Article Text

Abstract
Donovanosis, a chronic cause of genital ulceration, has recently been the subject of renewed interest after a long period of relative obscurity. The causative organism, Calymmatobacterium granulomatis, has been cultured for the first time in many years and a polymerase chain reaction diagnostic using a colorimetric detection system has been developed. Phylogenetic analysis confirms close similarities with the genus Klebsiella and a proposal made that C granulomatis be reclassified as Klebsiella granulomatis comb nov. Azithromycin has emerged as the drug of choice and should be used if the diagnosis is confirmed or suspected. In donovanosis endemic areas, syndromic management protocols for genital ulceration may need to be adapted locally. A significant donovanosis epidemic was reported in Durban from 1988–97 but the current status of this epidemic is unclear. The donovanosis elimination programme among Aboriginals in Australia appears successful and is a model that could be adopted in other donovanosis endemic areas. Overall, the incidence of donovanosis seems to be decreasing. Increased attention would undoubtedly be paid to donovanosis if policy makers recognised more readily the importance of genital ulcers in fuelling the HIV epidemic.
- donovanosis
- granuloma inguinale
- genital ulcer disease, sexually transmitted infections
- Africa
Statistics from Altmetric.com
Donovanosis (granuloma inguinale) usually causes genital ulceration that bleeds readily to the touch. The condition is often described in the medical literature as forgotten or overlooked. Following the discovery and introduction of antibiotics there was an immediate upsurge in interest that quickly waned and the disease attracted little attention until the late 1980s when genital ulcers were identified as a significant co-factor in facilitating HIV transmission.
The causative organism is generally recognised as Calymmatobacterium granulomatis, a Gram negative pleomorphic bacterium. A proposal that the organism be reclassified as Klebsiella granulomatis comb nov, based on a phylogenetic similarity of 99% with K pneumoniae and K rhinoscleromatis has been put forward.1 However, another study found lesser phylogenetic similarities of 95% and 94% respectively with the genera Klebsiella and Enterobacter and concluded C granulomatis was a unique species.2
Donovanosis is found in diverse areas of the world, most of which have limited medical research capabilities. Recent scientific work on the infection has come mainly from South Africa, Australia, and India. The condition tends to be found in populations that are marginalised, impoverished, and with limited powers of advocacy. Considerable uncertainty still surrounds many aspects of donovanosis including the natural history, disease classification, treatment, and even the most suitable name for the condition.
A review of the history of donovanosis demonstrates marked interest by a small number of motivated physicians and scientists. This situation still exists today and probably reflects the fact that tropical causes of genital ulcer disease (GUD) have been, and continue to be, largely ignored by both most healthcare professionals and policy makers alike.3 This review article focuses on recent developments in donovanosis including epidemiological trends, clinical appearances, diagnostic tests in different settings, treatment, and disease control and prevention.
EPIDEMIOLOGY
Donovanosis has a curious geographical distribution with “hotspots” in Papua New Guinea, KwaZulu-Natal, and eastern Transvaal in South Africa, parts of India and Brazil, and among the Aboriginal community in Australia. Sporadic cases are reported elsewhere in southern Africa, the West Indies, and South America. The largest epidemic was reported among the Marind-anim people in Papua New Guinea where, between 1922–52, 10 000 cases were identified from a population of 15 000.4
Recent accurate data for most endemic areas are limited. In Papua New Guinea donovanosis is still prevalent and was the second most common cause of GUD after genital herpes in a study at five health centres in 1989–90.5 However, a more recent World Health Organization (WHO) consensus report states that donovanosis has apparently become very rare in Papua New Guinea.6 In Pondicherry, south India, donovanosis accounted for 14% of genital ulcer cases referred to an STI clinic, 15% of whom were HIV positive between 1993–7,7 but in north India the incidence decreased significantly in the 1990s.8 In Jamaica, the prevalence of donovanosis diagnosed on clinical grounds in STI clinic patients was 4.1% in 1982–3 and 2.3% in 1990–1.9 In Brazil, donovanosis accounted for 0.3% of just over half a million STI cases reported between 1987–96.10
In Durban during the late 1980s and 1990s a significant epidemic of donovanosis emerged—3153 cases were reported from the main STI clinic in 1997.11,12 Also in Durban, among men and women with genital ulcers, Donovan bodies were identified in 11% and 16% respectively.13,14 After 1997 STIs in Durban were classified syndromically under the overall heading of genital ulcers without mention of likely specific aetiologies, resulting in the loss of important donovanosis surveillance information. A more recent genital ulcer aetiology survey in men in Durban diagnosed donovanosis in only 4%.15 However, it is unknown whether tissue smears for Donovan bodies were prepared from the first swab taken from ulcers with clinical signs of donovanosis, an important factor in increasing the yield of positive results.16 In addition to the peak in Durban in 1997, a further peak was noted in 1969–74.11 Overall, the pattern of reported cases of donovanosis in South Africa has been variable. Before the 1980s Freinkel suggested that there were only a few cases in the country and that the disease had all but disappeared.17 A more likely scenario is that the condition attracted little interest and went unrecognised or was misdiagnosed as lymphogranuloma inguinale or lymphogranuloma venereum (LGV).18
The relative paucity of interest in donovanosis by public health authorities in most endemic countries is in marked contrast with the situation in Australia where a proactive approach was launched in the mid-1990s with the aim of eliminating the condition from the country.19,20 The programme was started in northern Australia supported by a dedicated donovanosis project coordinator. This innovation has been successful with surveillance data showing that the incidence decreased from 117 in 1994 to 12 in 2000 although a slight increase was reported in 2001.21 The project has four designated officers who coordinate clinical protocols, perform health promotion, validate epidemiological data, ensure laboratory quality control, and assist in the follow up of hard to reach cases (Frank Bowden, personal communication, January 2002).
Although donovanosis is generally regarded as an STI mainly affecting the genital area, the possibility remains that lesions are not always sexually transmitted but occur through faecal contamination and autoinoculation.22 Carter has reviewed the literature and made the observation that in publications making direct statements about the mode of transmission of donovanosis, 72% of authors before 1947 stated that donovanosis was not sexually transmitted compared with 8% after 1947.23 Arguments cited in support of an STI origin are:
History of sexual exposure in most patients before the appearance of lesions
Increased incidence in age groups with highest sexual activity
Lesions on the cervix only
Anal lesions found in homosexual men practising receptive anal intercourse
Genital infection usual
Concurrent STIs
Outbreaks linked to a specific sex worker.
Factors against an STI origin are:
Occurrence in young children and sexually inactive adults
Relatively rare in sex workers
Rare in sexual partners of index cases
Unusual sites of primary non-genital lesions
No well defined incubation period.
The latter contention is supported by both the low co-infection rates in sexual partners of index cases in Papua New Guinea and the United States24,25 but contradicted by both a history in index cases of sexual contact with specific female sex workers26,27 and the higher prevalence in sexual partners in India where 26 (52%) partners of 50/165 index cases, were co-infected with donovanosis.28 Cases in children are often attributed to sitting on the laps of infected adults rather than sexual abuse.29 Transmission may occur during vaginal delivery and careful cleansing of neonates born to infected mothers is recommended.30
CLINICAL APPEARANCES
The incubation period is uncertain. Estimates range between 1–360 days,31 3–40 days,32 14–28 days,33 and 17 days.34 This wide range is probably multifactorial and may reflect either late presentation and denial or non-sexual transmission. The finding that experimental lesions were induced in humans 50 days after inoculation is a more realistic assessment.35
Infection usually starts as a firm papule or subcutaneous nodule that ulcerates. Classically there are four types of donovanosis: (1) ulcerogranulomatous—the commonest type, beefy red, non-tender ulcers that bleed readily to the touch and may become quite extensive if left untreated (fig 1); (2) hypertrophic or verrucous ulcer—growth usually with an irregular edge, sometimes completely dry (fig 2); (3) necrotic—foul smelling deep ulcer causing tissue destruction; (4) dry, sclerotic, or cicatricial lesion with fibrous and scar tissue.

Typical beefy red donovanosis penile ulcer.

Hypertrophic donovanosis ulcer with a regular margin.
The genital region is affected in 90% of cases and the inguinal area in 10%. The anatomical areas affected most frequently are, in men, the coronal sulcus, subpreputial region, and anus and in women, the labia minora, fourchette, and occasionally the cervix and upper genital tract. Ulcers are more common in uncircumcised men with poor standards of genital hygiene. Extragenital lesions account for 6% of cases and are the subject of ever increasing numbers of case reports. Sites of infection include lip, gums, cheek, palate, pharynx, neck, nose, larynx, and chest.33,36 Rarely, disseminated donovanosis with spread to bone and liver may occur and is usually associated with pregnancy and cervical infection.
Differential diagnosis
In areas where donovanosis is prevalent, physicians with good clinical skills should be able to make the diagnosis with a reasonable degree of accuracy.37 However, ulcers may sometimes be difficult to differentiate from primary syphilitic chancres, condylomata lata of secondary syphilis, chancroid, and large HIV associated herpes ulcers. Amoebiasis and carcinoma of the penis should be considered if lesions are destructive or necrotic. Donovanosis associated pseudoelephantiasis may mimic LGV. Donovanosis is often long standing and the possibility of dual infection with one or other of the classic causes of GUD should always be considered. Cervical donovanosis may mimic both carcinoma and tuberculosis of the cervix. Extragenital lesions may present atypically often leading to protracted delay in the diagnosis.
DIAGNOSTIC TESTS IN DIFFERENT SETTINGS
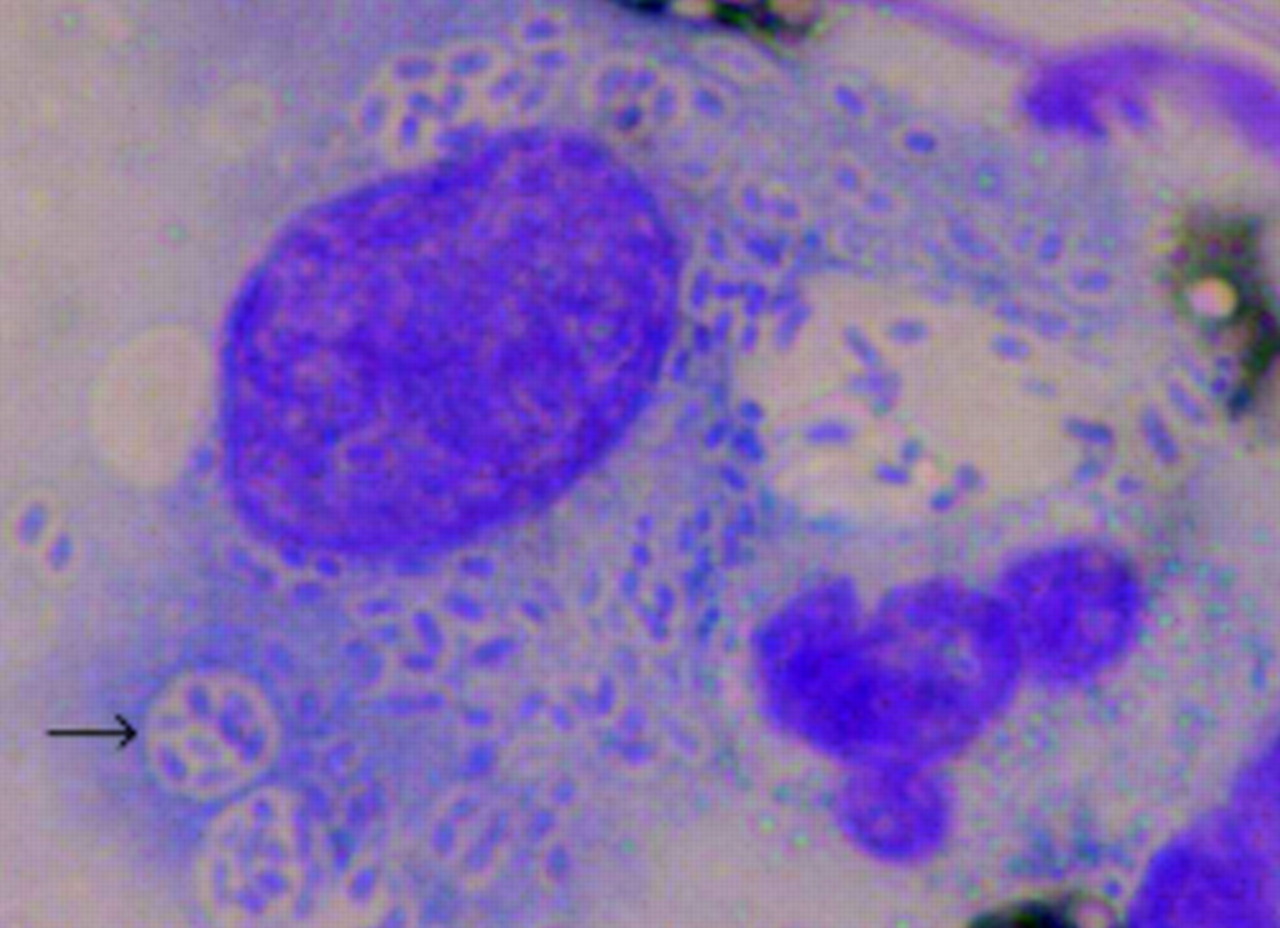
If possible the diagnosis of donovanosis should be confirmed before antibiotics are given. Confirmation is by the identification of typical intracellular Donovan bodies within large mononuclear cells either in smears obtained directly from tissue or biopsy samples (figs 3 and 4). These characteristic cells are 25–90 μm in diameter while the Donovan bodies are 0.5–0.7 by 1–1.5 μm and may or may not be capsulated.33
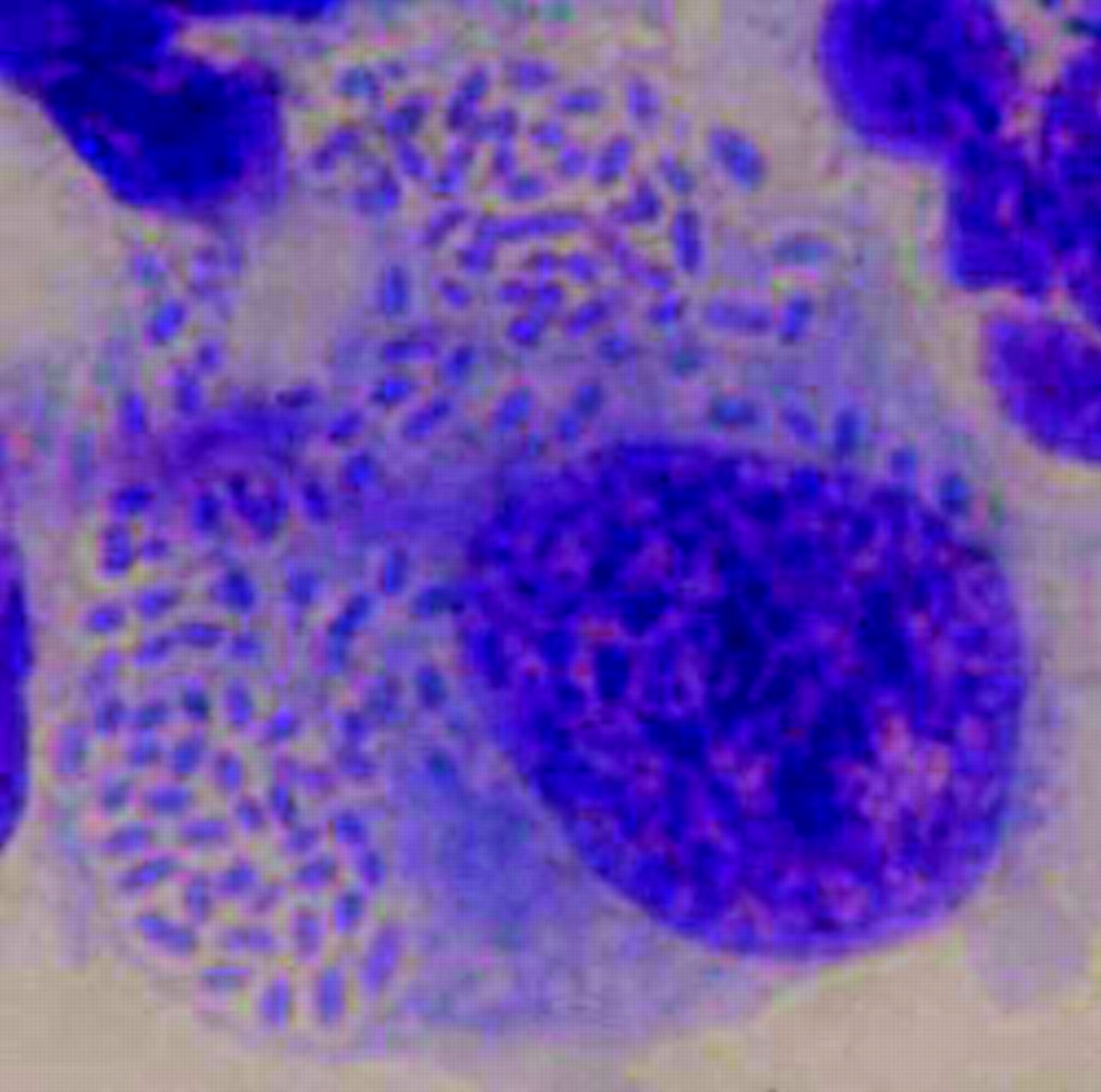
Tissue smear stained by rapid Giemsa (RapiDiff) technique showing numerous Donovan bodies in a monocyte.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tissue smear stained by rapid Giemsa (RapiDiff) technique showing numerous Donovan bodies in monocytes including some in intracytoplasmic cysts (arrow).
Donovanosis may be diagnosed in a variety of developing world settings. The following are examples of possible scenarios and recommended diagnostic tests.
Busy STI clinic with microscope and facilities for staining smears; patients may not return
Tissue smears can be undertaken in patients quickly and accurately. The key to maximising the sensitivity of this technique lies in the preparation of the slide. Many donovanosis ulcers have superadded infection and/or debris that should be removed by rolling a cotton tipped swab across the lesion gently to minimise bleeding. Next, the site of the lesion should be stabilised so that sufficient pressure can be applied to the ulcer while taking the smear. This is particularly important in men in whom lesions are found mainly on the penis. Examiners should wear gloves on both hands and stabilise the penis with one hand while using the other to roll a cotton tipped swab firmly across the surface of the ulcer without causing bleeding if possible. This swab is then rolled, equally as firmly, across a slide on a flat surface so that the material from the ulcer is spread evenly. The slide is then air dried and stained by a rapid Giemsa method using eosin and thiazine solutions.38 This whole process should not take longer than a few minutes. Rapid staining with pinacyanole is also effective.39 Cleaning ulcers with sterile saline is usually not necessary and may actually limit the amount of material collected on the swab from the surface of the ulcer.
If multiple swabs are taken from ulcers to detect other pathogens, it is important that, if donovanosis is considered likely, the smear for Donovan bodies is taken first so that adequate material can be obtained from the surface of the ulcer. Clearly, most ulcers will be dry after a few swabs have been taken and it will then be difficult to demonstrate Donovan bodies in superficial tissue smears however likely the diagnosis on clinical grounds.
Well staffed STI clinic; patient likely to return next day
Specimens from sites just below the surface of the ulcer are more likely to yield positive results than those from superficial tissue. Pieces of tissue obtained by using a forceps and scalpel from the advancing surface of the ulcer can be crushed between two slides taking care not to cause drying of the specimen by prolonged spreading.40 Staining is by a slow overnight Giemsa method or Leishman’s or Wright’s stain. Alternatively, the clean undersurface of the tissue can be smeared along a glass slide.41 Proper cleansing of the lesion will increase the sensitivity of these techniques and is recommended. If time allows, biopsy, fixing in formaldehyde, embedding in paraffin and slow, overnight, Giemsa should provide optimal results.42
Lesions biopsied and patients return for results
Patients in this group are often seen in antenatal or gynaecological clinics. Biopsies can be done under local anaesthetic and examined by histology. The best stains to use are either Giemsa or silver rather than haematoxylin and eosin. Histological changes of donovanosis usually show epithelial proliferation and a heavy inflammatory infiltrate of plasma cells, neutrophils, and few lymphocytes. Biopsy is usually required to confirm the diagnosis for the necrotic and sclerotic variants and sometimes for hypertrophic lesions.
Culture
Following a report describing the culture of C granulomatis from faeces in 1962,22 and a subsequent gap of 35 years, multiplication of C granulomatis in a monocyte co-culture system was achieved in Durban43 while in Darwin the organism was grown using a modified chlamydia culture.44 Transmission electron microscopy can be used to compare the ultrastructural features of C granulomatis from different specimens.45
Polymerase chain reaction
Although polymerase chain reaction (PCR) techniques have been reported from two centres, the process is still really only available as a research tool and requires further evaluation.2,46 Initially, Bastian et al achieved amplification of Klebsiella-like sequences using primers targeting the PhoE gene.46 A diagnostic PCR was developed using the observation that two unique base changes in the phoE gene eliminate HaeIII restriction sites enabling clear differentiation from closely related species of Klebsiella.47 This method has been refined further into a colorimetric PCR test that could be used by diagnostic laboratories.48
Serology
An indirect immunofluorescent technique was developed using thin sections of donovanosis lesions as a source of antigen with good results for established lesions but with a low sensitivity for early infection.49 While the test might be useful in population studies in endemic areas it is not accurate enough at the individual level to be acceptable for confirmatory diagnosis.
Other
Donovan bodies have been identified from Papanicolaou smears used in routine cervical cytology screening.50 Additional methods used in the past that have only limited relevance now include antigen detection, complement fixation, and skin tests.
Missing the diagnosis
The diagnosis of donovanosis, particularly when associated with extragenital lesions, is often missed in non-endemic areas because it is not suspected.51 In areas where the condition is well known and described, a high index of clinical suspicion should be maintained for unusual manifestations of genital ulcers and other skin lesions appearing in extragenital sites.
It is interesting to speculate about other areas where donovanosis might be prevalent and not recognised. For example, a study in Swaziland, an area bordering on a donovanosis endemic zone in eastern Transvaal,52 described a number of large ulcers diagnosed by chlamydia antibody testing as LGV, a condition classically associated with small ulcers, while only one case of donovanosis was identified.53
MANAGEMENT
The optimal way to manage a possible case of donovanosis is to establish the diagnosis as soon as possible so that definitive first line treatment and specific health education can be given. This may not always be possible, in which case standard syndromic management for genital ulcers will ensure treatment at the time of presentation. However, evaluation of syndromic management protocols for GUD in donovanosis endemic areas has yet to be undertaken. In the absence of a confirmed diagnosis, antibiotics recommended for most GUD syndromic management protocols to cover syphilis and chancroid may or may not work for donovanosis. Treatment for chancroid may be inadequate for donovanosis in both dose and duration and the limitations of syndromic protocols must be recognised. Furthermore, education and counselling are probably more important for donovanosis than chancroid, a condition in which single dose treatment may be effective and lesions are of shorter duration. In settings without adequate laboratory back up and where donovanosis is prevalent, it is advisable that definitive treatment for donovanosis be given presumptively.
Management of donovanosis requires application of all the tried and trusted principles of STI control. Firstly, a rapport should be established with the patient. Many sufferers with donovanosis will have had lesions for a long time and will be extremely depressed. They may have low self esteem because of the physical nature of the lesions—large genital sores with an offensive odour—and may have delayed in presenting for help because of a sense of shame. This delay in itself will probably have resulted in lesions becoming larger thereby compounding previous anxieties. Many patients will have seen numerous medical practitioners often with limited interest in both STIs and genital ulceration. Reassurance about what the diagnosis is, how it will be treated, and the good prognosis expected are essential from the outset.
Drug treatment
There is a dilemma in recommending optimal treatment for donovanosis depending upon whether or not strict syndromic guidelines for GUD are recommended and adhered to. In most areas where donovanosis is found, chancroid is also prevalent and has a higher incidence. Syndromic protocols recommend treatment for syphilis and chancroid, usually with erythromycin for the latter.54 However, erythromycin is not the drug of choice for donovanosis, although it is recommended in pregnancy. If erythromycin is to be effective, higher doses are required for donovanosis than for chancroid.55 Currently, azithromycin is probably the best drug available for donovanosis in that it can be given intermittently, the total pill count is low, directly observed therapy is possible, and treatment can usually be stopped before ulcers have healed completely.56,57
Treatment recommendations
WHO guidelines recommend azithromycin 1 g immediately then 500 mg daily but do not state the duration of therapy.54 In Australia doses of either 1 g weekly for 4–6 weeks or less if healing is complete or 500 mg once daily for 1 week only were adequate.56 The Centers for Disease Control and Prevention (CDC) recommends 1 g weekly for at least 3 weeks or until all lesions have healed.58
Other antibiotics that may be effective if given for 3 weeks or until ulcers have healed fully include the following58:
co-trimoxazole 160–800 mg twice daily
ciprofloxacin 750 mg twice daily
doxycycline 100 mg twice daily
gentamicin 1 mg/kg three times daily intramuscularly or intravenously if no response in the first few days with other regimens.
Antibiotics introduced more recently and known to be effective include: ceftriaxone,59 norfloxacin (lower bioavailability than other quinolones),60 trovofloxacin.61
Pregnancy
Erythromycin 500 mg four times daily for at least 3 weeks.58
Duration of treatment, follow up, and sexual contacts
Patients should be followed up until resolution of any sign of disease. Recurrence is said to occur despite good initial responses.58 Epidemiological treatment can be considered in the absence of signs and symptoms in sexual partners of index cases. Female partners should be examined and a speculum examination included to detect possible cervical infection.
Complications
Carcinoma is the most serious complication but is relatively rare—0.25% in Rajam and Rangiah’s series33 although Donovania granulomatis antigens were found in nine of 62 cases of penile carcinoma in Jamaica.62 The histological distinction between squamous cell carcinoma and donovanosis may sometimes be difficult in which case a therapeutic trial of antibiotic treatment should always be given and the response monitored. Surgery may be required for advanced intractable lesions that cause tissue destruction.63 Other coexisting STIs, particularly syphilis, should always be suspected in cases that delay in presentation.
DONOVANOSIS AND HIV
In Durban, in a population where HIV had been recognised only recently, the proportion of men with donovanosis and HIV increased significantly as the duration of lesions increased suggesting that HIV was acquired through sexual intercourse in the presence of ulcers.64 Despite this, no specific control measures for donovanosis were introduced locally and indeed with the move to decentralise STI treatment and provide syndromic management, trained staff were withdrawn. Subsequently, the prevalence of HIV escalated rapidly in Durban reaching levels of >35% among antenatal clinic attenders by 2000.
The general consensus on the natural history of chancroid and syphilis in HIV infected individuals is unclear and so it is too with donovanosis. In pregnant women in Durban with donovanosis, the clinical presentation and outcome of disease were unaltered by HIV65 while in Mumbai, India, ulcers took longer to heal in HIV positive subjects (mean 26 days versus 17 days) despite similar CD4 counts in HIV positive and negative groups.66 Donovanosis failed to respond to conventional treatment with combinations of co-trimoxazole, tetracycline, and thiamphenicol in two AIDS patients in Brazil.67 As yet, there are no data about the efficacy of azithromycin in HIV positive patients although it would be expected to be effective.
DISEASE CONTROL AND PREVENTION
The limited geographical distribution of the disease would enable specific targeted interventions in areas with foci of infection.68 Specific programmes were first implemented in Papua New Guinea where house to house visits and medical examinations in Goilala district identified and treated donovanosis successfully with antibiotics in 3.4% of the population.29 The other earlier and larger epidemic in Papua New Guinea was controlled by annual examination and registration of the population, compulsory treatment and even admission to hospital with police guarding the wards.4 Elimination of donovanosis was a target set by a number of states in the United States when antibiotics first became available and there is no doubt that these programmes contributed significantly to the virtual demise of the condition in that country as did the improvement in overall hygienic standards. The evaluation of the current donovanosis initiative among Aboriginal communities in Australia, which has produced extremely encouraging initial results, will be awaited with interest.21
Despite the obvious benefits of tackling donovanosis with a public health approach aiming at elimination, patients with donovanosis appreciate a case management approach. Many with the condition have, in the past, virtually given up hope of being cured and suffered psychological sequelae while others have been driven to suicide. Careful explanation and reassurance are therefore very important to allay patients’ fears and restore faith in contemporary medicine that may be limited following previous medical mismanagement.
Improved control of donovanosis cannot be promoted in isolation from the other causes of GUD that also facilitate HIV transmission. They too have been largely ignored despite the very large number of HIV infections attributable to GUD in countries worst affected by the epidemic.69 In many of these countries, HIV has barely reached the political agenda and it is clear that there is still some way to go before the importance of GUD is acknowledged and research findings are turned into action on the ground.
CONCLUSIONS
Over the past 15 years, there has been renewed interest in donovanosis. The organism has been cultured after a gap of many years and a PCR test developed that should enable molecular diagnosis to be undertaken by well equipped diagnostic laboratories. These new molecular techniques should help to answer some of the remaining outstanding questions about the condition. For example, confirmation or not of sexual transmission should become clear by using PCR on stool samples from infected individuals to see if autoinoculation is a likely mode of transmission. It would also be interesting to undertake serial PCR tests on samples obtained after treatment has been started. Definitive diagnosis of donovanosis is often hindered by the early disappearance of Donovan bodies on tissue smears after the start of treatment. Furthermore, it is likely that a number of persistent ulcers in which pathogens were not identified could now be attributed to donovanosis by using PCR. While further developments of the multiplex PCR to incorporate donovanosis primers are awaited, it is disappointing that this technique has still not become more widely available.
Although comparative trials are yet to be undertaken, azithromycin has emerged as the treatment of choice and its use is justified if there is a reasonable index of suspicion that donovanosis is likely in the absence of diagnostic confirmatory tests. Treatment can be given once weekly and it is unnecessary to give it until complete healing is achieved because of the long half life. While further trials are needed to investigate the response of HIV positive subjects with significant immune impairment, the likelihood is that azithromycin will be effective in most situations.
Despite the evidence that has accumulated implicating GUD with enhanced transmission of HIV, few interventions have used this knowledge to produce specific targeted initiatives. Further attention would be paid to donovanosis if the importance of genital ulcers in fuelling the HIV epidemic were recognised more readily. Continued vigilance should be maintained so that the diagnosis of donovanosis is neither forgotten nor missed. Early diagnosis and treatment will have significant benefit not only for affected communities but also infected individuals who have often had a poor deal in the past.
REFERENCES
Footnotes
-
Series editor: David Lewis
Linked Articles
- Brief Encounters
- Web Top 10