edema
(redirected from interstitial edema)Also found in: Dictionary, Thesaurus, Encyclopedia.
Edema
Definition
Description
Causes and symptoms
- Immobility. The leg muscles normally contract and compress blood vessels to promote blood flow with walking or running. When these muscles are not used, blood can collect in the veins, making it difficult for fluid to move from tissues back into the vessels.
- Heat. Warm temperatures cause the blood vessels to expand, making it easier for fluid to cross into surrounding tissues. High humidity also aggravates this situation.
- Medications. Certain drugs, such as steroids, hormone replacements, nonsteroidal anti-inflammatory drugs (NSAIDs), and some blood pressure medications may affect how fast fluid leaves blood vessels.
- Intake of salty foods. The body needs a constant concentration of salt in its tissues. When excess salt is taken in, the body dilutes it by retaining fluid.
- Menstruation and pregnancy. The changing levels of hormones affect the rate at which fluid enters and leaves the tissues.
- Heart failure. When the heart is unable to maintain adequate blood flow throughout the circulatory system, the excess fluid pressure within the blood vessels can cause shifts into the interstitial spaces. Left-sided heart failure can cause pulmonary edema, as fluid shifts into the lungs. The patient may develop rapid, shallow respirations, shortness of breath, and a cough. Right-sided heart failure can cause pitting edema, a swelling in the tissue under the skin of the lower legs and feet. Pressing this tissue with a finger tip leads to a noticeable momentary indentation.
- Kidney disease. The decrease in sodium and water excretion can result in fluid retention and overload.
- Thyroid or liver disease. These conditions can change the concentration of protein in the blood, affecting fluid movement in and out of the tissues. In advanced liver disease, the liver is enlarged and fluid may build-up in the abdomen.
- Malnutrition. Protein levels are decreased in the blood, and in an effort to maintain a balance of concentrations, fluid shifts out of the vessels and causes edema in tissue spaces.
- Blood clots. Clots can cause pooling of fluid and may be accompanied by discoloration and pain. In some instances, clots may cause no pain.
- Weakened veins. Varicose veins, or veins whose walls or valves are weak, can allow blood to pool in the legs. This is a common condition.
- Infection and inflammation. Infection in leg tissues can cause inflammation and increasing blood flow to the area. Inflammatory diseases, such as gout or arthritis, can also result in swelling.
- Lymphedema. Blocked lymph channels may be caused by infection, scar tissue, or hereditary conditions. Lymph that can't drain properly results in edema. Lymphedema may also occur after cancer treatments, when the lymph system is impaired by surgery, radiation, or chemotherapy.
- Tumor. Abnormal masses can compress leg vessels and lymph channels, affecting the rate of fluid movement.
Diagnosis
Treatment
- Reducing sodium intake. A high sodium level causes or aggravates fluid retention.
- Maintaining proper weight. Being overweight slows body fluid circulation and puts extra pressure on the veins.
- Exercise. Regular exercise stimulates circulation.
- Elevation of the legs. Placing the legs at least 12 in (30.5 cm) above the level of the heart for 10-15 minutes, three to four times a day, stimulates excess fluid re-entry into the circulatory system.
- Use of support stocking. Elastic stockings, available at most medical supply or drug stores, will compress the leg vessels, promoting circulation and decreasing pooling of fluid due to gravity.
- Massage. Massaging the body part can help to stimulate the release of excess fluids, but should be avoided if the patient has blood clots in the veins.
- Travel breaks. Sitting for long periods will increase swelling in the feet and ankles. Standing and/or walking at least every hour or two will help stimulate blood flow.
Alternative treatment
Key terms
Resources
Organizations
edema
[ĕde´mah]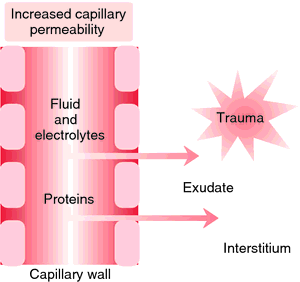
During the initial stage of pulmonary edema, patients may complain of restlessness and anxiety and the feeling that they are getting a common cold. Other signs include a persistent cough, slight dyspnea, and intolerance to exercise. On auscultation, rales can be heard over the dependent portion of the lung. As fluid continues to fill the pulmonary interstitial spaces the dyspnea becomes more acute, respirations increase in rate, and there is audible wheezing. The cough becomes productive of frothy sputum tinged with blood, giving it a pinkish hue. Eventually, if the condition persists, the patient becomes less responsive to stimuli as levels of consciousness decrease. Ventricular arrhythmias develop and breath sounds diminish. In some patients these phases are telescoped as the pulmonary edema develops rapidly and the final stages of respiratory insufficiency are evident in a very short period of time.
Treatment is aimed at enhancing gas exchange, reducing fluid overload, and strengthening and slowing the heart beat. To accomplish these goals the patient is often given oxygen by mask or through mechanically assisted ventilation. Drug therapy includes diuretics to remove excess alveolar fluid and morphine to relieve anxiety and reduce the effort of breathing. Administration of other medications depends on the cause of the edema, as well as what other problems the patient may be having.
e·de·ma
(e-dē'mă),edema
alsooedema
(ĭ-dē′mə)edema
Fluid retention, water retention Physical exam An excess of fluid in cells or tissues due to disease or injury, quantified as 1+, 2+, 3+. See Angioneurotic edema, Brawny edema, Cerebral edema, Cyclic edema, Cytotoxic edema, Flash pulmonary edema, Hereditary angioneurotic edema, High-altitude cerebral edema, High-altitude pulmonary edema, Leukoedema, Macular edema, Malignant edema, Pedal edema, Pseudopapillaedema, Pulmonary edema.e·de·ma
(ĕ-dē'mă)Synonym(s): oedema.
edema
(e-de'ma) (-de'mat-a) plural.edemasplural.edemata [Gr. oidema, swelling, tumor])
Etiology
Edema may result from increased permeability of the capillary walls; increased capillary pressure due to venous obstruction or heart failure; lymphatic obstruction; disturbances in renal function; reduction of plasma proteins; inflammatory conditions; fluid and electrolyte disturbances, esp. those causing sodium retention; malnutrition; starvation; or chemical substances such as bacterial toxins, venoms, caustics, and histamine. Diagnostic studies ( thorough history, physical examination, urinalysis, serum chemistries and liver functions, thyroid function, and chest x-ray) help determine the cause and guide treatment.
Treatment
Bed rest helps relieve lower extremity edema. Sitting with the feet and legs elevated may also reduce edema in the lower extremities. Dietary salt should be restricted to less than 2 g/day. Fluid intake may be restricted to about 1500 ml in 24 hr. This prescription may be relaxed when free diuresis has been attained. Diuretics relieve swelling when renal function is good and when any underlying abnormality of cardiac function, capillary pressure, or salt retention is being corrected simultaneously. Any effective diuretic may be used. Diuretics are contraindicated in preeclampsia and when serum potassium levels are very low (< 3.0 mEq/dl). They may be ineffective in edema associated with advanced renal insufficiency. The diet in edema should be adequate in protein, high in calories, and rich in vitamins. Patients with significant edema should weigh themselves daily to gauge fluid loss or retention.
Patient care
Edema is documented according to type (pitting, nonpitting, or brawny), extent, location, symmetry, and degree of pitting. Areas over bony prominences are palpated for edema by pressing with the fingertip for 5 sec, then releasing. Normally, the tissue should immediately rebound to its original contour; therefore the depth of indentation is measured and recorded. The patient is questioned about increased tightness of rings, shoes, waistlines of garments, and belts. Periorbital edema is assessed; abdominal girth and ankle circumference are measured; and the patient's weight and fluid intake and output are monitored. Fragile edematous tissues are protected from damage by careful handling and positioning and by providing and teaching about special skin care. Edematous extremities are mobilized and elevated to promote venous return, and lung sounds auscultated for evidence of increasing pulmonary congestion. Prescribed therapies, including sodium restriction, diuretics, ACE inhibitors, protein replacement, and elastic stockings are provided, and the patient is instructed in their use.
angioneurotic edema
Angioedema.Berlin edema
Commotio retinae.brain edema
edema bullosum vesicae
cardiac edema
cerebral edema
Brain edema.dependent edema
diabetic macular edema
edema of the glottis
Symptoms
Initially, hoarseness and, later, complete aphonia characterize this condition. Other symptoms are extreme dyspnea, at first on inspiration only, but later also on expiration; stridor; and a barking cough when the epiglottis is involved.
high-altitude pulmonary edema
Abbreviation: HAPEinflammatory edema
laryngeal edema
malignant edema
negative pressure pulmonary edema
edema neonatorum
)
)
pitting edema
post-traumatic edema
Traumatic edema.pretibial edema
pulmonary edema
Etiology
Fluid may seep out of the alveolar capillaries if these blood vessels are damaged and become excessively permeable to liquids (noncardiogenic pulmonary edema) or if hydrostatic pressures within blood vessels exceed the strength of the normal alveolar capillary wall (cardiogenic pulmonary edema). Cardiogenic pulmonary edema can result from any condition that compromises left ventricular function, causing elevations in pulmonary venous and capillary hydrostatic pressures (congestive heart failure), including myocardial infarction, ischemia, or myocardial stunning; severe valvular heart disease; arrhythmias; excessive intravenous fluid administration; and diastolic dysfunction.
Noncardiogenic pulmonary edema usually results from blood vessel injury, as happens in the adult respiratory distress syndrome (sepsis, shock, aspiration pneumonia, airway obstruction). Occasionally, protein-rich fluid floods the lungs from drug exposure (such as heroin overdose), hypoalbuminemia, high-altitude exposure (mountain sickness), fresh water aspiration in near drowning, hemorrhage in or around the brain, or other conditions. Pulmonary edema can occur as a chronic or acute condition.
Symptoms
Chronic symptoms include dyspnea or exertion, nocturnal dyspnea, orthopnea, and cough. When pulmonary edema develops rapidly, patients experience a rapid onset of shortness of breath and suffocation and often demonstrate labored, noisy breathing; cough producing frothy, bloody sputum; gasping; anxiety; palpitations; and altered mental status caused by inadequate oxygenation. Signs of the condition include a rapid respiratory rate, heaving of the chest and abdomen, intercostal muscle retractions, diffuse crackles on lung exam, and, often, cold, clammy skin with diaphoresis and cyanosis. Tachycardia, jugular vein distension, and a diastolic (S3) gallop occur. As cardiac output decreases, the pulse becomes thready, and blood pressure falls. Pulmonary artery catheterization helps identify left-sided failure (elevated pulmonary wedge pressures), and arterial blood gases show hypoxia. Profound respiratory alkalosis occurs when patients hyperventilate when trying to increase their oxygenation; acidosis may occur with respiratory fatigue and failure. To improve the movement of air into and out of the chest, the patient will often sit upright to breathe and resist lying down.
Treatment
Oxygen (in high concentrations by cannula, face mask, or nonrebreather mask) should be administered immediately. Assisted ventilation (continuous positive airway pressure [CPAP] or intubation with mechanical ventilation) may be needed to reach acceptable levels of PaO2 and improve acid-base balance. Morphine sulfate, nitrate vasodilators (IV nitroglycerin or nitroprusside) and loop diuretics are typically given to patients with cardiogenic pulmonary edema to improve dyspnea, alter preload and afterload on the heart, and promote diuresis. Angiotensin-converting enzyme inhibitors, inotropic drugs (digoxin), antiarrhythmic agents, beta-adrenergic blockers, human B-type natriuretic peptide, and phosphodiesterase inhibitors may be used in selected circumstances. Bronchodilators may also be administered. Depending on the underlying cause, invasive interventions may occasionally include coronary angiography, intra-aortic balloon pump therapy, or surgical interventions such as coronary artery revascularization or valve repair, or ventricular assist device therapy.
Prognosis
The outlook is good if the condition is stabilized or reversed with treatment.
Patient care
The patient's head is elevated; respirations and ventilatory effort are assessed. Oxygen is administered as prescribed, with care taken to limit the flow rate in patients whose respiratory drive is compromised. The lungs are auscultated for adventitious breath sounds such as crackles, gurgles, and wheezes, and the heart is assessed for apical rate and gallops. The patient is monitored for a cough productive of pink, frothy sputum. The skin is checked for diaphoresis and pallor or cyanosis. A medication history is collected, esp. for cardiac or respiratory drugs and use of recreational drugs. The patient's cardiac rate and rhythm, blood pressure, and oxygen saturation levels are monitored continuously. An intravenous (IV) line administering normal saline solution (NSS) is inserted at a keep-vein-open rate to provide access for medication administration. Prescribed first-line drug therapy is administered, and the patient's response to the drugs is evaluated. IV morphine slows respirations, improves hemodynamics, and reduces anxiety. It should be administered before initiating continuous positive air pressure (CPAP). CPAP improves oxygenation and decreases cardiac workload, thus decreasing the need for intubation and ventilation with positive end-expiratory pressure (PEEP). An indwelling urinary catheter is inserted to monitor the patient's fluid status; diuresis should begin within 30 min of administration of an IV loop diuretic. Pulmonary edema is a life-threatening respiratory emergency. Everyone involved with the patient must remain calm and quiet, provide ongoing reassurance, and validate everything occurring through basic and simply understood explanations. After the crisis resolves, health care providers should discuss with the patient his or her feelings about the episode and give thorough explanations of what occurred. The at-risk patient is taught early warning signs to act on immediately (such as weight gain or increasing peripheral edema), in an effort to recognize and prevent future episodes. Medications and dietary and lifestyle restrictions are explained (low-sodium diet, losing weight, smoking cessation), and written information provided for home review. The patient should be encouraged to enroll in a cardiac rehabilitation program (as applicable) for regular exercise tailored to his condition.
purulent edema
reexpansion pulmonary edema
Abbreviation: RPE, REPEReinke edema
See: Reinke edemasalt-induced edema
traumatic edema
edema
see OEDEMA.oedema
e·de·ma
(ĕ-dē'mă)Patient discussion about edema
Q. does mosquito bites considered as an edema a bet with a friend- please help solve an issue an help me win a new I pod :)
Q. what is "pulmonary edema" and what are the risks? my Dr. told me I'm in a risk group for pulmonary edema, he tried to explain what it is but i didn't understand fully...if someone may give me a brief explanation- I'll appreciate it!