Cerveau perçoit irritation des nerfs comme douleur des dermatomes T1-T4
Douleur écrasante, pression, oppression de la poitrine: Souvent rétrosternale, avec radiation à épaule, cou et l'intérieur des deux bras (D>G) (Apparition: au repos, crescendo)
IrritaNon des branches cardiaques du nerf vague
AcNvaNon réponse vasovagale
Fatigue, étourdissements, nausée, vomissement
↓ volume systolique (VS) ↓ debit cardiaque (DC)
Activité sympathique (pour essayer de maintenir DC)
Sueurs (diaphorèse)
Peau moite
VasoconstricNon généralisé
Vasoconstriction des artérioles de peaux
Peau froide
Interstitium
pulmonaire
mou ↓
compliance
pulmonaire
d
Fluide compresse les voies respiratoires, ↑ résistance au flux d’air
Abrévia8ons:
• a/n – au niveau
À Noter: Douleur myocardique ischémique peut présenter différemment entre les patients, mais les symptômes récurrents habituellement présentent les mêmes pour un patient donné.
Muscles respiratoires travaillent plus fort pour venNler les poumons
Essoufflement
(difficulté à respirer)
Légende:
Physiopathologie
Mécanisme
Signe/Symptôme/Résultats de Laboratoire
Complications
Publié Janvier 20, 2013 sur www.thecalgaryguide.com")
Marfan-Syndrome

Dural ectasia
(widening of the dural sac)
Diminished and disorganized dural elastic fibres
Abnormalities in connective tissues
Tear in the aortic intima (innermost layer of aorta)
Aortic dissection
Type A (tear in ascending aorta) > Type B (tear in descending aorta)
Back pain
Sensory and motor deficits
Ectopia lentis
(lens dislocation)
Development of lung bullae and blebs
Rupture of bullae/blebs
Pneumothorax
** Abnormal properties of lens + cornea
** Scoliosis
** Myopia
Tall stature Chest wall (pectus)
Inherited (autosomal dominant) or de novo mutation in FBN1 gene
Distortion of neural roots
Thinning of ciliary zonules of the eye
Weakness and rupture of alveolar tissue
Production of aberrant or reduced fibrillin-1
Formation of unstable microfibrils in extracellular matrix of connective tissues
**
inactivate TGF-β1
↑ production of matrix metalloproteinases
↑ cellular signaling cascades
↑ production of growth factors in the endocardium
Cell proliferation and apoptosis suppression in mitral valve leaflets
Change in valvular architecture
Mitral prolapse
Mitral regurgitation
↑ degradation of extracellular matrix
Thinning of the aortic media
Weakness of the aortic wall
Inability of fibrillin- 1 to sequester and
↑ TGF-β1 signalling
Abbreviations
• TGF-β: Transforming
growth factor beta (a cytokine)
Notes
**The underlying
mechanisms are unclear
Authors:
Tony Gu Reviewers: Amanda Nguyen Davis Maclean Yan Yu* Michelle Keir*
* MD at time of publication
Aortic root dilation
Aortic valve leaflets stretched outwards, unable to fully close
Aortic regurgitation
Aneurysmal dilation of the abdominal & thoracic aorta
Aortic rupture
Stroke
Blood enters and pressurizes a ‘false lumen’
Obstruction of aortic branches
End organ malperfusion
** deformities
** Joint hypermobility
Thumb sign: Thumb tip extends from palm of hand when thumb is folded into closed wrist
Wrist sign: thumb and fifth finger of the hand overlap when grasping opposite wrist
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published June 28, 2020 on www.thecalgaryguide.com")
GU-changes-in-pregnancy

Mechanism unclear, possibly 1) ↑ circulating anti- angiogenic factorsà ↑ permeability of glomerular basement membrane, or 2) ↑ plasma volumeà↓ oncotic pressure of plasma at the glomerulus
Proteinuria
> 300 mg/day, abnormal in pregnancy
↑ hCG level
Dilation of renal vasculature
↑ renal vascular & interstitial volume
↑ filtration surface area
Overwhelming load of glucose to proximal tubule
↑ urine output
↑ relaxin secreted by placenta
Mechanism not well understood
↓ osmotic threshold for ADH release & thirst
↑ ADH secretion & ↑ oral hydration
Incomplete reabsorption of glucose
Glucosuria
Encourage bacterial growth in the urine
Urinary tract infection (e.g. cystitis, pyelonephritis)
↑ serum progesterone
Uterine rotation as uterus enlarge due to presence of large bowel
Ureter compression (R > L)
Ureterovesical reflux (back-flow of urine into the ureters/kidneys)
Dilatation of ureters (R > L) (hydroureter) & renal pelvis (hydronephrosis)
Progesterone competes with aldosterone
↓ sodium reabsorption
↓ plasma sodium concentration
Hyponatremia of pregnancy* (pathological if < 130 mEq/L)
*Despite factors favoring sodium excretion, there is a net retention of sodium during pregnancy from adaptation of the renal tubules
↑ urinary stasis
↑ excretion of creatinine and urea in urine
↓ serum creatinine and urea
↓ ureteral toneà ↑potential for ureter dilation
Mechanism not well understood
↓ peristalsis of ureters
↑ urinary frequency (voiding > 7x/day)
↑ nocturia (voiding ≥ 2x/night)
↓ oncotic pressure of plasma intra-vascularly àwater leaves blood, enters interstitial tissue, and stays there in gravity-dependent regions of the body
Pedal +/- ankle edema
Author: Simonne Horwitz Reviewers: Claire Lothian, Crystal Liu, Ronald Cusano*, Candace O’Quinn*, Yan Yu* * MD at time of publication
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published June 28, 2020 on www.thecalgaryguide.com")
Retinal-Detachment-Pathogenesis
 e.g. macular degeneration
Formation of fibrous tissue bands in vitreous cavity
Bands contract and exert a tractional (pulling) force on the retina
Retina is pulled off the choroid layer at the back of the eye by tractional forces, without a retinal tear
Tractional Retinal Detachment (TRD):
Retina is pulled off the choroid layer at the back of the eye in the absence of retinal tears
Posterior Vitreous Detachment
For complete pathogenesis and clinical findings see: Calgary Guide – Posterior Vitreous Detachment: Pathogenesis and Clinical Findings
Note: Not every retinal tear leads to retinal detachment
Parts of the gel- like vitreous humour detach from the retina
↑ Age
Vitreous gel liquification
Vascular Damage Optic disc Anomalies Degenerative Conditions
During rotational eye movement, the vitreous humour moves within the vitreous cavity
Strong tractional forces transmitted to retina through remaining attachments
Retinal Tear: Physical defect in the retina associated with vitreous traction
Defect held open by vitreoretinal traction
Defect in retina allows vitreous fluid to gain access into sub retinal space
Tumour/ Malignancy
Idiopathic
Rhegmatogenous Retinal Detachment (RRD): Accumulation of sub retinal fluid due to a tear in the retina allowing liquid vitreous gel to get underneath the retina
Separation of the retina from choroid layer at the back of the eye
Inflammatory/Infectious Conditions
↑ Permeability of choroid or retinal blood vessels
Fluid leaks out of retinal/choroid blood vessels
Accumulation of fluid beneath retina and without retinal tear or vitreous traction
Exudative Retinal Detachment (ERD):
Fluid accumulation in subretinal space in the absence or tears or traction from the vitreous
Retinal Detachment:
Sight threatening condition, considered ocular emergency
See Calgary Guide slide: Retinal Detachment: Clinical findings
Legend:
Pathophysiology
Mechanism
Sign/Symptom/Lab Finding
Complications
Published July 11, 2020 on www.thecalgaryguide.com")