by Ritchie C. Shoemaker, MD
Medical Director, Center for Research on Biotoxin Associated Illnesses
David Lark
Mycologist, MouldLabs, Australia
James C. Ryan, PhD
Chief Science Officer, ProgeneDx

Editor’s Note: Exposure to mold in water-damaged buildings (WDBs) causes a frustrating number of puzzling symptoms and eventually leads to chronic inflammatory response syndrome (CIRS), as explained in the first article of this five-part series, published in the July 2019 issue. In Parts 2 and 3 (August/September 2019; October 2019), the authors explained how to maintain the building envelope and CIRS diagnosis procedures.
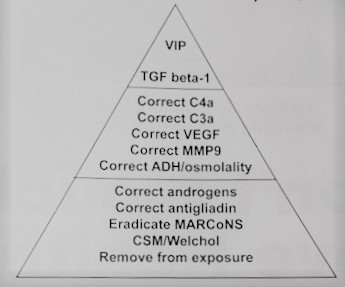
The Treatment Steps
Removal from exposure is the first step in treatment. This is followed by use of bile acid sequestrants, including cholestyramine or Welchol. Removal of biofilm-forming MARCoNS (multiple antibiotic-resistant coagulase negative staphylococci) is our third step.
(4) Correction of antigliadin anti-body positivity in non-celiac patients is key, with removal of dietary gluten indicated for those with the antigliadin antibodies. The role of MSH (alpha melanocyte stimulating hormone) deficiency is paramount in antigliadin antibody positivity and gluten sensitivity.
(5) Antidiuretic hormone (ADH) dysregulation of osmolality is shown routinely in over 80% of CIRS patients. Dysregulation can mean absolute high or low ADH; absolute high or low osmolality; or too little ADH for a given osmolality; or too much ADH for a given osmolality. These findings are paralleled by those that we see as abnormal for ACTH and cortisol. By looking at these two pairs of labs, we look at disruption of normal feedback relationships in MSH deficient patients.

(6) Androgen deficiency can be due to hypothalamic dysregulation of gonadotrophins, especially when MSH is low. A second mechanism for “Low T” is increased activity of aromatase. This enzyme converts androgens to estrone and then to estradiol. Don’t simply prescribe androgens!
(7) We must correct MMP-9, an indicator of pro-inflammatory cytokine effect on endothelial cells.
(8) We must also correct low (or high!) levels of VEGF. Interestingly, the effective use of omega-3s for correction of MMP-9 and VEGF has been a welcome addition to treatment.
(9) When C3a is elevated, there is presence of a bacterial membrane in blood. The membrane will serve as a source of attachment of the fragment of complement activation called C4bC2a that then provides a mechanism for attachment of C3 that will then lead to attachment of C5, 6, 7, 8 and 9. Complement puts a hole in bacterial cell, lysing the cell.

(10) C4a is probably the most important proinflammatory marker we have as part of the complement cascade. There is an enzyme, mannose binding protein associated serine protease-2 (MASP2), that can autoactivate. If that occurs, C4a will be produced even when no stimulation of MASP2 by antigen is occurring. This unique finding suggests “sicker quicker.”
(11) Reduction of TGF beta-1 is mandatory, not just for its role as a pro-inflammatory cytokine but also for its role activating a whole series of metabolic pathways involved with T-regulatory cell function in tissue and reduction of autoimmunity.
The last step is use of vasoactive intestinal polypeptide (VIP). See below.
SAIIE
An adaptation of the treatment protocol permits use of a diagnostic, prospective re-exposure trial. Called “Sequential Activation of Innate Immune Effects (SAIIE),” this protocol is used when we must show causation. As opposed to a case/control study, one that lets us conclude an association of exposure with symptoms, visual contrast sensitivity (VCS) deficits, proteomics or transcriptomic abnormalities, a prospective study design can confirm the presence of the epidemiologic concept of risk and therefore, causation.
We take a known case, a patient who meets the GAO case definition, use the Shoemaker Protocol to correct symptoms, VCS, and proteomics. Before starting, we know that the building suspected to be making the patient ill is contaminated. We will also know that the building where the patient is staying is safe (using ERMI or HERTSMI-2).
The first step, after informed consent is obtained, is after RX 1 (AC1, usually beginning on Friday). Symptoms, VCS and selected labs (C4a, MMP9, leptin, VEGF and von Willebrand’s profile) are recorded. All CIRS meds are stopped; the patient is kept away from the suspect building for three days, after having been exposed to “the ubiquitous fungi of the world.” On Monday morning, having completed the prospective trial of no-known exposure to a water-damaged building (WDB), symptoms, VCS, and labs are repeated. This step, called Home Off Meds (HOC), ends when blood is drawn on Monday.
The patient then enters the suspect building each day for three days, with study measures done daily. On Tuesday AM, symptoms, VCS and labs are performed, showing us what happened on day 1 of re-exposure (BOC-1, Tuesday). The patient re-enters the building. Symptoms, VCS and labs are performed on Wednesday, telling us what happened on day 2 of exposure (BOC-2). The patient returns to the WDB a third time, with symptoms, VCS and labs done on Thursday (BOC-3) showing us what happened on Wednesday, day 3. If the building is causative, by BOC-3 VCS will fall, symptoms will increase to approximately 95% of initial levels; labs will show distinctive profiles sorted by day of trial. Because the lab changes are stereotyped, according to known physiology, a scoring system can be applied to not only quantitate recrudescence of symptoms, but recrudescence of objective parameters as well.
As an aside, this protocol readily shows absence of validity to alternative hypotheses regarding causation, such as presence of mycotoxins in urine1 reflecting fungal infection, for example.
Perspective on Medical Rx

In the course of 23 years working on CIRS, there have been relatively few novel therapies that have stood the test of time. The Shoemaker Protocol is one of those therapies; it is marked by one intervention at a time for 30 days in sequence, with monitoring of diagnostic biomarkers before and after any given intervention. This methodical approach lets us identify what is working with treatment and what is not.

Initially, when symptoms persisted beyond (a) removal from exposure and then (b) use of binders, it was almost a trial and error approach to patient-centered research that brought the protocol to its current status. The protocol is fluid in the sense that there are new approaches to treatment that are evolving as the disease itself evolves. A simple example is the emergence of multiple unusual bacterial resistances in MARCoNS, initially in users of anti-fungal medications. A previously effective nasal spray, used safely and effectively from 2002-2015, became useless in a span of weeks. Sharing plasmids for bacterial resistance, likely due to horizontal gene transfer, is what the promiscuous MARCoNS do! What happened? The organisms changed; our treatments changed to continue to be effective.
Perspective on Treatment of WDB
The treatment protocol begins with one step that has been called the hardest of all: removal from exposure. Removal from exposure can mean either literally moving away from a school, workplace or residence; or removing particulates from the air and elimination of reservoirs of potential particulates found inside WDBs. Remediation of a building can be expensive; alternatively, correction of particulate reservoirs can be agonizingly obsessive, especially when remediation isn’t completed. The advantage of clearing the air and reservoirs of particulates is that we are not talking about burning a house down or leaving all possessions, walking out with the clothes you have on. What we are talking about is correction of the source of inhalation of particulates, understanding we may not have eliminated all potential sources of contamination.
Remediation is a subject for many thousands of words on another day. A few concepts will be shared here. Follow the ABCs: Abate the water intrusion. Building materials that are contaminated must be removed (or be encapsulated if structurally irreplaceable). Clean reservoirs on possessions; clean reservoirs in air; and clean reservoirs on walls, floors and ceilings. Every room must be cleaned in a given building if air from one room could get into another. Even though many individuals aren’t going to be affected by CIRS; cleaning must be performed assuming that all who enter the rooms in the future are CIRS patients. Finally, if you are talking with a remediator who doesn’t use HERTSMI-2 to clear a building as cleaned, you can’t assume the building is safe for a CIRS patient to re-occupy.
The Shoemaker Protocol is a methodical approach to treating chronic inflammatory response syndrome.
By taking another look at the section on definition of WDB, we can look at our check list for what has been found to be present and what is not present; stated another way, what is not safe about the house and what is safe about the house, for example. We know that there is no such thing as a safe basement even though people do all they can to make such structures safe. In treatment, there will be a dedicated air sanitation device running 24/7 in the basement. We look for maintenance of ambient humidity to be less than 55%. Sometimes that will require use of a dehumidifier with a transport mechanism combined with the dehumidifier to convey moisture removed from the air safely outside.
For prevention of exposure I often will use “three machines” approach. This approach will use an air sanitizer as the “heavy lifter.” I have no conflicts of interest to disclose in this regard, but I do use Air Oasis devices liberally, with a recent paper presented in January 2019, showing use of an Air Oasis device, the iAdaptAir, alone corrected transcriptomic abnormalities in a CIRS case,2 without causing adverse changes in a control.
The second machine is a HEPA filter. HEPA means high efficiency particulate air but it involves passing air in an indoor environment through a filter that is 0.3 microns in diameter when it starts, understanding that there will be reduction of pore size over time as particles can clog the filter (NB: clean filters regularly) with use of HEPA filters. In my cynical moments, I sometimes think that there is only one manufacturer of HEPA devices in the world, with a stack of different machine labels to be put on similar HEPA devices and shipped to the US. It seems that the less expensive devices perform equally as well as expensive devices if there is the 0.3-micron pore size filter. HEPA filters are often used one to a floor in a building, with one in the crawl space or the basement. Moving the HEPA units every twelve hours or so (but not between the basement and main house) helps deal with the boundary layer problem. Finally, with an Air Oasis sanitizer in use which will remove particulates from the air by essentially making them so heavy that they will precipitate on the floor, we must have a mechanism to vacuum these particulates up and remove them from the indoor space. So, the three machines are an air sanitizer, HEPA filter, and a vacuum cleaner (HEPA is better).
I do not feel that we need to use expensive machines, we just need to use inexpensive machines regularly, moving them from spot to spot and room to room (twice a day each!) to disrupt boundary layers of air, keeping airborne particulates in circulation and available for removal.
Selected Aspects of Treatment
Once we have begun the process of removal from exposure then we need to verify that the case definition has been met. As the case definition is satisfied, use of bile acid sequestrants begins. The oldest and least well tolerated of these compounds is cholestyramine (CSM). CSM has a positively charged nitrogen side chain built into a polystyrene chain. This long molecule is not absorbed so that when it is swallowed there will be a location of binding action beyond the stomach, in the duodenum and jejunum where CSM will bind to bile acids and biotoxins. CSM has been used for years to bind hydrocarbons such as DDT and DDE as well as PCBs but also will bind unusual compounds such as the M protein of Arava, a rheumatoid arthritis drug, as well as dioxin. CSM is organic glue! Once glued, down the tubes!
A less gastrointestinal troublemaker is Welchol (colesevelam), which is another bile acid sequestrant. CSM is taken one scoop (4 grams of active ingredient) four times a day on an empty stomach, waiting 30 minutes before eating or taking medication. Welchol on the other hand, is taken with food already in the stomach to prevent mild symptoms of reflux. The dose of Welchol is 625 mg, two tablets taken three times a day with food.
Many people will want the better efficacy of CSM, which does have 25% more binding sites compared to Welchol. I often suggest a “combo program,” taking CSM first thing in the morning and at bedtime, with Welchol taken with lunch and supper. The combo causes far less disruption of daily activities.
Unfortunately, despite our concerted efforts, we could never show salutary changes in objective biomarkers after we used “natural” binders like clay (bentonite), charcoal, pectin, chitin or chitosan, chlorella and more. Added to the “confirmation of no-benefit” list was absence of improvement in VCS scores.
A word on reduction of TGF beta-1. This step is vital for adequate performance of the treatment protocol. TGF beta-1 is a cytokine that has both pro- and anti-inflammatory responses. The difference between the two is due to tissue receptors including retinoic acid orphan receptor (ROR). In order to determine the role of TGF beta-1 in the complex issues of abnormalities in regulation of gene transcription, use of the test “Genomic Expression: Inflammation Explained” (GENIE) is recommended.
Treatment of elevated TGF beta-1 is accomplished by use of losartan (sold as Cozaar) a mild anti-hypertensive in the ARB class. If systolic blood pressure is less than 120, we can’t use losartan due to the risk of hypotensive episodes. Patients are recommended to measure blood pressures at least twice a day for at least two weeks at home with a reliable blood pressure measuring device to know whether there is blood pressure present over 120 that would sustain use of losartan. If blood pressures stay at, say 130/90, then losartan can be initiated in adults. The adult dose is 12.5 mg at bed, increasing to 25 mg as tolerated. Losartan is the only ARB that has the breakdown product, named EXP 3179, that lowers TGF beta-1. The rights to use of this molecule belong to Merck. One would hope that sometime in the future we would see a pure anti-TGF beta-1 medication made available to the public.
VIP: The last step is step #12, that being use of vasoactive intestinal polypeptide (VIP) to (i) correct residual proteomic abnormalities; (ii) correct transcriptomic abnormalities; (iii) correct grey matter nuclear atrophy. Simply stated, VIP is a remarkably safe regulatory neuropeptide that has been used in humans as a nasal spray in the US since 2008. It has a much longer prior history of use in Europe. VIP is currently available as a compounded medication; two groups are actively working with the FDA to create an IND.
VIP, 50 mcg/0.1ml, is most often used one spray taken four times a day independent of fasting. It has shown the ability to reduce pulmonary hypertension and markedly improve exercise tolerance. Higher doses are used for correction of transcriptomic abnormalities and gray matter nuclear atrophy. Please review the module on use of VIP before prescribing it. The module is found on www.survivingmold.com.
VIP in MCS: Some patients who are markedly intolerant of foods, medications and organic substances will have difficulty using cholestyramine or Welchol. For these patients, “mini-dose” VIP has been used with excellent results. By dosing VIP at 1/100 dilution with a steadily increasing number of doses used per day (“ramping up”), up to six doses a day, can then lead to 1/10 dilution following the same increasing dose schedule. Once 1/100 and then 1/10 are tolerated, then full-strength VIP can be initiated for approximately three weeks at which time VIP can be stopped. At that time, medications can usually be taken without adverse effects.
References
1. Kawamoto M, Page E. Notes from the field: use of unvalidated urine mycotoxin tests for the clinical diagnosis of illness-US 2014. MMWR 2015; 64(6): 157-158.
2. Shoemaker R, Lark D, Bennert J. Conference proceedings; Mold Congress, Fort Lauderdale, Florida, 1/16/2019. Clinical effects of air purification on transcriptomic profiles from two asymptomatic subjects.


Ritchie C. Shoemaker, MD, remains active in the field of biotoxin-associated illnesses, the focus of his practice since 1997. At that time, an outbreak of unexplained human illness, associated with exposure to blooms of a dinoflagellate, Pfiesteria piscicida, attracted his attention and interest. Pfiesteria was the first example of an acute and then chronic biotoxin-associated illness recognized and published in peer reviewed literature. Shoemaker’s two papers on diagnosis and then treatment were the first in the world’s literature on acquisition of illness from Pfiesteria in the wild. Since that time, other sources of biotoxin associated illnesses have come forward including other dinoflagellates, cyanobacteria and, most importantly, organisms resident in water damaged buildings. Shoemaker has spent the last 22 years treating patients and conducting research that unveils the extraordinary complexity of these illnesses, now called chronic inflammatory response syndromes (CIRS). Starting with no biomarkers and now progressing to over 25, CIRS has been shown to have abnormalities in proteomics and transcriptomics with differential gene activation, the final ultimate pathway of disease production in the world of chronic fatigue.
His collaboration with Dr. James C Ryan, transcriptomist, has led to multiple publications that have application, not just to chronic fatiguing illnesses but to the inflammatory illnesses of the 21st century including atherosclerosis, diabetes, obesity, and autoimmune illness.
As Shoemaker’s work has progressed on the complex problems of grey matter nuclear atrophy, a small but growing cohort of patients with multinuclear atrophy and cognitive impairment have led to improvements that may have application to illnesses such as Alzheimer’s disease.



