

I. Executive summary
1. Potential reintroduction of restrictions in Autumn and Winter 2021 would occur in a different context from their prior use: higher population level immunity from vaccinations, potential waning immunity for those vaccinated early, dominance of Delta variant, end of furlough scheme and areas of enduring transmission that have experienced disproportionate health, mortality and economic impacts.
2. Examining 12 behavioural interventions across 30 countries, there was no sign of decline in effectiveness (measured by cases, hospitalisations, deaths) of interventions when they were reintroduced for a second or third time. This suggests that reintroduction could be effective, albeit in a different context as noted above. [medium confidence]
3. There has been a drop in all self-reported COVID-19 behavioural interventions, particularly wearing a face covering, avoiding contact and physical distancing. [medium confidence] If measures are reintroduced, clear communications are required, setting out the rules, benefits of adherence and responsibility for enforcement.
4. We reiterate SPI-B advice on the need for people to have ongoing capability, opportunity and motivation to engage in sustained behaviours that are Normal, Easy, Attractive and Routine (NEAR). [footnote 1] [footnote 2] Co-production and extensive stakeholder engagement is critical to the success of interventions. [footnote 1] [footnote 3]
Face coverings
5. A large body of evidence demonstrates the effectiveness of face coverings in reducing transmission and to a lesser extent protecting the wearer (see EMG Consensus statement, SAGE 96). [high confidence] There is public confusion regarding effectiveness and required settings, and who is responsible for enforcement. If introduced, there are potentially higher demands on police and businesses, which may lead to lack of compliance and confrontations. [medium to low confidence]
6. Clear face covering regulations could focus on: a) settings where they are required; b) explicit definition of settings (defining for example, what constitutes a crowded indoor space); c) the settings where face coverings are mandatory or voluntary, d) who will be responsible for enforcing regulations; and, e) implications of lack of adherence (for example, health, financial).
7. Communications regarding reintroduction of face coverings would benefit from a focus on a to d above in addition to: a) emphasising updated scientific evidence on effectiveness, b) clarifying how and why they work; and, c) reiterating correct usage and which face coverings are effective.
8. Some members of the public may resist reintroduction of mandatory face coverings and changing perceptions of risk may empower anti-authoritarian narratives or prompt public protests. Making something mandatory shapes risk perception and would enhance legitimacy for those requiring them as a condition of entry. [medium confidence] It would also create expectations for public figures serving as role models to demonstrate adherence in the required settings.
Vaccine certification
9. Several criteria are to be considered before introducing COVID-19 certification, including that it: meets benchmarks for immunity; accommodates differences in efficacy between vaccines and emerging variants; has clearly defined uses; is internationally standardised; is based on a platform of interoperable technologies; keeps personal data secure; meets legal and ethical (equity and non-discrimination) standards; is portable and affordable for individuals, businesses and governments; and that conditions of use are understood and accepted by certificate holders. [footnote 4] [footnote 5]
10. Public opinion regarding certification varies by the setting in which it is introduced and related to trust, with lower support in poorer communities, some ethnic groups or those with vaccine scepticism. [medium confidence] If introduced, it would be important to be explicit about the specific settings in which certification will be used and who is exempted. Clarification regarding who will enforce certification is important as it places potential heavy burdens on public-facing staff and police and creates dynamics that amplify social tensions or unlicensed events. International examples show ensuring sufficient time for those implementing certification could ease their introduction.
11. A primary analysis for this paper examined the impact of introducing COVID-19 certification on vaccine uptake. [footnote 6] Mirroring an RCT, the model compared 6 countries (Denmark, Israel, Italy, France, Germany, Switzerland) that introduced certification (May to August 2021), with 20 control countries. Estimates provide a counterfactual trend of what would have happened in virtually identical circumstances if certificates were not introduced on daily COVID-19 vaccine doses.
12. Data from an analysis of the international experience of certification suggests that if vaccine certification was introduced and tied to particular settings, it could increase vaccine uptake in certain groups. However, given already higher levels of uptake in older age groups (in comparison to France, Italy when certificates were introduced), the absolute impact would be smaller, tied more to greater than 20 seconds. [medium confidence] Targeted community-based vaccine interventions are likely to be more effective than certification for some lower socioeconomic and minority ethnic groups. [footnote 7] [footnote 8]
Advice to work from home (WFH)
13. WFH can be an effective measure to reduce infection, but measures and communications should recognise the ability to WFH exists for half of employees and varies according to occupation, socioeconomic status, demographic traits and regional variations in industry. [high confidence]
14. Communication and measures to reintroduce WFH could benefit from engagement with businesses and employers and acknowledge differences and inequalities to avoid provoking protest and resistance.
15. Given that many employees cannot WFH and lack autonomy to follow some behavioural guidelines, employers should provide clear guidance and encourage measures to ensure safety for those that remain in close proximity to workers, customers or patients (such as ventilation, distancing, face coverings). [footnote 9]
16. Employers should develop measures to cope with the potential of longer-term WFH implications of mental and physical health, work-life balance, and security and productivity concerns. WFH raises new policy and legal questions for employers related to health and safety, insurance, work organisation, data security and ambiguity in claims for the costs for the employee (such as, heating, internet). Coordination and support for business such as guidelines, fiscal support, inspections or enforcement could make them more likely to support and promote the introduction of restrictions for their employees.
Communicating risks to the public
17. Trust can increase or decrease willingness to engage with measures outlined in the Autumn and Winter plan. Trust is linked to the credibility of the communicator, with independent health professionals and experts garnering the highest levels. Trust increases when the public feels they are trusted to follow the guidance and not perceived as targeted or blamed. Positive media and political coverage will facilitate increased trust. [medium to high confidence]
18. Trust can be eroded by unclear and inconsistent messaging, government officials and role models not engaging in behaviours in line with guidance, interventions that unintentionally increase stigma for specific communities and not acknowledging the experiences of exclusion by some groups. [high to medium confidence]
19. Funding to support local communication campaigns aligned with national guidelines is beneficial. Programmes such as Community Champions programmes are well positioned to share messages about reintroducing restrictions and are responsive to new and unanticipated challenges. [medium confidence] This includes sharing information via trusted sources (healthcare professionals, community leaders and individuals embedded in networks such as schools, support groups and youth clubs) and engaging in a two-way dialogue to address specific concerns.
20. Messaging needs to be clear and agile to address the complex and changing situation, have a clear rationale, be tailored to address the informational needs of different groups and be consistent with role modelling by public figures on the behaviours being advocated.
21. Wearing face coverings is the most visible behaviour in the Autumn and Winter plan and if reintroduced should be modelled by government officials and role models to signal their importance and all measures included in the plan.
22. Specific guidance should be developed on how to reduce transmission in diverse household structures including large or multigenerational households. [footnote 10] [footnote 11]
Test and trace, adherence to self-isolation and staying at home when sick
23. Test and Trace, adherence to self-isolation and staying at home when sick with influenza-like illness is part of an array of interventions, alongside physical distancing and face coverings.
24. To increase uptake of the NHS COVID app, recent studies indicate that even minimal monetary incentives can be effective, and some messaging (such as video) has a limited effect. [footnote 12] [medium to high confidence]
25. Improving the current low rate of asymptomatic testing would require a concerted effort from Government and employers. Since 4 October 2021, a “collect code” is required to receive packs of lateral flow tests from the pharmacy. [footnote 13] The introduction of any barrier seems likely to reduce the number of people who access testing. [high confidence]
26. Given the likely increase in cold and flu symptoms in autumn and winter and difficulty for the public to distinguish between these symptoms and COVID-19 symptoms, maintaining or improving the proportion of people with COVID-19 who request a test will require clear communications. Communications should focus on what specific symptoms necessitate testing and encourage people to take an early test even for mild symptoms, regardless of whether an obvious transmission event has occurred. [medium to high confidence]
27. Clear communication of why it is important to stay at home when ill, even if a negative COVID-19 test result is obtained, may encourage and enable more people to take time off, reducing transmission. This is particularly likely to be effective if communication comes from multiple routes (including Government, employers, schools, universities) and if conducted as part of a series of strategies intended to support people to take time off when ill. [high confidence]
28. Ensuring people are aware they can access support and providing enhanced payments and practical support for people in lower income communities and precarious employment is likely to increase engagement with Test and Trace. [medium confidence]
II. Maintaining COVID-19 safe behaviours in Autumn and Winter 2021 and effectiveness of reintroduction of behavioural interventions
29. Since late July, the UK has had significantly higher reported infections than most European countries. In early October, cases are approximately 500 per million (pm), compared to approximately 50 (Spain), approximately 70 (France) and approximately100 (Germany) pm. [footnote 14] [footnote 15] Since early September, UK COVID-19 death rates are also higher (1.5 to 2 per million) compared to 0.5 to 1 pm in France, Spain, Germany respectively, but current UK death and hospitalisation rates are falling. [footnote 16] [high confidence]
30. The divergent UK trajectory is likely attributed to interrelated factors: (1) different pandemic trajectories (for example, Alpha, Delta variants); (2) England was the first nation in Europe to end most COVID-19 behavioural restrictions on 19 July, with others retaining restrictions on large gatherings, physical distancing, COVID-19 passports and mandatory masks; (3) most European countries now have higher vaccination levels, mostly attributed to the earlier vaccination of under 16s. Since September, high UK infection rates are driven by 0 to 19 years returning to school. [footnote 16] This is likely to level off with the vaccination programme and natural immunity. Given the predicted rise in flu viruses and difficulty for the public to distinguish symptoms, non-COVID-19 winter viruses could place considerable pressure on the NHS.
31. Reintroduction of restrictions as outlined in the Autumn and Winter 2021 plan will be implemented in a very different context. This includes vaccinations and higher population level immunity and strengthened partnerships between formal authorities and community organisations as a result of a nationally funded Community Champions scheme. [footnote 17] However, there are concerns related to the Delta variant or other emerging variants of concern, waning of immunity, timing of immunisation of children 12 and older and the end of the furlough scheme. New Zealand’s strategy, for instance of very strict lockdowns and measures worked well with only 27 deaths, but has been recently challenged by the Delta variant combined with comparatively low levels of vaccine uptake (roughly 48 per cent of eligible population with 2 doses). [footnote 18] If restrictions are reintroduced, they will also be in a context where some groups have experienced increased deprivation and financial hardship related to the pandemic, areas of enduring transmission where rates have been consistently higher than the national average, [footnote 19] and communities that have experienced disproportionately rates of COVID-19 and higher mortality. [footnote 20] [footnote 21]
Behavioural evidence
32. Previous SPI-B evidence in April 2021 regarding sustaining behaviours suggested that as restrictions eased, COVID-19 protective behaviours would not be sustained as restrictions were eased. [footnote 1] Data examining COVID-19 behavioural interventions has largely been from self-reported surveys, mobility and observational data. Using a daily sample of Facebook data (N= roughly 1,400 per day) in the UK, Figure 1 shows the percentage of individuals reporting COVID-19 related behaviours from 01 April to 22 September 2021. [footnote 22] We see relative stability, with the largest drops in wearing a face covering (mask) (from 81 per cent to 51 per cent), avoiding contact with others (86 per cent to 46 per cent) and seeing other people in a physically distanced manner (43 per cent to 17 per cent). An important caveat is that self-report may produce over-inflated estimates of some behaviours. [footnote 23] [footnote 24] [footnote 25] Although there is selectivity with the Facebook data, findings are broadly in line YouGov [footnote 26] and Ipsos Mori, [footnote 27] suggesting similar self-reported trends. Data from CCTV footage found that 39 per cent were reported to be wearing a face mask while travelling, [footnote 28] highlighting the importance of drawing from multiple types of data. [medium confidence]
33. Given the recent reintroduction of behavioural interventions in some countries, there is limited evidence. For this reason, we engaged in a primary analysis to examine the relationship between the introduction of 12 behavioural interventions (for example, school closing, testing, face coverings), for a first, second or third reintroduction with reported COVID-19 cases, deaths and hospitalisations, the latter being a rough proxy for effectiveness of measures. A description of the data, measures and analytical methods are included in Appendix 1, comparing 30 countries in Europe, USA, Canada and Israel.
Figure 1. Percentage of individuals reporting different behavioural measures, 1 April to 22 September 2021, United Kingdom.
Source: Figure produced by SPI-B authors from Facebook and University of Maryland data [footnote 22] as of 22 September 2021, UK.
34. Figure 2 plots daily reported COVID-19 cases in the time period surrounding the introduction of behavioural interventions for the first, second and third time. The comparability of each repeated intervention is limited by differences in reporting of cases in the early phases of COVID-19. Countries engaged in different testing procedures and some only started to report cases later, suggesting that the data will have underreporting for the first introduction. Moreover, some interventions – such as the closure of public transport, protection of the elderly or stricter testing policies – were only introduced once (or twice for a small number of countries) or were continuously maintained at a high level. Another caveat is that behavioural interventions are part of a complex ecosystem of behavioural measures that interact and are hence difficult to measure in isolation. [low to medium confidence]
35. Comparing the second and third reintroduction of different interventions, we observe similar patterns around school closing, workplace closing, stay at home rules, restrictions on gatherings, and mandatory face coverings. Figure 2 does not indicate a difference in the temporal pattern of COVID-19 cases following the first or higher order reintroduction of measures. Case growth first stagnates and rates start to decline in a similar manner across most interventions. Other measures such as cancellation of public events and restrictions on internal movement exhibit a faster downward trend in the number of cases following the third reintroduction compared to the second reintroduction. Only international travel restrictions were associated with a slower decrease in cases after the third compared to the second reintroduction. We note however, that this descriptive analysis does not control for the vaccine rates, which varied in timing and levels across the countries. Results are less pronounced in relation to COVID-related deaths and hospitalisations (Figures A1 and A2), also likely to attributed to the introduction of vaccinations in later periods. [low to medium confidence]
Figure 2. Daily COVID-19 cases around the introduction and re-introduction of different non-pharmaceutical interventions for selected countries.
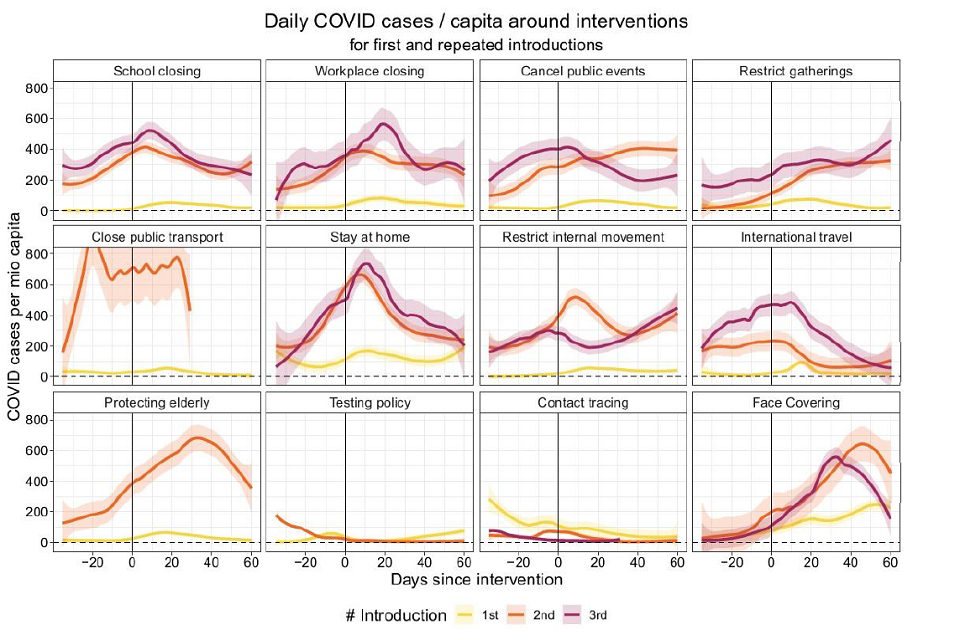
Notes: Figure produced by SPI-B authors, LOESS smoother with 30 distance span. Underreporting likely for first introduction. Included countries (see Appendix).
Recommendations
36. Given a drop in all types of self-reported behavioural interventions, if measures are to be reintroduced, clear rules, communication, clarity of benefits and responsibility of enforcement are required. We reiterate SPI-B advice on the need for people to have ongoing capability, opportunity and motivation to engage in sustained behaviour that are Normal, Easy, Attractive and Routine (NEAR). [footnote 1] [footnote 2] Co-production and extensive stakeholder engagement will be critical to the success of interventions and research and monitoring. [footnote 1] [footnote 3]
37. There is no evidence of the declining effectiveness (defined as rising cases, deaths and hospitalisation) of the repeated reintroduction of most behavioural measures across 30 countries, suggesting that particularly in light of increasing vaccination uptake, measures will remain effective to reintroduce.
III. Contingency Planning: Moving from recommended to mandated behaviour
Legally mandating face coverings in additional settings
Behavioural evidence
38. A large body of evidence demonstrates the effectiveness of face coverings in reducing transmission and to a lesser extent protecting the wearer (see EMG Consensus statement, SAGE 96). [footnote 29] [footnote 30] [high confidence] There is public confusion regarding effectiveness and required settings, and who is responsible for enforcement. [medium to low confidence]
39. Recent research demonstrating the effectiveness of face coverings includes evidence such as a systematic review and meta-analysis of case-control studies which concluded that wearing a face covering reduced the risk of COVID-19 infection, [footnote 31] in addition to both infection and mortality. [footnote 32] Others examined the comparative efficacy of reducing the transmission of aerosols by type of protective covering or shield. [footnote 33] A recent non peer reviewed large RCT in Bangladesh found that the when properly worn, face coverings reduced symptomatic infection by 9.3 per cent. [footnote 34] There is also evidence of the effectiveness of masks in preventing airborne transmission, particularly in relation to coughing and sneezing35 or breathing, speaking and other airborne drivers of transmission. [footnote 36] [high confidence]
40. We lack empirical studies of how the public will respond to reintroductions of mandatory face covering requirements. During the 1918 pandemic reintroduction was met with resistance, although this differed amongst socio-demographic groups. [footnote 37] Compliance was initially high, but after the reintroduction of mask requirements resistance increased, leading to the formation of the Anti-Mask League. [footnote 30]
41. Compliance with face coverings was high at the onset of restrictions in most countries, reaching approximately 80 to 85 per cent for British, [footnote 27] Canadian [footnote 38] and American [footnote 39] adults. Although compliance for mask-wearing fell in the US, in September 2021 a majority reported that there are situations in which face coverings should be mandatory such as airplanes and public transport. [footnote 40] A cross-sectional survey of individuals in five cities without a culture of wearing masks in Australia, the UK and USA (N=2,150, March to July 2020) found that usage decreased by age (for those aged over 50), that risk perception affected usage and that usage did not result in a net-change in other risk-mitigation behaviours.41 Compliance did not wane in the 5 months under observation. [footnote 42] [medium to low confidence]
42. The CoMix survey in the UK for data up to 29 September 2021 found that self-reported facemask wearing reduced to below 70 per cent. The use of face coverings remained high in both Wales and Scotland (more than 85 per cent of participants) where use in particular settings remained mandatory. [footnote 43] We find comparable findings using Facebook data [footnote 22] comparing face covering usage across multiple settings (Figure 3), where we see that wearing a mask has gone down in general, but self-reported face covering wearing remains relatively high on public transit (90 per cent to 69 per cent) and when shopping indoors (92 per cent to 69 per cent). A marked drop over this period has been self-reported wearing a mask at large indoor events (65 per cent to 29 per cent) or indoors at a restaurant (75 per cent to 32 per cent). Self-reported data documented here are in line with other polling such as YouGov [footnote 26] and Ipsos Mori, [footnote 27] suggesting similar reporting trends. Notably, the sharpest drop is in people reporting that they saw others wearing a mask, which went from around 66 per cent in late May to 17 per cent in September 2021. This raises the issue of the validity of relying on self-reporting of behaviour alone, which may solicit socially desirable responses, and flags the need for calibration using multiple data types. [footnote 24] [medium confidence]
43. Face coverings can also mitigate the unequal effects of exposure to COVID-19. A study modelling positive COVID-19 tests (N = 409,009) nested in 72,866 households using the Covid Infection Study found that the level of autonomy in the ability to comply with COVID-19 behavioural measures (such as ability to maintain physical distancing at work, work at home, avoid public transport) had a large and statistically significant effect on positive infections only when people did not wear a face covering or mask. [footnote 21] Those who were unable to maintain physical distance at work, unable to avoid public transport and women from large households were more likely to become infected, suggesting that many individuals unable to follow guidance are at a higher risk of infection. [high confidence]
Figure 3. Percentage of individuals reporting mask wearing across various settings, 01 April to 22 September 2021, United Kingdom.
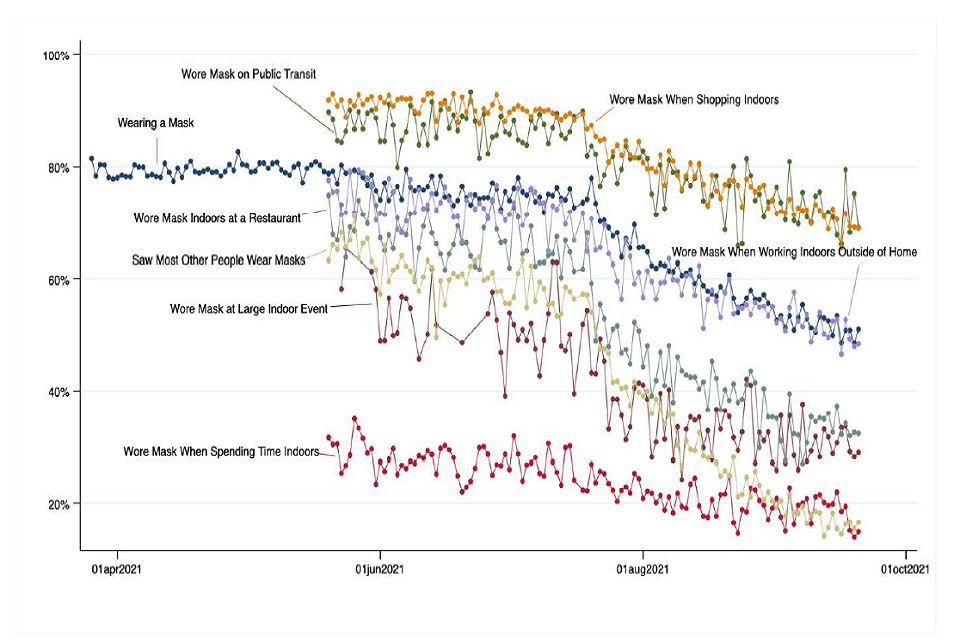
Source: Figure produced by authors from Facebook and University of Maryland data [footnote 22] as of 22 September 2021.
44. A persistent finding is that individuals overestimate certain risks and the extent to which control measures mitigate risk. [footnote 44] There is a minority who actively reject wearing masks and some other safety precautions, often gathering health information from alternative sources. [footnote 45] Government policy to make mask wearing compulsory in additional settings may be seen as illegitimate and resisted by the latter. A core factor driving resistance is an aversion to the feeling of being forced. [footnote 46] [medium confidence]
45. Conversely, making something mandatory also shapes risk perception and gives the public a sign that the policy is more serious, with signalling being a more important driver of behaviour than enforcement. [footnote 47] [medium confidence] A recent cluster randomised trial in Norway in 9 grocery stores found that free distribution of masks increased their usage by 6 percentage points to 91.7 per cent and practically all had both nose and mouth covered. [footnote 48] [medium to high confidence] In most cases, the reintroduction of compulsion would legitimise the requirement of employers and venue owners to require face coverings as a ‘condition of entry’, which in turn will make the wearing of masks normative and hence legitimate. People entering such premises have complied with these requirements historically and there is little reason to assume that would no longer be the case. [footnote 30] Given a background context of increasing pressure on the NHS, the majority are unlikely to engage in widespread resistance, especially if they see face coverings as reducing the risk of more stringent measures being introduced. [footnote 49]
46. Nonetheless, resistance can be expected from those who regard wearing masks as either unnecessary or as a form of social control. CCTV data shows that significant numbers of people are not wearing face coverings on the TfL network in London, for example, even though it is a requirement for them to do so. [footnote 28] There are reports of confrontations between passengers on the TfL network who adhere to the rules and those who do not. Overall, there has been a decline in the use of face coverings on the public transport network in England, broadly coinciding with the move to Step 4 of the Government’s Roadmap, after which they were no longer mandated in national regulations. Some operators continue to require that face coverings are worn on their services in England, via conditions of carriage. (Face coverings remain a legal requirement on public transport in Northern Ireland, Scotland and Wales.) The situation appears to have become more confused because of mixed messaging around the specific conditions where mask wearing is compulsory. (For example, terms like ‘among strangers’ and ‘when crowded’ should be avoided). [footnote 50]
47. More enforcement of existing rules combined with the reintroduction of compulsion in other settings would remove ambiguity and may decrease tension on public transport and similar contexts. Attempts to impose this policy (for example, threatening ejection for not wearing a mask during a football match) could provoke confrontations and disorder. This may be more likely to happen at this point in the pandemic than earlier, because of the difficulties of reintroducing measures after a long period of ‘freedom’ and changing perceptions of risk, raised expectations when restrictions are lifted and as a result of the success of vaccination. The reintroduction of compulsion may empower and legitimise anti-authoritarian narratives. As such, the level of protest against control measures is likely to increase. Enforcement would also entail additional demands on police, although there may be some ambiguity as to who is responsible for enforcement in certain cases. [medium confidence]
Recommendations
48. A large body of evidence demonstrates the effectiveness of face coverings in reducing transmission and, to a lesser extent, protecting the wearer (see EMG Consensus statement, SAGE 96). [high confidence] There is public confusion regarding effectiveness and required settings, and who is responsible for enforcement. If introduced, there are potentially higher demands on police and businesses, which may lead to lack of compliance and confrontations. [medium to low confidence]
49. Clear face covering regulations could focus on: a) settings they are required; b) explicit definition of settings (defining for example, what constitutes a crowded indoor space); c) the settings where face coverings are mandatory or voluntary; d) who will be responsible for enforcing regulations; and, e) implications of lack of adherence (such as health, financial).
50. Communications regarding reintroduction of face coverings would benefit from a focus on a to d above in addition to: a) emphasizing updated scientific evidence on effectiveness, b) clarifying how and why they work; and, c) reiterating correct usage and which face coverings are effective.
51. Some members of the public may resist reintroduction of mandatory face coverings and changing perceptions of risk may empower anti-authoritarian narratives or prompt public protests. Making something mandatory shapes risk perception and would enhance legitimacy for those requiring them as a condition of entry. [medium confidence] It would also create expectations for public figures serving as role models to demonstrate adherence in the required settings.
IV. Mandatory vaccine-only COVID-status certification
Behavioural evidence
52. The Autumn and Winter plan suggests the use of vaccine only certification. [footnote 51] Vaccine-only certification schemes have been launched in Scotland and certain provinces in Canada (Quebec, Manitoba, BC, Ontario) in September and October 2021, which could provide useful comparators. [footnote 52] COVID-19 certification is required in Wales as of 11 October 2021, requiring proof of vaccination or a negative later flow test. [footnote 53]
53. Vaccination passports for infectious diseases already exist in the form of the Yellow Card or International Certificate of Vaccination or Prophylaxis (ICVP). [footnote 5] Vaccine requirements for international travel are known to incentivise vaccination and are relatively uncontroversial. [footnote 54] The paper-based Yellow Card, however, has little protection against forgery, does not incorporate digital technology nor a verifiable link with the holder. [footnote 55] [high confidence]
54. Vaccine Certification has been largely introduced internationally using three options of proof of: double vaccination, negative PCR or lateral flow test or viral antibody serological test, the latter demonstrating natural infection within the last 6 months as a protection against illness. [footnote 5] Negative tests and proof of natural immunity were often introduced when the population did not yet have the opportunity to be fully vaccinated. Certification would need to be resilient against uncertainty around the rate at which immunity to COVID-19 vaccination attenuates, [footnote 4] [footnote 5] and that relationship with onward transmission and hospitalisations, [footnote 56] differences between vaccines and changes in vaccine efficacy against emerging variants. [footnote 4] [high confidence].
55. Inferences about public opinion on certification is in the form of polls, petitions and survey research. According to a YouGov poll in August 2021, around 60 per cent of Britons supported the introduction of vaccine passports, with 30 per cent who ‘strongly’ support them and 32 per cent saying that would be opposed. [footnote 57] Public reaction is reliant on whether certification is perceived as enabling or restricting, with certification controls seen by some as restricting previously entitled rights. Support varies by the setting they would be employed, and is higher for international travel, care homes, hospitals and large events. [footnote 58] Certification is unwelcome if it restricts access to essential goods and services. [medium to high confidence]
56. Drawing from international examples where it has been introduced, enforcement of certification is likely to place heavy burdens on public-facing staff and police and may create dynamics that amplify inequality and social tensions.[footnote 59] When introduced widely in the Netherlands for a second time on 25 September 2021 for hospitality and most events, there was considerable opposition from the hospitality sector who felt it was not their responsibility to carry out the checks. [footnote 60] Dutch media reports after the first week suggest that the majority of businesses and clients complied, with some mixed reports of businesses not checking the app, few fines, many cancellations of bookings (such as for restaurants, parties) and a staff shortage of enforcement officers. [footnote 61] [medium confidence]
57. Public opinions differ by socio-demographic group. Results from a large national UK survey in April (N = 17,611) found that mandatory vaccination passports could reduce vaccine intentions, particularly in socio-economic groups that cluster in large urban areas. [footnote 62] Resistance is unlikely among the vaccinated and may be stronger in lower income communities and among certain ethnic groups in which there is greater vaccine scepticism and lower trust in authorities. [low to medium confidence]
58. For public acceptance, certification needs to be useable on interoperable technologies and ensure equitable access (for example paper for those with no App, international students or visitors, secure for private data with verifiable credentials, portable for use across multiple venues) and meet ethical equity and non-discrimination standards. [footnote 5] [footnote 63] Certification has been shown to present opportunities for fraud, such as when it was introduced the Netherlands in late June 2021 and in spite of a well-designed App, staff at the door did not verify the QR code against personal credentials. [footnote 59] [medium confidence]
59. Introduction could also empower and further legitimise those adhering to anti-authoritarian narratives that have been fuelling demonstrations in urban areas in England throughout the pandemic and some of the attacks on national infrastructure (particularly if digital technology is used). As such, the level of protest against control measures may increase. [footnote 64] If introduced in nightclubs and similar venues, it may result in growing demand for unlicensed musical events (UMEs). These are likely to attract vaccinated young people as well as unvaccinated because of the perceived unfairness of certification and a desire to be with others in their peer group. Recent surveys indicate that fewer young people report that they are more unlikely to be vaccinated if vaccine passports are introduced. [footnote 62] [footnote 65] UMEs place considerable burden on police resources and have in some cases led to violent confrontations. [footnote 66] UMEs taking place in the heart of communities which already feel disadvantaged or discriminated against may be particularly problematic as they have the potential to spark wider disorder.[medium confidence]
Behavioural evidence modelling the link of COVID-status certification with COVID-19 cases and vaccination uptake
60. Several countries have introduced COVID-19 certification, [footnote 5] which allows an analysis of whether the introduction of certification has impacted actual vaccine uptake and infections. There are numerous media and public health accounts linking vaccine certification to increased vaccine uptake, [footnote 67] [footnote 68] yet it has remained anecdotal. A primary analysis used synthetic control modelling to examine the impact of the announcement of COVID-19 certification and its introduction on age-specific vaccine uptake and infections in the 6 countries of Denmark, Israel, Italy, France, Germany and Switzerland during 2021. [footnote 6] This modelling approach is akin to a RCT and allows a counterfactual comparison of the 6 case countries where certification was introduced compared to 20 comparable control countries where it was not introduced, matched by key time-varying characteristics (such as demographics, vaccination and infection levels, stringency other non-pharmaceutical interventions). All 6 countries implemented certificates with restricted access to at least some frequently used public venues such as restaurants, nightclubs or public events, with the details of the data and method, timing and specifications of each certification, plus eligibility of different age groups surrounding that period described in the study. [footnote 6]
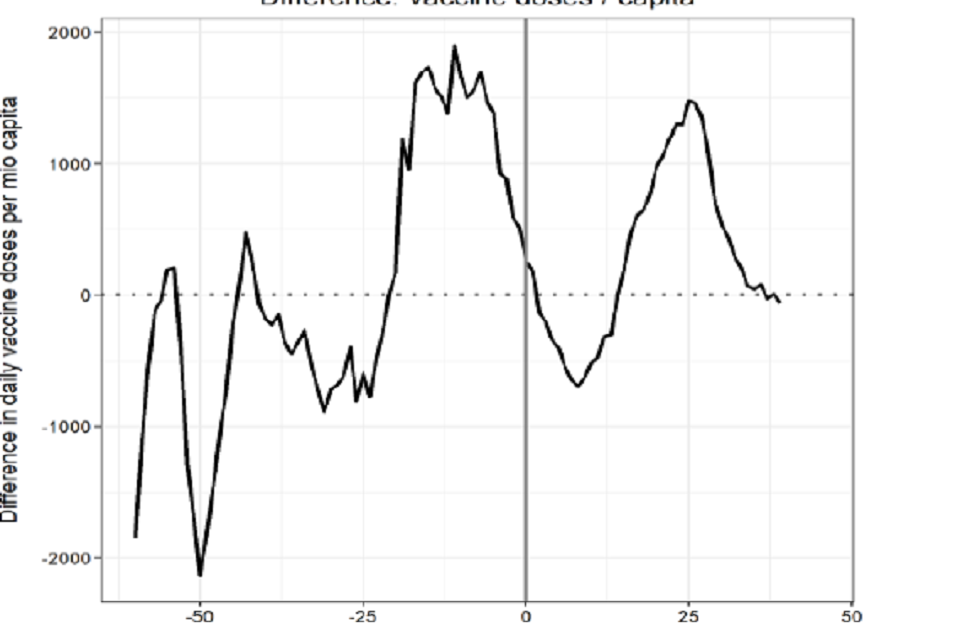
61. Figure 4 shows the results for France and depicts the development over time of new daily vaccinations per million by the treated country (certification) and synthetic control group (countries with no certification) (left panel) and the difference in daily vaccine doses per million around the day of the actual COVID-19 mandatory certificate on 09 August 2021 (pass sanitaire) (right panel). Results show that France had a lower rate of daily vaccinations per capita compared to other similar countries until 3 weeks prior to the intervention and then daily vaccinations started to rise to an above-average level from 21 days before the intervention (an anticipation effect), and a continuation of the positive effect after the intervention.
62. Quantifying this (right panel, Figure 4), the anticipation effect up to 20 days before certification was introduced in France meant that vaccine uptake exceeded the control country by 25,895 vaccines per million capita in total or stated in absolute terms, 1,749,589 doses. Vaccine uptake up to 40 days after certification was introduced exceeded the control country by 11,434 vaccines per million capita in total or 772,563 doses in absolute terms. Thus in total there was an increase of approximately 2.5 million doses or the relative measure of 37,329 per million attributed to this intervention.
Figure 4. Daily new vaccinations in France around the introduction of a mandatory COVID-19 health certificate for several venues as compared to a reweighted Synthetic Control group.
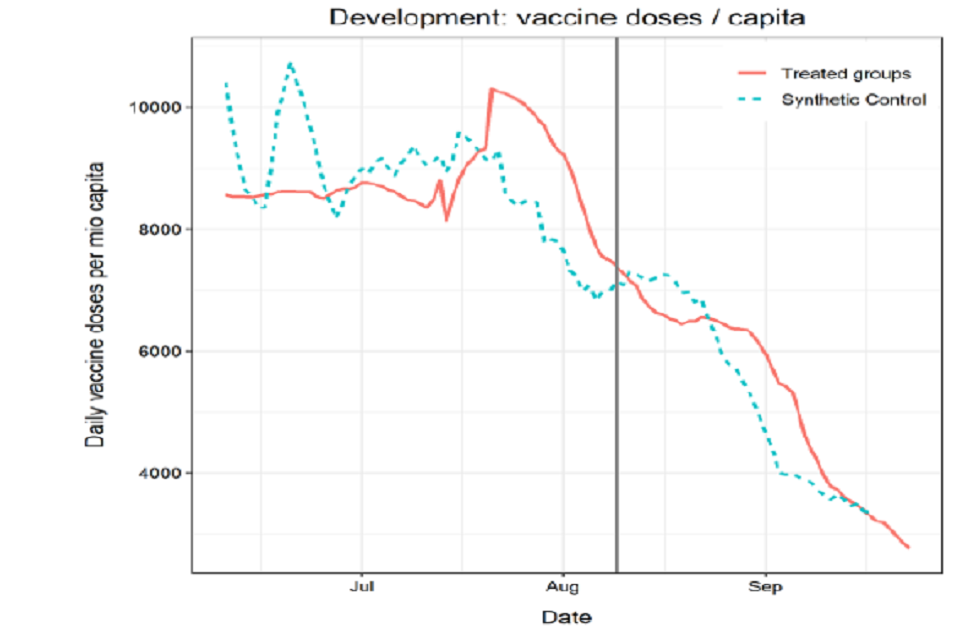
Data sources: Our World in Data (https://github.com/owid/covid-19-data), Oxford COVID-19 Government Response Tracker (https://github.com/OxCGRT/covid-policy-tracker). Control pool: AUT, BEL, CAN, CZE, ESP, FIN, GBR, GRC, HRV, IRL, LTU, LUX, NLD, NOR, POL, PRT, SVK, SVN, SWE, USA.
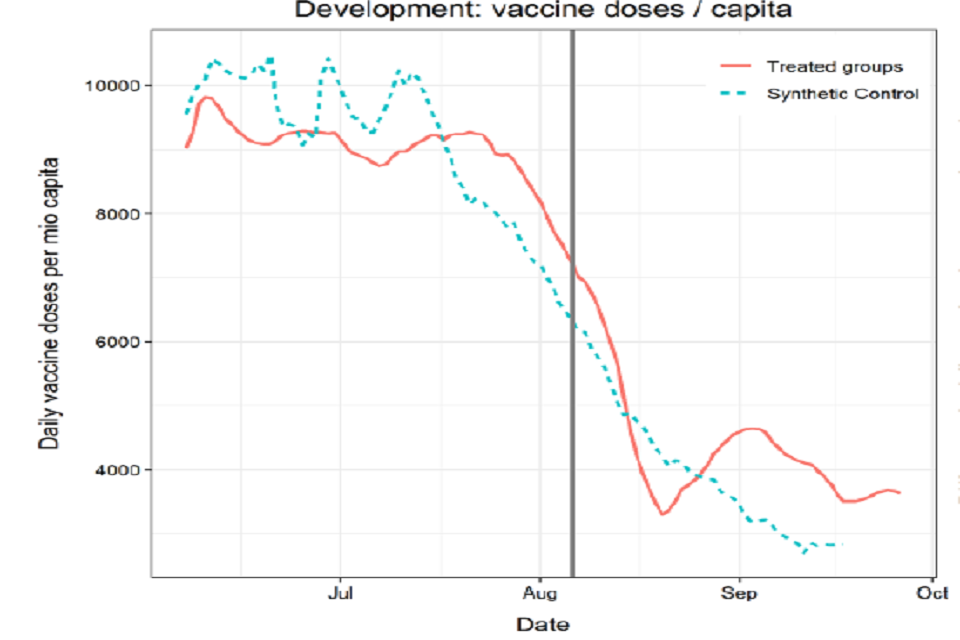
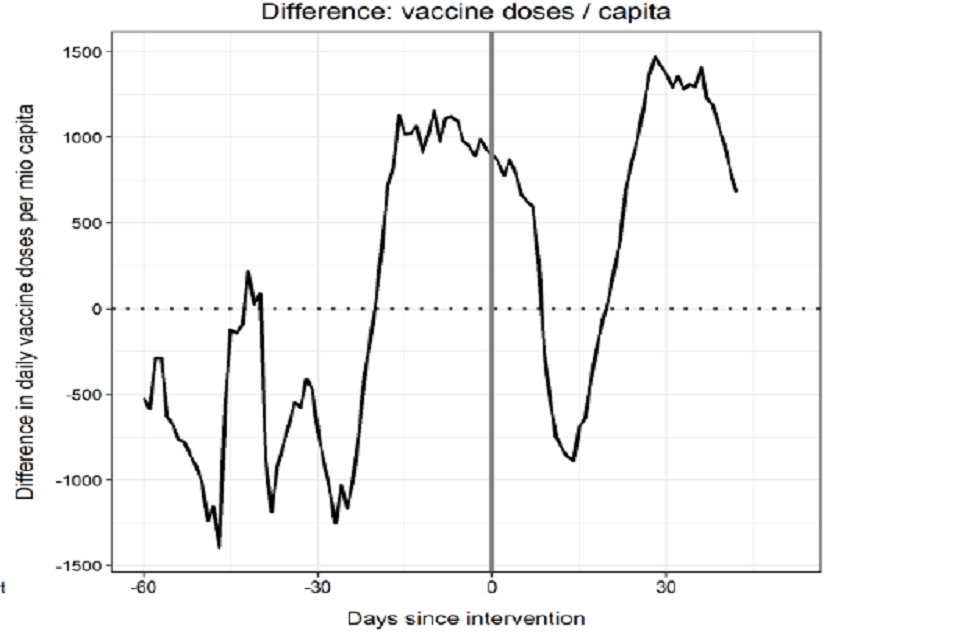
63. For Italy (Figure 5), there is again a shift from a below-average rate of daily vaccinations until the announcement of the Green Pass, showing an anticipation effect and an increase in daily vaccinations directly afterwards at 30 days after implementation. Quantifying this graph, we see a similar surge in Italy, but somewhat higher than France after the intervention (see [footnote 6] for all figures). In Israel, there was a limited anticipation effect, but a surge of 241,286 vaccines per million capita in total up to 40 days after which in absolute terms was 2,120,849 doses. Supplementary results using different estimation methods using all countries confirm this long-lasting upward shift in vaccination rates among countries that implemented COVID-19 certifications.
Figure 5. Daily new vaccinations in Italy around the introduction of a mandatory COVID-19 health certificate for several venues as compared to a reweighted Synthetic Control group.
Data sources: Our World in Data (https://github.com/owid/covid-19-data), Oxford COVID-19 Government Response Tracker (https://github.com/OxCGRT/covid-policy-tracker). Control pool: see previous figure.
64. The results of the analysis from Denmark, Germany and Switzerland and age-specific analyses are shown in the paper. [footnote 6] Youth and certain groups demonstrate higher levels of vaccine complacency due to a lower assessment of the risk of COVID-19, [footnote 69] [footnote 70] suggesting certification could be one mechanism to increase uptake to reach vaccine immunity threshold levels to protect the broader population. Age-specific analyses in France and Italy show a strong effect of both anticipation and uptake afterwards for 25- to 49-year-olds and in Italy for those 18 to 25 years. Although it differs per country, the age effect is related to a combination of the settings of where certificates were introduced that disproportionately impacted youth (nightclubs, large events) and changes in the eligibility criteria to extend vaccinations to younger age groups. [footnote 6] A descriptive fine-grained age-specific analysis in some countries revealed that particularly those below the age of 20 had the highest increased uptake, followed by those 20 to 29 years, holding for both first and second doses. When introduced in particular settings such as in Switzerland (nightclubs, events with more than 1,000 people) higher uptake was found in the younger age groups. When certification was extended to broader settings (events with more than 30 people, entire hospitality sector, leisure activities), the strongest effect on vaccine uptake was on the youngest group, but increased uptake was also observed in older groups. [medium to high confidence]
Recommendations
65. Several criteria are to be considered before introducing COVID-19 certification, including that it: meets benchmarks for immunity; accommodates differences in efficacy between vaccines and emerging variants; has clearly defined uses, is internationally standardised, is based on a platform of interoperable technologies; keeps personal data secure; meets legal and ethical (equity and non-discrimination) standards; is portable and affordable for individuals, businesses and governments; and that conditions of use are understood and accepted by certificate holders. [footnote 4] [footnote 5]
66. If introduced, it would be important to be explicit about the specific settings in which certification will be used and who is exempted. Clarification regarding who will enforce certification is important as it places potential heavy burdens on public-facing staff and police and creates dynamics that amplify social tensions or unlicensed events. Since public opinions of vaccine certification varies by the setting, if it is introduced in domestic settings, it is beneficial to be explicit about which specific setting such as large indoor events, nightclubs, care homes and hospitals and never for essential services and exemptions. Sufficient time for those implementing certification to put these measures in place could ease their introduction.
67. Data from an analysis of the international experience of certification suggests that if vaccine certification was introduced and tied to particular settings, it could increase vaccine uptake in certain groups. However, given already higher levels of uptake in older age groups (in comparison to France, Italy when certificates were introduced), the absolute impact would be smaller, tied more to < 20s. Targeted community-based vaccine interventions are likely to be more effective than certification for some lower socioeconomic and minority ethnic groups. Given that youth and certain groups have higher levels of vaccine complacency due to a lower assessment of the risk of COVID-19, certification could be one mechanism to increase uptake to reach vaccine immunity threshold levels to protect the broader population. Certification is only one measure that is unlikely to be effective for all social groups and is part of a broader ecosystem of interventions to protect public health and increase vaccine uptake. Given that uptake increases directly following the announcement, measures could account for a potential surge of vaccination appointments, and then higher levels for a period after implementation.
V. Advising individuals to work from home (WFH)
Behavioural evidence
68. Working from home (WFH) where possible has been shown as an effective measure to reduce infection risk. [footnote 71] WFH was lifted in England on 19 July 2021 as part of the previous ‘Step 4’ easing of restrictions, a period that coincided with the summer period and school vacations. As illustrated in working from home levels in Figure 1 but also ONS data, around 40 to 50 per cent of employees had occupations and working conditions that allowed them to WFH. [footnote 72] [high confidence]
69. An individual’s ability to work from home is strongly associated with their occupation, socioeconomic status, demographic traits [footnote 73] and due to industry differences across the UK, [footnote 72] as well as region of residence. [footnote 74] The COVID-19 Rapid Survey of Adherence to Interventions conducted in January and February 2021 (N = 1,422) found that non-essential workplace attendance was significantly and independently associated with sociodemographic variables and personal circumstances. [footnote 73] Even if WFH is introduced, a large proportion of employees continue to work in physical settings for essential services. These are often environments where they are in close proximity to other workers, customers or patients, which was also mirrored by higher mortality rates in these occupations in March to December 2020 in the UK [footnote 75] and US. [footnote 76] SPI-B provided previous guidance on managing infection risk in high contact occupations. [footnote 9] [high confidence]
70. Even when advised to work from home, individuals from lower socioeconomic backgrounds are less likely to be able to do so, since barriers exist for the adoption of these behaviours. [footnote 74] In the UK, for instance, groups least likely to be able to self-isolate or work from home tend to be those with the lowest savings. [footnote 74] [high confidence] Public awareness of these inequalities could also be used to challenge the legitimacy of the government’s overall approach to COVID-19 polices which may itself provoke both protest and resistance.
71. Evidence on the broader consequences of home or remote working is linked to mental and physical health, work-life balance, digital and security concerns and productivity. A systematic review of remote working identified stress and fatigue as central issues [footnote 77] with multiple studies finding evidence of ‘technostress’, ‘Zoom fatigue’ [footnote 78] and work overload, invasion of privacy and role ambiguity. [footnote 75] A large study of over 61,000 Microsoft employees in the US during the first 6 months of the pandemic in 2020 found that remote work resulted in more static and siloed work and generated more narrow collaboration networks, making it harder for employees to acquire and share new skills. [footnote 79] Although continued work-from-home and isolation has been associated with psychological outcomes such as depression, anxiety, loneliness, and financial worry, [footnote 77] [footnote 80] there is some evidence that remote working for some demographic groups has been a convenience, particularly with regards to reducing commuting times. [footnote 81] WFH has also been related to reinvigoration of commuter town communities, changes in city centres, real estate and city planning. [footnote 75] [high confidence].
72. Pooling a database of over 150 company practices, [footnote 82] [footnote 83] remote working also raises new policy and legal requirements for employers related to health and safety, insurance, work organisation, data security and ambiguity in claims for the costs of heating, internet and electricity for the employee. [footnote 75] [footnote 82] [footnote 84] Some employers are also concerned about drops in productivity, though some studies suggesting that for particular tasks remote working can result in higher productivity. [footnote 85] Workers may also demand the right to work remotely, which requires employers and regulators to adapt working policies.
73. As summarised elsewhere, [footnote 75] support from businesses for remote working will be required in the form of regulating time pressure, providing clarity on the expectation of working hours, [footnote 86] reducing role conflict and clarifying worker autonomy, [footnote 77] [footnote 87] building teams that interact, [footnote 88] regular face-to-face and hybrid days in the office to maintain networks of support, [footnote 89] many shown to reduce the level of exhaustion in employees. [high confidence]
74. For individuals living in large (6 or more people) or multigenerational households, the advice to WFH may result in a sense of fatalism that it will be difficult to minimise the risk of infection. This is particularly if one member of the household is a key worker and therefore unable to WFH or if someone gets COVID-19, either due to insufficient physical space to self-isolate and or due to care giving roles (towards children and adults) which cannot be fulfilled if self-isolation is required. [footnote 90] In line with previous SPI-B recommendations, specific guidance should be developed on how to reduce transmission in diverse households including large, multigenerational and houses of multiple occupation. [footnote 10] [footnote 91] Information about the importance of ventilation, particularly during winter months when houses will be colder, and financial support to address concerns about increased costs of heating due to ventilation may be necessary for households experiencing financial hardship. This will be particularly important as energy bills are projected to increase in Autumn to Winter 2021. [high confidence]
Recommendations
75. WFH can be an effective measure to reduce infection. Measures and communications could recognise that the ability to WFH exists for around half of the population and varies according to occupation, socioeconomic status, demographic traits and regional variations in industry. Employers would benefit from developing guidelines to ensure worker safety for employees that remain in close proximity to other workers, customers or patients (such as ventilation, distancing, face coverings). Communication and measures to reintroduce WFH could benefit from engagement with businesses and acknowledge these differences and inequalities to avoid the policy provoking protest and resistance.
76. Employers could benefit from developing measures to cope with the potential WFH implications of mental and physical health, work-life balance, security and productivity concerns. Working from home raises new policy and legal questions for employers related to health and safety, insurance, work organisation, data security and ambiguity in claims for the costs for the employee (such as heating, internet). Coordination and support for business such as guidelines, fiscal support, inspections or enforcement could make them more likely to support and promote the introduction of restrictions for their employees.
77. Specific guidance on how to reduce transmission in diverse household structures including large or multigenerational households remains important to communicate.
VI. Communicating risks to the public
Behavioural evidence
78. When communicating risks to the public, trust is important as it can increase or decrease willingness to engage with the measures outlined in the Autumn and Winter plan. Trust in public health messages is linked to how credible and legitimate the communicator and source of information is. Healthcare professionals are one of the most trusted sources but when affiliated with central government, this trust decreases. [footnote 92] The relationship of trust in central government messaging has declined over the course of the pandemic. A DHSC survey asked participants whether ‘Information from the Government about coronavirus can be trusted’. Responses have varied, being highest in late March to early April 2020, just after the first lockdown had started, but lowest in October 2020 when the second wave started and almost as low again in late July 2021. A nationally representative survey (N = 1,476) of adults in the UK in December 2020, combined with 5 focus groups found that trust in health institutions and experts were core predictors of vaccine intentions. [footnote 45] Those who were the most vaccine hesitant had a general mistrust in government and more often obtained information from unregulated social media sources. [footnote 45] This decline in trust can be attributed to several factors including unclear and inconsistent messaging in the earlier stages of the pandemic, [footnote 93] government officials and role models not modelling behaviour in line with guidance, [footnote 92] [footnote 93] central government interventions unintentionally increasing stigma due to prolonged periods of lockdown in specific areas and disproportionate press and political coverage on specific communities, [footnote 92] [footnote 94] [footnote 95] and the recent publication of a government report which does not acknowledge the experiences of trauma and exclusion experienced by minority ethnic groups. [footnote 95] Localised messages, shared by trusted communicators that are embedded within a wider provision of support, is more acceptable and accessible to some groups. [footnote 8] [high to medium confidence]
79. In the earlier stages of the pandemic, many voluntary and mutual aid groups mobilized to support communities by providing practical, social and emotional support. [footnote 96] However, many of these groups could not be sustained over the longer period particularly when the furlough scheme ended as there was less available time and resources to provide on-going support. The closure of community spaces and periods of isolation during lockdown have resulted in weakening of social ties and support networks in some areas. Building social infrastructures with resources and support is likely to increase the reach of key messages of about reintroducing restrictions. [medium confidence]
80. There are increased opportunities to develop local and rapid response initiatives to support reintroduction of restrictions. National level funding for Community Champions programmes has produced greater coordination between local authorities, the third sector and community organisations. The programme has facilitated the coordination of activities such as setting up vaccination hubs, circulation of translated materials in multiple languages online and face-to-face, as well as facilitating a two-way dialogues addressing concerns within specific neighbourhoods. Increased connectivity between local authorities and community organisations has resulted in increased trust and cohesion between local authorities and community organisations, better understanding of communities, and provision of support that is aligned with the needs of the community. The decentralised structure of the Community Champions programme enables schemes to be responsive to new challenges and re-divert resources and funding allocation as required. [footnote 8] [footnote 97] [high confidence] This new infrastructure of Community Champions is well positioned to respond to new and unanticipated challenges. This includes sharing communications about reintroducing restrictions and engaging in two-way dialogue to address concerns which, if left unresolved, is linked to mistrust and possibly less engagement with the behaviours outlined in the plan.
81. Experiences of earlier stages of the pandemic highlight the importance of reintroducing restrictions within a collective identity framework with communications about shared goals and shared identity [footnote 98] to minimise the impact of stigma which can arise from targeting specific communities. Targeted messaging can have the opposite intended effect as groups may feel singled out and highlighted as ‘problematic groups’ creating a sense of blame for higher infection rates. Trusted communicators include local credible sources such as religious and community leaders, [footnote 99] and healthcare professionals who are viewed as having more authority to share messages about vaccines compared with individuals that do not have a scientific background. [footnote 100] Tailored communication is essential for making messages accessible to diverse, local communities but this should be aligned with the same message that all communities receive. Namely mode of delivery and content structure may vary, but the core message is the same. [high to medium confidence]
Recommendations
82. Messaging needs to be clear and agile to address the complex and changing situation, have a clear rationale, be tailored to address the informational needs of different groups and be consistent with role modelling by public figures on the behaviours being advocated. Specific guidance should be developed on how to reduce transmission in diverse household structures including large or multigenerational households.
83. Funding to support local communication campaigns that are aligned with national guidelines will be required, such as Community Champions programmes, which are well positioned to share messages about reintroducing restrictions and are responsive to new and unanticipated challenges. This includes sharing information via trusted sources and engaging in two-way dialogue to address specific concerns that relate to the behaviours included in the Autumn and Winter Plan. Trusted communicators include local credible sources such as healthcare professionals, community leaders, and individuals that are embedded in wider support networks such as schools, support groups and youth clubs.
84. Communication should include a clear rationale for guidance to avoid confusion. Wearing face coverings is the most visible behaviour in the Autumn and Winter plan and should be modelled by government advisors to reinforce the importance of this, and all measures included in the plan. Trust in messages is likely to increase when the general public feel that they are trusted to follow the guidance and do not feel that they are being targeted or blamed. Positive media and political coverage will facilitate this process of increasing trust.
VII. Test and Trace, adherence to self-isolation and staying at home when sick
Behavioural evidence
85. The NHS COVID-19 app successfully averted a large number of COVID-19 cases, with predictions ranging from 100,000 to 900,000 cases. [footnote 101] Over the same period, total cases numbered 1.9 million. [footnote 101] High uptake is recognised as the key to the effectiveness of digital contract tracing. Usage has declined over time. [footnote 12] [medium to high confidence]
86. Twice weekly lateral flow tests are currently recommended by the UK Government. Asymptomatic testing is credited with detecting around a quarter of all cases reported each day. [footnote 51] Current uptake of asymptomatic testing is low, with 25 per cent of asymptomatic survey respondents reporting having taken one or more tests for coronavirus in the past week. [footnote 102]
87. Current policy requires people to take a PCR test when they experience one of the 3 main symptoms of COVID-19. Survey data suggest that, of those who take a test, around 45 per cent self-report that they used a lateral flow test alone, rather than a PCR. [footnote 107] Whether an increase in testing triggered by the ready availability of lateral flow tests offsets the decrease in sensitivity that lateral flow tests have is unclear.
88. Adherence to self-isolation among people who receive a positive PCR test result and who are in contact with NHS Test and Trace are good. [footnote 103] However, most people who have one of the 3 “main symptoms” of COVID-19 do not take a test. [footnote 102] Increasing the number of people who take a test when symptomatic has been a persistent challenge throughout the pandemic. [footnote 104] One of the key barriers to taking a test is that some symptom experiences do not fit with people’s expectations of what COVID-19 is like, or with the broader and less severe profile of COVID-19 symptoms that may be becoming more prevalent at this stage of the pandemic and with high rates of vaccination. [footnote 105] [footnote 106] In particular, mild symptoms, individual symptoms, symptoms that are more non-specific (and in particular cough), symptoms with a short duration and symptoms that occur in the absence of an obvious potential transmission event are less likely to lead someone to take a test. [footnote 102] [medium confidence] A resurgence of seasonal respiratory viruses is likely to increase the absolute number of tests that are requested [high confidence]. However, because it also provides people with a ready non-COVID-19 related explanation for their symptoms, it may also decrease the proportion of people with mild COVID-19 who request a test. [medium to high confidence]
89. The Autumn and Winter Plan calls for people to stay at home when they have an influenza-like illness. Multiple factors affect whether someone attends work, university or school when suffering from a seasonal respiratory virus. [footnote 108] These include the provision of sick leave, organisational culture, fear of disciplinary action, lack of cover for work, a sense of professional obligation, fear of work building up, concern about burdening co-workers, concern about being seen as weak, not feeling you are sufficiently ill to warrant time off, and financial worries [medium confidence] Many of these factors have been exacerbated by the pandemic. At the same time, ability to WFH and motivation to protect others from respiratory illness have become more common. [medium confidence]
90. Financial barriers may be incurred as a result of engaging with Test and Trace and self-isolation for lower income communities and people working in precarious employment. A proportionate response where more financial and practical support is available in areas that will be most impacted by the reintroduction of measures will be required to overcome barriers to testing and self-isolation. [footnote 97] Financial barriers to testing have been overcome in some lower income areas when additional local authority payments were available for self-isolation resulting in increased engagement with NHS Test and Trace. [footnote 8] Additional financial support may also address beliefs that engaging with testing invites a self-inflicted punitive and restrictive regime which contributes to reluctance to engage with Test and Trace. [footnote 109] [medium confidence]
Recommendations
91. Digital contact tracing and the NHS COVID-19 app should be understood as comprising part of an ecosystem of interventions, such as physical distancing and face coverings. Digital contact tracing should be considered as a counterpart to manual tracing, since the 2 approaches do not entirely overlap with respect to the individuals traced. [footnote 101] Usage has declined but high uptake is instrumental to the success of the app. [footnote 12] To increase the uptake of the app, recent studies indicate that even minimal monetary incentives can be effective, and some messaging (such as video) has a limited effect. [footnote 12]
92. Given that asymptomatic testing is low, improving the rate of asymptomatic testing would require a concerted effort from Government and employers. While lateral flow tests remain free for the public for the time being, from 4 October 2021, a “collect code” is required in order to receive packs from the pharmacy. [footnote 13] The introduction of any barrier to distribution seems likely to reduce the number of people who access testing.
93. Given an increase the likely increase in cold and flu symptoms in autumn and winter, maintaining or improving the proportion of people with COVID-19 who request a test will require clear communications. Communications should focus on what specific symptoms necessitate testing, and also encourage people to take an early test even for mild, individual symptoms regardless of whether an obvious transmission event has occurred.
94. Given that many individuals report using a lateral test alone, clarifying the benefits of PCRs for symptomatic testing, and the limitations of using a lateral flow test in this situation (since multiple tests are more likely to pick up infection), [footnote 110] may help to improve PCR uptake and detection of influenza.
95. Clear communication of why it is important to stay at home when ill, even if a negative COVID-19 test result is obtained, may encourage and enable more people to take time off, reducing transmission. This is particularly likely to be effective if communication comes from multiple routes (including Government and employers) and if conducted as part of a series of strategies intended to support people to take time off when ill.
96. Ensuring people are aware they can access support and providing enhanced payments and practical support for people in lower income communities and precarious employment is likely to increase engagement with Test and Trace.
Appendix 1. Reintroduction of measures
Data. Information on COVID-19 related health indicators is taken from Our World in Data. [footnote 111] [footnote 112] The database collects and harmonises information on COVID-19 indicators cases, deaths, vaccinations on a daily basis. We then linked these indicators to data from the Oxford COVID-19 Government Response Tracker (OxCGRT), [footnote 25] which provides information on the implementation and stringency of non-pharmaceutical interventions on a daily basis across countries.
Measures. The health-related outcomes were all adjusted by population (per million) and are: a) daily confirmed cases of COVID-19, b) daily confirmed deaths attributed to COVID-19, c) the number of COVID-19 patients in hospital on a given day, and, also d) daily new COVID-19 vaccination doses administered. In all cases, we relied on the 7-day smoothed rolling average.
Analytical methods and approach. To descriptively compare the effectiveness of repeated interventions, we overlay the COVID-19 related cases, deaths and hospitalised patients before and after the implementation of several measures. Since once question was to provide evidence related to reintroduction of interventions, we differentiated between the first, second and third implementation. We note that some measures have not been repeatedly implemented, such as for instance the closure of public transport or stricter testing policies. Whilst the first (closure public transport) was only introduced sparsely, the latter (stricter testing policies) remained in place over the entire period.
The descriptive graphs show the development around the introduction of policy intervention by fitting a trend line based on smoothed conditions means. For this purpose, we used a LOESS smoother with 30 per cent distance span and 95 per cent confidence intervals. We included all countries providing data on hospital patients (though not all countries contribute to each graph): AUT, BEL, BGR, CAN, CHE, CYP, CZE, DNK, ESP, EST, FIN, FRA, GBR, HRV, HUN, IRL, ISL, ISR, ITA, LTU, LUX, LVA, NLD, NOR, POL, PRT, SVK, SVN, SWE, USA.
Figure A1. Daily COVID-19 related deaths around the introduction and re-introduction of different non-pharmaceutical interventions for selected countries.
Notes: Figure produced by SPI-B authors, LOESS smoother with 30 distance span. Underreporting likely for first introduction. Included countries: Austria, Belgium, Bulgaria, Canada, Switzerland, Cyprus, Czech Republic, Denmark, Spain, Estonia, Finland, France, Great Britain, Croatia, Hungary, Ireland, Iceland, Israel, Italy, Lithuania, Luxembourg, Latvia, Netherlands, Norway, Poland, Portugal, Slovakia, Slovenia, Sweden, USA.
Figure A2. Current total COVID-19 related hospital patients around the introduction and re-introduction of different non-pharmaceutical interventions for selected countries.
Notes: Figure produced by SPI-B authors, LOESS smoother with 30 distance span. Underreporting likely for first introduction. Included countries: see Figure A1.