
A Longitudinal Study of Chronic Periodontitis in Two Cohorts of Community-Dwelling Elderly Australians

Abstract
:1. Introduction
2. Methods
2.1. Study Design, Setting and Participants
2.2. Data Collection
2.3. Outcome Variables
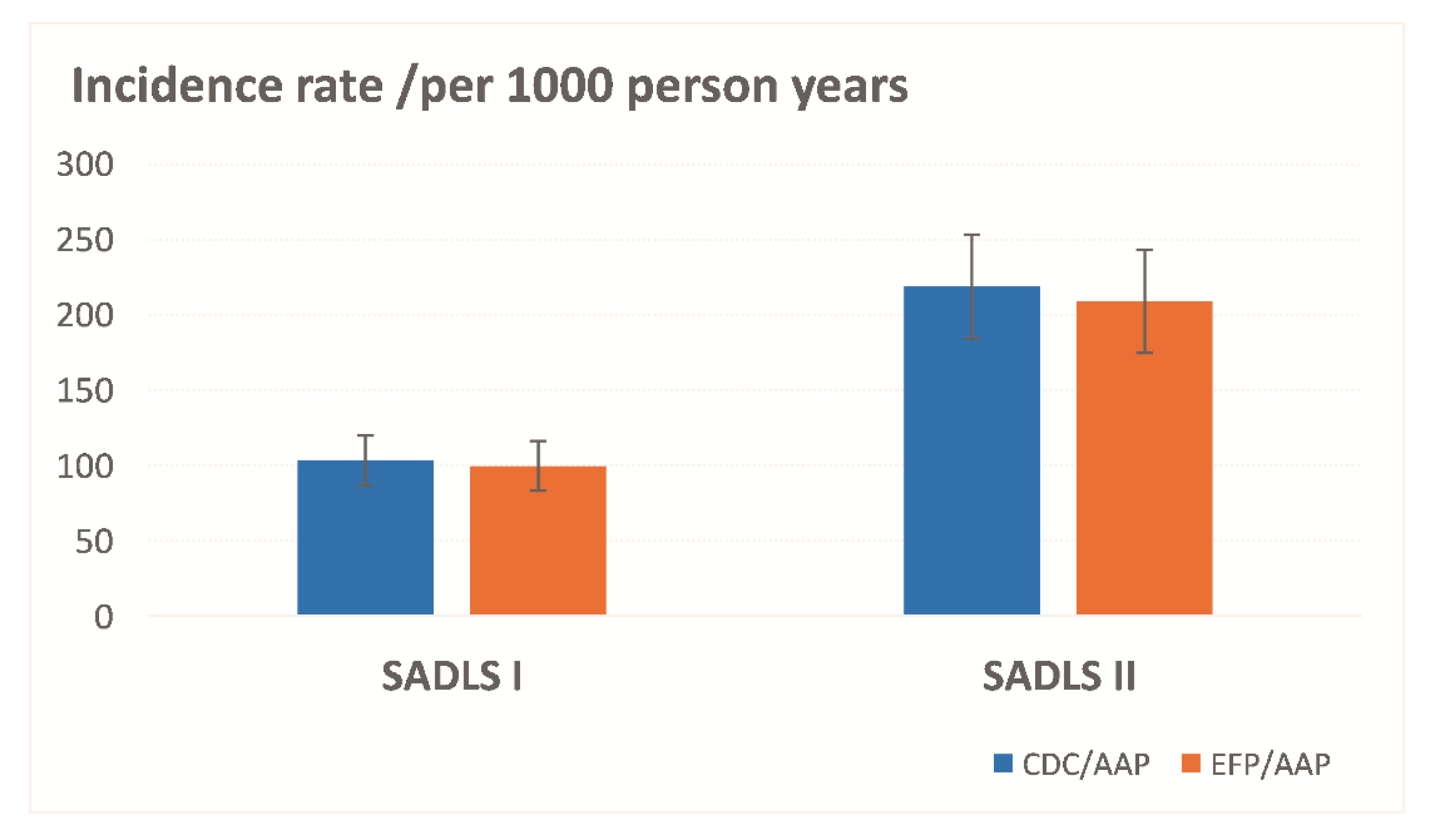
- The incidence of periodontitis (new cases) was defined from the baseline to two-year follow-up in the two studies as from no indication of periodontitis (‘No disease’) to some indication of periodontitis, such as: (1) from none to mild, moderate or severe periodontitis under the AAP/CDC case definition; and (2) from No/gingivitis to stage I, Stage II or Stage III–IV under the EFP/AAP case definition.
- The progression of periodontitis was defined from baseline to two-year follow-up in the two studies as: (1) from mild to moderate or severe, or from moderate to severe to tooth loss due to periodontitis under AAP/CDC case definition; and (2) from Stage I to Stage II, III or IV to tooth loss due to periodontitis under the EFP/AAP case definition.
2.4. Covariates
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W.; GBD 2015 Oral Health Collaborators. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef] [PubMed]
- Eke, P.I.; Borgnakke, W.S.; Genco, R.J. Recent epidemiologic trends in periodontitis in the USA. Periodontol. 2000 2020, 82, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Borgnakke, W.S.; Ogawa, H.; Yamaga, T.; Sato, M.; Minagawa, K.; Ansai, T.; Yoshihara, A.; Miyazaki, H. Effect of lifestyle on 6-year periodontitis incidence or progression and tooth loss in older adults. J. Clin. Periodontol. 2018, 45, 896–908. [Google Scholar] [CrossRef]
- Peres, M.A.; Lalloo, R. Tooth loss, denture wearing and implants: Findings from the National Study of Adult Oral Health 2017–2018. Aust. Dent. J. 2020, 65, S23–S31. [Google Scholar] [CrossRef]
- Lindner, M.; Arefnia, B.; Ivastinovic, D.; Sourij, H.; Lindner, E.; Wimmer, G. Association of periodontitis and diabetic macular edema in various stages of diabetic retinopathy. Clin. Oral Investig. 2021, 26, 505–512. Available online: https://link.springer.com/article/10.1007%2Fs00784-021-04028-x (accessed on 1 November 2021). [CrossRef] [PubMed]
- Chambrone, L.; Foz, A.M.; Guglielmetti, M.R. Periodontitis and chronic kidney disease: A systematic review of the association of diseases and the effect of periodontal treatment on estimated glomerular filtration rate. J. Clin. Periodontol. 2013, 40, 443–456. [Google Scholar] [CrossRef]
- Bourgeois, D.; Inquimbert, C.; Ottolenghi, L.; Carrouel, F. Periodontal Pathogens as Risk Factors of Cardiovascular Diseases, Diabetes, Rheumatoid Arthritis, Cancer, and Chronic Obstructive Pulmonary Disease—Is There Cause for Consideration? Microorganisms 2019, 7, 424. [Google Scholar] [CrossRef]
- Luo, L.S.; Luan, H.H.; Wu, L.; Shi, Y.J.; Wang, Y.B.; Huang, Q.; Xie, W.Z.; Zeng, X.T. Secular trends in severe periodontitis incidence, prevalence and disability-adjusted life years in five Asian countries: A comparative study from 1990 to 2017. J. Clin. Periodontol. 2021, 48, 627–637. [Google Scholar] [CrossRef]
- Slade, G.D.; Spencer, A.J.; Roberts-Thomson, K.F. Australia’s Dental Generations: The National Survey of Adult Oral Health 2004–06. Australian Institute of Health and Welfare. 2007. Available online: https://www.aihw.gov.au/reports/dental-oral-health/australias-dental-generations-survey-2004-06/contents/table-of-contents (accessed on 1 November 2021).
- Ha, D.H.; Spencer, A.J.; Ju, X.; Do, L.G. Periodontal diseases in the Australian adult population. Aust. Dent. J. 2020, 65, S52–S58. [Google Scholar] [CrossRef]
- Slade, G.D.; Spencer, A.J. Periodontal attachment loss among adults aged 60+ in South Australia. Community Dent. Oral Epidemiol. 1995, 23, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.J.; Brunelle, J.A.; Carlos, J.P.; Brown, L.J.; Loe, H. Oral Health of United States Adults. The National Survey of Oral Health in US Employed Adults and Settlors. 1985–1986. Bethesda; Publication No. 87-2868; National Institute of Dental Research, National Institutes of Health (NIH): Boston, MA, USA, 1987.
- Page, R.C.; Eke, P.I. Case definitions for use in population-based surveillance of periodontitis. J. Periodontol. 2007, 78, 1387–1399. [Google Scholar] [CrossRef] [PubMed]
- Del Pinto, R.; Pietropaoli, D.; Munoz-Aguilera, E.; D’Aiuto, F.; Czesnikiewicz-Guzik, M.; Monaco, A.; Guzik, T.J.; Ferri, C. Periodontitis and Hypertension: Is the Association Causal? High Blood Press. Cardiovasc. Prev. 2020, 27, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, H.; Berglund, J.S.; Renvert, S. Periodontitis, tooth loss and cognitive functions among older adults. Clin. Oral Investig. 2018, 22, 2103–2109. [Google Scholar] [CrossRef] [PubMed]
- Baeza, M.; Morales, A.; Cisterna, C.; Cavalla, F.; Jara, G.; Isamitt, Y.; Pino, P.; Gamonal, J. Effect of periodontal treatment in patients with periodontitis and diabetes: Systematic review and meta-analysis. J. Appl. Oral Sci. 2020, 28, e20190248. [Google Scholar] [CrossRef]
- Sanz-Sánchez, I.; Montero, E.; Citterio, F.; Romano, F.; Molina, A.; Aimetti, M. Efficacy of access flap procedures compared to subgingival debridement in the treatment of periodontitis. A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47, 282–302. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S. On behalf of the EFP Workshop Participants and Methodological Consultants. Treatment of stage I–III periodontitis—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef]
- Loos, B.G. Systemic markers of inflammation in periodontitis. J. Periodontol. 2005, 76, 2106–2115. [Google Scholar] [CrossRef]
- Pink, C.; Kocher, T.; Meisel, P.; Dörr, M.; Markus, M.R.; Jablonowski, L.; Grotevendt, A.; Nauck, M.; Holtfreter, B. Longitudinal effects of systemic inflammation markers on periodontitis. J. Clin. Periodontol. 2015, 42, 988–997. [Google Scholar] [CrossRef]
- Leite, F.R.M.; Nascimento, G.G.; Scheutz, F.; López, R. Effect of Smoking on Periodontitis: A Systematic Review and Meta-regression. Am. J. Prev. Med. 2018, 54, 831–841. [Google Scholar] [CrossRef]
- Eke, P.I.; Dye, B.A.; Wei, L.; Slade, G.D.; Thornton-Evans, G.O.; Borgnakke, W.S.; Taylor, G.W.; Page, R.C.; Beck, J.D.; Genco, R.J. Update on Prevalence of Periodontitis in Adults in the United States: NHANES 2009 to 2012. J. Periodontol. 2015, 86, 611–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| AAP/CDC | EFP/AAP | ||
|---|---|---|---|
| The American Association of Periodontology and the U.S. Centres for Disease Control and Prevention Case Definition [14] | The 2018 European Federation of Periodontology/American Academy of Periodontology Classification [2] | ||
| None/mild | Mild periodontitis is the presence of either two sites between adjacent teeth where CAL < 4 mm and PD < 5 mm. | Stage I | Periodontitis severity stage I is the presence of each tooth where 1 mm ≤ CAL ≤ 2 mm; no tooth loss due to periodontitis. |
| Moderate | Moderate periodontitis is the presence of either two sites between adjacent teeth where 4 mm ≤ CAL ≤ 6mm or at least two such sites have PD ≥ 5 mm. | Stage II | Periodontitis severity stage II is the presence of each tooth where 3 mm ≤ CAL ≤ 4mm; no tooth loss due to periodontitis. |
| Severe | Severe periodontitis is at least two sites between adjacent teeth where CAL ≥ 6 mm and there is at least one site PPD ≥ 5 mm. | Stage III–IV | Periodontitis severity stage III-IV is the presence of each tooth where CAL ≥ 5 mm or there is at last one site PPD ≥ 6 mm; or had tooth loss due to periodontitis of ≥4 teeth. |
| SADLS I (1991–1992) (n = 567) | SADLS II (2013–2014) (n = 201) | |||
|---|---|---|---|---|
| N | 95% CI | N | 95% CI | |
| Sample demographic characteristics | ||||
| Age groups | ||||
| 60–64 | 157 | 27.7 (24.0–31.4) | 54 | 27.4 (21.1–33.7) |
| 65–69 | 153 | 27.0 (23.3–30.6) | 65 | 33.0 (26.4–39.6) |
| 70–74 | 94 | 16.6 (13.5–19.6) | 41 | 20.8 (15.1–26.5) |
| 75–79 | 101 | 17.8 (14.7–21.0) | 21 | 10.7 (6.3–15.0) |
| 80–84 | 49 | 8.6 (6.3–11.0) | 12 | 6.1 (2.7–9.5) |
| ≥85 | 13 | 2.3 (1.1–3.5) | 4 | 2.0 (0.0–4.0) |
| Sex | ||||
| Female | 227 | 40.0 (36.0–44.1) | 91 | 46.0 (39.0–53.0) |
| Male | 340 | 60.0 (55.9–64.0) | 107 | 54.0 (47.0–61.0) |
| Married status | ||||
| Married/De-facto | 420 | 74.1 (70.5–77.7) | 148 | 75.1 (69.0–81.2) |
| Single | 147 | 25.9 (22.3–29.5) | 49 | 24.8 (18.8–31.0) |
| Born in Australia | ||||
| Yes | 387 | 68.4 (64.5–72.2) | 143 | 74.5 (68.3–80.7) |
| No | 179 | 31.6 (27.8–35.5) | 49 | 25.5 (19.3–31.7) |
| Education level | ||||
| Tertiary | 193 | 34.1 (30.2–38.1) | 36 | 18.3 (12.8–23.7) |
| Trade/diploma degree | 113 | 20.0 (16.7–23.3) | 61 | 31.0 (24.5–37.5) |
| Secondary | 260 | 45.9 (41.8–50.1) | 100 | 50.8 (43.7–57.8) |
| Household income | ||||
| High | 137 | 25.6 (21.9–29.3) | 64 | 37.4 (30.1–44.8) |
| Medium | 177 | 33.0 (29.0–37.0) | 49 | 28.7 (21.8–35.5) |
| Low | 222 | 41.4 (37.2–45.6) | 58 | 33.9 (26.8–41.1) |
| Oral health-related behaviours | ||||
| Dental insured | ||||
| Had | 244 | 43.4 (39.3–47.5) | 126 | 63.3 (56.6–70.1) |
| No | 318 | 56.6 (52.5–60.7) | 73 | 36.7 (29.9–43.4) |
| Smoke status | ||||
| Never smoked | 252 | 44.9 (40.8–49.0) | 116 | 59.2 (52.2–66.1) |
| Used smoker | 245 | 43.7 (39.6–47.8) | 72 | 36.7 (29.9–43.5) |
| Current smoker | 64 | 11.4 (8.8–14.0) | 8 | 4.1 (1.3–6.9) |
| Alcohol drinking | ||||
| No | 136 | 24.0 (39.3–47.5) | 36 | 18.3 (12.8–23.7) |
| Yes | 430 | 76.0 (72.4–79.5) | 161 | 81.7 (76.3–87.2) |
| Dental behaviours | ||||
| Oral hygiene (Tooth brushing) | ||||
| At least twice/day | 361 | 63.7 (59.7–67.6) | 138 | 69.3 (62.9–75.8) |
| Less than twice/day | 206 | 36.3 (32.4–40.3) | 61 | 30.7 (24.2–37.1) |
| Last dental visiting | ||||
| Less than 12 months | 360 | 63.7 (59.7–67.7) | 139 | 70.2 (63.8–76.6) |
| More than 12 months | 205 | 36.3 (32.3–40.3) | 59 | 29.8 (23.4–36.2) |
| Reasons for dental visiting | ||||
| Check | 252 | 44.7 (40.7–48.8) | 89 | 46.1 (39.0–53.2) |
| Problem | 312 | 55.3 (51.2–59.4) | 104 | 53.9 (46.8–61.0) |
| General Health | SADLS I (1991–1992) (n = 567) | SADLS II (2013–2014) (n = 201) | ||
|---|---|---|---|---|
| N | 95% CI | N | 95% CI | |
| Asthma | ||||
| No | 525 | 92.6 (90.4–94.8) | 165 | 86.8 (82.0–91.7) |
| Yes | 42 | 7.4 (5.2–9.6) | 25 | 13.2 (8.3–18.0) |
| Arthritis | ||||
| No | 280 | 49.5 (45.3–53.6) | 97 | 51.9 (44.6–59.1) |
| Yes | 286 | 50.5 (46.4–54.7) | 90 | 48.1 (40.9–55.4) |
| Cancer | ||||
| No | 502 | 88.8 (86.2–91.5) | 159 | 84.6 (79.4–89.8) |
| Yes | 63 | 11.2 (8.5–13.8) | 29 | 15.4 (10.2–20.6) |
| Cataracts | ||||
| No | 472 | 83.2 (80.2–86.3) | 147 | 80.3 (74.5–86.1) |
| Yes | 95 | 16.8 (13.7–19.8) | 36 | 19.7 (13.9–25.5) |
| COPD | ||||
| No | 505 | 89.2 (86.7–91.8) | 167 | 90.8 (86.5–95.0) |
| Yes | 61 | 10.8 (8.2–13.3) | 17 | 9.2 (5.0–13.5) |
| Diabetes | ||||
| No | 542 | 95.6 (93.9–97.3) | 161 | 85.2 (80.1–90.3) |
| Yes | 25 | 4.4 (2.7–6.1) | 28 | 14.8 (9.7–19.9) |
| Hypertension | ||||
| No | 365 | 64.4 (60.4–68.3) | 94 | 49.5 (42.3–56.6) |
| Yes | 202 | 35.6 (31.7–39.6) | 96 | 50.5 (43.4–57.7) |
| Heart diseases | ||||
| No | 465 | 82.3 (79.1–85.5) | 170 | 91.9 (87.9–95.9) |
| Yes | 100 | 17.7 (14.5–20.9) | 15 | 8.1 (4.1–12.1) |
| Osteoporosis or hip fracture | ||||
| No | 546 | 96.5 (94.4–98.0) | 168 | 89.8 (85.5–94.2) |
| Yes | 20 | 3.5 (2.0–5.1) | 19 | 10.2 (5.8–14.5) |
| Stroke | ||||
| No | 529 | 93.5 (91.4–95.5) | 182 | 97.3 (95.0–99.7) |
| Yes | 37 | 6.5 (4.5–8.6) | 5 | 2.7 (0.3–5.0) |
| Chronic diseases (At least one) | ||||
| No | 123 | 21.7 (18.3–25.1) | 29 | 14.7 (9.7–19.7) |
| Had | 444 | 78.3 (74.9–81.7) | 168 | 85.3 (80.3–90.3) |
| Number of diseases | ||||
| 0 | 123 | 21.7 (18.3–25.1) | 29 | 14.7 (9.7–19.7) |
| 1 | 163 | 28.7 (25.0–32.5) | 62 | 31.5 (24.9–38.0) |
| 2 | 151 | 26.6 (23.0–30.3) | 53 | 26.9 (20.7–33.2) |
| 3 | 79 | 13.9 (11.1–16.8) | 30 | 15.2 (10.2–20.3) |
| 4 | 34 | 6.0 (4.0–8.0) | 15 | 7.6 (3.9–11.4) |
| 5 | 10 | 1.8 (0.7–2.9) | 6 | 3.0 (0.6–5.5) |
| 6 | 6 | 1.1 (0.2–1.9) | 2 | 1.0 (0.0–2.4) |
| 7 | 1 | 0.2 (0.0–0.5) | 0 | 0.0 (0.0–0.0) |
| SADLS I (n = 567) | SADLS II (n = 201) | |||
|---|---|---|---|---|
| CDC/AAP | EFP/AAP | CDC/AAP | EFP/AAP | |
| IRR (95% CI) | IRR (95% CI) | IRR (95% CI) | IRR (95% CI) | |
| Sample demographic characteristics | ||||
| Age groups | ||||
| 60–64 | ref | ref | ref | ref |
| 65–69 | 0.87 (0.57–1.35) | 1.19 (0.76–1.87) | 1.01 (0.69–1.49) | 1.22 (0.79–1.90) |
| 70–74 | 0.98 (0.61–1.59) | 1.22 (0.74–2.02) | 0.68 (0.40–1.17) | 0.92 (0.53–1.60) |
| 75–79 | 1.01 (0.63–1.60) | 1.31 (0.80–2.12) | 0.98 (0.57–1.69) | 1.35 (0.78–2.40) |
| 80–84 | 0.87 (0.46–1.63) | 1.09 (0.56–2.07) | 0.90 (0.43–1.86) | 1.13 (0.53–2.39) |
| ≥85 | 1.37 (0.57–3.28) | 1.27 (0.44–3.66) | 0.54 (0.10–3.02) | 0.68 (0.12–3.82) |
| Sex | ||||
| Female | ref | ref | ref | ref |
| Male | 1.70 (1.19–2.40) | 1.44 (1.02–2.05) | 0.87 (0.63–1.20) | 0.87 (0.62–1.21) |
| Married status | ||||
| Married/De-facto | ref | ref | ref | ref |
| Single | 0.79 (0.54–1.17) | 0.95 (0.65–1.37) | 0.80 (0.53–1.21) | 0.91 (0.61–1.37) |
| Born in Australia | ||||
| Yes | ref | ref | ref | ref |
| No | 1.33 (0.97–1.84) | 1.34 (0.98–1.88) | 1.01 (0.70–1.45) | 1.07 (0.74–1.55) |
| Education level | ||||
| Tertiary | ref | ref | ref | ref |
| Trade/diploma degree | 0.92 (0.58–1.47) | 0.73 (0.43–1.23) | 0.96 (0.62–1.51) | 1.00 (0.64–1.56) |
| Secondary | 1.06 (0.75–1.51) | 1.12 (0.79–1.60) | 0.88 (0.58–1.35) | 0.78 (0.50–1.20) |
| Household income | ||||
| High | ref | ref | ref | ref |
| Medium | 1.14 (0.79–1.64) | 1.11 (0.76–1.62) | 0.93 (0.60–1.44) | 1.04 (0.66–1.65) |
| Low | 1.00 (0.66–1.51) | 1.08 (0.72–1.62) | 0.87 (0.57–1.34) | 0.94 (0.60–1.47) |
| Oral health and related behaviours | ||||
| Dental insured | ||||
| Had | ref | ref | ref | ref |
| No | 1.07 (0.78–1.48) | 1.17 (0.84–1.62) | 1.05 (0.75–1.45) | 0.92 (0.65–1.31) |
| Smoke status | ||||
| Never smoked | ref | ref | ref | ref |
| Used smoker | 1.71 (1.19–2.46) | 1.54 (1.06–2.22) | 0.83 (0.58–1.18) | 0.74 (0.50–1.08) |
| Current smoker | 2.18 (1.39–3.44) | 1.94 (1.21–3.10) | 1.23 (0.66–2.27) | 0.98 (0.46–2.09) |
| Alcohol drinking | ||||
| No | ref | ref | ref | ref |
| Yes | 1.44 (0.95–2.18) | 1.19 (0.80–1.76) | 1.05 (0.68–1.60) | 0.99 (0.64–1.51) |
| Oral hygiene (Tooth brushing) | ||||
| At least twice/day | ref | ref | ref | ref |
| Less than twice/day | 1.19 (0.86–1.63) | 1.10 (0.79–1.52) | 1.22 (0.89–1.68) | 1.25 (0.89–1.73) |
| Last dental visiting | ||||
| Less than 12 months | ref | ref | ref | ref |
| More than 12 months | 0.84 (0.60–1.18) | 0.84 (0.60–1.18) | 1.13 (0.81–1.57) | 0.91 (0.63–1.32) |
| Reasons for dental visiting | ||||
| Check | ref | ref | ref | ref |
| Problem | 1.01 (0.74–1.39) | 1.09 (0.79–1.51) | 0.93 (0.67–1.29) | 0.93 (0.66–1.31) |
| General health | ||||
| Asthma | ||||
| No | ref | ref | ref | ref |
| Yes | 1.29 (0.76–2.22) | 1.21 (0.69–2.14) | 0.94 (0.57–1.57) | 1.12 (0.69–1.81) |
| Arthritis | ||||
| No | ref | ref | ref | ref |
| Yes | 0.96 (0.70–1.33) | 1.11 (0.8–1.54) | 0.98 (0.71–1.35) | 0.88 (0.62–1.23) |
| Cancer | ||||
| No | ref | ref | ref | ref |
| Yes | 1.26 (0.80–2.00) | 1.33 (0.83–2.08) | 1.22 (0.83–1.82) | 1.20 (0.79–1.83) |
| Cataracts | ||||
| No | ref | ref | ref | ref |
| Yes | 1.49 (1.03–2.16) | 1.00 (0.64–1.56) | 1.02 (0.68–1.54) | 1.02 (0.66–1.57) |
| COPD | ||||
| No | ref | ref | ref | ref |
| Yes | 0.77 (0.43–1.40) | 0.98 (0.58–1.68) | 1.09 (0.64–1.86) | 1.16 (0.68–1.98) |
| Diabetes | ||||
| No | ref | ref | ref | ref |
| Yes | 1.59 (0.88–2.89) | 1.00 (0.46–2.24) | 1.61 (0.87–2.96) | 2.09 (1.01–4.33) |
| Hypertension | ||||
| No | ref | ref | ref | ref |
| Yes | 0.94 (0.67–1.32) | 0.92 (0.64–1.30) | 0.83 (0.60–1.14) | 0.91 (0.65–1.27) |
| Heart disease | ||||
| No | ref | ref | ref | ref |
| Yes | 1.39 (0.96–2.02) | 1.34 (0.91–1.97) | 0.60 (0.25–1.40) | 0.80 (0.38–1.67) |
| Osteoporosis or hip fracture | ||||
| No | ref | ref | ref | ref |
| Yes | 0.24 (0.03–1.60) | 0.24 (0.04–1.66) | 1.25 (0.78–1.98) | 1.01 (0.58–1.76) |
| Stroke | ||||
| No | ref | ref | ref | ref |
| Yes | 1.50 (0.89–2.53) | 0.95 (0.48–1.90) | 1.87 (1.17–2.98) | 1.97 (1.23–3.15) |
| Chronic diseases (At least one) | ||||
| No | ref | ref | ref | ref |
| Had | 1.07 (0.72–1.64) | 0.77 (0.53–1.11) | 1.06 (0.67–1.70) | 1.24 (0.73–2.11) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ju, X.; Harford, J.; Luzzi, L.; Mejia, G.; Jamieson, L.M. A Longitudinal Study of Chronic Periodontitis in Two Cohorts of Community-Dwelling Elderly Australians. Int. J. Environ. Res. Public Health 2022, 19, 11824. https://doi.org/10.3390/ijerph191811824
Ju X, Harford J, Luzzi L, Mejia G, Jamieson LM. A Longitudinal Study of Chronic Periodontitis in Two Cohorts of Community-Dwelling Elderly Australians. International Journal of Environmental Research and Public Health. 2022; 19(18):11824. https://doi.org/10.3390/ijerph191811824
Chicago/Turabian StyleJu, Xiangqun, Jane Harford, Liana Luzzi, Gloria Mejia, and Lisa M. Jamieson. 2022. "A Longitudinal Study of Chronic Periodontitis in Two Cohorts of Community-Dwelling Elderly Australians" International Journal of Environmental Research and Public Health 19, no. 18: 11824. https://doi.org/10.3390/ijerph191811824