General Topics

KEY POINTS
- Burn injuries are more common in low- and middle-income countries. Timely resuscitation and early grafting have improved survival following significant burn injury.
- Anaesthetic management of burn injuries must prioritise the short-term impact on upper airway function as a result of inhalational injury.
- Pulmonary oedema can occur following inhalational burn injuries or after severe burn injuries as a result of systemic inflammatory response syndrome.
- Appropriate early fluid resuscitation in severe burn injuries improves survival rates and can be guided by accessing special fluid resuscitation guidelines based on estimates of the skin area that is injured.
- Intraoperative management of severe burn injuries should focus on specific airway management, restoration of intravascular volume, careful monitoring and judicious drug administration.
- Pain control in severe burn injuries is complex, often requiring high-dose opioids including methadone as well as multiple adjuncts such as ketamine, lignocaine, clonidine and other non-opioid analgesics.
INTRODUCTION
Burn injuries contribute significantly to the global burden of disease and remain a leading cause of worldwide morbidity.1 Consequences of burn injury are dictated by the severity of tissue damage, ranging from simple first aid management to intensive and specialised interventions such as advanced resuscitation, complex pain management, progressive techniques of wound care management and major surgery. From a global perspective, more than 8 000 000 new cases of burns occur annually, with more than 95% of burn deaths occurring in low- and middle-income countries.2,3 Anaesthetic management of patients suffering from burn injury is complex, with special focus on fluid resuscitation, airway management, analgesia and infection control.
CAUSE OF BURN
A burn injury can have multiple aetiologies. Most aetiologies occur as a result of direct skin contact with a chemical, heat, electrical, friction or radiation source, causing damage to superficial tissues. The specific mechanism and extent of burn injury can strongly influence prognosis.
Inhalation injury occurs in 20% of burn injuries and arises from inhalation of smoke components that damage oropharyngeal and pulmonary airway structures. Burn patients with an inhalation injury are at risk of higher mortality due to sequalae that include asphyxiation from carbon monoxide poisoning, acute pulmonary oedema and bronchospasm. Systemic inflammatory response syndrome (SIRS) can also contribute, causing severe lung injury as well as organ failure.
PATHOPHYSIOLOGY OF BURN INJURY
Acute
An acute burn injury causes immediate localised effects as well as systemic effects, the extent of which can be improved though early intervention. Immediately following a burn insult, the local area undergoes cell death. This can be extremely painful due to activation of exposed injured nerve endings. In addition, tissue injury causes the release of many inflammatory mediators including histamine, leukotrienes, kinins and prostaglandins, which may initiate a systemic response if a large enough burn area is involved.
Burns involving more the 25% of total body surface area (TBSA) are at increased risk of systemic inflammatory response.4 In this early stage within the first 48 hours, also referred to as the ‘ebb phase’, a systemic response can lead to shock associated with low peripheral vascular resistance, decreased cardiac output, increased vascular permeability, hypercoagulability and hypoalbuminaemia, all of which can compromise potentially viable areas of tissue.5 Early careful wound management and rapid fluid resuscitation can reduce the TBSA susceptible to ischaemia and tissue damage. Following the initial metabolic changes, a ‘plateau phase’ occurs for a number of days in which an individual can experience hyperdynamic circulation as well as increased oxygen and glucose consumption.5
Long Term
Significant burn injury can result in chronic pain and have a negative impact on quality of life.6 More than half of patients with significant burn injuries report chronic pain years after the injury. The pathophysiology of chronic pain in burn injury is multifactorial. It involves prolonged intense nociceptive pain arising from damaged tissues and neuropathic pain arising from specific damage to, and inflammation involving, injured nerve fibres. Injured tissues as well as donor tissues can be affected. Repeated painful dressing changes can potentially prolong pain but are required to minimise infection and promote healing after burn injury. Additional factors accompanying chronic pain include scarring that interferes with musculoskeletal function, as well as psychological sequelae that result from physical disfiguration and potential loss of livelihood.7 It comes as no surprise that pain management of burns requires specialised care to minimise long-term sequelae.
BURN SEVERITY
Burn injuries are classified according to depth and involve the epidermis alone (first degree), dermis and epidermis (second degree or partial thickness) or epidermis, dermis and hypodermis (third degree or full thickness) (Figure). Full-thickness burns require significant intervention in the form of surgical debridement, full excision and grafting.8 Early excision and grafting, within 3 days of injury, has led to significant reduction in mortality from 45% to 9% in patients with greater than 30% TBSA burns that did not involve inhalation injury.9
When determining burn severity, patient age, TBSA involved, depth and mechanism of burn as well as specific body areas affected are considered. Notably, first-degree burns, involving the epidermis alone, otherwise known as superficial burns, are not counted in calculations of TBSA involvement.10 There is no consensus classification for what constitutes a major burn. One way of conceptualising major burns are burns that may need specialist intervention. The American Burn Association provides a helpful description of burn characteristics likely to benefit from specialist burns management (Table 1).11
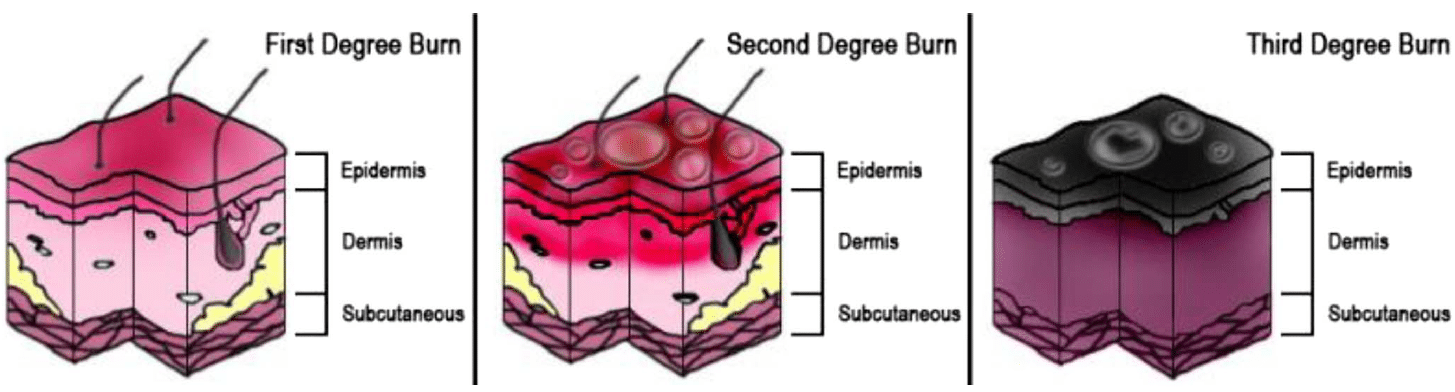
Figure. Diagram of burn degree. Source: Persian Poet Gal, distributed under Creative Commons Attribution 3.0 License 2006.
RESUSCITATION
Airway
Patients with a major burn injury often require immediate airway management, which can be challenging. Moreover, airway status can evolve rapidly after burn injury and may necessitate intervention at an early stage to secure the airway before it becomes more difficult to manage.12
Airway management can be complicated by limitation in mouth opening, airway and facial oedema and difficulties interpreting airway anatomy. Techniques to consider include either direct or video laryngoscopy for intubation, awake fibre-optic intubation, laryngeal mask insertion (if required for transient airway control) and, less commonly, emergency cricothyroid puncture and tracheostomy. Additional considerations may include securing airway devices with suturing, as tape or ties may not adhere to inflamed tissues or may interfere with burned areas that will require ongoing surgical management.
The role of early intubation in patients with burn injury has been recently questioned. Current guidelines from the International Society for Burn Injury suggest the only indication for intubation or tracheostomy should be for cases of current or evolving impairment of airway patency.13 Clinical signs include airway swelling, soot contamination of airway secretions, increasing work of breathing, hoarseness, stridor, dysphagia or increased salivation. This emphasises the importance of continued clinical assessment and early intervention should airway signs show a clear pattern of deterioration.
Breathing
Pulmonary complications, such as pulmonary oedema, remain a major cause of mortality after severe or inhalational burn injury.14 Symptoms include wheezing, hoarseness, bronchorrhoea and excessive sputum production together with tachypnoea and low oxygen saturations. Pulmonary oedema after burn injury can arise from 2 mechanisms: direct irritation by heat, smoke or chemicals or as part of a stereotypical lung response to severe injury, through systemic inflammation (SIRS). Patients with signs of inhalation injury or compromised pulmonary function may require oxygen therapy, continuous positive airway pressure or intubation and controlled ventilation.
Circulation/Fluid Resuscitation
Bleeding from wounds, evaporative losses and systemic responses involving vasoactive and inflammatory mediators can lead to impaired organ perfusion after burn injury. The phenomenon, known as ‘burn shock’, presents as marked hypoperfusion and hypovolemia occurring within the first 24 hours after a major burn and necessitating aggressive fluid resuscitation.15 Inadequate fluid resuscitation results in worsening burn injury and higher mortality.16 Burn shock remains the most common cause of death from severe burn injury in the first week.17
Various formulas have been devised to provide estimates of both rate and volume of fluid resuscitation (Table 2). Historically, the modified Brooke formula was used as well as the Parkland formula. The rule of 10 formula is a recent addition. These formulas are best used in the context of full assessment of vital sign patterns, urine output and cardiac filling pressures and trending creatinine.
While crystalloid is an accepted form of therapy for volume loss after burn injury, it may be more appropriate to transfuse colloid when intravascular volume levels are critical as part of a restrictive fluid strategy.18 More restrictive strategies are recommended for blood transfusions; transfusing for haemoglobin <7 g/dL compared with <10 g/dL revealed no difference in mortality or length of stay.19 Major burn injuries can also trigger disseminated intravascular coagulation. This may be exacerbated by the presence of haemodilution as a result of rapid resuscitation, endothelial damage, systemic inflammatory response or hypothermia.20 Current guidelines recommend factor replacement for the management of Disseminated intravascular coagulation (DIC) in these patients, with antifibrinolytic treatments such as tranexamic acid being reserved for those patients experiencing DIC as well as severe bleeding.21
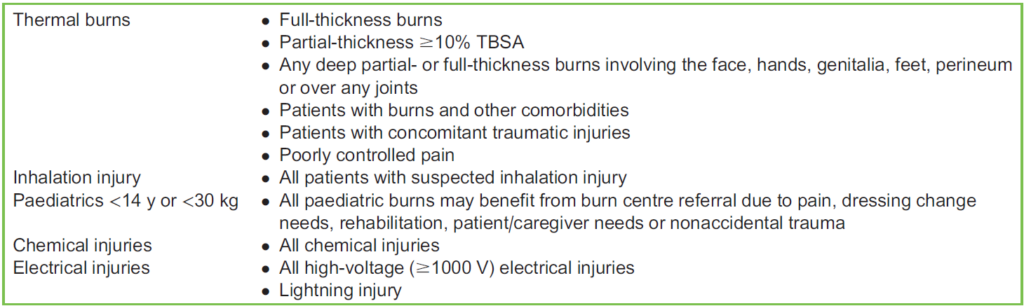
Table 1. Classifications of Burns Requiring Consideration for Transfer to Specialised Burn Centre. TBSA indicates total body surface area

Table 2. Commonly Used Fluid Resuscitation Formulas for a 60-kg Person Over 24 hours. Half of the total calculated volume should be administered in the first 8 hours in both the Parkland and Brooke formula. TBSA indicates total body surface area
TYPES OF SURGERIES
The purpose of surgery is to remove dead and unviable tissue to avoid infection and ongoing fluid loss and replace it with healthy skin or a reasonable substitute that can either temporarily or permanently cover the wound. Grafts can be classified as autografts (harvested from normal skin from the same patient) and can be either split-thickness (covers the epidermis and part of the dermis) or full-thickness (covers epidermis, dermis and hypodermis) or allografts (harvested from humans) or xenografts (harvested from nonhumans or synthetic material).
Where the patient’s own skin is not available, allografts or xenografts can be considered as a temporary cover for 1 to 2 weeks. This is an area of ongoing research. Donor material derived from cadaveric or living relative donor skin can be used as allografts. As well, a number of xenografts have been derived from porcine, bovine, synthetic, human, amniotic membrane and cultured cell sources.22
Operations involving excisions of burns and donor skin for grafting can result in deceptively high losses of blood because of the potentially large surface areas involved. Surgical use of topical vasopressors can further confuse volume loss estimates by temporarily elevating blood pressure in settings in which there is low intravascular volume. A pattern of continued high heart rate, together with falls in both blood pressure and cardiac filling pressure, may indicate hypovolemia that is unmasked after the effects of any vasopressor have worn off. This should be addressed with volume therapy and blood transfusion as appropriate.
ANAESTHETIC CONSIDERATIONS
Monitoring
Depending on the site of burn injury, intraoperative monitoring of patients with burn injuries can be difficult. Pulse oximetry may not function on fingers or toes, with alternative sites such as the nose, ear or tongue often needing to be used instead. Rarely, arterial blood gases might have to be used to estimate oxygenation level. Temperature probes are essential. The monitoring site can include oral, axillary, tympanic, rectal, bladder or oesophagus depending on the injured areas. Noninvasive blood pressure measurement is possible if the cuff can be applied to nonburnt areas; otherwise, invasive blood pressure monitoring is required. Electrocardiograms may be difficult to obtain as the adhesive may not stick to burnt tissues. Options for electrocardiogram monitoring include needle electrodes or skin staples.
Airway Considerations
Patients with burns are often transferred intubated and ventilated from intensive care or high-dependency unit facilities, so care must be taken to transfer patients to theatre without incident and to maintain existing ventilation therapies (positive end- expiratory pressure, pressure control, lower fractional oxygen therapies). Patients who are not intubated may present all the challenges previously discussed in the resuscitation section and may require strategies to manage difficult intubation scenarios. Suxamethonium may be safely used in burn patients in the first 48 hours. After that, however, its use may cause an exaggerated hyperkalaemic response in acutely burned patients.12
Analgesia
Analgesia for severe burn injuries can be challenging to manage. Opioid requirements in these patients can be significant and remain the mainstay of analgesia in severe burn injury.23 In many cases, high-dose infusions of opioids and sedatives are commenced to aid endotracheal tube tolerance. This may create opioid tolerance, leading to higher opioid requirement. Specialist pain management is desirable in these patients, with strategies such as opioid rotation, introduction of opioid-sparing analgesic strategies and careful opioid de-escalation.
Opioid-sparing agents include ketamine and lignocaine infusion.24 As a patient with burn injury progresses in their care from major graft surgery to ward-based dressings changes, ketamine as well as non-opioid analgesia is often added to existing opioid therapy to facilitate conscious sedation. Nonpharmacologic therapies such as virtual reality devices and music therapy have shown some promise in recent years to aid dressing changes, particularly in the paediatric burn population.25
Vascular Access
Since significant fluid shifts and volume losses occur in this patient population, vascular access is crucial but may also present special challenges. Invasive monitoring and large-bore venous lines are essential as burn patients have large, exposed surface areas leading to unexpectedly high losses, especially during first presentation and during surgical procedures. Such access can facilitate rapid fluid resuscitation, provide access and monitoring as well as facilitate inotropic support.26 Lines should be sited in areas that are not in the surgical field. Suturing and ties rather than standard vascular access adhesive dressings may be needed. The use of ultrasound to visualise arteries and veins may be required to guide placement.
Nutrition and Thermoregulation
Adequate nutritional support is essential in severe burn management, particularly in individuals with burns exceeding 40% TBSA who experience doubling of their basal metabolic rate.7 The enteral route is preferred to facilitate postpyloric feeding to avoid effects of associated gastric stasis. If regular oral feeding is not possible, nasogastric or total parental nutrition options must be explored, as insufficient nutrition following a burn injury has been correlated with increased mortality.27
As discussed above, monitoring of temperature in patients with severe burns can be challenging, but is vital for detecting thermodysregulation. This can involve severe hypothermia due to heat and fluid loss as well as profound hyperthermia, which can lead to multiorgan failure. Hyperthermia in major burn patients can be a sign of altered hypothalamic thermal setpoint, a sign of an infectious complication or transfusion reaction. All episodes of hyperthermia must be investigated appropriately as infections contribute to approximately half of all deaths due to burn injury.28
PHARMACOLOGIC CONSIDERATIONS
Patients with significant burn injuries have altered pharmacodynamic responses as well as alterations in pharmacokinetic parameters such as volume of distribution, levels of protein binding and hepatic and renal clearance.12, 29 These pathophysiological changes mean that careful titration and monitoring of commonly used anaesthetic drugs may be required.
Burn injury–related changes cause proliferation of extrajunctional acetylcholine receptors that release more potassium into the extracellular space, predisposing to life-threatening hyperkalaemia when suxamethonium is used. This risk appears to be greatest in patients more than 48 hours after and for up to 1 year postinjury.30
Nondepolarising neuromuscular blocking agents (NMBAs) may also have altered pharmacodynamics in burn patients, and this is thought to be multifactorial. An increased dose of rocuronium 1.2 to 1.5 mg/kg for rapid sequence induction is recommended, with effective paralysis time being approximately 90 seconds compared with 60 seconds in the nonburn population.31 This is thought to be due, at least in part, to the aforementioned presence of extrajunctional acetylcholine receptors, which bind nondepolarising NMBAs and will compete with junctional receptors.
Plasma protein concentration and binding capabilities may be drastically altered after severe burn injury. Significant hypoalbuminemia can occur due to protein-rich fluid loss and decreased hepatic synthesis. In addition, alpha 1-acid glycoprotein (AAG) concentrations can increase as part of the inflammatory response following significant burn injury. These can affect protein-bound anaesthetic and analgesic drugs. Drugs bound to albumin may be present in a higher free concentration. Conversely, drugs, such as local anaesthetics and analgesic agents, such as alfentanil, which are primarily bound to AAG, will have lower free concentrations than in the nonburn population.32 Pharmacodynamic changes may also arise as a result of continued exposure to opioid therapy for relief of sustained pain, resulting in opioid tolerance.33
LONG-TERM CONSIDERATIONS
Improved resuscitation management and surgical techniques have led to improved mortality rates following severe burn injury. Despite this, survivable burn injuries can create long-term issues that can significantly affect quality of life. Approximately 1 of every 3 patients develops at least 1 contracture following a burn injury, which can limit mobility and function.34 These contractures can require further surgeries many months after the original injury and cause additional scarring as well as contribute to chronic pain. Careful consideration must be given to airway management, muscle relaxant choice as well as positioning during surgery in these patients.
SUMMARY
Burn injuries affect millions of individuals each year, carry significant morbidity and mortality and disproportionately occur in lower socioeconomic populations. Anaesthetic and resuscitative strategies need to be adapted specifically for this patient population due to airway dangers, haemodynamic perturbations, direct effects of injuries, acute and chronic pain and altered responses to drug therapy. Ongoing management and follow-up in this patient population is essential, with many patients experiencing long-term issues years after the initial injury.
REFERENCES
- Jeschke MG, van Baar ME, Choudhry MA, et al. Burn injury. Nat Rev Dis Primers. 2020;13:6(1):11.
- Peck MD. Epidemiology of burns throughout the world. Part I: distribution and risk factors. Burns. 2011;37(7):1087-1100.
- Yakupu A, Zhang J, Dong W, et al. The epidemiological characteristic and trends of burns globally. BMC Public Health. 2022: 22:1596.
- Vivó C, Galeiras R, del Caz MD. Initial evaluation and management of the critical burn patient. Med Intensiva. 2016;40(1): 49-59.
- Jeschke MG. Postburn hypermetabolism: past, present, and future. J Burn Care Res. 2016;37(2):86-96.
- Moi AL, Haugsmyr E, Heisterkamp H. Long-term study of health and quality of life after burn injury. Ann Burns Fire Disasters. 2016;31;29(4):295-299.
- McGovern C, Puxty K, Paton L. Major burns: part 2. Anaesthesia, intensive care and pain management. BJA Educ. 2022;22(4): 138-145.
- Martin NA, Falder S. A review of the evidence for threshold of burn injury. Burns. 2017;43(8):1624-1639.
- Herndon DN, Barrow RE, Rutan RL, et al. A comparison of conservative versus early excision. Therapies in severely burned patients. Ann Surg. 1989;209(5):547-552.
- Browning JA, Cindass R. Burn debridement, grafting, and reconstruction. StatPearls. Accessed January 5, 2023. https:// www.ncbi.nlm.nih.gov/books/NBK551717/
- American Burn Association. Guidelines for burn patient referral. Accessed January 9, 2023. https://ameriburn.org/resources/ burnreferral/
- Bittner EA, Shank E, Woodson L, Martyn JA. Acute and perioperative care of the burn-injured patient. Anesthesiology. 2015;122(2):448-464.
- International Society for Burn Injury Practice Guidelines Committee; Steering Subcommittee; Advisory Subcommittee. ISBI practice guidelines for burn care. Burns. 2016;42(5):953-1021.
- Jones SW, Williams FN, Cairns BA, Cartotto R. Inhalation injury: pathophysiology, diagnosis, and treatment. Clin Plast Surg. 2017;44(3):505-511.
- Guilabert P, Usúa G, Martı´n N, et al. Fluid resuscitation management in patients with burns: update. Br J Anaesth. 2016;117(3): 284-296.
- Barrow RE, Jeschke MG, Herndon DN. Early fluid resuscitation improves outcomes in severely burned children. Resuscitation. 2000;45:91-96.
- Swanson JW, Otto AM, Gibran NS, et al. Trajectories to death in patients with burn injury. J Trauma Acute Care Surg.2013;74(1):282-288.
- Comish P, Walsh M, Castillo-Angeles M, et al. Adoption of rescue colloid during burn resuscitation decreases fluid administered and restores end-organ perfusion. Burns. 2021;47(8):1844-1850.
- Palmieri TL, Holmes JH IV, Arnoldo B, et al. Transfusion Requirement in Burn Care Evaluation (TRIBE): a multicenter randomized prospective trial of blood transfusion in major burn injury. Ann Surg. 2017;266(4):595-602.
- Glas GJ, Levi M, Schultz MJ. Coagulopathy and its management in patients with severe burns. J Thromb Haemost. 2016; 14(5):865-874.
- Levi M, Toh CH, Thachil J, Watson HG. Guidelines for the diagnosis and management of disseminated intravascular coagulation. British Committee for Standards in Haematology. Br J Haematol. 2009;145(1):24-33.
- Palackic A, Duggan RP, Campbell MS, et al. The role of skin substitutes in acute burn and reconstructive burn surgery: an updated comprehensive review. Semin Plast Surg. 2022;12;36(1):33-42.
- Patterson DR, Sharar SR. Burn pain. In: Fishman SM, Ballantyne JC, Rathmell JP, eds. Bonica’s Management of Pain. 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2010:754.
- Attia A, Emam A, Atta T, et al. Lidocaine infusion for the treatment of burn pain: a review of recent updates. Burns Open.2022;6(4):195-199.
- Kipping B, Rodger S, Miller K, et al. Virtual reality for acute pain reduction in adolescents undergoing burn wound care: a prospective randomized controlled trial. Burns. 2012;38:650-657.
- Bishop S, Maguire S. Anaesthesia and intensive care for major burns. Contin Educ Anaesth Crit Care Pain. 2012;12(3): 118-122.
- Clark A, Imran J, Madni T, Wolf SE. Nutrition and metabolism in burn patients. Burns Trauma. 2017;17(5):11.
- Lachiewicz AM, Hauck CG, Weber DJ, Cairns BA, van Duin D. Bacterial infections after burn injuries: impact of multidrug resistance. Clin Infect Dis. 2017;29;65(12):2130-2136.
- Blanchet B, Jullien V, Vinsonneau C, et al. Influence of burns on pharmacokinetics and pharmacodynamics of drugs used in the care of burn patients. Clin Pharmacokinet. 2008;47(10):635-654.
- Jeevendra Martyn JA, Richtsfeld M, Warner DO. Succinylcholine-induced hyperkalemia in acquired pathologic states: etiologic factors and molecular mechanisms. Anesthesiology. 2006;104:158-169.
- Han TH, Martyn JA. Onset and effectiveness of rocuronium for rapid onset of paralysis in patients with major burns: priming or large bolus. Br J Anaesth. 2009;102(1):55-60.
- Martyn JAJ, Abernathy DA, Greenblatt DJ. Plasma protein binding of drugs after severe burns injury. Clin Pharm Ther. 1984; 35:535-539.
- Dumas EO, Pollack GM. Opioid tolerance development: a pharmacokinetic/pharmacodynamic perspective. AAPS J. 2008; 10(4):537-551.
- Goverman J, Mathews K, Goldstein R, et al. Adult contractures in burn injury. J Burn Care Res. 2017;38(1):e328-e336.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/