
Exchangeable Zinc Pool Size Reflects Form of Zinc Supplementation in Young Children and Is Not Associated with Markers of Inflammation

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
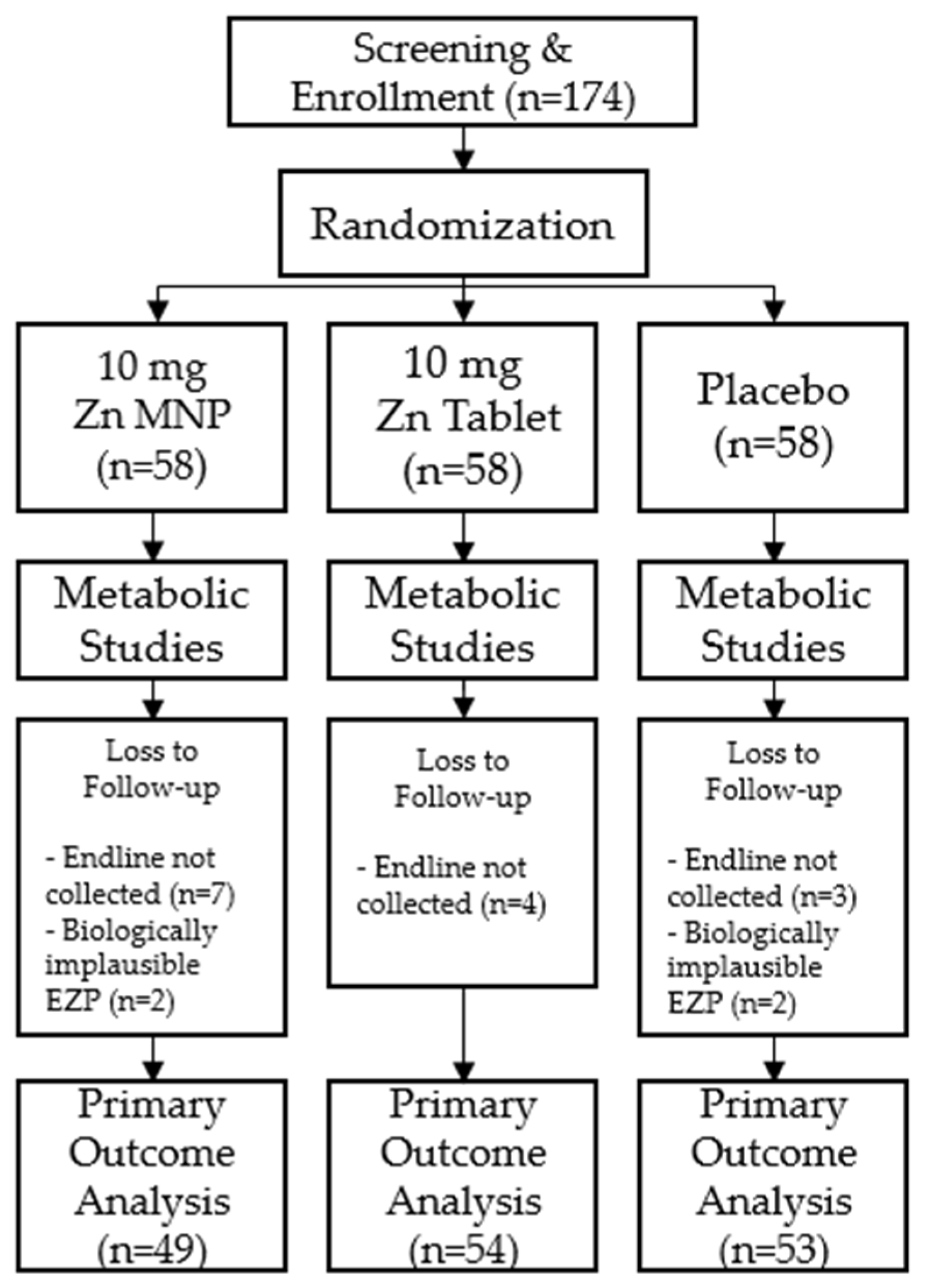
2.1. Study Design
2.2. Participants
2.3. Power and Sample Size
2.4. Intervention
2.5. Preparation and Administration of IV Zinc Isotopes
2.6. Sample Collections
2.7. Sample Analyses
2.8. Data Calculations and Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- King, J.C.; Brown, K.H.; Gibson, R.S.; Krebs, N.F.; Lowe, N.M.; Siekmann, J.H.; Raiten, D.J. Biomarkers of Nutrition for Development (BOND)-zinc review. J. Nutr. 2016, 146, 858S–885S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, L.V.; Hambidge, K.M.; Naake, V.L.; Hong, Z.; Westcott, J.L.; Fennessey, P.V. Size of the zinc pools that exchange rapidly with plasma zinc in humans: Alternative techniques for measuring and relation to dietary zinc intake. J. Nutr. 1994, 124, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Krebs, N.F.; Westcott, J.E.; Culbertson, D.L.; Sian, L.; Miller, L.V.; Hambidge, K.M. Comparison of complementary feeding strategies to meet zinc requirements of older breastfed infants. Am. J. Clin. Nutr. 2012, 96, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, L.; Long, J.; Mondal, P.; Westcott, J.; Islam, M.M.; Ahmed, M.; Ahmed, T.; Krebs, N. Exchangeable Zinc Pool (EZP) size in Bangladeshi toddlers at risk of environmental enteric dysfunction (EED) is not influenced by inflammation (OR07-03-19). Curr. Dev. Nutr. 2019, 3 (Suppl. 1), nzz034.OR07-03-19. [Google Scholar] [CrossRef] [Green Version]
- Miller, L.V.; Hambidge, K.M.; King, J.C.; Westcott, J.E.; Krebs, N.F. Predictors of the size of the exchangeable zinc pool differ between children and adults. J. Nutr. 2017, 147, 187–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, M.M.; McDonald, C.M.; Krebs, N.F.; Westcott, J.; Rahman, A.E.; El Arifeen, S.; Ahmed, T.; King, J.C.; Black, R.E. Study protocol for a randomized, double-blind, community-based efficacy trial of various doses of zinc in micronutrient powders or tablets in young Bangladeshi children. Nutrients 2018, 10, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, M.M.; Black, R.E.; Krebs, N.F.; Westcott, J.; Long, J.; Islam, K.M.; Peerson, J.M.; Sthity, R.A.; Khandaker, A.M.; Hasan, M.; et al. Different doses, forms, and frequencies of zinc supplementation for the prevention of diarrhea and promotion of linear growth among young Bangladeshi children: A six-arm, randomized, community-based efficacy trial. J. Nutr. 2022, nxab439. [Google Scholar] [CrossRef] [PubMed]
- Ariff, S.; Krebs, N.F.; Soofi, S.; Westcott, J.; Bhatti, Z.; Tabassum, F.; Bhutta, Z.A. Absorbed zinc and exchangeable zinc pool size are greater in Pakistani infants receiving traditional complementary foods with zinc-fortified micronutrient powder. J. Nutr. 2014, 144, 20–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, J.M.; Mondal, P.; Westcott, J.E.; Miller, L.V.; Islam, M.M.; Ahmed, M.; Mahfuz, M.; Ahmed, T.; Krebs, N.F. Zinc absorption from micronutrient powders is low in Bangladeshi toddlers at risk for environmental enteric dysfunction (EED) and may increase dietary zinc requirements. J. Nutr. 2019, 149, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Erhardt, J.G.; Estes, J.E.; Pfeiffer, C.M.; Biesalski, H.K.; Craft, N.E. Combined measurement of ferritin, soluble transferrin receptor, retinol binding protein, and C-reactive protein by an inexpensive, sensitive, and simple sandwich enzyme-linked immunosorbent assay technique. J. Nutr. 2004, 134, 3127–3132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The R Foundation for Statistical Computing Platform: x86_64-apple-darwin17.0 (64-bit), 4.0.2; Vienna, Austria. 2020. Available online: https://www.r-project.org/ (accessed on 20 November 2021).
- Mondal, P.; Long, J.M.; Westcott, J.E.; Islam, M.M.; Ahmed, M.; Mahfuz, M.; Ahmed, T.; Miller, L.V.; Krebs, N.F. Zinc absorption and endogenous fecal zinc losses in Bangladeshi toddlers at risk for environmental enteric dysfunction. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 874–879. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Panel on Micronutrients. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press: Washington, DC, USA, 2001.
- Greffeuille, V.; Fortin, S.; Gibson, R.; Rohner, F.; Williams, A.; Young, M.F.; Houghton, L.; Ou, J.; Dijkhuizen, M.A.; Wirth, J.P.; et al. Associations between zinc and hemoglobin concentrations in preschool children and women of reproductive age: An analysis of representative survey data from the Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) Project. J. Nutr. 2021, 151, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- McDonald, C.M.; Suchdev, P.S.; Krebs, N.F.; Hess, S.Y.; Wessells, K.R.; Ismaily, S.; Rahman, S.; Wieringa, F.T.; Williams, A.M.; Brown, K.H.; et al. Adjusting plasma or serum zinc concentrations for inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 2020, 111, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Liuzzi, J.P.; Lichten, L.A.; Rivera, S.; Blanchard, R.K.; Aydemir, T.B.; Knutson, M.D.; Ganz, T.; Cousins, R.J. Interleukin-6 regulates the zinc transporter Zip14 in liver and contributes to the hypozincemia of the acute-phase response. Proc. Natl. Acad. Sci. USA 2005, 102, 6843–6848. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| 10 mg Zn MNP (n = 49) | 10 mg Zn Tablet (n = 54) | Placebo (n = 53) | |
|---|---|---|---|
| Sex, % male | 48% | 48% | 51% |
| Age, mo | 9.4 (1.1) | 9.2 (1.1) | 9.5 (1.0) |
| Length, cm | 68.7 (2.5) | 69.1 (2.8) | 68.8 (2.7) |
| Weight, kg | 7.6 (0.9) | 8.0 (1.1) | 7.7 (1.0) |
| Length-for-age z-score | −1.5 (1.0) | −1.2 (1.1) | −1.5 (1.1) |
| Weight-for-age z-score | −1.3 (1.0) | −0.9 (1.1) | −1.2 (1.1) |
| Weight-for-length z-score | −0.7 (0.9) | −0.3 (1.0) | −0.5 (1.0) |
| 10 mg Zn MNP (n = 49) | 10 mg Zn Tablet (n = 54) | Placebo (n = 53) | p-Value | |
|---|---|---|---|---|
| Baseline | ||||
| EZP, mg | 37.7 (6.2) | 38.0 (7.8) | 35.6 (7.8) | 0.190 |
| EZP, mg/kg | 5.0 (0.7) | 4.9 (1.1) | 4.6 (0.9) | 0.074 |
| Serum zinc, µg/dL * | 71.5 (10.0) | 67.3 (13.2) | 69.9 (15.6) | 0.266 |
| AGP, g/L * | 0.7 (0.4) | 0.8 (0.5) | 0.7 (0.4) | 0.292 |
| CRP, mg/L * | 1.4 (3.0) | 2.2 (5.4) | 0.9 (1.8) | 0.205 |
| Endline | ||||
| EZP, mg | 44.5 (13.4) a | 52.1 (16.5) b | 37.6 (9.1) a | <0.0001 |
| EZP, mg/kg | 5.3 (1.6) a | 5.9 (1.9) b | 4.4 (1.0) a | <0.0001 |
| Serum zinc, µg/dL ** | 83.1 (16.3) a | 95.5 (22.1) b | 74.2 (16.2) a | <0.0001 |
| AGP, g/L *** | 0.8 (0.4) | 0.7 (0.3) | 0.8 (0.4) | 0.367 |
| CRP, mg/L *** | 1.8 (4.1) | 2.0 (4.5) | 2.4 (4.5) | 0.783 |
| Δ EZP, mg | 6.8 (14.3) a | 14.1 (14.7) b | 2.7 (10.6) a | <0.0001 |
| Δ EZP, mg/kg | 0.3 (1.8) a | 1.1 (1.9) b | −0.2 (1.2) a | 0.0004 |
| Δ Serum zinc, µg/dL**** | 15.1 (27.4) a | 28.2 (25.0) b | 4.4 (18.3) a | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Long, J.M.; Khandaker, A.M.; Sthity, R.A.; Westcott, J.E.; Matveev, A.; Black, R.E.; King, J.C.; Islam, K.M.; El Arifeen, S.; Ahmed, T.; et al. Exchangeable Zinc Pool Size Reflects Form of Zinc Supplementation in Young Children and Is Not Associated with Markers of Inflammation. Nutrients 2022, 14, 481. https://doi.org/10.3390/nu14030481
Long JM, Khandaker AM, Sthity RA, Westcott JE, Matveev A, Black RE, King JC, Islam KM, El Arifeen S, Ahmed T, et al. Exchangeable Zinc Pool Size Reflects Form of Zinc Supplementation in Young Children and Is Not Associated with Markers of Inflammation. Nutrients. 2022; 14(3):481. https://doi.org/10.3390/nu14030481
Chicago/Turabian StyleLong, Julie M., Afsana Mim Khandaker, Rahvia Alam Sthity, Jamie E. Westcott, Andrei Matveev, Robert E. Black, Janet C. King, Kazi Munisul Islam, Shams El Arifeen, Tahmeed Ahmed, and et al. 2022. "Exchangeable Zinc Pool Size Reflects Form of Zinc Supplementation in Young Children and Is Not Associated with Markers of Inflammation" Nutrients 14, no. 3: 481. https://doi.org/10.3390/nu14030481